Large intestine
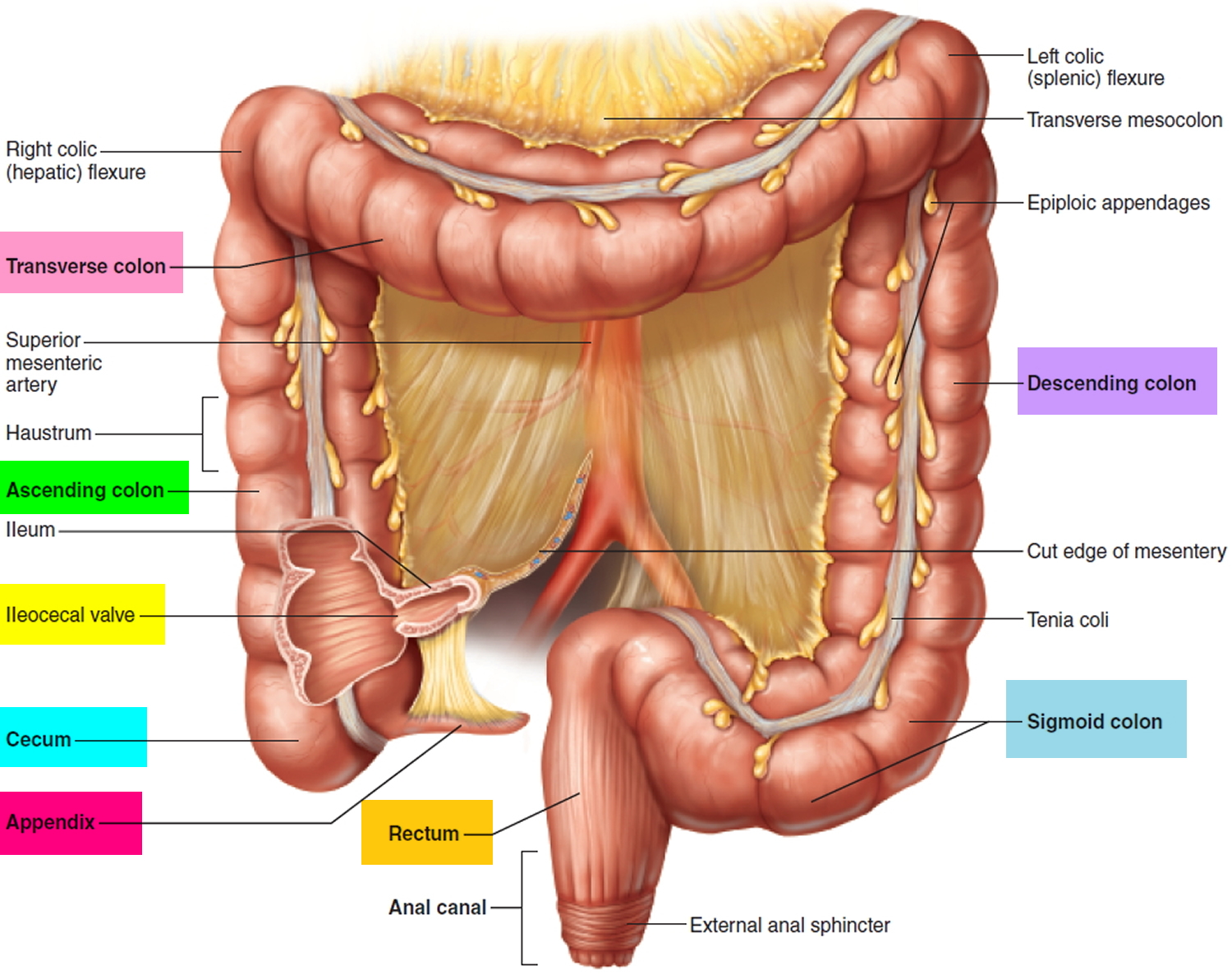
The large intestine also known as the colon, extends from the distal end of the ileum to the anus, a distance of approximately 1.5 m in adults (5 ft) long, making up one-fifth of the length of the gastrointestinal (GI) tract and 6.5 cm (2.5 in.) in diameter. The large intestine is named for its relatively large diameter, not its length. The large intestine consists of the cecum, appendix, ascending colon, transverse colon, descending colon, rectum, and anal canal.
The large intestine is responsible for processing indigestible food material (chyme) after most nutrients are absorbed in the small intestine. The large intestine performs an essential role by absorbing water, vitamins, salts and electrolytes from the gut contents, thus forming feces.
Beginning in the right groin as the cecum, with its associated appendix, the large intestine continues upward as the ascending colon through the right flank and into the right hypochondrium. The ascending colon begins at the ileocecal valve and passes up the right side of the abdominal cavity. It makes a 90° turn at the right colic (hepatic) flexure, near the right lobe of the liver, and crosses the abdomen as the transverse colon to the left hypochondrium. At this position, just below the spleen, the large intestine bends downward, forming the left colic flexure (splenic flexure) and continues as the descending colon through the left flank and into the left groin. Ascending, transverse, and descending colons thus form a squarish, three-sided frame around the small intestine.
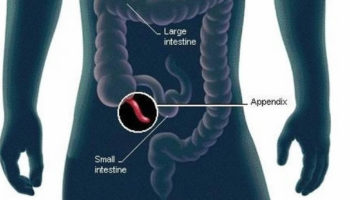
The cecum is a blind pouch in the lower right abdominal quadrant inferior to the ileocecal valve. Attached to its lower end is the appendix, a blind tube 2 to 7 cm long. The appendix is densely populated with lymphocytes and is a significant source of immune cells.
Figure 1. Large intestine
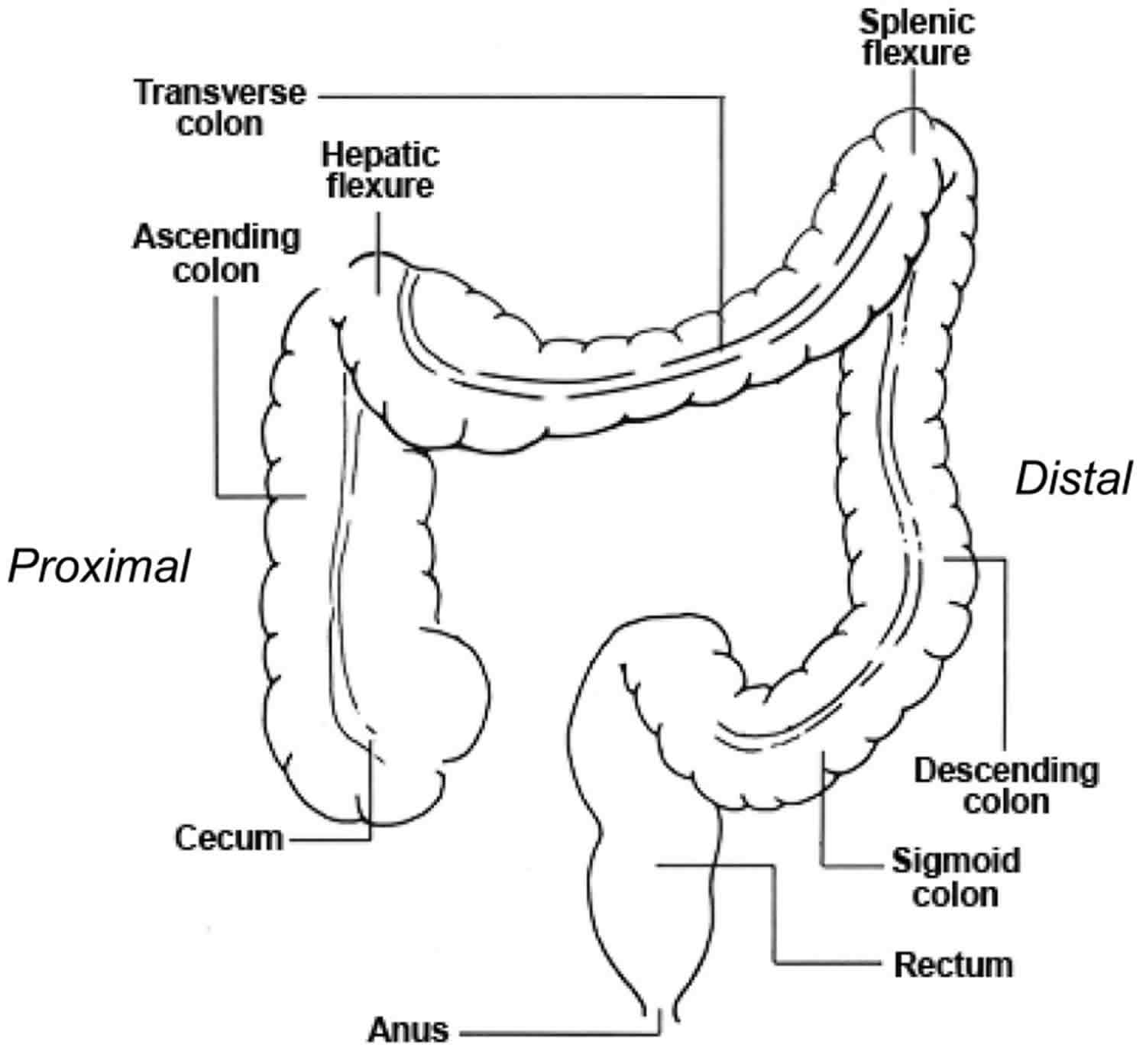
The pelvic cavity is narrower than the abdominal cavity, so at the hip bone, the colon turns medially and travels along the iliac fossa before turning downward at the pelvic inlet into the pelvic cavity. The resulting S-shaped portion of the tract is called the sigmoid colon. Visual examination of this region is performed with an instrument called a sigmoidoscope. In the pelvic cavity, the large intestine continues as the rectum, about 15 cm long. Despite its name, the rectum is not quite straight but has three lateral curves as well as an anteroposterior curve. It has three infoldings called transverse rectal folds (rectal valves), which enable it to retain feces while passing gas.
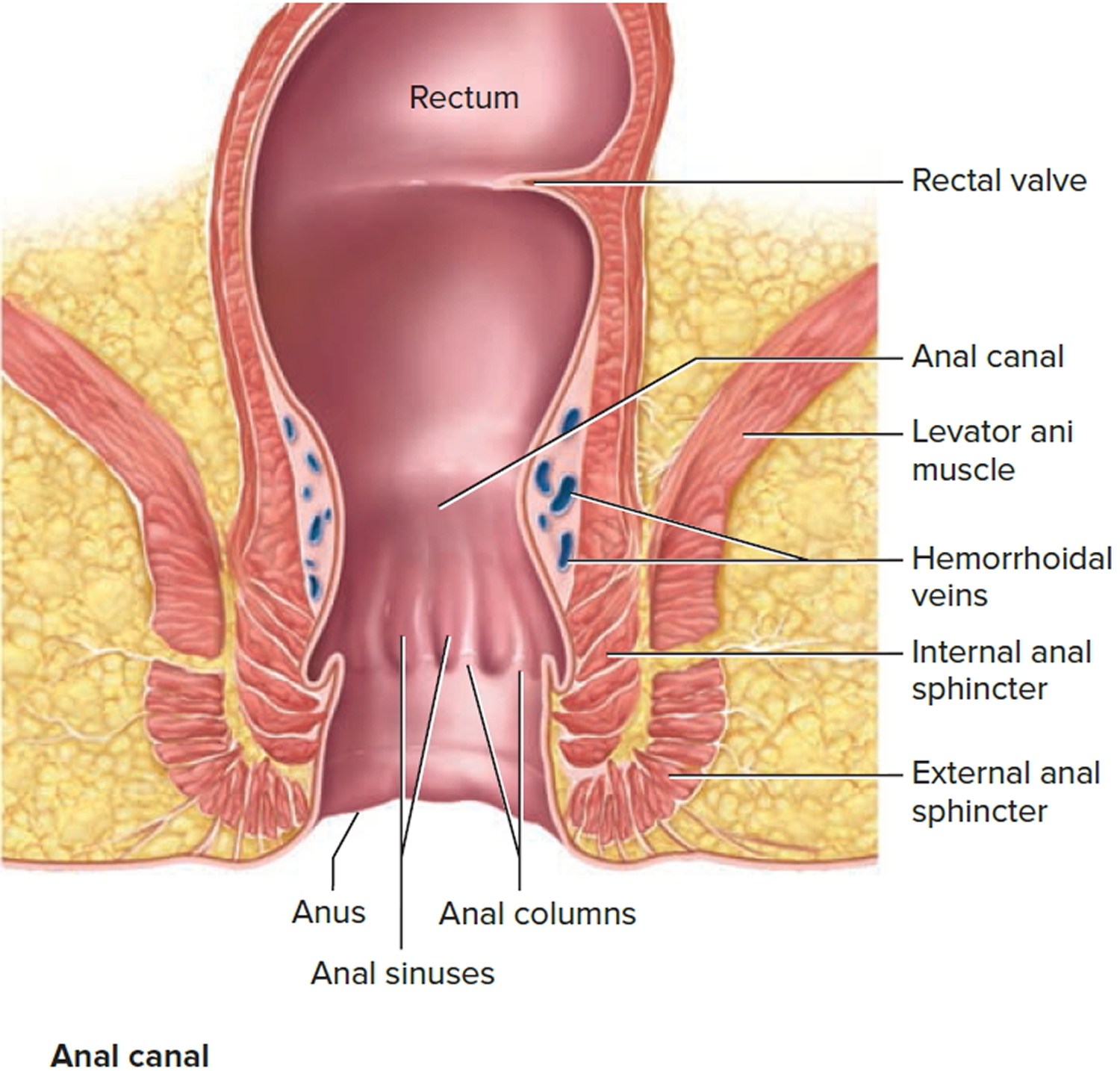
The final 3 cm of the large intestine is the anal canal, which passes through the levator ani muscle of the pelvic floor and terminates at the anus. Here, the mucosa forms longitudinal ridges called anal columns with depressions between them called anal sinuses. As feces pass through the canal, they press the sinuses and cause them to exude extra mucus and lubricate the canal during defecation. Prominent hemorrhoidal veins form superficial plexuses in the anal columns and around the orifice. Unlike veins in the limbs, they lack valves and are particularly subject to distension and venous pooling. Hemorrhoids are permanently distended veins that protrude into the anal canal or form bulges external to the anus. They can result from the impaired venous return that occurs in obesity and pregnancy.
The muscularis externa of the colon is unusual. Although it completely encircles the colon just as it does the small intestine, its longitudinal fibers are especially concentrated in three thickened, ribbonlike strips. Each strip is called a taenia coli. The muscle tone of the taeniae coli contracts the colon lengthwise and causes its wall to bulge, forming pouches called haustra (singular, haustrum). Haustra are conspicuous in colonic X-rays of living patients, because they disappear when muscle tone is lost at death. In the rectum and anal canal, the longitudinal muscle forms a continuous sheet and haustra are absent. The anus is regulated by two sphincters: an internal anal sphincter composed of smooth muscle of the muscularis externa and an external anal sphincter composed of skeletal muscle of the pelvic diaphragm.
The ascending and descending colon are retroperitoneal and have a serosa only on the anterior surface, whereas the transverse and sigmoid colon are entirely enclosed in serosa and anchored to the posterior abdominal wall by the mesocolon. The serosa of the transverse through sigmoid colon often has omental appendages, also called epiploic appendages, are fat-filled pouches of visceral peritoneum that hang from the intestine. Their significance is unknown.
Figure 2. Large intestine location
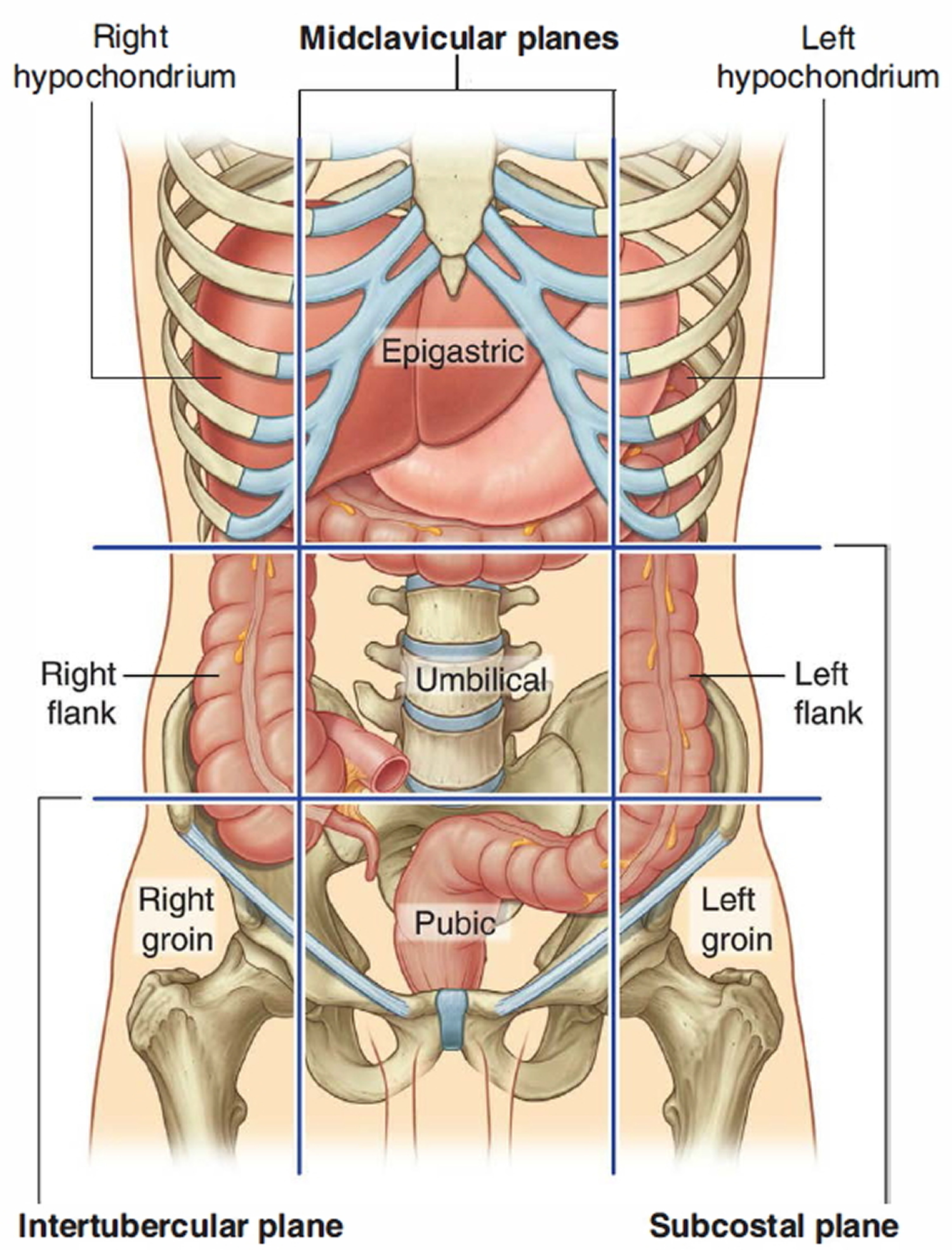
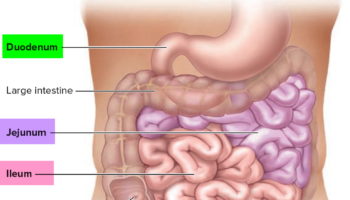
Figure 3. Large intestine and small intestine
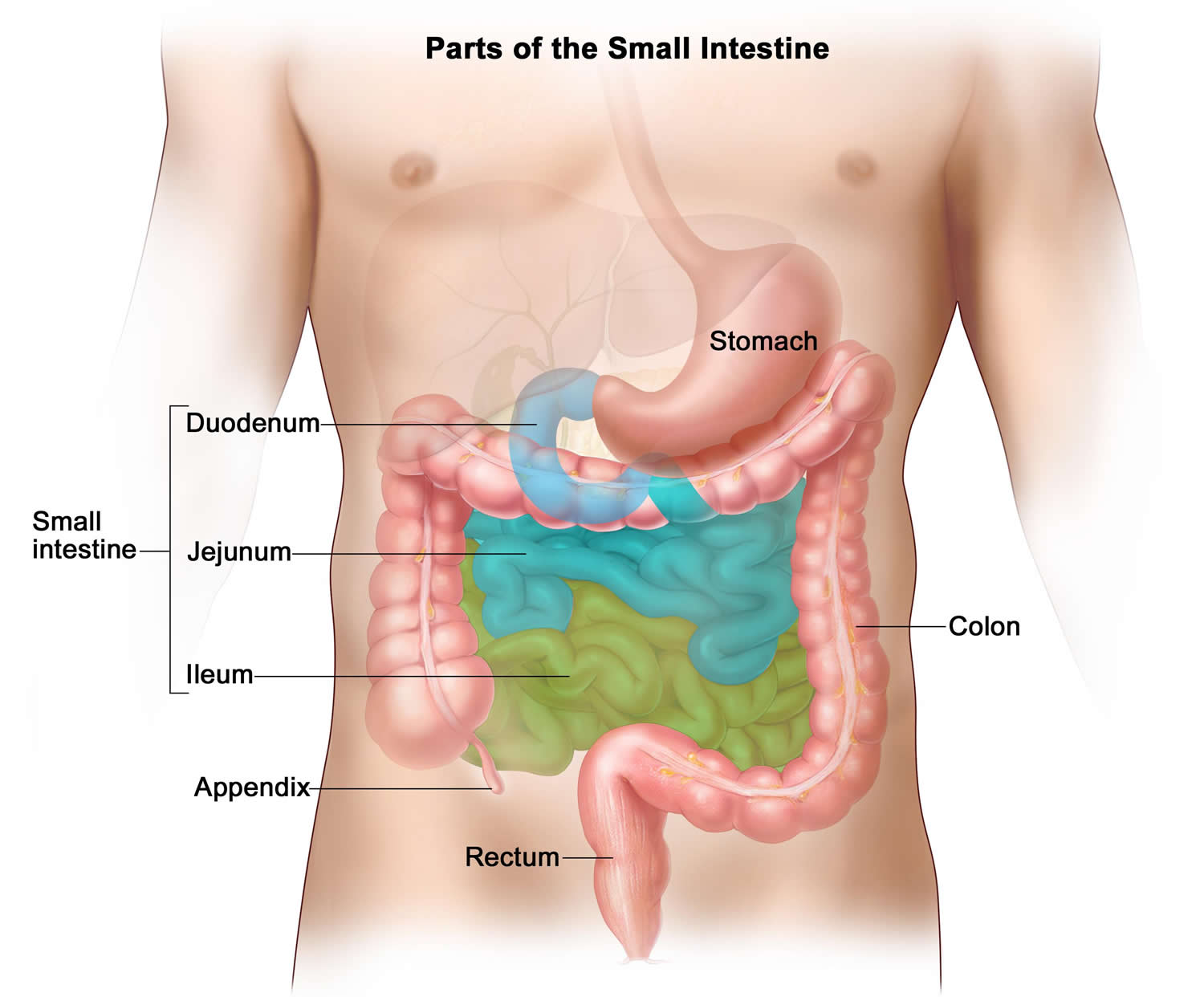
Figure 4. Anal canal
Blood supply to the large intestine
The large intestine is served by mesenteric arteries and veins much like the small intestine. Branches of the superior mesenteric artery fan out to supply the ascending colon and most of the transverse colon; the inferior mesenteric artery supplies the rest of the transverse colon as well as the descending and sigmoid colon and the rectum. The superior and inferior mesenteric veins drain the same parts of the large intestine as the correspondingly named arteries and drain into the hepatic portal system.
Function of large intestine
The large intestine has 3 primary functions: absorbing water and electrolytes, producing and absorbing vitamins, and forming and propelling feces toward the rectum for elimination. By the time indigestible materials have reached the colon, most nutrients and up to 90% of the water has been absorbed by the small intestine. The role of the ascending colon is to absorb the remaining water and other key nutrients from the indigestible material, solidifying it to form stool. The descending colon stores feces that will eventually be emptied into the rectum. The sigmoid colon contracts to increase the pressure inside the colon, causing the stool to move into the rectum. The rectum holds the feces awaiting elimination by defecation.
Functions of the large intestine:
- Haustral churning, peristalsis, and mass peristalsis drive contents of colon into rectum.
- Bacteria in large intestine convert proteins to amino acids, break down amino acids, and produce some B vitamins and vitamin K.
- Absorption of some water, ions, and vitamins.
- Formation of feces.
- Defecation (emptying rectum).
Motility
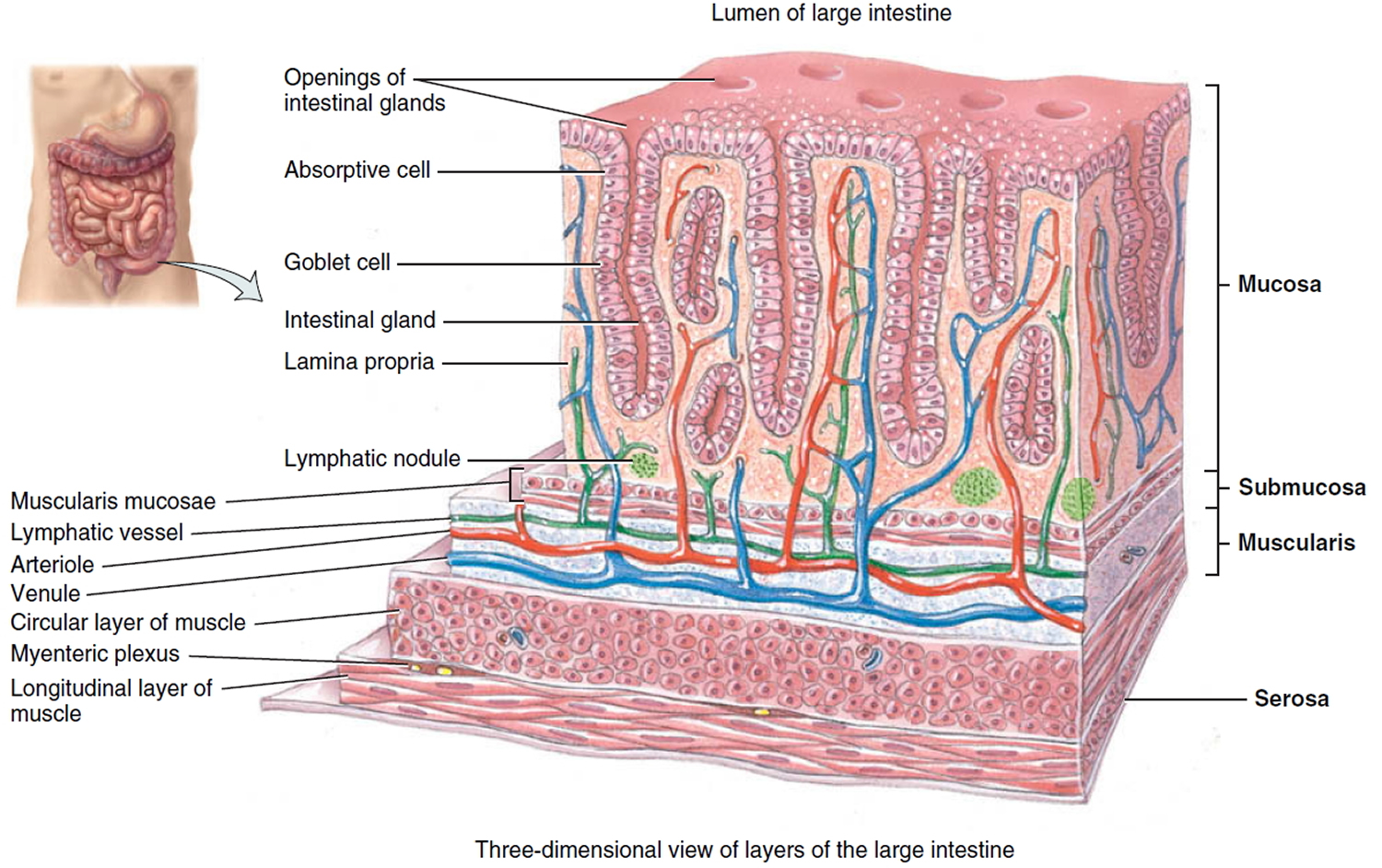
The intestinal wall is made up of multiple layers. The 4 layers of the large intestine from the lumen outward are the mucosa, submucosa, muscular layer, and serosa. The muscular layer is made up of 2 layers of smooth muscle, the inner, circular layer, and the outer, longitudinal layer. These layers contribute to the motility of the large intestine. There are 2 types of motility present in the colon, haustral contraction and mass movement. Haustra are saccules in the colon that give it its segmented appearance. Haustral contraction is activated by the presence of chyme and serves to move food slowly to the next haustra, along with mixing the chyme to help with water absorption. Mass movements are stronger and serve to move the chyme to the rectum quickly.
Absorption of Water and Electrolytes
Absorption of water occurs by osmosis. Water diffuses in response to an osmotic gradient established by the absorption of electrolytes. Sodium is actively absorbed in the colon by sodium channels. Potassium is either absorbed or secreted depending on the concentration in the lumen. The electrochemical gradient created by the active absorption of sodium allows for this. Chloride ions are exchanged for bicarbonate ions across an electrochemical gradient.
Production/Absorption of Vitamins
The colon also plays a role in providing required vitamins through an environment that is conducive for bacterial cultivation. The colon houses trillions of bacteria that protect our gut and produce vitamins. The bacteria in the colon produce substantial amounts of vitamins by fermentation. Vitamin K and B vitamins, including biotin, are produced by the colonic bacteria. These vitamins are then absorbed into the blood. When dietary intake of these vitamins is low in an individual, the colon plays a significant role in minimizing vitamin disparity.
Mechanism
The wall of the large intestine contains the typical four layers found in the rest of the gastrointestinal tract: mucosa, submucosa, muscularis, and serosa. The mucosa consists of simple columnar epithelium, lamina propria (areolar connective tissue), and muscularis mucosae (smooth muscle). The epithelium contains mostly absorptive and goblet cells. The absorptive cells function primarily in water absorption; the goblet cells secrete mucus that lubricates the passage of the colonic contents. Both absorptive and goblet cells are located in long, straight, tubular intestinal glands (crypts of Lieberkühn) that extend the full thickness of the mucosa. Solitary lymphatic nodules are also found in the lamina propria of the mucosa and may extend through the muscularis mucosae into the submucosa.
Compared to the small intestine, the mucosa of the large intestine does not have as many structural adaptations that increase surface area. There are no circular folds or villi; however, microvilli are present on the absorptive cells. Consequently, much more absorption occurs in the small intestine than in the large intestine.
The mucosa of the large intestine has a simple columnar epithelium in all regions except the lower half of the anal canal, where it has a nonkeratinized stratified squamous epithelium. The latter provides more resistance to the abrasion caused by the passage of feces. There are no circular folds or villi in the large intestine, but there are intestinal crypts. They are deeper than in the small intestine and have a greater density of goblet cells; mucus is their only significant secretion. The lamina propria and submucosa have an abundance of lymphatic tissue, providing protection from the bacteria that densely populate the large intestine.
The submucosa of the large intestine consists of areolar connective tissue. The muscularis consists of an external layer of longitudinal smooth muscle and an internal layer of circular smooth muscle. Unlike other parts of the gastrointestinal tract, portions of the longitudinal muscles are thickened, forming three conspicuous bands called the teniae coli that run most of the length of the large intestine. The teniae coli are separated by portions of the wall with less or no longitudinal muscle. Tonic contractions of the bands gather the colon into a series of pouches called haustra (shaped like pouches), which give the colon a puckered appearance. A single layer of circular smooth muscle lies between teniae coli. The serosa of the large intestine is part of the visceral peritoneum. Small pouches of visceral peritoneum filled with fat are attached to teniae coli and are called omental (fatty) appendices.
Figure 5. Large intestine anatomy
Mechanical Digestion in the Large Intestine
The passage of chyme from the ileum into the cecum is regulated by the action of the ileocecal sphincter. Normally, the valve remains partially closed so that the passage of chyme into the cecum usually occurs slowly. Immediately after a meal, a gastroileal reflex intensifies peristalsis in the ileum and forces any chyme into the cecum. The hormone gastrin also relaxes the sphincter. Whenever the cecum is distended, the degree of contraction of the ileocecal sphincter intensifies.
Movements of the colon begin when substances pass the ileocecal sphincter. Because chyme moves through the small intestine at a fairly constant rate, the time required for a meal to pass into the colon is determined by gastric emptying time. As food passes through the ileocecal sphincter, it fills the cecum and accumulates in the ascending colon.
The most common type of colonic motility is a type of segmentation called haustral contractions, which occur about every 30 minutes. Distension of a haustrum with feces stimulates it to contract. This churns and mixes the residue, promotes water and salt absorption, and passes the residue distally to another haustrum. Peristalsis also occurs, although at a slower rate (3–12 contractions per minute) than in more proximal portions of the tract. A final type of movement is mass peristalsis, a strong peristaltic wave that begins at about the middle of the transverse colon and quickly drives the contents of the colon into the rectum. Because food in the stomach initiates this gastrocolic reflex in the colon, mass peristalsis usually takes place three or four times a day, during or immediately aft er a meal. They last about 15 minutes and move residue several centimeters at a time. Mass peristalsis occur especially in the transverse to sigmoid colon, often within an hour after breakfast, moving the feces that accumulated and stretched the colon overnight.
The large intestine takes 36 to 48 hours to reduce the residue of a meal to feces, with the residue spending the greatest time (about 24 h) in the transverse colon. The colon doesn’t chemically change the residue, but reabsorbs water and electrolytes (especially NaCl) from it. Feces usually consist of about 75% water and 25% solids. The solids are about 30% bacteria, 30% undigested dietary fiber, 10% to 20% fat, and smaller amounts of protein, sloughed epithelial cells, salts, mucus, and other digestive secretions. The fat is not from the diet but from bacteria and broken-down epithelial cells.
Chemical Digestion in the Large Intestine
The final stage of digestion occurs in the colon through the activity of bacteria that inhabit the lumen. Mucus is secreted by the glands of the large intestine, but no enzymes are secreted. Chyme is prepared for elimination by the action of bacteria, which ferment any remaining carbohydrates and release hydrogen, carbon dioxide, and methane gases. These gases contribute to flatus (gas) in the colon, termed flatulence when it is excessive. Bacteria also convert any remaining proteins to amino acids and break down the amino acids into simpler substances: indole, skatole, hydrogen sulfide, and fatty acids. Some of the indole and skatole is eliminated in the feces and contributes to their odor; the rest is absorbed and transported to the liver, where these compounds are converted to less toxic compounds and excreted in the urine.
Bacteria also decompose bilirubin to simpler pigments, including stercobilin, which gives feces their brown color. Bacterial products that are absorbed in the colon include several vitamins needed for normal metabolism, among them some B vitamins and vitamin K.
Large Intestine Microbes and Gas
The large intestine harbors about 800 species of bacteria collectively called the gut microbiome. You have a mutually beneficial relationship with many of these. You provide them with room and board while they provide you with nutrients from your food that you are not equipped to extract on your own. For example, they digest cellulose, pectin, and other plant polysaccharides for which you have no digestive enzymes, and you absorb the resulting sugars. Thus, you get more nutrition from your food because of these bacteria than you would get without them. Indeed, one person may get more calories than another from the same amount of food because of differences in their bacterial populations. Some bacteria also synthesize B vitamins and vitamin K, which are absorbed by the colon. This vitamin K is especially important because the diet alone usually does not provide enough to ensure adequate blood clotting.
One of the less desirable and sometimes embarrassing products of these bacteria is intestinal gas. The large intestine contains about 7 to 10 L of gas, expelling about 500 mL/day as flatus and reabsorbing the rest. Much of this is swallowed air that has worked its way through the digestive tract, but the gut microbes add to it. Painful cramping can result when undigested nutrients pass into the colon and furnish an abnormal substrate for bacterial action, so the bacteria produce excess gas—for example, in lactose intolerance. Flatus is composed mostly of nitrogen (N2), carbon dioxide (CO2), hydrogen (H2), methane (CH4), hydrogen sulfide (H2S), and two amines: indole and skatole. Indole, skatole, and H2S produce most of the odor of flatus and feces, whereas the others are odorless. The hydrogen gas is combustible and has been known to explode during the use of electrical cauterization in surgery.
Absorption and Feces Formation in the Large Intestine
By the time chyme has remained in the large intestine 3–10 hours, it has become solid or semisolid because of water absorption and is now called feces. Chemically, feces consist of water, inorganic salts, sloughed-off epithelial cells from the mucosa of the gastrointestinal tract, bacteria, products of bacterial decomposition, unabsorbed digested materials, and indigestible parts of food. Although 90% of all water absorption occurs in the small intestine, the large intestine absorbs enough to make it an important organ in maintaining the body’s water balance. Of the 0.5–1.0 liter of water that enters the large intestine, all but about 100–200 mL is normally absorbed via osmosis. The large intestine also absorbs ions, including sodium and chloride, and some vitamins.
The Defecation Reflex
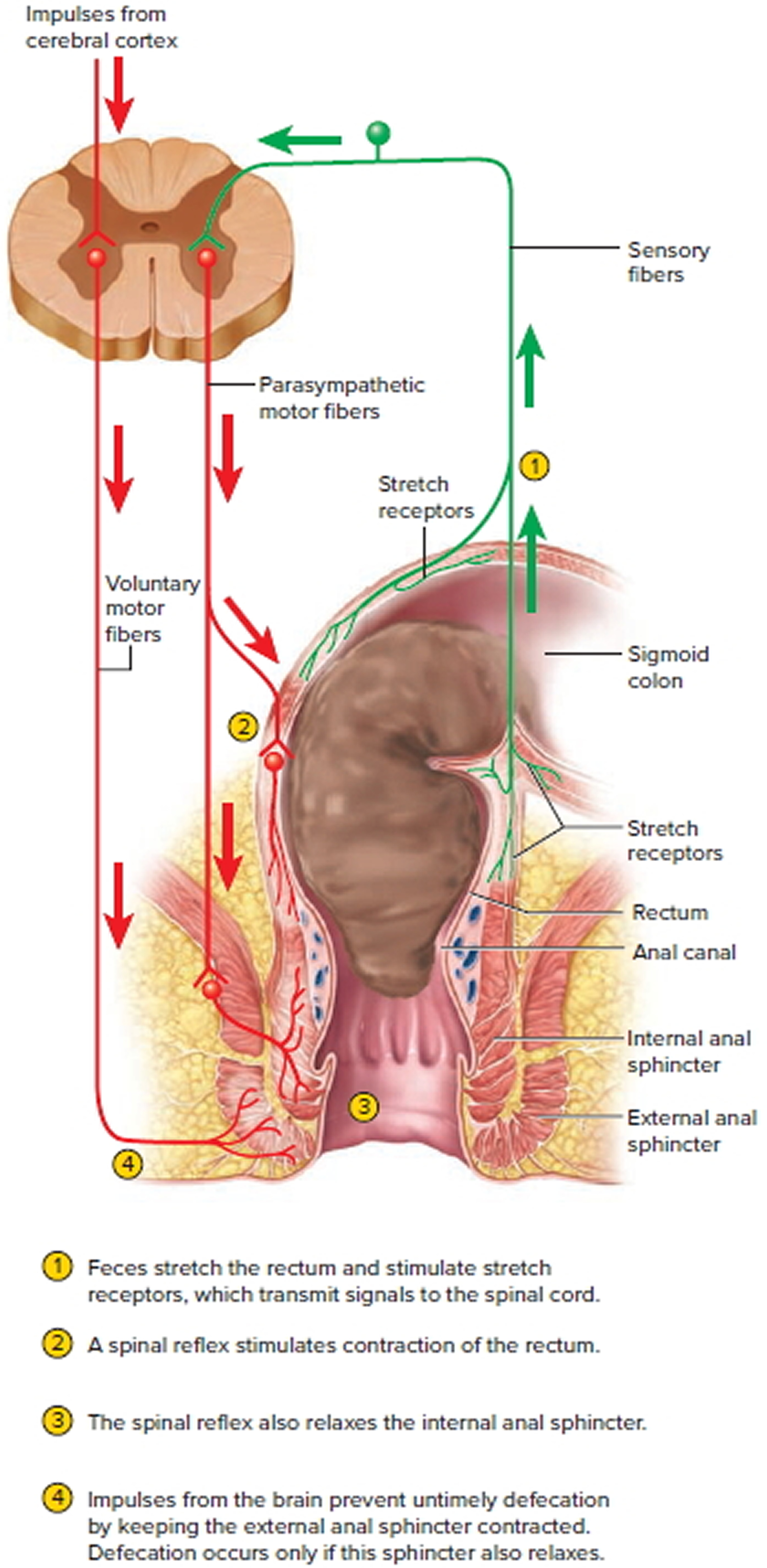
Mass peristaltic movements push fecal material from the sigmoid colon into the rectum. The resulting distension of the rectal wall stimulates stretch receptors, which initiates a defecation reflex that results in defecation, the elimination of feces from the rectum through the anus. The defecation reflex occurs as follows: In response to distension of the rectal wall, the receptors send sensory nerve impulses to the sacral spinal cord.
Motor impulses from the cord travel along parasympathetic nerves back to the descending colon, sigmoid colon, rectum, and anus. The resulting contraction of the longitudinal rectal muscles shortens the rectum, thereby increasing the pressure within it. This pressure, along with voluntary contractions of the diaphragm and abdominal muscles, plus parasympathetic stimulation, opens the internal anal sphincter.
The external anal sphincter is voluntarily controlled. If it is voluntarily relaxed, defecation occurs and the feces are expelled through the anus; if it is voluntarily constricted, defecation can be postponed. Voluntary contractions of the diaphragm and abdominal muscles aid defecation by increasing the pressure within the abdomen, which pushes the walls of the sigmoid colon and rectum inward. If defecation does not occur, the feces back up into the sigmoid colon until the next wave of mass peristalsis stimulates the stretch receptors, again creating the urge to defecate. In infants, the defecation reflex causes automatic emptying of the rectum because voluntary control of the external anal sphincter has not yet developed.
Figure 6. Defecation neural control
The amount of bowel movements that a person has over a given period of time depends on various factors such as diet, health, and stress. The normal range of bowel activity varies from two or three bowel movements per day to three or four bowel movements per week. Diarrhea is an increase in the frequency, volume, and fluid content of the feces caused by increased motility of and decreased absorption by the intestines. When chyme passes too quickly through the small intestine and feces pass too quickly through the large intestine, there is not enough time for absorption. Frequent diarrhea can result in dehydration and electrolyte imbalances. Excessive motility may be caused by lactose intolerance, stress, and microbes that irritate the gastrointestinal mucosa.
Constipation refers to infrequent or difficult defecation caused by decreased motility of the intestines. Because the feces remain in the colon for prolonged periods, excessive water absorption occurs, and the feces become dry and hard. Constipation may be caused by poor habits (delaying defecation), spasms of the colon, insufficient fiber in the diet, inadequate fluid intake, lack of exercise, emotional stress, and certain drugs. A common treatment is a mild laxative, such as milk of magnesia, which induces defecation. However, many physicians maintain that laxatives are habit-forming, and that adding fiber to the diet, increasing the amount of exercise, and increasing fluid intake are safer ways of controlling this common problem.
Large intestine problems
Pathology of the large intestine is common. One out of every 10 Americans over the age of 40 have diverticular disease, and around 3 million people in the United States have inflammatory bowel disease 1. It is important to incorporate a healthy diet and lifestyle to maintain a properly functioning colon. Eating a diet high in fiber and drinking plenty of water allows food to easily move through the colon, keeping the colon relatively clean, which can decrease the risk of diverticular disease. It is also important to maintain healthy colonic flora. Maintaining healthy colonic flora will decrease the risk of abdominal bloating, gas, diarrhea, constipation, and infectious colitis.
Disorders of Large Intestinal Motility
Irritable Bowel Syndrome
Irritable bowel syndrome is thought to be due to psychological factors influencing the motility of the large intestine via the extrinsic autonomic nervous system. During times of stress, segmentation contractions may be increased or decreased, resulting in constipation or diarrhea.
Hirschsprung Disease: Megacolon
Hirschsprung disease is a disorder at birth that occurs when nerve cells are absent (Auerbach’s Plexus) in the muscles of the colon. This affects motility in the colon, making it difficult to pass stool.
Diverticulosis/Diverticulitis
Diverticulosis is a disorder in which pockets develop in the colonic mucosa due to the weakness of the muscle layers in the colon wall. This usually occurs over time from chronic attrition of the aging process. Diverticulitis can develop if these pockets get infected or inflamed, causing abdominal pain and change in bowel movements. Diverticular disease is very common, especially in older adults.
Large Intestine Inflammation
Inflammatory Bowel Disease
Inflammatory bowel disease includes either Crohn’s disease or ulcerative colitis. Both cause inflammation and scarring within the digestive tract, disrupting the normal function. The cause of inflammatory bowel disease is not known but is likely due to an abnormal response of the immune system. Ulcerative colitis is confined to the large intestine, whereas Crohn’s disease can occur anywhere in the GI (gastrointestinal) tract, from mouth to anus.
Ischemic colitis
Ischemic colitis is more common in the elderly and occurs when there is decreased blood flow to the colon. Decreased blood flow can cause inflammation or injury to the colon. Some causes of ischemic colitis are atherosclerosis of arteries, low blood pressure, blood clots, and bowel obstruction.
Infectious colitis
Infectious colitis can occur from many different viruses, bacteria, or parasites. Infectious colitis most commonly occurs due to ingestion of contaminated food or water, introducing the infectious organism into the colon. The most common causes are Escherichia coli, Campylobacter, Shigella, and Salmonella. These infectious organisms invade the colon, cause inflammation, and affect the normal function, causing abdominal pain and diarrhea. Clostridium difficile is another organism that can cause colitis in association with antibiotic use. Clostridium difficile is part of healthy, normal flora in the colon but can cause problems if it overgrows. Antibiotic use can destroy other susceptible normal flora in the colon, allowing overgrowth and invasion of Clostridium difficile.
- Azzouz LL, Sharma S. Physiology, Large Intestine. [Updated 2018 Jun 14]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2018 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK507857[↩]


{kind=link}