Contents
What is a laminectomy
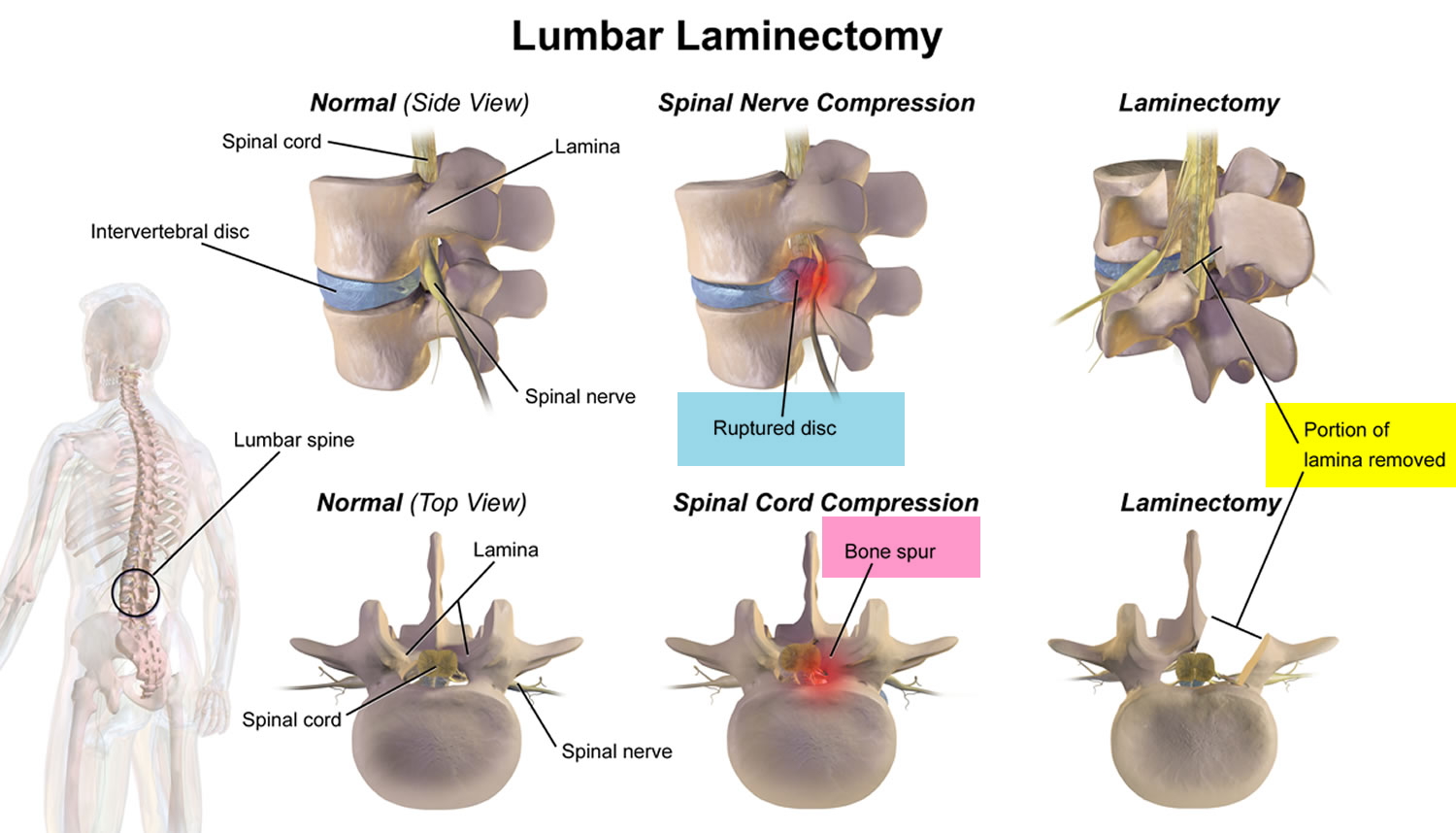
A laminectomy is a surgery on your back or neck to remove the lamina (see Figures 1 to 6 below), the back part of a vertebra that covers your spinal canal. Laminectomy opens up your spinal canal so your spinal nerves have more room. Laminectomy may be done along with a diskectomy, foraminotomy, and spinal fusion. Laminectomy also known as decompression surgery, laminectomy enlarges your spinal canal to relieve pressure on the spinal cord or nerves. A laminectomy is done if your spinal cord or the nerves of the spine are compressed. The pressure might be due to problems with your bones, your joints or the discs in your spine, which can occur in people who have arthritis in their spines. These overgrowths are sometimes referred to as bone spurs, but they’re a normal side effect of the aging process in some people. The pressure may also be due to other problems such as an injury, infection or tumor. The pressure might cause numbness, tingling or pain in the arms or legs. Laminectomy is designed to stop pressure on your spinal cord or on the spinal nerves in your neck or back. Laminectomy may also be done to remove bone spurs in your spine.
Laminectomy is generally used only when more-conservative treatments — such as medication, physical therapy or injections have failed to relieve symptoms. Laminectomy may also be recommended if symptoms are severe or worsening dramatically.
Before a laminectomy is done, your doctor will first look into the reason for the spinal cord or the spinal nerves pressure and will carry out a scan, such as an MRI or CT scan. The doctor will also examine your spine, muscle strength, reflexes and sense of feeling.
Pressure on the spinal cord or nerves can cause problems such as:
- numbness, cramping or pain in your back, neck, arms or legs
- weakness in the arm or leg
- difficulty or poor balance when walking
- problems with bowel movement or urinating
If you have these problems there may be other treatments, such as physiotherapy and medication, that might be tried first before the surgeon considers that a laminectomy would be suitable for you.
Lumbar laminectomy
Lumbar laminectomy is a surgical procedure to relieve discomfort, cramps, pain, tingling and numbness in the buttocks or legs caused by pressure on the spinal cord, the cauda equina or spinal nerve roots.
The aim of surgery is to remove the pressure by opening the spinal canal and widening it from the back. The surgeon removes bone and other tissue pressing on the affected nerves, providing more space for the nerves and reducing irritation and inflammation.
Laminectomies are typically performed to treat lumbar spinal stenosis. This is a narrowing of the spinal canal that contains the spinal cord and the spinal nerves that arise from the spinal cord, as shown in Figure 2 below. At the lumbar level of L1, the spinal cord becomes a nerve bundle called the cauda equina.
Other treatment for spinal problems
Even with signs of spinal nerve pressure, such as sciatica, recovery without any treatment may occur. Alternative treatment to surgery isn’t always possible, but generally should be tried first.
Other treatment options may include:
- stabilization exercises
- stretching and strengthening exercises
- cortisone injections
- non-steroidal anti-inflammatory drugs (NSAIDS) or a course of oral steroids
- training on how to safely use your back (such as proper lifting techniques)
- physiotherapy
- switching to ergonomic furniture.
Discectomy (removal of the disc) without laminectomy may also be an option, and this can sometimes be done as day surgery as a lumbar microdiscectomy.
Key points
- A laminectomy is a surgical incision into the backbone to obtain access to the spinal cord.
- One of the most common reasons for laminectomy is a prolapsed or herniated intervertebral disc.
- Occasionally, the operation doesn’t work and the original symptoms remain.
- At other times, the operation isn’t expected to relieve symptoms, but is performed to prevent the area from deteriorating further.
Why is laminectomy done
Bony overgrowths within the spinal canal can narrow the space available for your spinal cord and nerves. This pressure can cause pain, weakness or numbness that can radiate down your arms or legs.
Because the laminectomy restores spinal canal space but does not cure you of arthritis, it more reliably relieves radiating symptoms from compressed nerves than it does back pain from spinal joints.
Your doctor may recommend laminectomy if:
- Conservative treatment, such as medication or physical therapy, fails to improve your symptoms
- You have muscle weakness or numbness that makes standing or walking difficult
- You experience loss of bowel or bladder control
In some situations, laminectomy may be necessary as part of surgery to treat a herniated spinal disk. Your surgeon may need to remove part of the lamina to gain access to the damaged disk.
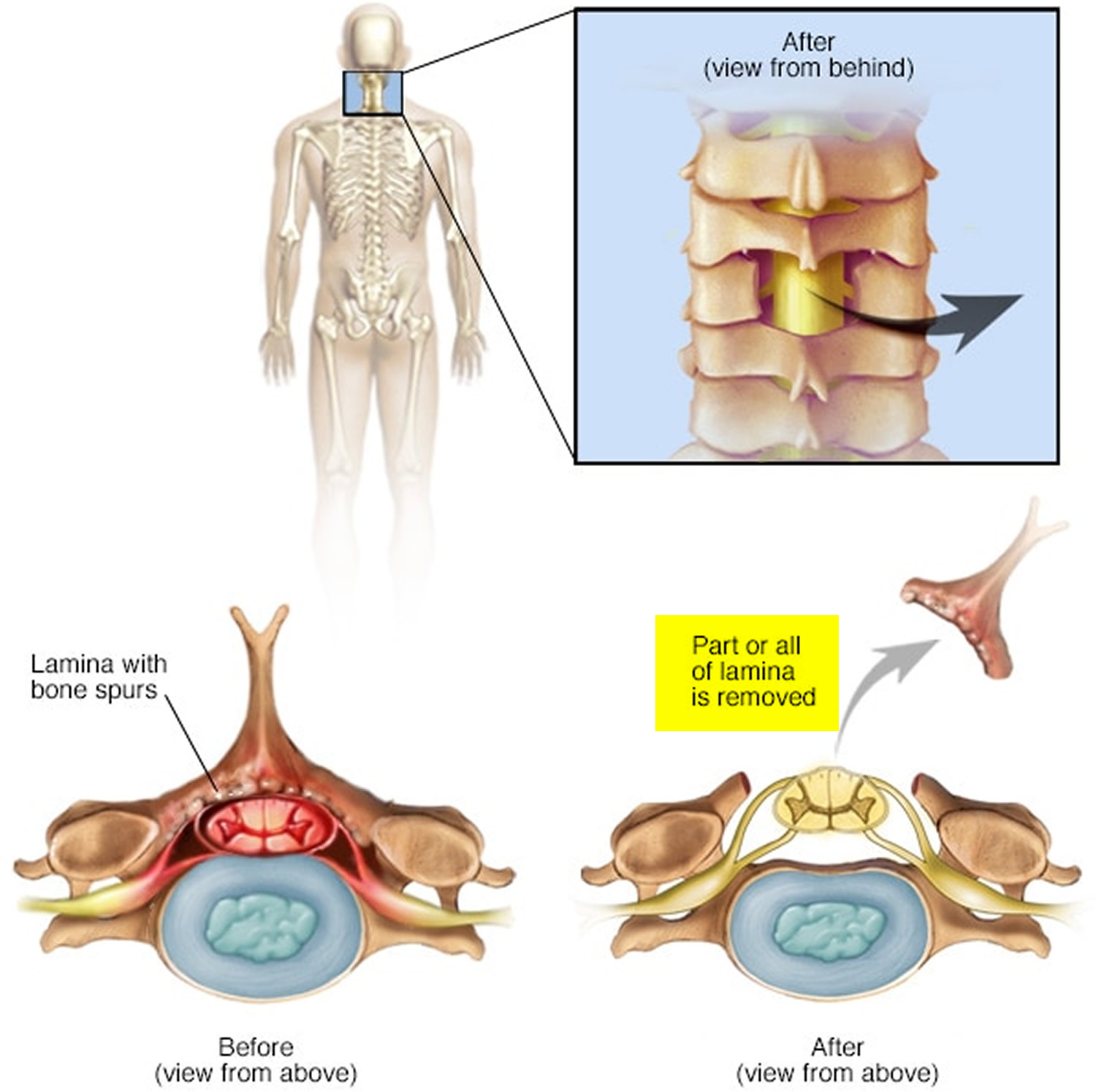
Figure 1. Vertebral lamina
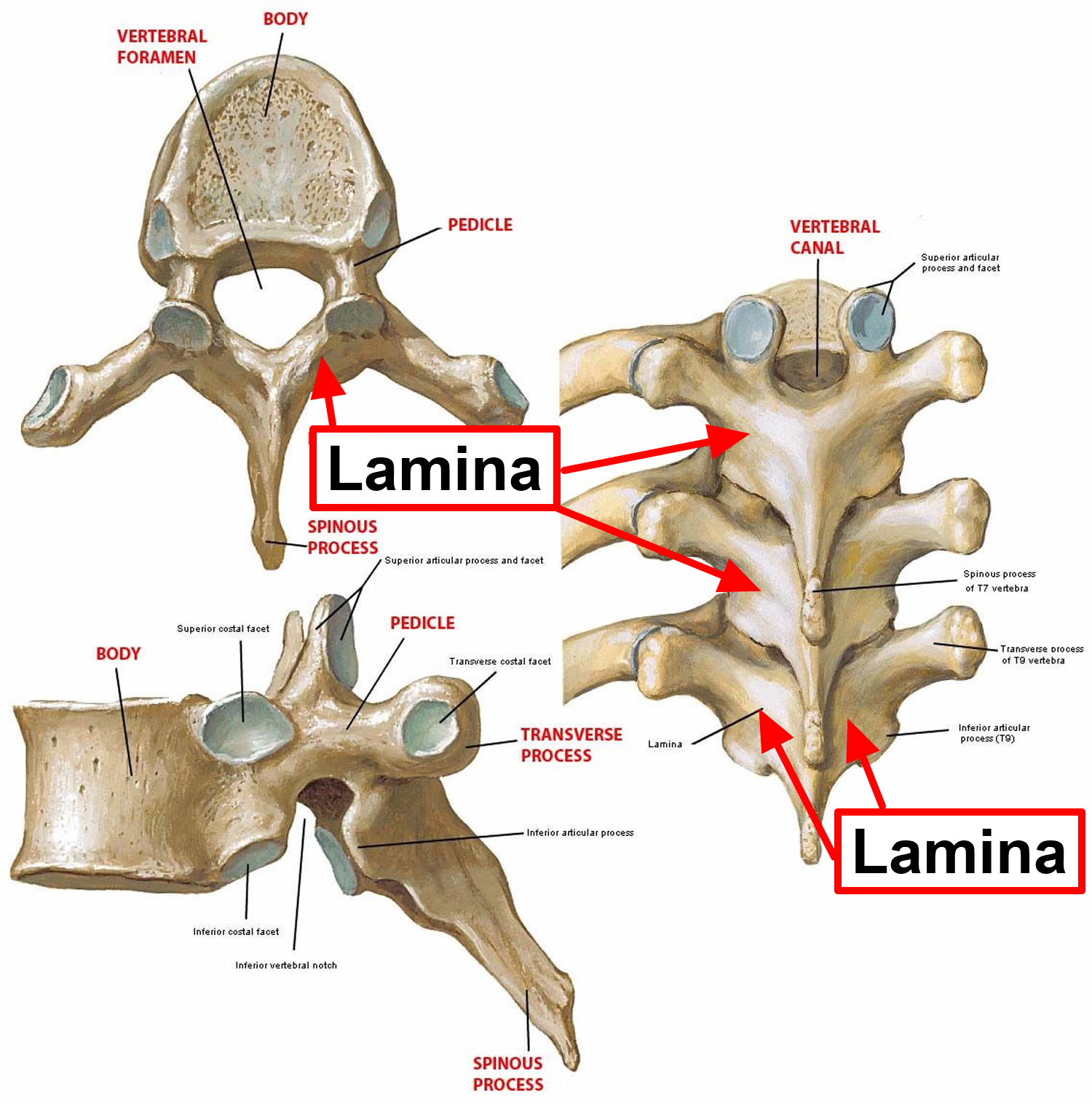
Figure 2. Lumbar laminectomy – a lumbar laminectomy involves the removal of the back portion of a vertebra in your lower back to create more room within the spinal canal.
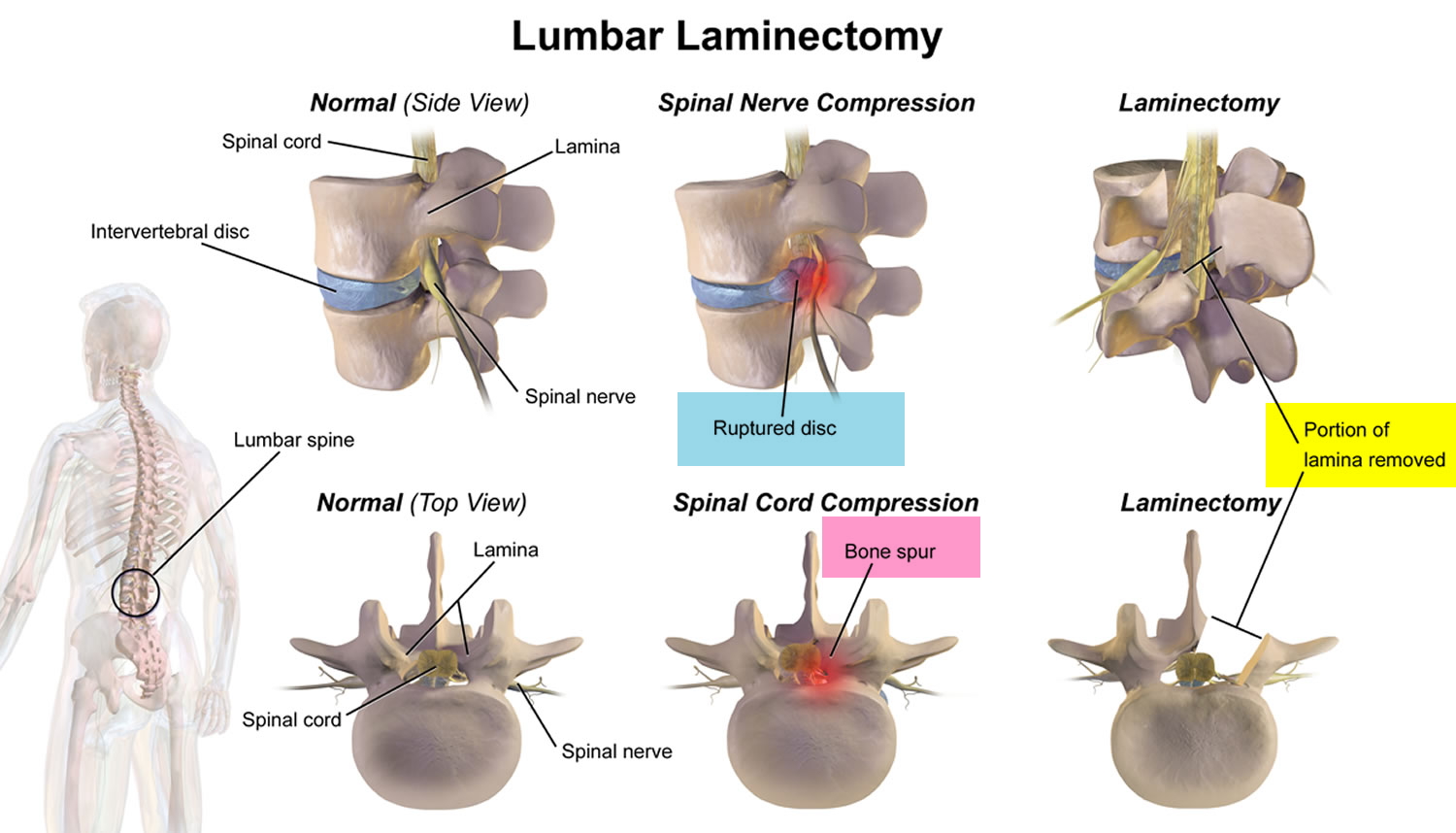
Figure 3. Spinal cord
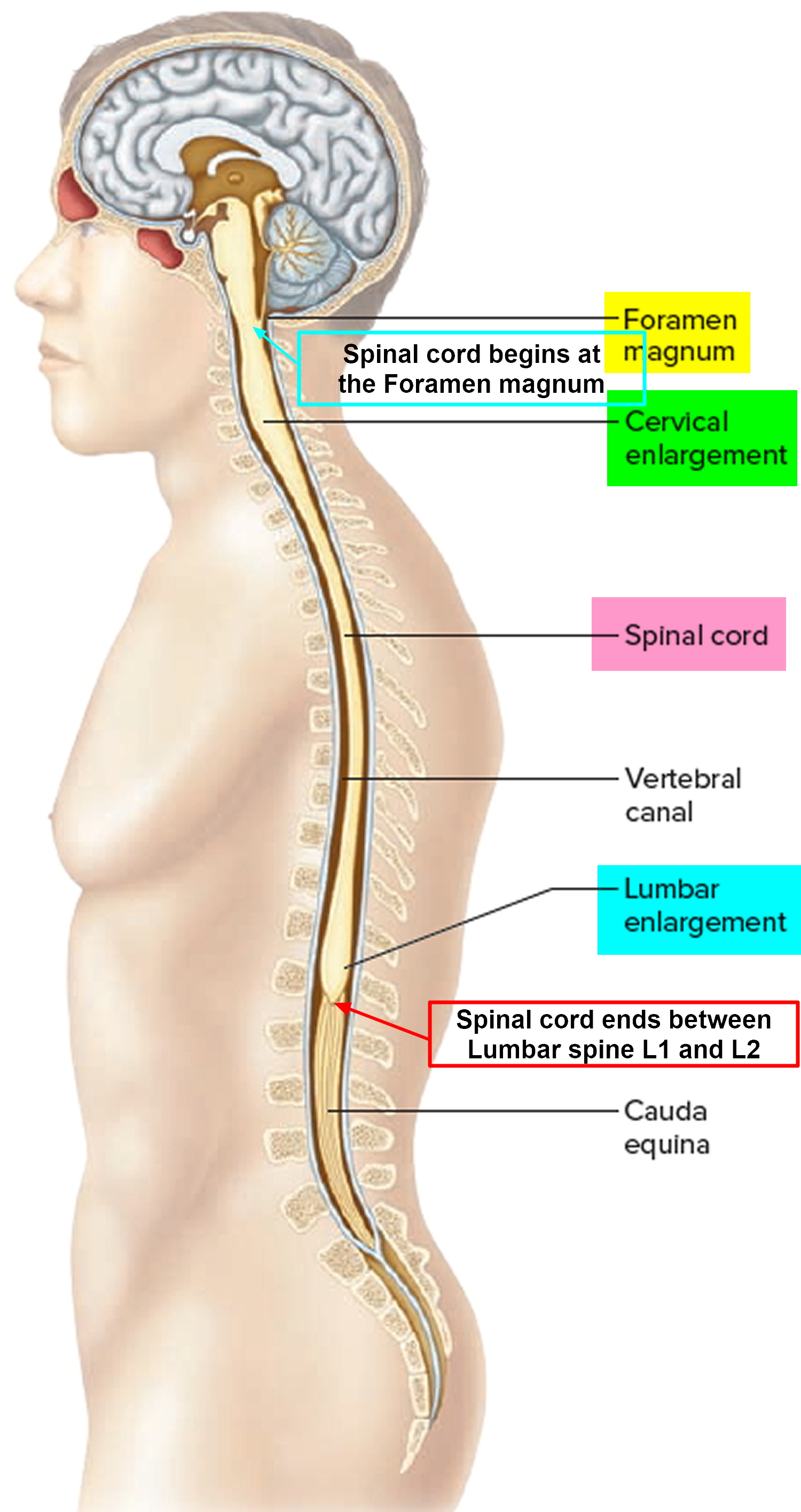
Figure 4. Spinal cord anatomy
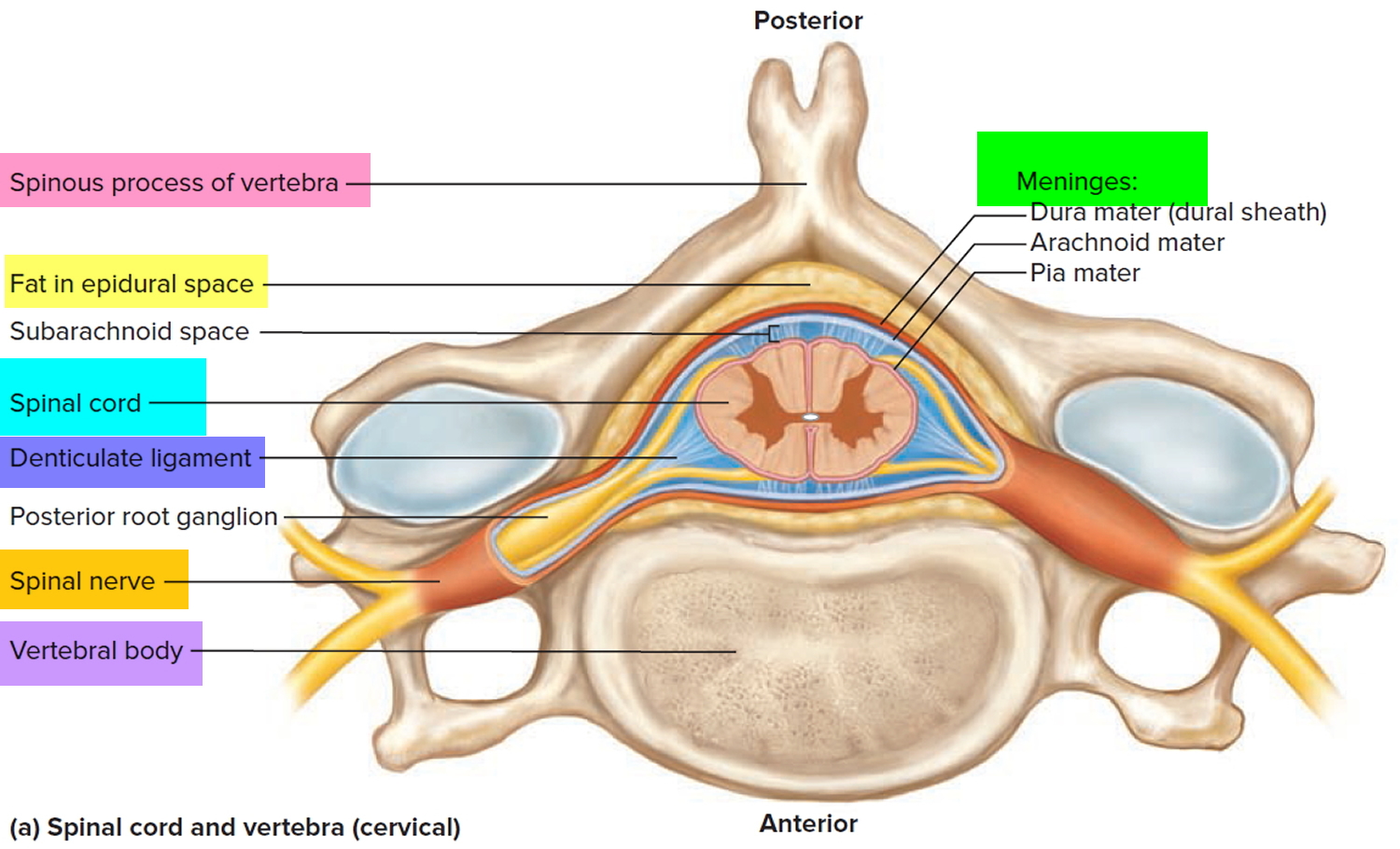
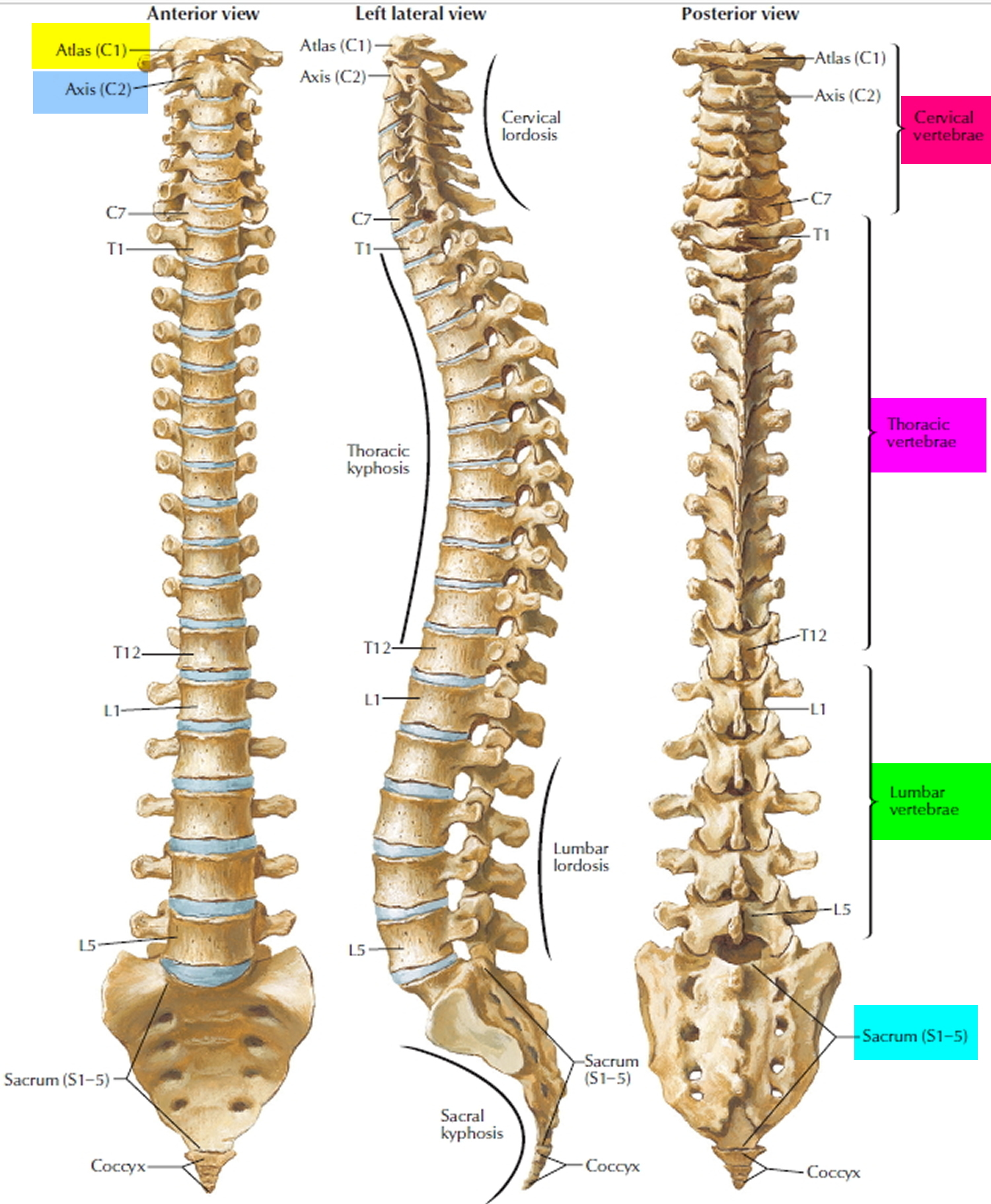
Figure 5. Vertebral column
Laminectomy complications
Laminectomy is generally a safe procedure. But as with any surgery, complications may occur. Potential complications include:
- Damage to a spinal nerve, causing pain, weakness, numbness or loss of feeling
- Spinal fluid leak, which can be repaired
- Paralysis, paraplegia or quadriplegia (depending on the site and severity of the spinal cord injury), which is very uncommon
- Bleeding – superficial or deep
- Infection or breakdown of the wound
- Blood clots in the legs
- Nerve injury
- Chest infection
- Damage to the dura (which covers the spinal cord) leading to leakage of spinal fluid
- Delayed instability.
The greatest risk of the surgery is that it might not work. People who have surgery for back pain don’t always feel better afterwards.
Laminectomy surgery
How you prepare
You’ll need to avoid eating and drinking for a certain amount of time before surgery. Your doctor can give you specific instructions about the types of medications you should and shouldn’t take before your surgery.
What happens during laminectomy
You will have a general anaesthetic, which means you will be unconscious and won’t feel any pain during the procedure.
Your surgical team will monitor your heart rate, blood pressure and blood oxygen levels throughout the procedure. After you’re unconscious and can’t feel any pain:
- The surgeon makes an incision in your neck or your back over the affected vertebrae and moves the muscles away from your spine as needed. Small instruments are used to remove the appropriate lamina. The size of the incision may vary depending on your condition and body size. Minimally invasive surgeries typically use smaller incisions than those used for open procedures.
- If laminectomy is being performed as part of surgical treatment for a herniated disk, the surgeon also removes the herniated portion of the disk and any pieces that have broken loose (diskectomy).
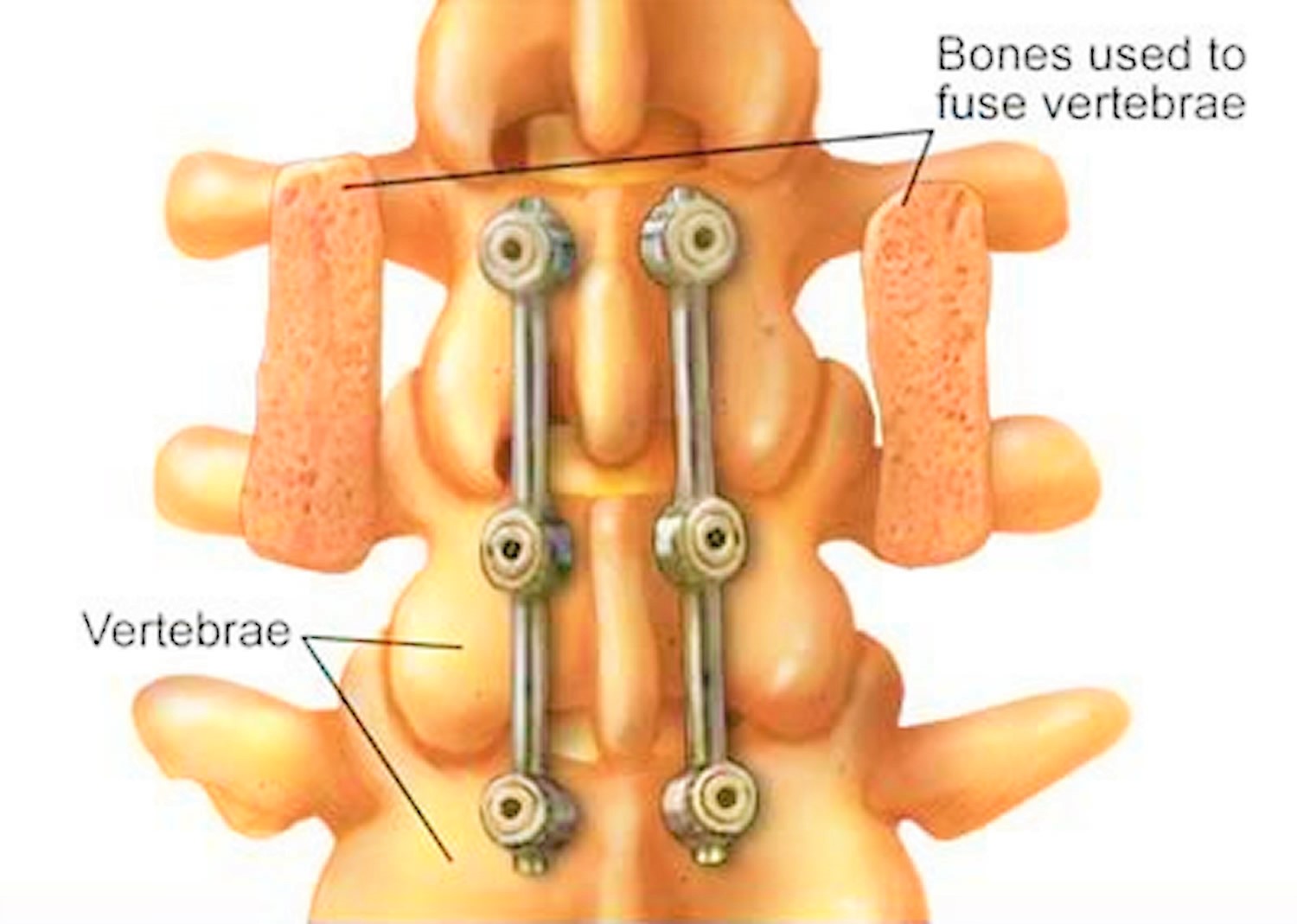
- If one of your vertebrae has slipped over another or if you have curvature of the spine, spinal fusion (join two or more vertebrae together) may be necessary to stabilize your spine. During spinal fusion, the surgeon permanently connects two or more of your vertebrae together using bone grafts and, if necessary, metal rods and screws to strengthen the spine after a laminectomy.
- Depending on your condition and individual needs, the surgeon may use a smaller (minimally invasive) incision and a special surgical microscope to perform the operation.
- Sometimes a small plastic tube will be put in to drain excess fluid. The tube will be removed a few days after surgery.
You should discuss all these possibilities beforehand.
Laminectomy recovery
After surgery, you’re moved to a recovery room where the health care team watches for complications from the surgery and anesthesia. You may also be asked to move your arms and legs. Your doctor may prescribe medication to relieve pain at the incision site.
You might go home the same day as the surgery, although some people may need few days hospital stay. Your doctor may recommend physical therapy, exercises or rehabilitation after a laminectomy to improve your strength and flexibility.
Depending on the amount of lifting, walking and sitting your job involves, you may be able to return to work within a few weeks. If you also have spinal fusion, your recovery time will be longer. Your doctor might also suggest that you protect your back from further stress by limiting lifting or heavy work.
Self-care after a laminectomy
Be guided by your doctor, but general suggestions include:
- Continue to take your medications as ordered, especially the full course of antibiotics.
- Avoid activities that strain the spine – such as sitting or standing for too long, flexing your spine, bending at the waist, climbing too many stairs or going for long trips in the car.
- Avoid wearing high-heeled shoes.
- Sleep on a firm mattress.
- Continue with any exercises you were shown in hospital. Gradually increase them, although if you develop pain, stop the activity.
- Beware of lifting, bending or twisting.
- Be guided by your physiotherapist and doctor as to what specific activities you can and can’t do, including walking and driving.
- Report any signs of infection to your doctor, such as wound redness or seeping, elevated temperature or persistent headaches.
Laminectomy results
Most people report measurable improvement in their symptoms after laminectomy, particularly a decrease in pain that radiates down the leg or arm. But this benefit may lessen over time if you have a particularly aggressive form of arthritis. Laminectomy is less likely to improve pain in the back itself.
Occasionally, laminectomy doesn’t work and the original symptoms remain. At other times, laminectomy isn’t expected to relieve symptoms, but is performed to prevent the area from deteriorating further. In this case, your original symptoms will probably remain, but not get any worse. Make sure to discuss your concerns and expectations with your doctor.
A regular exercise program following surgery is most important to increase your spinal muscle strength and flexibility, and to protect against future injury. This is usually started in hospital and continued as an outpatient.
Cervical laminectomy
Cervical laminectomy is a surgical procedures to treat symptoms of cervical nerve root or spinal cord compression. Cervical laminectomy is usually performed under general anaesthesia. Patients with cervical spinal cord compression will generally have these symptoms: neck stiffness; unilateral or bilateral deep, aching neck, arm and shoulder pain; and possibly stiffness or clumsiness while walking. Cervical spinal cord compression usually develops insidiously. In the early stages of cervical spinal cord compression, complaints of neck stiffness are common because of the presence of advanced cervical spondylosis 1. Other common complaints include crepitus in the neck with movement; brachialgia, which is characterized as a stabbing pain in the pre- or postaxial border of the arm, elbow, wrist or fingers; a dull “achy” feeling in the arm; and numbness or tingling in the hands. Cervical laminectomy can treat spinal canal stenosis, a narrowing of the spinal canal. Cervical laminectomy surgery can remove the pressure on nerves and spinal cord by opening the spinal canal and widening it. The surgeon creates more space around the spinal cord and the nerve roots. This may reduce inflammation and irritation.
In patients with a disc herniation between the sixth and seventh vertebrae, pain radiates into the shoulder, upper arm, elbow, and index and middle fingers. It is typically unilateral. Numbness and weakness follow the same distribution.
The hallmark symptom of cervical spinal cord compression is weakness or stiffness in the legs 1, 2. Patients with cervical spinal cord compression may also present with unsteadiness of gait. Weakness or clumsiness of the hands in conjunction with the legs is also characteristic of cervical spinal cord compression. Symptoms may be asymmetric particularly in the legs. Loss of sphincter control or frank incontinence is rare; however, some patients may complain of slight hesitancy on urination.
Common symptoms:
- Clumsy or weak hands
- Leg weakness or stiffness
- Neck stiffness
- Pain in shoulders or arms
- Unsteady gait
Common signs:
- Atrophy of the hand musculature
- Hyperreflexia
- Lhermitte’s sign (intermittent electric shock-like sensation down the center of the back following flexion of the neck)
- Sensory loss.
Spinal stenosis occurs mainly in older patients due to age-related changes such as:
- osteoarthritis of the spine and degenerative changes in cervical vertebrae
- enlargement of facet joints
- thickening of facet-joint tissue
- formation of bone spurs on a vertebra
- thickening, hardening and calcification of spinal ligaments
- thinning of intervertebral discs
- herniated or bulging discs
- forward displacement or “slippage” of one vertebra over another.
These conditions cause a decrease in space around the spinal nerves or spinal cord, increasing the risk of compression.
Other conditions that can lead to spinal stenosis include:
- rheumatoid arthritis of the spine
- epidural abscess
- spinal cord tumour
- Paget’s disease
- acute vertebral trauma
- congenital spinal stenosis
- scoliosis (curvature of the spine)
- achondroplasia (a hereditary condition).
Figure 6. Cervical laminectomy – a cervical laminectomy involves the removal of the back portion of a vertebra in your neck to create more room within the spinal canal.
Cervical spinal cord compression diagnosis
The physical and neurologic examination is used to confirm the presence of spinal cord dysfunction. Flexion of the neck may cause a generalized “electric shock-like” sensation down the center of the back, referred to as Lhermitte’s sign. Atrophy of the hands, particularly the intrinsic musculature, may be present.
Sensory abnormalities have a variable pattern on examination. Loss of vibratory sense or proprioception in the extremities (especially the feet) can occur. Superficial sensory loss may be asymmetric and persons are variably affected. The sensory examination may be confounded by the presence of diabetes mellitus and a concurrent peripheral neuropathy.
A characteristic physical finding of cervical spinal cord compression is hyperreflexia. The biceps and supinator reflexes (C5 and C6) may be absent, with a brisk triceps reflex (C7). This pattern is almost pathognomonic of cord compression because of cervical spondylosis at the C5-C6 interspace 3. Ankle clonus and Babinski’s sign (pathologic extension of the great toe elicited by stroking the foot) in the feet may also be revealed. Hoffmann’s sign (a reflex contraction of the thumb and index finger after nipping the middle finger) is a subtle indicator of spinal cord dysfunction. A stiff or spastic gait is also characteristic of cervical spinal cord compression in its later stages.
When cervical spondylosis is isolated to the C6-7, C7-T1 spinal levels, the arm reflexes may be normal. A hyperactive pectoralis muscle reflex elicited by tapping the pectoralis tendon in the deltopectoral groove causing adduction and internal rotation of the shoulder is a sign of cord compression in the upper cervical spine (C2-3, C3-4 spinal levels) 4. The “dynamic” Hoffmann’s sign (when a typical Hoffmann’s sign is elicited after having the patient flex and extend the neck multiple times) may be an indicator of early cervical spinal cord compression 5. Hyperreflexia may be absent in cervical spinal cord compression patients who have concurrent diabetes, causing a peripheral neuropathy.
Imaging and Diagnostic Studies
Magnetic resonance imaging (MRI) of the cervical spine is the procedure of choice during the initial screening process of patients with suspected cervical spinal cord compression 6. MRI is noninvasive and provides images of the spine and spinal cord in several planes (Figure 3). In addition to giving an assessment of the degree of spinal canal stenosis, an MRI can identify intrinsic spinal cord lesions that can also present with myelopathy (e.g., tumors). High signal changes seen in the spinal cord of patients with cervical spinal cord compression may indicate myelomalacia or permanent spinal cord damage.
Computed tomography (CT) is complementary to MRI. CT scan may give a more accurate assessment of the amount of canal compromise because it is superior to MRI in evaluating bone (osteophytes) 7. Myelography or the intrathecal injection of a contrast agent is used in conjunction with CT scan. Since the advent of MRI, the use of myelography has decreased; however, it still provides useful information in some instances for surgical planning. Plain radiographs alone are of little use as an initial diagnostic procedure.
Treatment Options
Evaluating the efficacy of any particular treatment strategy for cervical spinal cord compression is difficult because reports show that as many as 18 percent of patients with cervical spinal cord compression will improve spontaneously, 40 percent will stabilize and approximately 40 percent will deteriorate if no treatment is given 8. Unfortunately, the current understanding of cervical spinal cord compression does not allow physicians to predict the course of a patient. Also, the literature regarding various treatment strategies (surgical and nonsurgical) for cervical spinal cord compression is flawed because of a lack of prospective controlled studies.
A decision whether to have laminectomy
As you make the decision whether to have surgery, make sure that you understand its risks, benefits and limitations. If you do not have surgery to relieve compression of a spinal nerve, further damage may occur, with more pain, numbness, paralysis or loss of bladder or bowel control.
Only you can decide if surgery is right for you. If you have any questions, ask your surgeon.
Nonsurgical Treatment
In patients who are mildly affected by cervical spinal cord compression, a “careful watching” approach can be taken. A variety of nonsurgical strategies have been used with variable success for the treatment of cervical spinal cord compression. These include cervical traction, cervical immobilization (collar or neck brace), skull traction and physical therapy. Cervical immobilization is the most commonly used treatment in the United States. Some studies demonstrate the benefits of wearing a brace, while other studies show that immobilization does not improve the patient’s condition 9. It has also been reported that symptomatic patients may deteriorate neurologically during bracing, causing many to advocate earlier surgical intervention 10. A nonsurgical approach is usually inadvisable.
Surgical Treatment
Once frank myelopathy occurs, surgical intervention is necessary. The primary goal of surgery is to decompress the spinal cord, thus giving the neural elements more room. Traditionally, cervical laminectomy, a posterior approach, has been used for surgical treatment of cervical spinal cord compression. However, over the past 20 years, it has been increasingly recognized that laminectomy is not appropriate for all patients. Further neurologic deterioration after laminectomy is attributed to a development of latent instability of the spine with development of kyphotic spinal deformities and to the inability of posterior approaches to directly address anterior vector compression secondary to osteophytic overgrowth.
For this reason, anterior approaches to the spine have been increasingly used 11. Through an anterior cervical approach, one can directly address and remove osteophytes and disc material for decompression of the spinal cord. Also, with the addition of interposition bone grafts and, in some cases, cervical plates (instrumentation) to promote spinal fusion, the development of instability of the neck can be prevented. A variety of factors must be considered when deciding whether to use an anterior or posterior approach, but the primary goal of both approaches is to provide adequate space for the spinal cord.
Many surgical series show “improvement,” or at least stabilization of symptoms with posterior and anterior approaches. After reviewing the surgical literature, one investigator found that the rate of successful outcome after surgery was at best 50 percent with the potential for significant postsurgical morbidity 11. The older surgical literature has been criticized because of the uncertainty of whether nonspondylotic myelopathy conditions (e.g., multiple sclerosis, ALS) had been sufficiently excluded before surgery 11.
A variety of factors determine success after surgery. Factors that may portend a less than satisfactory surgical outcome include severe preoperative neurologic deficits, abnormal signal changes within the spinal cord and/or spinal cord atrophy seen on MRI, and severity of cord compression seen on radiographic studies 12, 13, 14.
Laminectomy discectomy
Discectomy is a surgical procedure to remove the damaged portion of a herniated disk in your spine. A herniated disk occurs when some of the softer material inside the disk pushes out through a crack in the tougher exterior. A herniated disk can irritate or compress nearby nerves and cause pain, numbness or weakness. Discectomy is most effective for treating pain that radiates down your arms or legs.
The discectomy procedure is less helpful for treating actual back pain or neck pain. Most people who have back pain or neck pain find relief with more-conservative treatments, such as physical therapy.
Your doctor may suggest discectomy if conservative, nonsurgical treatments haven’t worked or if your symptoms worsen. There are several ways to perform a discectomy. Many surgeons now prefer minimally invasive discectomy, which uses small incisions and a tiny video camera for viewing the procedure.
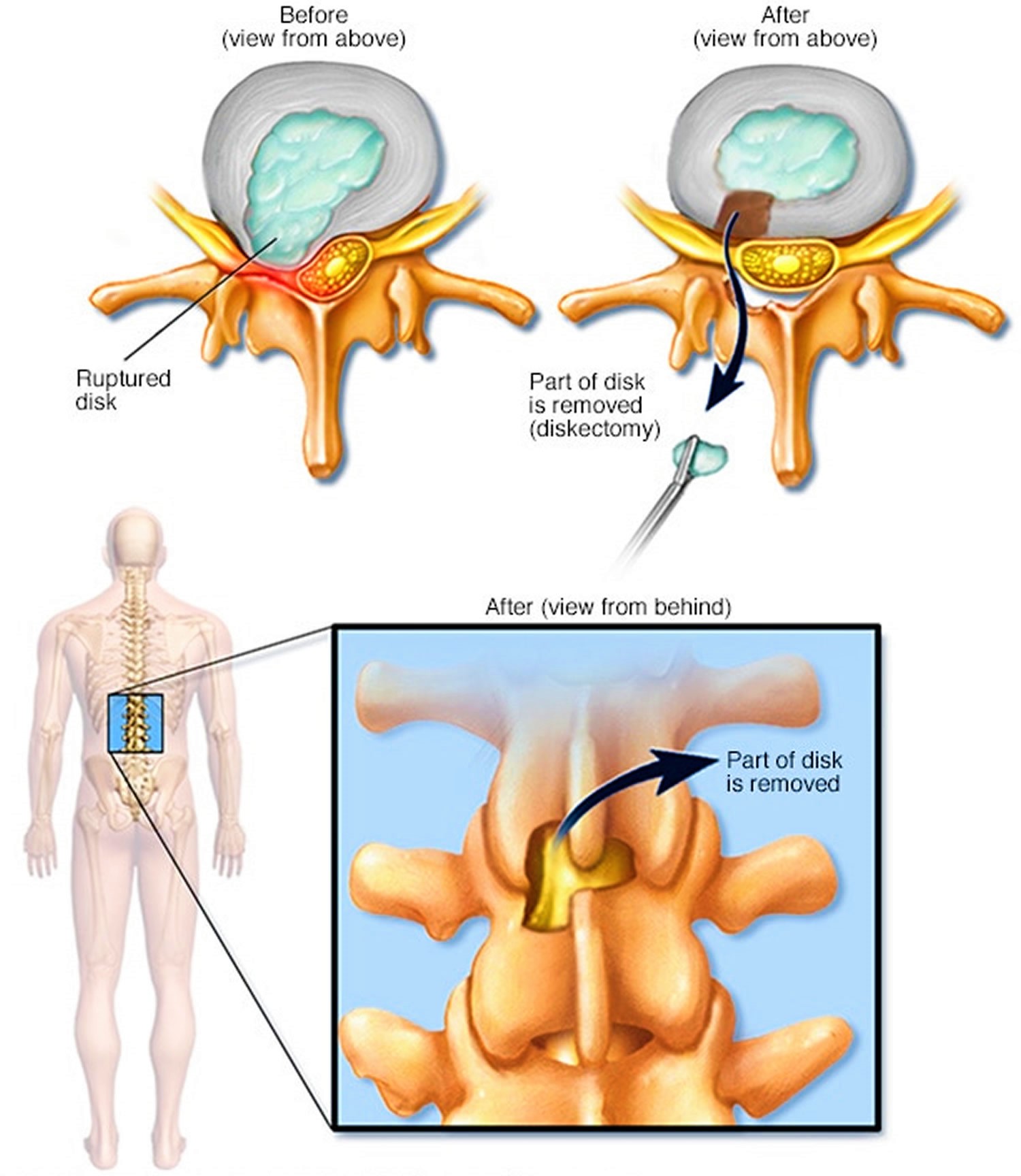
Figure 7. Discectomy
 Why discectomy is done
Why discectomy is done
A discectomy is performed to relieve the pressure a herniated disk (also called a slipped, ruptured or bulging disk or disk prolapse) places on a spinal nerve. A herniated disk occurs when some of the softer material inside the disk pushes out through a crack in the tougher exterior.
Your doctor may recommend discectomy if:
- You have trouble standing or walking because of nerve weakness
- Conservative treatment, such as physical therapy or steroid injections, fails to improve your symptoms after six to 12 weeks
- Pain radiating into your buttocks, legs, arms or chest becomes too much to manage
Discectomy risks and possible complications
Discectomy is considered a safe procedure. But as with any surgery, discectomy carries a risk of complications. Potential complications include:
- Bleeding
- Infection
- Leaking spinal fluid
- Injury to blood vessels or nerves in and around the spine
How you prepare for a discectomy surgery
You’ll likely need to avoid eating and drinking for a certain amount of time before surgery. If you take blood-thinning medications, you may need to adjust your dosing schedule before surgery. Your doctor will give you specific instructions.
During discectomy procedure
Surgeons usually perform discectomy using general anesthesia, so you’re unconscious during the procedure. Small amounts of spinal bone and ligament may be removed to gain access to the herniated disk.
Ideally, just the fragment of disk that is pinching the nerve is removed, relieving the pressure but leaving most of the disk intact.
If the entire disk must be taken out, your surgeon may need to fill the space with a piece of bone — taken from a deceased donor or from your own pelvis — or a synthetic bone substitute. The adjoining vertebrae are then fused together with metal hardware.
Discectomy recovery
After surgery, you’re moved to a recovery room where the health care team watches for complications from the surgery and anesthesia. You may be healthy enough to go home the same day you have surgery, although a short hospital stay may be necessary — particularly if you have any serious pre-existing medical conditions.
Depending on the amount of lifting, walking and sitting your job involves, you may be able to return to work in two to six weeks. If you have a job that includes heavy lifting or operating heavy machinery, your doctor may advise you to wait six to eight weeks before returning to work.
Discectomy results
Discectomy reduces herniated disk symptoms in most people who have clear signs of nerve compression, such as radiating pain. However, discectomy may not be a permanent cure, because it doesn’t do anything to reverse the process that allowed the disk to become herniated in the first place.
To avoid re-injuring your spine, your doctor may recommend weight loss, prescribe a low-impact exercise program, and ask that you limit some activities that involve extensive or repetitive bending, twisting or lifting.
Laminectomy and spinal fusion
Spinal fusion is a surgical procedure used to correct problems with the small bones in the spine (vertebrae). It is essentially a “welding” process. The basic idea is to fuse together two or more vertebrae so that they heal into a single, solid bone. This is done to eliminate painful motion or to restore stability to the spine.
Spine surgery is usually recommended only when your doctor can pinpoint the source of your pain. To do this, your doctor may use imaging tests, such as x-rays, computerized tomography (CT) scans, and magnetic resonance imaging (MRI) scans.
Spinal fusion may help relieve symptoms of many back problems, including:
- Degenerative disk disease
- Spondylolisthesis
- Spinal stenosis
- Scoliosis
- Fractured vertebra
- Infection
- Herniated disk
- Tumor
Spinal fusion eliminates motion between vertebrae. It also prevents the stretching of nerves and surrounding ligaments and muscles. It is an option when motion is the source of pain, such as movement that occurs in a part of the spine that is arthritic or unstable due to injury, disease, or the normal aging process. The theory is if the painful vertebrae do not move, they should not hurt.
If you have leg pain or arm pain in addition to back pain, your surgeon may also perform a decompression (laminectomy). This procedure involves removing bone and diseased tissues that are putting pressure on spinal nerves.
Fusion will take away some spinal flexibility, but most spinal fusions involve only small segments of the spine and do not limit motion very much. The majority of patients will not notice a decrease in range of motion. Your surgeon will talk with you about whether your specific procedure may impact flexibility or range of motion in your spine.
Figure 8. Spinal fusion
Lumbar and cervical spinal fusion procedure
Lumbar and cervical spinal fusion have been performed for decades. There are several different techniques that may be used to fuse the spine. There are also different “approaches” your surgeon can take to reach your spine.
- Your surgeon may approach your spine from the front. This is called an anterior approach and requires an incision in the lower abdomen for a lumbar fusion or in the front of the neck for a cervical fusion.
- A posterior approach is done from the back.
- In a lateral approach, your surgeon approaches your spine from the side.
Minimally invasive techniques have also been developed. These allow fusions to be performed with smaller incisions.
The right procedure for you will depend on the nature and location of your disease.
Bone Grafting
All spinal fusions use some type of bone material, called a bone graft, to help promote the fusion. Generally, small pieces of bone are placed into the space between the vertebrae to be fused.
A bone graft is primarily used to stimulate bone healing. It increases bone production and helps the vertebrae heal together into a solid bone. Sometimes larger, solid pieces are used to provide immediate structural support to the vertebrae.
In the past, a bone graft harvested from the patient’s pelvis was the only option for increasing the material needed for fusing the vertebrae. This type of graft is called an autograft. Harvesting a bone graft requires an additional incision during the operation. It lengthens surgery and can cause increased pain after the operation.
If you are having a laminectomy procedure, the surgeon may harvest your bone from the site of the laminectomy decompression and use it as the graft. This type of graft is called a local autograft. The bone is essentially recycled; it is moved from where it is compressing your nerves to the area the surgeon wants to fuse.
One alternative to harvesting a bone graft is an allograft, which is cadaver bone. An allograft is typically acquired through a bone bank.
Today, several artificial bone graft materials have also been developed:
- Demineralized bone matrices. Calcium is removed from cadaver bone to create demineralized bone matrices. Without the mineral, the bone can be changed into a putty or gel-like consistency. Demineralized bone matrices are usually combined with other grafts, and may contain proteins that help in bone healing.
- Bone morphogenetic proteins. These very powerful synthetic bone-forming proteins promote a solid fusion. They are approved by the U.S. Food and Drug Administration for use in the spine in certain situations. Autografts may not be needed when bone morphogenetic proteins are used.
- Synthetic bone. Synthetic bone grafts are made from calcium/phosphate materials and are often called “ceramics.” They are similar in shape and consistency to autograft bone.
Your surgeon will discuss with you the type of bone graft material that will work best for your condition and procedure.
Immobilization
After bone grafting, the vertebrae need to be held together to help the fusion progress. Your surgeon may suggest that you wear a brace.
In many cases, surgeons will use plates, screws, and rods to help hold the spine still. This is called internal fixation, and may increase the rate of successful healing. With the added stability from internal fixation, most patients are able to move earlier after surgery.
Laminectomy and spinal fusion complications
As with any surgery, there are risks associated with spinal fusion. Your doctor will discuss each of the risks with you before your procedure and will take specific measures to help avoid potential complications. Potential risks and complication of spinal fusion include:
- Infection. Antibiotics are regularly given to the patient before, during, and often after surgery to lessen the risk of infections.
- Bleeding. A certain amount of bleeding is expected, but this is not typically significant. It is not usually necessary to donate blood before spinal fusion.
- Pain at graft site. A small percentage of patients will experience persistent pain at the bone graft site.
- Recurring symptoms. Some patients may experience a recurrence of their original symptoms. There are various causes for this. If your original symptoms recur, inform your doctor so that he or she can determine what is causing your symptoms.
- Pseudarthrosis. This is a condition in which there is not enough bone formation. Patients who smoke are more likely to develop a pseudarthrosis. Other causes include diabetes and older age. Moving too soon—before the bone is able to start fusing—may also result in a pseudarthrosis. If this occurs, a second surgery may be needed in order to obtain a solid fusion.
- Nerve damage. It is possible that nerves or blood vessels may be injured during these operations. These complications are very rare.
- Blood clots. Another uncommon complication is the formation of blood clots in the legs. These pose significant danger if they break off and travel to the lungs.
Warning Signs
It is important that you carefully follow any instructions from your doctor relating to the warning signs of blood clots and infection. These complications are most likely to occur during the first few weeks after surgery.
Blood clots. Warning signs of a possible blood clot include:
- Swelling in the calf, ankle or foot
- Tenderness or redness, which may extend above or below the knee
- Pain in the calf
Occasionally, a blood clot will travel through the bloodstream and may settle in the lungs. If this happens, you may experience sudden chest pain and shortness of breath or coughing. If you experience any of these symptoms, you should notify your doctor immediately. If you cannot reach your doctor, have someone take you to the hospital emergency room or call your local emergency services number.
Infection following spine surgery occurs very rarely. Warning signs of infection include:
- Redness, tenderness, and swelling around the wound edges
- Drainage from the wound
- Pain or tenderness
- Shaking chills
- Elevated temperature, usually above 101°F if taken with an oral thermometer
If any of these symptoms occur, you should contact your doctor or go to the nearest emergency room immediately.
Laminectomy and spinal fusion recovery
Pain Management
After surgery, you will feel some pain. This is a natural part of the healing process. Your doctor and nurses will work to reduce your pain, which can help you recover from surgery faster.
Medications are often prescribed for short-term pain relief after surgery. Many types of medicines are available to help manage pain, including opioids, nonsteroidal anti-inflammatory drugs (NSAIDs), and local anesthetics. Your doctor may use a combination of these medications to improve pain relief, as well as minimize the need for opioids.
Be aware that although opioids help relieve pain after surgery, they are a narcotic and can be addictive. Opioid dependency and overdose has become a critical public health issue in the U.S. It is important to use opioids only as directed by your doctor. As soon as your pain begins to improve, stop taking opioids. Talk to your doctor if your pain has not begun to improve within a few days of your surgery.
Rehabilitation
The fusion process takes time. It may be several months before the bone is solid, although your comfort level will often improve much faster. During this healing time, the fused spine must be kept in proper alignment. You will be taught how to move properly, reposition, sit, stand, and walk.
Your symptoms will gradually improve, as will your activity level. Right after your operation, your doctor may recommend only light activity, like walking. As you regain strength, you will be able to slowly increase your activity level. Physical therapy is typically started from 6 weeks to 3 months after surgery. Your surgeon will talk with you about whether physical therapy is needed in your situation.
Maintaining a healthy lifestyle and following your doctor’s instructions will greatly increase your chances for a successful outcome.
Post laminectomy syndrome
Post-laminectomy syndrome or “Failed Back Surgery Syndrome” is defined by the International Association for the Study of Pain as back pain, with or without referred or radiating pain, that is located mainly in the lower limbs, is of unknown origin and persists or begins after surgical procedures are performed to treat lumbar disc herniations 15. Although not well known, post laminectomy syndrome is an important cause of chronic back pain. Low back pain is a common complaint, with a reported peak prevalence in the adult population of 37 % and a lifetime prevalence between 60 and 85 %. In addition to the suffering and disability that post laminectomy syndrome may inflict on patients, its impact on society is considerable 16.
Compared with other models of chronic pain, post laminectomy syndrome patients with neuropathic pain experience intense levels of pain, lower quality of life, greater disability and higher rates of unemployment 16. As many as one-third of the patients undergoing surgery for the correction of lumbar disc conditions experience recurrent postoperative symptoms 17. Walker 18 states that 20–40 % of the patients undergoing lumbar surgery will not experience benefits from the procedure and that the condition will worsen in 1–10 %.
The main causes of post laminectomy syndrome are foraminal stenosis, internal disc extrusion, pseudoarthrosis and neuropathic pain, which in combination account for more than 70 % of the cases 19.
Several authors 20 have suggested that the misinterpretation that a herniated disc is causing low back pain is the most common reason behind the spinal surgeries that result in post-laminectomy chronic pain syndrome beginning immediately after the procedures. This misinterpretation may be partially caused by an overestimation of the anatomical findings that are revealed during the imaging evaluations but are not related to the lumbago and usually do not explain the pain or justify surgical intervention. The overvaluation of complementary exams by contemporary medicine might be responsible for the high prevalence of post laminectomy syndrome. Hasty diagnoses using imaging methods rather than clinical observations can lead to unnecessary treatments (including surgery) that, in turn, cause iatrogenic conditions.
It should also be noted that this subject is controversial. Some investigations have shown beneficial results from laminectomy surgery. A prospective non-randomized observational study 21 suggests that patients who suffer from low back pain caused by lumbar disc herniations and who undergo surgery exhibit positive responses to treatment, as do those patients who are treated conservatively. The same investigation has also demonstrated that patients who opt for interventional treatment report significantly greater improvements than those who elect nonsurgical treatments; however, the study was non-randomized and supported only by subjective reports from the patients, warranting a careful interpretation of the results. However, a controlled and randomized cohort study 22 has demonstrated that patients with disc herniations who are treated surgically experience significantly greater improvements in their pain, function, satisfaction and self-assessments of their progress over 4 years of follow-up compared with patients who are treated conservatively, despite worse results for the motor activity in the former group after surgery.
The pain stems from the involvement of various anatomical structures and manifests itself in various and unique ways in each patient 23. Chronic pain is debilitating and often resistant to pharmacological, rehabilitational, psychotherapeutic and surgical treatments 24. Chronic pain evokes emotions that may be equally disabling or even more disabling than the actual underlying condition that caused it. The pain can generate ideas about hypothetical losses and physical disability, which together can affect the emotional, social, cultural and family performance of the patient. Many patients’ lives begin to be solely centered on their pain. Their physical, mental and social deterioration—as well as the immobility caused by fear of exacerbating the pain—may result in a worsening of the associated mental illnesses and difficulties associated with their treatment. The difficulties that the patients encounter in understanding their problems and finding a cure, combined with a lack of coherent explanations from the professionals who assist them, destabilize and worsen their mental states 25.
A detailed psychiatric evaluation revealed that most of the post laminectomy syndrome patients had defined psychiatric diagnoses, were suffering from personality disorders, had normal pre-pain personalities or suffered from reactive depression 26. These results confirm the influence of chronic pain on the process of mental health, which requires psychological and/or psychiatric counseling for the management of these individuals to obtain satisfactory results in their treatment.
- Adams RD, Victor M. Diseases of the spinal cord, peripheral nerve and muscle. In: Adams RD, Victor M, eds. Principles of neurology. 5th ed. New York:McGraw-Hill, Health Professions Division, 1993:1100–1.[↩][↩]
- Brain NR, Northfield D, Wilkinson M. The neurological manifestations of cervical spondylosis. Brain. 1952;75:187–225.[↩]
- Patten J. Neurological differential diagnosis. 2d ed. New York: Springer, 1996.[↩]
- Watson JC, Broaddus WC, Smith MM, Kubal WS. Hyperactive pectoralis reflex as an indicator of upper cervical spinal cord compression. Report of 15 cases. J Neurosurg. 1997;86:159–61.[↩]
- Denno JJ, Meadows GR. Early diagnosis of cervical spondylotic myelopathy. A useful clinical sign. Spine. 1991;16:1353–5.[↩]
- Al-Mefty O, Harkey LH, Middleton TH, Smith RR, Fox JL. Myelopathic cervical spondylotic lesions demonstrated by magnetic resonance imaging. J Neurosurg. 1988;68:217–22.[↩]
- Freeman TB, Martinez CR. Radiological evaluation of cervical spondylotic disease: limitation of magnetic resonance imaging for diagnosis and preoperative assessment. Perspect Neurol Surg. 1992;3:34–6.[↩]
- Kumar VG, Rea GL, Mervis LJ, McGregor JM. Cervical spondylotic myelopathy: functional and radiographic long-term outcome after laminectomy and posterior fusion. Neurosurgery. 1999;44:771–8.[↩]
- Roberts AH. Myelopathy due to cervical spondylosis treated by collar immobilization. Neurology. 1966;16:951–4.[↩]
- Zeidman SM, Ducker TB. Cervical disk diseases: part 1. Treatment options and outcomes. Nuerosurgy Quarterly. 1992;2:116–43.[↩]
- Saunders RL. Corpectomy for cervical spondylotic myelopathy. In: Menezes AH, Sonntag VK, eds. Principles of spinal surgery. New York: McGraw-Hill Companies, Health Professions Division, 1996: 559–69.[↩][↩][↩]
- Naderi S, Ozgen S, Pamir MN, Ozek MM, Erzen C. Cervical spondylotic myelopathy: surgical results and factors affecting prognosis. Neurosurgery. 1998;43:43–50.[↩]
- Bucciero A, Vizioli L, Tedeschi G. Cord diameters and their significance in prognostication and decisions about management of cervical spondylotic myelopathy. J Neurosurg Sci. 1993;37:223–8.[↩]
- Chiles BW 3d, Leonard MA, Choudhri HF, Cooper PR. Cervical spondylotic myelopathy: patterns of neurological deficit and recovery after anterior cervical decompression. Neurosurgery. 1999;44:762–70.[↩]
- Merskey H, Bogduk N. Classification of chronic pain—descriptions of chronic pain syndromes and definitions of pain terms. Seatle: IASP Press; 2004.[↩]
- Chan CW, Peng P. Failed back surgery syndrome. Pain Med. 2011;12:577–606. doi: 10.1111/j.1526-4637.2011.01089.x https://www.ncbi.nlm.nih.gov/pubmed/21463472[↩][↩]
- McKinstry CS, Bell KE. The failed back syndrome: the diagnostic contribution of computed tomography. Ulster Med J. 1990;59:122–130 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2448294/pdf/ulstermedj00079-0025.pdf[↩]
- Walker BF. Failed back surgery syndrome. COMSIG Rev. 1992;1:3–6 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2050006/pdf/cr011-003b.pdf[↩]
- Rodrigues FF, Dozza DC, de Oliveira CR, de Castro RG. Failed back surgery syndrome: casuistic and etiology. Arq Neuropsiquiatr. 2006;64:757–761. doi: 10.1590/S0004-282X2006000500011 https://www.ncbi.nlm.nih.gov/pubmed/17057881[↩]
- Teixeira MJ, Yeng LT, Garcia OG, Fonoff ET, Paiva WS, Araujo JO. Failed back surgery pain syndrome: therapeutic approach descriptive study in 56 patients. Rev Assoc Med Bras. 2011;57:282–287. doi: 10.1016/S0104-4230(11)70060-4 https://www.ncbi.nlm.nih.gov/pubmed/21691691[↩]
- An analysis of reasons for failed back surgery syndrome and partial results after different types of surgical lumbar nerve root decompression. Bokov A, Isrelov A, Skorodumov A, Aleynik A, Simonov A, Mlyavykh S. Pain Physician. 2011 Nov-Dec; 14(6):545-57. https://www.ncbi.nlm.nih.gov/pubmed/22086096/[↩]
- Surgical vs nonoperative treatment for lumbar disk herniation: the Spine Patient Outcomes Research Trial (SPORT) observational cohort. Weinstein JN, Lurie JD, Tosteson TD, Skinner JS, Hanscom B, Tosteson AN, Herkowitz H, Fischgrund J, Cammisa FP, Albert T, Deyo RA. JAMA. 2006 Nov 22; 296(20):2451-9. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2562254/[↩]
- Hedtmann A. The so-called post-discotomy syndrome—failure of intervertebral disk surgery? Z Orthop Ihre Grenzgeb. 1992;130:456–466. doi: 10.1055/s-2008-1039653 https://www.ncbi.nlm.nih.gov/pubmed/1492448[↩]
- Fiume D, Sherkat S, Callovini GM, Parziale G, Gazzeri G. Treatment of the failed back surgery syndrome due to lumbo-sacral epidural fibrosis. Acta Neurochir Suppl. 1995;64:116–118. doi: 10.1007/978-3-7091-9419-5_25. https://www.ncbi.nlm.nih.gov/pubmed/8748597[↩]
- Garcia JBS, Rodrigues DP, Leite DRB, do Nascimento Câmara S, da Silva Martins K, de Moraes ÉB. Clinical evaluation of the post-laminectomy syndrome in public hospitals in the city of São Luís, Brazil. BMC Research Notes. 2015;8:451. doi:10.1186/s13104-015-1400-9 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4574019/[↩]
- Clinical features of the failed-back syndrome. Long DM, Filtzer DL, BenDebba M, Hendler NH. J Neurosurg. 1988 Jul; 69(1):61-71. https://www.ncbi.nlm.nih.gov/pubmed/2967891/[↩]





{kind=link}