
Contents
What is ketonuria
Ketonuria occurs when high levels of ketone bodies (acetone, acetoacetate, and beta-hydroxybutyrate) which occur when fatty acids are broken down for energy are present in the urine. Ketone bodies can be measured with a urinalysis. Results range from 0 (not detected) to +4 (high amount detected). Ketosis is a natural state the body finds itself in when it is using fat as its main fuel. This occurs when following a very low carb, ketogenic diet or “keto diet”, and often during intermittent fasting too. Ketosis can be beneficial for a number of people but there are certain groups, such as people with type 1 diabetes, that need to be more careful. In these groups, very high ketone levels would lead to diabetic ketoacidosis (DKA), a dangerous situation caused by a lack of sufficient insulin.
Ketogenesis is a metabolic pathway that produces ketone bodies, which provide an alternative form of energy for the body. The body is constantly producing small amounts of ketone bodies that can make 22 adenosine triphosphate (ATP) each in normal circumstances, and it is regulated mainly by insulin. In a state of ketosis, ketone body production is increased when there are decreased carbohydrates or increased fatty acids. However, ketoacidosis can occur if too many ketone bodies accumulate, such as in cases uncontrolled diabetes.
Ketones which are not used for fuel are excreted out of the body via the kidneys and the urine.
Nutritional ketosis occurs when there is not enough carbohydrate in the diet to meet the body’s energy requirements. In this situation, the body switches over from burning sugar to burning fat as its main fuel.
Fat, whether from the diet or the body’s stores, is broken down into ketones in the liver. These ketones are an efficient energy source for many organs, particularly the brain.
Everyone has ketones in their blood at very low levels, under normal conditions. When the body enters ketosis, and so switches to burning mostly fat, levels of ketones in the blood increase.
Ketonuria can be dangerous if ketones levels become high and may need to be monitored amongst people with diabetes who are prone to high blood glucose levels.
Ketones tend to be produced as a result of insufficient insulin in the body and therefore people with type 1 diabetes, in particular, are at a greater risk of ketonuria.
High ketone levels may indicate diabetic ketoacidosis (DKA), a complication of diabetes that can lead to a coma or even death.
An overproduction of ketone bodies through increased ketogenesis can pose a problem due to their acidic nature.
Glucose is the primary carbon-based substrate in blood necessary for the production of adenosine triphosphate (ATP), which is the energy currency of cells after glucose is metabolized during glycolysis, Kreb’s cycle and the electron transport chain. Ketone bodies are fat-derived fuels used by tissues at the time of limited glucose availability. Hepatic generation of ketone bodies is usually stimulated by the combination of low insulin levels and high counter-regulatory hormone levels including glucagon.
Low insulin levels are seen inherently in as either an absolute or relative deficiency in type 1 diabetes or a relative deficiency with insulin resistance in type 2 diabetes. In alcoholic or starvation conditions, low insulin levels are secondary to absolute or relative hypoglycemia. This unfavorable ratio of insulin to glucagon activates hormone-sensitive lipase, which breaks down triglycerides in peripheral fat stores, releasing long-chain fatty acids and glycerol. The fatty acids undergo beta-oxidation in the hepatic mitochondria and generate acetyl-CoA. With the generation of large quantities of acetyl-CoA in the more severe forms of each of these conditions, the oxidative capacity of the Krebs cycle gets saturated, and there is a spillover entry of acetyl-CoA into the ketogenic pathway and subsequent generation of ketone bodies. An increased anion gap metabolic acidosis occurs when these ketone bodies are present as they are unmeasured anions.
Diabetic ketoacidosis (DKA) occurs when there is a lack of, or resistance to, insulin. This usually occurs in people with type 1 diabetes, although it can happen to people with advanced type 2 diabetes as well. In most cases of type 2 diabetes, enough insulin production continues to prevent excessive ketogenesis.
Due to the lack of glucose brought in by insulin, cells start to produce glucose via gluconeogenesis. This process, along with existing glucose that cannot be brought in with insulin, greatly elevates serum glucose levels. The threshold for diabetic ketoacidosis (DKA) is a glucose level of 250. However, it is typically greater than this amount.
Once carbohydrate stores are depleted and gluconeogenesis cannot occur anymore, ketogenesis is substantially increased, and there are larger amounts of ketone bodies produced. Due to the acidic nature of beta-hydroxybutyrate and acetoacetate, this causes an anion gap metabolic acidosis.
On presentation, diabetic ketoacidosis (DKA) patients are usually very dehydrated from being hyperglycemic. The high glucose levels lead to osmotic diuresis, involving greater osmole concentrations (in this case the osmole being glucose) that cause an increased osmotic pressure, which leads to reduced water reabsorption in the kidneys. Along with being dehydrated, patients typically present with confusion, nausea, vomiting, and abdominal pain. Because of the acidosis, patients often breathe very deeply and rapidly to eliminate carbon dioxide and cause a respiratory alkalosis. This process is known as Kussmaul breathing, and, over time, a patient can experience respiratory distress due to the prolonged exertion of respiratory muscles. Cerebral edema can occur in severe cases of DKA. Because of the acetone produced by ketogenesis, patients can have breath that smells fruity or like nail polish remover.
The main goal of treating diabetic ketoacidosis (DKA) is to resolve the metabolic acidosis, which involves giving glucose and insulin to not only lower blood glucose levels but also to downregulate the ketogenic pathway and decrease the number of ketone bodies produced.
Ketoacidosis also can occur with severe alcoholism and prolonged starvation.
Alcoholic ketoacidosis 1 occurs in patients with chronic alcohol abuse and liver disease and usually develops following abrupt withdrawal of alcohol or an episode of acute intoxication. It is not uncommon for the ingested ethanol to have already been metabolized, leading to low or normal serum levels when checked. In normal alcohol metabolism, the ingested ethanol is oxidized to acetaldehyde and then to acetic acid with the enzyme alcohol dehydrogenase, during which process the coenzyme nicotinamide adenine dinucleotide (NAD+) is reduced to NADH. The acetic acid can be shunted towards ketogenesis in favorable insulin/glucagon concentrations, which is seen in hypoglycemia. In addition to this, the increased NADH further suppresses gluconeogenesis and reduces free glucose, perpetuating ketogenesis 2. After abrupt withdrawal, rising catecholamine levels as a bodily response cause lipolysis and ketosis. The high ratio of NADH to NAD+ also favors the reduction of acetoacetate to beta-hydroxybutyrate.
In extremes of starvation, after the exhaustion of the free glucose and after that, the body’s glycogen reserves, fatty acids become the primary fuel source. This usually happens after 2 or 3 days of fasting. After several days of fasting, protein catabolism starts and muscles are broken down, releasing amino acids and lactate into the bloodstream, which can be converted into glucose by the liver. This biochemical process is responsible for the wasting and cachexia seen during starvation.
How to do a urine ketone test
Before testing, check the expiry date on the tub to ensure the strips are good for use. Also check the instructions which will tell you how long you need to wait, after urine is applied to the strip, before checking the color chart.
The process for ketone testing will then usually follow steps similar to these:
- Remove a strip from the tub, taking care not to touch the spongy end of the strip
- Pass urine over the test area of the strip or, alternatively, collect urine in a container and then dip the test area of the strip into the urine
- Begin timing immediately after applying urine – the strip will begin to change color
- After a set number of seconds (check the instructions), compare the color of the test area to the color chart on the side of the tub of strips
- Disregard any color changes that might happen after the set number of seconds has passed
What should the ketone test results be?
- Under 0.6 mmol/L – a normal blood ketone value
- 0.6 to 1.5 mmol/L – indicates that more ketones are being produced than normal, test again later to see if the value has lowered
- 1.6 to 3.0 mmol/L – a high level of ketones and could present a risk of ketoacidosis. It is advisable to contact your healthcare team for advice.
- Above 3.0 mmol/L – a dangerous level of ketones which will require immediate medical care.
For people with diabetes on insulin, having high ketone levels should be regarded as potentially dangerous.
Ketone testing for weight loss
Some people use ketone testing as a way to test whether their body is breaking down fat. Higher ketone levels indicates a greater likelihood of weight loss.
Groups at greater risk of ketoacidosis
Some people are at risk of ketoacidosis.
Groups at risk of ketoacidosis include, but is not limited to, people with:
- Type 1 diabetes
- Cystic fibrosis-related diabetes
- Pancreatectomy
- Type 2 diabetes with very little pancreatic function
It is possible, and can be beneficial, for people in these groups to follow a ketogenic lifestyle. However, it is important that your doctor is aware of your intention before you start.
Your health team can help you with regard to how best to monitor for ketones and prevent ketoacidosis occurring.
Ketosis vs ketoacidosis
Whereas ketosis is an important natural state allowing the body to run on fat for energy, diabetic ketoacidosis (DKA) is a dangerous and potentially fatal condition.
Diabetic ketoacidosis (DKA) occurs during situations of ‘internal starvation’ mainly in people with type 1 diabetes, when not enough insulin has been administered.
In this case, the body does not have enough insulin to allow blood glucose into cells. The body believes it is starving and so breaks down fat and protein into ketones at an alarming rate, far above what is seen in nutritional ketosis.
In most cases, ketoacidosis develops when there are both high ketone levels and high blood glucose.
In most people nutritional ketosis is beneficial.
Regularly achieving nutritional ketosis has been linked with improvements in:
- Weight loss
- Blood glucose control in diabetes
- Epilepsy
- Overall metabolic health
Research also suggests that nutritional ketosis may have benefits for people with Parkinson’s disease, Alzheimer’s disease and may help to reduce the chance of developing certain forms of cancer.
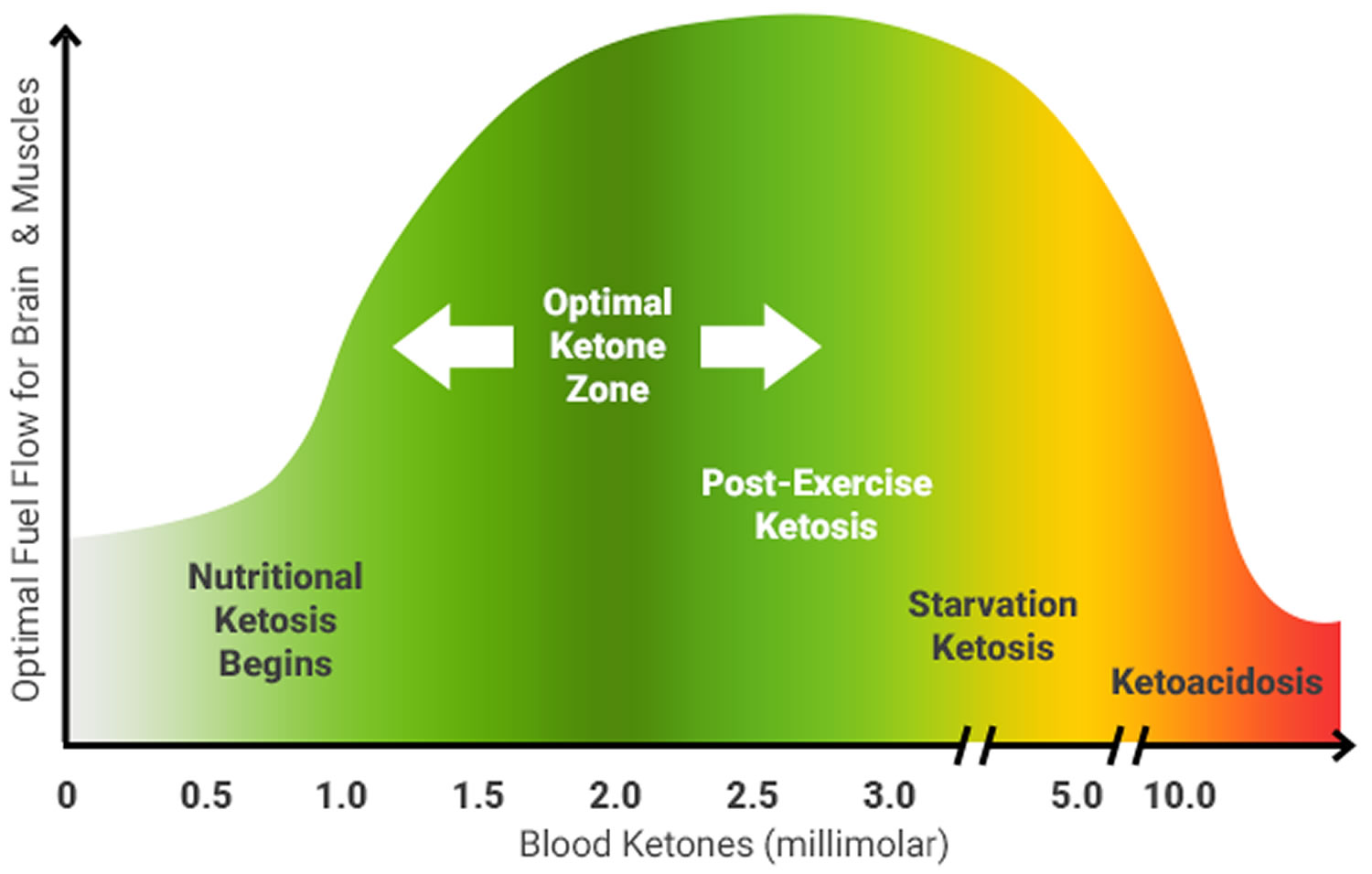
Ketone levels between 0.5 and 3 mmol/L are considered nutritional ketosis. Ketones are measurable in a number of ways, including blood monitors, breathalyzers and urine testing strips. Of these, urine strips are the least effective, as they only measure the ketones that your body is getting rid of, and not the ones it’s using.
The graph below shows the range of blood ketone levels for ketosis and ketoacidosis.
Figure 1. Blood ketone levels for ketosis and ketoacidosis
Ketonuria causes
Ketonuria may occur for different reasons, depending on your type of diabetes and whether you have a particularly low daily intake of carbohydrate such as during fasting or undergoing a ketogenic diet.
Other conditions can cause you to test positive for ketonuria. These include:
- Eating disorders, malnutrition, and other conditions where the body does not take in enough calories
- Pregnancy. Sometimes pregnant women will develop blood ketones. If high levels are found, it can mean gestational diabetes, a type of diabetes that only affects pregnant women.
If you have type 1 diabetes or produce very little of your own insulin, then your body will start to produce ketones if it has too little insulin for a significant period of time, such as a few hours or more.
When this happens, the body, not having sufficient insulin to get energy into the body’s cells, breaks down body tissue (fat and muscle) into ketones, which can be used as fuel without the need for insulin.
However, high levels of ketones in combination with high blood glucose levels (hyperglycemia) can make you feel ill and can lead to a dangerous state called ketoacidosis.
If you are following a ketogenic diet that is very low in carbohydrate and low in calories, the body may need to compensate by breaking down fat to produce ketones for use as energy.
As long as your body always has sufficient insulin, either your own insulin or that which you inject, then ketoacidosis should not occur. Ketonuria may also develop during periods of fasting.
Whilst ketogenic diets have become popular amongst a significant number of people with diabetes, particularly those with type 2 diabetes, they have not been recommended by some health organization because of questions surrounding whether they are safe and effectiveness enough to be followed on a long term basis.
Ketoacidosis is a metabolic state associated with pathologically high serum and urine concentrations of ketone bodies, namely acetone, acetoacetate and beta-hydroxybutyrate. During catabolic states, fatty acids are metabolized to ketone bodies, which can be readily utilized for fuel by individual cells in the body. Of the three major ketone bodies, acetoacetic acid is the only true ketoacid chemically, while beta-hydroxybutyric acid is a hydroxy acid, and acetone is a true ketone.
Diabetic ketoacidosis (DKA) can occur in patients with diabetes mellitus, most frequently associated with relative insulin deficiency. This may be caused by a precipitating physiologic stress or in some cases, may be the initial clinical presentation in patients with previously undiagnosed diabetes. Some of the more common risk factors that can precipitate the development of extreme hyperglycemia and subsequent ketoacidosis are infection, non-adherence to insulin therapy, acute major illnesses like myocardial infarction, sepsis, pancreatitis, stress, trauma, and the use of certain medications, such as glucocorticoids or atypical antipsychotic agents which have the potential to affect carbohydrate metabolism 4.
Diabetic ketoacidosis occurs more frequently with type 1 diabetes, although 10% to 30% of cases occur in patients with type 2 diabetes 5, in situations of extreme physiologic stress or acute illness. According to the morbidity and mortality review of the Centers for Disease Control and Prevention (CDC), diabetes itself is one of the most common chronic conditions in the world and affects an estimated 30 million people in the United States. Age-adjusted diabetic ketoacidosis hospitalization rates were on the downward trend in the 2000s but have steadily been increasing from there after till the mid-2010s at an average annual rate of 6.3% 6, while there has been a decline in in-hospital case-fatality rates during this period.
Alcoholic ketoacidosis occurs in patients with chronic alcohol abuse. Patients can have a long-standing history of alcohol use and may also present following binges. Acetic acid is a product of metabolism of alcohol and also a substrate for ketogenesis. The conversion to acetyl CoA and subsequent entry into various pathways or cycles, one of which is the ketogenesis pathway is determined by the availability of insulin in proportion to the counter-regulatory hormones. The prevalence of alcoholic ketoacidosis correlates with the incidence of alcohol abuse without racial or gender differences in incidence. It can occur at any age and mainly in chronic alcoholics but rarely in binge drinkers 7.
Under normal conditions, cells rely on free blood glucose as the primary energy source, which is regulated with insulin, glucagon, and somatostatin. As the name implies, starvation ketoacidosis is a bodily response to prolonged fasting hypoglycemia, which decreases the insulin secretion, shunting the biochemistry towards lipolysis and the oxidation of the by-product fatty acids to ensure a fuel source for the body. For starvation ketosis, mild ketosis generally develops after a 12- to 14-hour fast and if there is no food source, as in the case of extreme socio-economic deprivation or eating disorders; this will cause the body’s biochemistry to transform from ketosis to ketoacidosis progressively as described below. It can be seen in cachexia due to underlying malignancy, patients with postoperative or post-radiation dysphagia and prolonged poor oral intake.
How do I avoid ketonuria?
High levels of ketones can be avoided by maintaining good control of blood glucose levels. For those who are insulin dependent, remembering to inject at the appropriate times can help to avoid ketone build up.
People at a higher risk of ketonuria, such as those with type 1 diabetes, are advised to monitor their blood glucose levels, and ketone testing may also be recommended.
Ketonuria symptoms
Symptoms of ketone build up include:
- Thirst
- Regular urination
- Nausea
- Dehydration
- Heavy breathing
- Dilated pupils
- Mental confusion (rare)
- Breath may also smell of fruit
Ketonuria treatment
As ketonuria tends to develop as a result of insufficient insulin, you may need to take extra insulin depending on the level of ketones. If you have a ketone level over 1.6 mmol/L, it is worth contacting your health team for advice.
- Allison MG, McCurdy MT. Alcoholic metabolic emergencies. Emerg. Med. Clin. North Am. 2014 May;32(2):293-301[↩]
- Krebs HA, Freedland RA, Hems R, Stubbs M. Inhibition of hepatic gluconeogenesis by ethanol. Biochem. J. 1969 Mar;112(1):117-24[↩]
- The Art and Science of Low Carbohydrate Living An Expert Guide to Making the Life-Saving Benefits of Carbohydrate Restriction Sustainable and Enjoyable by Jeff S Volek, PhD, RD and Stephen D Phinney, MD, PhD. May 19, 2011[↩]
- Newcomer JW. Second-generation (atypical) antipsychotics and metabolic effects: a comprehensive literature review. CNS Drugs. 2005;19 Suppl 1:1-93[↩]
- Nyenwe EA, Kitabchi AE. The evolution of diabetic ketoacidosis: An update of its etiology, pathogenesis and management. Metab. Clin. Exp. 2016 Apr;65(4):507-21[↩]
- Benoit SR, Zhang Y, Geiss LS, Gregg EW, Albright A. Trends in Diabetic Ketoacidosis Hospitalizations and In-Hospital Mortality – United States, 2000-2014. MMWR Morb. Mortal. Wkly. Rep. 2018 Mar 30;67(12):362-365[↩]
- Alcoholic Ketoacidosis. Howard RD, Bokhari SRA. StatPearls [Internet]. StatPearls Publishing; Treasure Island (FL): Dec 18, 2018.[↩]





{kind=link}