Contents
What is hydronephrosis
Hydronephrosis is the swelling of one or both kidneys due to a build-up of urine. Hydronephrosis refers to dilation of the pelvis and calyceals of the kidney where urine is collected. Hydronephrosis happens when urine can’t drain from a kidney and builds up in the kidney as a result. Hydronephrosis can occur from a blockage or obstruction in the tubes that drain urine from the kidneys (ureters) or from an anatomical defect that doesn’t allow urine to drain properly. Hydronephrosis can occur in one (unilateral hydronephrosis) or both kidneys (bilateral hydronephrosis).
The increased pressure of extra urine within the kidney decreases the blood filtration rate and may cause structural damage to kidney cells. This decrease in function is often reversible if the underlying condition is corrected but if the duration is prolonged, the damage is often permanent.
Hydronephrosis is often referred to as being ‘prenatal’ or ‘antenatal.’ The term prenatal means the hydronephrosis was noticed in the child before birth. Antenatal means the hydronephrosis was noted after birth.
Hydronephrosis can happen at any age. Hydronephrosis is a common congenital condition that is found in about one out of every 500 babies. In very rare cases, hydronephrosis can be developed later in life as well. Hydronephrosis in children may be diagnosed during infancy or sometimes during a prenatal ultrasound before the baby is born.
Today, hydronephrosis is usually first diagnosed on prenatal ultrasounds. Finding hydronephrosis while the baby is the womb has become more common because of advances in prenatal ultrasounds. Before the advancement in this technology, children born with hydronephrosis may not have been diagnosed until they began to show symptoms, or were not identified at all. Many children who are diagnosed with hydronephrosis before they are born will have the condition resolve on its own while the child is young, without medical intervention.
Hydronephrosis may or may not cause symptoms. When they occur, signs and symptoms of hydronephrosis might include:
- Pain in the side and back (flank pain) that may travel to the lower abdomen or groin
- Urinary problems, such as pain with urination or feeling an urgent or frequent need to urinate
- Nausea and vomiting
- Fever
- Failure to thrive, in infants
Hydronephrosis is found on an imaging test such as:
- MRI of the abdomen
- CT scan of the kidneys or abdomen
- Intravenous pyelogram (IVP)
- Kidney scan
- Ultrasound of the kidneys or abdomen
Hydronephrosis treatment depends on the cause of the kidney swelling. Treatment may include:
- Placing a stent (tube) through the bladder and ureter to allow urine to flow from the kidney into the bladder
- Placing a tube into the kidney through the skin, to allow the blocked urine to drain out of the body into a drainage bag
- Antibiotics for infections
- Surgery to correct the blockage or reflux
- Removal of any stone that is causing blockage
People who have only one kidney, who have immune system disorders such as diabetes or HIV, or who have had a transplant will need treatment right away.
People who have long-term hydronephrosis may need antibiotics to reduce the risk of UTI.
Urinary tract system
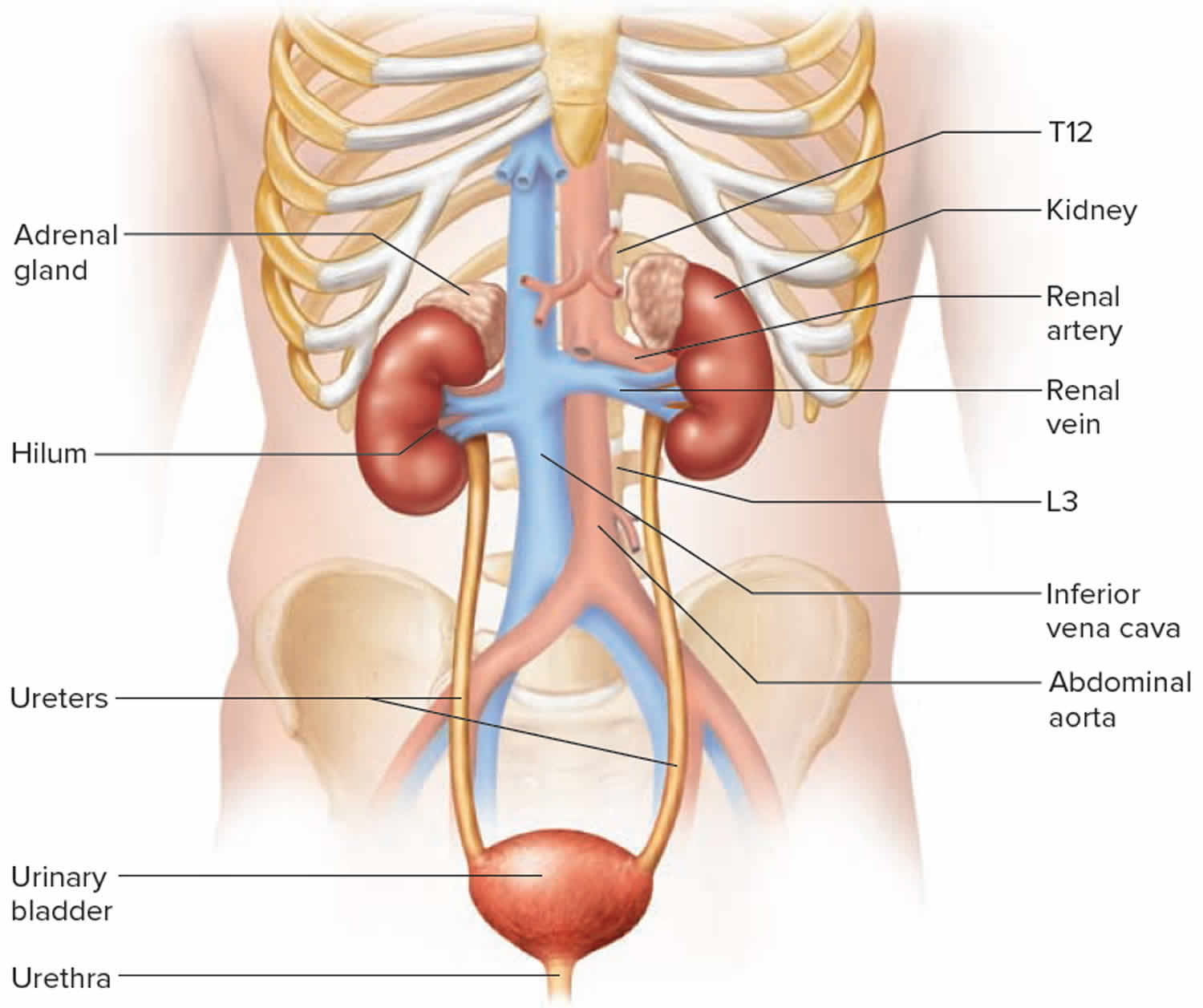
The main function of the urinary tract is to remove wastes and fluid from the body. The urinary tract has four parts: the kidneys, the ureters, the bladder and urethra. The urine is formed when the kidneys filter blood and remove excess waste materials and fluid. Urine collects into a part of the kidney called the renal pelvis. From the renal pelvis, the urine travels down a narrow tube called the ureter into the bladder. The bladder slowly fills up with urine, which empties from the body through another small tube called the urethra. Hydronephrosis occurs when there is either a blockage of the outflow of urine, or reverse flow of urine already in the bladder (called reflux) that can cause the renal pelvis to become enlarged.
Figure 1. Kidney anatomy
Fetal hydronephrosis
Fetal hydronephrosis represents the abnormal dilatation of the fetal renal collecting system, with pelviureteric junction obstruction the most commonly encountered cause. Antenatal (before birth) hydronephrosis has emerged as one of the most common fetal abnormalities. Due to the increased use of prenatal ultrasound, it is now seen in 1-3 out of 100 pregnancies. Fetal hydronephrosis can be detected as early as the first trimester of pregnancy and, in most cases, is followed throughout the remainder of the pregnancy with repeated ultrasounds.
Fetal hydronephrosis causes
Marked hydronephrosis (particularly in the 3rd trimester) can result from a number of pathologies, which include:
- posterior urethral valves: in males
- congenital pelviureteric junction obstruction: the commonest cause of fetal hydronephrosis 1)
- congenital vesicoureteric junction obstruction
- ureterocoele(s)
- urethral agenesis
- congenital megaloureter
- megacystis microcolon syndrome
- megacystis megaureter syndrome 2)
- fetal vesicoureteric reflux
- prune-belly syndrome (rare)
Associations
- Down syndrome: more so with mild renal pelvic dilatation (low association)
Fetal hydronephrosis diagnosis
Antenatal ultrasound
In the second trimester, the severity of fetal hydronephrosis may be graded as 3):
- mild hydronephrosis: anteroposterior renal pelvic diameter measures ≥5 mm (≥4 mm at 16-20 weeks)
- moderate/severe hydronephrosis: anteroposterior renal pelvic diameter measures ≥7 mm or if there is associated calyceal dilatation
- persistent hydronephrosis: ≥10 mm in the 3rd trimester
Ancillary sonographic features:
- dilatation of the renal calyces
- dilated ureter if the obstruction is distal
- concurrent oligohydramnios if there is a bilateral obstruction (or unilateral obstruction with significantly impaired renal function in the other kidney)
Fetal hydronephrosis treatment and prognosis
Management will depend on the underlying pathology. The degree of renal pelvic dilatation correlates with the outcome. A renal pelvic anteroposterior diameter of 9 mm or more, and a pelvic-to-renal anteroposterior diameter ratio of 0.45 before 32 weeks of gestation and 0.52 thereafter are considered to be useful for the detection of a severe outcome postnatally 4).
Hydronephrosis in babies
Hydronephrosis in babies also called neonatal hydronephrosis, is most commonly diagnosed antenatally as fetal pylectasis, and in the majority of cases is due to pelvi-ureteric junction obstruction.
Kidney ultrasound
- renal pelvis anterior-posterior diameter of >7-10 mm is considered significant 5); this is not absolute and varies by institution
- calyceal dilatation is present in more severe hydronephrosis
Hydronephrosis in babies causes
- pelvi-ureteric junction (PUJ) obstruction (50% of cases) 6)
- vesicoureteric reflux (~20% of cases) 7)
- posterior urethral valves (~10% of cases) 8)
- vesico-ureteric junction (VUJ) obstruction
- megacystis megaureter
- multicystic dysplastic kidneys
Hydronephrosis in babies treatment and prognosis
The estimated incidence of neonatal hydronephrosis that has clinical significance is 1 in 600 and most cases will resolve without intervention 9).
Hydronephrosis in children
Many children with mild hydronephrosis may not have any symptoms and the condition may never be detected. In severe cases of hydronephrosis, those associated with the blockage of urine, children may experience acute kidney pain, bleeding or urinary tract infections.
Hydronephrosis in pregnancy
Maternal hydronephrosis in pregnancy often results as a physiological phenomenon due to the presence of the fetus. It is estimated that up to 90% of women have some degree of asymptomatic dilatation of the renal calyces, the renal pelves and the upper two-thirds of the ureters during pregnancy 10). It is thought to be most pronounced in primigravid females and the hydronephrosis is often more prominent on the right side 11).
As the fetus grows, hydronephrosis usually develops during the second trimester. A mechanical compression of the ureter between the gravid uterus and iliopsoas muscle is generally thought to be the mechanism 12).
Very rarely other entities such as urinary tract calculi can complicate the picture. The prevalence of ureteric calculi in pregnancy is low and is estimated around 0.03-0.4% depending on the population.
There may be an association between gestational hydronephrosis and increased frequency of ascending urinary tract infection.
Kidney ultrasound will show renal pelvic and proximal dilatation. In order to differentiate pure physiological hydronephrosis from a worsening of an existing hydronephrosis due to an underlying pathology (e.g. urinary tract calculus), some authorities have devised charts showing the upper limit of normals allowable for gestation.
Hydronephrosis in pregnancy treatment and prognosis
In most cases, hydronephrosis in pregnancy disappears within a few weeks after birth. The vast majority of asymptomatic cases are treated conservatively 13) especially since most cases of physiological calyectasis do not impair renal function. Ureteral catheters may be introduced in selected symptomatic cases. If however the kidney is obstructed with superimposed infection, prompt surgical decompression is warranted in addition to antibiotic therapy 14).
Bilateral hydronephrosis
Bilateral hydronephrosis is the enlargement of the parts of the kidney that collect urine. Bilateral means both sides.
Bilateral hydronephrosis causes
Bilateral hydronephrosis occurs when urine is unable to drain from the kidney into the bladder. Hydronephrosis is not itself a disease. It occurs as a result of a problem that prevents urine from draining out of the kidneys, ureters, and bladder.
Disorders linked with bilateral hydronephrosis include:
- Acute bilateral obstructive uropathy – sudden blockage of the kidneys
- Bladder outlet obstruction – blockage of the bladder, which does not allow drainage
- Chronic bilateral obstructive uropathy – a gradual blockage of both kidneys is most often from a common singular obstruction
- Neurogenic bladder – poorly functional bladder
- Posterior urethral valves – flaps on the urethra that causes poor emptying of the bladder (in boys)
- Prune belly syndrome – poorly emptying bladder that causes distention of the belly
- Retroperitoneal fibrosis – increased scar tissue that blocks the ureters
- Ureteropelvic junction obstruction – blockage of the kidney at the point where the ureter enters the kidney
- Vesicoureteric reflux – backup of the urine from the bladder up to the kidney
- Uterine prolapse – when the womb (uterus) drops down and presses into the vaginal area
Bilateral hydronephrosis symptoms
In a baby, signs of a problem are often found before birth during a pregnancy ultrasound.
A urinary tract infection in a newborn baby can signal a blockage in the kidney. An older child who gets repeat urinary tract infections should also be checked for blockage.
A higher than normal number of urinary tract infections is often the only symptom of the problem.
Common symptoms in adults may include:
- Back pain
- Nausea, vomiting
- Fever
- Need to urinate often
- Decreased urine output
- Blood in the urine
Bilateral hydronephrosis possible complications
- Irreversible kidney damage may result from conditions that cause hydronephrosis.
Bilateral hydronephrosis diagnosis
The following tests can show bilateral hydronephrosis:
- CT scan of the abdomen or kidneys
- Intravenous pyelogram (IVP) (used less often)
- Pregnancy (fetal) ultrasound
- Renal scan
- Ultrasound of the abdomen or kidneys
Bilateral hydronephrosis treatment
Placing a tube into the bladder (Foley catheter) may open the blockage. Other treatments include:
- Draining the bladder
- Relieving pressure by placing tubes in the kidney through the skin
- Placing a tube (stent) through the ureter to allow urine to flow from the kidney to bladder
The underlying cause of the blockage needs to be found and treated once the buildup of urine is relieved.
Bilateral hydronephrosis prognosis
Surgery performed while the baby is in the womb or shortly after birth can have good results in improving kidney function.
Return of renal function can vary, depending on the length of obstruction.
Hydronephrosis grading
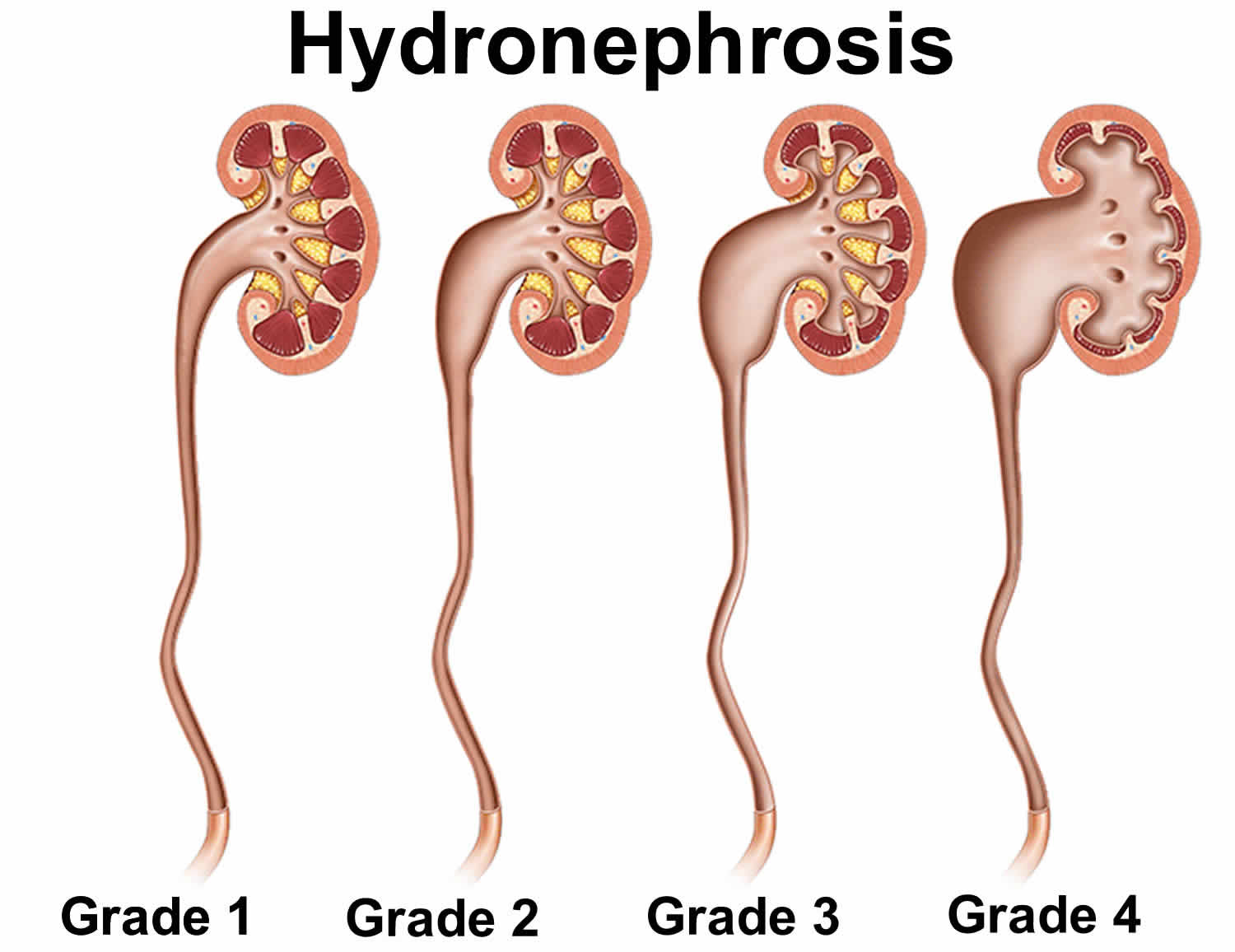
Grading systems of hydronephrosis have been devised to communicate the degree of upper collecting system dilatation. The most common hydronephrosis grading system used is the Society of Fetal Urology grading of neonatal and infant hydronephrosis. The Society of Fetal Urology has created a universal grading system of hydronephrosis that ranges from grade 1 (most mild) to grade 5 (most severe). The grading system is based on how dilated the kidney and the amount of renal paranchemya present.
Hydronephrosis grading systems (including the Society of Fetal Urology) are controversial in terms of their intra-rater and inter-rater reliability 15), 16), 17).
Hydronephrosis is also categorized as:
- mild,
- moderate, or
- severe
depending on the extent of the dilation in the area of the kidney where urine is collected is enlarged or dilate.
Often children who have hydronephrosis are born with this condition.
The Society for Fetal Urology hydronephrosis grading system:
Grade 0
- no dilatation, calyceal walls are apposed to each other
Grade 1 (mild)
- dilatation of the renal pelvis without dilatation of the calyces (can also occur in the extrarenal pelvis)
- no parenchymal atrophy
Grade 2 (mild)
- dilatation of the renal pelvis (mild) and calyces (pelvicalyceal pattern is retained)
- no parenchymal atrophy
Grade 3 (moderate)
- moderate dilatation of the renal pelvis and calyces
- blunting of fornices and flattening of papillae
- mild cortical thinning may be seen
Grade 4 (severe)
- gross dilatation of the renal pelvis and calyces, which appear ballooned
- loss of borders between the renal pelvis and calyces
- renal atrophy seen as cortical thinning
Figure 2. Hydronephrosis grading
Mild hydronephrosis
In mild hydronephrosis, the renal papillae – the point of transition between pyramids and minor calyces – are preserved while the major calyces are enlarged due to increased urinary volume and pressure. Sonographically, this appears as an anechoic triangle at the renal pelvis, tapering to the proximal junction with the ureter.
Moderate hydronephrosis
Moderate hydronephrosis is characterized by further dilation of the calyces, obliteration of the renal papillae, and blunting and rounding of the pyramids. The sonographic appearance of moderate hydronephrosis takes the form of an anechoic “bear paw,” with the dilated calyces representing finger-like projections. Cortical involvement distinguishes moderate from severe hydronephrosis.
Severe hydronephrosis
In severe hydronephrosis, the calyces coalesce into a single, large, anechoic space. The renal cortex is the only remaining recognizable structure, and this too is compressed (its normal thickness is about 1 cm) due to increased pressure within the renal sinus. Without a known etiology, severe hydronephrosis should prompt further diagnostic testing.
Hydronephrosis causes
Normally, urine goes from the kidney to the tube that drains the kidney (ureter), to the bladder and then out of the body. But, sometimes urine backs up or remains inside the kidney or in the ureter. That’s when hydronephrosis can develop.
Some common causes of hydronephrosis include:
- Partial obstruction or blockage in the urinary tract.
- Urinary tract blockages often form where the kidney meets the ureter, at a point called the ureteropelvic junction (UPJ obstruction).
- Less commonly, blockages may occur where the ureter meets the bladder at what’s called the ureterovesical junction (UVJ obstruction).
- In the urethra in boys (posterior urethral valve). Posterior urethral valves (PUV) are an obstruction that occurs prior to birth in males that is caused by pieces of tissue in the area of the prostatic urethra.
- A ureter may be associated with a ureterocele. Ureterocele occurs when the ureter does not develop properly and causes a balloon-like obstruction at the end of the ureter and a small pouch into the bladder.
- Vesicoureteral reflux. Vesicoureteral reflux happens when urine flows backward through the ureter from the bladder up into the kidney and may affect one or both ureters (the tubes that carry urine from the kidney to the bladder). Normally, urine flows only one way in the ureter. Urine flowing the wrong way makes it difficult for the kidney to empty properly and causes the kidney to swell.
- Ectopic ureter: An ectopic ureter drains urine somewhere outside the bladder.
- Neurogenic bladder: Neurogenic bladder is a condition in which the nerves that carry messages from the bladder to the brain and from the brain to the muscles of the bladder do not work properly.
- No significant abnormality. The dilation in many of these kidneys eventually resolves over time.
Less-common causes of hydronephrosis include kidney stones, a tumor in the abdomen or pelvis, and problems with nerves that lead to the bladder.
Hydronephrosis is usually caused by another underlying illness or risk factor. Causes of hydronephrosis include, but are not limited to, the following illnesses or risk factors:
- Kidney stone
- Congenital blockage (a defect that is present at birth)
- Blood clot
- Scarring of tissue (from injury or previous surgery)
- Tumor or cancer (examples include bladder, cervical, pelvis, colon, abdomen or prostate)
- Enlarged prostate (noncancerous)
- Blockage from an enlarged uterus during pregnancy
- Urinary tract infection (or other diseases that cause inflammation of the urinary tract)
- Blockage of a ureter due to scarring caused by prior infections, surgeries, or radiation treatments
- Problems with the nerves that supply the bladder
Hydronephrosis symptoms
Hydronephrosis may or may not cause symptoms.
Common symptoms include:
- Flank pain
- Abdominal mass, especially in children
- Nausea and vomiting
- Urinary tract infection (UTI)
- Fever
- Painful urination (dysuria)
- Increased urinary frequency
- Increased urinary urgency
The main symptom is pain, either in the side and back (known as flank pain), abdomen or groin. Other symptoms can include pain during urination, other problems with urination (increased urge or frequency, incomplete urination, incontinence), nausea and fever. These symptoms depend on the cause and severity of urinary blockage.
Hydronephrosis diagnosis
Hydronephrosis is most commonly diagnosed on routine prenatal ultrasounds completed after 10 weeks of gestation. Children diagnosed with hydronephrosis while in the womb or later in life often receive renal ultrasounds, Lasix renal scans and/or voiding cystourethrograms so that the urology team may gain a more complete understanding of the hydronephrosis and monitor the child’s condition.
Tests for diagnosing hydronephrosis may include:
- Blood test to evaluate kidney function
- Urine test to check for signs of infection or urinary stones that could cause a blockage
- Renal bladder ultrasound imaging exam, during which your doctor can view the kidneys, bladder and other urinary structures to identify potential problems
- Voiding cystourethrogram: An X-ray exam that uses a special dye and a catheter (tube) is placed through your child’s urethra into the bladder. The tube will be used to slowly fill the bladder with a solution. While the bladder is being filled, a special machine (fluoroscopy) is used to take pictures. The radiologist looks to see if any of the solution is going back up into the kidneys. This study confirms the diagnosis of vesicoureteral reflux. Additional pictures are taken while your child is urinating. The radiologist will look at the urethra while urine is passing to be sure there is no blockage noted (posterior urethral valve).
- MAG III renal scan: This study will be performed to determine how each kidney is functioning and the degree of blockage, if noted. An intravenous line (IV) is used to inject a special solution called an isotope into the veins. The isotope makes it possible to see the kidneys clearly. Pictures of the kidneys will be taken with a large X-ray machine that rotates around your child.
- MRI/MRU: MRI is a radiation-free diagnostic procedure that uses a combination of a large magnet, radiofrequencies and a computer to produce detailed images of the body. Magnetic resonance urography (MRU) creates detailed pictures of the kidneys, ureters and bladder.
An ultrasound is typically used to confirm a diagnosis. This procedure uses sound waves to create an image of your kidneys. A doctor can also confirm a diagnosis with x-rays, computerized tomography (CT) and magnetic resonance imaging (MRI). Diagnosis could also involve a cystoscopy, which uses a long tube with a light and camera at the end (cytoscope) that allows the doctor to look inside the bladder and urethra.
Blood and urine tests can also check kidney function. The doctor can also check for blood in the urine, which can be caused by a kidney stone, infection or other factor.
Hydronephrosis treatment
Hydronephrosis is usually treated by addressing the underlying disease or cause, such as a kidney stone or infection. Some cases can be resolved without surgery. Infections can be treated with antibiotics. A kidney stone can pass through by itself or might be severe enough to require removal with surgery.
- Mild to moderate hydronephrosis. Your doctor may opt for a wait-and-see approach to treatment, as hydronephrosis could resolve on its own. Even so, your doctor may recommend preventive antibiotic therapy to lower the risk of urinary tract infections.
- Severe hydronephrosis. When hydronephrosis makes it hard for the kidney to function — as can happen in more-severe cases or in cases that involve reflux — surgery may be recommended to eliminate the blockage or correct the reflux. Left untreated, severe hydronephrosis could lead to permanent kidney damage. Rarely, it can cause kidney failure.
In cases of severe blockage and hydronephrosis, excess urine may need to be removed using either a catheter to drain urine from the bladder or a special tube called a nephrostomy that drains urine from the kidney. The key to treatment is to get it addressed as soon as possible in order to avoid any permanent damage to the kidneys.
Severe cases of urinary blockage and hydronephrosis can damage the kidneys and lead to kidney failure. If kidney failure occurs, treatment will be needed with either dialysis or a kidney transplant.
In most cases, however, hydronephrosis does resolve successfully if treated promptly. In the meantime, because hydronephrosis typically affects only one kidney, the other kidney can do the work for both.
Hydronephrosis treatment at home
There is no home treatment for hydronephrosis. In some cases, your doctor may refer you or your child to a doctor who specializes in conditions affecting the urinary system (urologist).
Hydronephrosis is monitored with ultrasounds. Most children will have an ultrasound completed about once every three months during their first year of life in order for the degree of hydronpehoris and its progression to be properly determined. Many children diagnosed prenatally with hydronpehrosis will see their condition resolve without surgical intervention. Most cases of mild and moderate hydronephrosis only need periodic monitoring.
If a child’s hydronephrosis worsens over time or is severe, medical intervention may be necessary. If this is the case, a surgery may be carried out by one of our fellowship-trained pediatric urologists. The most common procedure completed to correct hydronephrosis is a pyeloplasty. During a pyeloplasty, the narrowed or obstructed part of the ureter is removed and the ureter is reconnected to the healthy portion of the kidney’s drainage system. The success rate of a pyeloplasty is about 95 percent. There are cases where other surgeries may be needed. Learn about postoperative care after pyeloplasty.
What are the long-term consequences of hydronephrosis?
Children with hydronephrosis typically lead normal lives, as most cases of the condition resolve early in their life, often without long-term consequence. Even children with hydronephrosis that does not quickly resolve typically have no kidney damage and will lead normal lives. In some cases, hydronpehrosis that is severe or left untreated may cause some degree of renal failure that may cause long-term complications for the child.
References [ + ]





{kind=link}