Contents
What is the xiphoid process
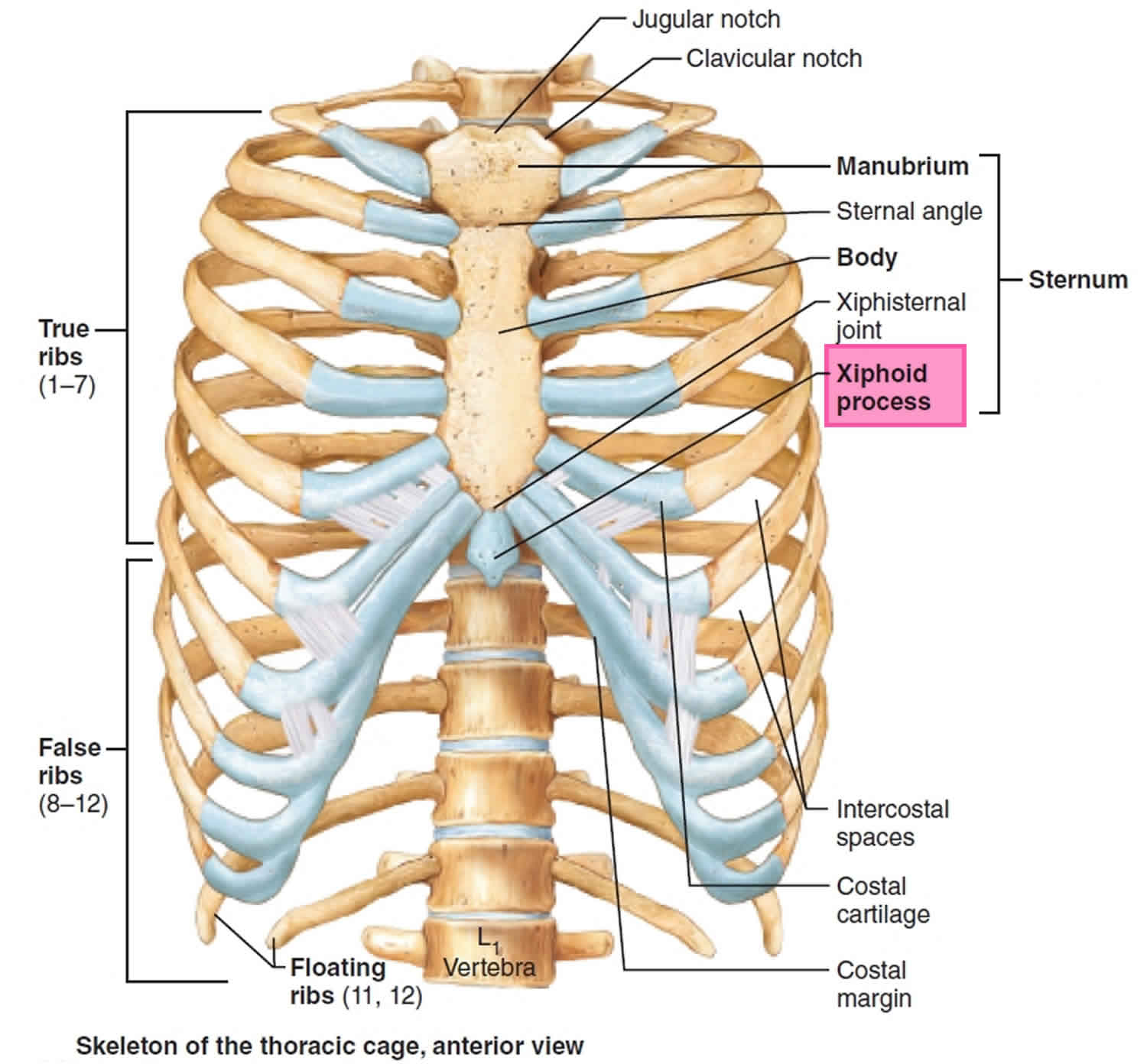
Xiphoid process also known as the xiphisternum, is the smallest part of the three sections of the sternum (see Figure 1). The xiphoid process shape is variable: it may be wide, thin and elongated, pointed, bifid, curved, or perforated. Xiphoid process begins as a cartilaginous structure in youth, which becomes ossified in the adult. The joints between the body of the sternum and the xiphoid process are usually symphyses. The joint between the body of the sternum and the xiphoid process often becomes ossified with age. On each side of its upper lateral margin is a demifacet for articulation with the inferior end of the seventh costal cartilage.
The adult sternum (Figure 1) consists of three major elements: the broad and superiorly positioned manubrium of the sternum, the narrow and longitudinally oriented body of the sternum, and the small and inferiorly positioned xiphoid process.
Figure 1. Sternum and Xiphoid process

Xiphoid process function
The xiphoid process serves as an attachment for several soft tissue structures that have rich innervation.
Table 1. The soft-tissues that attach to the xiphoid process and their innervation
| Aspect | Attachment | Innervation |
| Anterior | The Linea Alba Fibres of Rectus Abdominis | Lower intercostal nerves |
| Lateral | The aponeurosis of the three flat muscles (external oblique, internal oblique, and transversus abdominis) | Lower intercostal nerves, Obliquus internus and Transversus also receive filaments from the anterior branch of the iliohypogastric and sometimes from the ilioinguinal nerves |
| Anterior costoxiphoid ligament | Lower intercostal nerves | |
| Posterior | Posterior costoxiphoid ligament | Lower intercostal nerves |
| Fibres from the diaphragm | Phrenic (C3,4,5), lower intercostal nerves | |
| Fibres from Transverse thoracis | Lower intercostal nerves |
The transversus thoracis muscles originate from the posterior aspect of the xiphoid process, the inferior part of the body of the sternum, and the adjacent costal cartilages of the lower true ribs. They pass superiorly and laterally to insert into the lower borders of the costal cartilages of ribs III to VI. They most likely pull these latter elements inferiorly. The transversus thoracis muscles lie deep to the internal thoracic vessels and secure these vessels to the wall.
The diaphragm is a thin musculotendinous structure that fills the inferior thoracic aperture and separates the thoracic cavity from the abdominal cavity. The diaphragm is attached peripherally to the:
- xiphoid process of the sternum,
- costal margin of the thoracic wall,
- ends of ribs XI and XII,
- ligaments that span across structures of the posterior abdominal wall, and
- vertebrae of the lumbar region.
Xiphoid process pain
Xiphoid process pain also called xiphodynia is a medical term used to describe an ‘uncommon’ syndrome with a constellation of symptoms ranging from upper abdominal pain, chest pain, sometimes throat and arm symptoms which are referred from the xiphisternal joint or the structures attached to the xiphoid process 1.
Xiphoid process pain (xiphodynia) is a condition involving referral of pain to the chest, abdomen, throat, arms and head from an irritated xiphoid process 1. There are no clear data relating to the incidence or prevalence of xiphoid process pain (xiphodynia). Most authors say that it is an uncommon disorder 2 while Lipkin et al 3 found the syndrome present in about 2 percent of the population of a general-hospital ward and stated that it is “far more common than is generally appreciated”. They went so far as to suggest that examination of the xiphoid should be part of the routine examination of any patient presenting with upper-abdominal or chest pain 3.
Xiphoid process pain cause
While xiphoid process pain (xiphodynia) is frequently insidious in onset, trauma may precipitate the syndrome. Acceleration/deceleration injuries 2, blunt trauma to the chest 2, unaccustomed heavy lifting and aerobics have been known to precipitate xiphodynia 4 likely because of the muscular attachments. The cases presented here 1 all gave a history of ‘trauma’ which appeared to be associated with the onset of symptoms.
Xiphoid process pain symptoms
Xiphoid process pain (xiphodynia) is a musculoskeletal disorder capable of producing a constellation of symptoms that mimic several common abdominal and thoracic diseases including:
- Cardiac chest pain
- Epigastric pain
- Nausea, vomiting and diarrhea
- Radiating pain into the back, neck, shoulders, arms and chest wall 4
Xiphoid process pain diagnosis
The diagnosis of xiphodynia is dependent upon the reproduction of the patient’s symptoms completely or in part by moderate pressure on the xiphoid process and its adjacent structures.
Even though xiphodynia often exists in the absence of any other medical condition, it has been demonstrated in conjunction with life-threatening disease such as cardiac disease including angina pectoris, myocardial infarction, and pericarditis 5. It is therefore imperative that any patient presenting to a primary health care provider with acute chest or abdominal pain be carefully investigated to establish a diagnosis and treatment plan. Where appropriate, emergency medical care must be rendered. In cases where a clear medical diagnosis cannot be established, a simple provocative test may uncover a symptomatic xiphoid process and establish the diagnosis of xiphodynia. In those patients who receive treatment for an established ‘medical condition’ in whom symptoms persist, consideration might be given to examining for xiphodynia.
Xiphoid process pain treatment
The literature suggests that xiphodynia is a self-limiting disorder to be treated with reassurance 5 or with analgesics, topical heat and cold, and an elastic rib belt 2. It is clear from these and other reported cases 5 that xiphodynia may not be self-limiting. The medical ‘treatment of choice’ is an injection of local anesthetic and steroid 6. Xiphoid injection, while often curative, is not without risk of complications including pleural or peritoneal perforation, pneumothorax, or infection 2.
Conservative physical therapies are worth a trial, however no evidence exists for their effectiveness with xiphodynia.
Xiphoid process protrusion
The hook-shaped xiphoid process has possible clinical consequences associated with it, e.g., mimicking an epigastric mass 7. Various anatomical variations of the xiphoid process have been reported and include a bifid, trifid, pointed, flat, wide, deflected or curved shape 8. Akin et al. 9 documented variations of the xiphoid process in 500 patients using multidetector computed tomography. Ventral deviation of the xiphoid process was present in 327 out of the 500 patients and accounted for the majority of xiphoid variations at 65.4% 9. However, only three out of the 500 patients (0.6%) presented with a hook-shaped xiphoid process that protruded dorsally. Mean length, width, and thickness were 50 mm, 22 mm, and 7.3 mm, respectively 9. Xie et al. 7 reported that the mean length, width, and thickness was 60.31, 23.42, and 8.25 mm in 943 sternums (41 cadavers and 902 patients), respectively.
Ateşoğlu et al. 10 reported that mean length, width, and thickness were 39 mm, 22 mm, and 6.6 mm in 97 adult males. Our findings illustrate a similar or above average length of the xiphoid process but a width and thickness that is less than the mean found in these studies. Empirically, it is thought that the mean length of the xiphoid process is approximately 2–3 cm. However, recent studies using computed tomography have revealed the mean length to be 4–6 cm, which is much longer. These differences might result from the difficulties in the visualization of the cartilaginous part of the xiphoid process or its differentiation from neighboring soft tissues 10.
Xie et al. 7 found that the dorsal, hook-shaped protrusion of the xiphoid process variation was present in 19 out of 943 (2.0%) cases and was found only in type II (pointed shape) processes. Mashriqi et al. 11 described a bifid xiphoid process that was orientated in the anterior direction which could also possess the risk of appearing as an epigastric mass during imaging. Even though various unusual variations of the xiphoid process can resemble an epigastric mass, directionality (anterior vs dorsally curved) of the variant could pose a red flag in terms of fractures involving the xiphoid process. Due to the liver’s proximity dorsal to the xiphoid process, the hook-shaped xiphoid process is already angled closer to the liver than when normally observed. A fracture of the xiphoid process could potentially puncture the liver or the heart during, for example, cardiopulmonary resucitation.
Overall, this unusual finding of a xiphoid process serves to provide a better understanding of current anatomical variations that exist pertaining to the xiphoid process 12. Further, it provides a means of proper diagnosis during imaging and surgical interventions.
- Simpson JK, Hawken E. Xiphodynia: a diagnostic conundrum. Chiropr Osteopat. 2007;15:13. Published 2007 Sep 15. doi:10.1186/1746-1340-15-13 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2045657[↩][↩][↩]
- Waldman S. Atlas of uncommon pain syndromes. Philadelphia: Saunders; Elsevier; 2003.[↩][↩][↩][↩][↩]
- Gray H. Anatomy of the Human Body. 1918; Philadelphia: Lea & Febiger; 2000.[↩][↩]
- Howell J. Xiphodynia: a report of three cases. J Emerg Med. 1992;10:435–438. doi: 10.1016/0736-4679(92)90272-U[↩][↩]
- Koren W, Shahar A. Xiphodynia Masking Acute Myocardial Infarction: A Diagnostic Cul-de-sac. Am J Emerg Med. 1998;16:177–178. doi: 10.1016/S0735-6757(98)90041-9[↩][↩][↩]
- Demir H, M P, Kirnap M, Calis M, Ikizceli I. Comparison of the Effects of Laser, Ultrasound, and Combined Laser + Ultrasound Treatments in Experimental Tendon Healing. Lasers in Surgery and Medicine. 2004;35:84–89. doi: 10.1002/lsm.20046[↩]
- Xie YZ, Wang BJ, Yun JS, Chung GH, Ma ZB, Li XJ, Kim IS, Chai OH, Han EH, Kim HT, Song CH. Morphology of the human xiphoid process: dissection and radiography of cadavers and MDCT of patients. Surg Radiol Anat. 2014;36:209–217[↩][↩][↩]
- Eid S, Iwanaga J, Oskouian RJ, Loukas M, Tubbs RS. Bifid xiphoid process: case report and review. Cureus. 2018;10:e3153[↩]
- Akin K, Kosehan D, Topcu A, Koktener A. Anatomic evaluation of the xiphoid process with 64-row multidetector computed tomography. Skeletal Radiol. 2011;40:447–452[↩][↩][↩]
- Ateşoğlu S, Deniz M, Uslu AI. Evaluation of the morphological characteristic and sex differences of sternum by multi-detector computed tomography. Folia Morphol (Warsz) 2018;77:489–497[↩][↩]
- Mashriqi F, D’Antoni AV, Tubbs RS. Xiphoid process variations: a review with an extremely unusual case report. Cureus. 2017;9:e1613[↩]
- Lachkar S, Iwanaga J, Tubbs RS. An elongated dorsally curved xiphoid process. Anat Cell Biol. 2019;52(1):102–104. doi:10.5115/acb.2019.52.1.102 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6449596[↩]


{kind=link}