
Contents
- What causes vaginal odor
What causes vaginal odor
Vaginitis is an inflammation or infection of the vagina that can cause itching, burning, pain, discharge, and bad odor 1. Vaginitis is also called vaginal infection or vaginal inflammation.
The vagina is the tubelike passage that connects the opening of the womb to the outside of a woman’s body. It is sometimes called the “birth canal.” There are a several types of vaginitis, each with its own causes, symptoms, and treatments.
As many as one third of women will have symptoms of vaginitis sometime during their lives 2. Vaginitis affects women of all ages but is most common during the reproductive years. Vaginal symptoms are a common reason women seek medical care. There are many types of vaginitis, each with its own cause, symptoms, and treatment. Pregnant women with some types of vaginitis may be at higher risk of preterm birth.
What is the Vagina
The vagina is a long fibromuscular canal about 8 to 10 cm long that allows for the discharge of menstrual fluid, receipt of the penis and semen, and birth of a baby. The vaginal wall is thin but very distensible. It consists of an outer adventitia, a middle muscularis, and an inner mucosa. The vagina tilts posteriorly between the urethra and rectum; the urethra is bound to its anterior wall. The vagina has no glands, but it is lubricated by the seepage of serous fluid through its walls (transudation) and by mucus from the cervical glands above it.
The mucosa of the vagina is continuous with that of the uterus. Histologically, it consists of nonkeratinized stratified squamous epithelium and areolar connective tissue that lies in a series of transverse friction ridges called rugae or vaginal rugae, which contribute to both male and female stimulation during intercourse (see Figures 1 and 2). Dendritic cells in the mucosa are antigen-presenting cells. Unfortunately, they also participate in the transmission of viruses—for example, HIV (the virus that causes AIDS)—to a female during intercourse with an infected male. The mucosa of the vagina contains large stores of glycogen, the decomposition of which produces organic acids. The resulting acidic environment retards microbial growth, but it also is harmful to sperm. Alkaline components of semen, mainly from the seminal vesicles, raise the pH of fluid in the vagina and increase viability of the sperm.
The vagina extends slightly beyond the cervix and forms blindended spaces (recesses) called fornices surrounding it. The fornix (= arch or vault) surrounds the vaginal attachment to the cervix. When properly inserted, a contraceptive diaphragm rests in the fornix, where it is held in place as it covers the cervix.
The lower end of the vagina at the vaginal orifice, the mucosa folds inward and forms a membrane, the hymen, which stretches across the opening. The hymen has one or more openings to allow discharge of menstrual fluid, but it usually must rupture to allow for intercourse. A little bleeding often accompanies the first act of intercourse; however, the hymen is commonly ruptured before then by tampons, medical examinations, or strenuous exercise.
Figure 1. Vagina
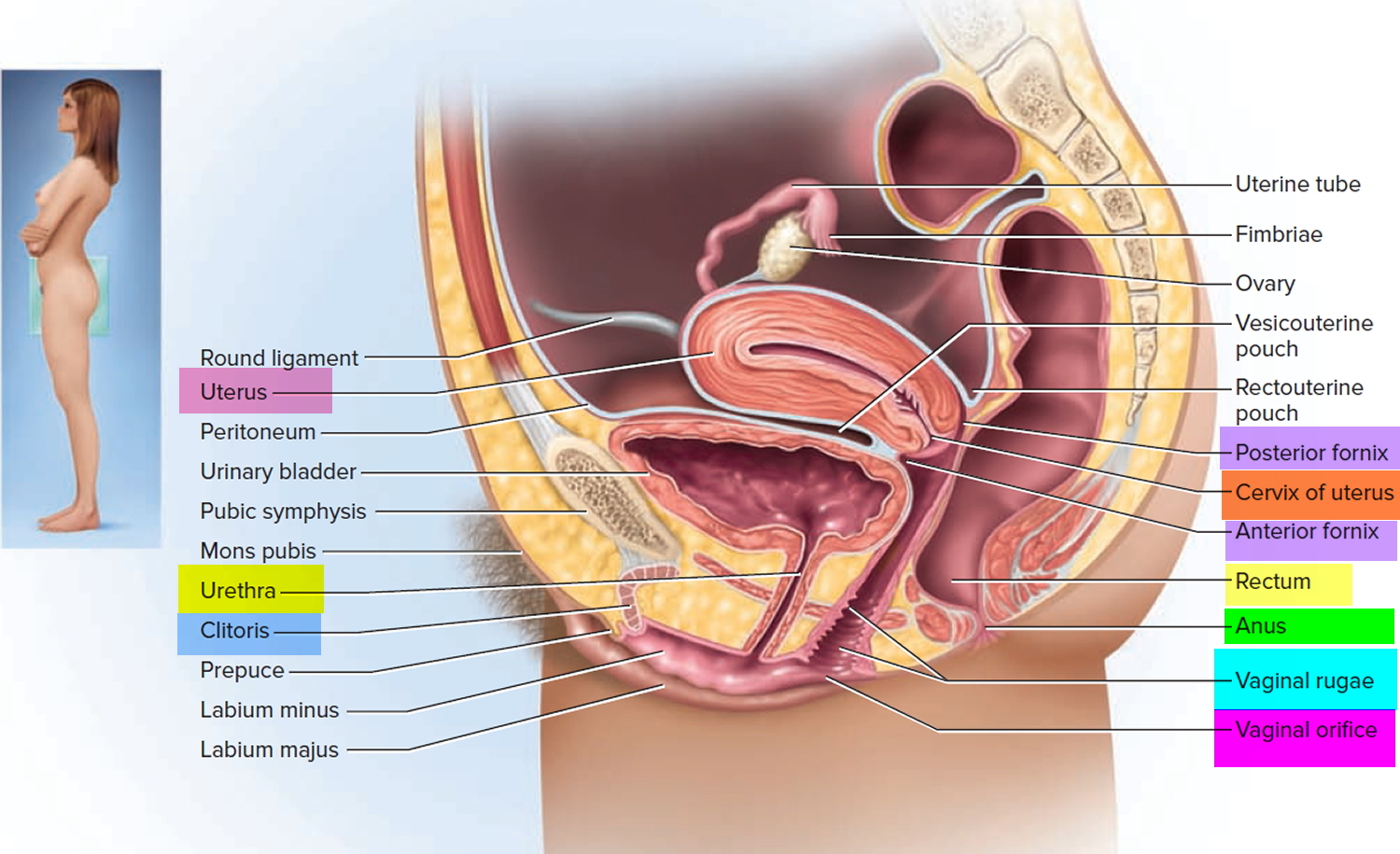
Note: The vagina communicates with the uterus by way of a narrow passage through the cervix called the cervical canal.
The vaginal epithelium is simple cuboidal in childhood, but the estrogens of puberty transform it into a stratified squamous epithelium. This is an example of metaplasia, the transformation of one tissue type to another. The epithelial cells are rich in glycogen.
Bacteria ferment this to lactic acid, which produces a low vaginal pH (about 3.5–4.0) that inhibits the growth of pathogens. This acidity is neutralized by the semen so it doesn’t harm the sperm. The mucosa also has antigen-presenting dendritic cells, which aid in immunity at this body orifice, but unfortunately are also a route by which HIV can invade the female body.
Figure 2. Lining of the vagina
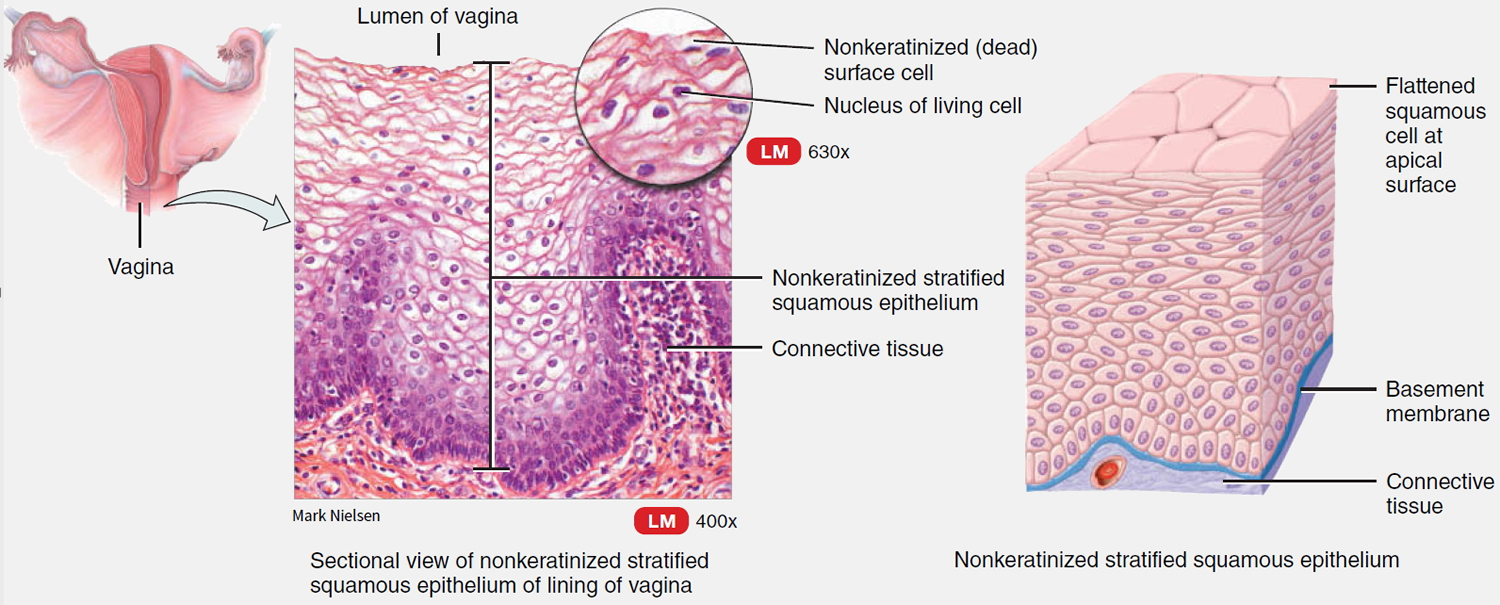
Note: The pH of the vagina is about 3.5 to 4.0.
What can cause vaginal odor ?
Vaginitis is often caused by infections. Some vaginal infections are passed through sexual contact. Some infections occur if there is a change in the balance of organisms normally found in the vagina 3.
In about 90% of affected women, vaginitis is caused by one of these types of infection 4:
- Bacterial vaginosis is the most common vaginal infection in women of childbearing age. It occurs when there are too many harmful (bad) bacteria and too few protective (good) bacteria in the vagina 5.
- Candida or “yeast” infection occurs when too much Candida grows in the vagina. Candida is yeast, which is a type of fungus frequently present in the vagina 6.
- Trichomoniasis. Trichomoniasis is a sexually transmitted disease caused by a single-cell parasite.
Vaginitis has other causes, too. For instance, some women are sensitive or allergic to vaginal sprays, douches, spermicides, soaps, detergents, and fabric softeners. These products can cause burning, itching, and discharge, even if there is no infection. Women also can have vaginal irritation caused by the natural lessening in estrogen levels during breast-feeding and after menopause.
A woman may have more than one cause of vaginitis at the same time 5.
How many women are affected by vaginitis ?
Most women will have vaginitis at some point in their lives. In the United States
- About 30% of women of childbearing age have bacterial vaginosis 7
- Nearly 75% of all adult women have had at least one yeast infection in their lifetime 8
- About 3% of women of childbearing age have trichomoniasis 9
Many women with vaginal infections have no symptoms. For instance, only 16% of women with bacterial vaginosis report vaginal symptoms. For every 100 women who do have symptoms such as pain, itching, and discharge 10.
- 40 to 45 women have bacterial vaginosis.
- 20 to 25 women have a yeast infection.
- 15 to 20 women have trichomoniasis.
Who gets vaginitis and who is at risk ?
Vaginitis affects women of all ages, races, and backgrounds. Some factors may increase a woman’s risk of getting certain types of vaginitis.
- A woman’s risk of getting bacterial vaginosis is higher if 11
- She has a new sex partner.
- She has more than one sex partner.
- She douches.
- A woman’s risk of getting a yeast infection is higher if 12
- She is pregnant.
- She has diabetes that is not controlled.
- She uses oral birth control (“the pill”).
- She douches or uses vaginal sprays.
- She uses certain antibiotics or steroid medicines.
- She has a weakened immune system, such as from HIV.
- A woman’s risk of getting trichomoniasis is higher if 13
- She has a new sex partner.
- She has more than one sex partner.
- She has a history of sexually transmitted diseases.
What are the symptoms of vaginitis ?
Symptoms depend on the type of vaginitis a woman has 10:
Bacterial vaginosis often causes a thin, milky discharge from the vagina that may have a “fishy” odor. It may also cause itching. Most women have no symptoms and only find out they have it during a routine gynecologic exam.
Yeast infections produce a thick, white discharge from the vagina that can look like cottage cheese. The discharge can be watery and often has no smell. Yeast infections usually cause the vagina and vulva to become itchy and red.
Trichomoniasis can cause itching, burning, and soreness of the vagina and vulva, as well as burning during urination. Some women have a “frothy” gray-green discharge, which may smell bad. Many women have no symptoms.
How do health care providers diagnose vaginitis ?
The most common infectious causes of vaginitis are bacterial vaginosis, vulvovaginal candidiasis, and trichomoniasis. Physicians traditionally diagnose vaginitis using the combination of symptoms, physical examination, pH of vaginal fluid, microscopy, and the whiff test. When combined, these tests have a sensitivity and specificity of 81 and 70 percent, respectively, for bacterial vaginosis; 84 and 85 percent for vulvovaginal candidiasis; and 85 and 100 percent for trichomoniasis when compared with the DNA probe standard 14.
Table 1 describes common causes, symptoms, and signs of vaginitis and Table 2 lists risk factors that contribute to the development of the condition.
Table 1. Causes, Symptoms, and Signs of Vaginal Odor
| Causes, Symptoms, and Signs of Vaginal Odor | |
| Type | Causes |
| Bacterial vaginosis | Gardnerella vaginalis, Mycoplasma hominis Anaerobic bacteria: Prevotella species, Mobiluncus species |
| Clinical symptoms: | |
| Discharge: | Malodorous; homogenous; clear, white, or gray; fishy odor |
| Pain: | Not primary symptom |
| Pruritus: | Not primary symptom |
| Clinical signs: | |
| Vagina: | No signs of inflammation |
| Vulva: | Unaffected |
| Type | Causes |
| Trichomoniasis | Trichomonas vaginalis |
| Clinical symptoms: | |
| Discharge: | Green-yellow, frothy |
| Pain: | Pain with sexual intercourse, vaginal soreness, dysuria |
| Pruritus: | Not primary symptom |
| Clinical signs: | |
| Vagina: | Signs of inflammation, “strawberry cervix” |
| Vulva: | Vestibular erythema may be present |
| Type | Causes |
| Vulvovaginal candidiasis | Candida albicans, Candida krusei, Candida glabrata |
| Clinical symptoms: | |
| Discharge: | White, thick, lack of odor |
| Pain: | Burning, dysuria, dyspareunia |
| Pruritus: | Frequent |
| Clinical signs: | |
| Vagina: | Signs of inflammation, edema |
| Vulva: | Excoriations |
| Type | Causes |
| Atrophic vaginitis | Estrogen deficiency |
| Clinical symptoms: | |
| Discharge: | Yellow, greenish, lack of odor |
| Pain: | Vaginal dryness, pain with sexual intercourse |
| Pruritus: | Rare |
| Clinical signs: | |
| Vagina: | Vagina mildly erythematous, easily traumatized |
| Vulva: | Vestibule thin and dry; labia majora lose their subcutaneous fat; labia minora irritated and friable |
| Type | Causes |
| Erosive lichen planus | Etiology is unknown |
| Clinical symptoms: | |
| Discharge: | Yellow or gray |
| Pain: | Intense pain, dyspareunia, postcoital bleeding |
| Pruritus: | Intense |
| Clinical signs: | |
| Vagina: | Erythema with friable epithelium |
| Vulva: | Erosions, white plaques |
| Type | Causes |
| Irritant or allergic contact dermatitis | Contact irritation or allergic reaction with episodic flares |
| Clinical symptoms: | |
| Discharge: | Minimal |
| Pain: | Burning on acute contact, soreness |
| Pruritus: | More likely in allergic reactions |
| Clinical signs: | |
| Vagina: | Vulvar erythema possible |
| Vulva: | Erythema with or without edema; vesicles or bullae rare |
Table 2. Risk Factors Contributing for Vaginitis
| Type of vaginitis | Risk factors |
|---|---|
Bacterial vaginosis | Low socioeconomic status, vaginal douching, smoking, use of an intrauterine contraceptive device, new/multiple sex partners, unprotected sexual intercourse, homosexual relationships, frequent use of higher doses of spermicide nonoxynol-9 |
Trichomoniasis | Low socioeconomic status, multiple sex partners, lifetime frequency of sexual activity, other sexually transmitted infections, lack of barrier contraceptive use, illicit drug use, smoking |
Vulvovaginal candidiasis | Vaginal or systemic antibiotic use, diet high in refined sugars, uncontrolled diabetes mellitus |
Atrophic vaginitis | Menopause, other conditions associated with estrogen deficiency, oophorectomy, radiation therapy, chemotherapy, immunologic disorders, premature ovarian failure, endocrine disorders, antiestrogen medication |
Irritant contact dermatitis | Soaps, tampons, contraceptive devices, sex toys, pessary, topical products, douching, fastidious cleansing, medications, clothing |
Allergic contact dermatitis | Sperm, douching, latex condoms or diaphragms, tampons, topical products, medications, clothing, atopic history |
In a review of studies published between 1966 and 2003, bacterial vaginosis was diagnosed in 22 to 50 percent of symptomatic women, vulvovaginal candidiasis in 17 to 39 percent, and trichomoniasis in 4 to 35 percent 15. Approximately 30 percent of symptomatic women remained undiagnosed after clinical evaluation 16. Among multiple individual symptoms and signs, only the following were found to be helpful for the diagnosis of vaginitis in symptomatic women 16:
- A lack of itching makes diagnosis of vulvovaginal candidiasis unlikely.
- A lack of perceived odor makes bacterial vaginosis unlikely.
- Presence of inflammatory signs is more commonly associated with vulvovaginal candidiasis.
- Presence of a fishy odor on examination is predictive of bacterial vaginosis.
- Lack of odor is associated with vulvovaginal candidiasis.
Individual symptoms and signs, pH level, and microscopy results often do not lead to an accurate diagnosis of vaginitis. Laboratory tests perform better than standard office-based evaluation for diagnosing causes of vaginitis 16, but they do not add substantially to the treatment threshold and are justified only in patients with recurrent or difficult-to-diagnose symptoms.
Table 3 describes laboratory tests used to diagnose infectious causes of vaginitis 16.
A cost-effectiveness analysis of diagnostic strategies for vaginitis undiagnosed by pelvic examination, wet-mount preparation, and related office tests showed that the least expensive strategy was to perform yeast culture, gonorrhea and chlamydia probes at the initial visit, and Gram stain and Trichomonas culture only when the vaginal pH exceeded 4.9. Other strategies cost more and increased duration of symptoms by up to 1.3 days 17.
Table 3. Laboratory Testing for Infectious Causes of Vaginitis
| Test | Bacterial vaginosis | Trichomoniasis | Vulvovaginal candidiasis | Cost* |
|---|---|---|---|---|
Point-of-care tests* | ||||
Amsel criteria | Sensitivity, 69%; specificity, 93% | NA | NA | $$ |
pH | pH > 5: sensitivity, 77%; specificity, 35% | pH > 5.4: sensitivity, 92%; specificity, 51% | pH < 4.9: sensitivity, 71%; specificity, 90% | $ |
Whiff test (the amine odor produced by mixing 10% potassium hydroxide solution with a sample of vaginal discharge) | Positive test: sensitivity, 67%; specificity, 93% | Positive test: sensitivity, 67%; specificity, 65% | Negative test | $ |
Fem Exam card (Cooper Surgical, Shelton, Conn.) Two colorimetric strips: card 1 measures pH and amine levels; card 2 measures proline aminopeptidase activity | Cards 1 and 2 combined: sensitivity, 91%; specificity, 61% | NA | NA | $$ |
Rapid (two minutes), less subjective than whiff test, easily performed | ||||
Microscopy (with 10% potassium hydroxide solution, saline) | Clue cells, bacilli with corkscrew motility, scant or absent lactobacilli | Motile protozoa with flagella; more leukocytes than epithelial cells | Budding filaments, mycelia with 10% potassium hydroxide solution | $ |
Sensitivity, 53 to 90%; specificity, 40 to 100% | Sensitivity, 50 to 70% (may be increased by vaginal lavage to 74%); specificity, 100% | Sensitivity, 61%; specificity, 77% | ||
pH, trimethylamine card (QuickVue Advance Quidel, San Diego, Calif.) | Sensitivity, 53%; specificity, 97% | NA | NA | $ |
Rapid, simple, comparable with pH and whiff test | ||||
Proline aminopeptidase card (Pip Activity TestCard, Litmus Concepts, Inc., Santa Clara, Calif.) Indirect test for a chemical produced by the organisms associated with bacterial vaginosis | Sensitivity, 70%; specificity, 81% | NA | NA | $ |
Rapid, simple, comparable with Fem Exam card 2 | ||||
OSOM Trichomonas Rapid Test (Genzyme Diagnostics, Cambridge, Mass.), uses color immunochromatographic “dipstick” technology with murine monoclonal antibodies | NA | Sensitivity, 90 to 100% 10 minutes to complete test | NA | $$$ |
BD Affirm VPIII Microbial Identification Test (BD Diagnostic Systems, Sparks, Md.) | Sensitivity, 95 to 100% 45 minutes to complete test | Sensitivity, 90 to 100% | Sensitivity, 90 to 100% | $$$ |
False-positive results may occur, especially in low-prevalence groups | ||||
Polymerase chain reaction: based on DNA amplification (Quest Diagnostics, Madison N.J.), Instagene Matrix (Bio-Rad Laboratories, Hercules, Calif.) | Effective at identifying bacteria responsible for bacterial vaginosis | Sensitivity, 80%; specificity, 97% | Polymerase chain reaction more sensitive than culture in detecting Candida; not yet commercially available as a diagnostic test | $$$ |
Reference laboratory testing* | ||||
Culture | Predictive value of a positive Gardnerella vaginalis culture is less than 50%; generally not recommended, but may have value in recalcitrant cases | InPouch Culture System (Biomed, White City, Ore.) | Positive culture alone does not necessarily indicate that the yeast identified are responsible for vaginal symptoms | $$$ |
Combined wet-mount preparation and culture kit; can be kept at room temperature for up to 18 hours; samples taken during menses were not adversely affected | ||||
Sensitivity, 81 to 100% | ||||
Patient-performed tests | ||||
Over-the-counter test for vaginal infections (Fem-V; Synova Healthcare, Inc., New York, NY) | Positive test suggests possibility of bacterial vaginosis and need for physician visit (20% false-positive rate) | Positive test suggests possibility of trichomoniasis and need for physician visit (20% false-positive rate) | Negative test suggests possibility of yeast infection | $ |
Over-the-counter antifungal treatment recommended (10% false-negative rate) | ||||
Over-the-counter rapid yeast detection test (Savyon Diagnostics, Ashdod, Israel): uses the concept of lateral flow immunoassay systems | NA | NA | Positive test: sensitivity, 73%; specificity, 84% | $ |
Patient-performed tests have results similar to physician-performed tests | ||||
Negative test: not sensitive enough to rule out yeast infection and avoid a culture | ||||
NA = not applicable.
*—Relative cost of testing does not include physician office charges.
What is Bacterial Vaginosis
Bacterial vaginosis is the most prevalent cause of vaginal discharge or malodor, occurring in up to 30 percent of women 18. It occurs when the normal Lactobacillus species in the vagina are replaced with anaerobic bacteria, resulting in reduced levels of hydrogen peroxide and organic acids usually present in the vagina.
The underlying cause of bacterial vaginosis is not fully understood. More than 50 percent of women with bacterial vaginosis are asymptomatic. The fishy odor caused by production of amines from anaerobic bacteria found in many of these patients is predictive of bacterial vaginosis 16. When vaginal alkalinity increases after sexual intercourse (with the presence of semen) and during menses (with the presence of blood), the odor becomes more prevalent 19. Vaginal discharge is a more common but less specific symptom. Bacterial vaginosis is not associated with vaginal mucosal inflammation and rarely causes vulvar itch 19.
Bacterial vaginosis, even when asymptomatic, is associated with a high incidence of endometritis, sexually transmitted diseases and pelvic inflammatory disease following abortion and gynecologic procedures in the general population. Pelvic inflammatory disease, a serious disease that can harm a woman’s reproductive organs and cause infertility 20. Having bacterial vaginosis increases a woman’s risk of preterm labor and preterm birth. Women who have it also are more likely to get an infection after having surgery such as an abortion or hysterectomy 11. Among women with bacterial vaginosis, no overall increased risk of developing pelvic inflammatory disease has been found 21. Bacterial vaginosis is associated with late miscarriages, premature rupture of membranes, and preterm birth 22. Both symptomatic and asymptomatic bacterial vaginosis have been strongly linked with an increased risk of human immunodeficiency virus (HIV) transmission 23.
Diagnosis of bacterial vaginosis
In clinical practice, bacterial vaginosis is diagnosed by the presence of three out of four Amsel criteria 24:
- Thin, homogenous vaginal discharge
- Vaginal pH greater than 4.5
- Positive whiff test (fishy amine odor when 10 percent potassium hydroxide solution is added)
- At least 20 percent clue cells (vaginal epithelial cells with borders obscured by adherent coccobacilli on wet-mount preparation or Gram stain).
In a prospective observational study of 269 women, a vaginal pH of more than 4.5 was found to be the most sensitive (89 percent) and a positive whiff test was the most specific (93 percent) method of detecting bacterial vaginosis 25. The positive presence of these two tests is as sensitive as three or more Amsel criteria 25. Culture of Gardnerella vaginalis is not recommended because of low specificity. Cervical cytology has no clinical value for diagnosing bacterial vaginosis, especially in asymptomatic women, because it has low sensitivity 26.
Treatment in non-pregnant women
Current treatment recommendations from the Centers for Disease Control and Prevention (CDC) are listed in Table 4. Nonpregnant women with symptomatic disease require antibacterial therapy to relieve vaginal symptoms. Other benefits of treatment include decreasing the risk of HIV and other sexually transmitted infections and reducing infectious complications following abortion or hysterectomy 26.
Table 4. CDC Recommended Treatment of Vaginitis
| Medication/dosage | Cost per course of therapy | |||
|---|---|---|---|---|
Bacterial vaginosis | ||||
Recommended regimen | ||||
Metronidazole (Flagyl) | $$ | |||
500 mg orally twice daily for seven days | ||||
Metronidazole gel (Metrogel) | $$$ | |||
One full applicator (5 g) intravaginally once daily for five days | ||||
Clindamycin 2% cream | $$$ | |||
One full applicator (5 g) intravaginally at bedtime for seven days | ||||
Alternative regimen | ||||
Tinidazole (Tindamax) | $$$ | |||
2 g orally for two days or 1 g for five days | ||||
Clindamycin | $$$ | |||
300 mg orally twice daily for seven days | ||||
Clindamycin ovules | $$$ | |||
100 mg intravaginally once daily at bedtime for three days | ||||
Pregnancy* | ||||
Metronidazole | $$ | |||
500 mg orally twice daily for seven days | ||||
Metronidazole | $$ | |||
250 mg orally three times daily for seven days | ||||
Clindamycin | $$ | |||
300 mg orally twice daily for seven days | ||||
Trichomoniasis | ||||
Recommended regimen | ||||
Metronidazole | $ | |||
2 g orally in a single dose | ||||
Tinidazole | $$$ | |||
2 g orally in a single dose | ||||
Alternative regimen | ||||
Metronidazole | $$ | |||
500 mg orally twice daily for seven days | ||||
Pregnancy* | ||||
Metronidazole | $ | |||
2 g orally in a single dose | ||||
Vulvovaginal candidiasis, uncomplicated | ||||
Butoconazole 2% cream (Gynazole-1)† | $$ | |||
5 g intravaginally once daily for three days | ||||
Butoconazole 2% cream, sustained release | $ | |||
5 g intravaginally in a single dose | ||||
Clotrimazole 1% cream† | $ | |||
5 g intravaginally once daily for seven to 14 days | ||||
Clotrimazole 2% cream† | $ | |||
5 g intravaginally once daily for three days | ||||
Miconazole 2% cream† | $ | |||
5 g intravaginally once daily for seven days | ||||
Miconazole 4% cream† | $ | |||
5 g intravaginally once daily for three days | ||||
Miconazole vaginal suppository† | ||||
100-mg vaginal suppository once daily for seven days | $ | |||
200-mg vaginal suppository once daily for three days | $$ | |||
1,200-mg vaginal suppository in a single dose | $$ | |||
Nystatin vaginal tablet | $ | |||
100,000-unit vaginal tablet once daily for 14 days | ||||
Tioconazole 6.5% ointment† | $$ | |||
5 g intravaginally in a single dose | ||||
Terconazole 0.4% cream | $$ | |||
5 g intravaginally once daily for seven days | ||||
Terconazole 0.8% cream | $$ | |||
5 g intravaginally once daily for three days | ||||
Terconazole vaginal suppository | $$ | |||
80-mg vaginal suppository once daily for three days | ||||
Fluconazole (Diflucan) | $$ | |||
150 mg orally in a single dose | ||||
Vulvovaginal candidiasis, complicated | ||||
Recurrent | ||||
Initial regimen | ||||
Any topical agent | ||||
Seven to 14 days | ||||
Fluconazole | $$$ | |||
100, 150, or 200 mg orally once daily every third day for three doses | ||||
Maintenance regimen | ||||
Fluconazole | $$$ | |||
100, 150, or 200 mg orally once weekly for six months | ||||
Severe | ||||
Any topical azole | $$ | |||
Intravaginally once daily for seven to 14 days | ||||
Fluconazole | $$$ | |||
150 mg orally once daily in two doses 72 hours apart | ||||
Vulvovaginal candidiasis, nonalbicans | ||||
Nonfluconazole azole (oral or topical) | $ | |||
Seven to 14 days | ||||
Boric acid gelatin capsule | $$ | |||
Intravaginally once daily for 14 days | ||||
Pregnancy* | ||||
Any topical azole | $$ | |||
Intravaginally once daily for seven days | ||||
CDC = Centers for Disease Control and Prevention.
*—After counseling patients about the potential risks and benefits of treatment, preferably after 37 weeks of gestation.
†—Available over the counter.
A Cochrane review of 24 randomized controlled trials showed that clindamycin and metronidazole (Flagyl) are equally effective, achieving clinical cure in 91 and 92 percent of cases, respectively, after two to three weeks of treatment 27. Six randomized controlled trials showed topical and oral antibiotic preparations to be equally effective. One disadvantage of oral regimens is a longer duration of treatment 27. Intravaginal clindamycin cream is preferred in case of allergy or intolerance to metronidazole. Metronidazole in a single 2-g dose has the lowest effectiveness for treating bacterial vaginosis and is no longer recommended. Metronidazole, 500 mg twice daily for one week, is effective for treating bacterial vaginosis and trichomoniasis.
Although lactobacillus probiotics are safe, there is no conclusive evidence that they are superior to or enhance the effectiveness of antibiotics in the treatment of bacterial vaginosis or prevent its recurrence 28. Treatment of sex partners and follow-up visits if symptoms are resolved are not recommended.
BACTERIAL VAGINOSIS IN PREGNANCY
Bacterial vaginosis is present in up to 20 percent of women during pregnancy. The effect of treating bacterial vaginosis in symptomatic or asymptomatic pregnant women on subsequent preterm delivery has produced conflicting results in clinical trials 29. The U.S. Preventive Services Task Force recommends against routine bacterial vaginosis screening of asymptomatic pregnant women at low risk of preterm delivery 30.
RECURRENT BACTERIAL VAGINOSIS
Most relapses of bacterial vaginosis occur within the first year and strongly correlate with new sex partners. Reported recurrence rates are 15 to 30 percent within three months 31. One randomized controlled trial on persistent bacterial vaginosis indicated that metronidazole gel 0.75% (Metrogel), used twice weekly for six months after initial treatment, effectively maintained a clinical cure for six months 32.
What is Trichomoniasis
Trichomoniasis increases a woman’s risk of getting or spreading other sexually transmitted diseases such as HIV 33. Trichomoniasis also may cause preterm labor or preterm birth 34.
Symptoms and signs of trichomoniasis are not specific, and diagnosis by microscopy is more reliable. Features suggestive of trichomoniasis are trichomonads seen with saline, leukocytes more numerous than epithelial cells, positive whiff test, and vaginal pH greater than 5.4. The wet-mount preparation is an inexpensive and quick test with variable sensitivity of 58 to 82 percent,40 and is influenced by the experience of the examiner and the number of parasites in the vaginal fluid sample. Adding examination of the spun urine specimen can increase the detection rate of Trichomonas vaginalis from 73 to 85 percent 35.
Treatment should not be based on a Papanicolaou (Pap) smear finding of trichomonads. Newer point-of-care tests (see Table 4) are more accurate but costly. In one study, the sensitivities of wet-mount preparation, microbiologic culture, rapid antigen testing, and nucleic acid amplification testing were 51, 75, 82, and 98 percent, respectively. Specificity was close to 100 percent for each method 36. Polymerase chain reaction analysis of samples from tampons and introital specimens is more accurate than vaginal or cervical swabs and Pap smears, and may be preferable for patient comfort 37.
Treatment for trichomoniasis
Almost any nitroimidazole drug given orally in a single dose or over a longer period results in parasitologic cure in 90 percent of cases 38. A single 2-g dose of metronidazole is adequate but can cause dyspepsia and metallic taste; compliant patients may prefer a longer regimen at a lower daily dosage with fewer adverse effects. Metronidazole in a dosage of 500 mg twice daily for seven days will treat bacterial vaginosis and trichomoniasis. Metronidazole in a dosage of 2 to 4 g daily for seven to 14 days is recommended for metronidazole-resistant strains.
The parasitologic cure rate of intravaginal nitroimidazole creams is an unacceptably low 50 percent. In RCTs, combined oral and intravaginal treatments have been more effective than oral treatment alone. Sex partners should be treated simultaneously 38. To reduce recurrence, partners should avoid resuming sexual intercourse until both have completed treatment and are asymptomatic. Test of cure is not required 26.
TRICHOMONIASIS IN PREGNANCY
A Cochrane review found that metronidazole is effective against trichomoniasis when taken by women and their partners during pregnancy. A trial of women treated before 23 weeks of gestation was stopped early because women taking metronidazole were more likely to give birth preterm and have low-birth-weight infants 39. The CDC recommends giving 2 g of metronidazole as a single dose, preferably after 37 weeks of gestation, and counseling patients about the potential risks and benefits of treatment.
What is Vulvovaginal Candidiasis
An estimated 75 percent of women will have at least one episode of vulvovaginal candidiasis, and 40 to 45 percent will have two or more.46 Changes in the host vaginal environment precipitate and induce pathologic effects of the organism.14 Several risk factors for vulvovaginal candidiasis are listed in Table 2.3–11
Diagnosis of vulvovaginal candidiasis
Although symptoms of vulvovaginal candidiasis such as pruritus, vaginal soreness, dyspareunia, and vaginal discharge are common, none of them are specific. Most patients can be diagnosed by microscopic examination of vaginal secretions with a 10% potassium hydroxide solution (sensitivity, 65 to 85 percent). Vaginal pH is usually normal (4.0 to 4.5). Vaginal culture should be considered in recurrently symptomatic women with negative microscopy and a normal pH. The Pap smear, although specific, is insensitive, with positive results in only about 25 percent of patients with culture-positive symptomatic vulvovaginal candidiasis. A rapid yeast detection test (Savyon Diagnostics) can be performed by the patient and costs less than $10, compared with a mean of $65 for the yeast culture 40. Polymerase chain reaction testing is considered the most sensitive method, but is very expensive.
Treatment of vulvovaginal candidiasis
On the basis of clinical presentation, microbiology, host factors, and response to therapy, vulvovaginal candidiasis can be classified as uncomplicated or complicated. Patients with uncomplicated vulvovaginal candidiasis are not pregnant, are otherwise healthy, and have all of the following:
- Mild to moderate disease
- Fewer than four episodes of candidiasis per year
- Pseudohyphae or hyphae visible on microscopy.
Treatment of uncomplicated vulvovaginal candidiasis involves a short course of antifungals 41; oral and topical preparations are similarly effective 42.
Patients with complicated vulvovaginal candidiasis have one or more of the following:
- Moderate to severe disease
- Four or more episodes of candidiasis per year
- Only budding yeast visible on microscopy
- Adverse host factors (e.g., pregnancy, diabetes mellitus, immunocompromise).
Treatment of complicated vulvovaginal candidiasis involves an intensive, longer course of antifungals (see Table 4).
Noninfectious Causes of Vaginitis
Irritant contact dermatitis and allergic contact dermatitis are two noninfectious causes of vaginitis. They may be associated with use of feminine hygiene products or contraceptive materials, among many other causes. Atrophic vaginitis can manifest clinically with symptoms of vaginal dryness, itching, discharge, irritation, and dyspareunia. It affects 10 to 40 percent of women who have conditions associated with estrogen deficiency 43. Diagnosis is based on history and physical findings, supplemented by vaginal pH levels, vaginal wet-mount preparation (to exclude superimposed infection), and, rarely, culture or cytology. Both systemic and topical estrogen treatments are effective in relieving symptoms. Topical vaginal estrogen is preferred because of the low systemic absorption and reduced risk of adverse effects compared with oral therapy. Estrogen-containing creams, pessaries, intravaginal tablets, and the estradiol vaginal ring appear equally effective for the symptoms of atrophic vaginitis 44.
In the meantime, to minimize vaginal odor:
- Wash your external genital area. During regular baths or showers, use a very small amount of mild, unscented soap and lots of water.
- Avoid douching. All healthy vaginas contain bacteria and yeast. The normal acidity of your vagina keeps bacteria and yeast in check. But douching can actually upset this delicate balance.
Does vaginitis affect a pregnant woman & her infant ?
Some types of vaginitis can cause problems during pregnancy.
Pregnant women with bacterial vaginosis are more likely to go into labor and give birth too early (preterm). Preterm infants may face a number of health challenges, including low birth weight and breathing problems. However, treating bacterial vaginosis in women who are pregnant has not been consistently found to reduce rates of preterm birth. For this reason, most pregnant women without symptoms are not screened for bacterial vaginosis. Some experts recommend screening pregnant women who have had a preterm infant before, whether or not they have symptoms 45.
Sexually transmitted types of vaginitis can be very harmful to a pregnant woman and her unborn child. Trichomoniasis can cause preterm labor and preterm birth. Some sexually transmitted infections can be passed from a mother to her infant before, during, or after birth. A pregnant woman should tell her doctor about symptoms of vaginitis. She also should get routine prenatal care, including screening tests for sexually transmitted infections 46.
Can vaginitis be prevented ?
These steps can help prevent vaginitis:
- Women who often get yeast infections may want to avoid clothes that hold in heat and moisture, such as pantyhose without a cotton lining, nylon panties, or tight jeans.
- Do not douche or use vaginal sprays because they can kill “good” bacteria or cause irritation.
- Practicing safe sex can help protect against sexually transmitted forms of vaginitis. Limiting the number of sex partners and using condoms are examples of safe sex.
- Vaginitis: Overview. Child Health and Human Development. https://www.nichd.nih.gov/health/topics/vaginitis/Pages/default.aspx[↩]
- Vaginitis. American Congress of Obstetricians and Gynecologists. https://www.acog.org/Patients/FAQs/Vaginitis[↩]
- Centers for Disease Control and Prevention. (2010). Self-study STD module—vaginitis. Retrieved March 23, 2012, from http://www2a.cdc.gov/stdtraining/self-study/vaginitis/default.htm[↩]
- Sobel, J. D. (1999). Vulvovaginitis in healthy women. Comprehensive Therapy, 25,335–346.[↩]
- Centers for Disease Control and Prevention. (2010). Bacterial vaginosis—CDC fact sheet. http://www.cdc.gov/std/bv/stdfact-bacterial-vaginosis.htm[↩][↩]
- National Institute of Allergy and Infectious Diseases. (2008). Vaginal yeast infection. http://www.niaid.nih.gov/topics/vaginalyeast/pages/default.aspx[↩]
- Koumans, E. H., Sternberg, M., Bruce, C., McQuillan, G., Kendrick, J., Sutton, M., et al. (2007). The prevalence of bacterial vaginosis in the United States, 2001–2004: Associations with symptoms, sexual behaviors, and reproductive health. Sexually Transmitted Diseases, 34, 864–869. http://journals.lww.com/stdjournal/Fulltext/2007/11000/The_Prevalence_of_Bacterial_Vaginosis_in_the.6.aspx[↩]
- Centers for Disease Control and Prevention. (2012). Genital/vulvovaginal candidiasis statistics. https://www.cdc.gov/fungal/diseases/candidiasis/genital/index.html[↩]
- Sutton, M., Sternberg, M., Koumans, E. H., McQuillan, G., Berman, S., & Markowitz, L. (2007). The prevalence of Trichomonas vaginalis infection among reproductive-age women in the United States, 2001–2004. Clinical Infectious Diseases, 45, 1319–1326. https://academic.oup.com/cid/article/45/10/1319/277782/The-Prevalence-of-Trichomonas-vaginalis-Infection[↩]
- Centers for Disease Control and Prevention. (2010). Self-study STD module—vaginitis. https://www2a.cdc.gov/STDTraining/Self-Study/vaginitis/[↩][↩]
- Centers for Disease Control and Prevention. (2010). Bacterial vaginosis—CDC fact sheet. https://www.cdc.gov/std/bv/stdfact-bacterial-vaginosis.htm[↩][↩]
- National Institute of Allergy and Infectious Diseases. (2008). Vaginal yeast infection. https://www.niaid.nih.gov/diseases-conditions/std-research[↩]
- Centers for Disease Control and Prevention. (2010). Sexually transmitted diseases treatment guidelines, 2010. https://www.cdc.gov/std/treatment/2010/default.htm[↩]
- Lowe NK, Neal JL, Ryan-Wenger NA. Accuracy of the clinical diagnosis of vaginitis compared with a DNA probe laboratory standard. Obstet Gynecol. 2009;113(1):89–95.[↩]
- Vaginitis: Diagnosis and Treatment. Am Fam Physician. 2011 Apr 1;83(7):807-815. http://www.aafp.org/afp/2011/0401/p807.html[↩][↩][↩][↩]
- Anderson MR, Klink K, Cohrssen A. Evaluation of vaginal complaints. JAMA. 2004;291(11):1368–1379.[↩][↩][↩][↩][↩]
- Carr PL, Rothberg MB, Friedman RH, Felsenstein D, Pliskin JS. “Shotgun” versus sequential testing. Cost-effectiveness of diagnostic strategies for vaginitis. J Gen Intern Med. 2005;20(9):793–799.[↩]
- Allsworth JE, Peipert JF. Prevalance of bacterial vagniosis: 2001–2004 National Health and Nutrition Examination Survey data. Obstet Gynecol. 2007;109(1):114–120.[↩]
- Livengood CH III, Thomason JL, Hill GB. Bacterial vaginosis: diagnostic and pathogenetic findings during topical clindamycin therapy. Am J Obstet Gynecol. 1990;163(2):515–520.[↩][↩]
- National Institute of Allergy and Infectious Diseases. (2008). Bacterial vaginosis. https://www.niaid.nih.gov/research/womens-health-research-advances[↩]
- Ness RB, Hillier SL, Kip KE, et al. Bacterial vaginosis and risk of pelvic inflammatory disease. Obstet Gynecol. 2004;104(4):761–769.[↩]
- Leitich H, Bodner-Adler B, Brunbauer M, Kaider A, Egarter C, Husslein P. Bacterial vaginosis as a risk factor for preterm delivery: a meta-analysis. Am J Obstet Gynecol. 2003;189(1):139–147.[↩]
- Martin HL, Richardson BA, Nyange PM, et al. Vaginal lactobacilli, microbial flora, and risk of human immunodeficiency virus type 1 and sexually transmitted disease acquisition. J Infect Dis. 1999;180(6):1863–1868.[↩]
- Amsel R, Totten PA, Spiegel CA, Chen KC, Eschenbach D, Holmes KK. Nonspecific vaginitis. Diagnostic criteria and microbial and epidemiologic associations. Am J Med. 1983;74(1):14–22.[↩]
- Gutman RE, Peipert JF, Weitzen S, Blume J. Evaluation of clinical methods for diagnosing bacterial vaginosis. Obstet Gynecol. 2005;105(3):551–556.[↩][↩]
- Centers for Disease Control and Prevention. Sexually transmitted diseases treatment guidelines 2010. Diseases characterized by vaginal discharge. http://www.cdc.gov/std/treatment/2010/toc.htm[↩][↩][↩][↩]
- Oduyebo OO, Anorlu RI, Ogunsola FT. The effects of antimicrobial therapy on bacterial vaginosis in non-pregnant women. Cochrane Database Syst Rev. 2009;(3):CD006055[↩][↩]
- Senok AC, Verstraelen H, Temmerman M, Botta GA. Probiotics for the treatment of bacterial vaginosis. Cochrane Database Syst Rev. 2009; (4):CD006289.[↩]
- McDonald HM, Brocklehurst P, Gordon A. Antibiotics for treating bacterial vaginosis in pregnancy. Cochrane Database Syst Rev. 2007;(1):CD000262.[↩]
- U.S. Preventive Services Task Force. Screening for bacterial vaginosis in pregnancy to prevent preterm delivery: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med. 2008;148(3):214–219.[↩]
- Ralph SG, Rutherford AJ, Wilson JD. Influence of bacterial vaginosis on conception and miscarriage in the first trimester: cohort study. BMJ. 1999;319(7204):220–223.[↩]
- Sobel JD, Ferris D, Schwebke J, et al. Suppressive antibacterial therapy with 0.75% metronidazole vaginal gel to prevent recurrent bacterial vaginosis. Am J Obstet Gynecol. 2006;194(5):1283–1289.[↩]
- Centers for Disease Control and Prevention. (2011). Trichomoniasis—CDC fact sheet. https://www.cdc.gov/std/trichomonas/STDFact-Trichomoniasis.htm[↩]
- National Institute of Allergy and Infectious Diseases. (2009). Trichomoniasis. https://www.niaid.nih.gov/diseases-conditions/sexually-transmitted-diseases[↩]
- Blake DR, Duggan A, Joffe A. Use of spun urine to enhance detection of Trichomonas vaginalis in adolescent women. Arch Pediatr Adolesc Med. 1999;153(12):1222–1225.[↩]
- Huppert JS, Mortensen JE, Reed JL, et al. Rapid antigen testing compares favorably with transcription-mediated amplification assay for the detection of Trichomonas vaginalis in young women. Clin Infect Dis. 2007;45(2):194–198.[↩]
- Witkin SS, Inglis SR, Polaneczky M. Detection of Chlamydia trachomatis and Trichomonas vaginalis by polymerase chain reaction in introital specimens from pregnant women. Am J Obstet Gynecol. 1996;175(1):165–167.[↩]
- Forna F, Gülmezoglu AM. Interventions for treating trichomoniasis in women. Cochrane Database Syst Rev. 2003;(2):CD000218.[↩][↩]
- Gülmezoglu AM. Interventions for trichomoniasis in pregnancy. Cochrane Database Syst Rev. 2002;(3):CD000220.[↩]
- Chatwani AJ, Mehta R, Hassan S, Rahimi S, Jeronis S, Dandolu V. Rapid testing for vaginal yeast detection: a prospective study. Am J Obstet Gynecol. 2007;196(4):309.e1–4.[↩]
- Nurbhai M, Grimshaw J, Watson M, Bond C, Mollison J, Ludbrook A. Oral versus intra-vaginal imidazole and triazole anti-fungal treatment of uncomplicated vulvovaginal candidiasis (thrush). Cochrane Database Syst Rev. 2007;(4):CD002845.[↩]
- Pappas PG, Kauffman CA, Andes D, et al.; Infectious Diseases Society of America. Clinical practice guidelines for the management of candidiasis: 2009 update by the Infectious Diseases Society of America. Clin Infect Dis. 2009;48(5):503–535.[↩]
- Greendale GA, Judd HL. The menopause: health implications and clinical management. J Am Geriatr Soc. 1993;41(4):426–436.[↩]
- Suckling JA, Lethaby A, Kennedy R. Local oestrogen for vaginal atrophy in postmenopausal women. Cochrane Database Syst Rev. 2006; (4):CD001500.[↩]
- Centers for Disease Control and Prevention. (2010). Sexually transmitted diseases treatment guidelines, 2010. https://www.cdc.gov/std/treatment/2010/[↩]
- Centers for Disease Control and Prevention. (2011). STDs & pregnancy—CDC fact sheet. https://www.cdc.gov/std/pregnancy/STDFact-Pregnancy.htm[↩]





{kind=link}