Contents
What is an ileostomy
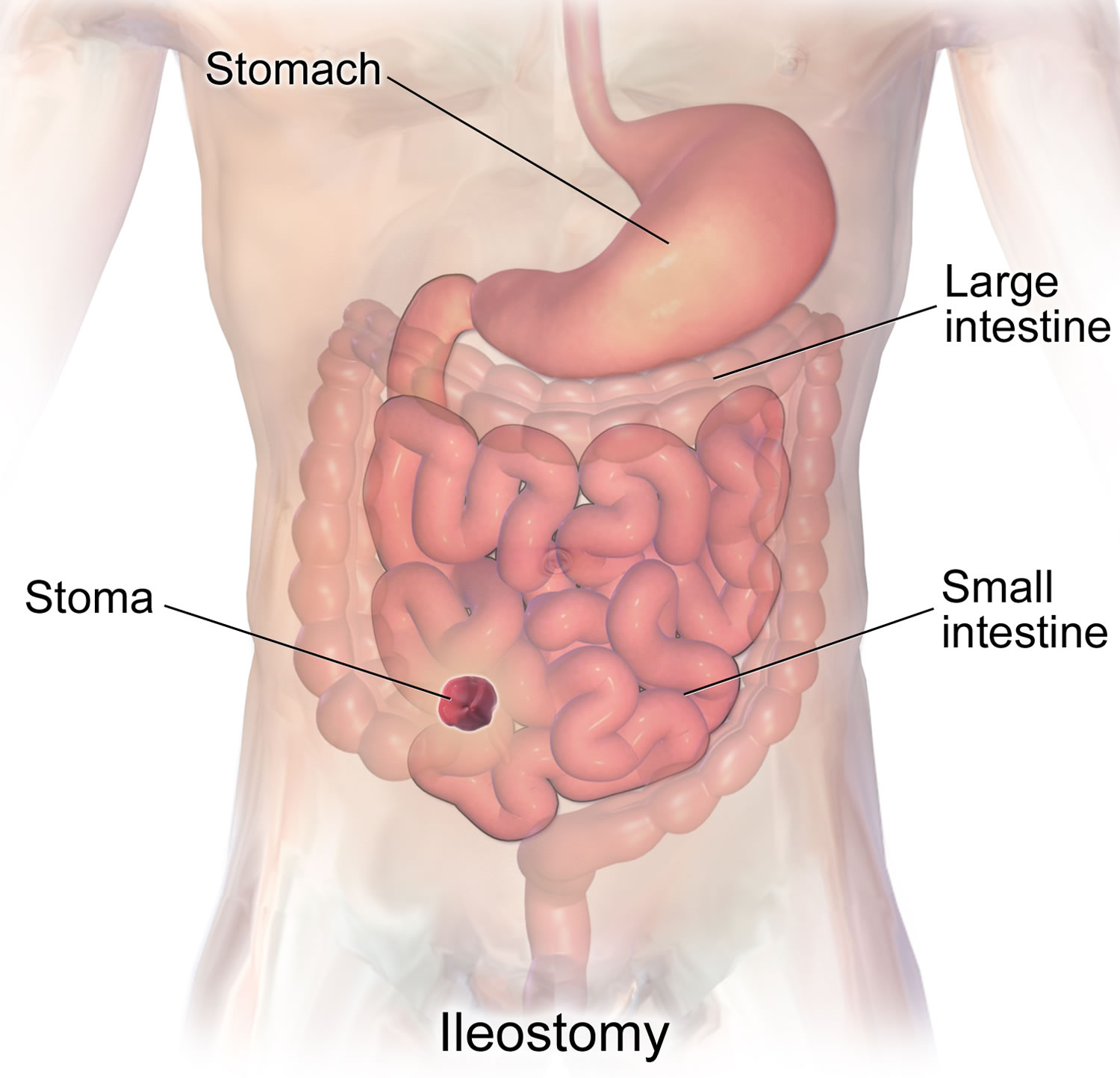
An ileostomy is a surgically made opening on the skin of the belly where the small bowel (small intestine) called the ileum is brought to the surface of your abdomen to form the stoma (the opening). An ileostomy replaces the rectum as the place where waste of the digestive system (stool) leaves your body. An ileostomy is typically made in cases where the end part of the small bowel is diseased, and is usually made on the right-hand side of your abdomen. Stools in this part of the small intestine are generally fluid or thick liquid and it is not solid like the stool that came from your rectum. Because a stoma has no muscle to control defecation, stools will need to be collected in an ileostomy bag. An ileostomy bag is placed over the stoma to collect waste products that usually pass through the colon (large intestine) and out of the body through the rectum and back passage (anus).
An ileostomy may be needed if the colon is damaged, inflamed or doesn’t work properly.
Most often the colon (large intestine) absorbs most of the water that you eat and drink. With an ileostomy in place, the colon is no longer being used. This means that the stool from your ileostomy has far more liquid than a typical bowel movement from the rectum.
The stool now comes out from the ileostomy and empties into a pouch that is attached to the skin around your stoma. The ileostomy bag is made to fit your body well. You must wear it all the time.
The waste that collects will be liquid or pasty, depending on what you eat, what medicines you take, and other things. Waste collects constantly, so you will need to empty the ileostomy bag 5 to 8 times a day.
Stomas do vary in size and shape from person to person. It will be shiny, wet and red, much like the inside of your mouth. You can expect it be swollen after surgery but the swelling will go down in time and your stoma may get smaller.
Figure 1. Small intestine
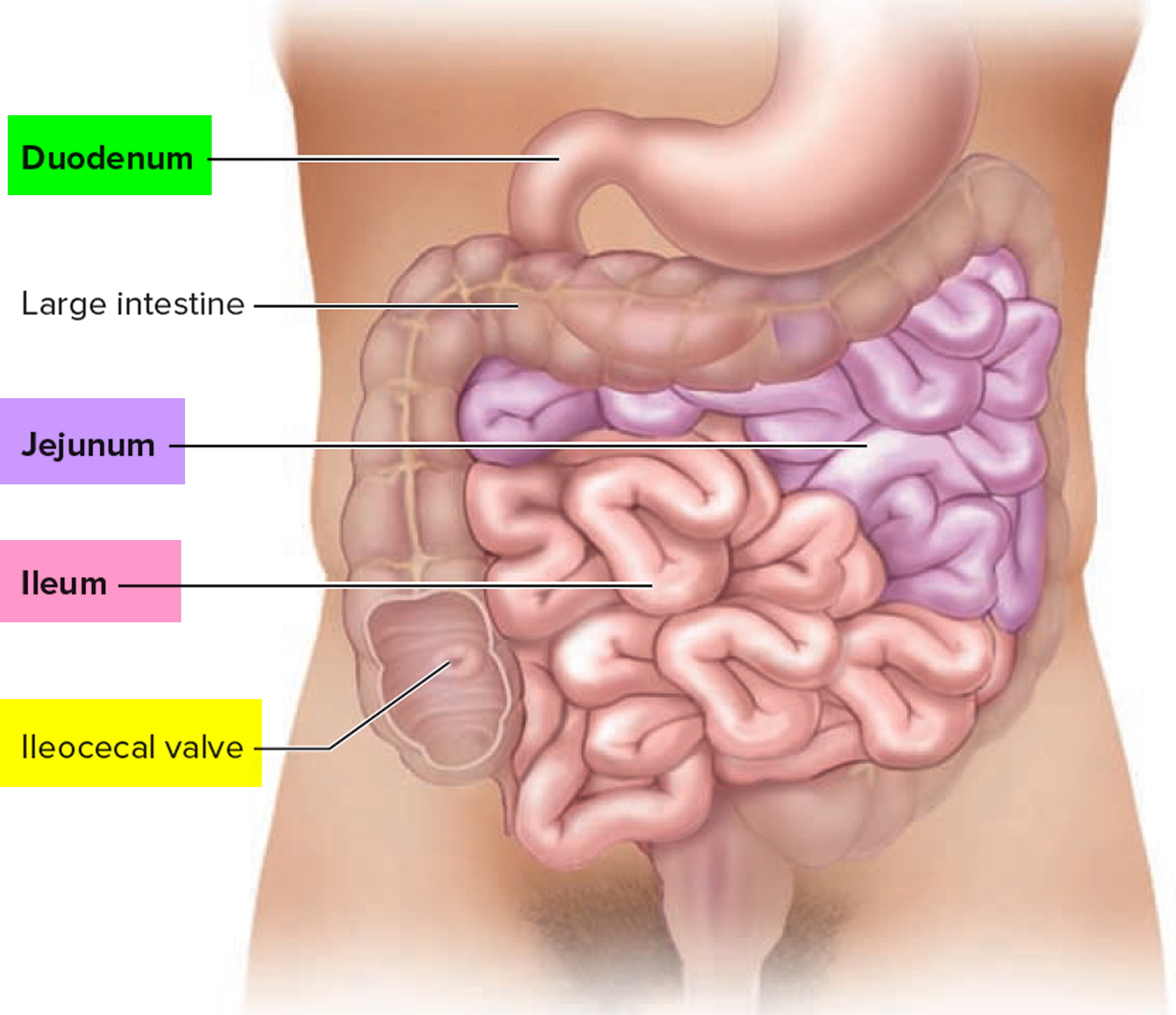
Figure 2. Ileostomy
When is an ileostomy needed?
An ileostomy is formed to either temporarily or permanently stop digestive waste passing through the full length of the small intestine or colon.
An ileostomy may be needed if the colon is damaged, inflamed or doesn’t work properly.
Some of the most common reasons why ileostomy surgery to form an ileostomy is carried out are described below.
There are a number of reasons why this may be necessary, including:
- to allow the small intestine or colon to heal after it’s been operated on – for example, if a section of bowel has been removed to treat bowel cancer
- to relieve inflammation of the colon in people with Crohn’s disease or ulcerative colitis
- to allow for complex surgery to be carried out on the anus or rectum
Crohn’s disease
Crohn’s disease is a long-term condition where the digestive system becomes inflamed. Common symptoms include:
- diarrhea
- abdominal pain
- extreme tiredness (fatigue)
Crohn’s disease can usually be controlled with medication, but surgery to create an ileostomy may sometimes be recommended to temporarily divert digestive waste away from the inflamed section of the digestive system to give it a chance to heal.
Ulcerative colitis
Ulcerative colitis is a long-term condition where the lining of the large intestine or large bowel (colon or rectum) becomes inflamed. Common symptoms include:
- bloody diarrhea
- abdominal pain
- a frequent need to pass stools
In most cases symptoms can be controlled with medication. However, surgery to remove the colon and form an ileostomy or ileo-anal pouch – an internal pouch to store stools created using the end of the small intestine – may be recommended if the condition is particularly severe or doesn’t respond to medication.
Bowel cancer
Bowel cancer is a type of cancer that develops inside the colon or rectum. Chemotherapy or radiotherapy, or a combination of both, may be used to shrink the cancer first, before the affected section of bowel is removed.
Depending on the size and position of the removed section of bowel, a temporary ileostomy, permanent ileostomy, or an ileo-anal pouch may be formed during the operation.
In some cases, a section of your colon may need to be diverted out of your tummy (abdomen). This is known as a colostomy, rather than an ileostomy.
Less common uses
Some of the less common reasons why surgery to form an ileostomy is needed are described below.
Familial adenomatous polyposis
Familial adenomatous polyposis (FAP) is a rare condition that triggers the growth of non-cancerous lumps of tissue inside the colon.
Although the lumps are non-cancerous to begin with, there’s a very high risk that, over time, at least one will turn cancerous. More than 99% of people with FAP have bowel cancer by the time they’re 50 years old.
Because of the high risk of developing cancerous lumps, it’s usually recommended that a person diagnosed with FAP has their colon removed. It’s usually replaced with an ileo-anal pouch, or occasionally a permanent ileostomy.
Bowel obstruction
A bowel obstruction occurs when part of the digestive system becomes blocked by food, fluids, or waste products. This can happen if part of the person’s digestive system is scarred or inflamed, or if their digestive system is unusually narrow.
If the colon becomes completely blocked, it’s usually necessary to remove the colon and form an ileostomy. This can be temporary or permanent, depending on the underlying cause of the obstruction.
Injury
A significant injury to the colon, such as a puncture or impact injury, can result in the colon becoming permanently damaged.
In these cases, it may be necessary to remove the colon and form an ileostomy. Whether this is a temporary or permanent ileostomy depends on the type and extent of the injury.
Ileostomy surgery
There are several different ways an ileostomy can be formed, depending on the reason why the operation is being carried out.
The opening in your abdomen where waste material exits the body after the operation (stoma) will normally be located on the righthand side.
However, you’ll usually meet a specialist stoma nurse before the operation to discuss specific possible locations. The stoma nurse may draw a dot on your abdomen to let the surgeon know where the preferred site is.
Ileostomy operations are carried out under general anaesthetic, which means you’ll be asleep during the procedure and won’t experience any pain as it’s carried out.
The main types of ileostomy are described below.
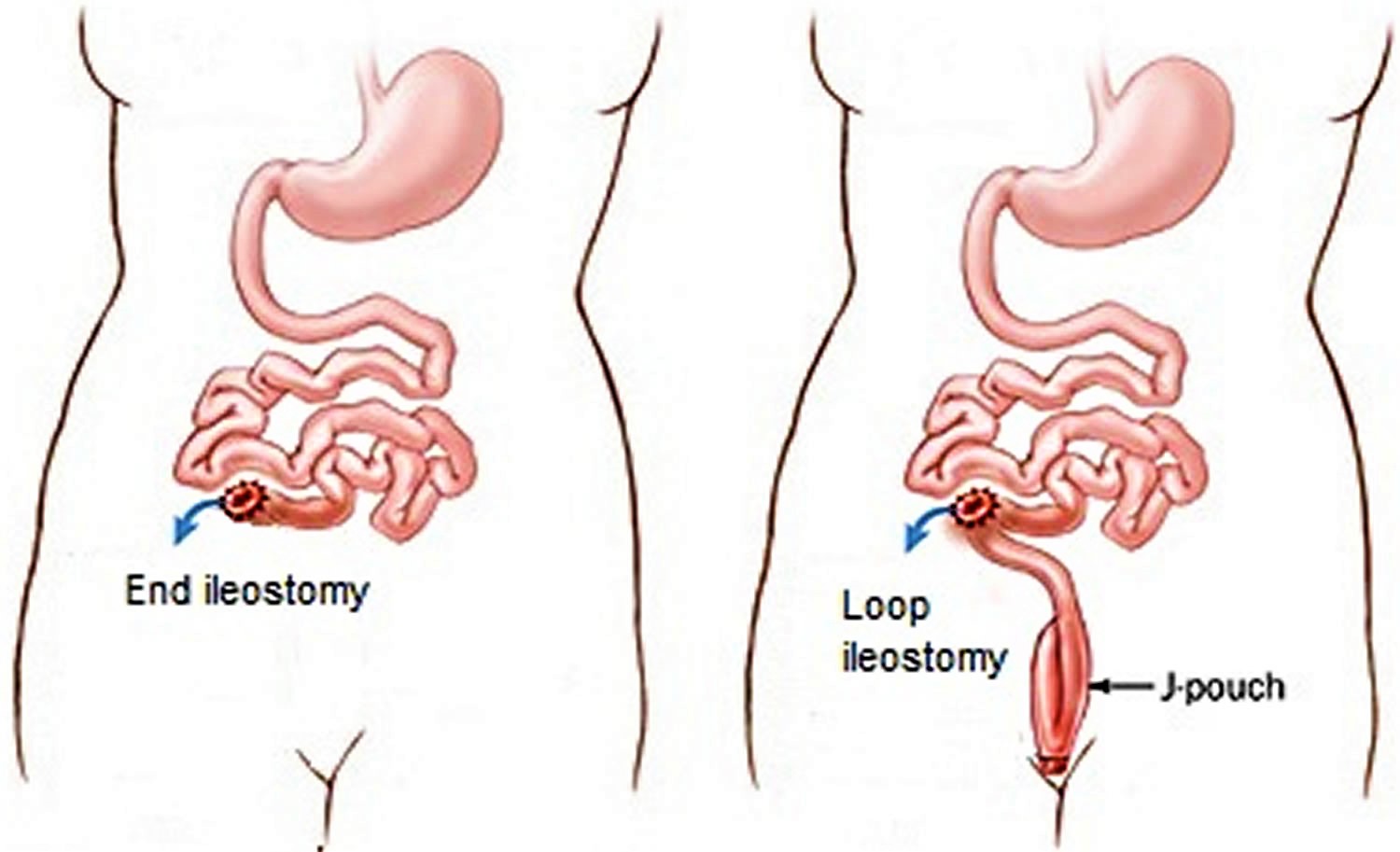
Figure 3. Types of ileostomy surgery
End ileostomy
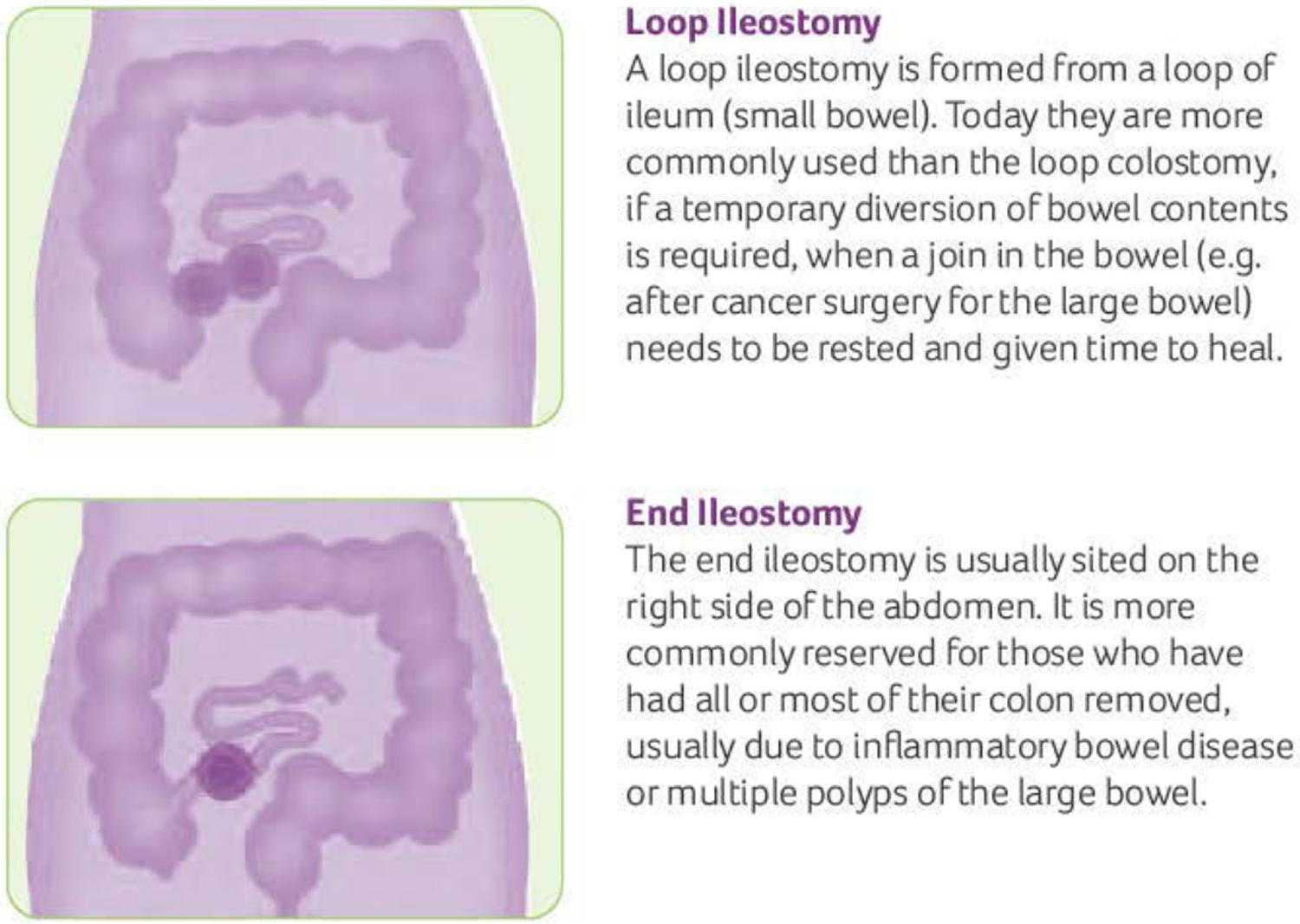
An end ileostomy is made when part of your large intestine (colon) is removed (or simply needs to rest) and the end of your small intestine is brought to the surface of the abdomen to form a stoma. An end ileostomy can be temporary or permanent.
The end of the small intestine (ileum) is divided and brought out of the abdomen through a smaller incision, and stitched on to the skin to form a stoma.
Over time, the stitches dissolve and the stoma heals on to the skin. After the operation, waste material comes out of the opening in the abdomen into a bag that goes over the stoma.
This type of ileostomy is often, but not always, permanent.
The permanent ileostomy is chosen in situations where it is too risky or not possible to re-join the two parts of the intestine.
The temporary ileostomy is relevant in situations where the diseased part of the large intestine (colon) has been removed and the remaining part needs to rest before the ends are joined together. It’s sometimes possible to reverse an end ileostomy if most of the large intestine (colon) has been sealed and left inside the abdomen. However, the surgeon will need to make a larger incision to locate and reattach the small and large intestines. It therefore takes longer to recover from this type of surgery and there’s a greater risk of complications.
Loop ileostomy
In a loop ileostomy, a loop of the small intestine is lifted above skin level and held in place with a stoma rod. A cut is made on the exposed bowel loop, and the ends are then rolled down and sewn onto the skin. In this way, a loop ileostomy actually consists of two stomas that are joined together. The colon and rectum are left in place.
The loop ileostomy is typically temporary and performed to protect a surgical join in the bowel. If temporary, it will be closed or reversed in a later operation.
To form a loop ileostomy, a loop of small intestine is pulled out through a cut (incision) in your abdomen.
This section of intestine is then opened up and stitched to the skin to form a stoma.
In these cases, the stoma will have two openings, although they’ll be close together and you may not be able to see both.
One of the openings is connected to the functioning part of your bowel. This is where waste products leave your body after the operation.
The other opening is connected to the “inactive” part of your bowel that leads down to your rectum.
The loop ileostomy is usually temporary and may be reversed during a second operation at a later date. There’s no time limit for having an ileostomy reversed and some people may live with one for several years before it’s reversed. Reversing a loop ileostomy is a relatively straightforward procedure that’s carried out under general anesthesia.
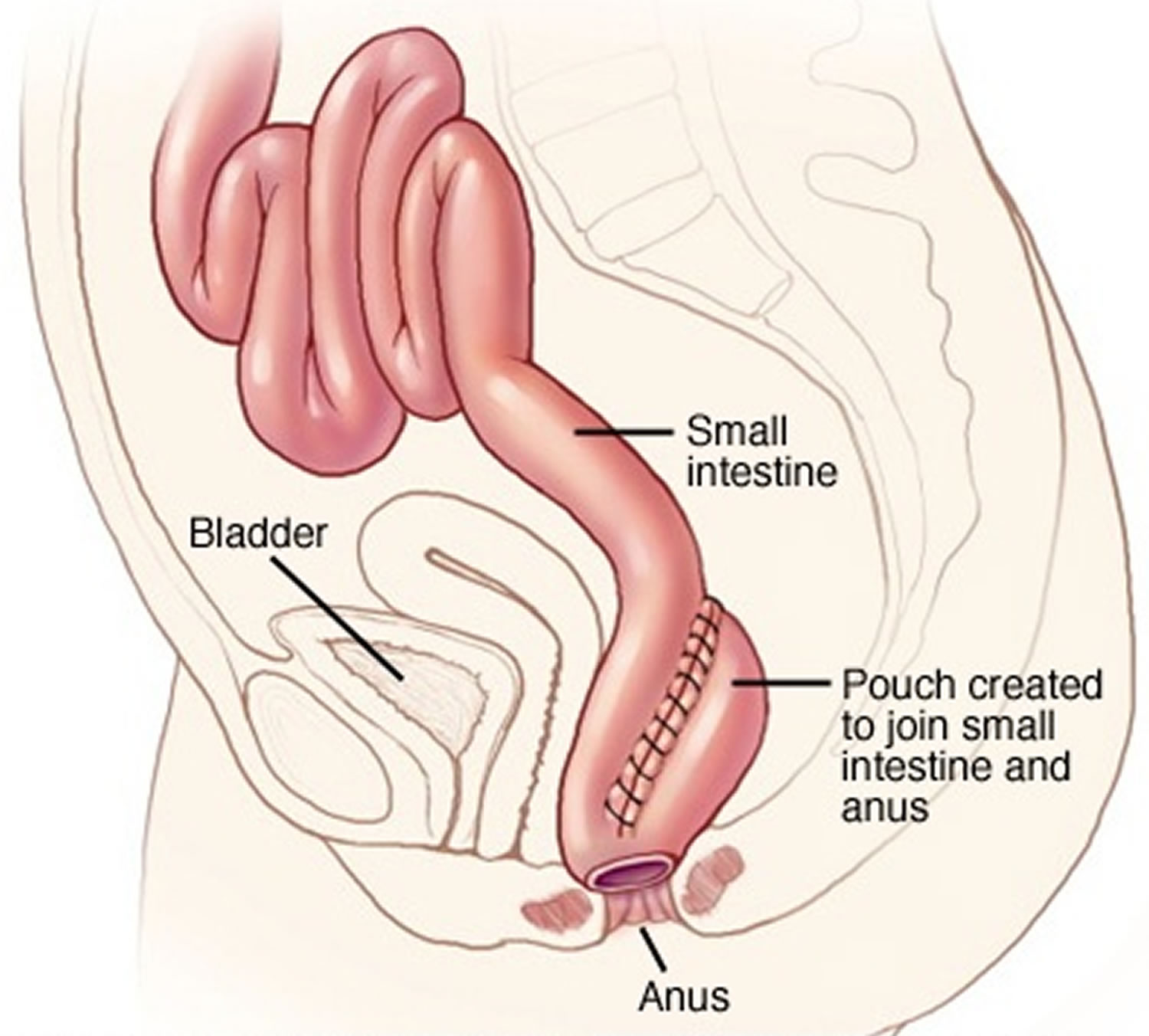
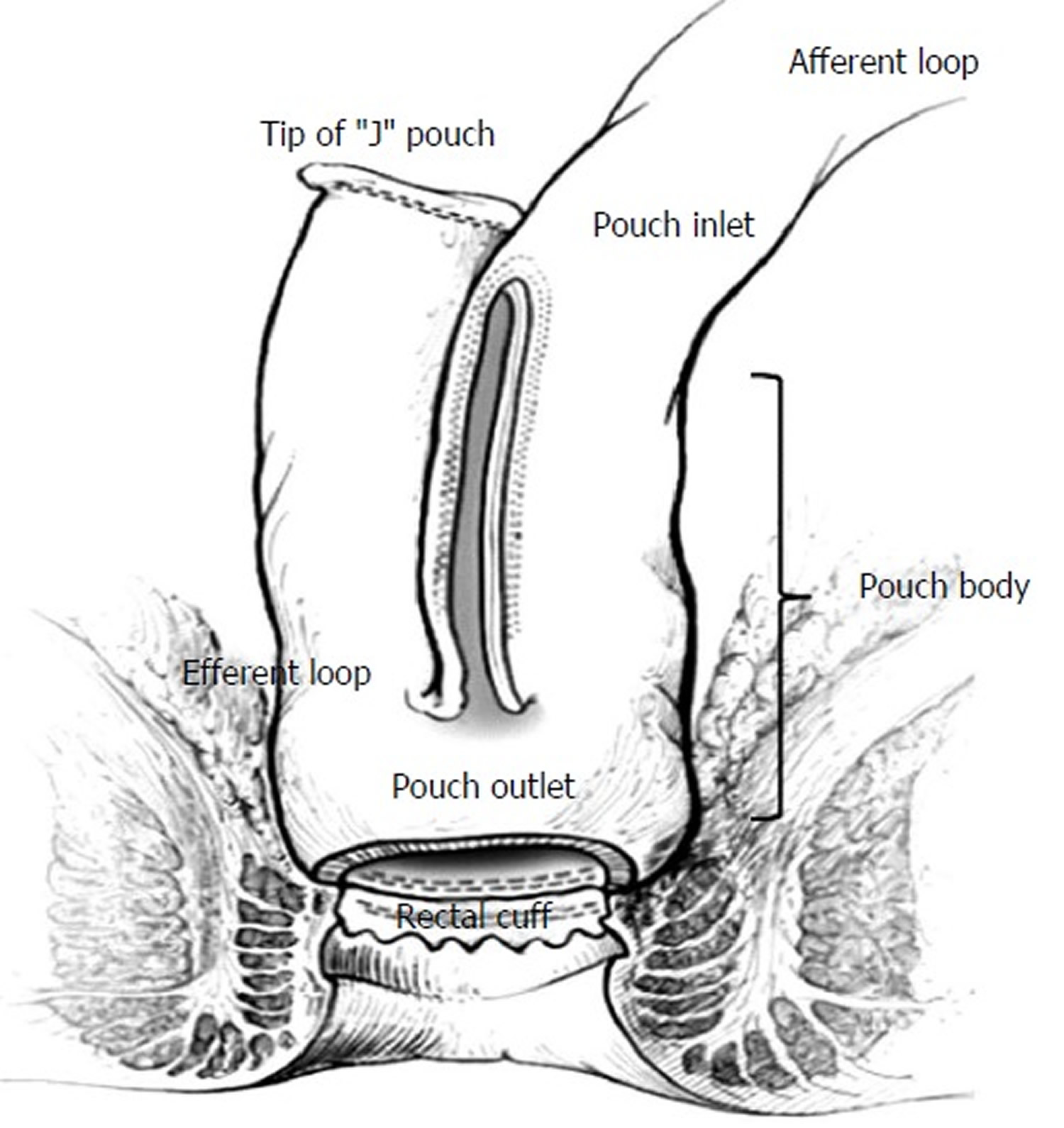
Ileo-anal pouch
In some cases, it may be possible to have a permanent internal ileo-anal pouch, also known as a J pouch, formed instead of an ileostomy.
An ileo-anal pouch is created from the ileum and joined to the anus, so waste material passes out of your body in the normal way. The pouch stores the waste material until you excrete it when you go the toilet.
The area around the pouch usually needs to heal before it’s used, so a temporary loop ileostomy may be created above the pouch. A second, smaller operation is usually carried out a few months later to close the loop ileostomy.
Figure 4. Ileo-anal pouch (J-pouch)
Ileostomy recovery
After an ileostomy surgery, you may need to stay in hospital for up to two weeks. During this time you’ll be taught how to look after your stoma by a specialist stoma nurse.
When you wake up after the operation, you may be attached to a drip placed directly into your vein that provides fluids (an intravenous drip) and have an oxygen mask or nasal tubes (cannula) to help you breathe. These will be removed as you recover.
A special bag is also placed over the opening in your abdomen (stoma). The stoma will initially appear large because the effects of surgery cause it to swell. It usually shrinks during the weeks after the operation, reaching its final size after about eight weeks.
Recovering from an ileostomy procedure can be challenging. Many people experience short-term physical and psychological problems, ranging from skin irritation around the stoma to feelings of anxiety and self-consciousness.
However, with practise and support from a designated stoma nurse, many people adjust and often find their quality of life improves after ileostomy surgery. This is especially true if they’ve been living for years with a condition such as Crohn’s disease.
Stoma nurse
While you’re recovering in hospital, a stoma nurse will teach you how to care for your stoma, including how to empty and change the bag.
They’ll also teach you how to keep your stoma and the surrounding skin clean and free from irritation. The nurse will explain the different types of equipment available and how to get new supplies.
Going home
You may need to stay in hospital for up to two weeks after the operation, although this varies depending on things like your general health and the type of operation.
Your stoma nurse or surgeon will give you advice about activities to avoid while you recover. Most normal activities are usually possible within eight weeks, although you’ll often be advised to avoid more strenuous activities for about three months.
Your abdomen will feel very sore initially during your recovery, but eventually settles down. You may also experience excessive gas (flatulence) and unpredictable discharge from your stoma during the first few weeks of recovery. This should start to improve as you recover from the effects of the operation.
Ileostomy complications
As with any surgical procedure, having an ileostomy surgery carries a risk of complications. Discuss the risks with your surgeon before the ileostomy procedure. Some of the problems people with an ileostomy experience include:
- a bowel obstruction – where the output of digestive waste is blocked
- vitamin B12 deficiency – caused by the removal of part of the intestine that absorbs vitamin B12
- stoma problems – such as widening or narrowing of the stoma, making it difficult to attach the external bag
Some of the main problems that can occur after an ileostomy or ileo-anal pouch procedure are described below.
Obstruction
Sometimes the ileostomy doesn’t function for short periods of time after surgery. This isn’t usually a problem, but if your stoma isn’t active for more than six hours and you experience cramps or nausea, you may have an obstruction.
If you think you may have an obstruction, contact your doctor or stoma nurse for advice. They may recommend:
- avoiding solid foods for the time being
- drinking plenty of fluids
- massaging your tummy and the area around your stoma
- lying on your back, pulling your knees up to your chest and rolling from side to side for a few minutes
- taking a hot bath for 15-20 minutes to help relax the muscles in your tummy
In persistent or severe cases, you may be advised to go to your nearest accident and emergency department as there’s a risk your bowel could burst (rupture).
Dehydration
You’re at an increased risk of becoming dehydrated if you have an ileostomy because the large intestine, which is either removed or unused if you have an ileostomy, plays an important role in helping absorb water from food waste.
This makes it important to make sure you drink enough fluids to keep your urine a pale yellow color to prevent complications of dehydration, such as kidney stones and even kidney failure.
Rectal discharge
People who have an ileostomy but have an intact large intestine often experience a discharge of mucus from their rectum.
Mucus is a liquid produced by the lining of the bowel that acts as a lubricant, helping the passage of stools. It’s still produced even though it no longer serves any purpose.
The mucus can vary from a clear “egg white” to a sticky, glue-like consistency. If there’s blood or pus in the discharge, contact your doctor as it may be a sign of infection or tissue damage.
Many people find the most effective method of managing rectal discharge is to sit on the toilet each day and push down as if passing a stool. This should help remove any mucus located in the rectum and prevent it building up.
Contact your doctor if you find this hard to do or it’s not helping, as you may need further treatment.
Vitamin B12 deficiency
Some people who have had an ileostomy will experience a gradual decrease in their levels of vitamin B12. Vitamin B12 plays an important role in keeping the brain and nervous system healthy.
This decrease is thought to occur because the part of the intestine removed during the procedure is responsible for absorbing some vitamin B12 from the food you eat.
In some people, the fall in vitamin B12 levels can cause a condition called vitamin B12 anemia, which is also sometimes known as pernicious anemia.
Symptoms of vitamin B12 anemia include:
- unexplained fatigue (extreme tiredness) and lethargy (lack of energy)
- breathlessness
- feeling faint
- irregular heartbeats (palpitations)
- headache
- hearing sounds coming from inside the body rather than from an outside source (tinnitus)
- loss of appetite
If you’ve had an ileostomy and experience any of these symptoms, contact your doctor. They’ll be able to arrange a blood test to check your vitamin B12 levels.
It’s important not to ignore these types of symptoms – if vitamin B12 deficiency is left untreated, it can cause more serious problems with your nervous system, such as memory loss and damage to the spinal cord.
If a diagnosis of vitamin B12 deficiency or anemia is confirmed, treating the condition is relatively straightforward and involves taking regular vitamin B12 supplements in the form of injections or tablets.
Stoma problems
Some people with an ileostomy experience problems related to their stoma, such as:
- irritation and inflammation of the skin around the stoma
- narrowing of the stoma (stoma stricture)
- widening of the stoma (stoma prolapse)
- an internal part of the body, such as an organ, pushing through a weakness in the muscle or surrounding tissue wall (parastomal hernia)
- the stoma sinking below the level of the skin after the initial swelling goes down (stoma retraction)
- the stoma may get longer with time as more of the bowel pushes itself out of the abdomen (prolapse)
If you think you may have a problem with your stoma, contact your doctor or stoma nurse for advice.
Skin irritation can usually be treated with topical treatments, such as a spray, but you may need to have further surgery to correct physical problems related to your stoma.
Phantom rectum
Phantom rectum is a complication that can affect people with ileostomies. The condition is similar to a phantom limb, where people who have had a limb amputated feel it’s still there.
People with phantom rectum feel like they need to go to the toilet, even though they don’t have a working rectum. This feeling can continue many years after surgery. Some people have found sitting on a toilet can help to relieve this feeling.
Pouchitis
Pouchitis is when an internal pouch becomes inflamed. It’s a common complication in people with an ileo-anal pouch or continent ileostomy.
Symptoms of pouchitis include:
- diarrhea, which is often bloody
- abdominal pains
- stomach cramps
- a high temperature (fever)
Speak to your doctor if you have symptoms of pouchitis. The condition can usually be successfully treated with a course of antibiotics.
Short bowel syndrome
This condition happens when surgery is done to remove a large part of the small intestine. Short bowel syndrome needs special attention because there’s not enough intestine left to absorb the nutrients the body needs.
People with short bowel syndrome must be under a doctor’s care. They must be closely watched to make sure they’re taking in enough calories, carbohydrates, proteins, fats, vitamins, and minerals. They can live a normal life, but must be careful to avoid diarrhea, and be within quick reach of medical care. The shorter the small intestine, the more watery the discharge will be. This may reduce the time a pouch can be worn because the skin barrier breaks down more rapidly.
Ileostomy care
A stoma is not sensitive to the touch but may bleed slightly if irritated or rubbed. This bleeding is normal but if it continues or if you see blood in your stool, contact your doctor.
The skin around your stoma (called the peristomal skin) should look and feel like the rest of the skin on your belly. It is important to keep stool off your skin to help prevent skin irritation.
- Sore Skin
If the skin around the stoma becomes red and inflamed this can be due to damage when removing the flange/base plate. Using an adhesive remover may help to prevent this. With a two-piece or drainable ileostomy bag the flange/base-plate remains in place for several days which reduces skin damage. Sore skin can also result from contact between the contents of the ileostomy bag and the skin. Stomas can change in size and shape so check the size of the stoma every few months to make sure the hole in the flange/base-plate fits snugly around the stoma, so that the skin is not exposed. If the problem continues, consult a stoma care nurse who can advise on special products which can heal the skin and do not interfere with the adhesion of the appliance.
- Bleeding
The stoma bleeds easily if it is rubbed a bit too hard. If the bleeding does not stop, or the blood is coming from inside the stoma, consult a stoma care nurse. The stoma may bleed more easily if anticoagulant drugs e.g. Warfarin, or aspirin, are being taken.
- Ballooning
This occurs when gas, expelled through the stoma, collects inside the bag causing it to inflate. Most bags have a filter which allows this gas to escape. Occasionally the filter will become blocked and the bag will need to be changed. If this is happening on a regular basis it may be worth trying a different bag which may have a more effective filter. To ensure the filter doesn’t get wet and become ineffective, when in the bath or shower, cover it with the sticky patch supplied in the box of stoma appliances.
- Pancaking
This occurs when, instead of dropping to the bottom of the bag, the bowel motion collects around the stoma and may seep between the flange and the skin. One of the reasons this happens is because there isn’t enough air in the bag and the two sides stick together. It may help to cover the filter with a sticky patch to prevent gas escaping from the bag or place a small piece of crumpled tissue inside the bag to keep the sides apart. Lubricating the inside of the bag with baby oil or a special gel may help the motion to drop to the bottom of the bag.
- Constipation
Eating more fiber and fruit should help to make motions softer. Constipation can also be the result of not drinking enough fluid or the side effect of medication e.g. certain painkillers or antidepressants (check with your doctor or pharmacist). Unless prescribed by the doctor or stoma care nurse do not use suppositories or enemas as the stoma will reject them. If the stoma has not worked for several days or there is pain or vomiting seek medical advice.
- Loose motions
If a large section of the colon has been removed it is likely that motions will always be fairly liquid and it may be easier to use a drainable bag. If motions are normally formed an episode of diarrhea could be due to a “stomach bug”, stress or emotional upset or certain medication e.g. antibiotics. If diarrhea persists it is important to seek medical advice.
- Odor
There will only be an odor when emptying or changing the bag. This can be reduced by spraying a deodorant or striking a match. Odor while the bag is in place could indicate a leakage or a faulty filter. Drops, gels, capsules and sachets are available to neutralize any odor inside the bag.
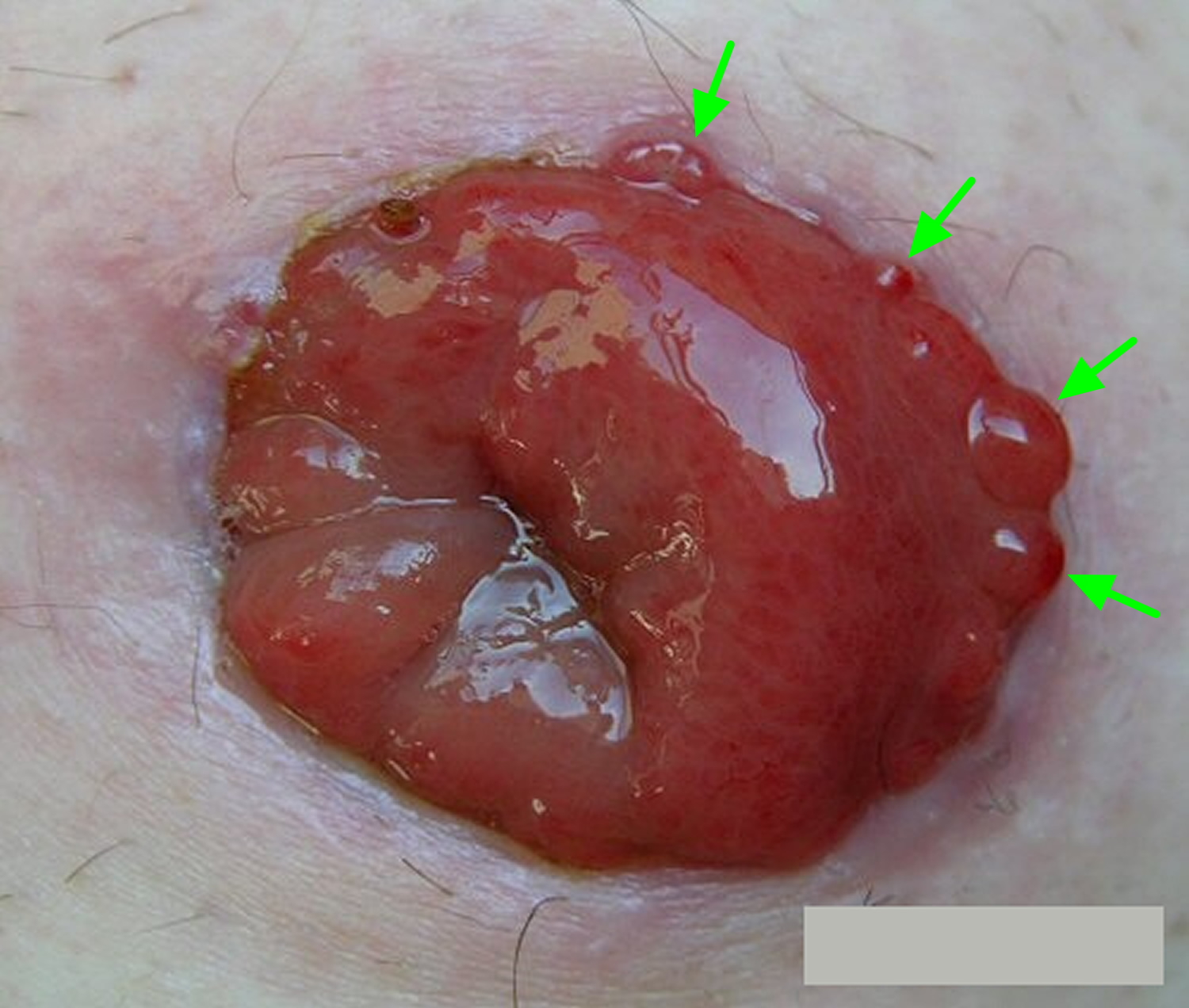
- Granulomas
Granulomas are very common and are small areas of over granulation tissue that appear as fleshy protuberances like tiny beads of varying sizes. Granulomas occur on the surface of the stoma or more commonly at the muco–cutaneous junction (the join between the bowel and the skin).
Granulomas develop as a result of over-healing of damaged skin or the stoma surface, possibly due to friction from the bag. Granulomas can be due to inflammation, infection or fecal irritation from the stomal output. Irritation from the ostomy appliance can also be a common cause. Some, but not all, stoma granulomas can cause bleeding and discomfort when touched when the skin around the stoma is being cleaned. This bleeding can cause problems with adherence of the ileostomy bag. Also, if they are large they may prevent pouch adhesion which may result in leakage problems.
What can you do to prevent stoma granulomas?
Ensure that the hole in the flange/baseplate of your pouch is the right size, so that the edge does not rub against the stoma. Good ileostomy bag changing techniques are an important part of reducing the risk of granuloma formation:
- Remove the used ileostomy appliance slowly and gently. Start at the top and support the skin as you go. Use adhesive remover spray/wipes to reduce damage to the skin.
- Wipe away any feces with toilet paper then wash the stoma and surrounding skin with warm water and dry the area thoroughly using dry wipes or kitchen
roll. - When fitting a new appliance, bend the top half away from the body so that you can see to fit the bottom half accurately around the stoma, then press the remainder of the flange into position.
Some people, however, appear to be more susceptible to the formation of granulomas than others.
Figure 5. Stoma granulomas
Available treatment
Your stoma care nurse will take you through the treatment available, the main option being 75% silver nitrate applied to the granulomas approximately two to three times a week. This needs to be done by a healthcare professional, either the stoma consultants, stoma care nurse or your doctor. A stoma Orabase paste can be applied to prevent friction on the stoma surface and a lubricating gel placed in the pouch can help prevent the pouch rubbing on the stoma surface. Other treatment options include the application of Haelan Tape or application of liquid nitrogen.
If you think you may have stoma granulomas, then please contact your stoma care nurse for a review. Some specially trained stoma care nurses and consultants may also use curette and cautery (a special instrument is used to cut out the granuloma and the wound is cauterised or burnt closed).
Will granulomas eventually go away without treatment?
Usually some form of treatment is required, even if it is only the application of Orabase Paste when the granuloma is very small. The earlier the treatment is started the better.
Are granulomas likely to re–occur?
Yes, some people do find that granulomas can re–occur and they should seek a stoma care nurse review as soon as they feel they have re–appeared.
Prolapsed stoma
A prolapse of the stoma occurs when the bowel protrudes through the stomal opening in the skin to a greater extent than was anticipated. The amount of protruding bowel can vary from 2-3cm to more than 10cm. Although when this first happens it can be very distressing and frightening it is usually not serious. However, a review by a stoma care nurse is essential.
A prolapse can occur in any stoma type but is more common in loop ileostomy. There are many causes, the most common are:
- An over sized hole made in the abdominal wall at surgery
- Increased abdominal pressure due to tumor, pregnancy, coughing and sneezing
- Excessive exertion e.g., heavy lifting
- Poorly developed abdominal muscular support (infants)
- Obesity
How do I manage a prolapsed stoma?
There are two ways of managing a prolapse:
- Conservative management
Your stoma care nurse will advise on how you should look after the stoma and give you help in reducing the swelling. He/she will also advise you on which specialist pouches are available and also on the use of abdominal support garments.
- Surgical management
If a prolapse is too large to manage conservatively, or if it has become discolored, surgical intervention may be required. This will involve removal of the prolapsed section of the bowel and resiting of the stoma.
If you have a prolapse stoma please contact your local stoma care nurse for advice and support.
Ileostomy bag
Ileostomy bag (also called stoma bags) is where you feces are collected as they leave your body via the stoma. Your stoma care nurse will help you to decide which ileostomy bag is best for you after your operation. Once you get home, you’ll soon start to discover that there are lots of different types of stoma bags. These are designed to meet the different needs of people with stoma have. You should consult your stoma care nurse before changing to a new product. There are also a wide range of accessories available. These include deodorizers, wipes, skin protective wipes, lotions and creams.
Table 1. How to choose the right ileostomy bag
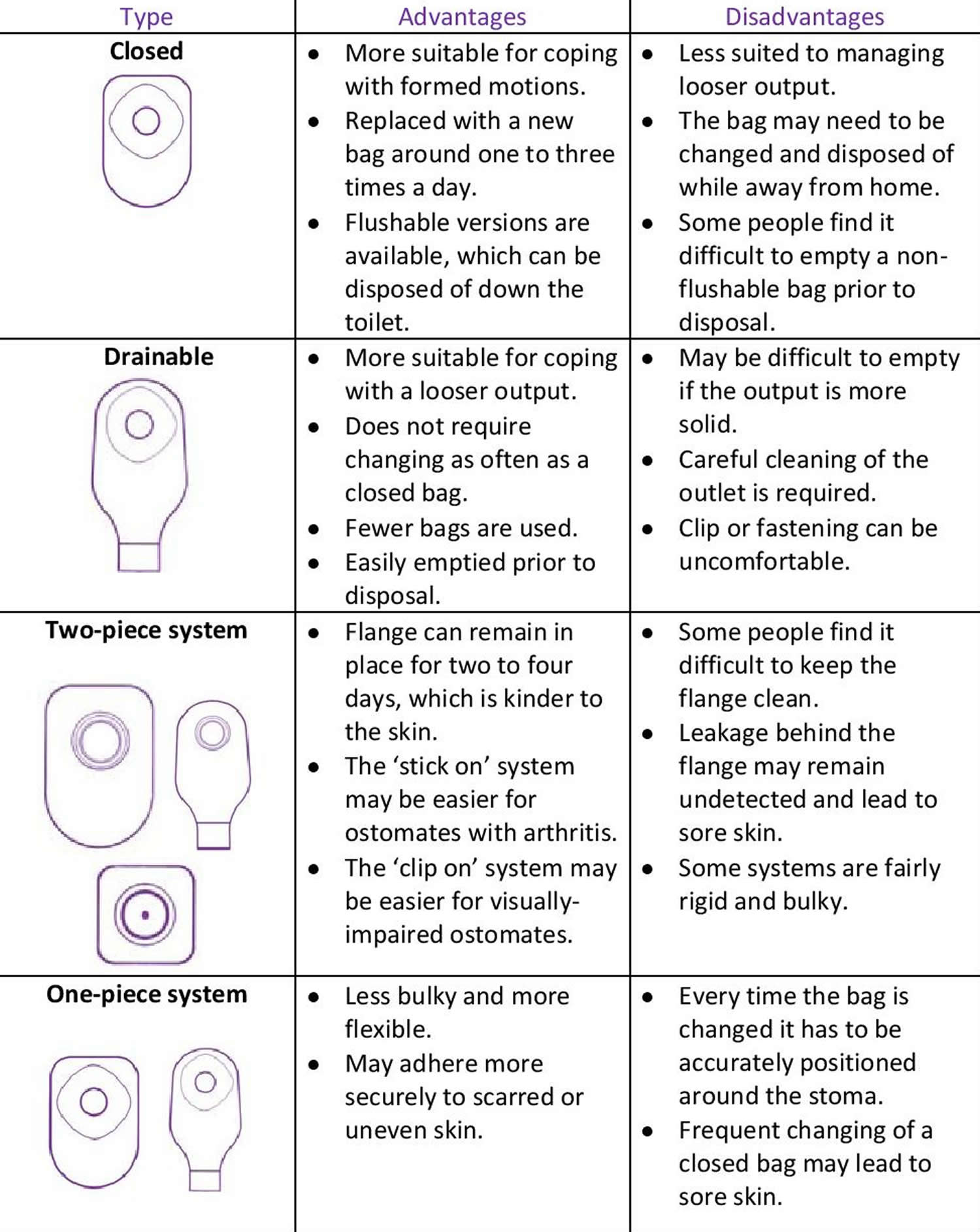
Figure 6. Different types of ileostomy bags
Living with a ileostomy bag
A ileostomy bag is often used to collect your poo (stools). It needs to be removed and replaced when full, usually one to three times a day.
There are also drainable bags that only need to be replaced every one or two days. These may be suitable for people who have particularly loose stools.
A specialist stoma nurse, who usually sees you before and after the ileostomy operation, will help you choose the most suitable ileostomy equipment.
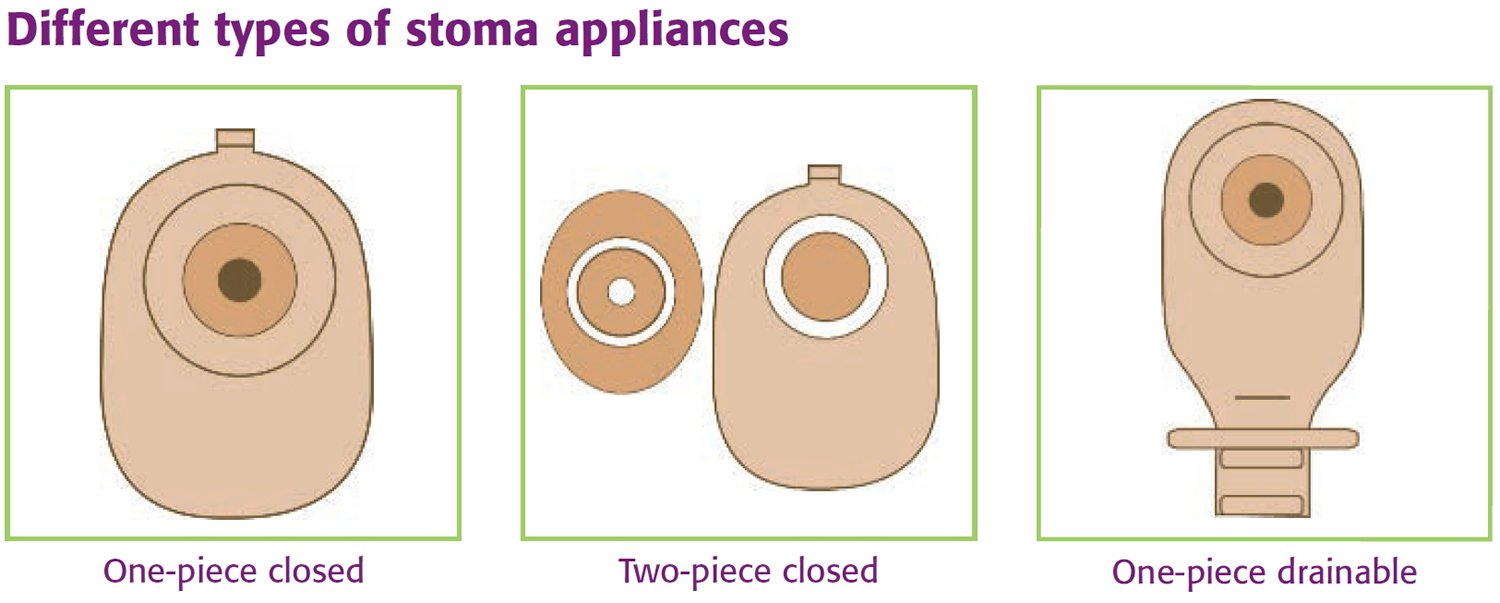
There’s a wide range of ileostomy appliances available, including:
- One-piece ileostomy bag – the bag and flange (part that sticks to your skin) are joined together; the appliance is removed when full and then disposed of
- Two-piece ileostomy bag – the bag and flange are separate, but can be connected; the flange can be left on your skin for several days, and the bag removed and disposed of several times a day
- Closed ileostomy bags which are mainly used for coping with formed motions. They are usually changed several times a day. Closed bags with a special liner which contains the motions and can be flushed down the toilet are available.
- Drainable ileostomy bags which are mainly used for coping with liquid motions. They may be worn for longer than closed bags as they can be emptied through an outlet at the bottom and then resealed with an integral Velcro seal or a clip.
Ileostomy appliances are made from non-allergic (hypoallergenic) materials to reduce skin irritation. They also contain special filters to prevent any unpleasant odors.
If you have regular and predictable bowel patterns, you may not always need to wear a ileostomy bag. But as occasional leakages can happen, it’s recommended that you wear a small stoma cap.
Additional products that can make living with a ileostomy more convenient include:
- support belts and girdles
- deodorizers that can be inserted into your appliance
- protective skin wipes
- sprays to remove adhesive
- protective stoma rings
- specially designed underwear and swimwear
Your stoma care nurse will be able to give you more information and advice about equipment.
How to change a ileostomy bag
Before you leave hospital your stoma care nurse will show you how to change your bag. She/he will also teach you how to use a stoma guide to check that the hole in the adhesive flange or base-plate is the correct size. If necessary, you will also be shown how to cut the right size and shape using a template.
A ileostomy bag is best changed when about three-quarters full. This makes the process easier and the ileostomate (a person with ileostomy) more comfortable. It is usually carried out in the bathroom, but if the ileostomate is seated, this can mean folds or creases form around the stoma making it difficult to achieve a good seal between the skin and the flange/base-plate. It may be best to remove the used ileostomy bag and attach the new one when the ileostomate is standing. However, if this is not possible then an alternative might be for the ileostomate to lay flat on a bed.
1. Before you begin
Check you have everything you need: water, soft wipes, a new ileostomy bag, any accessories you use and a plastic disposal bag.
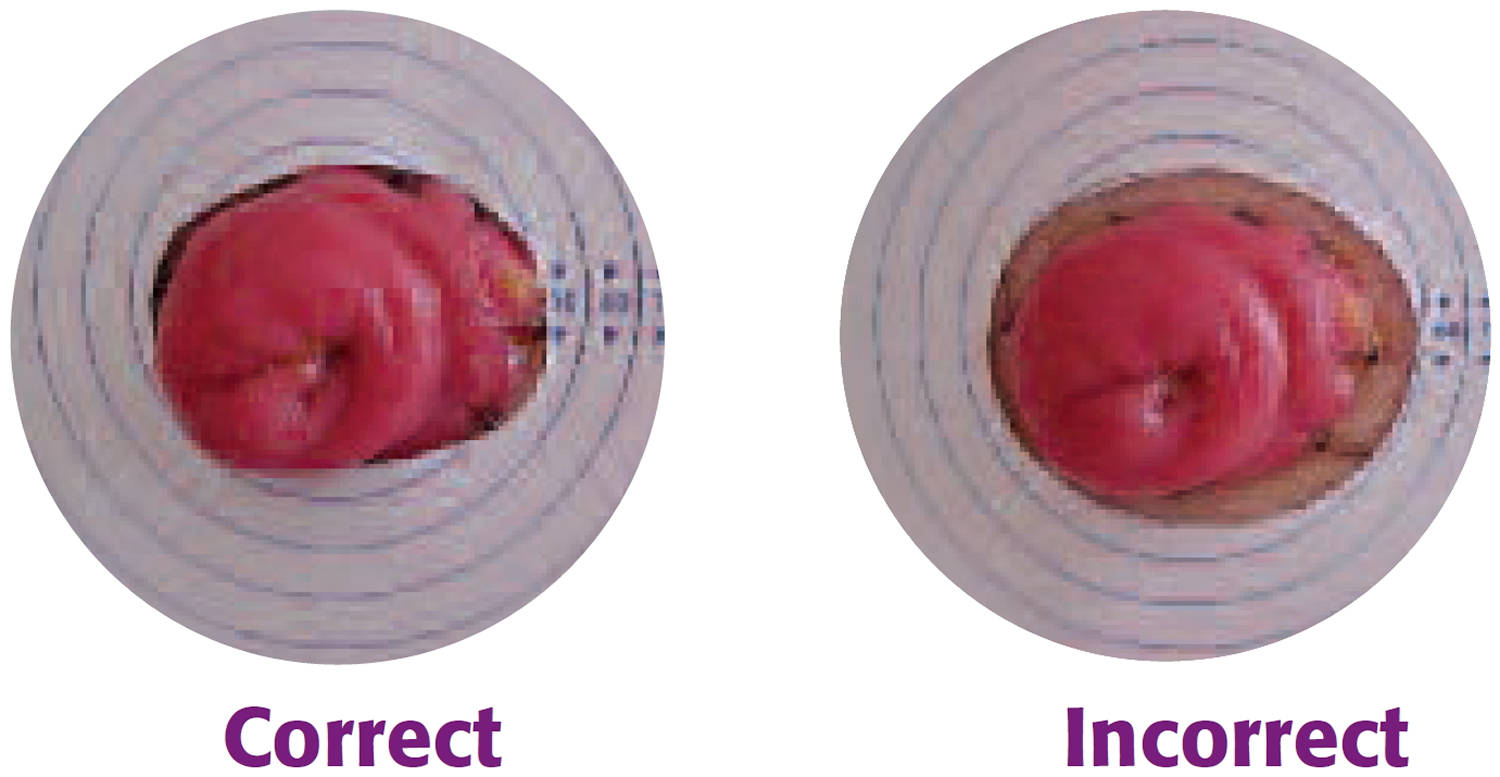
Check whether the hole in the adhesive flange/base-plate has been pre-cut to the size and shape of the stoma. If not, use a template to mark the outline of the stoma and using curved scissors, trim to the correct shape. If the hole is too large skin will show and be irritated by the contents of the bag, which can make it sore. If the hole is too small, it may rub against the stoma and cause it to swell.
Tips:
If you wear a one–piece pouch use the backing paper/film that protects the adhesive on the flange to check that the hole is the correct size. Hold the backing film around your stoma; it can be difficult to see if you are looking down so it may be helpful to stand in front of a mirror or ask someone else to check for you.
There should be a 1–2mm gap all around to prevent the edges of the hole rubbing on the stoma, whilst still ensuring that the contents of the pouch do not come into contact with the skin.
Figure 6. Measuring and cutting a hole in the base-plate of the ileostomy bag
2. Removing the old ileostomy bag
Remove the old bag, working slowly and gently from the top to the bottom of the flange. medical adhesive remover (available on prescription) can be used to avoid damaging the skin. It is wiped or sprayed beneath the flange as it is peeled away from the skin.
Check the skin around the stoma for any early signs of irritation. Gently clean the stoma and surrounding skin with warm water. Do not use soaps, disinfectants, harsh solvents or baby wipes as these often contain perfume or moisturizers and may affect how the flange/base-plate sticks, or may irritate the skin.
Remember the stoma bleeds easily if it is rubbed too hard, but bleeding should stop quickly. If blood comes from inside the stoma, contact your stoma care nurse.
3. Fitting the new ileostomy bag
Gently pat the skin until it is completely dry. If you are prone to sore skin, barrier wipes, sprays and lotions are available.
When your skin is completely dry, fit the new ileostomy bag (or base plate), making sure it is secure all the way round. When fitting a one-piece ileostomy bag, it helps to bend the top half of the flange away from your body, so that you can see to fit the bottom half around the stoma. Then, with the flat of your hand, press the remainder of the flange in position. The warmth of your hand will ensure that it adheres snugly. Press the flange/base-plate in place for at least half a minute to make sure the seal is secure.
If using a two-piece ileostomy bag, then attach the bag to the base-plate.
4. Disposal of used ileostomy appliances
Seal the used appliance inside a disposal bag (provided free by suppliers). In a nursing home this can be disposed of with other clinical waste.
The used ileostomy appliance may be wrapped up well and put in the dustbin. Some people prefer to empty the contents of the stoma bag into the toilet before discarding it in this way.
Ileostomy bags with liners that contain the stools and can be flushed down the toilet are now available.
Ileostomy diet
In the first few weeks after your ileostomy surgery, you’ll usually be advised to follow a low-fiber diet.
This is because having a high-fiber diet can increase the size of your stools, which can cause the bowel to become temporarily blocked. After around eight weeks, you’ll usually be able to resume a normal diet.
As you recover, you should try to eat a healthy, balanced diet that includes plenty of fresh fruit and vegetables – at least five portions a day – and wholegrains.
If you decide to introduce new foods into your diet after surgery, try to introduce them slowly, at the rate of one type of food each meal. This will allow you to judge the effects of the food on your digestive system.
You may find it useful to keep a food diary so you can keep a record of the food you’ve eaten and how you feel afterwards. For example, you may find you experience diarrhea after eating spicy foods, or after drinking alcohol or caffeinated drinks.
Dehydration
If you no longer have a large intestine (colon), you’re at greater risk from dehydration. This is because one of the functions of the colon is to reabsorb water and minerals back into the body.
It’s therefore important to drink plenty of water if you have an ileostomy, particularly in hot weather or during periods where you’re more active than normal. Sachets of fluid replacement solutions to help reduce dehydration are also available from pharmacies.
Living with an ileostomy
Although it can be difficult to adjust at first, having an ileostomy doesn’t mean you can’t have a full and active life.
Many people with a stoma say their quality of life has improved since having an ileostomy because they no longer have to cope with distressing and uncomfortable symptoms.
However, if you’re finding it difficult to adjust after your operation, it may help to get in contact with others who have had similar experiences through support groups.
Ileostomy equipment
Before and after the ileostomy procedure, you’ll see a nurse who specialises in helping people with a stoma. The nurse will advise you about equipment you’ll need and how to manage your stoma.
Stoma bags
Your stoma will produce liquid digestive waste that can range from a watery consistency to a consistency similar to porridge, which is collected in a stoma bag.
There’s a wide range of stoma bags available, but a specialist stoma nurse can help you choose the most suitable appliance for you.
To help reduce skin irritation, stoma bags are made from hypoallergenic (non-allergic) material, and contain special filters to help ensure the bags don’t release any unpleasant odors.
They can be easily drained through an opening in the bottom and can be concealed under everyday clothes.
It’s usually best to empty your bag into a toilet when it’s about one-third full as this prevents the bag bulging underneath your clothes.
You’ll usually be advised to replace the bags and dispose of them in the general rubbish – not down the toilet – every one or two days.
At first, living with an ileostomy can be a distressing experience. It may take some time before you get used to it, but with practise and the support of your stoma nurse and family, using stoma bags will become routine.
Other equipment and products
There are also additional products that can make living with an ileostomy more convenient, including:
- support belts and girdles
- deodorizers that can be inserted into your appliance
- protective skin wipes
- adhesive remover sprays
- protective stoma guards
Your stoma care nurse will be able to advise you about the most appropriate equipment to help you manage your ileostomy successfully.
Ordering and paying for equipment
You’ll be given an initial supply of stoma bags before you leave hospital, as well as your prescription information. Let your doctor know your prescription information so they can make a note of it in your medical records and issue prescriptions in the future.
Your prescription can either be taken to the chemist or sent to a specialist supplier who will deliver the appliances. There’s no need to stockpile supplies, but it’s recommended that you order more appliances while you still have plenty left so you don’t run out.
Smell and wind
In the first few weeks after surgery, you may experience a lot of gas (flatulence). This is harmless, but it can be embarrassing and uncomfortable. This problem should subside as your bowels recover from the effects of surgery.
Chewing food thoroughly and not eating foods that cause gas can help. These include:
- beans
- broccoli
- cabbage
- cauliflower
- onions
- eggs
Fizzy drinks and beer also cause gas. Don’t skip meals to try to prevent gas because it will make the problem worse.
If the problem persists, your doctor or stoma nurse should be able to recommend a medicine that can help to reduce gas.
Many people also worry their external bag will smell. However, all modern appliances have air filters with charcoal in them, which neutralises the smell. If necessary, special liquids and tablets that are placed in the bags are available to reduce any odour.
Medication
Many medicines are designed to dissolve slowly in your digestive system. This means some medications may not be as effective if you have an ileostomy because they could come straight out into your bag.
Let your doctor or pharmacist know about your stoma so they can recommend an alternative type of medicine, such as an uncoated pill, powder or liquid.
In women, having a ileostomy can affect the effectiveness of oral contraceptive pills, so you may want to discuss alternative forms of contraception with your doctor or pharmacist.
Physical activities
Once you’ve fully recovered from surgery, there’s no reason you can’t return to most of your normal activities, including work, sports, traveling and having sex.
Speak to your stoma nurse before returning to your normal activities, however, as they can offer advice about issues you may need to take into consideration now you have an ileostomy.
For example, they can advise you about wearing protective stoma guards while playing sports, or stocking up on ileostomy products before traveling.
Living with an Continent Ileostomy (ileo-anal) pouch
Living with an ileo-anal pouch is different from living with an ileostomy because the procedure doesn’t involve creating a stoma in the tummy (abdomen). Instead, digestive waste is stored in an internal pouch and excreted through the rectum and anus.
If you’ve had an ileo-anal pouch (J-pouch), you may find you need to empty it up to 20 times a day during the first few days after the operation.
However, the number of times you need to go to the toilet will slowly reduce as the pouch expands and you get used to controlling muscles that surround it.
Most people find their pouch activity settles down after 6 to 12 months, although the number of bowel movements will differ from person to person.
Improving muscle control
Exercising the muscles that control the passing of stools (pelvic floor muscles) can help make going to the toilet easier if you have an ileo-anal pouch. It can also reduce the likelihood of accidental leaks during the first few weeks after the operation.
Pelvic floor exercises, as outlined below, are a good way of improving your muscle control:
- sit or lie comfortably with your knees slightly apart
- without moving your abdominal muscles, squeeze the muscle around the back passage as if you’re trying to stop passing wind
- hold this contraction as long as you can – at least two seconds, increasing up to 10 seconds as you improve
- relax for the same amount of time before repeating
Ideally aim for 10 short, fast and strong contractions.
Anal soreness
Anal soreness or itchiness is common in people with an ileo-anal pouch. Having regular baths should help to relieve this. Using a skin protection cream is also recommended. Your doctor will be able to advise you about the best cream for you.
Ileostomy reversal
If your ileostomy is intended to be temporary, further surgery will be needed to reverse it at a later date.
The reversal operation will only be carried out when you’re in good health and fully recovered from the effects of the original ileostomy operation. This will usually be several weeks or months after the initial surgery, or sometimes even longer.
There’s no time limit for having an ileostomy reversed and some people may live with one for several years before it’s reversed.
Reversing a loop ileostomy is a relatively straightforward procedure that’s carried out under general anaesthetic.
A cut (incision) is made around the stoma and the section of small intestine is pulled out of the tummy (abdomen). The area that had been divided to form the stoma is then stitched back together and placed back inside the abdomen.
It’s also sometimes possible to reverse an end ileostomy if most of the large intestine (colon) has been sealed and left inside the abdomen.
However, the surgeon will need to make a larger incision to locate and reattach the small and large intestines. It therefore takes longer to recover from this type of surgery and there’s a greater risk of complications.
Recovering from ileostomy reversal surgery
Most people are well enough to leave hospital within three to five days of having ileostomy reversal surgery.
While you recover, you may have diarrhea and need to go to the toilet more often than normal.
It can take a few weeks for these problems to settle and your bowel activity may never return to the way it was before you had the ileostomy operation.
If necessary, your doctor can prescribe medication to relieve diarrhea until things improve.
You may also experience a sore anus after the reversal operation. This should improve as the anus becomes used to having stools pass through it again, although common barrier creams can help.
The reversal operation is usually a smaller procedure than the initial ileostomy procedure. However, it still takes several weeks to fully recover.





{kind=link}