
Contents
Joints in the body
Any point where two bones meet is called a joint (articulation), whether or not the bones are mobile at that interface. Joints, or articulations, link the bones of the skeletal system into a functional whole—a system that supports the body, permits effective movement, and protects the softer organs. Joints such as the shoulder, elbow, and knee are remarkable specimens of biological design—self-lubricating, almost frictionless, and able to bear heavy loads and withstand compression while executing smooth and precise movements. Yet it is equally important that other joints be less movable or even immobile. Such joints are better able to support the body and protect delicate organs. The vertebral column, for example, is only moderately mobile, for it must allow for flexibility of the torso and yet protect the delicate spinal cord and support much of the body’s weight. Bones of the cranium must protect the brain and sense organs, but need not allow for movement (except during birth); thus, they are locked together by immobile joints.
The science of joint structure, function, and dysfunction is called arthrology. The study of musculoskeletal movement is kinesiology. This is a branch of biomechanics, which deals with a broad variety of movements and mechanical processes in the body, including the physics of blood circulation, respiration, and hearing.
The name of a joint is typically derived from the names of the bones involved. For example, the atlanto–occipital joint is where the atlas meets the occipital condyles; the glenohumeral joint is where the glenoid cavity of the scapula meets the humerus; and the radioulnar joint is where the radius meets the ulna.
Joints can be classified according to the manner in which the adjacent bones are bound to each other, with corresponding differences in how freely the bones can move. Authorities differ in their classification schemes, but one common view places the joints in four major categories: bony, fibrous, cartilaginous, and synovial
joints.
Bony Joints
A bony joint, or synostosis, is an immobile joint formed when the gap between two bones ossifies and they become, in effect, a single bone. Bony joints can form by ossification of either fibrous or cartilaginous joints. An infant is born with right and left frontal and mandibular bones, for example, but these soon fuse seamlessly into a single frontal bone and mandible. In old age, some cranial sutures become obliterated by ossification and the adjacent cranial bones, such as the parietal bones, fuse. The epiphyses and diaphyses of the long bones are joined by cartilaginous joints in childhood and adolescence, and these become bony joints in early adulthood. The attachment of the first rib to the sternum also becomes a bony joint with age.
Fibrous Joints
A fibrous joint is also called a synarthrosis. It is a point at which adjacent bones are bound by collagen fibers that emerge from one bone, cross the space between them, and penetrate into the other. There are three kinds of fibrous joints: sutures, gomphoses, and syndesmoses. In sutures and gomphoses, the fibers are very short and allow for little or no movement. In syndesmoses, the fibers are longer and the attached bones are more mobile.
Figure 1. Fibrous joints
Note: (a) A suture between the parietal bones. (b) A gomphosis between a tooth and the jaw. (c) A syndesmosis between the tibia and fibula.
Sutures
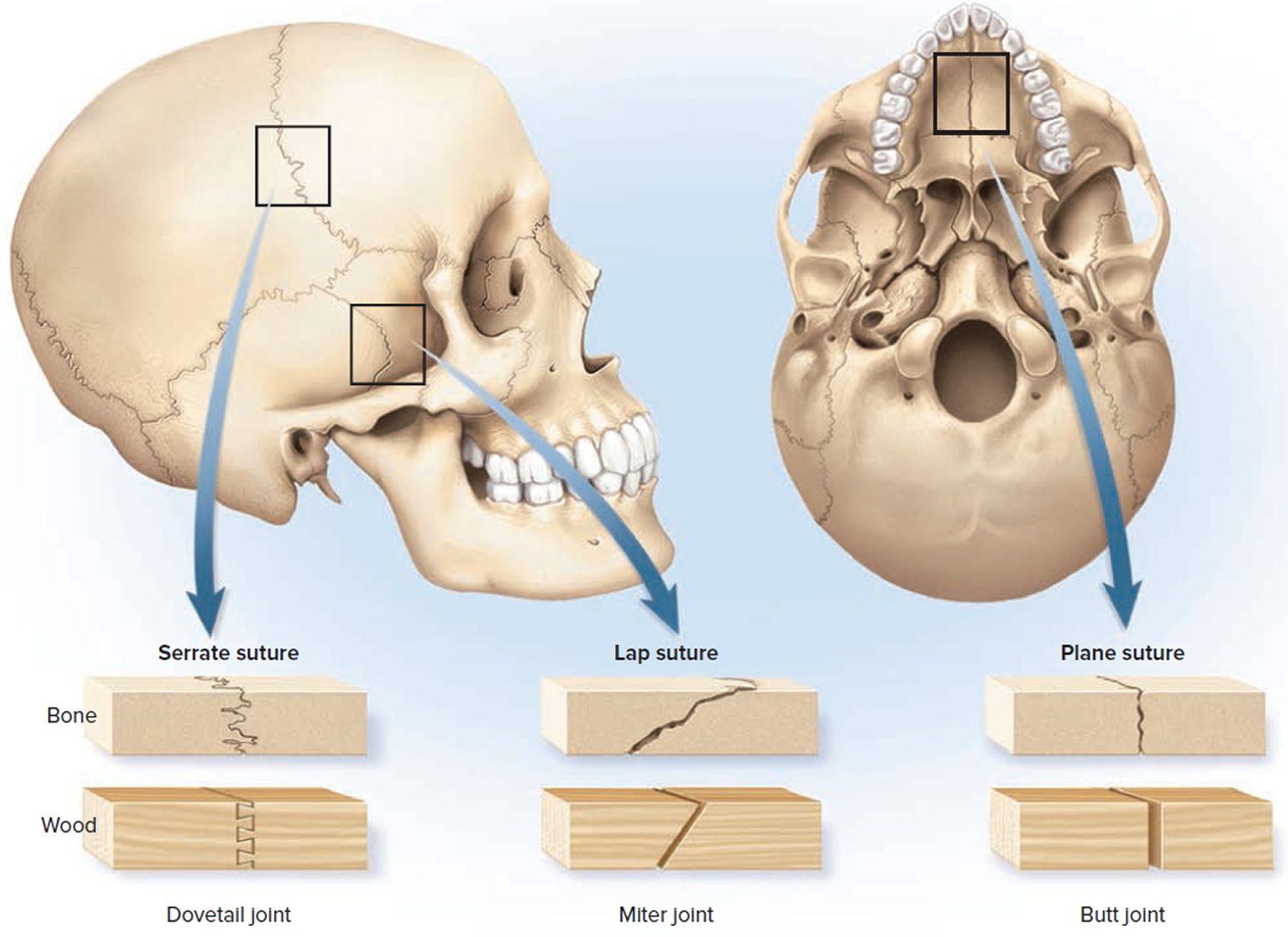
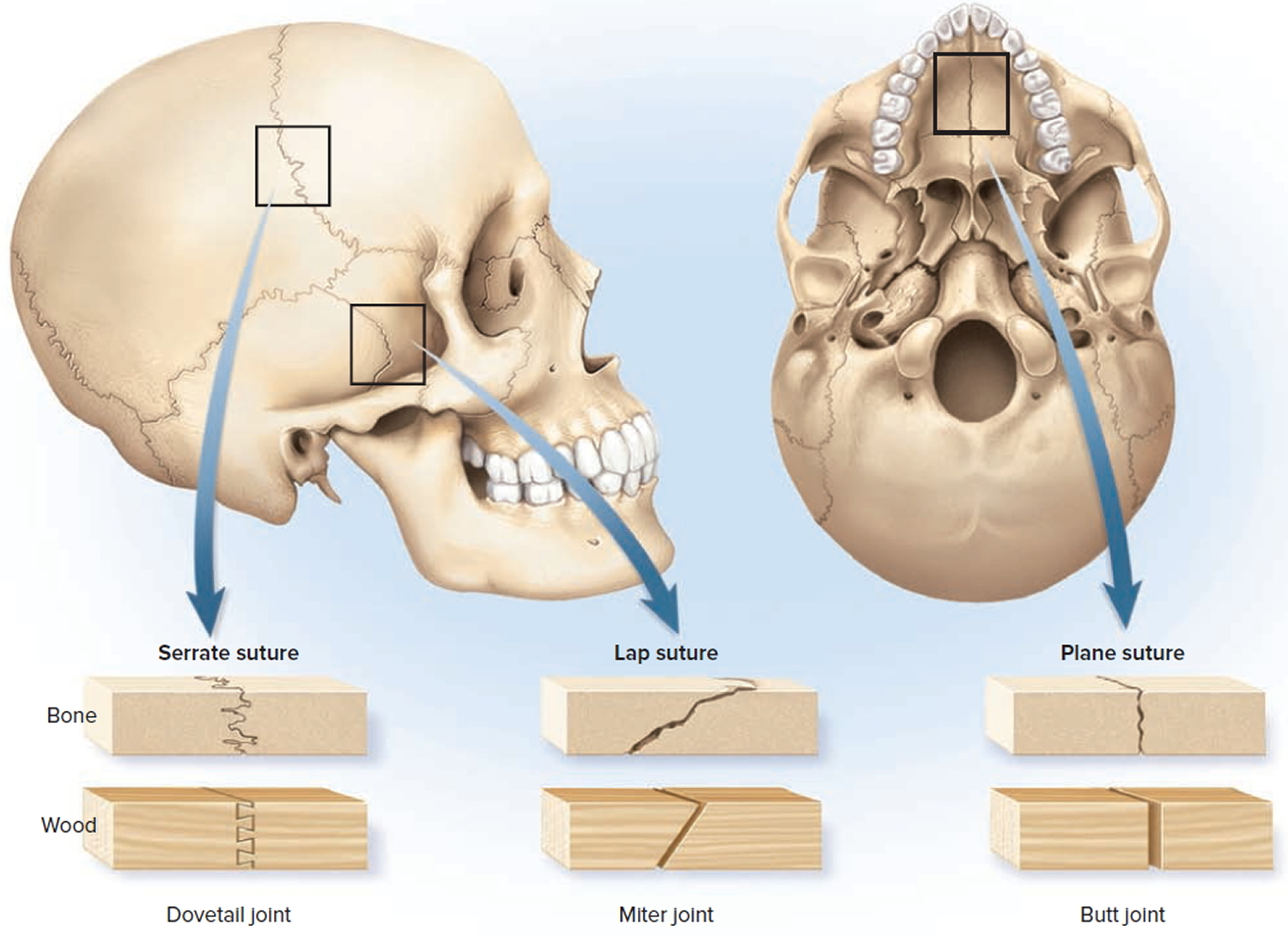
Sutures are immobile or only slightly mobile fibrous joints that closely bind the bones of the skull to each other; they occur nowhere else. Sutures can be classified as serrate, lap, and plane sutures. Readers with some knowledge of woodworking may recognize that the structures and functional properties of these sutures have something in common with basic types of carpentry joints.
Serrate sutures appear as wavy lines along which the adjoining bones firmly interlock with each other by their serrated margins, like pieces of a jigsaw puzzle. Serrate sutures are analogous to a dovetail wood joint. Examples include the coronal, sagittal, and lambdoid sutures that border the parietal bones.
Lap (squamous) sutures occur where two bones have overlapping beveled edges, like a miter joint in carpentry. On the surface, a lap suture appears as a relatively smooth (nonserrated) line. An example is the squamous suture where the temporal bone meets the sphenoid and parietal bones. The beveled edge of the temporal bone.
Plane (butt) sutures occur where two bones have straight nonoverlapping edges. The two bones merely border on each other, like two boards glued together in a butt joint. This type of joint is represented by the intermaxillary suture in the roof of the mouth.
Figure 2. Sutures joint
Gomphoses
Even though the teeth are not bones, the attachment of a tooth to its socket is classified as a joint called a gomphosis. The term refers to its similarity to a nail hammered into wood. The tooth is held firmly in place by a fibrous periodontal ligament, which consists of collagen fibers that extend from the bone matrix of the jaw into the dental tissue. The periodontal ligament allows the tooth to move or give a little under the stress of chewing. Along with associated nerve endings, this slight tooth movement allows you to sense how hard you are biting and to sense a particle of food stuck between the teeth.
Syndesmoses
A syndesmosis is a fibrous joint at which two bones are bound by relatively long collagenous fibers. The separation between the bones and length of the fibers give these joints more mobility than a suture or gomphosis has. An especially mobile syndesmosis exists between the shafts of the radius and ulna, which are joined by a broad fibrous interosseous membrane. This permits such movements as pronation and supination of the forearm. A less mobile syndesmosis is the one that binds the distal ends of the tibia and fibula together, side by side.
Cartilaginous Joints
A cartilaginous joint is also called an amphiarthrosis. In these joints, two bones are linked by cartilage. The two types of cartilaginous joints are synchondroses and symphyses.
Figure 3. Cartilaginous joints
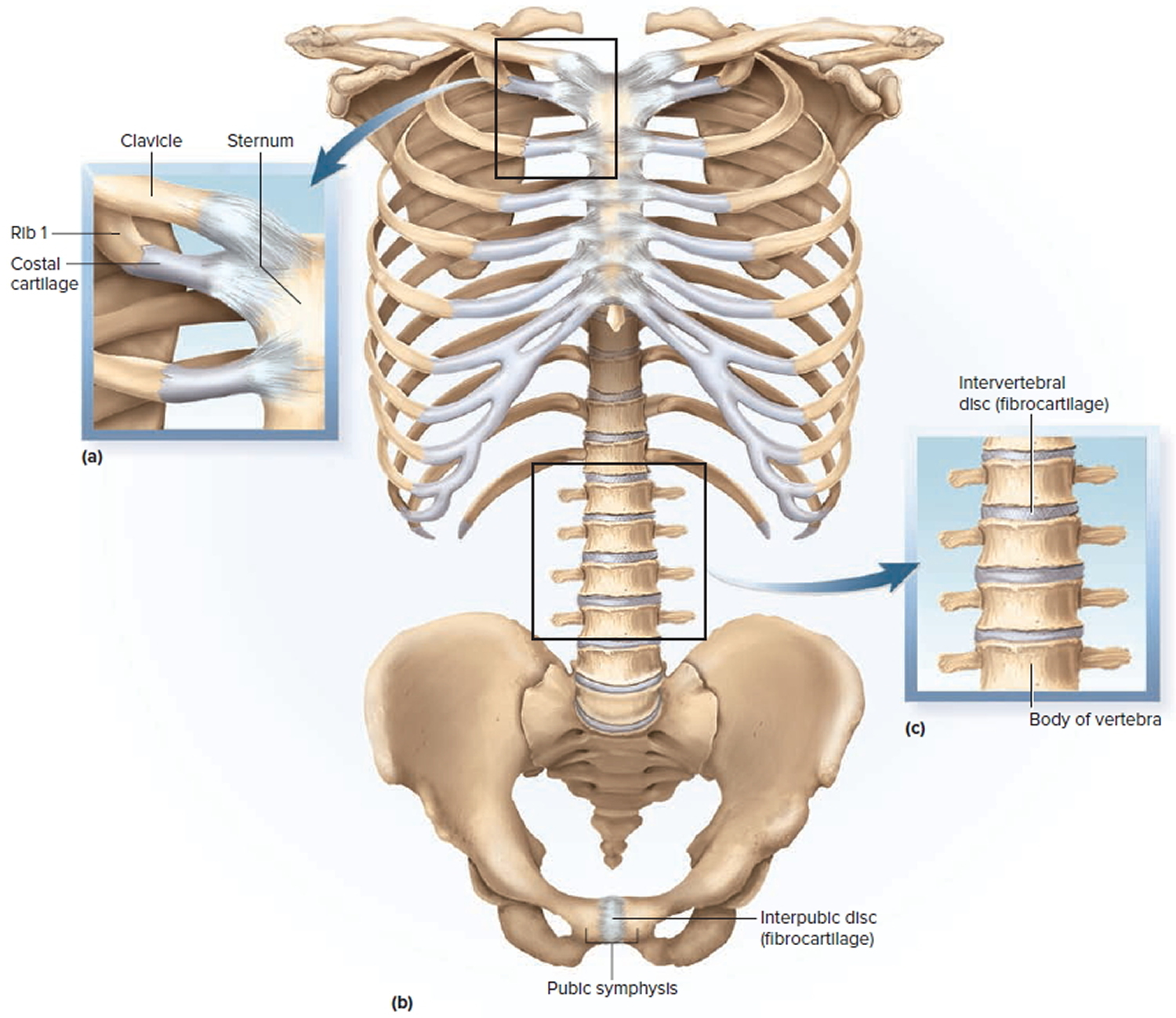
Note: a) A synchondrosis, represented by the costal cartilage joining rib 1 to the sternum. (b) The pubic symphysis. (c) Intervertebral discs, which join adjacent vertebrae to each other by symphyses.
Synchondroses
A synchondrosis is a joint in which the bones are bound by hyaline cartilage. An example is the temporary joint between the epiphysis and diaphysis of a long bone in a child, formed by the cartilage of the epiphyseal plate. Another is the attachment of the first rib to the sternum by a hyaline costal cartilage. The other costal cartilages are joined to the sternum by synovial joints.
Symphyses
In a symphysis, two bones are joined by fibrocartilage. One example is the pubic symphysis, in which the right and left pubic bones are joined anteriorly by the cartilaginous interpubic disc. Another is the joint between the bodies of two vertebrae, united by an intervertebral disc. The surface of each vertebral body is covered with hyaline cartilage. Between the vertebrae, this cartilage becomes infiltrated with collagen bundles to form fibrocartilage. Each intervertebral disc permits only slight movement between adjacent vertebrae, but the collective effect of all 23 discs gives the spine considerable flexibility.
Synovial Joints
The most familiar type of joint is the synovial joint, also called a diarthrosis. Ask most people to point out any joint in the body, and they are likely to point to a synovial joint such as an elbow, knee, or knuckle. Many synovial joints, like these examples, are freely mobile. Others, such as the joints between the wrist and ankle bones and between the articular processes of the vertebrae, have more limited mobility.
Synovial joints are the most structurally complex type of joint and are the type most likely to develop uncomfortable and crippling dysfunctions. They are the most important joints for such professionals as physical and occupational therapists, athletic coaches, nurses, and fitness trainers to understand well. Their mobility makes the synovial joints especially important to the quality of life. Reflect, for example, on the performance extremes of a young athlete, the decline in flexibility that comes with age, and the crippling effect of rheumatoid arthritis.
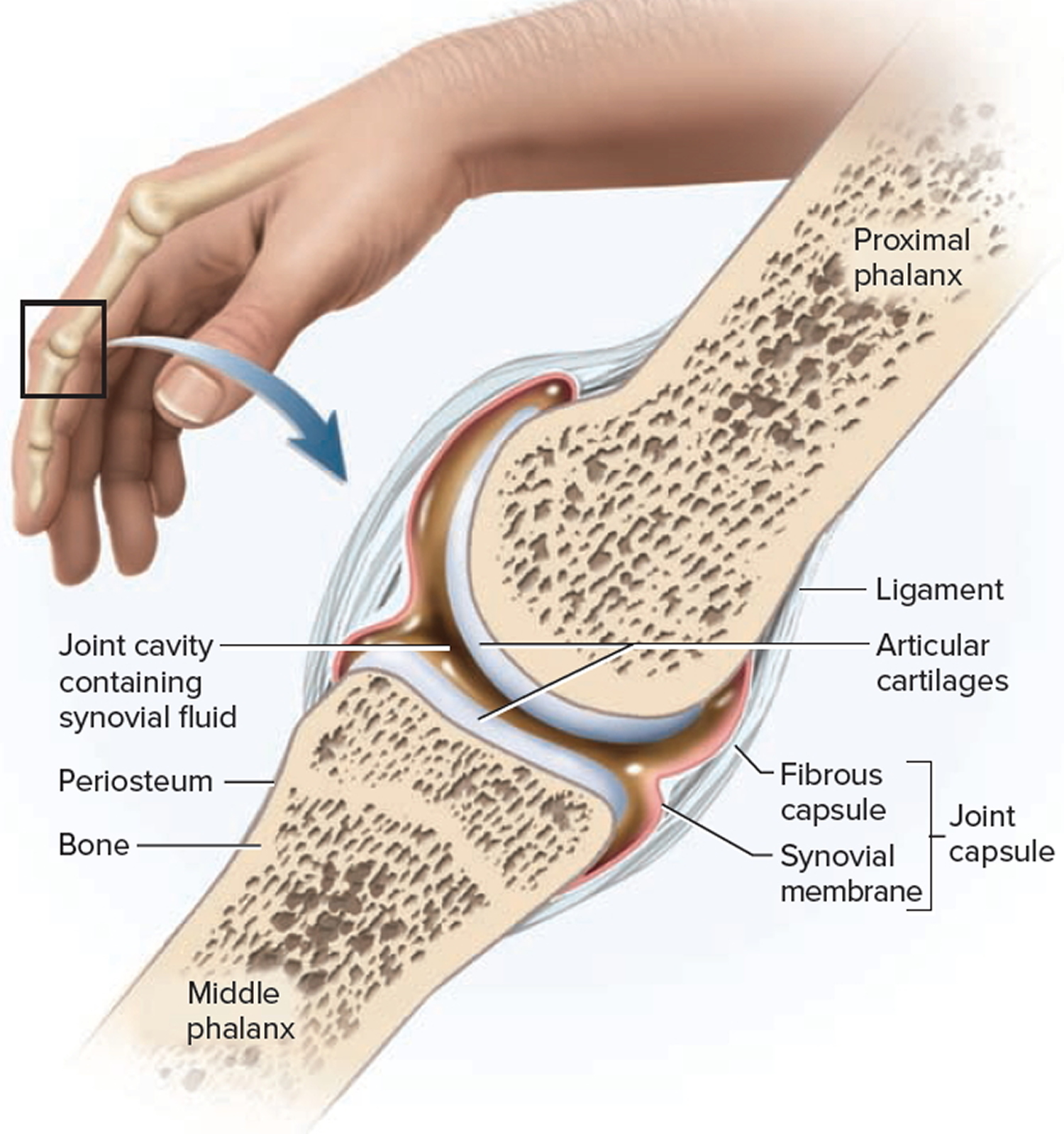
In synovial joints, the facing surfaces of the two bones are covered with articular cartilage, a layer of hyaline cartilage up to 2 or 3 mm thick. These surfaces are separated by a narrow space, the joint (articular) cavity, containing a slippery lubricant called synovial fluid. This fluid, for which the joint is named, is rich in albumin and hyaluronic acid, which give it a viscous, slippery texture similar to raw egg white. It nourishes the articular cartilages, removes their wastes, and makes movements at synovial joints almost friction-free. A connective tissue joint (articular) capsule encloses the cavity and retains the fluid. It has an outer fibrous capsule continuous with the periosteum of the adjoining bones, and an inner, cellular synovial membrane.
The synovial membrane is composed mainly of fibroblast-like cells that secrete the fluid, and is populated by macrophages that remove debris from the joint cavity. Joint capsules and ligaments are well supplied with lamellar corpuscles and other sensory nerve endings that enable the brain to monitor limb positions and joint movements.
In a few synovial joints, fibrocartilage grows inward from the joint capsule and forms a pad between the articulating bones. In the jaw (temporomandibular) joint, at both ends of the clavicle (sternoclavicular and acromioclavicular joints), and between the ulna and carpal bones, the pad crosses the entire joint capsule and is called an articular disc. In the knee, two cartilages extend inward from the left and right but do not entirely cross the joint. Each is called a meniscus because of its crescent-moon shape. These cartilages absorb shock and pressure, guide the bones across each other, improve the fit between the bones, and stabilize the joint, reducing the chance of dislocation.
Accessory structures associated with a synovial joint include tendons, ligaments, and bursae. A tendon is a strip or sheet of tough collagenous connective tissue that attaches a muscle to a bone. Tendons are often the most important structures in stabilizing a joint. A ligament is a similar tissue that attaches one bone to another.
A bursa is a fibrous sac of synovial fluid located between adjacent muscles, where a tendon passes over a bone, or between bone and skin. Bursae cushion muscles, help tendons slide more easily over the joints, and sometimes enhance the mechanical effect of a muscle by modifying the direction in which its tendon pulls. Tendon (synovial) sheaths are elongated cylindrical bursae wrapped around a tendon, seen especially in the hand and foot. They enable tendons to move back and forth more freely in such tight spaces as the wrist and ankle.
Figure 4. Synovial joint
Classes of Synovial Joints
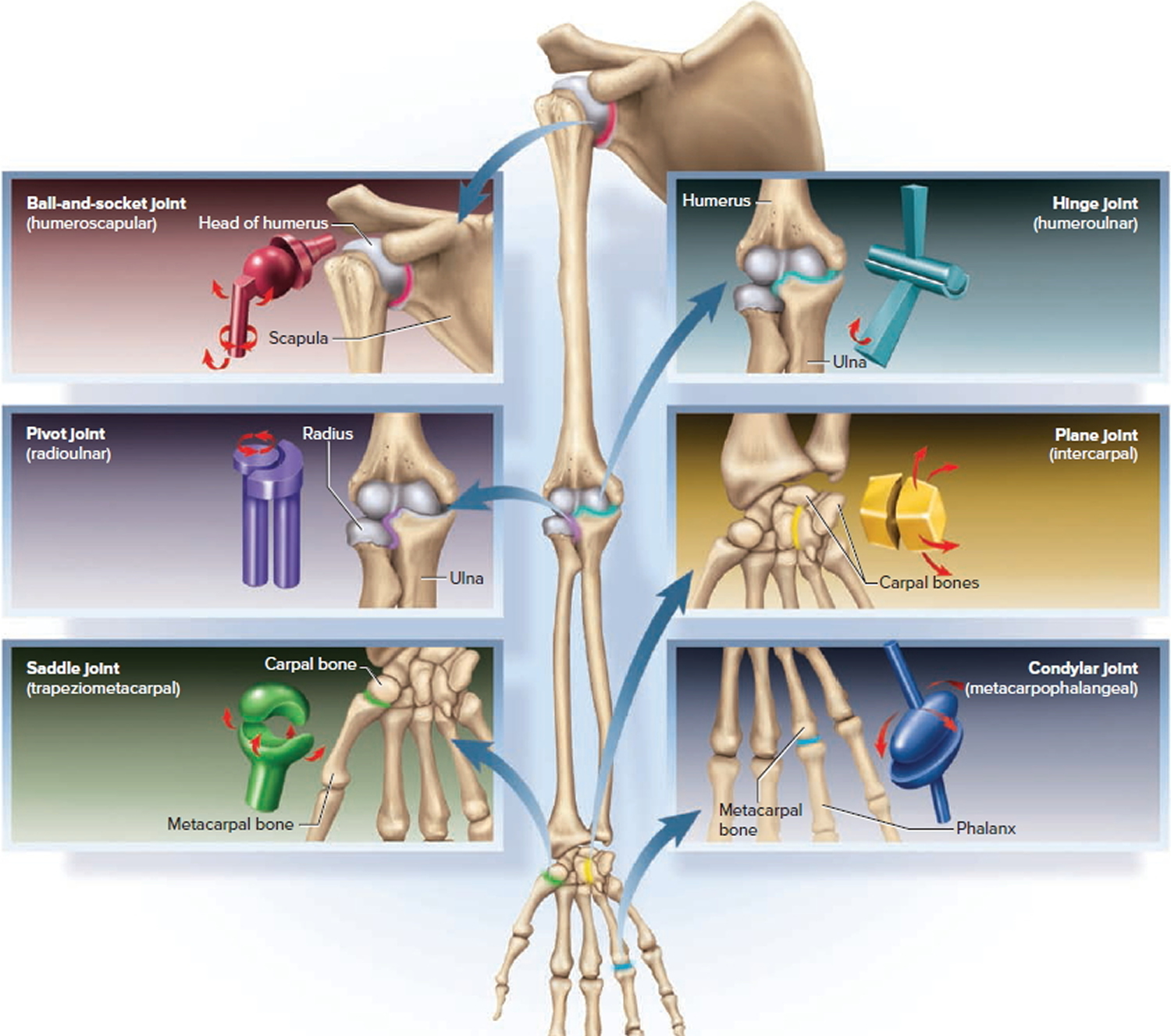
There are six fundamental types of synovial joints, distinguished by the shapes of their articular surfaces and their degrees of freedom. We will begin by looking at these six types in simple terms, but then see that this is an imperfect classification for reasons discussed at the end. All six types can be found in the upper limb. They are listed here in descending order of mobility: one multiaxial type (ball-and-socket), three biaxial types (condylar, saddle, and plane), and two monaxial types (hinge and pivot).
- Ball-and-socket joints. These are the shoulder and hip joints—the only multiaxial joints in the body. In both cases, one bone (the humerus or femur) has a smooth hemispherical head that fits into a cuplike socket on the other (the glenoid cavity of the scapula or the acetabulum of the hip bone).
- Condylar (ellipsoid) joints. These joints exhibit an oval convex surface on one bone that fits into a complementary shaped depression on the other. The radiocarpal joint of the wrist and metacarpophalangeal joints at the bases of the fingers are examples. They are biaxial joints, capable of movement in two planes. To demonstrate this, hold your hand with the palm facing you. Make a fist, and these joints flex in the sagittal plane. Fan your fingers apart, and they move in the frontal plane.
- Saddle joints. Here, both bones have a saddle-shaped surface—concave in one direction (like the front-to-rear curvature of a horse’s saddle) and convex in the other (like the left-to-right curvature of a saddle). The clearest example of this is the trapeziometacarpal joint between the trapezium of the wrist and metacarpal I at the base of the thumb. Saddle joints are biaxial. The thumb, for example, moves in a frontal plane when you spread the fingers apart, and in a sagittal plane when you move it as if to grasp a tool such as a hammer. This range of motion gives us and other primates that invaluable anatomical hallmark, the opposable thumb. Another saddle joint is the sternoclavicular joint, where the clavicle articulates with the sternum. The clavicle moves vertically in the frontal plane at this joint when you lift a suitcase, and moves horizontally in the transverse plane when you reach forward to push open a door.
- Plane (gliding) joints. Here the bone surfaces are flat or only slightly concave and convex. The adjacent bones slide over each other and have relatively limited movement. Plane joints are found between the carpal bones of the wrist, the tarsal bones of the ankle, and the articular processes of the vertebrae. Their movements, although slight, are complex. They are usually biaxial. For example, when the head is tilted forward and back, the articular facets of the vertebrae slide anteriorly and posteriorly; when the head is tilted from side to side, the facets slide laterally. Although any one joint moves only slightly, the combined action of the many joints in the wrist, ankle, and vertebral column allows for a significant amount of overall movement.
- Hinge joints. These are essentially monaxial joints, moving freely in one plane with very little movement in any other, like a door hinge. Some examples are the elbow, knee, and interphalangeal (finger and toe) joints. In these cases, one bone has a convex (but not hemispherical) surface, such as the trochlea of the humerus and the condyles of the femur. This fits into a concave depression on the other bone, such as the trochlear notch of the ulna and the condyles of the tibia.
- Pivot joints. These are monaxial joints in which a bone spins on its longitudinal axis like the axle of a bicycle wheel. There are two principal examples: the atlantoaxial joint between the first two vertebrae, and the radioulnar joint at the elbow. At the atlantoaxial joint, the dens of the axis projects into the vertebral foramen of the atlas and is held against the anterior arch of the atlas by the transverse ligament. As the head rotates left and right, the skull and atlas pivot around the dens. At the radioulnar joint, the anular ligament of the ulna wraps around the neck of the radius. During pronation and supination of the forearm, the disclike radial head pivots like a wheel turning on its axle. The edge of the wheel spins against the radial notch of the ulna like a car tire spinning in snow.
Figure 5. Six types of synovial joints
Some joints cannot be easily classified into any one of these six categories. The jaw joint, for example, has some aspects of condylar, hinge, and plane joints. It clearly has an elongated condyle where it meets the temporal bone of the cranium, but it moves in a hingelike fashion when the mandible moves up and down in speaking, biting, and chewing; it glides slightly forward when the jaw juts (protracts) to take a bite; and it glides from side to side to grind food between the molars. To observe the importance of the forward glide, try to open your mouth while pushing the jaw posteriorly with the heel of your hand; it is difficult to open the mouth more than 1 or 2 cm when there is resistance to protraction of the mandible.
The knee is a classic hinge joint, but has an element of the pivot type; when we lock our knees to stand more effortlessly, the femur pivots slightly on the tibia. The humeroradial joint acts as a hinge joint when the elbow flexes and a pivot joint when the forearm pronates.
The Jaw Joint
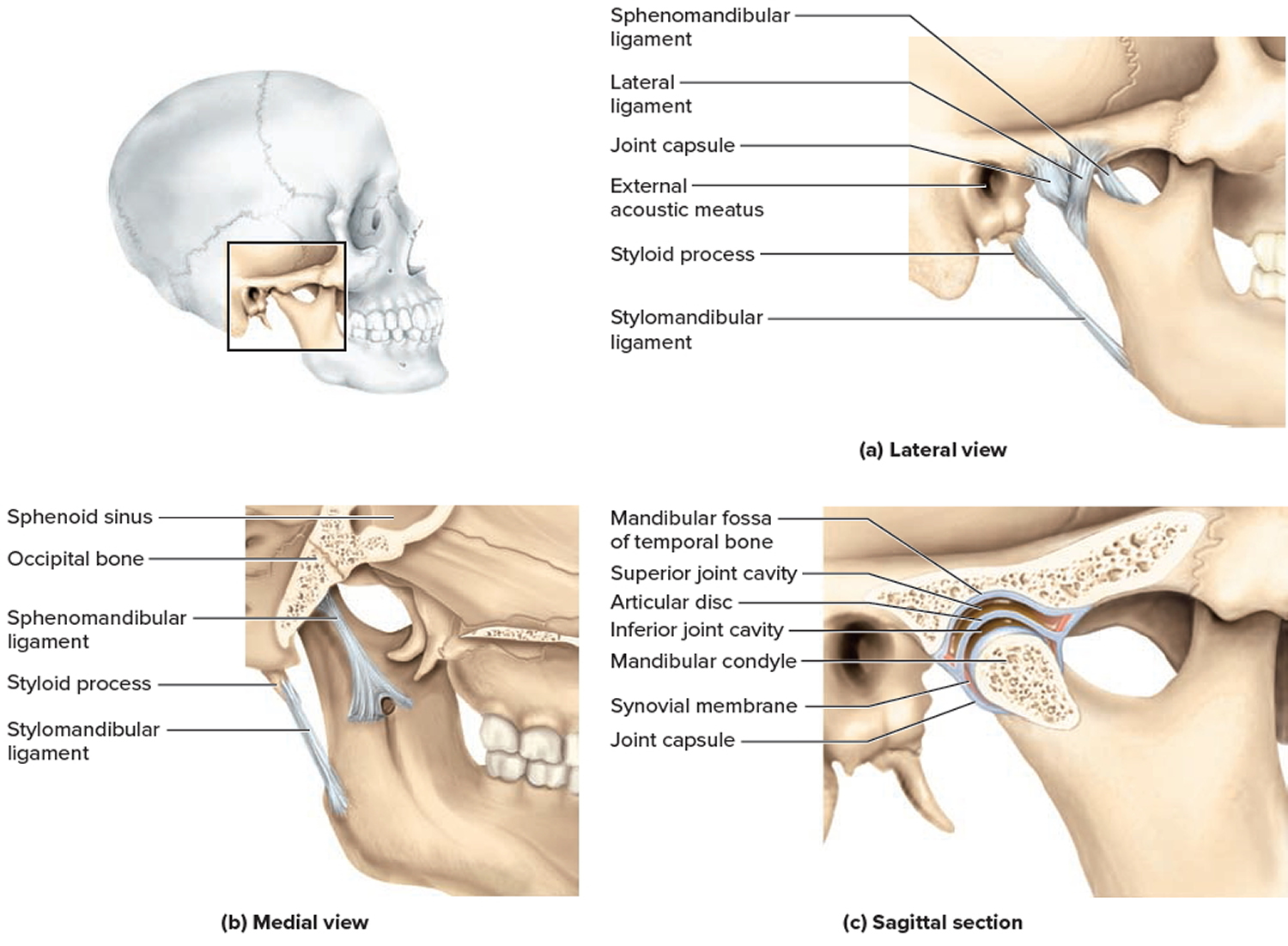
The temporomandibular (jaw) joint (TMJ) is the articulation of the condyle of the mandible with the mandibular fossa of the temporal bone. You can feel its action by pressing your fingertips against the jaw immediately anterior to the ear while opening and closing your mouth. The synovial cavity of the TMJ is divided into superior and inferior chambers by an articular disc, which permits lateral and medial excursion of the mandible. Two ligaments support the joint. The lateral ligament prevents posterior displacement of the mandible. If the jaw receives a hard blow, this ligament normally prevents the condylar process from being driven upward and fracturing the base of the skull. The sphenomandibular ligament on the medial side of the joint extends from the sphenoid bone to the ramus of the mandible. A stylomandibular ligament extends from the styloid process to the angle of the mandible but is not part of the TMJ proper.
A deep yawn or other strenuous depression of the mandible can dislocate the TMJ by making the condyle pop out of the fossa and slip forward. The joint is relocated by pressing down on the molars while pushing the jaw posteriorly.
Figure 6. Temporomandibular joint (TMJ)
The Shoulder Joint
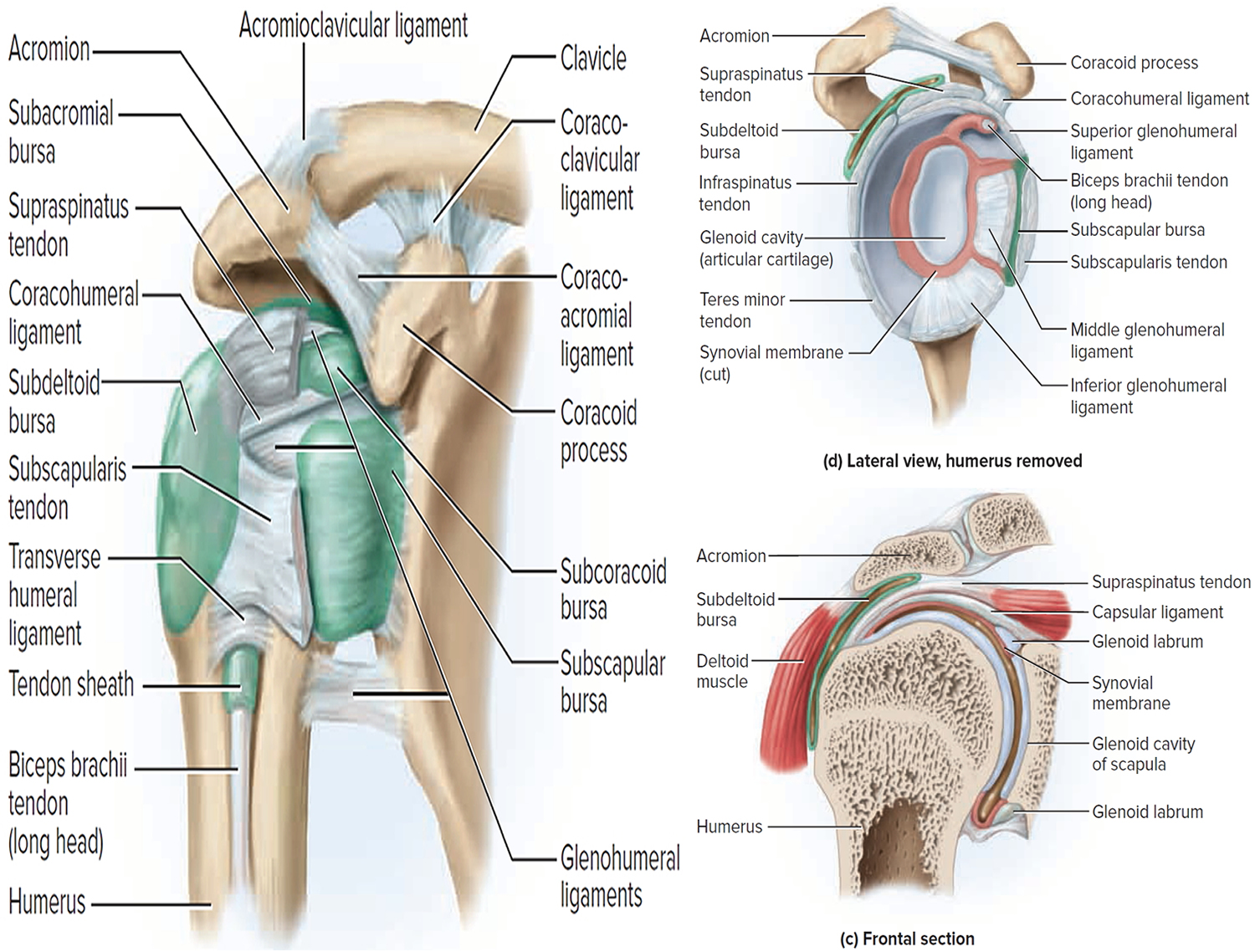
The glenohumeral (humeroscapular) joint, or shoulder joint, is where the hemispherical head of the humerus articulates with the glenoid cavity of the scapula. Together, the shoulder and elbow joints serve to position the hand for the performance of a task; without a hand, shoulder and elbow movements are almost useless. The relatively loose shoulder joint capsule and shallow glenoid cavity sacrifice joint stability for freedom of movement. The cavity, however, has a ring of fibrocartilage called the glenoid labrum around its margin, making it somewhat deeper than it looks on a dried skeleton.
The shoulder is stabilized mainly by the biceps brachii muscle on the anterior side of the arm. One of its tendons arises from the long head of the muscle, passes through the intertubercular groove of the humerus, and inserts on the superior margin of the glenoid cavity. It acts as a taut strap that presses the humeral head against the glenoid cavity. Four additional muscles help to stabilize this joint: the supraspinatus, infraspinatus, teres minor, and subscapularis. Their tendons form the rotator cuff, which is fused to the joint capsule on all sides except the inferior.
Five principal ligaments also support this joint. Three of them, called the glenohumeral ligaments, are relatively weak and sometimes absent. The other two are the coracohumeral ligament, which extends from the coracoid process of the scapula to the greater tubercle of the humerus, and the transverse humeral ligament, which extends from the greater to the lesser tubercle of the humerus and forms a tunnel housing the tendon from the long head of the biceps.
Four bursae occur at the shoulder. Their names describe their locations: the subdeltoid, subacromial, subcoracoid, and subscapular bursae. The deltoid is the large muscle that caps the shoulder, and the other bursae are named for parts of the scapula.
Figure 7. Shoulder joint
The Elbow Joint
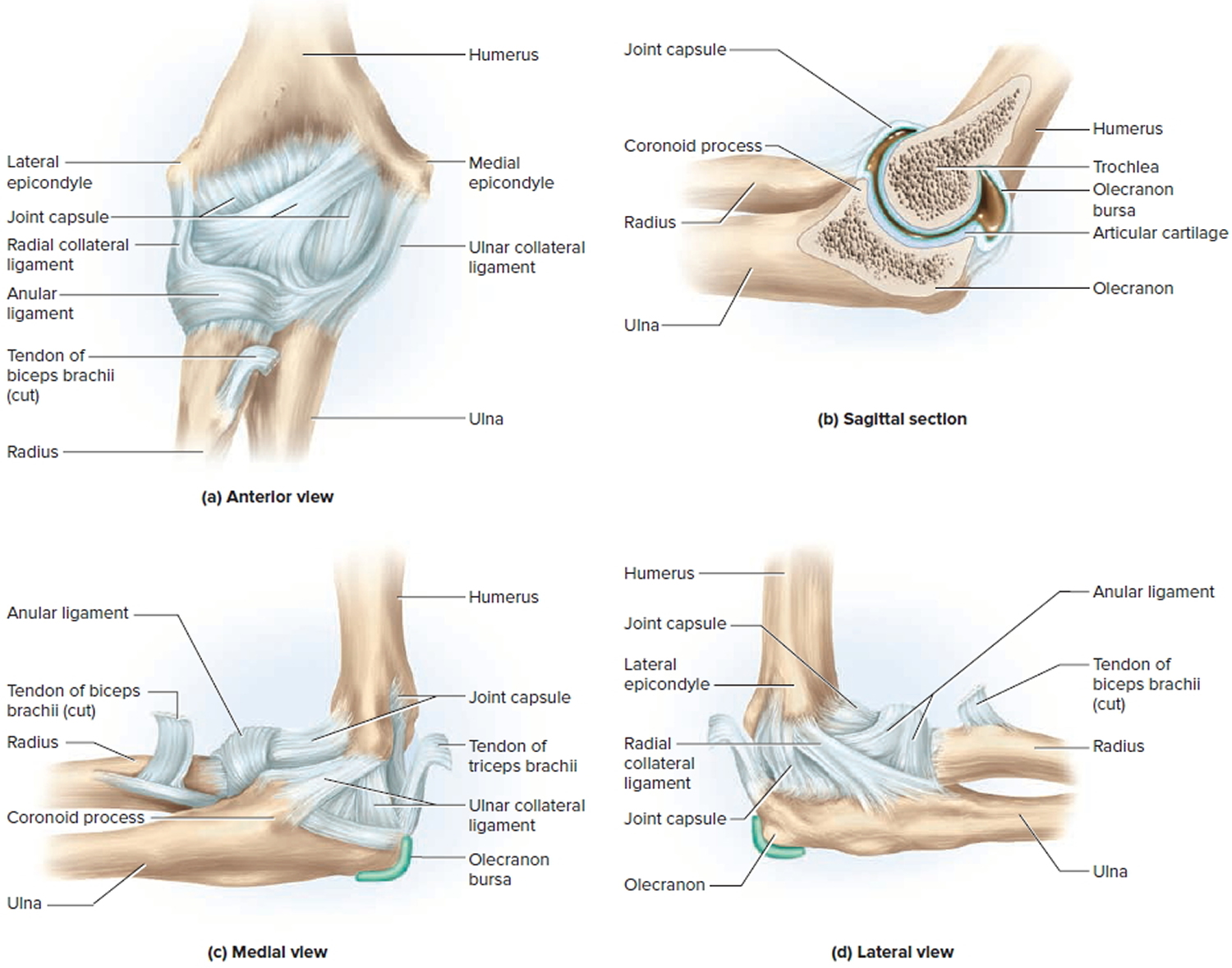
The elbow is a hinge joint composed of two articulations: the humeroulnar joint where the trochlea of the humerus joins the trochlear notch of the ulna, and the humeroradial joint where the capitulum of the humerus meets the head of the radius. Both are enclosed in a single joint capsule. On the posterior side of the elbow, there is a prominent olecranon bursa to ease the movement of tendons over the joint. Side-to-side motions of the elbow joint are restricted by a pair of ligaments: the radial (lateral) collateral ligament and ulnar (medial) collateral ligament.
Another joint occurs in the elbow region, the proximal radioulnar joint, but it is not involved in the hinge. At this joint, the edge of the disclike head of the radius fits into the radial notch of the ulna. It is held in place by the anular ligament, which encircles the radial head and is attached at each end to the ulna. The radial head rotates like a wheel against the ulna as the forearm is pronated or supinated.
Figure 8. Elbow joint
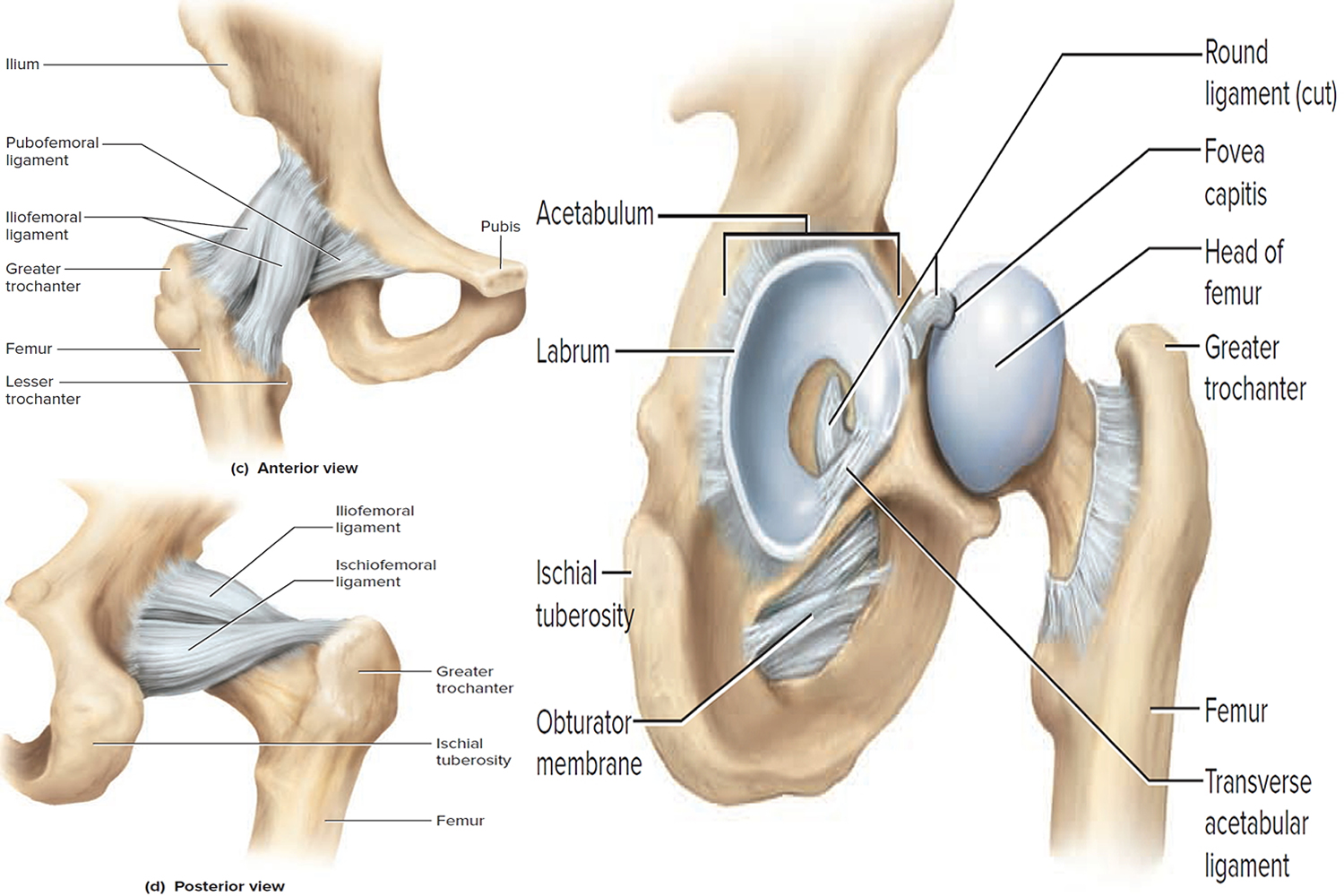
The Hip Joint
The coxal (hip) joint is the point where the head of the femur inserts into the acetabulum of the hip bone. Because the coxal joints bear much of the body’s weight, they have deep sockets and are much more stable than the shoulder joint. The depth of the socket is somewhat greater than you see on dried bones because of a horseshoeshaped ring of fibrocartilage, the acetabular labrum, attached to its rim. Dislocations of the hip are rare, but some infants suffer congenital dislocations because the acetabulum is not deep enough to hold the head of the femur in place. If detected early, this condition can be treated with a harness, worn for 2 to 4 months, that holds the head of the femur in the proper position until the joint is stronger.
Figure 9. Hip joint
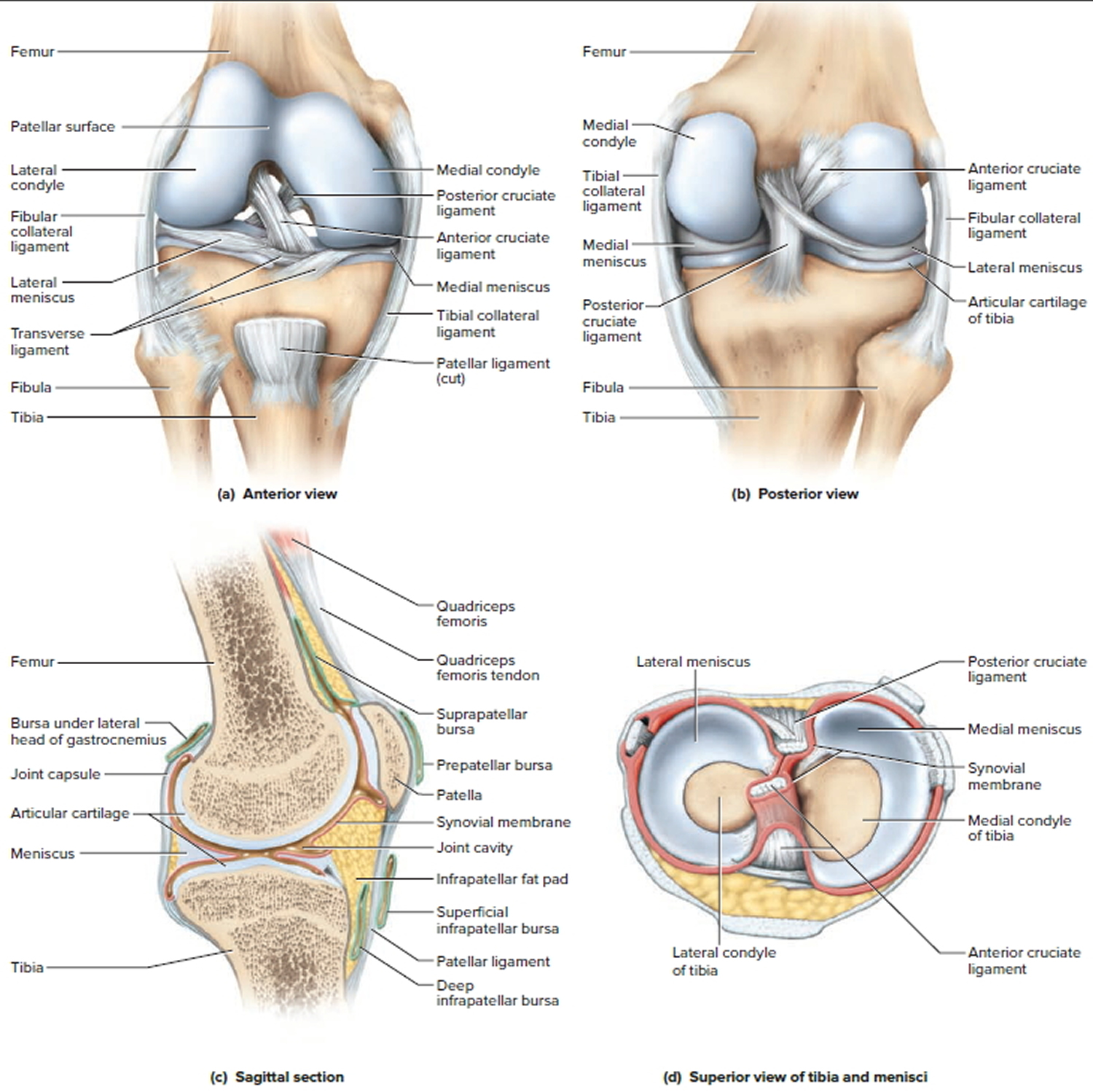
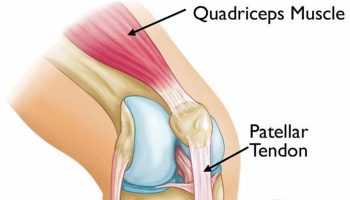
The Knee Joint
The tibiofemoral (knee) joint is the largest and most complex diarthrosis of the body. It is primarily a hinge joint, but when the knee is flexed it is also capable of slight rotation and lateral gliding. The patella and patellar ligament also articulate with the femur to form a gliding patellofemoral joint. The joint capsule encloses only the lateral and posterior aspects of the knee joint, not the anterior. The anterior aspect is covered by the patellar ligament and the lateral and medial patellar retinacula. These are extensions of the tendon of the quadriceps femoris muscle, the large anterior muscle of the thigh. The knee is stabilized mainly by the quadriceps tendon in front and the tendon of the semimembranosus muscle on the rear of the thigh. Developing strength in these muscles therefore reduces the risk of knee injury. The joint cavity contains two C-shaped cartilages called the lateral and medial menisci (singular, meniscus) joined by a transverse ligament. The menisci absorb the shock of the body weight jostling up and down on the knee and prevent the femur from rocking from side to side on the tibia.
The posterior popliteal region of the knee is supported by a complex array of extracapsular ligaments external to the joint capsule and two intracapsular ligaments within it. The extracapsular ligaments include two collateral ligaments that prevent the knee from rotating when the joint is extended—the fibular (lateral) collateral ligament and the tibial (medial) collateral ligament—and other ligaments. The two intracapsular ligaments lie deep within the joint. The synovial membrane folds around them, however, so that they are excluded from the fluid-filled synovial cavity. These ligaments cross each other in the form of an X; hence, they are called the anterior cruciate ligament (ACL) and posterior cruciate ligament (PCL). These are named according to whether they attach to the anterior or posterior side of the tibia, not for their attachments to the femur. When the knee is extended, the ACL is pulled tight and prevents hyperextension. The PCL prevents the femur from sliding off the front of the tibia and prevents the tibia from being displaced backward. The ACL is one of the most common sites of knee injury.
Figure 10. Knee joint
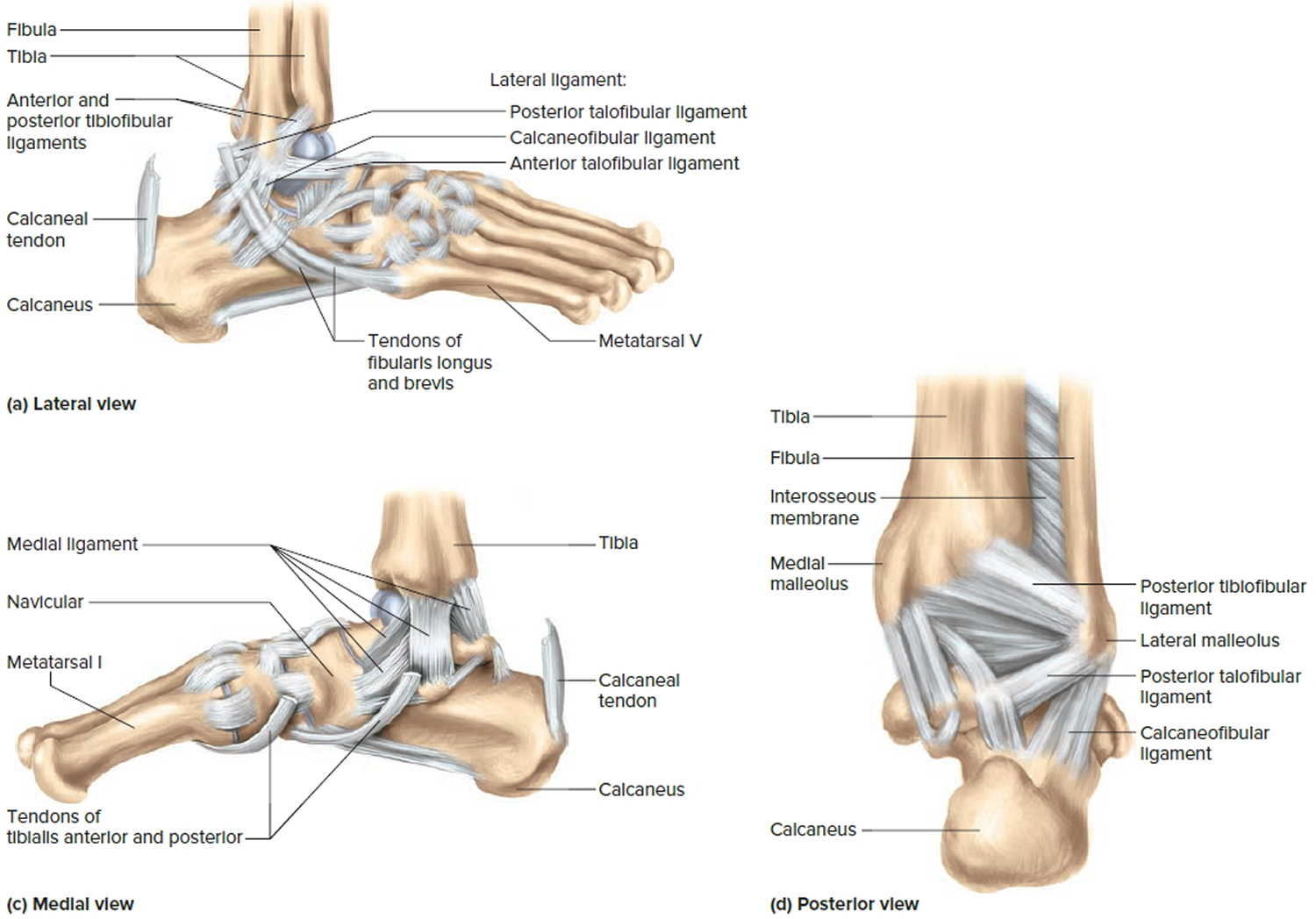
The Ankle Joint
The talocrural (ankle) joint includes two articulations—a medial joint between the tibia and talus and a lateral joint between the fibula and talus, both enclosed in one joint capsule. The malleoli of the tibia and fibula overhang the talus on each side like a cap and prevent most side-to-side motion. The ankle therefore has a more restricted range of motion than the wrist.
The ligaments of the ankle include (1) anterior and posterior tibiofibular ligaments, which bind the tibia to the fibula; (2) a multipart medial (deltoid) ligament, which binds the tibia to the foot on the medial side; and (3) a multipart lateral (collateral) ligament, which binds the fibula to the foot on the lateral side. The calcaneal (Achilles) tendon extends from the calf muscles to the calcaneus. It plantarflexes the foot and limits dorsiflexion. Plantar flexion is limited by extensor tendons on the anterior side of the ankle and by the anterior part of the joint capsule.
Sprains (torn ligaments and tendons) are common at the ankle, especially when the foot is suddenly inverted or everted to excess. They are painful and usually accompanied by immediate swelling. They are best treated by immobilizing the joint and reducing swelling with an ice pack, but in extreme cases may require a cast or surgery.
Figure 11. Ankle joint

{kind=link}