
Contents
What is hyponatremia
Hyponatremia is defined as low levels of sodium in the serum, that is less than 135mmol/L or 135 mEq/L (normal range is between 135mmol/L and 145mmol/L or 135 and 145 milliequivalents per liter [mEq/L]). Sodium is the predominant positively charged ion (cation) in the body’s extracellular fluid. Sodium plays a key role in your body. It helps maintain normal blood pressure, supports the work of your nerves and muscles, and regulates your body’s fluid balance. Severe hyponatremia is when the serum sodium levels are below 125mmol/L. Hyponatremia results in primarily brain-related (neurological) symptoms. If serum sodium levels fall quickly, brain swelling (cerebral edema), fits (seizures), coma and even death may result. Fortunately, serum sodium can be easily monitored, and this complication can be prevented in many patients.
Hyponatremia occurs in approximately 1% of hospitalized patients. Incidence rates can be much higher in cancer patients, for example between 15-50% in small cell lung cancer. Decreased serum sodium levels in cancer patients usually occur due to fluid overload, which is caused by inappropriate levels of hormone that prevents excretion of free water (antidiuretic hormone – ADH or vasopressin). This is known as the syndrome of inappropriate secretion of ADH (SIADH), and is easily the most common cause of hyponatremia in cancer patients.
Malignant illness can cause hyponatremia in a variety of ways. These include:
- Decreased kidney (renal), adrenal or thyroid function (insufficiency)
- Factors relating to medical treatment (iatrogenic factors)
- Syndrome of inappropriate secretion of ADH (SIADH)
- Central nervous system (CNS) lesions, lung disease or nausea causing physiologic increases in ADH secretion.
- Adaptive circulatory mechanisms such as low blood pressure, heart failure or liver cirrhosis.
Syndrome of inappropriate secretion of ADH (SIADH) is the most common cause of hyponatremia in patients with cancer.
Other Mechanisms that can cause hyponatremia include:
- Increased thyroid hormones (hyperthyroidism) and adrenal insufficency.
- Excessive salt excretion (salt-wasting) in drug-induced kidney damage, adrenal insufficiency or use of specific medications that increase urine excretion (thiazide diuretics).
- Chemotherapy.
- Chemotherapy and associated nausea and vomiting.
- Overhydration with fluids containing less sodium than normal blood (hypotonic fluids).
Hyponatremia is usually caused by an excess of total body water relative to sodium levels. It is most often caused by water retention combined with excessive administration of fluids.
Water retention usually occurs as a result of increased ADH secretion due to a reduced volume of blood within the vessels (intravascular volume). This decreased intravascular volume may be due to excessive swelling when the body’s fluid has shifted outside of the blood vessels (edematous state) or true volume depletion (e.g. from blood loss).
The syndrome of inappropriate ADH secretion (SIADH) involves the inability of the kidney to dilute urine even though the plasma has become less concentrated. It is defined as an inappropriately high urine concentration (osmolality) at the same time as decreased serum osmolality.
As the early stages of hyponatremia may be asymptomatic, laboratory findings are useful in making the diagnosis. Diagnosis of SIADH is made by finding low serum sodium and low serum concentration (osmolality) (20 mmol/L) in a patient with normal intravascular volume.
Kidney, liver, heart, adrenal and thyroid function must all be normal for the diagnosis of SIADH to be made.
Treatment depends on patient symptoms and the underlying cause of the hyponatremia. Life-threatening situations must be treated supportively; an airway tube (intubation) may be necessary and medications to stop fits (anticonvulsant medications) should be considered in patients with seizures. Low sodium (hypotonic) IV fluids should be avoided, as these worsen the condition.
Serum sodium must be corrected at the appropriate rate; asymptomatic patients require slow (0.5mmol/L/hr) replacement, whereas patients who show symptoms require more rapid intervention (1-2mmol/L/hr). This rapid correction is only indicated for the first 1-3 hours of treatment, with the remainder of correction (aim is to increase serum sodium levels by 12-15mmol/L) occurring over 24 hours.
Most cases of hyponatremia due to SIADH develop gradually, and gradual correction is appropriate unless there are neurological symptoms. The central nervous system reacts to hyponatremia in a specific way. If levels change too quickly, nerve cell swelling and damage may occur. Slow sodium replacement is required to prevent fluid shifting rapidly from the cells, which can cause a specific type of damage to the brain (cerebral pontine myelinolysis). Treatment of the underlying cancer may or may not be successful in reducing the ectopic ADH secretion, and this is not considered treatment enough on its own.
The other important factor in the management of hyponatremia is fluid management. If the cause is decreased blood volume, this must be addressed appropriately. Administration of normal saline (salt water with the same sodium concentrations as blood) corrects both the fluid loss and the low sodium levels, whilst suppressing ADH secretion and encouraging free water excretion. Salt and water restriction are appropriate in cases of hyponatremia due to oedematous states. This must be accompanied by treatment of the underlying cause of the edema.
Because SIADH is a state of excess free water, it is treated initially by limiting the total free water intake. If limiting free water is unsuccessful, a specific type of antibiotic (demeclocycline, a tetracycline antibiotic), can be used to inhibit the activity of ADH on the kidney, but it is relatively slow to take action. Treatment with 3% saline +/- a medication to increase fluid excretion (diuretic – frusemide) is recommended if CNS symptoms are present. If the syndrome is chronic, frusemide or salt tablets may be used for long term treatment. The underlying tumor must also be treated.
Body Fluid Compartments and Fluid Homeostasis
A body fluid is usually a liquid that is produced by the body and consists of water and dissolved solutes. In lean adults, body fluids constitute between 55% and 60% of total body mass in females and males, respectively (Figure 1).
Body fluids are present in two main “compartments”—inside cells and outside cells.
Body Fluid Composition
- Intracellular fluid (ICF): About two-thirds of body fluid is intracellular fluid (intra- = within) or cytosol, the fluid within cells has high concentrations of potassium, phosphate, and magnesium ions. It includes a greater concentration of sulfate ions and lesser concentrations of sodium, chloride, calcium, and bicarbonate ions than does extracellular fluid. Intracellular fluid also has a greater concentration of protein than does plasma. Figure 3 shows these relative concentrations.
- Extracellular fluids (ECF): The other third, called extracellular fluid (ECF) (extra- = outside), is outside cells and includes all other body fluids. Extracellular fluid (ECF) generally are similar in composition, including high concentrations of sodium, chloride, calcium, and bicarbonate ions and lesser concentrations of potassium, magnesium, phosphate, and sulfate ions. The blood plasma portion of extracellular fluid has considerably more protein than does either interstitial fluid or lymph. About 80% of the ECF is interstitial fluid (inter- =between), which occupies the microscopic spaces between tissue cells, and 20% of the extracellular fluid (ECF) is blood plasma, the liquid portion of the blood. Other extracellular fluids that are grouped with interstitial fluid include lymph in lymphatic vessels; cerebrospinal fluid in the nervous system; synovial fluid in joints; aqueous humor and vitreous body in the eyes; endolymph and perilymph in the ears; and pleural, pericardial, and peritoneal fluids between serous membranes.
Figure 1. Body fluid compartments
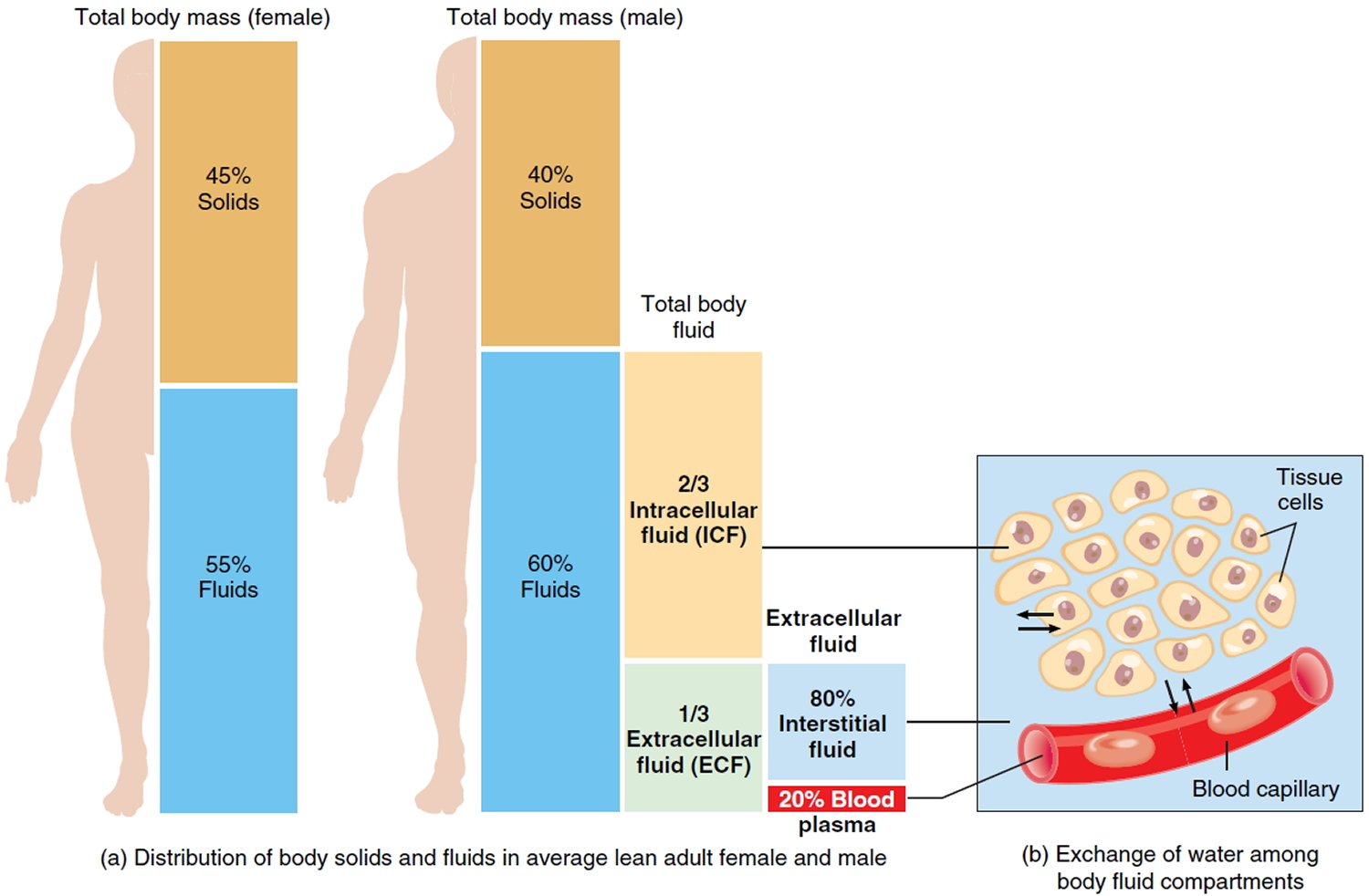
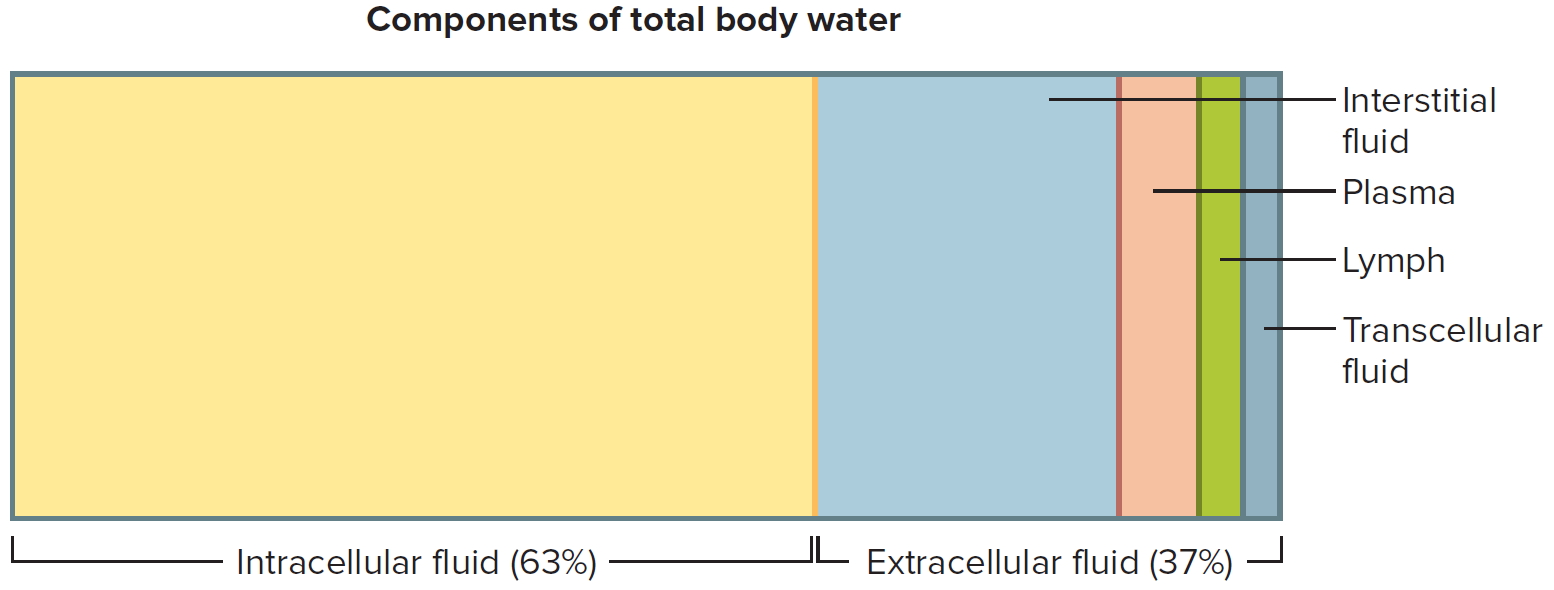
Figure 2. Components of total body water
Two general “barriers” separate intracellular fluid, interstitial fluid, and blood plasma.
- The plasma membrane of individual cells separates intracellular fluid from the surrounding interstitial fluid. The plasma membrane is a selectively permeable barrier: It allows some substances to cross but blocks the movement of other substances. In addition, active transport pumps work continuously to maintain different concentrations of certain ions in the cytosol and interstitial fluid.
- Blood vessel walls divide the interstitial fluid from blood plasma. Only in capillaries, the smallest blood vessels, are the walls thin enough and leaky enough to permit the exchange of water and solutes between blood plasma and interstitial fluid.
The body is in fluid balance when the required amounts of water and electrolytes are present and are correctly proportioned among the various compartments. Water is by far the largest single component of the body, making up 45–75% of total body mass, depending on age, gender, and the amount of adipose tissue (fat) present in the body. Obese people have proportionally less water than leaner people because water comprises less than 20% of the mass of adipose tissue. Skeletal muscle tissue, by contrast, is about 65% water. Infants have the highest percentage of water, up to 75% of body mass. The percentage of body mass that is water decreases until about 2 years of age. Until puberty, water accounts for about 60% of body mass in boys and girls. In lean adult males, water still accounts for about 60% of body mass. However, lean adult females have more subcutaneous fat than do lean adult males. Thus, their percentage of total body water is lower, accounting for about 55% of body mass.
Figure 3. Intracellular (ICF) and Extracellular (ECF) fluid electrolyte concentrations
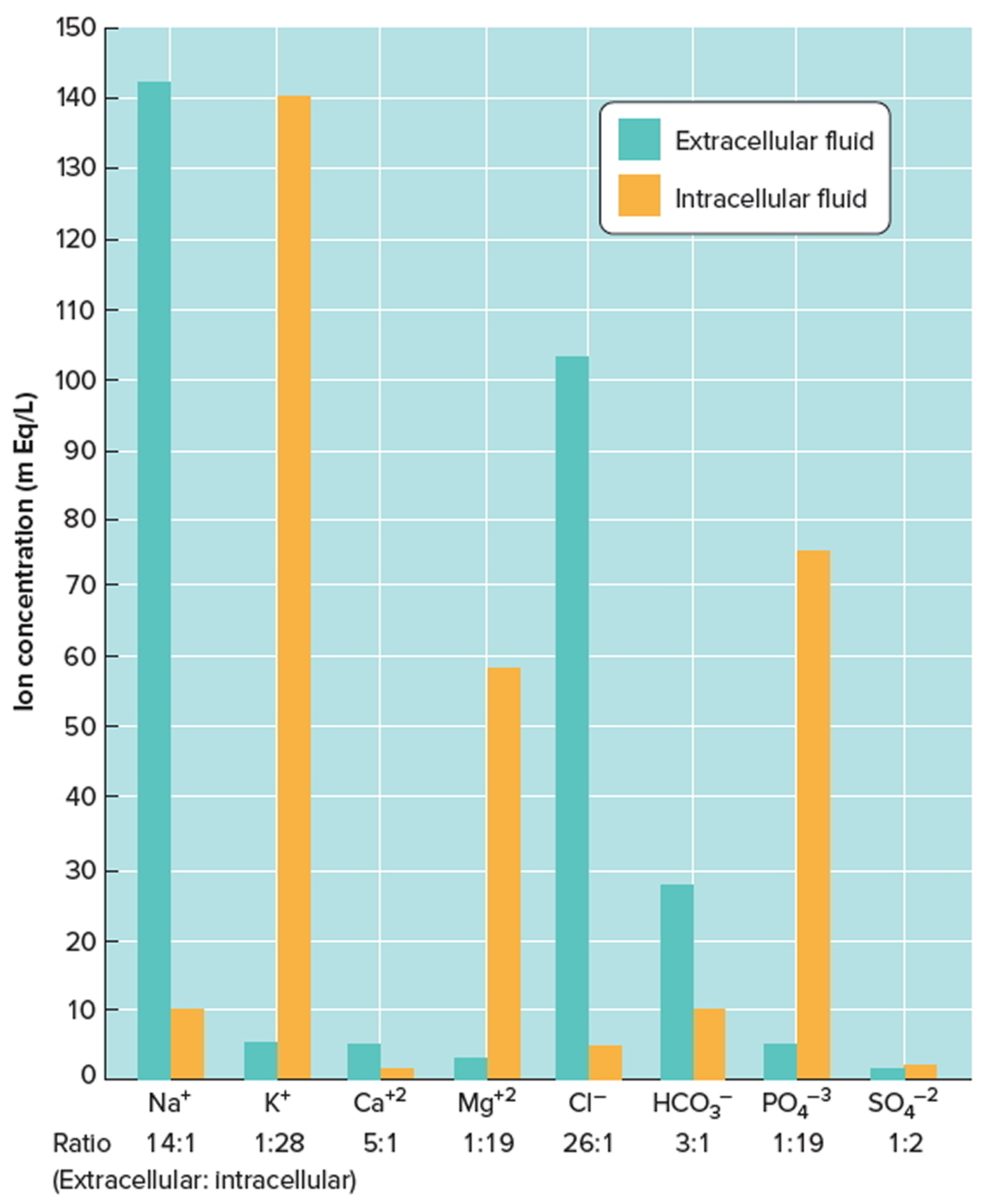
Note: Extracellular fluids have relatively high concentrations of sodium (Na+), calcium (Ca+2), chloride (Cl−), and bicarbonate (HCO3−) ions. Intracellular fluid has relatively high concentrations of potassium (K+), magnesium (Mg+2), phosphate (PO4−3), and sulfate (SO4−2) ions.
[Source 1]The processes of filtration, reabsorption, diffusion, and osmosis allow continual exchange of water and solutes among body fluid compartments. Yet the volume of fluid in each compartment remains remarkably stable. The pressures that promote filtration of fluid from blood capillaries and reabsorption of fluid back into capillaries. Because osmosis is the primary means of water movement between intracellular fluid and interstitial fluid, the concentration of solutes in these fluids determines the direction of water movement. Because most solutes in body fluids are electrolytes, inorganic compounds that dissociate into ions, fluid balance is closely related to electrolyte balance. Because intake of water and electrolytes rarely occurs in exactly the same proportions as their presence in body fluids, the ability of the kidneys to excrete excess water by producing dilute urine, or to excrete excess electrolytes by producing concentrated urine, is of utmost importance in the maintenance of homeostasis.
Sources of Body Water Gain and Loss
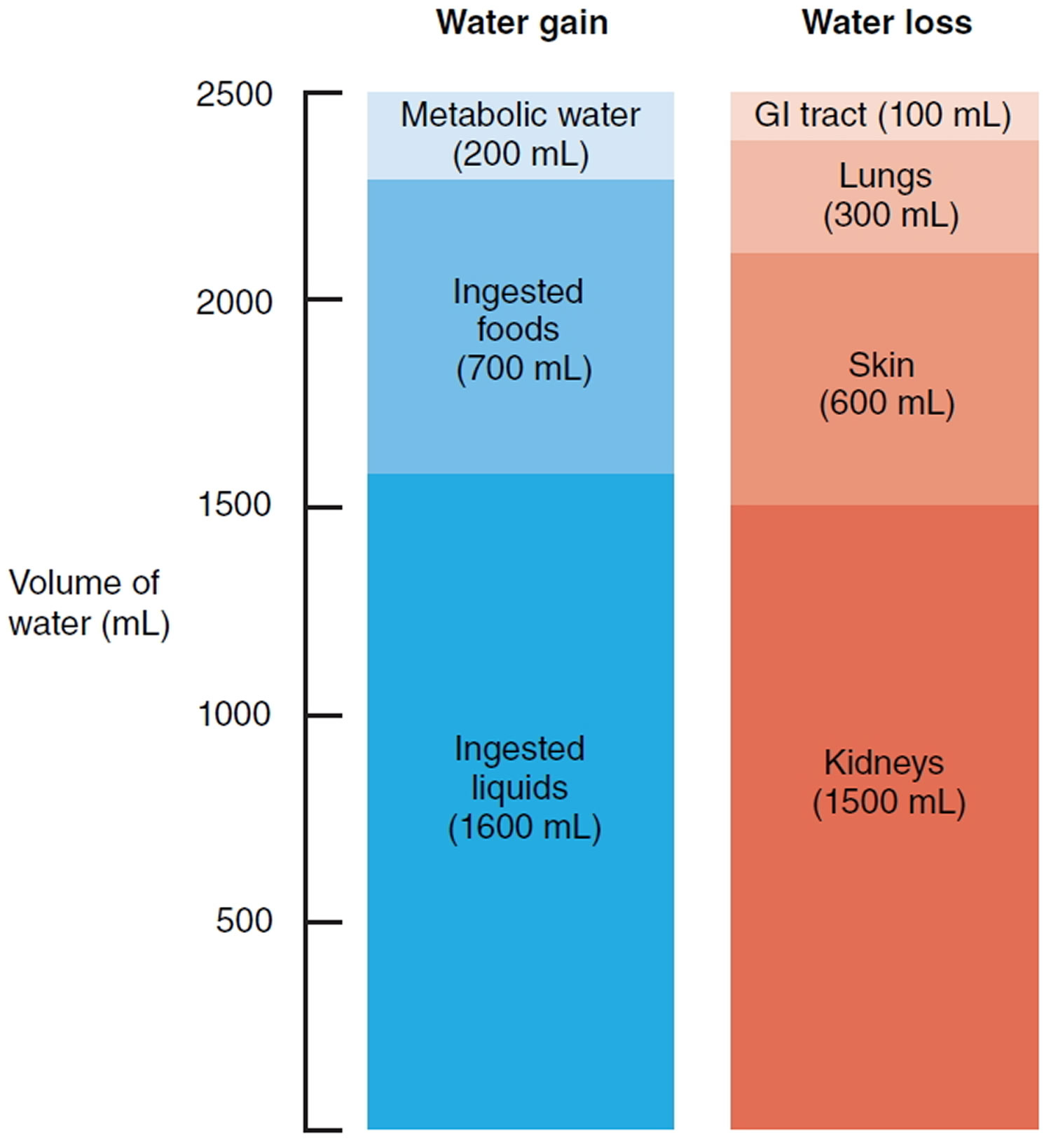
The body can gain water by ingestion and by metabolic synthesis (Figure 4). The main sources of body water are ingested liquids (about 1600 mL) and moist foods (about 700 mL) absorbed from the gastrointestinal (GI) tract, which total about 2300 mL/day. The other source of water is metabolic water that is produced in the body mainly when electrons are accepted by oxygen during aerobic respiration and to a smaller extent during dehydration synthesis reactions. Metabolic water gain accounts for only 200 mL/day. Daily water gain from these two sources totals about 2500 mL.
Normally, body fluid volume remains constant because water loss equals water gain. Water loss occurs in four ways. Each day the kidneys excrete about 1500 mL in urine, the skin evaporates about 600 mL (400 mL through insensible perspiration— sweat that evaporates before it is perceived as moisture—and 200 mL as sweat), the lungs exhale about 300 mL as water vapor, and the gastrointestinal tract eliminates about 100 mL in feces. In women of reproductive age, additional water is lost in menstrual flow. On average, daily water loss totals about 2500 mL. The amount of water lost by a given route can vary considerably over time. For example, water may literally pour from the skin in the form of sweat during strenuous exertion. In other cases, water may be lost in diarrhea during a GI tract infection.
Figure 4. Sources of daily water gain and loss under normal conditions. Numbers are average volumes for adults.
Regulation of Body Water Gain
The volume of metabolic water formed in the body depends entirely on the level of aerobic respiration, which reflects the demand for ATP (Adenosine triphosphate is the energy packets in your cells that is essential for life and your body to function) in body cells. When more ATP is produced, more water is formed. Body water gain is regulated mainly by the volume of water intake or how much fluid you drink. An area in the hypothalamus known as the thirst center governs the urge to drink.
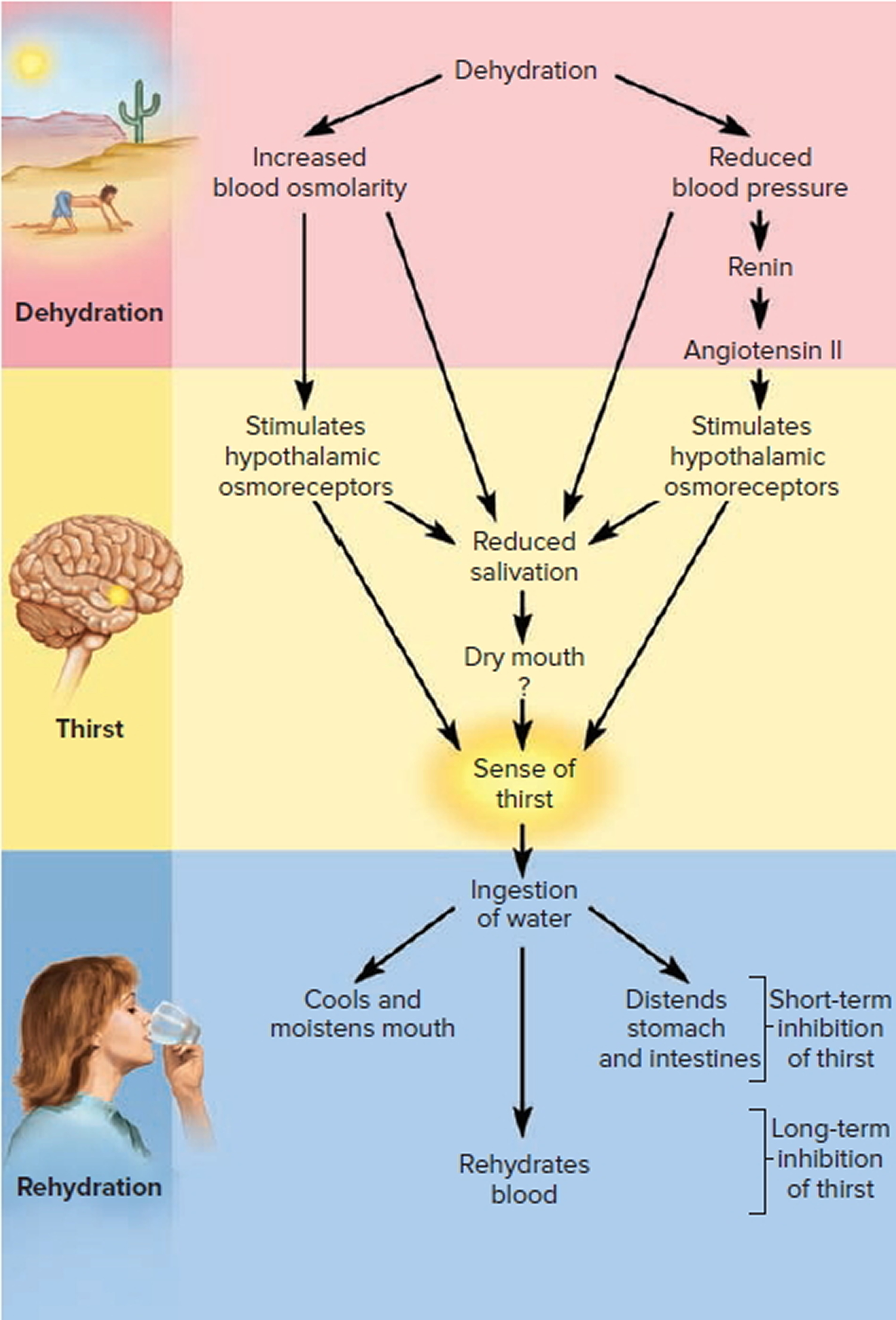
When water loss is greater than water gain, dehydration—a decrease in volume and an increase in osmolarity of body fluids— occurs. A decrease in blood volume causes blood pressure to fall. Increased activity from osmoreceptors in the hypothalamus, triggered by increased blood osmolarity, stimulates the thirst center in the hypothalamus (Figure 5).
Other signals that stimulate the thirst center come from:
- Volume receptors in the atria that detect the decrease in blood volume,
- Baroreceptors in blood vessels that detect the decrease in blood pressure,
- Angiotensin II that is formed due to activation of the renin-angiotensin-aldosterone pathway by the decrease in blood pressure, and
- Neurons in the mouth that detect dryness due to a decreased flow of saliva. As a result of these stimuli, the sensation of thirst increases, which usually leads to increased fluid intake (as long as fluids are available) and restoration of normal fluid volume.
Overall, fluid gain balances fluid loss. Sometimes, however, the sensation of thirst does not occur quickly enough or access to fluids is restricted, and significant dehydration ensues. This happens most oft en in elderly people, in infants, and in those who are in a confused mental state. When heavy sweating or fluid loss from diarrhea or vomiting occurs, it is wise to start replacing body fluids by drinking fluids even before the sensation of thirst occurs.
Figure 5. Regulation of water intake
Regulation of Electrolyte and Water Loss
Even though the loss of water and electrolytes through sweating and exhalation increases during exercise, elimination of excess body water or electrolytes occurs mainly by control of their loss in urine. The extent of urinary salt (NaCl) loss is the main factor that determines body fluid volume. The reason for this is that “water follows electrolytes” in osmosis, and the two main electrolytes in extracellular fluid (and in urine) are sodium ions (Na+) and chloride ions (Cl−). In a similar way, the main factor that determines body fluid osmolarity is the extent of urinary water loss.
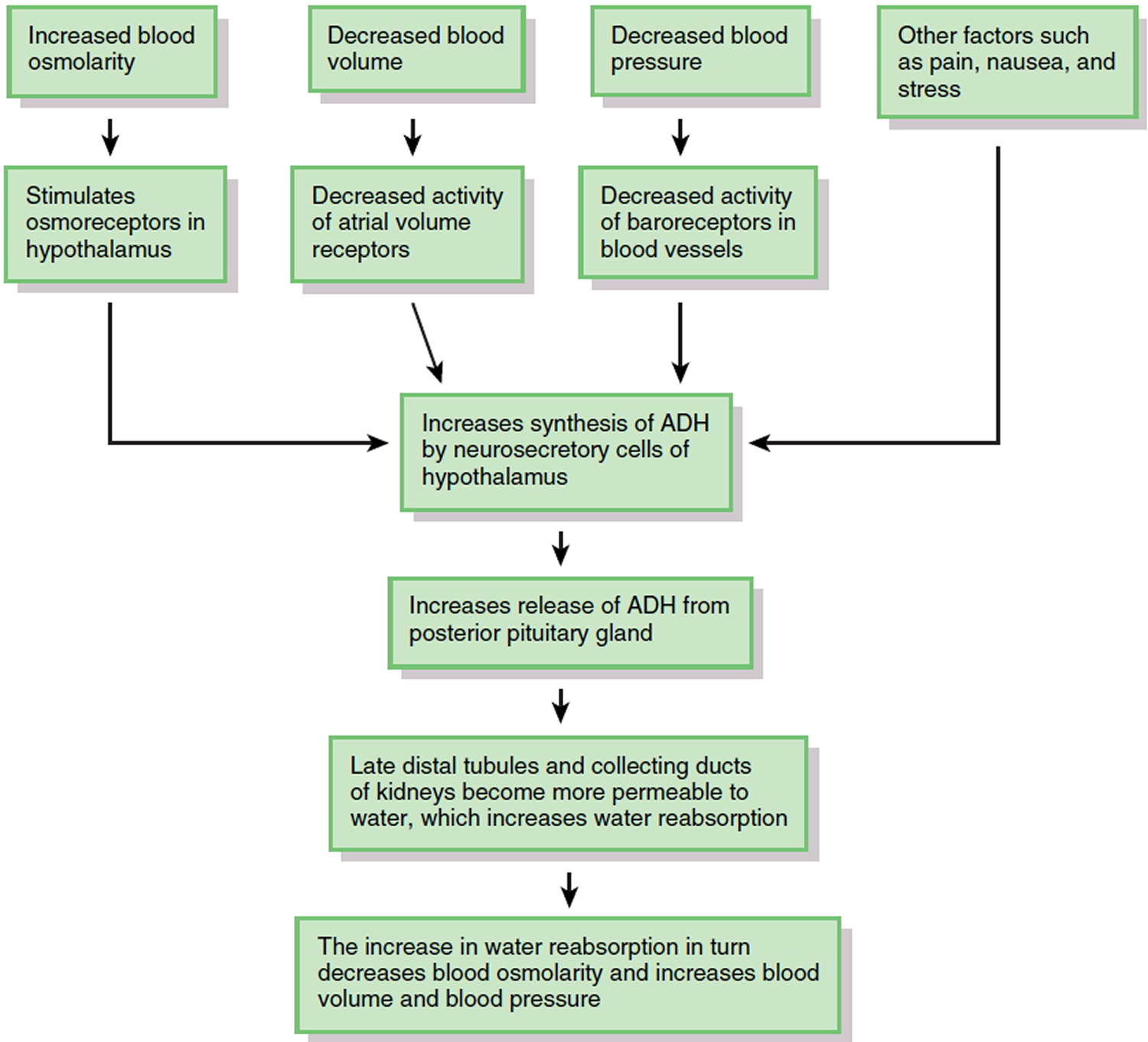
The major hormone that regulates water loss is antidiuretic hormone (ADH). This hormone, also known as vasopressin, is produced by neurosecretory cells in the hypothalamus and stored in the posterior pituitary gland. When the osmolarity of body fluids increases, osmoreceptors in the hypothalamus not only stimulate thirst; they also increase the synthesis and release of ADH (Figure 6). ADH promotes the insertion of water-channel proteins (aquaporin-2) into the apical membranes of principal cells in the late distal tubules and collecting ducts of the kidneys. As a result, the permeability of these cells to water increases. Water molecules move by osmosis from the renal tubular fluid into the cells and then from the cells into the bloodstream. This results in a decrease in blood osmolarity, an increase in blood volume and blood pressure, and the production of a small volume of concentrated urine. Once the body has adequate water, the ADH level in the bloodstream decreases. As the amount of ADH in the blood declines, some of the aquaporin-2 channels are removed from the apical membrane via endocytosis. Consequently, the water permeability of the principal cells decreases and more water is lost in the urine.
Factors other than blood osmolarity influence ADH secretion (Figure 6). A decrease in blood volume or blood pressure also stimulates ADH release. Atrial volume receptors detect the decrease in blood volume, and baroreceptors in blood vessels detect the decrease in blood pressure. ADH release is also stimulated by factors that are unrelated to water balance, such as pain, nausea, and stress. Secretion of ADH is inhibited by alcohol, which is why consumption of alcoholic beverages promotes diuresis (voiding large amounts of urine).
Figure 6. Role of Antidiuretic Hormone (ADH) in water balance
Because your daily diet contains a highly variable amount of NaCl (salt), urinary excretion of Na+ and Cl− must also vary to maintain homeostasis. Hormones regulate the urinary loss of Na+ ions, Cl− ions usually follow Na+ ions because of electrical attraction or because they are transported along with Na+ ions via symporters. The two most important hormones that regulate the extent of renal Na+ reabsorption (and thus how much is lost in the urine) are aldosterone and atrial natriuretic peptide.
- Aldosterone. When there is a decrease in blood pressure, which occurs in response to a decrease in blood volume, or when there is a deficiency of Na+ in the plasma, the kidneys release renin, which activates the renin-angiotensin-aldosterone pathway. Once aldosterone is formed, it increases Na+ reabsorption in the late distal tubules and collecting ducts of the kidneys, which relieves the Na+ deficiency in the plasma. Because antidiuretic hormone (ADH) is also released when blood pressure is low, water reabsorption accompanies Na+ reabsorption via osmosis. This conserves the volume of body fluids by reducing urinary loss of water.
- Atrial natriuretic peptide. An increase in blood volume, as might occur aft er you finish one or more supersized drinks, stretches the atria of the heart and promotes release of atrial natriuretic peptide (ANP). ANP promotes natriuresis, elevated excretion of Na+ into the urine. The osmotic consequence of excreting more Na+ is loss of more water in urine, which decreases blood volume and blood pressure. In addition to stimulating the release of ANP, an increase in blood volume also slows the release of renin from the kidneys. When the renin level declines, less aldosterone is formed, which causes reabsorption of filtered Na+ to slow in the late distal tubules and collecting ducts of the kidneys. More filtered Na+ and water (due to osmosis) thus remain in the tubular fluid to be excreted in the urine.
Table 1. Summary of Factors That Maintain Body Water Balance
FACTOR | MECHANISM | EFFECT |
| Thirst center in hypothalamus | Stimulates desire to drink fluids. | Water gained if thirst is quenched. |
| Antidiuretic hormone (ADH), also known as vasopressin | Promotes insertion of water-channel proteins (aquaporin-2) into apical membranes of principal cells in collecting ducts of kidneys. As a result, water permeability of these cells increases and more water is reabsorbed. | Reduces loss of water in urine. |
| Aldosterone | By promoting urinary reabsorption of Na+, increases water reabsorption via osmosis. | Reduces loss of water in urine. |
| Atrial natriuretic peptide (ANP) | Promotes natriuresis, elevated urinary excretion of Na+, accompanied by water. | Increases loss of water in urine. |
Hyponatremia causes
What causes hyponatremia
Sodium is found mostly in the body fluids outside the cells. Sodium is an electrolyte (mineral). It is very important for maintaining blood pressure. Sodium is also needed for nerves, muscles, and other body tissues to work properly.
When the amount of sodium in fluids outside cells drops below normal, water moves into the cells to balance the levels. This causes the cells to swell with too much water. Brain cells are especially sensitive to swelling, and this causes many of the symptoms of low sodium.
With low sodium level (hyponatremia), the imbalance of water to sodium is caused by one of three conditions:
- Euvolemic hyponatremia — total body water increases, but the body’s sodium content stays the same
- Hypervolemic hyponatremia — both sodium and water content in the body increase, but the water gain is greater
- Hypovolemic hyponatremia — water and sodium are both lost from the body, but the sodium loss is greater
Hyponatremia can be caused by:
- Certain medications. Some medications, such as some water pills (diuretics), antidepressants and pain medications, can cause you to urinate or perspire more than normal.
- Heart, kidney and liver problems. Congestive heart failure and certain diseases affecting the kidneys or liver (liver cirrhosis) can cause fluids to accumulate in your body, which dilutes the sodium in your body, lowering the overall level.
- Syndrome of inappropriate anti-diuretic hormone (SIADH). In this condition, high levels of the anti-diuretic hormone (ADH) are produced, causing your body to retain water instead of excreting it normally in your urine.
- Chronic, severe vomiting or diarrhea. This causes your body to lose fluids and electrolytes, such as sodium.
- Drinking too much water. Because you lose sodium through sweat, drinking too much water during endurance activities, such as marathons and triathlons, can dilute the sodium content of your blood. Drinking too much water at other times can also cause low sodium.
- Dehydration. Taking in too little fluid can also be a problem. If you get dehydrated, your body loses fluids and electrolytes.
Hormonal changes. Adrenal gland insufficiency (Addison’s disease) affects your adrenal glands’ ability to produce hormones that help maintain your body’s balance of sodium, potassium and water. Low levels of thyroid hormone also can cause a low blood-sodium level.
The recreational drug Ecstasy. This amphetamine increases the risk of severe and even fatal cases of hyponatremia. - Burns that affect a large area of the body
- Sweating
Risk factors for hyponatremia
The following factors may increase your risk of hyponatremia:
- Age. Older adults may have more contributing factors for hyponatremia, including age-related changes, taking certain medications and a greater likelihood of developing a chronic disease that alters the body’s sodium balance.
- Certain drugs. Medications that increase your risk of hyponatremia include thiazide diuretics as well as some antidepressants and pain medications. In addition, the recreational drug Ecstasy has been linked to fatal cases of hyponatremia.
- Conditions that decrease your body’s water excretion. Medical conditions that may increase your risk of hyponatremia include kidney disease, syndrome of inappropriate anti-diuretic hormone (SIADH) and heart failure, among others.
- Intensive physical activities. People who drink too much water while taking part in marathons, ultramarathons, triathlons and other long-distance, high-intensity activities are at an increased risk of hyponatremia.
Hyponatremia prevention
Treating the condition that is causing low sodium can help.
If you play sports or do other vigorous activity, drink fluids such as sports drinks that contain electrolytes to keep your body’s sodium level in a healthy range.
The following measures may help you prevent hyponatremia:
- Treat associated conditions. Getting treatment for conditions that contribute to hyponatremia, such as adrenal gland insufficiency, can help prevent low blood sodium.
- Educate yourself. If you have a medical condition that increases your risk of hyponatremia or you take diuretic medications, be aware of the signs and symptoms of low blood sodium. Always talk with your doctor about the risks of a new medication.
- Take precautions during high-intensity activities. Athletes should drink only as much fluid as they lose due to sweating during a race. Thirst is generally a good guide to how much water or other fluids you need.
- Consider drinking sports beverages during demanding activities. Ask your doctor about replacing water with sports beverages that contain electrolytes when participating in endurance events such as marathons, triathlons and other demanding activities.
- Drink water in moderation. Drinking water is vital for your health, so make sure you drink enough fluids. But don’t overdo it. Thirst and the color of your urine are usually the best indications of how much water you need. If you’re not thirsty and your urine is pale yellow, you are likely getting enough water.
Hyponatremia outlook (prognosis)
Outcome depends on the condition that is causing the problem. Low sodium that occurs in less than 48 hours (acute hyponatremia), is more dangerous than low sodium that develops slowly over time. When sodium level falls slowly over days or weeks (chronic hyponatremia), the brain cells have time to adjust and swelling may be minimal.
Hyponatremia possible complications
In severe cases, low sodium can lead to:
- Decreased consciousness, hallucinations or coma
- Brain herniation
- Death
In acute hyponatremia, sodium levels drop rapidly — resulting in potentially dangerous effects, such as rapid brain swelling, which can result in coma and death.
In chronic hyponatremia, sodium levels drop gradually over 48 hours or longer — and symptoms and complications are typically more moderate.
Premenopausal women appear to be at the greatest risk of hyponatremia-related brain damage. This may be related to the effect of women’s sex hormones on the body’s ability to balance sodium levels.
Hyponatremia signs and symptoms
Signs and symptomsof hyponatremia
- Confusion, irritability, restlessness
- Convulsions (seizures)
- Fatigue
- Headache
- Loss of appetite
- Loss of energy and fatigue
- Muscle weakness, spasms, or cramps
- Nausea, vomiting
- Coma
Hyponatremia diagnosis
The health care provider will perform a complete physical examination and ask about your symptoms.
The signs and symptoms of hyponatremia occur in many conditions, it’s impossible to diagnose the condition based on a physical exam alone. To confirm low blood sodium, your doctor will order blood tests and urine tests.
Lab tests that can confirm and help diagnose low sodium include:
- Comprehensive metabolic panel (includes blood sodium, normal range is 135 to 145 mEq/L, or 135 to 145 mmol/L)
- Osmolality blood test
- Urine osmolality
- Urine sodium (normal level is 20 mEq/L in a random urine sample, and 40 to 220 mEq/L for a 24-hour urine test).
Hyponatremia treatment
The cause of low sodium must be diagnosed and treated. Hyponatremia treatment is aimed at addressing the underlying cause, if possible. If cancer is the cause of the condition, then radiation, chemotherapy, or surgery to remove the tumor may correct the sodium imbalance.
If you have moderate, chronic hyponatremia due to your diet, diuretics or drinking too much water, your doctor may recommend temporarily cutting back on fluids. He or she also may suggest adjusting your diuretic use to increase the level of sodium in your blood.
Other treatments depend on the specific type of hyponatremia.
Treatments may include:
- Fluids through a vein (IV). Your doctor may recommend IV sodium solution to raise the sodium levels in your blood. This often requires a stay in the hospital.
- Medicines to relieve symptoms. You may take medications to manage the signs and symptoms of hyponatremia, such as headache, nausea and seizures.
- Limiting water intake
- Hole’s Essentials of Human Anatomy and Physiology 13th edition. Published by McGraw-Hill Education, 2 Penn Plaza, New York, NY 10121.[↩]





{kind=link}