Contents
- What are clogged pores
What are clogged pores
Clogged pores also called comedones are the skin-coloured, small bumps (papules) frequently found on the forehead and chin of those with acne. Comedones (the plural of comedo) can be open (blackheads) or closed by skin (whiteheads), and can occur with acne or without acne.
Clogged pores (comedones) are dilated or widened hair follicles (pores) in the skin. Keratin (skin debris) combines with oil and bacteria to clog the follicles.
- Open comedones are blackheads; black because of surface pigment (melanin), rather than dirt. The keratinous contents can be expressed or extracted.
- Closed comedones are whiteheads; the follicle is completely blocked and are uninflamed skin-coloured papules. They must be punctured to remove their contents.
- Microcomedones are so small that they are not visible to the naked eye
- Macrocomedones are facial closed comedones that are larger than 2–3 mm in diameter
- A giant comedo is a type of cyst in which there is a clear blackhead-like opening in the skin
- Solar comedones are found on the cheeks and chin of older people, and are thought to be due to sun damage.
What is comedonal acne ?
Comedonal acne is a pattern of acne in which most lesions are comedones. Comedonal acne most often affects the forehead and chin.
What are solar comedones ?
Solar or senile comedones arise on the face of the middle-aged and elderly. They affect areas that have been exposed to sunlight over a long period of time, particularly the cheeks, which may become yellow and leathery (solar elastosis).
The comedones may be open (blackheads) or closed (whiteheads). There may also be larger cysts.
Solar comedones are not related to acne vulgaris and do not usually become inflamed. They are however very persistent.
Figure 1. Clogged pores on forehead (open comedones – “blackheads”)

Figure 2. Clogged pores on face (closed comedones – “whiteheads”)

What causes clogged pores ?
Clogged pores (comedones) arise when cells lining the sebaceous duct proliferate (cornification), and there is increased sebum production. A comedo is formed by the debris blocking the sebaceous duct and hair follicle. It is now known that comedones also involve inflammation (see causes of acne).
The development of comedones may involve the following factors:
- Excessive activity of the male sex hormone 5-testosterone (DHT) within skin cells
- Reduced linoleate (the salt of the essential fatty acid, linoleic acid) in sebum causing more scale and reduced barrier function
- Proinflammatory cytokines (cell signalling proteins), such as Interleukin 1 (IL-1) and IL-8, produced by cells lining the follicle in response to activation of the innate immune system
- Free fatty acids made from sebum by acne bacteria
- Overhydrated skin premenstrually, from moisturisers or in humid conditions
- Contact with certain chemicals including oily pomades, isopropyl myristate, propylene glycol and some dyes in cosmetics
- Rupture of the follicle by injury such as squeezing pimples, abrasive washing, chemical peels or laser treatments
- Smoking – comedonal acne is more common in smokers than in non-smokers
- Certain dietary factors may contribute to comedonal acne, particularly milk products and high glycemic-index foods (sugars and fats)
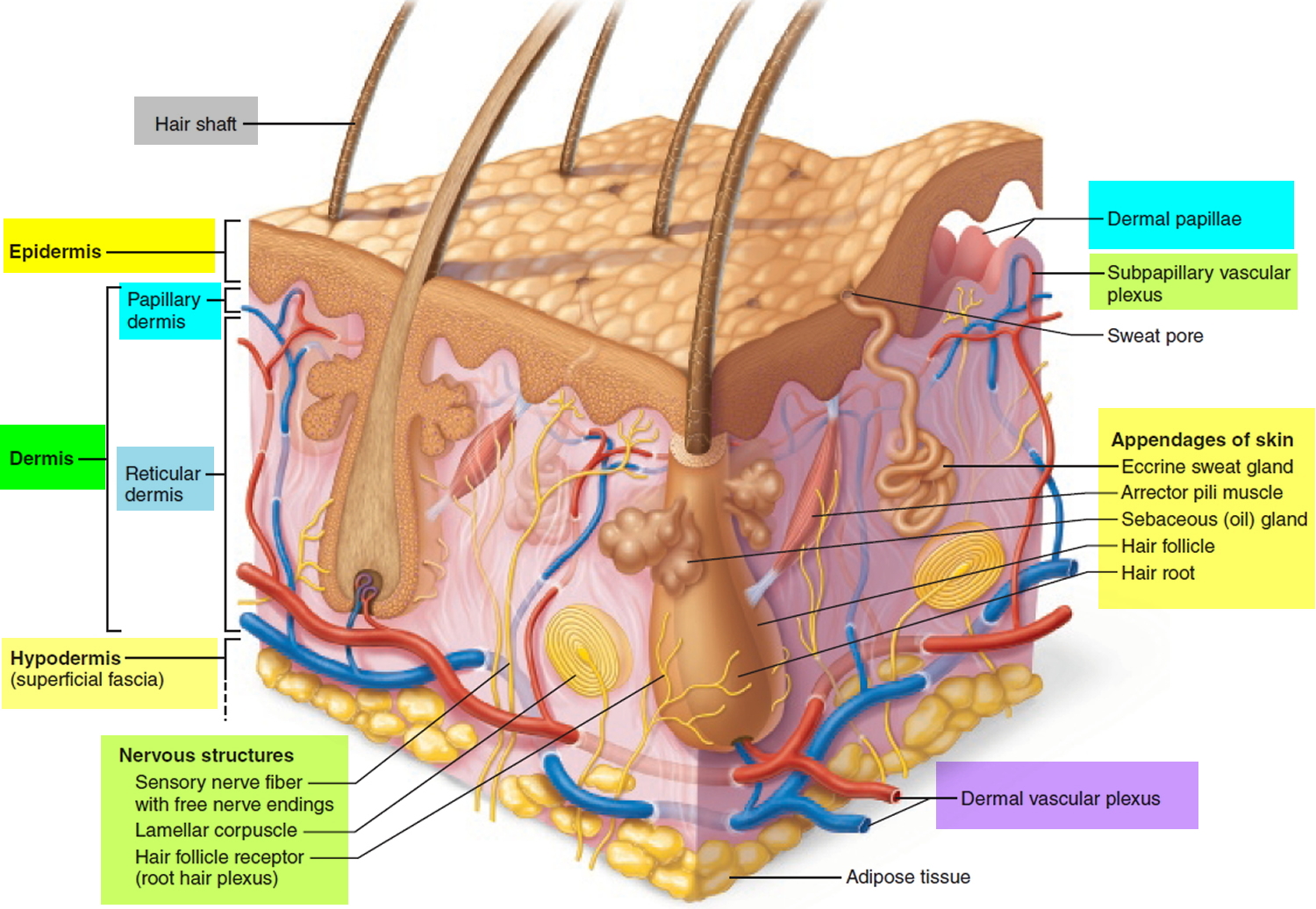
Figure 3. Skin and Hair structure
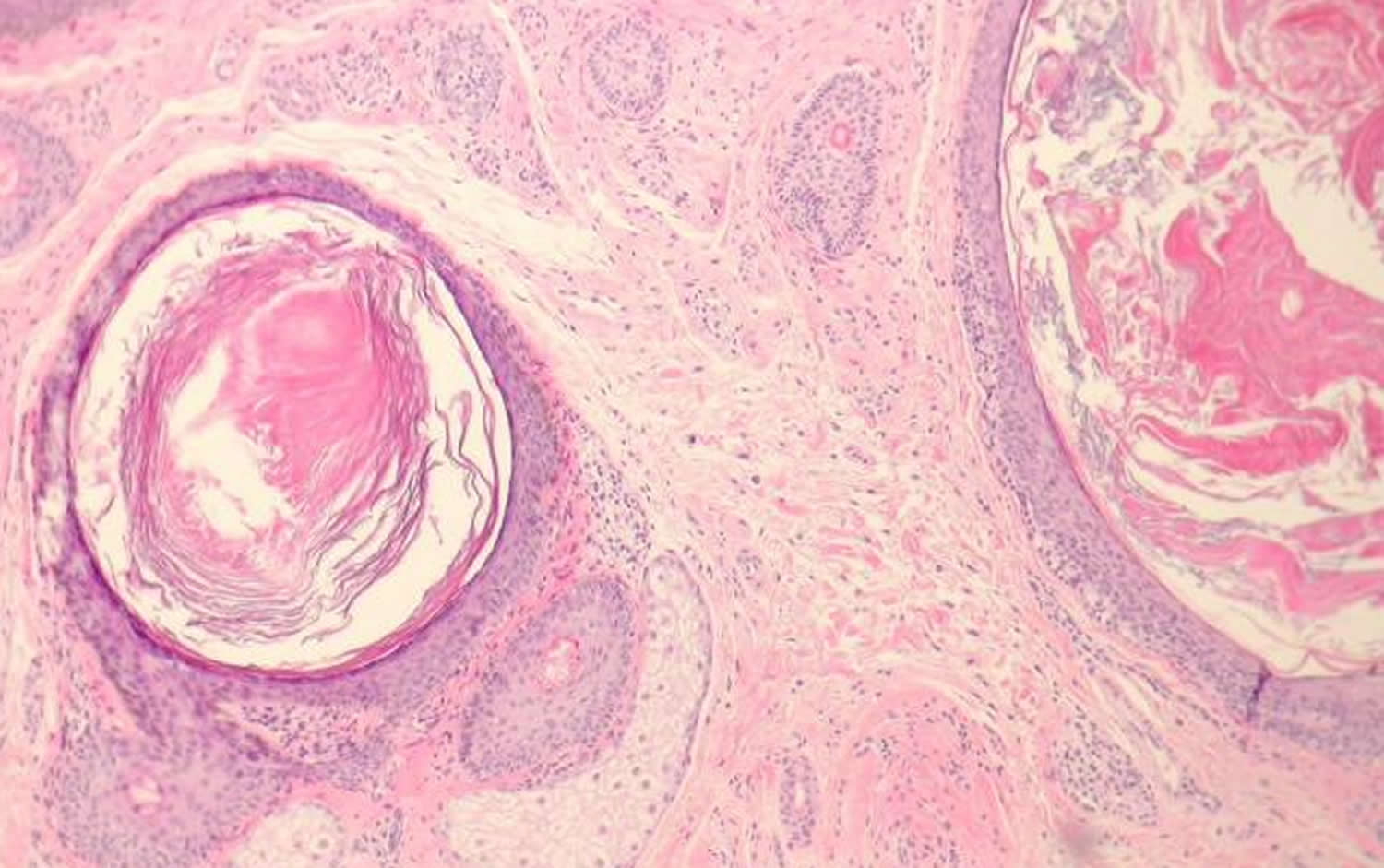
Histology of comedonal cyst
Sections of open comedones show massive follicular dilation (figure 4). The dilated follicles are filled with keratin. These may be filled with cellular debris and/or inflammatory cells. Closed comedones do not show a patent follicular channel to the surface.
Figure 4. Clogged pores histology
What is clogged pores treatment / treatment for comedonal acne ?
If you have comedonal acne, choose oil-free cosmetics and wash twice daily with a mild soap and water. It is best to stop smoking and to have a diet that is low in sugar, fat and dairy products.
Choose “comedolytic” topical medications. These should be applied once or twice daily as a thin smear to the entire area affected. It may take several weeks to months before worthwhile improvement occurs. Treatment needs to be continued long-term (sometimes for many years).
Suitable topical agents include:
- Benzoyl peroxide
- Azelaic acid
- Salicylic acid +/- sulfur and resorcinol
- Glycolic acid
- Retinoids such as tretinoin, isotretinoin, adapalene (these require a doctor’s prescription)
Benzoyl peroxide
Benzoyl peroxide is an over-the-counter bactericidal agent that comes in a wide array of concentrations and formulations. No particular form has been proven better than another 1. Benzoyl peroxide is unique as an antimicrobial because it is not known to increase bacterial resistance 2. It is most effective for the treatment of mild to moderate mixed acne when used in combination with topical retinoids 3. Benzoyl peroxide may also be added to regimens that include topical and oral antibiotics to decrease the risk of bacterial resistance 3. Salicylic acid is present in a variety of over-the-counter cleansing products. These products have anticomedonal properties and are less potent than topical retinoids, but there have been only limited high-quality studies examining their effectiveness 1.
Azelaic acid
Azelaic acid should be considered for use in pregnant women. The cream formulation (Azelex) is approved by the U.S Food and Drug Administration (FDA) for the treatment of acne vulgaris, but the gel (Finacea) has significantly better bioavailability 1. It has mixed antimicrobial and anticomedonal effects, and may be effective for the treatment of mild to moderate inflammatory or mixed acne 4.
Salicylic acid
Salicylic acid belongs to a group of medicines known as keratolytics. It is used in the treatment of scaly skin diseases where the skin has become thickened, scaly and flaky. Topical preparations of salicylic acid, either alone or in combination with other medicines, can be used to treat the following common scaly skin conditions:
- Viral warts
- Psoriasis
- Seborrhoeic dermatitis
- Chronic atopic dermatitis
- Lichen simplex
- Ichthyosis
- Acne
In acne, topical salicylic acid helps slow down shedding of the cells inside the follicles, preventing clogging. Salicylic acid also helps break down blackheads and whiteheads.
Salicylic acid works by softening keratin, a protein that forms part of the skin structure. This helps to loosen dry scaly skin making it easier to remove. When salicylic acid is used in combination with other medicines it takes off the upper layer of skin allowing the additional medicines to penetrate more effectively.
Salicylic acid preparations come in many forms and strengths from 0.5% up to 30%. For acne use salicylic acid 0.5% oil-free acne wash (Neutrogena®).
Topical retinoids
Topical retinoids are versatile agents in the treatment of acne (Table 1) 5, 6. They prevent the formation and reduce the number of comedones, making them useful against noninflammatory lesions. Topical retinoids also possess anti-inflammatory properties, making them somewhat useful in the treatment of inflammatory lesions 5. Topical retinoids are indicated as monotherapy for noninflammatory acne and as combination therapy with antibiotics to treat inflammatory acne. Additionally, they are useful for maintenance after treatment goals have been reached and systemic drugs are discontinued. Overall, adapalene (Differin) is the best tolerated topical retinoid. Limited evidence suggests that tazarotene (Tazorac) is more effective than adapalene and tretinoin (Retin-A). There is no evidence that any formulation is superior to another 5.
Many brand-name creams containing the retinoids retinol and retinaldehyde can be obtained over the counter at pharmacies and supermarkets.
Adapalene gel has received approval from the FDA in the USA for over-the-counter use of acne treatment in patients 12 or older (July 2016).
Adapalene is also available to treat acne in combination with benzoyl peroxide, as Epiduo® gel.
The more potent topical retinoids available on prescription are:
- ReTrieve™ cream (tretinoin)
- Retin-A™ Cream (tretinoin or retinoic acid)
- Retinova™ Cream (tretinoin emollient)
- Isotrex™ Gel (isotretinoin)
- Differin™ Gel, Cream (adapalene).
Table 1. Selected Topical Retinoids for the Treatment of clogged pores
| Agent | FDA pregnancy category | Adverse effects | Available formulations | Estimated cost generic (brand)* |
|---|---|---|---|---|
Adapalene (Differin) | C | Local erythema, peeling, dryness, pruritus, stinging | Cream, lotion (0.1%) | $125 ($363) |
Gel (0.1%, 0.3%) | ||||
Adapalene/benzoyl peroxide (Epiduo) gel (0.1%/2.5%) | NA ($269) | |||
Tazarotene (Tazorac) | X | Local erythema, peeling, dryness, pruritus, stinging | Cream, gel (0.05%, 0.1%) | NA ($240) |
Tretinoin (Retin-A) | C | Local erythema, peeling, dryness, pruritus, stinging | Cream (0.025%, 0.05%, 0.1%) | $27 ($130) |
Gel (0.01%, 0.025%, 0.05%) | $24 ($19 to $105) | |||
Microsphere gel (0.04%, 0.1%) | NA ($170) |
FDA = U.S. Food and Drug Administration; NA = not available.
*—Estimated retail price of one month’s treatment based on information obtained at http://www.lowestmed.com.
Prescription oral medications for comedonal acne include:
- Hormonal therapy
- Isotretinoin
Antibiotics can also improve comedonal acne but are usually prescribed for inflammatory acne (acne vulgaris).
Oral isotretinoin
Oral isotretinoin is FDA-approved for the treatment of severe recalcitrant acne. Evidence suggests that it is also useful for less severe acne that is treatment resistant 1. The usual dosage for severe treatment-resistant acne is 0.5 to 1.0 mg per kg per day for about 20 weeks, or a cumulative dose of 120 mg per kg 7. Initial flare-ups can be minimized with a beginning daily dosage of 0.5 mg or less per kg 1. Total cumulative doses of less than 120 mg increase relapse rates, and doses of more than 150 mg increase the incidence of adverse effects without producing greater benefits 7. Approximately 40 percent of patients achieve long-term remission with a 120-mg cumulative dose, 40 percent require retreatment with topical therapy or oral antibiotics and 20 percent require retreatment with isotretinoin 8. Patients with moderate acne may respond to lower dosages (0.3 mg per kg per day) and experience fewer adverse effects 9.
Physicians, distributors, pharmacies, and patients must register in the iPLEDGE program (http://www.ipledgeprogram.com) before using isotretinoin. This program was established to prevent pregnancy in patients taking the medication. Isotretinoin is a potent teratogen (an agent which causes malformation of an embryo) and is associated with abnormalities of the face, eyes, ears, skull, central nervous system, cardiovascular system, thymus, and parathyroid glands. Negative pregnancy tests are mandated before starting therapy, then monthly before receiving a prescription refill, immediately after taking the last dose and one month after taking the last dose. The use of isotretinoin has been suggested to worsen depression and increase the risk of suicide, but no causal relationship has been established 1. Required laboratory monitoring during therapy includes a complete blood count, fasting lipid panel, and measurement of liver transaminase levels. Common adverse effects include headaches, dry skin and mucous membranes, and gastrointestinal upset 10.
Oral contraceptives (birth control pills)
Several estrogen-containing oral contraceptives are FDA-approved for the treatment of acne 10. These agents generally are considered second-line therapies, but they may be considered first-line treatments in women with adult-onset acne or perimenstrual flare-ups 11. A 2009 Cochrane review found that these agents are effective in reducing inflammatory and noninflammatory lesions. However, there is insufficient evidence to recommend one agent over another, including those that are FDA approved versus those that are not. There is also no evidence to support their use over other studied therapies 1.
Spironolactone (Aldactone)
Spironolactone (Aldactone) is an androgen receptor antagonist with unclear effectiveness in the treatment of acne. It is usually reserved as a second- or third-line agent, or as an alternative to isotretinoin for women who cannot use this medication. A 2009 systematic review found insufficient evidence to recommend the use of spironolactone for the treatment of acne 12. Common adverse effects include menstrual irregularities and breast tenderness. It is a potassium-sparing diuretic and may cause severe hyperkalemia. Additionally, it is a potential teratogen (an agent which causes malformation of an embryo) 13.
Surgical treatments are sometimes recommended to remove persistent comedones:
- Cryotherapy
- Electrosurgery (cautery or diathermy)
- Microdermabrasion.
- Strauss JS, Krowchuk DP, Leyden JJ, American Academy of Dermatology/American Academy of Dermatology Association, et al. Guidelines of care for acne vulgaris management. J Am Acad Dermatol. 2007;56(4):651–663.[↩][↩][↩][↩][↩][↩][↩]
- Thiboutot D, Zaenglein A, Weiss J, Webster G, Calvarese B, Chen D. An aqueous gel fixed combination of clindamycin phosphate 1.2% and benzoyl peroxide 2.5% for the once-daily treatment of moderate to severe acne vulgaris: assessment of efficacy and safety in 2813 patients. J Am Acad Dermatol. 2008;59(5):792–800.[↩]
- Thiboutot D, Gollnick H, Bettoli V, et al. New insights into the management of acne: an update from the Global Alliance to Improve Outcomes in Acne group. J Am Acad Dermatol. 2009;60(5 suppl):S1–S50.[↩][↩]
- Frampton JE, Wagstaff AJ. Azelaic acid 15% gel: in the treatment of papulopustular rosacea. Am J Clin Dermatol. 2004;5(1):57–64.[↩]
- Thielitz A, Abdel-Naser MB, Fluhr JW, Zouboulis CC, Gollnick H. Topical retinoids in acne—an evidence-based overview. J Dtsch Dermatol Ges. 2008;6(12):1023–1031.[↩][↩][↩]
- Hamilton RJ. Tarascon Pocket Pharmacopoeia. Sudbury, Mass.: Jones & Bartlett; 2011.[↩]
- Strauss JS, Rapini RP, Shalita AR, et al. Isotretinoin therapy for acne: results of a multicenter dose-response study. J Am Acad Dermatol. 1984;10(3):490–496.[↩][↩]
- White GM, Chen W, Yao J, Wolde-Tsadik G. Recurrence rates after the first course of isotretinoin. Arch Dermatol. 1998;134(3):376–378.[↩]
- Amichai B, Shemer A, Grunwald MH. Low-dose isotretinoin in the treatment of acne vulgaris. J Am Acad Dermatol. 2006;54(4):644–646.[↩]
- James WD. Clinical practice. Acne. N Engl J Med. 2005;352(14):1463–1472.[↩][↩]
- Katsambas AD, Dessinioti C. Hormonal therapy for acne: why not as first line therapy? Facts and controversies. Clin Dermatol. 2010;28(1):17–23.[↩]
- Brown J, Farquhar C, Lee O, Toomath R, Jepson RG. Spironolactone versus placebo or in combination with steroids for hirsutism and/or acne. Cochrane Database Syst Rev. 2009(2):CD000194.[↩]
- Aldactone [package insert]. New York, NY: Pfizer Inc.; 2011.[↩]





{kind=link}