Contents
- What is keratitis
- What is the cornea
- Bacterial keratitis
- Fungal keratitis
- Herpes keratitis
- Acanthamoeba keratitis
- Ulcerative keratitis
- Superficial punctate keratitis
- Staph marginal keratitis
- How To Prevent Eye and Corneal Infection With Proper Contact Lens Care
- Keratitis symptoms
- Keratitis causes
- Keratitis complications
- Keratitis diagnosis
- Keratitis treatment
What is keratitis
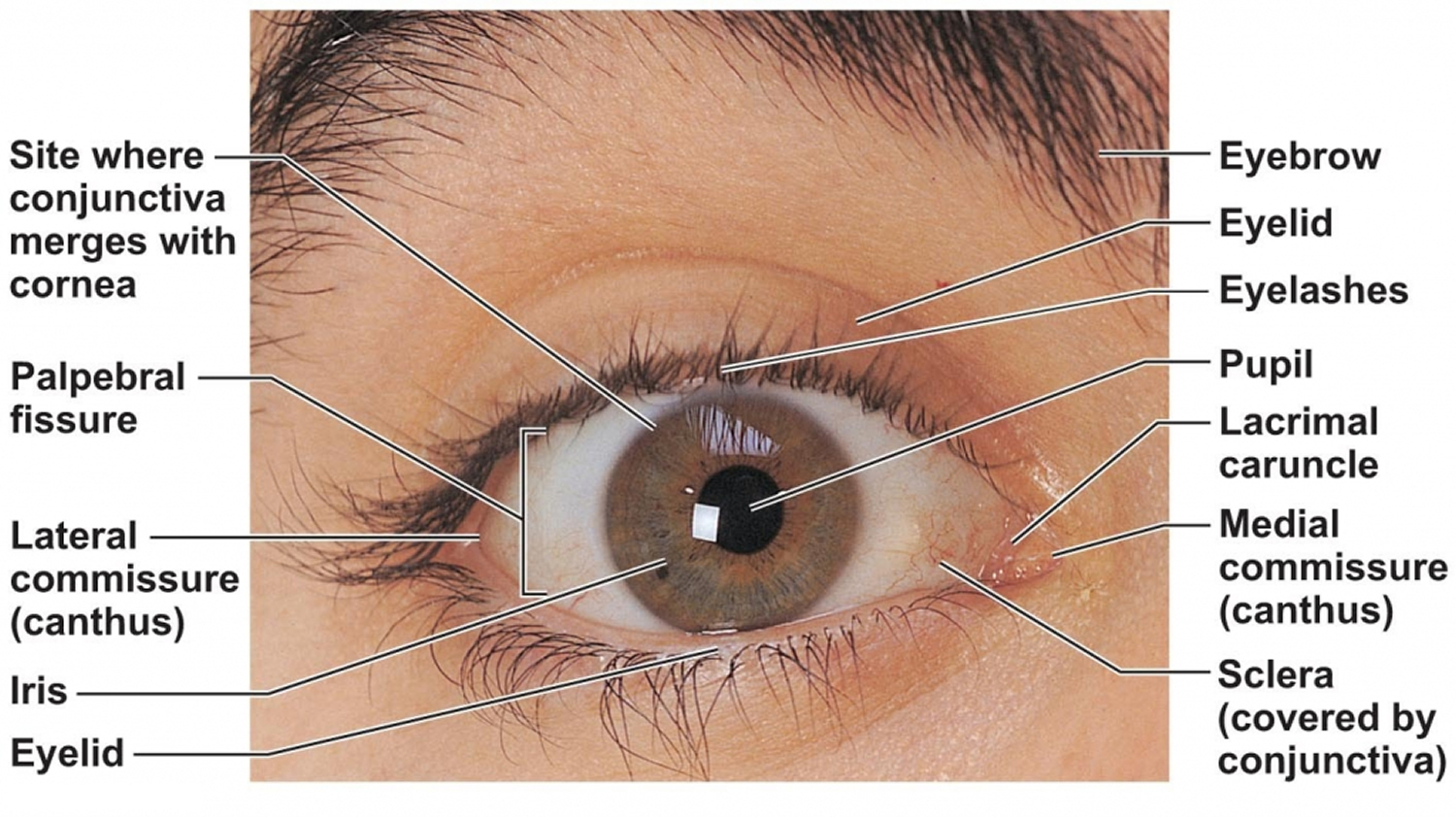
Keratitis is an infection or inflammation of the cornea. The cornea is the clear, dome-shaped window of the front of your eye (Figures 1 and 2).
In general, keratitis could be infective and noninfective. Differentiating between them is crucial in managing both. Careful clinical examination, aided by laboratory investigations, could help in correct diagnosis and proper management.
Even though both conditions may involve all age groups, infective keratitis occurs more frequently in children and adults. To describe precisely the ocular features of these conditions, the clinician must be well trained in slit-lamp biomicroscopy. Other magnifiers like loupes and spectacles may not reveal the depth of the lesion and other associated clinical signs.
Infective and noninfective keratitis may overlap each other. Noninfective keratitis may become infective by pathogenic or nonpathogenic microbes and may result in sight-threatening complications. Infective keratitis could also be suppurative and nonsuppurative. Suppurative keratitis is frequently caused by bacteria and fungi. Nonsuppurative infective keratitis could be viral, spirochaetal, parasitic or immune-related stromal necrosis.
Infective nonsuppurative keratitis
Frequently seen a few decades ago, it is rarely seen now (e.g., interstitial keratitis due to tuberculosis, leprosy and syphilis). Often they are insidious, chronic and bilateral. There may be obvious associated signs and symptoms of systemic disease. Diagnosis is often clinical, but the laboratory investigations to rule out or confirm tuberculosis, leprosy and syphilis may provide more information to clinch the diagnosis.
The causative agents of infective keratitis frequently isolated in India are 1:
- Bacteria: Gram-positive cocci and Gram-negative bacilli
- Fungi: Filamentous fungi
- Viral: Herpes simplex virus
- Parasite: Acanthamoeba species
Non-infective keratitis
The more common entities of noninfective keratitis are 2:
- Peripheral ulcerative keratitis (PUK) due to auto-immune diseases
- Phlyctenular keratitis
- Vernal ulcer or shield ulcer
- Staphylococcal marginal keratitis
- Contact lens-related sterile infiltrates
- Meta herpetic ulcer
Peripheral ulcerative keratitis (see Figure 9 below) is rare and diagnosis is often by exclusion. Mooren ulcer , senile marginal degeneration, sclerokeratitis and peripheral corneal melt of rheumatoid origin are some of the few to think about, when the clinician encounters a nonhealing peripheral corneal ulcer. All these are progressive with remissions and relapses. Confirmation of diagnosis may warrant a battery of immunological and bio-chemical investigations like IgM rheumatoid factor, c-ANCA, p-ANCA, circulating antibodies, such as ANA, anti-DNA and anti-SM; which could narrow down the spectrum of etiology.
Vernal keratitis or vernal ulcer is not uncommon. The diagnosis is confirmed by the presence of papillae on the tarsal conjunctiva of the upper lid and Tranta′s dots at limbus or pigmentation involving bulbar conjunctiva. It is mostly seen in children and adolescents with the classic symptom of itching. Vernal ulcer is usually unilateral and involves the superior 1/3rd of the cornea. In a few patients, it may lead to plaque formation and the shield ulcer is graded according to the density of the plaque (Figure 1) 3.
Figure 1. Vernal keratitis (shield ulcer with plaque)

Phlyctenular keratitis is often noticed in children with a history of recurrent attacks; lesion may show superficial vascularization like pannus or leash of vessels with scarring due to previous attacks. Even though tuberculosis etiology was attributed often, other micro-organisms like staphylococcus and candida can also cause similar lesions 4. Phlyctenular keratitis represents type IV hypersensitivity response.
Noninfectious keratitis can be caused by a minor injury or from wearing contact lenses too long. Infection is the most common cause of keratitis. Infectious keratitis can be caused by bacteria, viruses, fungi or parasites. Often, these infections are also related to contact lens wear, especially improper cleaning of contact lenses or overuse of old contact lenses that should be discarded.
Superficial keratitis involves the outer layers of the cornea. After this form of keratitis heals, there is usually no scar on the cornea.
Deep keratitis affects deeper layers of the cornea. There can be a scar on the cornea after it heals, which may or may not affect your vision. This will depend on the location of the scar.
Other types of keratitis:
- Amoebic keratitis, which is an infection with amoeba. It is often caused by Acanthamoeba and usually affects contact lens wearers.
- Bacterial keratitis, which is an infection with bacteria
- Fungal keratitis, which is an infection with fungus
- Herpes keratitis, which is an infection with herpes simplex or herpes zoster viruses
- Photokeratitis, due to intense ultraviolet (UV) radiation exposure. Examples include snow blindness or welder’s arc eye.
What is the cornea
The cornea is the eye’s outermost layer. It is the clear, domeshaped surface that covers the front of the eye. It plays an important role in focusing your vision.
Although the cornea is clear and seems to lack substance, it is actually a highly organized group of cells and proteins. Unlike most tissues in the body, the cornea contains no blood vessels to nourish or protect it against infection. Instead, the cornea receives its nourishment from the tears and aqueous humor (a fluid in the anterior portion of the eye) that fills the chamber behind it. The cornea must remain transparent to refract light properly, and the presence of even the tiniest blood vessels can interfere with this process. To see well, all layers of the cornea must be free of any cloudy or opaque areas.
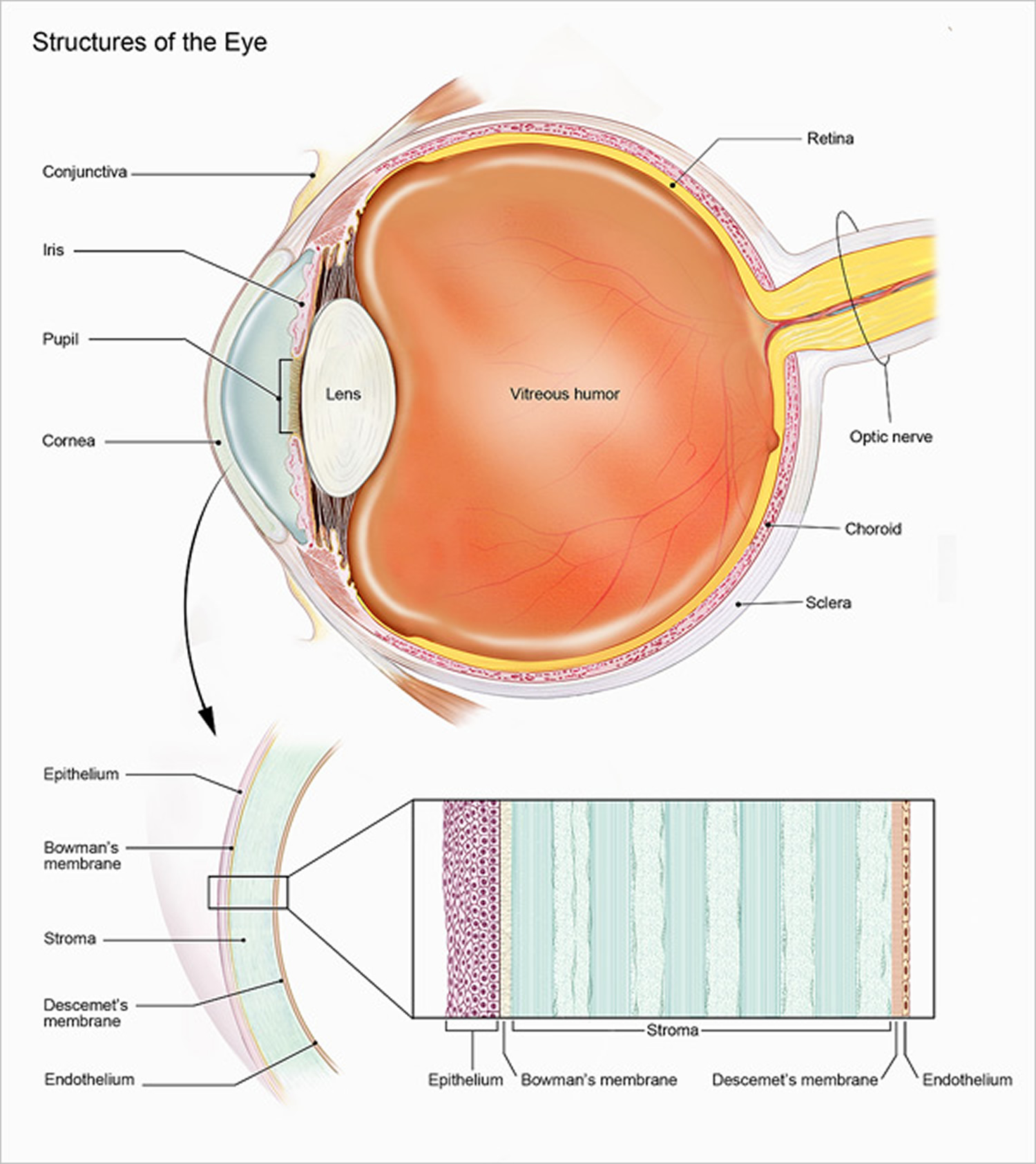
The corneal tissue is arranged in five basic layers, each having an important function.
These five layers are:
Epithelium
The epithelium is the cornea’s outermost layer. Its primary functions are to:
- block the passage into the eye of foreign material, such as dust, water, and bacteria; and
- provide a smooth surface to absorb oxygen and nutrients from tears, which are then distributed to the other layers of the cornea.
The epithelium is filled with thousands of tiny nerve endings, which is why your eye may hurt when it is rubbed or scratched. The part of the epithelium that epithelial cells anchor and organize themselves to is called the basement membrane.
Bowman’s membrane
The next layer behind the basement membrane of the epithelium is a transparent film of tissue called Bowman’s layer, composed of protein fibers called collagen. If injured, Bowman’s layer can form a scar as it heals. If these scars are large and centrally located, they may cause vision loss.
Stroma
Behind Bowman’s layer is the stroma, which is the thickest layer of the cornea. It is composed primarily of water and collagen. Collagen gives the cornea its strength, elasticity, and form. The unique shape, arrangement, and spacing of collagen proteins are essential in producing the cornea’s light-conducting transparency.
Descemet’s Membrane
Behind the stroma is Descemet’s membrane, a thin but strong film of tissue that serves as a protective barrier against infection and injuries. Descemet’s membrane is composed of collagen fibers that are different from those of the stroma, and are made by cells in the endothelial layer of the cornea (see above). Descemet’s membrane repairs itself easily after injury.
Endothelium
The endothelium is the thin, innermost layer of the cornea. Endothelial cells are important in keeping the cornea clear. Normally, fluid leaks slowly from inside the eye into the stroma. The endothelium’s primary task is to pump this excess fluid out of the stroma. Without this pumping action, the stroma would swell with water and become thick and opaque.
In a healthy eye, a perfect balance is maintained between the fluid moving into the cornea and the fluid pumping out of the cornea. Unlike the cells in Descemet’s membrane, endothelial cells that have been destroyed by disease or trauma are not repaired or replaced by the body.
Figure 2. Human eye
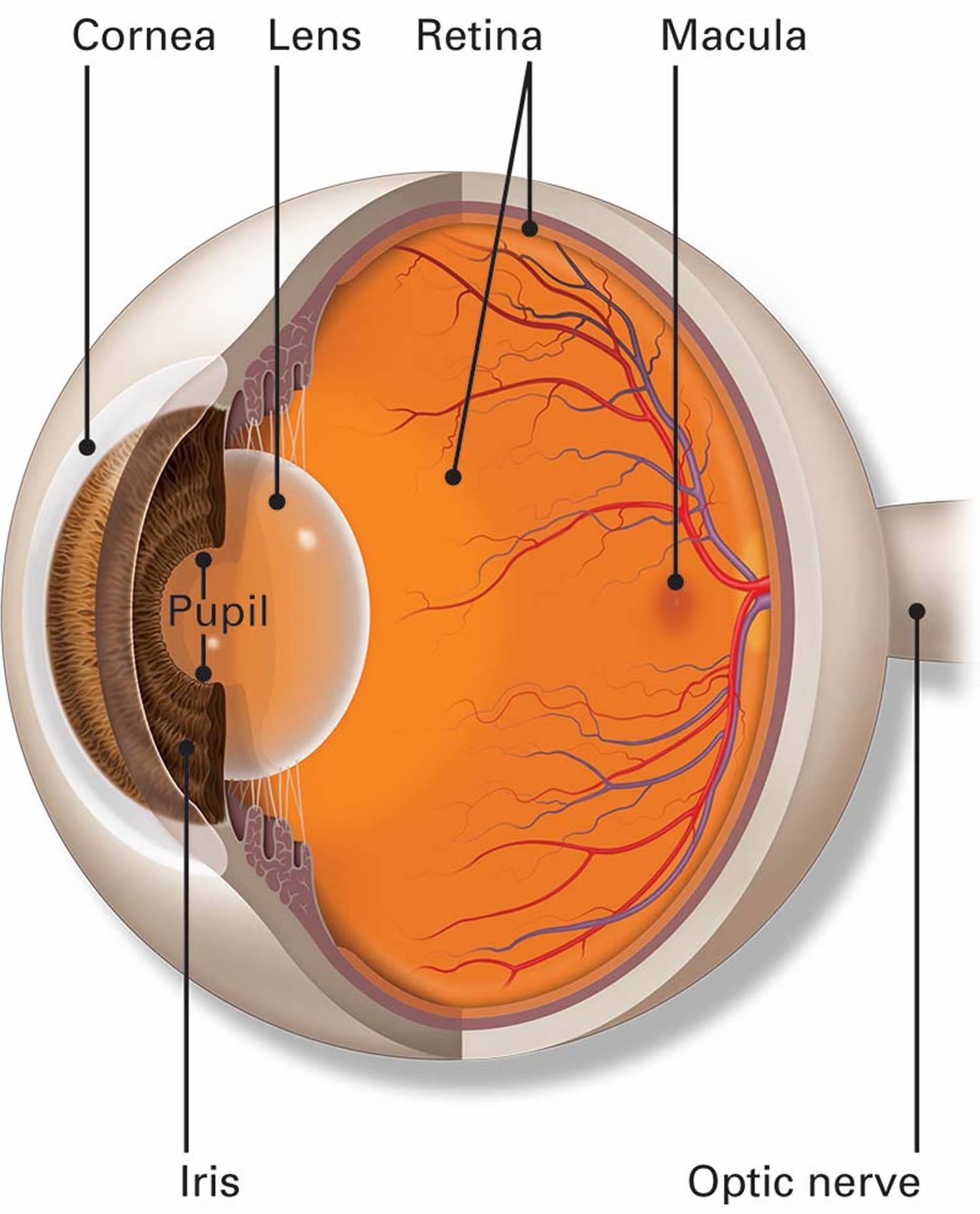
The cornea
Bacterial keratitis
Bacterial keratitis is a bacterial infection of the cornea. Bacterial keratitis usually develops quickly. Left untreated it can cause blindness.
All over the world, bacterial keratitis is more common than fungal keratitis, but this does not hold true for India and other tropical countries 5.
There are many different bacteria that cause keratitis.
The two bacteria most commonly responsible for this type of infection in the U.S. are:
- Staphylococcus aureus
- Pseudomonas aeruginosa
The two main causes of bacterial keratitis are:
- contact lens use, especially extended-wear lenses
- eye injury
You risk an infection from contact lenses if you wear them too long or do not take care of them correctly. Proper care of your contacts will lower your risk of developing a keratitis infection.
Figure 3. Bacterial keratitis

Bacterial keratitis symptoms
Symptoms of bacterial keratitis may include:
- pain in the eye (often sudden)
- reduced vision
- increased light sensitivity
- excessive tearing
- discharge from your eye
See your ophthalmologist right away if you have any of these symptoms. This is especially important if they come on suddenly. If not treated, a bacterial keratitis eye infection can lead to blindness. Treatment must start right away to prevent vision loss.
To diagnose bacterial keratitis, your ophthalmologist will discuss your symptoms with you. They may gently scrape the eye to take a small sample and test it for infection.
Bacterial keratitis treatment
Bacterial keratitis is usually treated with antibiotic drops. Drops are usually put in frequently. Treatment may also involve steroid drops. You may need to return to your ophthalmologist several times.
If you and your ophthalmologist find and treat bacterial keratitis early, you may preserve your vision. In severe cases decreased vision or blindness may be the result. This is also true if the infection affects the center of the cornea. Sometimes a cornea transplant is needed to restore vision.
Fungal keratitis
Fungal keratitis is an infection of the cornea. The cornea is the clear, dome-shaped window of the front of your eye and focuses light into your eye. Fungal keratitis can develop quickly from an eye injury or contact lens use. It can cause blindness if it is not treated. In some cases, treatment cannot restore vision. In these cases, permanent vision impairment or blindness may occur.
There are many different fungi that can infect the cornea such as Fusarium, Aspergillus or Candida 6. Fusaria (singular Fusarium) are common fungi found in soil, water, and plants throughout the world. They are particularly common in warmer climates.
In some countries such as India and Nepal, fungal keratitis are the majority of microbial keratitis 7. In 21% of the patients with fungal keratitis, contact lens wear has been documented 8; whereas this rate was reported to be 10% elsewhere 9. Fungal pathogens have been found in up to 4.8% of contact lens associated keratitis 10.
A worldwide outbreak of fungal keratitis in 2006 has been associated with the solution, ReNuMoistureLoc 11. The rate of fusarium keratitis decreased after recall of this product; however, an increased number of contact lens-related fungal keratitis has been reported in 2007 & 2008, as demonstrated in 78 eyes of fungal keratitis collected from 1999 to 2008 12.
Risk factors for fungal keratitis
Contact lens wear was the leading risk factor for the fungal keratitis, particularly those caused by yeast-like fungi 13. Moreover, extended wear schedules increase this risk 8. Indeed, the risk is highest in extended wear of hydrogel lenses compared with silicone hydrogel, while rigid gas permeable contact lenses have the lowest risk. Other risk factors include trauma specially with vegetative material, topical steroids and underlying systemic diseases 14.
Fungal keratitis can happen after an injury to the cornea involving plant material. One example is getting hit in the eye with a palm branch.
People who have a low immune response can also get fungal keratitis if they come in contact with the fungus. There is also a risk of developing fungal keratitis with contact lens use. Proper use and care of contact lenses can reduce your risk of getting a fungal infection if you wear contacts. Ask your ophthalmologist about proper contact lens care.
Figure 4. Fungal keratitis (early)
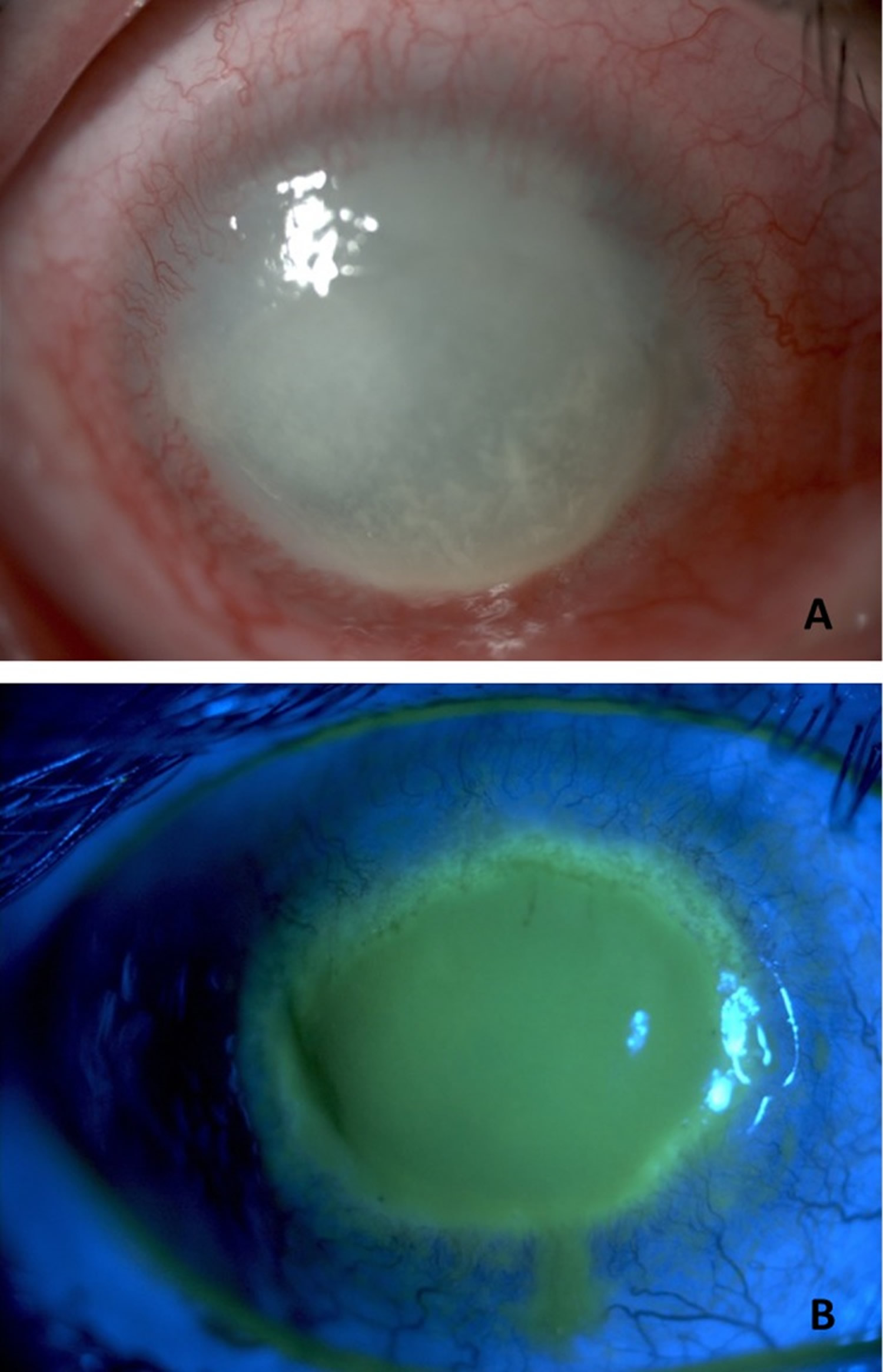
Figure 5. Fungal keratitis


Note: (A) Fusarium keratitis showing neither a ring infiltrate nor a raised lesion. (B) Aspergillus flavus keratitis showing a ring infiltrate and feathery borders. (C) Dematiaceous fungal keratitis showing macroscopic pigmentation and a raised lesion.
Fungal keratitis symptoms
Symptoms of fungal keratitis may include:
- reduced vision
- pain in the eye (often sudden)
- increased light sensitivity
- tearing
- excessive tearing or discharge from your eye
See your ophthalmologist right away if you experience any of these symptoms. This is especially important if these symptoms come on suddenly. You must start treatment right away to prevent possible blindness.
Fungal keratitis treatment
Your ophthalmologist may gently scrape the eye to take a small sample of material. They will test the sample for infection. This test will help diagnose whether your infection is fungal keratitis or bacterial keratitis.
Treatment of fungal keratitis usually includes antifungal eye drops and oral medications. If these medicines are not effective, you may need surgery, including corneal transplantation. In some cases, even corneal surgery will not restore vision. In these cases, permanent vision impairment or blindness may occur. That is why it is so important to see your ophthalmologist at the first sign of any ocular infection.
Exchanging the lens with a more oxygen-permeable contact lens, changing wearing schedule from extended wear to daily wear, switching to rigid gas permeable lenses instead of soft lenses, and discontinuing contact lenses in cases of active progressive corneal new vessels are recommended 15. Anti-angiogenic therapy of the cornea (subconjunctival or intrastromal), as well as corticosteroids and non-steroidal anti-inflammatory agents, can help in cases with active neovascularizations that may endanger the survival of corneal graft or ocular surface health 16. Laser photocoagulation of new vessels, photodynamic therapy, electrocoagulation, and stem cell transplant are surgical interventions recommended in severe cases 17.
Herpes keratitis
Herpes keratitis is a viral infection of the eye caused by the herpes simplex virus (HSV). There are two major types of the herpes simplex virus:
- Type I herpes simplex virus is the most common and primarily infects the face, causing the familiar “cold sore” or “fever blister.”
- Type II herpes simplex virus is the sexually transmitted form of herpes, infecting the genitals.
While both Type I and Type II herpes can spread to the eye and cause infection, Type I herpes simplex virus is by far the most frequent cause of eye infections. Infection can be transferred to the eye by touching an active lesion (a cold sore or blister) and then your eye.
Type I herpes is very contagious and is commonly transmitted by skin contact with someone who has the virus. Almost everyone — about 90 percent of the population — is exposed to Type I herpes, usually during childhood.
Herpes simplex virus (HSV) causes a spectrum of ocular diseases, but most prominent among them are epithelial and stromal keratitis. Recurrence in the same eye is the hallmark of this common viral infection involving the human cornea.
After the original infection, the virus lies in a dormant state, living in nerve cells of the skin or eye. Reactivation can be triggered in a number of ways, including:
- stress
- sun exposure
- fever
- trauma to the body (such as injury or surgery)
- menstruation
- certain medications
Once herpes simplex is present in the eye, it typically infects the eyelids, conjunctiva and cornea. It may also infect the inside of the eye; however, this is much less common.
Herpes zoster opthalmicus
Fifty to 72% of patients with periocular zoster will have ocular involvement. The frontal branch of the trigeminal nerve is by far the most frequently involved nerve.13 Involvement of the nasociliary branch can often herald ophthalmic involvement due to its innervation to the eye. The classic Hutchinson′s sign (eruptions on the side of the tip of the nose) is evidence of nasociliary involvement and has 85% reliability that the eye will be involved 18. Herpes zoster begins with a prodrome of severe one-sided headache, malaise, fever and chills, followed by erythema and papules in 2 or 3 days. Occasionally, zoster may develop without vesicles and rarely can affect both sides of the ophthalmic division 2. Previous attack of chickenpox may be present. When a young patient gets zoster, one should always rule out HIV infection or other immune-compromised diseases.
Figure 6. Herpes keratitis

Note: Slit lamp photograph of a patient with herpes stromal keratitis demonstrating opacity and neovascularization of the cornea.
Herpes keratitis symptoms
The symptoms of herpes keratitis may include pain, redness, blurred vision, tearing, discharge and sensitivity to light.
If the infection is superficial, involving only the cornea’s outer layer (called the epithelium), it will usually heal without scarring. However, it if involves the deeper layers of cornea (which can happen after time), the infection may lead to scarring of the cornea, loss of vision and sometimes even blindness.
Left untreated, herpes keratitis can severely damage your eye.
Herpes keratitis treatment
Treatment of herpes keratitis depends on its severity. Mild infection is typically treated with topical and sometimes oral antiviral medication. Your ophthalmologist may gently scrape the affected area of the cornea to remove the diseased cells. In case of severe scarring and vision loss, a corneal transplant may be required.
It is very important to consult an ophthalmologist before beginning any treatment, because some medications or eyedrops may actually make the infection worse.
There is no complete cure for herpes; once the virus is in the body, you cannot get rid of it. However, if you develop herpes keratitis, there are some things you can do to help prevent recurring outbreaks:
- If you have an active cold sore or blister, avoid touching your eyes.
- Steroids can increase the herpes virus in the body. You should not use steroid eye drops unless you are taking an anti-viral medicine as well.
- Stop wearing contact lenses if you keep getting infections.
- See an ophthalmologist immediately if symptoms of ocular herpes return.
Acanthamoeba keratitis
Acanthamoeba keratitis is a sight-threatening infection of the cornea cause by free-living amoebae of the genus Acanthamoeba 19. Acanthamoeba are ubiquitous microorganisms and are considered opportunistic pathogens in humans 20. Interestingly, acanthamoeba keratitis is increasingly being recognized as a severe sight-threatening ocular infection, worldwide. Although contact lens wear is the leading risk factor for acanthamoeba keratitis, Acanthamoeba species can cause infection in non-contact lens wearers. Patients with acanthamoeba keratitis may experience pain with photophobia, ring-like stromal infiltrate, epithelial defect and lid oedema. If acanthamoeba keratitis is not treated adequately and aggressively, it can lead to loss of vision. In India and most developing countries where contact lenses are not popular, trauma is the most common predisposing factor and patients of acanthamoeba keratitis suffer from prolonged and significant morbidity from delay in diagnosis due to lack of awareness and misunderstanding about clinical signs and symptoms among physicians and non-availability of anti-Acanthamoeba drugs 20.
In the United States, an estimated 85% of acanthamoeba keratitis cases are related to contact lenses. In developed countries, the incidence of acanthamoeba keratitis is about 1–33 cases per million contact lens wearers 21. Indeed, almost 80% of acanthamoeba keratitis cases are associated with soft contact lenses. Although only 12% of acanthamoeba keratitis cases have been attributed to rigid gas permeable lenses, at least a part of this difference might be related to lower prevalence of rigid gas permeable lens use compared with soft lenses 22. However, these figures should not encourage rigid gas permeable wearers to be less obsessed with their lens care.
Risk factors for acanthamoeba keratitis
Contact lens wear is the main risk factor for acanthamoeba keratitis, which should be considered in any suspicious keratitis in contact lens wearers. Patients with acanthamoeba keratitis can presumably experience pain associated with photophobia, ring-like stromal infiltrate, epithelial defect, radial perineuritis, and lid edema 22. The clinical picture varies at different stages of the disease and the classical ring-shaped infiltration is seen in advanced stages. Diagnosis of acanthamoeba keratitis requires confocal scan of the cornea or special culture and staining techniques. Delayed diagnosis results in deeper invasion, lower response to treatment, and poorer visual outcomes 23. Usually, singular amoebae gain access to the lens case through tap water or air, swiftly grow to high densities in the lens if the case is not cleaned correctly and regularly, and subsequently attach to the lens and infect the eye. Wearers of soft contact lenses who use multipurpose solutions are at greater risks given that acanthamoeba sticks particularly well to the hydrophilic plastic of these lenses 22. Additionally, soft lenses are the most commonly used, also by occasional wearers (e.g., once a week for sport) or cosmetic colored lenses for social events. Indeed, these patterns are risk factors for poor compliance to lens care 24.
For prophylaxis of any kind of infectious keratitis including acanthamoeba keratitis, the use of tap water is forbidden, the lens case should be cleaned with hand rubbing and subsequently air dried, contact lenses should be cleaned and kept by using a proper cleaning method, and the lens cases must be exchanged at least every three months (preferably monthly) 25. Many multipurpose solutions have added anti-acanthamoeba agents such as polyhexamethylenebiguanide (PHMB), though their effectiveness in the clinical setting needs to be documented. The best method of disinfection remains the two-step hydrogen peroxide systems. Moreover, heat disinfection is highly effective in eradication of the acanthamoeba parasite 26.
Figure 7. Acanthamoeba keratitis
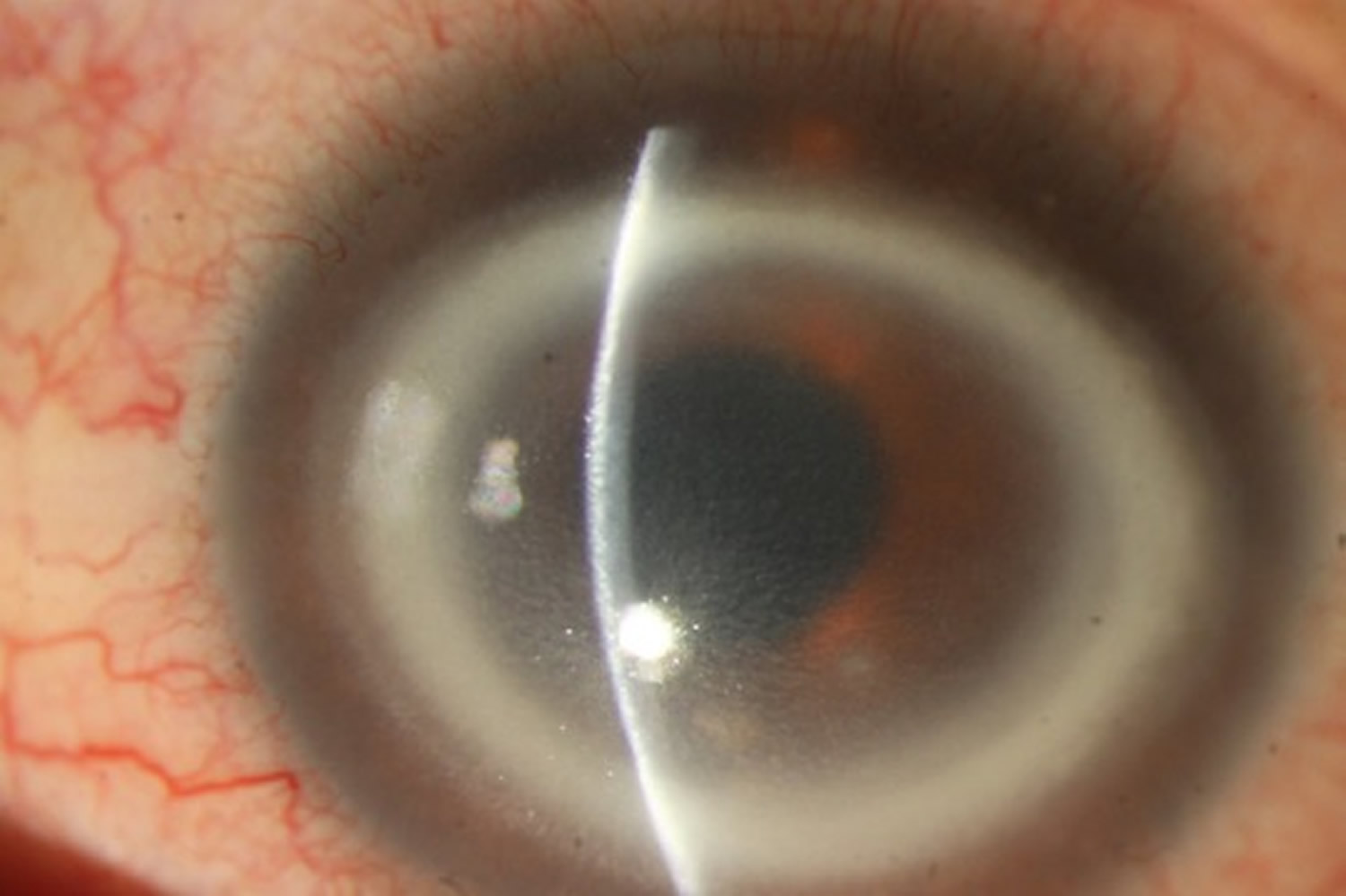

Figure 8. Acanthamoeba keratitis
Note: (A) Corneal melting and vascularization in a patient with Acanthamoeba keratitis. (B) Observed corneal damage in Acanthamoeba keratitis is shown after sodium fluorescein application.
Acanthamoeba keratitis treatment
In the case of suspicious acanthamoeba keratitis based on the clinical setting, confocal corneal scan and appropriate culture media (e.g., non-nutrient agar with bacterial overlay or buffered charcoal-yeast extract agar) and staining methods (e.g., acridine orange, calcofluor white, or indirect immunofluorescence antibody) are recommended. Currently, acanthamoeba keratitis treatment is based on topical antimicrobial agents that can accomplish high concentrations at the infection site 25. Considering the presence of a cyst form in acanthamoeba, which is totally resistant to therapy, a combined therapy is advisable 27. Chlorhexidine and PHMB (polyhexamethylene biguanide) are considered the most effective drugs for treating acanthamoeba keratitis infections; especially when combined, they are effective against both cysts and trophozoites 28. Most of the currently used topical agents are effective against trophozoites and cysts of Acanthamoeba such as biguanides, (i) PHMB (polyhexamethylene biguanide), which is effective at low concentrations (0.02%), but is unfortunately toxic to human corneal cells 29, and (ii) chlorhexidine, which is effective against both amoebic forms, and at minimal concentrations is not toxic to corneal epithelial cells 29. Chlorhexidine 0.02% is often used in combination with aromatic diamidines such as 0.1% propamidine isethionate Brolene® (Sanofi, UK), 0.15% dibromopropamidine, hexamidine 0.1% Desomedine© (Chauvin, France) and neomycin, showing good results if the treatment is applied early in the development of the infection 29. Other medications such as neomycin, paromomycin, voriconazole, miconazole, and imidazoles/triazoles family drugs are also effective against acanthamoeba. Failure to response to medical treatment necessitates surgical interventions such as corneal graft.
Ulcerative keratitis
Peripheral ulcerative keratitis is type of crescent-shaped inflammatory damage that occurs in the limbal region of the cornea. Peripheral ulcerative keratitis is always combined with an epithelial defect and the destruction of the peripheral corneal stroma. Peripheral ulcerative keratitis may have a connection to systemic conditions, such as long-standing rheumatoid arthritis (RA), systemic lupus erythematosus (SLE), granulomatosis with polyangiitis (formerly known as Wegener’s granulomatosis), relapsing polychondritis, classic polyarteritis nodosa and its variants, microscopic polyangiitis, and Churg-Strauss syndrome. However, the most common connection is with rheumatoid arthritis (RA).
Differentiating peripheral ulcerative keratitis from other infective peripheral corneal lesions is mostly based on clinical diagnosis. Mooren ulcer will have a typical lesion in the interpalpebral area, peripheral gutter with edematous or necrotic over-hanging edges [Fig. 4]. Sclera is not involved, which aids in differentiating from rheumatoid and other autoimmune diseases. In 35-40% of patients, Mooren ulcer is bilateral and the reported risk factors are corneal surgery, corneal trauma and hookworm infestation. Natural evolution of Mooren ulcer could be either perforation or conjunctivilization of Descemet′s bed resulting in blindness. Mooren ulcer could occur in any sex and age group.5
Figure 9. Peripheral ulcerative keratitis with Mooren ulcer
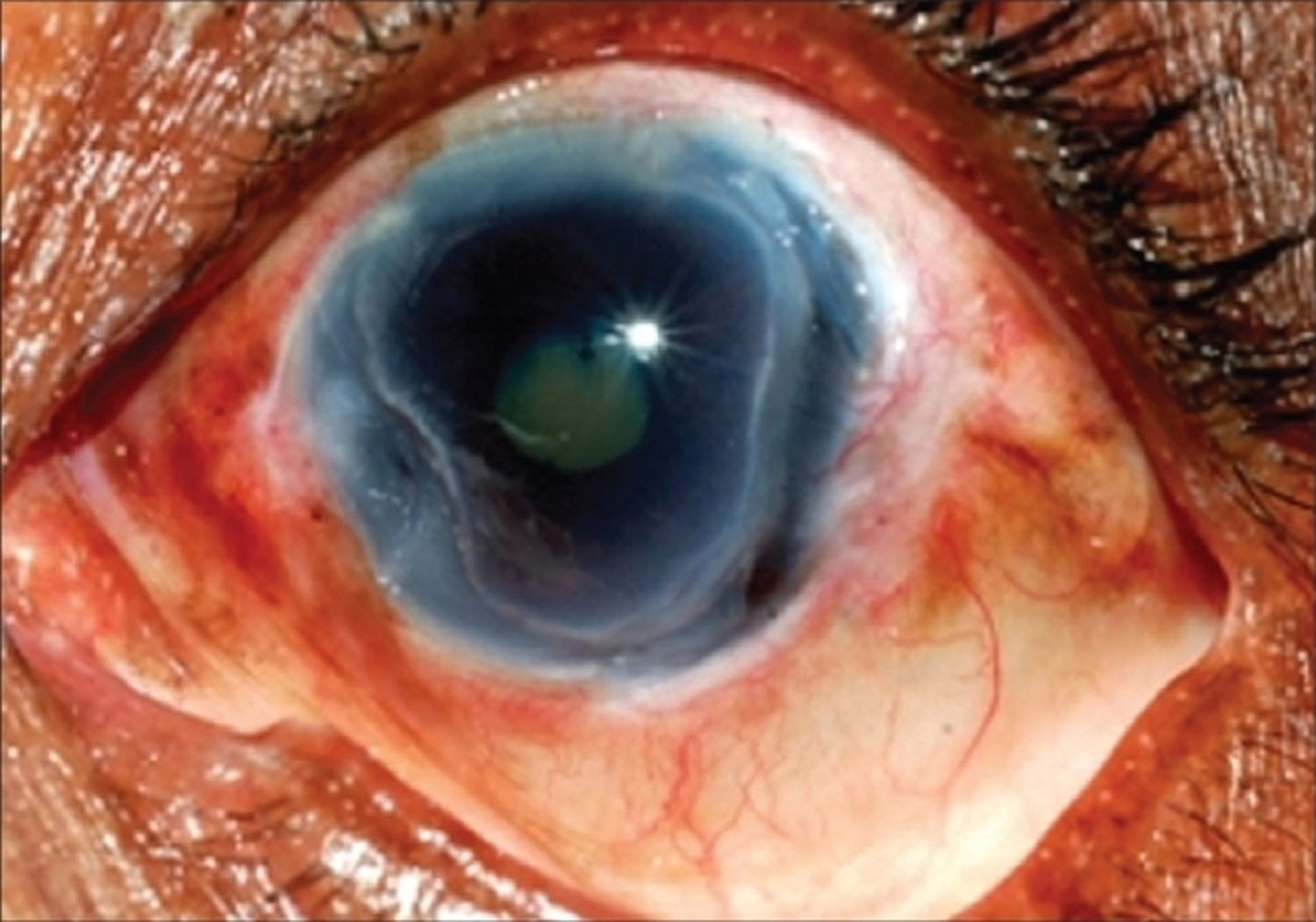
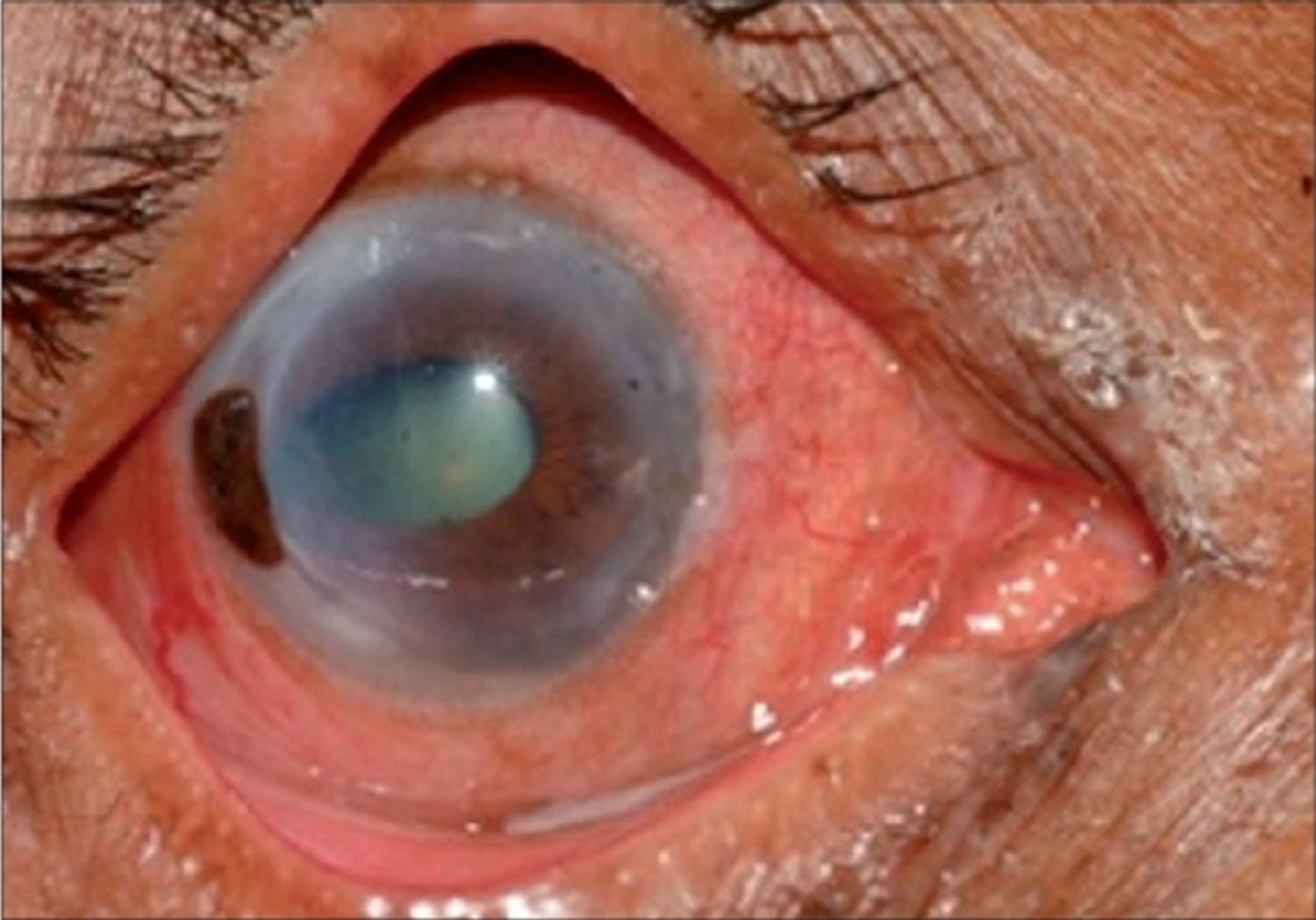
Figure 10. Peripheral ulcerative keratitis – Mooren ulcer with perforation
Autoimmune diseases are systemic inflammatory diseases that generally involve most of the organs in the body, such as the synovium of the diarthrodial joints. Rheumatoid arthritis (RA) and systemic lupus erythematosus (SLE) are the most common autoimmune diseases.
According to an investigation, peripheral ulcerative keratitis was the second most common ocular complication of autoimmune diseases compared with anterior uveitis, which ranks first place. In a previous study, among the three most frequent underlying diseases, rheumatoid arthritis occupied 34–42% of samples with peripheral ulcerative keratitis. Systemic lupus erythematosus (SLE) and granulomatosis with polyangiitis (formerly known as Wegener’s granulomatosis) are on its heels 30.
The eye, especially the ocular surface, is frequently invaded by autoimmune diseases. In some cases, it may be the first sign of the disease 31. In addition to corneal damage, which is a rare and late manifestation, other common ocular manifestations are keratoconjunctivitis sicca (dry eye disease), episcleritis, scleritis, uveitis, and retinal vasculitis 32. The most frequent ocular manifestation of autoimmune diseases is dry eye disease (keratoconjunctivitis sicca) 33. However, the most destructive and severe ophthalmological manifestation of autoimmune diseases is peripheral ulcerative keratitis (peripheral ulcerative keratitis) 32.
The clinical manifestations of peripheral ulcerative keratitis include ocular irritation, pain, redness, photophobia, and corneal opacity. One serious complication of peripheral ulcerative keratitis that is associated with rheumatoid arthritis (RA) and other autoimmune diseases is corneal perforation and loss of vision 34. The ulceration may occur in either central or paracentral regions 32. Due to the peculiarity of the peripheral cornea, it is well vascularized and available for the deposition of circulating immune complexes via the capillary network, and the pathological manifestations are more likely to be present in the periphery. Corneal extracellular stroma is composed of highly organized lamellae of collagen fibrils embedded in a framework of glycosaminoglycans 35. Fibrocytes and macrophages express human leukocyte antigen DR (HLA-DR) in the corneal matrix, facilitating the direct antigenic stimulation and/or production of local inflammatory mediators 36. Research suggests that both humoral and cellular immunity are associated with the pathogenesis of autoimmune systemic diseases 37. A common and recommended therapeutic method for autoimmune disease patients with peripheral ulcerative keratitis is systemic medicine, including nonsteroidal anti-inflammatory drugs (NSAIDS), corticosteroids, systemic immunosuppressive chemotherapy 38, and surgical therapy. Recently, biological therapy has become a novel therapeutic method.
Ulcerative keratitis treatment
Topical Treatment
Patients who suffer from granulomatosis with polyangiitis (formerly known as Wegener’s granulomatosis) combined with peripheral ulcerative keratitis are not sensitive to local corticosteroid therapy unless a subsequent systemic immunosuppressive therapy is used 39.
Surgical Treatment
Traditional therapy may fail to heal intractable granulomatosis with polyangiitis (formerly known as Wegener’s granulomatosis). According to a study by Lu et at. 40, the combination of conjunctivectomy with cryotherapy is effective. The main theory is that necrotic tissue, immune complexes, inflammatory cells, and protein lysozymes are affected. Corneal perforation is a serious complication of peripheral ulcerative keratitis in granulomatosis with polyangiitis (formerly known as Wegener’s granulomatosis). Surgical reinforcement is necessary for treatment 41.
Systemic Treatment
Both oral and intravenous cyclophosphamide, in combination with corticosteroids, are good choices for patients with this disease. Cyclophosphamide 2 mg/kg per day and prednisone 1 mg/kg per day have been shown to be appropriate for the treatment of peripheral ulcerative keratitis with granulomatosis with polyangiitis (formerly known as Wegener’s granulomatosis) by Watkins et al. 42. Azathioprine is safer and less effective than cyclophosphamide. Limited granulomatosis with polyangiitis (formerly known as Wegener’s granulomatosis) usually responds to methotrexate, while active antineutrophil cytoplasm antibody (ANCA)-associated vasculitis responds to rituximab 39. Abatacept, which targets CTLA4-Ig, is used on a small scale in patients and has good prospects. Campath-1H® (anti-CD52) can reduce circulating lymphocytes and is used in patients with refractory ANCA-associated small vessel vasculature (30 or 60 mg). Inhibitors of IL-17, the IL-17 receptor, IL-12/IL-23, and the C5a receptor are still under investigation 43. Biological therapy, such as TNF inhibitors, has also not undergone large-scale investigations 44 (Table 1).
Table 1. The therapy of peripheral ulcerative keratitis associated with autoimmune diseases
| Therapy | Classification | Agent | Target |
|---|---|---|---|
| Topical therapy | Corticosteroid | Prednisolone | Immune system 45 |
| Immunosuppressant | Cyclosporine A | Antigen-triggered signal transduction in T lymphocytes and expression of many lymphokines (IL-2) and antiapoptotic proteins 46 | |
| Collagenase inhibitors | l% medroxyprogesterone | Collagenase 47 | |
| 20% acetylcysteine | |||
| Surgical therapy | Cyanoacrylate glue, conjunctival flap, lamellar patch flap, or penetrating keratoplasty 48, conjunctivectomy combined with cryotherapy (mentioned in SLE) 49 | ||
| Systemic therapy | Corticosteroid | Prednisolone | Immune system 45 |
| Immunosuppressant | MTX | Immune system 32 | |
| CTX | |||
| Cyclosporine | |||
| Azathioprine | |||
| Biologic therapy | Etanercept | TNF-α 50 | |
| Infliximab | |||
| Adalimumab | |||
| Golimumab | |||
| DMARDs | |||
| Rituximab | B cell 51 | ||
| Etanercept | |||
| Adalimumab | |||
| Abatacept | T cell 52 | ||
| Anakinra | IL-1 52 | ||
| Tocilizumab | IL-6 52 | ||
| Ixekizumab | IL-17 53 | ||
| Secukinumab | |||
| Brodalumab | |||
| Ustekinumab | IL-12/IL-23 50 | ||
| Guselkumab | IL-23 50 | ||
| Belimumab (mentioned in SLE) | BAFF 54 | ||
| INF (interferon alpha and gamma), TLRs, pDCs, and JAK/STAT inhibitors (mentioned in SLE) | INF (interferon alpha and gamma), TLRs, pDCs, and JAK/STAT | ||
Most of the therapies are similar. However, there are some different places among these diseases.
Superficial punctate keratitis
Thygeson’s superficial punctate keratitis is is a potentially chronic condition characterized clinically by ocular irritation, tearing, photophobia, and visual disturbance but has minimal clinical manifestations in the cornea 55. Thygeson’s superficial punctate keratitis usually develops bilaterally, and slit lamp microscopic examination reveals aggregates of punctate fluorescein staining in the corneal epithelium that correspond to elevated and coarse granular opacities 56. Although the cause of Thygeson’s superficial punctate keratitis remains unclear, viral infection, allergic reactions, and immune responses to viral infection have been proposed to play a pathogenesis role.
Thygeson’s superficial punctate keratitis usually occurs in the second to third decade of life, though patients of all ages can be affected. It has a chronic course characterized by exacerbations and remissions. The duration of the disease ranges from 1 month to 24 years; some cases of a longer course of up to 41 years have been described as well 57.
The management of Thygeson’s superficial punctate keratitis varies with disease severity. During quiescent periods with minimal irritation, simple lubricating drops or no treatment is sufficient 58. During acute exacerbations, topical corticosteroids have been found to decrease signs and symptoms 59. Therapeutic contact lenses can be used to reduce the irritation in more symptomatic patients 58.
Lubricant eyedrops, eyedrops containing a low dose of corticosteroid, and soft contact lenses are options for medical management. In vivo imaging of eyes affected by Thygeson’s superficial punctate keratitis has been performed by confocal microscopy 60. The images revealed highly refractive microdots and refractive bodies immediately below the corneal epithelium, in Bowman’s layer, and in the anterior stroma. Morphological changes of keratocytes were also apparent in the previous reports.
Figure 11. Thygeson’s superficial punctate keratitis
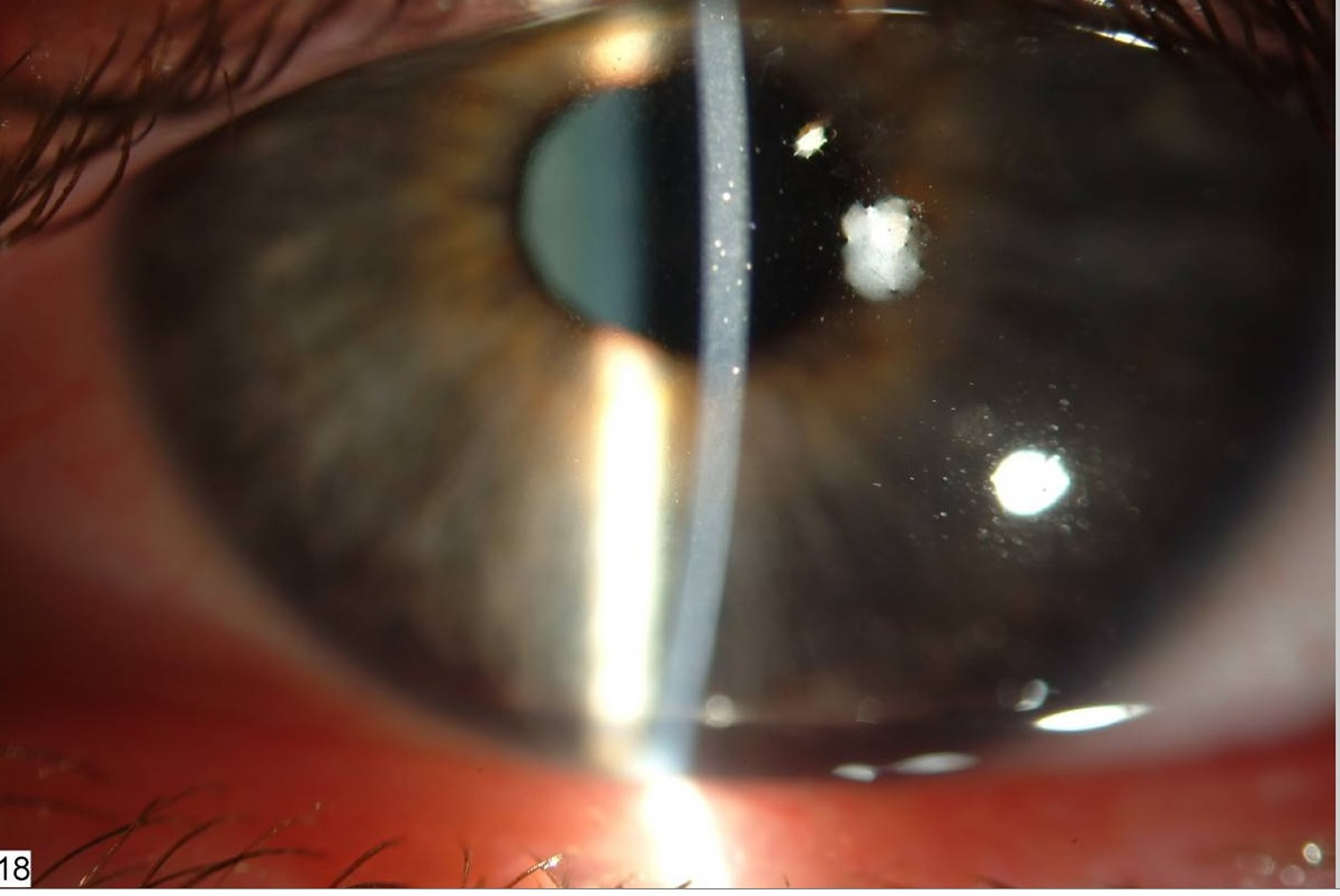
Staph marginal keratitis
Staphylococcal marginal keratitis is non-infectious and results from an enhanced cell-mediated immune-mediated response to Staphylococcus aureus bacterial antigens present with lid margin disease, typically presenting with peripheral corneal infiltrates with overlying epithelial loss adjacent to the limbus; staphylococcal marginal keratitis stains with fluorescein, separated by an interval of clear cornea 61. Staphylococcal marginal keratitis is mostly bilateral, involves the lower half of cornea, adjacent to the limbus, having a clear zone of cornea between the lesion and limbus. Being uniform in size, discrete and horizontally oval, there may be an oval or round scar due to previous attacks. Most of these patients may have associated blepharitis, meibomitis and rarely acne rosacea 62.
The ulcers may be round or arcuate, single or multiple, unilateral or bilateral. Marginal keratitis is a common cause of a red, uncomfortable eye, often presenting bilaterally with peripheral, discrete infiltration with circum-limbal sparing (Figure 11). Treatment is with a combination of topical antibiotics and steroids. Response to antibiotic and steroid therapy is usually rapid; failure to respond should prompt investigation for alternative causes of peripheral corneal ulceration 63. Anterior chamber inflammation is rare 64. Although unusual, in severe cases, a hypopyon may develop and potentially cause diagnostic confusion; a detailed history and examination to exclude risk factors for endophthalmitis are required.
Endophthalmitis (an infection inside the eye) is an important differential in a case presenting with a red, painful eye and hypopyon (pus inside the eye), such as that seen in Figure 13. Owing to its sight-threatening nature, it needs to be excluded carefully. Causes and risk factors are described below (Table 2 below). There were no risk factors for endophthalmitis in the patient shown in Figure 10; this, together with the preceding chronic history, total lack of pain and normal B-scan ultrasonography, made endophthalmitis very unlikely.
Figure 12. Staphylococcal marginal keratitis
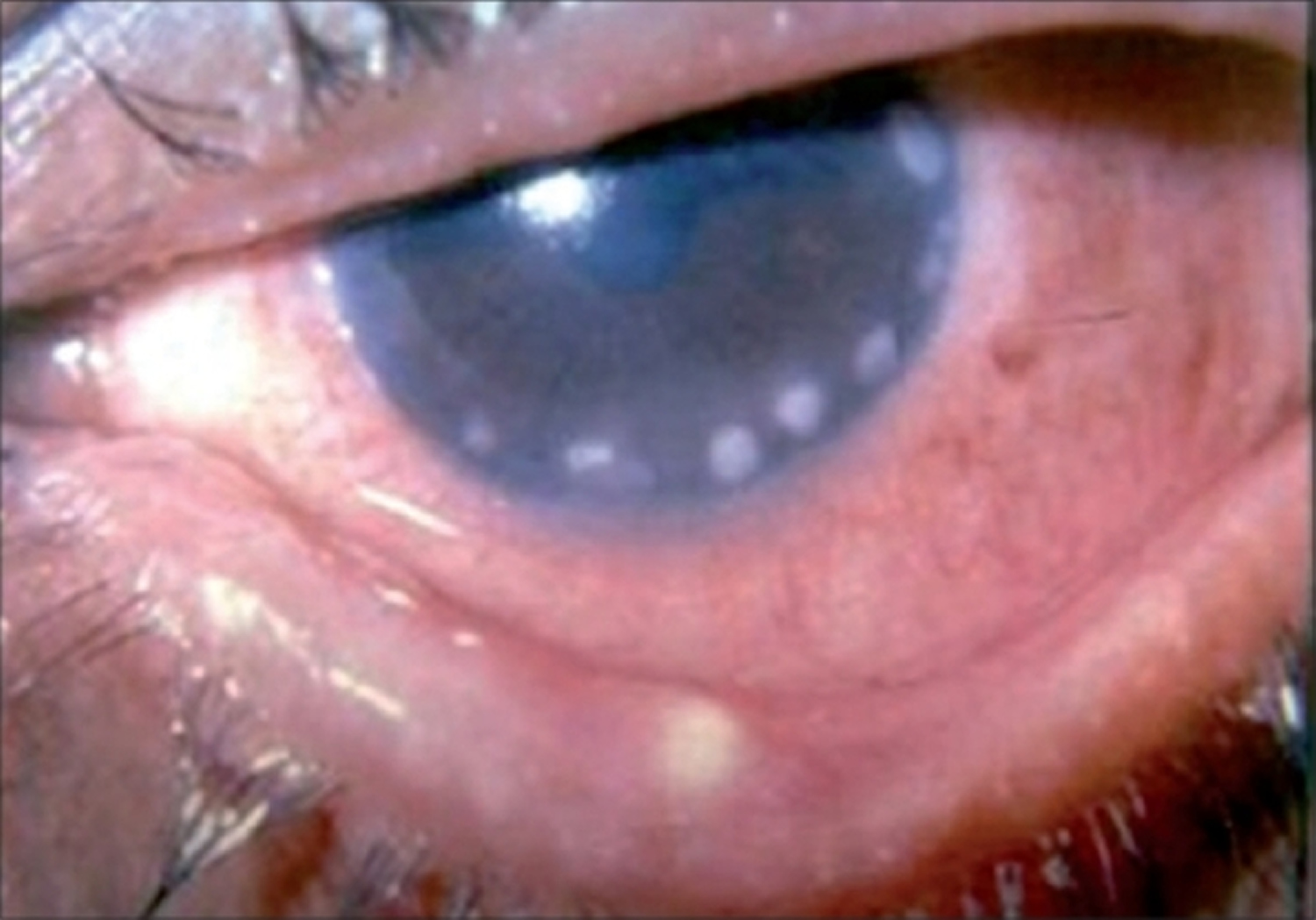
Figure 13. Staphylococcal marginal keratitis with hypopyon
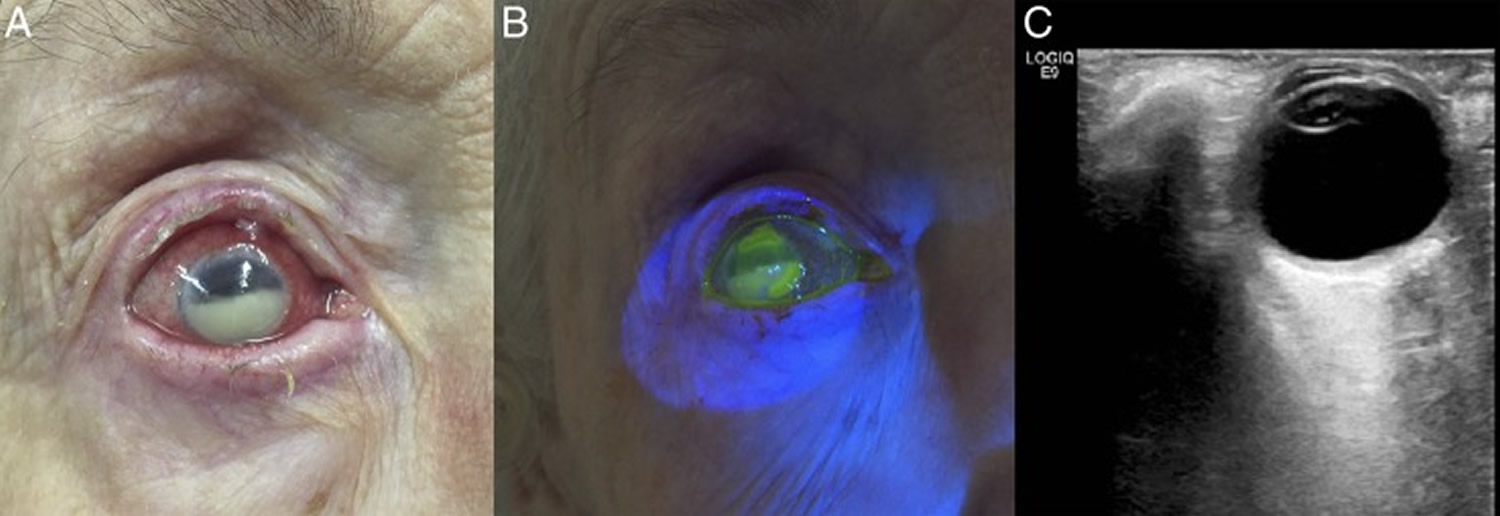
Note: (A) Two large peripheral marginal corneal epithelial defects with subepithelial stromal infiltration were present measuring approximately 4.5 and 4.0 mm in length, between 10 and 2 o’clock and 3 and 9 o’clock, respectively, 1.5 mm from the limbus. A 4.5 mm hypopyon was present. (B) The marginal epithelial defects staining brightly with fluorescein sodium 1% eye drops under cobalt blue filter. (C) B-scan ultrasound image of the right eye showing no evidence of endophthalmitis.
[Source 63]Table 2. Types of endophthalmitis, causative organisms and risk factors
| Type of endophthalmitis | Most common organisms | Risk factor(s) |
|---|---|---|
| Acute post-cataract | Coagulase-negative staphylococci (70% of cases), other Gram-positive cocci (25%) | Complicated surgery (vitreous loss, prolonged procedure) Periocular infection (eyelid, lacrimal) Diabetes mellitus |
| Chronic post-cataract | Propionibacterium acnes | Complicated surgery (vitreous loss, prolonged procedure) Periocular infection (eyelid, lacrimal) Diabetes mellitus |
| Post-intravitreal injection | Coagulase-negative staphylococci, viridans streptococci | Contaminated equipment Allergy to povidone iodine |
| Bleb related | Streptococci, Haemophilus influenzae | Thin walled leaking bleb |
| Post-traumatic | Bacillus cereus, coagulase-negative staphylococci (fungi in some cases) | Penetrating trauma Organic matter Intraocular foreign body |
| Endogenous bacterial | Staphylococcus aureus, streptococci, Gram-negative bacilli (eg, Klebsiella) |
|
| Candida (mostly endogenous) | Candida spp |
|
| Mould (mostly exogenous) | Aspergillus, Fusarium |
|
How To Prevent Eye and Corneal Infection With Proper Contact Lens Care
Follow your eye care provider’s instructions to wear, clean and store your contacts. These are some things to keep in mind:
- Wash your hands with soap and water and dry them with a lint-free towel before handling your contacts.
- Minimize contact with water. Remove lenses before going swimming or in a hot tub.
- Do not rinse or store your contacts in water (tap or sterile water).
- Do not put your lenses in your mouth to wet them.
- Do not use saline solution and rewetting drops to disinfect lenses. Neither is an effective or approved disinfectant.
- Follow your eye care professional’s schedule for wearing and replacing your contacts.
- Use the “rub and rinse” method to clean your contacts. Rub your contact lenses with your fingers, then rinse them with solution before soaking. Use this method even if the solution you are using is a “no-rub” variety.
- Rinse the contact lens case with fresh solution — not water. Then leave the empty case open to air dry.
- Keep the contact lens case clean and replace it regularly, at least every three months. Lens cases can be a source of contamination and infection. Do not use cracked or damaged lens cases.
- Do not re-use old solution or “top off” the solution in your lens case.
- Do not transfer contact lens solution into smaller travel-size containers.
- Do not allow the tip of the solution bottle to touch any surface. Keep the bottle tightly closed when not in use.
- Never wear your lenses after storage for 30 or more days without disinfecting them again.
Some forms of viral keratitis, such as keratitis caused by the herpes virus, can’t be completely eliminated. But the following steps may control viral keratitis recurrences:
- If you have a cold sore or a herpes blister, avoid touching your eyes, your eyelids and the skin around your eyes unless you’ve thoroughly washed your hands.
- Don’t use corticosteroid eyedrops unless they have been prescribed by a specialist knowledgeable about viral keratitis and the need for careful monitoring. Corticosteroid drops can increase your risk of developing viral keratitis and, if a viral infection does occur, these drops can make it more severe.
- If you wear contact lenses and have multiple recurrences of viral keratitis, discontinuing your use of contact lenses may decrease your risk of recurrences. Discuss this option with your eye doctor.
Keratitis symptoms
Signs and symptoms of keratitis include:
- Eye redness
- Eye pain
- Excess tears or other discharge from your eye
- Difficulty opening your eyelid because of pain or irritation
- Blurred vision
- Decreased vision
- Sensitivity to light (photophobia)
- A feeling that something is in your eye
Keratitis causes
Causes of keratitis include:
- Injury. If an object scratches the surface of one of your corneas or penetrates a cornea, keratitis without an infection may result. In addition, an injury may allow bacteria or fungi to gain access to the cornea through the damaged surface, causing infectious keratitis.
- Contaminated contact lenses. Bacteria, fungi or parasites — particularly the microscopic parasite acanthamoeba — may inhabit the surface of a contact lens or contact lens carrying case. The cornea may become contaminated when the lens is in your eye, resulting in infectious keratitis.
- Viruses. Viruses such as the herpes viruses (herpes simplex and herpes zoster) and the virus that causes chlamydia may cause keratitis.
- Contaminated water. Chemicals in water such as those used in swimming pools may irritate the cornea and weaken the delicate surface tissue of the cornea (corneal epithelium), resulting in a chemical keratitis. This is usually short-lived and may last only minutes to hours. Bacteria, fungi and parasites in water — particularly in oceans, rivers, lakes and hot tubs — can enter your eyes when you’re swimming or bathing and result in keratitis. If you’re exposed to these microorganisms, a healthy cornea is unlikely to become infected. But if you’ve experienced some previous breakdown of the corneal epithelium, such as from wearing a contact lens too long, your cornea may be vulnerable to infection.
Risk factors for keratitis
Factors that may increase your risk of keratitis include:
- Contact lenses. Wearing contact lenses increases your risk of both infectious and noninfectious keratitis. The risk typically stems from not disinfecting lenses properly, wearing contact lenses while swimming, wearing them longer than recommended, or using water or homemade solutions to store and clean lenses. Keratitis is more common in people who use extended-wear contacts, or wear contacts continuously, than in those who use daily wear contacts and take them out at night.
- Reduced immunity. If your immune system is weakened due to disease or medications, you’re at higher risk of developing keratitis.
- Warm climate. If you live in a warm, humid climate, your risk of keratitis is increased, particularly if plant material gets into your eyes. Plant material can scratch the corneal epithelium and chemicals from the plant can cause an inflammation, which may then lead to an infection.
- Corticosteroids. Use of corticosteroid eyedrops to treat an eye disorder can increase your risk of developing infectious keratitis or worsen existing keratitis.
- Eye injury. If one of your corneas has been damaged from an injury in the past, you may be more vulnerable to developing keratitis.
Keratitis complications
Potential complications of keratitis include:
- Chronic corneal inflammation
- Chronic or recurrent viral infections of your cornea
- Open sores on your cornea (corneal ulcers)
- Corneal swelling and scarring
- Temporary or permanent reduction in your vision
- Blindness
Keratitis diagnosis
Your doctor will review your medical history and your symptoms, conduct an eye examination, and perform tests to diagnose keratitis.
Diagnosing keratitis typically involves the following:
- Eye exam. Your doctor will perform a general examination of your eye. It may be uncomfortable to open your eye for the exam, but it’s important that your doctor be able to examine your eye. The exam will include an effort to determine how well you can see (visual acuity), usually using standard eye charts.
- Penlight exam. Your doctor may examine your eye using a penlight, to check your pupil’s reaction, size and other factors. Your doctor may apply a stain to the surface of your eye, to help identify the extent and character of surface irregularities and ulcers of the cornea.
- Slit-lamp exam. Your doctor may examine your eyes with a special instrument called a slit lamp, which provides a bright source of light and magnification. This instrument uses an intense line of light — a slit-like beam — to illuminate your cornea, iris, lens, and the space between your iris and cornea. The light allows your doctor to view these structures with high magnification to detect the character and extent of keratitis, as well as the effect it may have on other structures of the eye.
- Laboratory analysis. Your doctor may take a sample of tears or some cells from your cornea for laboratory analysis to determine the cause of keratitis and to help develop a treatment plan for your condition.
Keratitis treatment
Noninfectious keratitis
Treatment of noninfectious keratitis varies depending on the cause. If your keratitis is caused by a scratch or extended contact lens wear, you may not need any treatment. If you’re having significant tearing and pain, you may need to apply prescription medicine to the eye and wear an eye patch until your condition improves.
Infectious keratitis
Treatment of infectious keratitis varies, depending on the cause of the infection.
- Bacterial keratitis. For mild bacterial keratitis, antibacterial eyedrops may be all you need to effectively treat the infection. If the infection is moderate to severe, you may need to take oral antibiotics.
- Fungal keratitis. Keratitis caused by fungi typically requires antifungal eyedrops and oral antifungal medication.
- Viral keratitis. If a virus is causing the infection, antiviral eyedrops and oral antiviral medications may be effective. But these medications may not be able to eliminate the virus completely, and viral keratitis may recur.
- Acanthamoeba keratitis. Keratitis that’s caused by the tiny parasite acanthamoeba can be difficult to treat. Antibiotic eyedrops may be helpful, but some acanthamoeba infections are resistant to medication.
If keratitis that doesn’t respond to medication, or if it causes permanent damage to the cornea that significantly impairs your vision, your doctor may recommend a cornea transplant.
- Agrawal V, Biswas J, Madhavan HN, Mangat G, Reddy MK, Saini JS, et al. Current perspectives in infectious keratitis. Indian J Ophthalmol. 1994;42:171–91. https://www.ncbi.nlm.nih.gov/pubmed/10576995[↩]
- Arffa RC. Grayson′s Diseases of the cornea. 4th ed. St.Louis: Mosby; 1997.[↩][↩]
- Sridhar MS, Sangwan VS, Bansal AK, Rao GN. Amniotic membrane transplantation in the management of shield ulcers of vernal keratoconjunctivitis. Ophthalmology. 2001;108:1218–22. https://www.ncbi.nlm.nih.gov/pubmed/11425678[↩]
- Arffa RC. Grayson′s Diseases of the cornea. 4th ed. St.Louis: Mosby; 1997[↩]
- Bharathi MJ, Ramakrishnan R, Vasu S, Meenakshi R, Palaniappan R. Aetiological diagnosis of microbial keratitis in South India: A study of 1618 cases. Indian J Med Microbiol. 2002;20:19–24. https://www.ncbi.nlm.nih.gov/pubmed/17657018[↩]
- Srinivasan M. Fungal keratitis. Curr Opin Ophthalmol. 2004;15:321–327. https://www.ncbi.nlm.nih.gov/pubmed/15232472[↩]
- Ng JK, Fraunfelder FW, Winthrop KL. Review and Update on the Epidemiology, Clinical Presentation, Diagnosis, and Treatment of Fungal Keratitis. Curr Fungal Infect Rep. 2013;7:293–300.[↩]
- Alfonso EC, Miller D, Cantu-Dibildox J, O’Brien TP, Schein OD. Fungal keratitis associated with non-therapeutic soft contact lenses. Am J Ophthalmol. 2006;142:154–155. https://www.ncbi.nlm.nih.gov/pubmed/16815266[↩][↩]
- Ritterband DC, Seedor JA, Shah MK, Koplin RS, McCormick SA. Fungal keratitis at the New York eye and ear infirmary. Cornea. 2006;25:264–267. https://www.ncbi.nlm.nih.gov/pubmed/16633023[↩]
- https://www.ncbi.nlm.nih.gov/pubmed/15604867[↩]
- Iyer SA, Tuli SS, Wagoner RC. Fungal keratitis: Emerging trends and treatment outcomes. Eye Contact Lens. 2006;32:267–271. https://www.ncbi.nlm.nih.gov/pubmed/17099386[↩]
- Yildiz EH, Abdalla YF, Elsahn AF, Rapuano CJ, Hammersmith KM, Laibson PR, et al. Update on fungal keratitis from 1999 to 2008. Cornea. 2010;29:1406–1411. https://www.ncbi.nlm.nih.gov/pubmed/20847685[↩]
- Thomas P, Kaliamurthy J. Mycotic keratitis: Epidemiology, diagnosis and management. Clin Microbiol Infect. 2013;19:210–220. https://www.ncbi.nlm.nih.gov/pubmed/23398543[↩]
- Gopinathan U, Garg P, Fernandes M, Sharma S, Athmanathan S, Rao GN. The epidemiological features and laboratory results of fungal keratitis: A 10-year review at a referral eye care center in South India. Cornea. 2002;21:555–559. https://www.ncbi.nlm.nih.gov/pubmed/12131029[↩]
- Abdelfattah NS, Amgad M, Zayed AA, Salem H, Elkhanany AE, Hussein H, et al. Clinical correlates of common corneal neovascular diseases: A literature review. Int J Ophthalmol. 2015;8:182–193. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4325264/[↩]
- Cursiefen C, Colin J, Dana R, Diaz-Llopis M, Faraj LA, Garcia-Delpech S, et al. Consensus statement on indications for anti-angiogenic therapy in the management of corneal diseases associated with neovascularisation: Outcome of an expert roundtable. Br J Ophthalmol. 2012;96:3–9. https://www.ncbi.nlm.nih.gov/pubmed/21712359[↩]
- Hassan AA, Ghoneim DF, El-dib AA, Ahmed SA, Abdel-Salam AM. Photothrombosis of Corneal Neovascularization by Photodynamic Therapy Utilizing Verteporfin and Diode Laser. Jo Lasers Med Sci. 2013;4:131–139. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4295361/[↩]
- Chang EJ, Dreyer EB. Herpes virus infections of the anterior segment. Int Ophthalmol Clin. 1996;36:17–28. https://www.ncbi.nlm.nih.gov/pubmed/8989597[↩]
- Lorenzo-Morales J, Khan NA, Walochnik J. An update on Acanthamoeba keratitis: diagnosis, pathogenesis and treatment. Parasite. 2015;22:10. doi:10.1051/parasite/2015010. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4330640/[↩]
- Garg P, Kalra P, Joseph J. Non-contact lens related Acanthamoeba keratitis. Indian Journal of Ophthalmology. 2017;65(11):1079-1086. doi:10.4103/ijo.IJO_826_17. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5700572/[↩][↩]
- Acanthamoeba Keratitis Fact Sheet [Health Professionals] Atlanta: Centers for Disease Control and Prevention. https://www.cdc.gov/parasites/acanthamoeba/health_professionals/acanthamoeba_keratitis_hcp.html[↩]
- Lorenzo-Morales J, Khan NA, Walochnik J. An update on Acanthamoeba keratitis: Diagnosis, pathogenesis and treatment. Parasite. 2015;22:10. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4330640[↩][↩][↩]
- Dart JK, Saw VP, Kilvington S. Acanthamoeba keratitis: Diagnosis and treatment update 2009. Am J Ophthalmol. 2009;14:487–499. https://www.ncbi.nlm.nih.gov/pubmed/19660733[↩]
- Radford C, Minassian D, Dart J. Acanthamoeba keratitis in England and Wales: Incidence, outcome, and risk factors. Br J Ophthalmol. 2002;86:536–542. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1771120/[↩]
- Anger C, Lally JM. Acanthamoeba: A review of its potential to cause keratitis, current lens care solution disinfection standards and methodologies, and strategies to reduce patient risk. Eye Contact Lens. 2008;34:247–253. https://www.ncbi.nlm.nih.gov/pubmed/18779663[↩][↩]
- Lim N, Goh D, Bunce C, Xing W, Fraenkel G, Poole TR, et al. Comparison of polyhexamethylene biguanide and chlorhexidine as monotherapy agents in the treatment of Acanthamoeba keratitis. Am J Ophthalmol. 2008;145:130–135. https://www.ncbi.nlm.nih.gov/pubmed/17996208[↩]
- Coulon C, Collignon A, McDonnell G, Thomas V. Resistance of Acanthamoeba cysts to disinfection treatments used in health care settings. J Clin Microbiol. 2010;48:2689–2697. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2916629/[↩]
- Lorenzo-Morales J, Khan NA, Walochnik J. An update on Acanthamoeba keratitis: Diagnosis, pathogenesis and treatment. Parasite. 2015;22:10. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4330640/[↩]
- Lorenzo-Morales J, Martín-Navarro CM, López-Arencibia A, Arnalich-Montiel F, Piñero JE, Valladares B. 2013. Acanthamoeba keratitis: an emerging disease gathering importance worldwide? Trends in Parasitology, 29(4), 181–187. https://www.ncbi.nlm.nih.gov/pubmed/23433689[↩][↩][↩]
- Levitt A. E., McManus K. T., McClellan A. L., Davis J., Goldhardt R., Galor A. Ocular inflammation in the setting of concomitant systemic autoimmune conditions in an older male population. Cornea. 2015;34(7):762–767. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4460602/[↩]
- Artifoni M., Rothschild P. R., Brézin A., Guillevin L., Puéchal X. Ocular inflammatory diseases associated with rheumatoid arthritis. Nature Reviews Rheumatology. 2014;10(2):108–116. doi: 10.1038/nrrheum.2013.185. https://www.ncbi.nlm.nih.gov/pubmed/24323074[↩]
- Clewes A. R., Dawson J. K., Kaye S., Bucknall R. C. Peripheral ulcerative keratitis in rheumatoid arthritis: successful use of intravenous cyclophosphamide and comparison of clinical and serological characteristics. Annals of the Rheumatic Diseases. 2005;64:961–962. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1755509/pdf/v064p00961.pdf[↩][↩][↩][↩]
- Murray P. I., Rauz S. The eye and inflammatory rheumatic diseases: the eye and rheumatoid arthritis, ankylosing spondylitis, psoriatic arthritis. Best Practice & Research Clinical Rheumatology. 2016;30(5):802–825. https://www.ncbi.nlm.nih.gov/pubmed/27964790[↩]
- Silva B. L., Cardozo J. B., Marback P., Machado F. C., Galvão V., Santiago M. B. Peripheral ulcerative keratitis: a serious complication of rheumatoid arthritis. Rheumatology International. 2010;30(9):1267–1268. https://www.ncbi.nlm.nih.gov/pubmed/19823839[↩]
- Watanabe R., Ishii T., Yoshida M., et al. Ulcerative keratitis in patients with rheumatoid arthritis in the modern biologic era: a series of eight cases and literature review. International Journal of Rheumatic Diseases. 2017;20(2):225–230. doi: 10.1111/1756-185X.12688. https://www.ncbi.nlm.nih.gov/pubmed/26179634[↩]
- Riley G. P., Harral R. L., Watson P. G., Cawston T. E., Hazleman B. L. Collagenase (MMP-1) and TIMP-1 in destructive corneal disease associated with rheumatoid arthritis. Eye. 1995;9:703–718. https://www.ncbi.nlm.nih.gov/pubmed/8849537[↩]
- Maseda D., Bonami R. H., Crofford L. J. Regulation of B lymphocytes and plasma cells by innate immune mechanisms and stromal cells in rheumatoid arthritis. Expert Review of Clinical Immunology. 2014;10(6):747–762. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5073792/[↩]
- Galor A., Thorne J. E. Scleritis and peripheral ulcerative keratitis. Rheumatic Diseases Clinics of North America. 2007;33:835–854. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2212596/[↩]
- Kubaisi B., Abu S. K., Foster C. S. Granulomatosis with polyangiitis (Wegener’s disease): an updated review of ocular disease manifestations. Intractable Rare Diseases Research. 2016;5(2):61–69. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4869584/[↩][↩]
- Lu C. W., Zhou D. D., Wang J., Hao J. L. Surgical treatment of peripheral ulcerative keratitis and necrotizing scleritis in granulomatosis with polyangiitis. Saudi Medical Journal. 2016;37(2):205–207. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4800921/[↩]
- Gu J., Zhou S., Ding R., Aizezi W., Jiang A., Chen J. Necrotizing scleritis and peripheral ulcerative keratitis associated with Wegener’s granulomatosis. Ophthalmology and Therapy. 2013;2(2):99–111. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4108142/[↩]
- Watkins A. S., Kempen J. H., Choi D., et al. Ocular disease in patients with ANCA-positive vasculitis. Journal of Ocular Biology Diseases and Informatics. 2009;3(1):12–19. doi: 10.1007/s12177-009-9044-4. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2933008/[↩]
- Tarzi R. M., Pusey C. D. Current and future prospects in the management of granulomatosis with polyangiitis (Wegener’s granulomatosis) Therapeutics and Clinical Risk Management. 2014;10:279–293. doi: 10.2147/TCRM.S41598. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4000246/[↩]
- White E. S., Lynch J. P. Pharmacological therapy for Wegener’s granulomatosis. Drugs. 2006;66(9):1209–1228. https://www.ncbi.nlm.nih.gov/pubmed/16827598[↩]
- Cordero-Coma M., Méndez R. S., Blanco A. C., Corral A. L., Calleja-Antolín S., Morales J. M. Adalimumab for refractory peripheral ulcerative keratitis. Journal of Ophthalmic Inflammation Infect. 2012;2(4):227–229. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3500990/[↩][↩]
- Steinberg J. S., Herwig M. C., Holz F. G., Loeffler K. U. Peripheral ulcerative keratitis in a 24-year-old patient. Der Ophthalmologe. 2014;111(8):772–774. https://www.ncbi.nlm.nih.gov/pubmed/24046173[↩]
- Subbarayal B., Chauhan S. K., Zazzo A., Dana R. IL-17 augments B cell activation in ocular surface autoimmunity. Journal of Immunology. 2016;197(9):3464–3470. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5101134/[↩]
- Brejchova K., Liskova P., Cejkova J., Jirsova K. Role of matrix metalloproteinases in recurrent corneal melting. Experimental eye Research. 2010;90(5):583–590. https://www.ncbi.nlm.nih.gov/pubmed/20153319[↩]
- Gottschalk T. A., Tsantikos E., Hibbs M. L. Pathogenic inflammation and its therapeutic targeting in systemic lupus erythematosus. Frontiers in Immunology. 2015;6:p. 550. doi: 10.3389/fimmu.2015.00550. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4623412/[↩]
- Meadow P. B., Nguyen J., Kesavarapu K. Tofacitinib citrate for ulcerative keratitis in a patient with rheumatoid arthritis. Case Reports in Rheumatology. 2014;2014:13. doi: 10.1155/2014/403452.403452 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4084676/[↩][↩][↩]
- Yu X., Wang C., Luo J., Zhao X., Wang L., Li X. Combination with methotrexate and cyclophosphamide attenuated maturation of dendritic cells: inducing treg skewing and Th17 suppression in vivo. Clinical and Developmental Immunology. 2013;2013:12. doi: 10.1155/2013/238035.238035 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3806152/[↩]
- Huerva V., Sanchez M. C., Traveset A., Jurjo C., Ruiz A. Rituximab for peripheral ulcerative keratitis with Wegener granulomatosis. Cornea. 2010;29:708–710. https://www.ncbi.nlm.nih.gov/pubmed/20458228[↩][↩][↩]
- Buch M. H., Smolen J. S., Betteridge N., et al. Updated consensus statement on the use of rituximab in patients with rheumatoid arthritis. Annals of the Rheumatic Diseases. 2011;70(6):909–920. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3086093/[↩]
- Shoughy S. S., Tabbara K. F. Ocular findings in systemic lupus erythematosus. Saudi Journal Ophthalmology. 2016;30(2):117–121. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4908056/[↩]
- Nagra PK, Rapuano CJ, Cohen EJ, Laibson PR. Thygeson’s superficial punctate keratitis: ten years’ experience. Ophthalmology. 2004;111:34–7. https://www.ncbi.nlm.nih.gov/pubmed/14711711[↩]
- Tabbara KF, Ostler HB, Dawson C, Oh J. Thygeson’s superficial punctate keratitis. Ophthalmology. 1981;88:75–7. https://www.ncbi.nlm.nih.gov/pubmed/6264365[↩]
- Tanzer DJ, Smith RE. Superficial punctate keratitis of thygeson: The longest course on record? Cornea. 1999;18:729–730. doi: 10.1097/00003226-199911000-00017 https://www.ncbi.nlm.nih.gov/pubmed/10571306[↩]
- Goldberg DB, Schanzlin DJ, Brown SI. Management of thygeson’s superficial punctate keratitis. American journal of ophthalmology. 1980;89:22–24. https://www.ncbi.nlm.nih.gov/pubmed/6892542[↩][↩]
- Thygeson P. Superficial punctate keratitis. J Am Med Assoc. 1950;144:1544–9. https://www.ncbi.nlm.nih.gov/pubmed/14794375[↩]
- Cheng LL, Young AL, Wong AK, Law RW, Lam DS. In vivo confocal microscopy of Thygeson’s superficial punctate keratitis. Clin Experiment Ophthalmol. 2004;32:325–7. https://www.ncbi.nlm.nih.gov/pubmed/15180847[↩]
- Srinivasan M, Mascarenhas J, Prashanth C. Distinguishing infective versus noninfective keratitis. Indian J Ophthalmol 2008;56:203–7. doi:10.4103/0301-4738.40358 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2636110/[↩]
- Cetinkaya A, Akova YA. Pediatric ocular acne rosacea: Long-term treatment with systemic antibiotics. Am J Ophthalmol. 2006;142:816–21. https://www.ncbi.nlm.nih.gov/pubmed/17056363[↩]
- Hoffman J, Hassan A. Severe staphylococcal marginal keratitis presenting with hypopyon. BMJ Case Reports. 2015;2015:bcr2015211979. doi:10.1136/bcr-2015-211979. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4550862/[↩][↩]
- Boto-de-Los-Bueis A, Del Hierro Zarzuelo A, García Perea A et al. Staphylococcus aureus Blepharitis Associated with Multiple Corneal Stromal Microabscess, Stromal Edema, and Uveitis. Ocul Immunol Inflamm 2015;23:180–3. doi:10.3109/09273948.2013.870214 https://www.ncbi.nlm.nih.gov/pubmed/24410378[↩]
- Durand ML. Endophthalmitis. Clin Microbiol Infect 2013;19:227–34. doi:10.1111/1469-0691.12118 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3638360/[↩]





{kind=link}