Contents
What is kidney cyst
Simple kidney cysts are abnormal, fluid-filled sacs that form in the kidneys 1. Simple kidney cysts are different from the cysts that develop when a person has polycystic kidney disease, which is a genetic disorder. Simple cysts are usually unilateral and solitary lesions with well-defined features. Simple kidney cysts do not enlarge the kidneys, replace their normal structure, or cause reduced kidney function like cysts do in people with polycystic kidney disease.
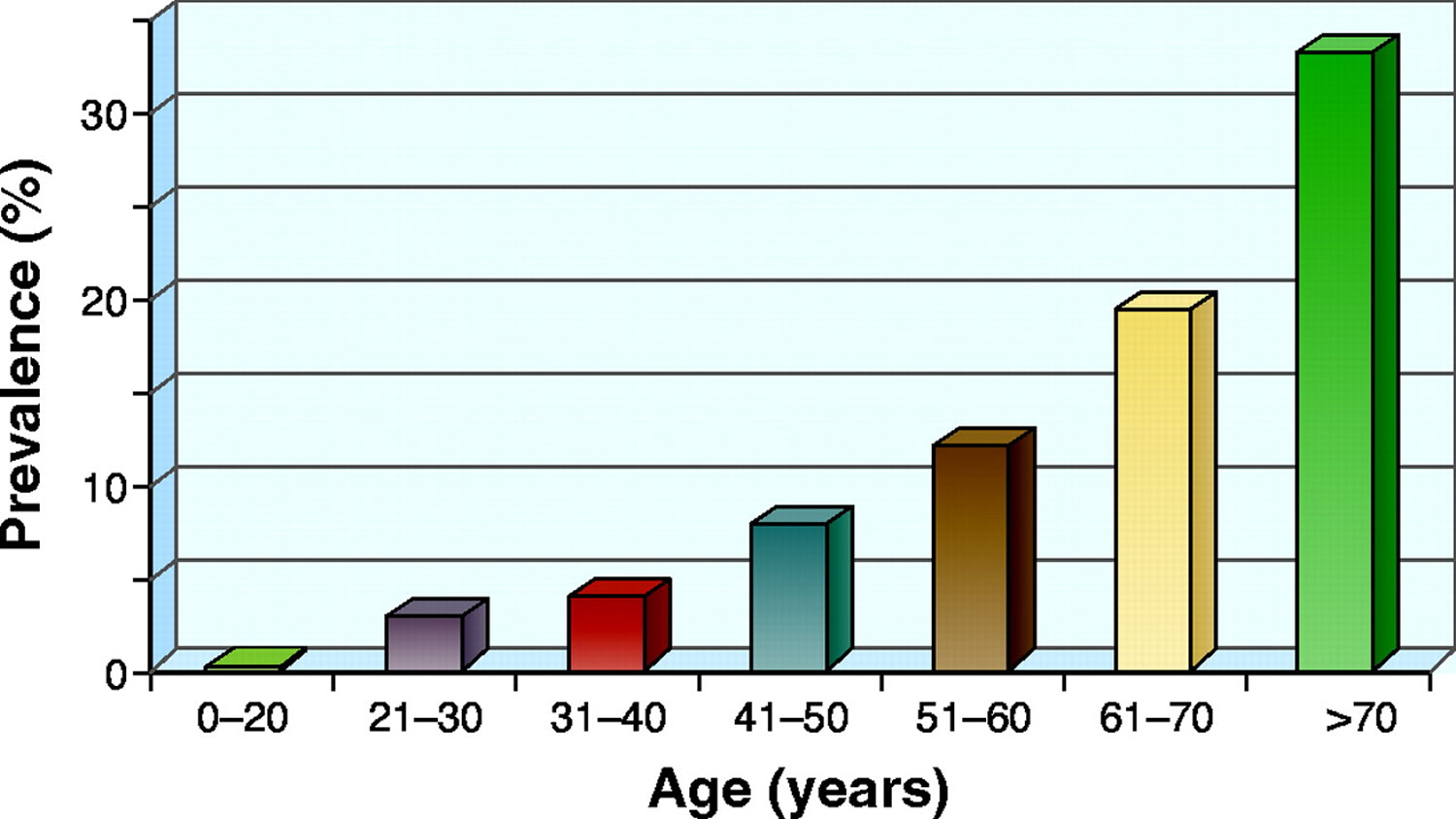
Simple cysts may be present at birth. Ultrasonography on approximately 30,000 fetuses in succession revealed an incidence of 0.09%, in most of whom the cysts resolved by birth 2. Only two of them persisted as simple benign cysts and in a third case heralded a unilateral multicystic dysplastic kidney. Between birth and 20 yr of age, the occurrence of new cysts is very rare but thereafter begins to increase in frequency, with an increased male-to-female ratio of approximately 2:1 in some studies 3. The reported overall prevalence of simple cysts is variable. Depending on the population and method of study, reported prevalences range from 5 to 41% but are likely in the range of 7 to 10%. Older autopsy studies reported their presence in 3 to 5% of cases 4.
Simple kidney cysts are more common as people age. An estimated 25 percent of people 40 years of age and 50 percent of people 50 years of age have simple kidney cysts 5.
Complications of simple kidney cysts are rare with a reported range of 2 to 4% 6. The principal complications are hemorrhage, infection, or rupture.
Figure 1. Age-related prevalence of simple kidney cysts
What causes simple kidney cysts ?
The cause of simple kidney cysts is not fully understood. Obstruction of tubules—tiny structures within the kidneys that collect urine—or deficiency of blood supply to the kidneys may play a role. Diverticula—sacs that form on the tubules—may detach and become simple kidney cysts. The role of genetic factors in the development of simple kidney cysts has not been studied.
What are the symptoms of simple kidney cysts ?
Simple kidney cysts usually do not cause symptoms or harm the kidneys. In some cases, however, pain can occur between the ribs and hips when cysts enlarge and press on other organs. Sometimes cysts become infected, causing fever, pain, and tenderness. Simple kidney cysts are not thought to affect kidney function, but one study found an association between the presence of cysts and reduced kidney function in hospitalized people younger than 60 years of age 5. Some studies have found a relationship between simple kidney cysts and high blood pressure. For example, high blood pressure has improved in some people after a large cyst was drained. However, this relationship is not well understood 8.
How are simple kidney cysts diagnosed ?
Most simple kidney cysts are found during imaging tests done for other reasons. When a cyst is found, the following imaging tests can be used to determine whether it is a simple kidney cyst or another, more serious condition. These imaging tests are performed at an outpatient center or hospital by a specially trained technician, and the images are interpreted by a radiologist—a doctor who specializes in medical imaging. Ultrasound may also be performed in a health care provider’s office. Anesthesia is not needed though light sedation may be used for people with a fear of confined spaces who undergo magnetic resonance imaging (MRI).
Ultrasound. Ultrasound uses a device, called a transducer, that bounces safe, painless sound waves off organs to create an image of their structure. An abdominal ultrasound can create images of the entire urinary tract. The images can be used to distinguish harmless cysts from other problems.
Simple kidney cysts are best defined using sonographic criteria. These include 9:
- Absence of internal echoes,
- Posterior enhancement,
- Round/oval shape and
- Sharp, thin posterior walls.
When all of the criteria are met, the cyst is benign and no follow-up is required.
Computerized tomography (CT) scan. CT scans use a combination of x-rays and computer technology to create three-dimensional (3-D) images. A CT scan may include the injection of a special dye, called contrast medium. CT scans require the person to lie on a table that slides into a tunnel-shaped device where the x-rays are taken. CT scans can show cysts and tumors in the kidneys.
Magnetic resonance imaging (MRI). MRI machines use radio waves and magnets to produce detailed pictures of the body’s internal organs and soft tissues without using x-rays. An MRI may include the injection of contrast medium. With most MRI machines, the person lies on a table that slides into a tunnel-shaped device that may be open ended or closed at one end; some newer machines are designed to allow the person to lie in a more open space. Like CT scans, MRIs can show cysts and tumors.
How are simple kidney cysts treated ?
Treatment is not needed for simple kidney cysts that do not cause any symptoms. Simple kidney cysts may be monitored with periodic ultrasounds.
Simple kidney cysts that are causing symptoms or blocking the flow of blood or urine through the kidney may need to be treated using a procedure called sclerotherapy. In sclerotherapy, the doctor punctures the cyst using a long needle inserted through the skin. Ultrasound is used to guide the needle to the cyst. The cyst is drained and then filled with a solution containing alcohol to make the kidney tissue harder. The procedure is usually performed on an outpatient basis with a local anesthetic.
If the cyst is large, surgery may be needed. Most surgeries can be performed using a laparoscope—a special tool with a small, lighted video camera. The procedure is usually done under general anesthesia in a hospital. The surgeon drains the cyst and then removes or burns away its outer tissue. This type of surgery allows for a smaller incision and quicker recovery.
Eating, Diet, and Nutrition
Eating, diet, and nutrition have not been shown to play a role in causing or preventing simple kidney cysts.
What is complex kidney cyst
Kidney cysts can be easily identified by means of diagnostic imaging methods and in many cases it is not necessary to resource to histopathological analysis 10. Renal cysts, in general, may be classified as “simple” or “complex.” “Simple” cysts are best defined using sonographic criteria (see above Simple Kidney Cyst diagnosis). Ultrasonography is helpful for simple cyst identification, but provides limited information with increasingly complex kidney cysts and solid masses. Complex kidney cysts or kidney cyst with solid components require a more detailed characterization to allow the determination of differential diagnoses and therapeutic approach and prognostic evaluation 11.
Because of such a necessity, Bosniak, in 1986 10, developed a classification system based on computed tomography (CT) imaging criteria allowing for the analysis of renal cysts’ contour and contents, presence of septations and/or calcifications, and enhancement after contrast agent injection. The Bosniak classification of renal cysts on the basis of their appearance and enhancement on CT is widely accepted by urologists and radiologists for the diagnosis, evaluation, and management of kidney cystic lesions. Whether labeled simple or complex or however reported radiologically, the terms used all are descriptive. Whenever concern of their association with neoplasms exists, a final diagnosis can be made only with histologic examination. Approximately 40 to 60% of class III and 85 to 100% of class IV cysts prove to be malignant 12, 13, 14.
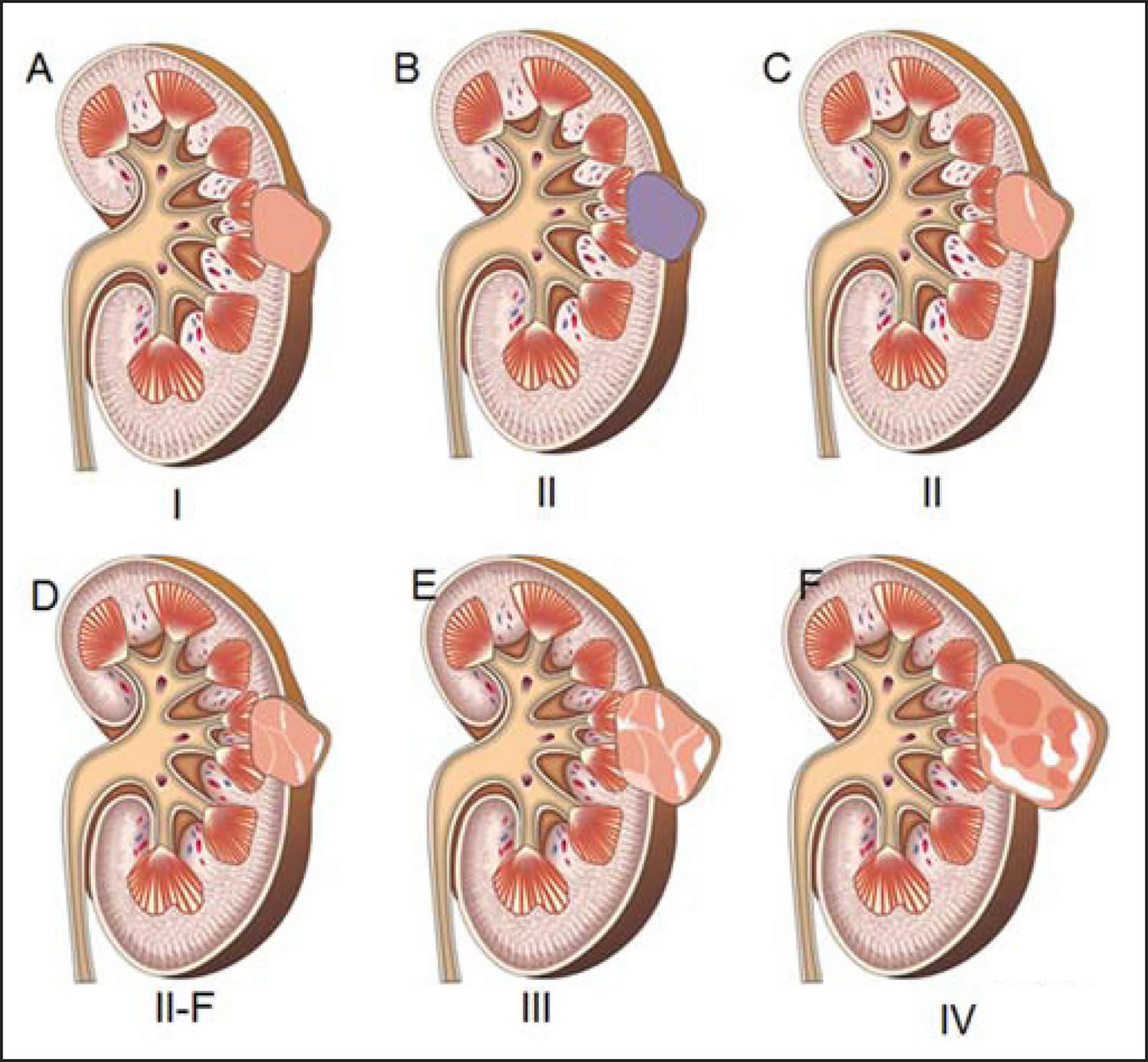
The Bosniak system consists of four categories based on triphasic CT findings, ranging from simple to complex cysts 15, as follows:
Table 1. The Bosniak classification of renal cystic disease
Category I: Malignant risk less than 1%; no follow-up required
|
Category II: Malignant risk less than 3%; no follow-up requiredCystic lesion with some abnormal radiological features
|
Category IIF: Malignant risk 5-10%; follow-up recommendedCystic lesion with increased abnormal findings
|
Category III: Malignant risk 40-60%; surgical excision recommendedMore complicated
|
Category IV: Malignant risk greater than 80%; surgical excision recommended
|
CATEGORY I
Simple kidney cysts (see Simple Kidney Cyst above) have no malignant potential and, as such, no follow-up is required.
CATEGORY II
Like those classified as category I, kidney cystic lesions classified as category II are also considered benign, but with a minimally complicated appearance. Such lesions may present with thin septations, thickness < 1 mm, besides small (1-2 mm), linear, parietal or septal calcifications 17.
In spite of being considered benign lesions 18, there are reports in the literature about rare renal lesions classified into category II, and identified as malignant and potentially malignant according anatomopathological analysis. In such cases, it is possible that the lesions’ characteristics have not been completely described, impairing an appropriate classification of the lesions. Also, other extremely rare cases of renal cell carcinomas on the walls of benign cysts are included in this context 19.
Thus, the differentiation of more complex lesions from those classified as (non surgical) category II makes the diagnosis more difficult, with greater interobserver variation, although it is extremely important since the prognosis and therapeutic approach to be adopted are different in such cases 20.
CATEGORY IIF
In 1993, Bosniak reviewed his original classification to include category IIF 21 for a group of minimally complicated cysts which do not fulfill the characteristics required to be included in category III, but are more complex than those included in category II. Their differentiation is subjective and difficult, with great interobserver variability, but it is essential, considering the different therapeutic approaches 22. Kidney lesions classified as category IIF are primarily benign, but their complexity requires serial follow-up (“F” for follow-up) to rule out (or not) the presence of malignancy 23. The appropriate follow-up time for determining IF a lesion is really benign is still to be established 24 and varies in the literature. Some authors report the beginning of the follow-up 6 months after the initial evaluation, in association with an annual routine for a minimum of 5 years 21, while others support a follow-up at 3, 6 and 12 months after the initial evaluation, in association with an annual routine 25. Such a radiological follow-up has shown to be a safe strategy, avoiding surgical intervention in 95% of cases 24.
Combined ultrasound and magnetic resonance imaging (MRI) should be considered in the follow-up of these patients, particularly for those under the age of 50, to reduce the exposition of such patients to radiation along the years 24. A lesion category IIF which does not present increase or morphological alterations is probably benign, despite the fact that the lesion growth rate is not taken into consideration in the Bosniak classification, and the radiologist should evaluate principally the morphological alterations 11.
CATEGORY III
Such lesions constitute really indeterminate renal findings, with a wide variety of aspects whose differentiation between malignant and benign cannot be reliably made by imaging methods. They present wall thickening and contrast-enhanced, irregular and thick septations, either with or without calcifications11 and may be demonstrated as multilocular cysts (whose walls present with linear fibrosis), hemorrhagic or infected cysts, multilocular cystic nephromas (containing blastemas cells), or cystic renal cell carcinomas. Therefore, there is a significant risk for malignancy 11.
The prevalence of malignancy among resected lesions classified as category III ranges from 31% to 100% 11, while other studies report a rate of malignancy between 40% and 60%. Such variations are due to the way the radiologist establishes the category, to the philosophy and preferential practice of the urologist who is treating the patient with indeterminate lesions 11.
CATEGORY IV
Occasionally, the differentiation between lesions in categories III and IV may be difficult, but it is not essential since both categories require surgery, despite the difference in the operative approach 26. Lesions in this category are cystic neoplasms which may present imaging findings similar to those of category III (wall thickening or gross and nodular septal thickening), but contrast-enhanced solid components are still observed adjacent to the lesion wall or septa. Until proven otherwise, such lesions are considered renal cell cancer with eminently surgical indication, since they are malignant in 95-100% of cases 11.
Summary of kidney cysts
There are no randomized controlled trials with regards to follow-up or management of kidney cystic masses, as such, the recommendations are primarily expert opinion 16.
At this time, category I and II renal cysts, do not require further imaging or follow-up. Patients in Category IIF, because of the approximate 5% malignant risk, do require periodic imaging. (There is no consensus or evidence based interval determined for follow-up imaging.) Combination of ultrasound and MRI should be considered as follow-up for Bosniak IIF and reduces the lifetime radiation dose (once the lesion has been characterized by triphasic CT scan) in patients younger than 50 years. For Category III (50% malignant risk) and category IV (75% to 90% malignant risk), surgical excision is recommended. Although MRI may add further information, it should be used as an adjunct to CT scans in difficult cases.
- Simple Kidney Cysts. National Institute of Diabetes and Digestive and Kidney Diseases. https://www.niddk.nih.gov/health-information/kidney-disease/simple-kidney-cysts[↩]
- Blazer S, Zimmer EZ, Blumenfeld Z, Zelikovic I, Bronshtein M :Natural history of simple renal cysts detected in pregnancy. J Urol 162: 812–814, 1999. https://www.ncbi.nlm.nih.gov/pubmed/10458386[↩]
- Al-Said J, O’Neill C:Reduced kidney size in patients with simple renal cysts. Kidney Int 64: 1059–1064, 2003. https://www.ncbi.nlm.nih.gov/pubmed/12911557[↩]
- Allen AC . The Kidney: Medical and Surgical Diseases, 2nd Ed., New York, Grune & Stratton, 1962, p 1297.[↩]
- Torres VE, Grantham JJ. Cystic diseases of the kidney. In: Brenner BM, ed. Brenner & Rector’s The Kidney. Vol. 2. 8th ed. Philadelphia: Saunders Elsevier; 2008: 1451–1453.[↩][↩]
- Bisceglia M, Galliani CA, Senger C, Stallone C, Sessna A :Renal cystic diseases: A review. Adv Anat Pathol 13: 26–56, 2006. https://www.ncbi.nlm.nih.gov/pubmed/16462154[↩]
- A Clinical View of Simple and Complex Renal Cysts. JASN September 1, 2009 vol. 20 no. 9 1874-1876. http://jasn.asnjournals.org/content/20/9/1874.long[↩]
- Zerem E, Imamovic G, Omerovic S. Simple renal cysts and arterial hypertension: does their evacuation decrease the blood pressure. Journal of Hypertension. 2009;27(10):2074–2078.[↩]
- Weber TM. Sonography of benign renal cystic disease. Ultras Clin. 2006;1:15–24.[↩]
- The current radiological approach to renal cysts. Bosniak MA. Radiology. 1986 Jan; 158(1):1-10. https://www.ncbi.nlm.nih.gov/pubmed/3510019/[↩][↩]
- Management of the incidental renal mass. Silverman SG, Israel GM, Herts BR, Richie JP. Radiology. 2008 Oct; 249(1):16-31. https://www.ncbi.nlm.nih.gov/pubmed/18796665/[↩][↩][↩][↩][↩][↩][↩]
- Bisceglia M, Galliani CA, Senger C, Stallone C, Sessna A. :Renal cystic diseases: A review. Adv Anat Pathol 13: 26–56, 2006. https://www.ncbi.nlm.nih.gov/pubmed/16462154[↩]
- Glassberg KI :Renal dysgenesis and cystic disease of the kidney. In: Campbell-Walsh Urology, 9th Ed., edited by Wein AJ, Kavousi LR, Novick AC, Partin WA, Peters CA Philadelphia, W.B. Saunders, 2007, pp 3343–3348.[↩]
- Hartman DS, Choyke PL, Hartman MS :A practical approach to the cystic renal mass. Radiographics 24: S101–S115, 2004. https://www.ncbi.nlm.nih.gov/pubmed/15486234[↩]
- How I do it: evaluating renal masses. Israel GM, Bosniak MA. Radiology. 2005 Aug; 236(2):441-50. https://www.ncbi.nlm.nih.gov/pubmed/16040900/[↩]
- Whelan TF. Guidelines on the management of renal cyst disease. Canadian Urological Association Journal. 2010;4(2):98-99. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2845761/[↩][↩]
- An update of the Bosniak renal cyst classification system. Israel GM, Bosniak MA. Urology. 2005 Sep; 66(3):484-8. https://www.ncbi.nlm.nih.gov/pubmed/16140062/[↩]
- Calcification in cystic renal masses: is it important in diagnosis? Israel GM, Bosniak MA. Radiology. 2003 Jan; 226(1):47-52. https://www.ncbi.nlm.nih.gov/pubmed/12511667/[↩]
- Laparoscopic partial nephrectomy for cystic masses. Spaliviero M, Herts BR, Magi-Galluzzi C, Xu M, Desai MM, Kaouk JH, Tucker K, Steinberg AP, Gill IS. J Urol. 2005 Aug; 174(2):614-9. https://www.ncbi.nlm.nih.gov/pubmed/16006923/[↩]
- Follow-up CT of moderately complex cystic lesions of the kidney (Bosniak category IIF). Israel GM, Bosniak MA. AJR Am J Roentgenol. 2003 Sep; 181(3):627-33. https://www.ncbi.nlm.nih.gov/pubmed/12933451/[↩]
- Problems in the radiologic diagnosis of renal parenchymal tumors. Bosniak MA. Urol Clin North Am. 1993 May; 20(2):217-30. https://www.ncbi.nlm.nih.gov/pubmed/8493746/[↩][↩]
- Bosniak category IIF and III cystic renal lesions: outcomes and associations. Smith AD, Remer EM, Cox KL, Lieber ML, Allen BC, Shah SN, Herts BR. Radiology. 2012 Jan; 262(1):152-60. https://www.ncbi.nlm.nih.gov/pubmed/22106359[↩]
- Complex cystic renal masses: characterization with contrast-enhanced US. Ascenti G, Mazziotti S, Zimbaro G, Settineri N, Magno C, Melloni D, Caruso R, Scribano E. Radiology. 2007 Apr; 243(1):158-65. https://www.ncbi.nlm.nih.gov/pubmed/17392251/[↩]
- Guidelines on the management of renal cyst disease. Whelan TF. Can Urol Assoc J. 2010 Apr; 4(2):98-9. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2845761/[↩][↩][↩]
- A clinical view of simple and complex renal cysts. Eknoyan G. J Am Soc Nephrol. 2009 Sep; 20(9):1874-6. http://jasn.asnjournals.org/content/20/9/1874.long[↩]
- Evaluation of cystic renal masses: comparison of CT and MR imaging by using the Bosniak classification system. Israel GM, Hindman N, Bosniak MA. Radiology. 2004 May; 231(2):365-71. https://www.ncbi.nlm.nih.gov/pubmed/15128983/[↩]





{kind=link}