
Contents
What is Kawasaki disease
Kawasaki disease is a serious illness that causes inflammation in the walls of medium-sized arteries throughout the body, that primarily affects young children and infants. The inflammation tends to affect the coronary arteries, which supply blood to the heart muscle. In fact Kawasaki Disease is the leading cause of acquired heart disease in infants and young children in the United States.
Studies in the United States have reported annual incidence rates of 6.5 to 15.5 per 100 000 among children less than 5 years of age, a male-female ratio of 1.5:1 and seasonal peaks in winter and spring 1. Worldwide, the highest incidence rate remains in Japan, where nationwide surveys have reported annual rates of about 100 per 100 000 among children in that age group, a male-female ratio of 1.4:1 and no consistent seasonal trends 2.
Over 4,000 children develop Kawasaki disease each year. Kawasaki disease mainly affects children under the age of five with 80-90% of patients under the age of 5 and older than 6 months 3.
Kawasaki disease is the leading cause of acquired heart disease in children. Although about 80 percent of patients are under five years of age, older children and teenagers can also get Kawasaki disease, but this is uncommon. Kawasaki disease is more common in boys than girls and the majority of cases are diagnosed in the winter and early spring. Kawasaki disease is not contagious.
Kawasaki disease is sometimes called mucocutaneous lymph node syndrome or Kawasaki syndrome, because it also affects lymph nodes, skin, and the mucous membranes inside the mouth, nose and throat.
The disease is named after Tomisaku Kawasaki, a Japanese pediatrician who first described the illness in the medical literature in 1967. Although it is more prevalent among children of Asian and Pacific Island descent, Kawasaki disease affects people of all racial and ethnic groups. It is estimated that more than 4,200 children are diagnosed with Kawasaki Disease in the U.S. each year. The cause of Kawasaki disease is unknown, although an agent, like a virus, is suspected. Kawasaki Disease occurs more frequently in those of Asian ancestry. There is no currently accepted scientific evidence that Kawasaki disease is caused by carpet cleaning or chemical exposure.
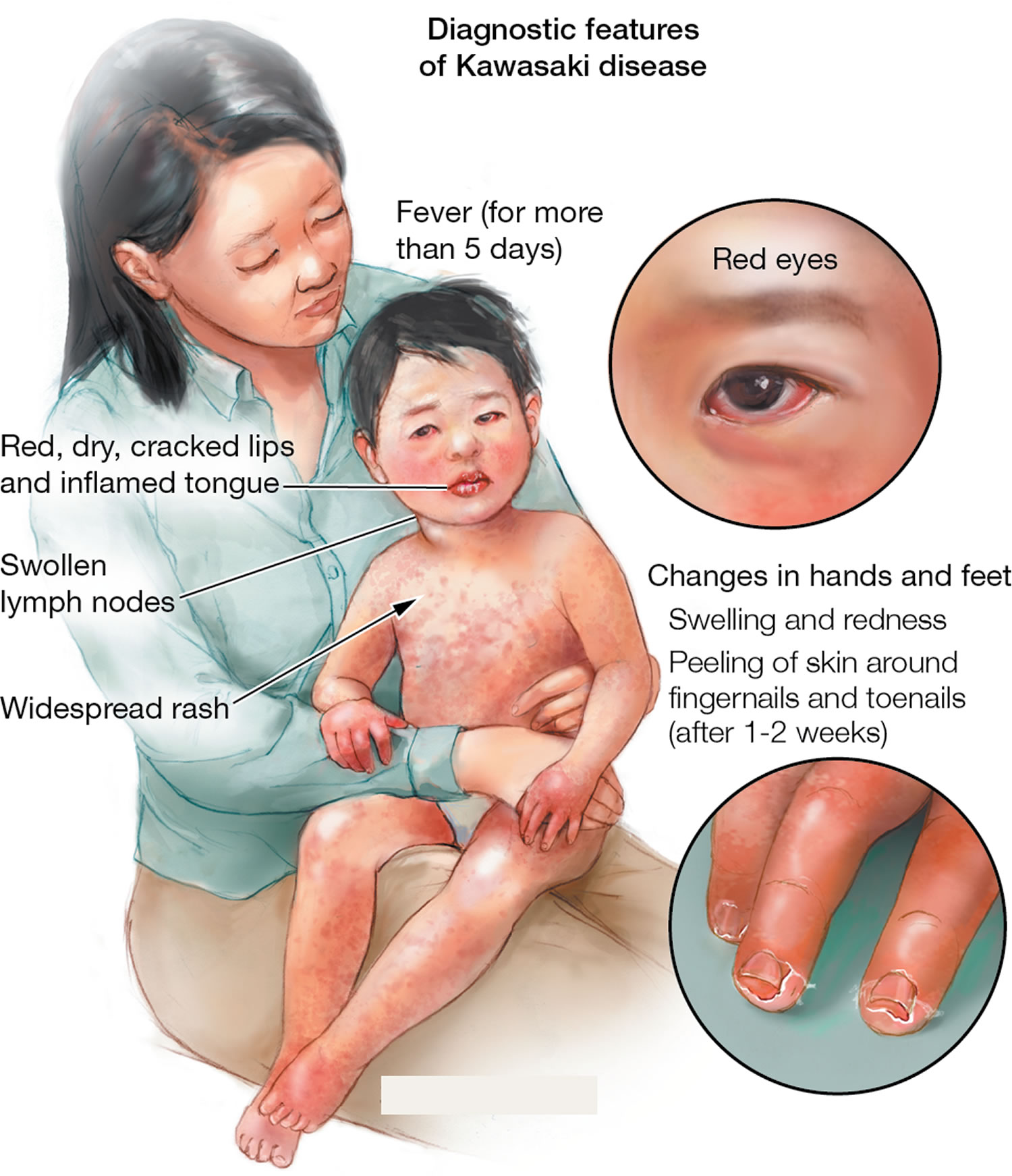
The characteristic symptoms of Kawasaki disease are a high temperature that lasts for more than five days, with:
- Rash, often worse in the groin area
- Swollen lymph nodes in the neck
- Bright red, swollen, cracked lips, “strawberry” tongue, which appears with shiny bright red spots after the top coating sloughs off
- Swollen hands and feet and redness of the palms and soles of the feet
- Red bloodshot eyes, without drainage or crusting
Early on, Kawasaki disease can affect the function of the heart muscle or the heart valves.
If Kawasaki disease is recognized and treated early, children can begin to feel better in a few days with a low likelihood of long-term heart issues. After a few weeks the symptoms become less severe, but may last longer. At this stage, the affected child may have peeling skin on their fingers and toes.
There is no specific test for Kawasaki disease; doctors make a clinical diagnosis based on a collection of symptoms and physical findings.
Understandably, children with these symptoms are extremely uncomfortable and irritable. Any parent whose child has persistent fever and any of these symptoms should take him or her to the doctor immediately.
With early recognition and treatment, full recovery can be expected.
Without treatment, about 25% of children develop heart disease involving the coronary arteries and 1-2% of patients die from complications of coronary blood vessel inflammation. Timely diagnosis and treatment (which usually includes intravenous gamma globulin) is highly effective in preventing coronary complications. Patients who have had Kawasaki should have an echocardiogram every 1-2 years to screen for heart problems.
Doctors continue to study the long-term outcome of children who do not appear to have coronary involvement. Other kinds of longer-term consequences (e.g., non-coronary) are extremely rare. There is no evidence that links Kawasaki disease with autism or a seizure disorder. A very small number of Kawasaki disease children might have a seizure in the early acute stage of Kawasaki disease when there are very high fevers, but there is no on-going or long term seizure prone condition.
Is Kawasaki disease contagious?
Kawasaki Disease is not contagious. It does not spread among family members or children in child care centers.
It is possible to get Kawasaki disease as an adult?
Kawasaki disease is extremely rare in older children, teens and adults. Rarely, an adult may have heart problems that may be caused by having had Kawasaki disease as a child that did not get diagnosed.
Figure 1. Kawasaki disease rash

Figure 2. Strawberry tongue

If your child has a fever for 4 to 5 days with some of the key signs and symptoms above, ask your doctor whether he or she could have Kawasaki Disease. It can be challenging to diagnose, so your child may have to be examined several times.
Kawasaki disease criteria
Kawasaki Disease begins with a high fever (>102 °F or 38.9 °C) for at least five days, along with other signs and symptoms.
- Rash all over the body but more severe in the diaper area.
- Red, bloodshot eyes without any pus, drainage, or crusting.
- Tender, swollen gland (lymph node) on one side of the neck.
- Swollen hands and feet with redness on the palms of the hands and the soles of the feet.
- Very red, swollen, and cracked lips; strawberry-like tongue with rough, red spots.
- Significant irritability and fussiness.
- Peeling fingers and toes (typically 2 to 3 weeks after the beginning of fever).
Kawasaki disease is characterized by fever and the following clinical features:
- (1) bilateral bulbar conjunctival injection with limbic sparing and without exudate;
- (2) erythematous mouth and pharynx, strawberry tongue, and red, cracked lips;
- (3) a polymorphous, generalized, erythematous rash that can be morbilliform, maculopapular, or scarlatiniform or may resemble erythema multiforme ;
- (4) changes in the peripheral extremities consisting of induration of the hands and feet with erythematous palms and soles, often with later periungual desquamation; and
- (5) acute, nonsuppurative, usually unilateral, cervical lymphadenopathy with at least one node 1.5 cm in diameter.
Kawasaki disease diagnosis may be delayed in patients who come to attention because of fever and unilateral cervical lymphadenitis, which mistakenly is thought to be bacterial lymphadenitis; a distinguishing feature is that in Kawasaki disease, lymphadenitis is unlikely to be necrotizing/suppurative on imaging studies.
For diagnosis of classic Kawasaki disease, patients should have fever for at least 5 days (or fever until the date of treatment if given before the fifth day of illness) and at least 4 of the above 5 features without alternative explanation for the findings. The presence of a concurrent or preceding viral upper respiratory infection does not exclude the diagnosis of Kawasaki disease. The epidemiologic case definition also allows diagnosis of incomplete Kawasaki disease when a patient has fewer than 4 principal clinical criteria in the presence of fever and coronary artery abnormalities.
Irritability, abdominal pain, diarrhea, and vomiting are common associated features. Other findings include urethritis with sterile pyuria (70% of cases), mild anterior uveitis (80%), mild elevation of hepatic transaminase levels (50%), arthritis or arthralgia (10%–20%), meningismus with cerebrospinal fluid pleocytosis (40%), pericardial effusion of at least 1 mm (less than 5%), gallbladder hydrops (less than 10%), and myocarditis manifested by congestive heart failure (less than 5%). A persistent resting tachycardia and the presence of an S3 gallop often are appreciated. Fine desquamation in the groin area can occur in the acute phase of disease (Fink sign). Inflammation or ulceration may be observed at the inoculation scar of previous bacille Calmette-Guérin immunization. Rarely, Kawasaki disease can present with what appears to be “septic shock” with need for intensive care; these children often have significant thrombocytopenia at admission. Group A streptococcal or Staphylococcus aureus toxic shock syndrome should be excluded in such cases.
Kawasaki disease long term effects
With early recognition and treatment, full recovery can be expected. However, 2% of patients die from complications of coronary blood vessel inflammation. Patients who have had Kawasaki should have an echocardiogram every 1-2 years to screen for heart problems.
Long-term health effects for children who do not have any coronary artery problems are very rare. Such children are expected to lead a normal life with no related health problems. Children with important coronary artery problems may develop clots or narrowing in the arteries, and need special medications and long-term check-ups, and, rarely heart surgery or catheter procedures. These children require routine assessments with an echocardiogram, ECG and blood work and less frequent assessments with an MRI or CT or stress test. Even still, these patients usually lead a normal life and can participate in play and exercise.
Kawasaki disease complications
Kawasaki disease is a leading cause of acquired heart disease in children, but with effective treatment, only a small percentage of children have lasting damage.
If Kawasaki disease is left untreated, it can lead to serious complications such as inflammation of the blood vessels. This can be particularly dangerous, because it can affect the coronary arteries—the blood vessels that supply blood to the heart. Aneurysms and/or narrowing of one or more coronary artery can also develop.
Heart complications include:
- Inflammation of blood vessels (vasculitis), usually the coronary arteries, that supply blood to the heart
- Inflammation of the heart muscle (myocarditis)
- Heart valve problems
An aneurysm is a ballooning out of a damaged and weakened blood vessel wall. Aneurysms increase the risk of blood clots forming and blocking the artery, which could lead to a heart attack or cause life-threatening internal bleeding. These can lead to angina, myocardial infarction (heart attack) or sudden death. When children are treated with intravenous gamma globulin (IVIG) up to 10 days into the illness and respond quickly, the risk of subsequent coronary artery abnormality is reduced to 2-4% and most of these have mild abnormalities many of which resolve. Therefore, it is extremely important that a diagnosis is made by 10th day of the illness. Treatment should begin as soon as possible.
For a very small percentage of children who develop coronary artery problems, Kawasaki disease is fatal, even with treatment.
Follow-up echocardiography is performed on all children with Kawasaki disease at about 6 to 8 weeks to look for coronary artery abnormalities and to check the heart is otherwise normal. If coronary artery abnormalities are demonstrated then ongoing anticoagulation treatment, such as daily aspirin, will be needed and further heart imaging will be required.
Aneurysm
Inflammation in the blood vessels that supply blood to the heart (coronary arteries) can cause a section of the artery wall to weaken.
As the blood passes through the weakened part of the artery wall, the blood pressure causes it to bulge outwards like a balloon. This is called an aneurysm.
Some aneurysms heal by themselves over time. However, sometimes a blood clot (thrombosis) can form in a weakened section of the artery.
This can cause either:
- a heart attack – where part of the heart muscle dies because it is starved of oxygen
- heart disease – where the heart’s blood supply is blocked or interrupted
In rare cases, the aneurysm can burst (rupture), which could cause severe internal bleeding.
It’s also possible for other major arteries to be affected, such as the brachial artery, the main blood vessel in the upper arm, or the femoral artery, the main blood vessel in the upper thigh.
Risk of complications
Around 25% of children with Kawasaki disease who don’t receive treatment – because the condition has been diagnosed incorrectly, for example – go on to experience heart-related complications.
The risk of developing complications is reduced for children who receive intravenous immunoglobulin (IVIG) to treat Kawasaki disease.
The heart-related complications associated with Kawasaki disease are serious, and may be fatal in 1-2% of cases. Children under the age of one are thought to be at higher risk of serious complications.
Coronary artery aneurysms
The prevalence of coronary artery aneurysms in children with Kawasaki disease has substantially decreased since the initiation of intravenous gamma globulin (IVIG) treatment. Coronary artery aneurysms develop in 18% to 23% of children who do not receive such treatment, as compared with 4% to 8% of those who receive it within 10 days of fever onset 4. Maximum coronary artery involvement is usually within the first 6 to 8 weeks from fever onset. In an Ontario, Canada, survey 24% (92/382) of patients had coronary artery ectasia (size of coronary artery larger than normal for age), 8% (31/382) had non-giant coronary artery aneurysms (internal diameter > 4 mm and < 8 mm), and less than 1% (3/382) had giant coronary artery aneurysms (internal diameter ≥ 8. mm) on their initial echocardiogram 5.
Risk factors for increased risk of coronary artery aneurysms
Factors associated with an increased risk of coronary artery aneurysms include male sex, age less than 1 year and fever lasting more than 10 days 6. In an Ontario, Canada, survey 5, patients in the youngest and oldest groups had the highest risk of coronary artery aneurysms, with 15% of patients less than 1 year and 17% of those 10 to 14 years having aneurysms, as compared with 8% of children 1 to 4 years of age and 6% of those 5 to 9 years. There was a trend toward a greater rate of aneurysms among patients who did not receive intravenous gamma globulin (IVIG) treatment than among those who did (18% v. 8%). Among the patients who received intravenous gamma globulin (IVIG) treatment, the rate of aneurysms was significantly lower if the treatment was given within 10 days of fever onset than after 10 days (6% v. 27%). Multiple logistic regression analysis revealed that no intravenous gamma globulin (IVIG) treatment within 10 days of fever onset was an independent risk factor for coronary artery aneurysms. After controlling for treatment, the risk of aneurysms remained highest in the youngest age group (less than 1 year of age).
These findings are consistent with a study in British Columbia, which also demonstrated that age less than 1 year, age 9 years and older, and a delay in diagnosis were important risk factors for coronary artery aneurysms 7.
Treating complications
If your child develops a serious heart abnormality, they may require medication or, in some cases, surgery.
Possible treatments include:
- anticoagulant medicines and antiplatelet medicines – medicines that stop the blood clotting, which may prevent your child having a heart attack if their arteries are particularly inflamed
- coronary artery bypass graft – surgery to divert blood around narrow or clogged arteries, and improve the blood flow and oxygen supply to the heart
- coronary angioplasty – a procedure to widen blocked or narrowed coronary arteries to improve the blood flow to the heart; in some cases, a short, hollow metal tube called a stent is inserted into the blocked artery to keep it open
Children with severe complications may have permanent damage to their heart muscles or valves, the flaps that control the flow of blood. They’ll have regular follow-up appointments with a heart specialist (cardiologist) so their condition can be closely monitored.
Complications in later life
If your child has had heart complications as a result of Kawasaki disease, they may have an increased risk of developing cardiovascular complications later in life. This includes conditions such as heart attacks and heart disease.
If your child has had complications from Kawasaki disease, it’s usually recommended that they have follow-up appointments with a specialist.
The cardiologist will be able to advise you about your child’s likelihood of developing further heart-related problems.
Kawasaki disease causes
The cause of Kawasaki disease is not known, although it is thought to be caused by an infectious agent such as bacteria, viruses or other environmental factors that creates an intense immune reaction, but none has been proven.
Genetic predisposition/susceptibility may also play a role. Currently, there are no specific diagnostic tests for Kawasaki disease and the diagnosis is largely a process of ruling out diseases that cause similar signs and symptoms. The majority of cases are diagnosed in winter and early spring. There is no evidence that Kawasaki disease is contagious.
Infection
The symptoms of Kawasaki disease are similar to those of an infection, so bacteria or a virus may be responsible. However, so far a bacterial or viral cause hasn’t been identified.
As Kawasaki disease isn’t contagious, it can’t be passed from one person to another. This makes it unlikely that it’s caused by a virus alone.
Kawasaki disease doesn’t usually affect babies under six months old, although sometimes very young children can develop the condition.
This suggests that newborn babies are protected by antibodies passed on to them by their mother, either before birth or during breastfeeding. Antibodies are proteins that destroy disease-carrying organisms.
As few older children and adults are affected by Kawasaki disease, they may be immune to whatever causes it. While many people are exposed to Kawasaki disease, only a few go on to develop the symptoms.
Genetics
The children who develop Kawasaki disease may be genetically predisposed to it. This means the genes they inherit from their parents may make them more likely to get the condition.
One theory is that rather than there being a single gene responsible for Kawasaki disease, it may be the result of many genes that each slightly increase the chances of a child developing the condition.
Kawasaki disease is more common in children from northeast Asia, especially Japan and Korea. This also suggests there may be a genetic cause.
Other theories
One theory is that Kawasaki disease may be an autoimmune condition, where the immune system attacks healthy tissues and organs.
Other theories suggest Kawasaki disease may be a reaction to certain medications or environmental pollutants, such as chemicals or toxins (poisons).
Kawasaki disease risk factors
Three things are known to increase your child’s risk of developing Kawasaki disease, including:
- Age. Children under 5 years old are most at risk of Kawasaki disease.
- Sex. Boys are slightly more likely than girls are to develop Kawasaki disease.
- Ethnicity. Children of Asian or Pacific Island descent, such as Japanese or Korean, have higher rates of Kawasaki disease.
Kawasaki disease signs and symptoms
Kawasaki disease symptoms usually appear in three phases.
The most important aspect of Kawasaki disease is the heart’s involvement. Kawasaki disease can cause inflammation of blood vessels in the coronary arteries, which can lead to aneurysms. Kawasaki is the leading cause of acquired heart disease in children.
First Phase – Acute Phase (weeks 1-2)
Kawasaki Disease begins with a high fever (>102 °F or 38.9 °C) for at least five days, along with other signs and symptoms.
- Rash all over the body but more severe in the diaper area.
- Red, bloodshot eyes without any pus, drainage, or crusting.
- Tender, swollen gland (lymph node) on one side of the neck.
- Swollen hands and feet with redness on the palms of the hands and the soles of the feet.
- Very red, swollen, and cracked lips; strawberry-like tongue with rough, red spots.
- Significant irritability and fussiness.
Skin Rash
Your child may have a blotchy, red rash on their skin. It usually starts in the genital area before spreading to the torso, arms, legs and face.
The spots are usually red and raised, but there will not be any blistering.
Hands and feet
The skin on your child’s fingers or toes may become red or hard, and their hands and feet may swell up.
Your child may feel their hands and feet are tender and painful to touch or put weight on, so they may be reluctant to walk or crawl while these symptoms persist.
Conjunctival injection
Conjunctival injection is where the whites of the eyes become red and swollen. Both eyes are usually affected, but the condition isn’t painful.
Unlike conjunctivitis, where the thin layer of cells that cover the white part of the eye (conjunctiva) becomes inflamed, fluid doesn’t leak from the eyes in conjunctival injection.
Lips, mouth, throat and tongue
Your child’s lips may be red, dry or cracked. They may also swell up and peel or bleed.
The inside of your child’s mouth and throat may also be inflamed. Their tongue may be red, swollen and covered in small lumps, also known as “strawberry tongue”.
Swollen lymph glands
If you gently feel your child’s neck, you may be able to feel swollen lumps on one or both sides. The lumps could be swollen lymph glands.
Lymph glands are part of the immune system, the body’s defence against infection. They may swell to over 1.5cm wide, feel firm and be slightly painful.
Phase 2 – Sub-acute (weeks 2-4)
During the sub-acute phase, your child’s symptoms will become less severe but may last longer. The fever should subside, but your child may still be irritable and in considerable pain.
In the second phase of the disease, your child may develop:
- Peeling of the skin on the hands and feet, especially the tips of the fingers and toes, often in large sheets (typically 2 to 3 weeks after the beginning of fever).
- Joint pain
- Diarrhea
- Vomiting
- Abdominal pain
- Urine that contains pus
- Feeling drowsy and lacking energy (lethargic)
- Headache
- Joint pain and swollen joints
- Yellowing of the skin and the whites of the eyes (jaundice)
It’s during the second phase of Kawasaki disease that complications are more likely to develop, such as a coronary artery aneurysm, which is a bulge in one of the blood vessels that supply blood to the heart.
Phase 3: Convalescent (weeks 4-6)
Your child will begin to recover during the third phase of Kawasaki disease, which is known as the convalescent phase.
In the third phase of the disease, signs and symptoms slowly go away unless complications develop. It may be as long as eight weeks before energy levels seem normal again.
Occasionally, complications can develop during the third phase of Kawasaki disease, but they’re more likely to develop before this stage.
Kawasaki disease diagnosis
There is no specific, single test to diagnose Kawasaki Disease.
Diagnosis is usually based on evaluation of classic symptoms. If Kawasaki disease is suspected, however, your doctor may order tests to monitor heart function (an echocardiogram and electrocardiogram). Other possible diagnostic tests include blood studies (complete blood count and blood sedimentation rate), chest x-ray and urinalysis. In addition, your doctor may refer you to a pediatric specialist in infectious disease, rheumatology or cardiology for assistance in diagnosis and treatment.
Kawasaki disease treatment
Treatment within 10 days of the start of the fever is highly effective in the prevention of coronary artery complications and most children will make a complete recovery without lasting damage. Without treatment, approximately 25% of children will develop some abnormalities of the coronary arteries.
Immediate treatment is critical to avoid permanent damage to the coronary arteries and heart. Standard treatment includes high doses of Intravenous gamma globulin (IVIG). Intravenous gamma globulin (IVIG) contains antibodies from donated blood. It is screened for viruses and bacteria before it is used as a treatment. If you are concerned about this, talk to your doctor.
Intravenous gamma globulin (IVIG) is given through an IV over 8 to 12 hours. Children may be given aspirin, as well, to lower the risk of heart problems. Children stay in the hospital for at least 24 hours after completing the intravenous gamma globulin (IVIG) dose to make sure the fever does not return and other symptoms are improving. The patient’s condition usually greatly improves within 24 hours of treatment.
Additional treatments may be necessary if a child does not respond well to the single dose of IVIG, the fever returns, or there are abnormal findings on the first echocardiogram. Another dose of intravenous gamma globulin (IVIG) or other medications that fight inflammation such as steroids, infliximab, or etanercept may be recommended. Pediatric specialists in rheumatology, infectious disease, or cardiology may be consulted in this situation.
Radiography (x-ray) of the chest may be used to look for changes in the aorta. Angiography or arteriography is used to help determine the location and appearance of vessels affected by the disease.
Most children go home from the hospital after a few days.
Children treated for Kawasaki Disease are sent home from the hospital on a low dose of aspirin to take by mouth every day for 6 to 8 weeks. As they recover, it is not uncommon for these children to be extra tired or seem “off” for several weeks. Rest is very important. Peeling of the hands and feet is expected and is not cause for alarm.
However, see your doctor right away if your child develops a fever or any of Kawasaki Disease’s signs or symptoms return. Further evaluation is needed. Your child may need to be readmitted to the hospital. While it is possible to have Kawasaki disease more than once, it is considered rare. Fewer than 2% of children have recurrences.
Follow-up Care
It is very important to closely monitor children who have had Kawasaki Disease for improvement and to check for the development of coronary aneurysms. Aneurysms most often form after the first couple of weeks of illness. Therefore, children should be scheduled for an echocardiogram and a check-up at 2 weeks and again at 6 to 8 weeks after their fever first started. More frequent follow up and echocardiograms will be necessary if there are abnormal findings on any of the echocardiograms.
Some children may experience joint pain, sensitivity to light or other eye concerns which are less common and usually resolved prior to discharge from the hospital. However, children with these concerns may be referred to rheumatology and ophthalmology for further assessment and management.
Note: Live viral vaccines should be postponed at least 11 months after intravenous gamma globulin (IVIG), because intravenous gamma globulin (IVIG) may render the vaccines in-effective. This includes the MMR (measles, mumps, rubella) and the Varicella (chicken pox) vaccines. Children over 6 months of age should receive the inactivated influenza (flu) vaccine injection.
Long-term follow-up
Children treated for Kawasaki Disease who do not develop aneurysms have an excellent long-term outcome.
If your child did not have any coronary artery abnormalities or had minor dilation that went away quickly, usually no further follow-up is required. However, it is important for them to follow a heart healthy diet and lifestyle. Cholesterol levels should be checked every 5 years.
At this time, it is not known if children with Kawasaki disease and normal echocardiograms are more likely to develop heart problems when they are adults, although it is very unlikely. All children should follow a healthy lifestyle, but it may be even more important in children who have had Kawasaki disease. A healthy lifestyle includes: making healthy food choices, no sugary drinks, putting limits on screen time, taking part in activities and exercise that your child enjoys every day, and avoiding known risk factors for heart disease, such as smoking.
Children who do have coronary aneurysms should be under the care of a pediatric cardiologist as they grow and will require special long-term care and follow-up.
Monitoring heart problems
If your child has any indication of heart problems, the doctor may recommend follow-up tests to monitor heart health at regular intervals, often at six to eight weeks after the illness began, and then again after six months.
If your child develops continuing heart problems, the doctor may refer you to a doctor who specializes in treating heart disease in children (pediatric cardiologist). In some cases, a child with a coronary artery aneurysm may require:
- Anticoagulant drugs. These medications — such as aspirin, clopidogrel (Plavix), warfarin (Coumadin, Jantoven) and heparin — help prevent clots from forming.
- Coronary artery angioplasty. This procedure opens arteries that have narrowed to the point that they impede blood flow to the heart.
- Stent placement. This procedure involves implanting a device in the clogged artery to help prop it open and decrease the chance of another blockage. Stent placement may accompany angioplasty.
- Coronary artery bypass graft. This operation involves rerouting the blood around a diseased coronary artery by grafting a section of blood vessel from the leg, chest or arm to use as the alternate route.
- Taubert KA, Rowley AH, Shulman ST. Seven-year national survey of Kawasaki disease and acute rheumatic fever. Pediatr Infect Dis J 1994;13:704-8. https://www.ncbi.nlm.nih.gov/pubmed/7970970[↩]
- Yanagawa H, Nakamura Y, Yashiro M, Ojima T, Tanihara S, Oki I, et al. Results of the nationwide epidemiologic survey of Kawasaki disease in 1995 and 1996 in Japan. Pediatrics 1998;102:e65.[↩]
- Kawasaki Disease in Infants & Young Children. https://www.healthychildren.org/English/health-issues/conditions/heart/Pages/Kawasaki-Disease.aspx[↩]
- Yanagawa H, Yashiro M, Nakamura Y, Kawasaki T, Kato H. Results of 12 nationwide epidemiological incidence surveys of Kawasaki disease in Japan. Arch Pediatr Adolesc Med 1995;149:779-83. https://www.ncbi.nlm.nih.gov/pubmed/7795769[↩]
- Recognition and management of Kawasaki disease. Ra K. Han, Brian Sinclair, Alice Newman, Earl D. Silverman, Gregory W. Taylor, Peter Walsh, Brian W. McCrindle. CMAJ Mar 2000, 162 (6) 807-812; http://www.cmaj.ca/content/162/6/807[↩][↩]
- Dajani AS, Taubert KA, Gerber MA, Shulman ST, Ferrieri P, Freed M, et al. Diagnosis and therapy of Kawasaki disease in children. Circulation 1993;87:1776-80. http://circ.ahajournals.org/content/87/5/1776[↩]
- Momenah T, Sanatani S, Potts J, Sandor GGS, Human DG, Patterson MWH. Kawasaki disease in the older child. Pediatrics 1998;102:e7.[↩]





{kind=link}