Contents
- What is large intestine pain
What is large intestine pain
Pain in the large intestine is pain that you feel anywhere between your chest and groin. This is often referred to as the abdomen, stomach region or belly. Acute abdominal pain has many potential underlying causes, ranging from benign, self-limited conditions to life-threatening surgical emergencies. The myriad causes of abdominal pain is broad, encompassing gastrointestinal, gynecologic, urologic, vascular, and musculoskeletal conditions. Although the patient history, physical examination, and laboratory test results can narrow the differential diagnosis, imaging is often required for definitive diagnosis and treatment.
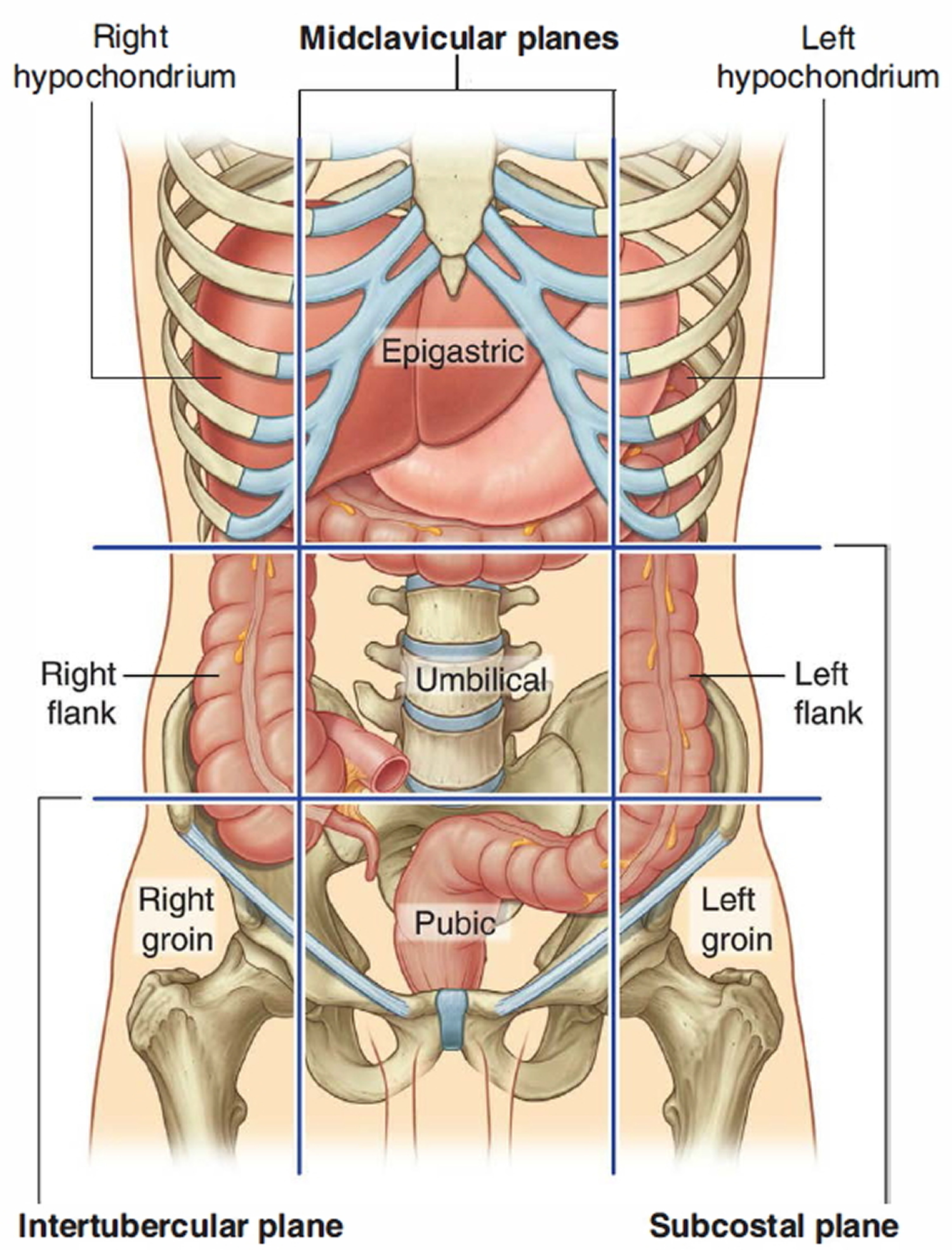
The large intestine consists of the cecum, appendix, colon, rectum, and anal canal. Your large intestine extends from the distal end of the ileum to the anus, a distance of approximately 1.5 m in adults (5 ft) long and 6.5 cm (2.5 in.) in diameter. Beginning in the right groin as the cecum, with its associated appendix, the large intestine continues upward as the ascending colon through the right flank and into the right hypochondrium. The ascending colon begins at the ileocecal valve and passes up the right side of the abdominal cavity. It makes a 90° turn at the right colic (hepatic) flexure, near the right lobe of the liver, and crosses the abdomen as the transverse colon to the left hypochondrium. At this position, just below the spleen, the large intestine bends downward, forming the left colic flexure (splenic flexure) and continues as the descending colon through the left flank and into the left groin. Ascending, transverse, and descending colons thus form a squarish, three-sided frame around the small intestine. The function of your large intestine is to absorb fluids and salts from the gut contents, thus forming feces.
The type, quality, onset, duration and location of abdominal pain are often a helpful starting point in differentiating the many potential underlying causes of abdominal pain.
To help physicians make the most appropriate diagnostic decisions for specific clinical conditions, below are a list of questions that can assist them to narrow down the potential causes of your abdominal pain.
When should you see a doctor or get urgent medical attention ?
If you answer YES to any of the following questions concerning your abdominal pain, you should contact your doctor immediately.
- Is your pain steady, severe, or regularly recurring ?
- Does your pain impair your ability to work or perform your routine activities ?
- Have you lost weight or your appetite ?
- Is your pain associated with nausea and vomiting ?
- Do you experience fever ?
- Have your bowel habits changed ?
- Do you experience difficulty in swallowing ?
- Does your pain awaken you from sleep ?
- Do you have a previous history of ulcers, gastro-esophageal reflux, gallstones, inflammatory bowel disease (ulcerative colitis, Crohnís disease), and intestinal surgery ?
- Are you taking any medicines that can cause ulcers, such as aspirin or other medications commonly used or prescribed for arthritis or headaches ?
Get medical help immediately if:
- You have abdominal pain that is sudden and sharp.
- You also have chest, neck or shoulder pain.
- You have pain in, or between, your shoulder blades with nausea.
- You’re vomiting blood or have blood in your stool.
- Your abdomen is stiff, hard and tender to touch.
- You are unable to pass stool, especially if you are also vomiting.
- You are currently being treated for cancer.
- You are vomiting blood or have blood in your stool (especially if bright red, maroon or dark, tarry black).
- You have chest, neck, or shoulder pain.
- You have tenderness in your belly, or your belly is rigid and hard to the touch.
- You are pregnant or could be pregnant.
- You had a recent injury to your abdomen.
- You have difficulty breathing.
What does your pain feel like ?
How bad your pain is does not always reflect the seriousness of the condition causing the pain.
For example, you might have very bad abdominal pain if you have gas or stomach cramps due to viral gastroenteritis.
However, life-threatening conditions, such as colon cancer or early appendicitis, may only cause mild pain or no pain.
Other ways to describe pain in your abdomen include:
- Generalized pain: This means that you feel it in more than half of your belly. This type of pain is more typical for a stomach virus, indigestion, or gas. If the pain becomes more severe, it may be caused by a blockage of the intestines.
- Localized pain: This is pain found in only one area of your belly. It is more likely to be a sign of a problem in an organ, such as the appendix, gallbladder, or stomach.
- Cramp-like pain: This type of pain is not serious most of the time. It is likely to be due to gas and bloating, and is often followed by diarrhea. More worrisome signs include pain that occurs more often, lasts than 24 hours, or occurs with a fever.
- Colicky pain: This type of pain comes in waves. It very often starts and ends suddenly, and is often severe. Kidney stones and gallstones are common causes of this type of belly pain.
- Constant pain. There may be some variation in the intensity but, overall, this type of pain is distinctively steady. Other descriptions which have been used include “aching, burning, gnawing, hunger, or sharp” pain. This type of pain can arise from deep inflammation involving any of the abdominal organs and the abdominal cavity. Ulcers, blockage of the gallbladder by stones, and local areas of infection called abscesses can cause this type of pain. Irritation of the inner lining of the esophagus by gastric acid and irritation of the outside of the intestines and body cavity by leakage of blood, intestinal contents, and bile can also cause this type of pain.
How long does the pain last ?
Pain which lasts for only seconds or a minute usually does not have a specific cause. Many people will experience a rare brief spell of abdominal pain, which is not serious. Pain which lasts for hours or days should be considered potentially serious and medical attention should be obtained.
When does the pain occur ?
Pain may occur spontaneously, at any time. Pain which awakens someone from sleep is regarded as potentially serious. It may occur before or after meals and before or after bowel movements. The heartburn pain of gastroesophageal reflux disease (GERD) may occur just after a meal. Gallbladder pain may develop after meals as can pain from the pancreas and intestinal obstruction. The irritable bowel syndrome (IBS) is a common gastrointestinal problem which typically is associated with gaseous or crampy pain after meals along with a sensation of bloating. Inflammatory diseases of the intestine associated with diarrhea often cause crampy pain before or after bowel movements.
Figure 1. Abdomen
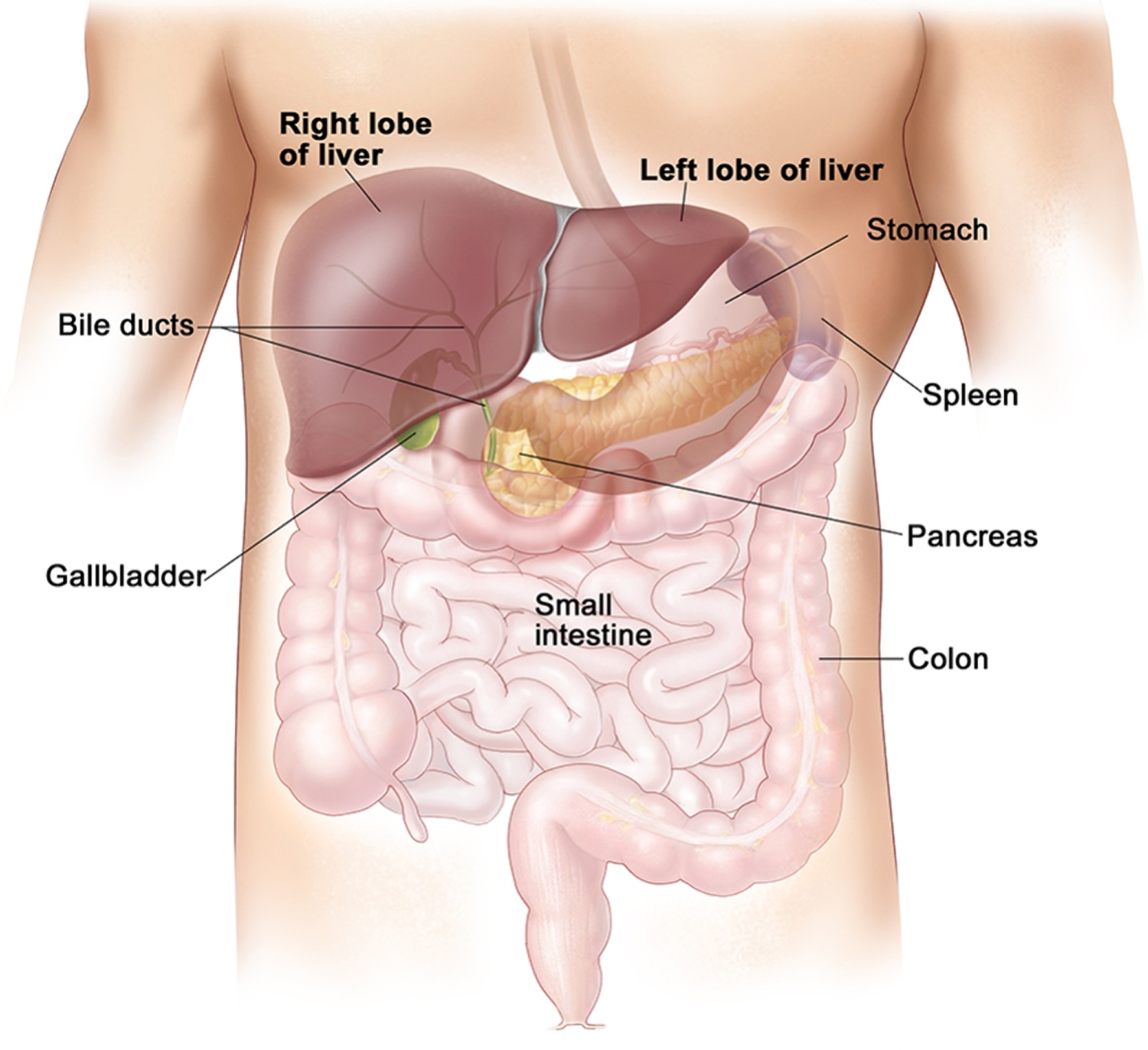
Figure 2. Large intestine
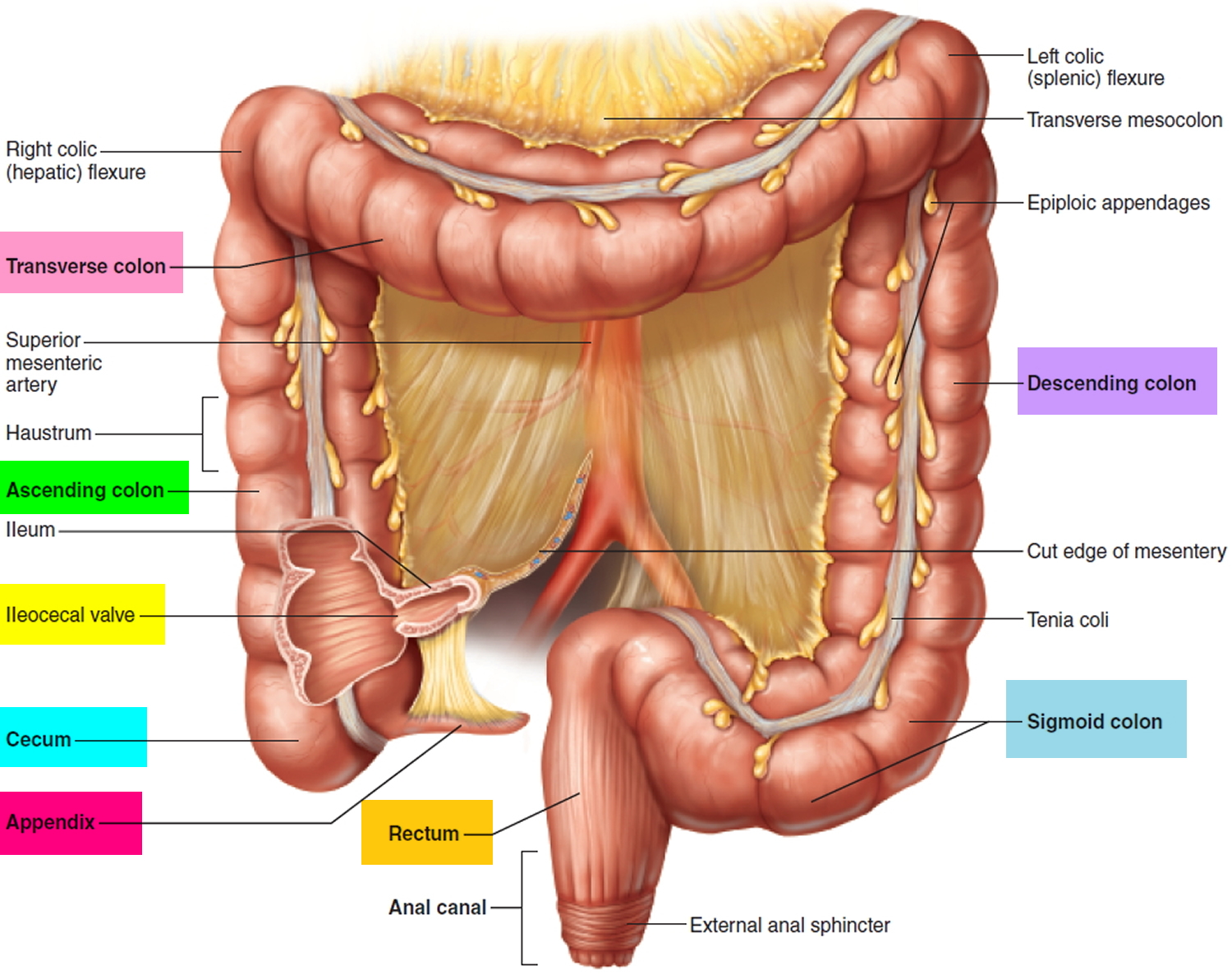
Figure 3. Large intestine location
Where is the pain located ?
The place where the pain is initially felt and where it may travel (radiate) is very important in determining the cause of the pain. Pain located in the center of the upper abdomen may arise from the esophagus, stomach, duodenum, liver, pancreas, or bile ducts. Pain from the gallbladder and an inflamed liver will more often be located toward the right side of the upper abdomen. Gallbladder pain may also radiate through the right shoulder blade. Pain from an ulcer or irritation of the pancreas may radiate through to the back. Pain arising from the small intestine can localize around the belly button.
Pain arising from the large intestine pain may localize to either the right, left, or middle of the abdomen below the belly button. Pain developing from inside the pelvis will often be experienced as a pressure-like discomfort in the rectal area. The most common locations of minor pain, often gas-like, are in the middle to upper abdomen and in the lower and left abdomen.
Right Upper Quadrant Pain
Acute cholecystitis (acute inflammation of the gallbladder) is a primary diagnostic consideration in patients presenting with new-onset right upper quadrant pain. History, physical examination, and laboratory testing are often insufficient for diagnosing acute cholecystitis without further workup 1. The American College of Radiology Appropriateness Criteria recommend ultrasonography as the initial imaging test for patients presenting with right upper quadrant pain 2. Although a meta-analysis of 57 studies from 1978 to 2010 showed that cholescintigraphy has better sensitivity and specificity (96% and 90%, respectively) than ultrasonography (81% and 83%, respectively) for detecting acute cholecystitis 3, ultrasonography is more readily available, can identify other potential causes of pain and does not expose the patient to ionizing radiation.
Right Lower Quadrant Pain
Acute appendicitis is the most common cause of right lower quadrant pain requiring surgery 4 and is the focus of imaging considerations in this location. The American College of Radiology Appropriateness Criteria recommend CT as the initial imaging test of choice for patients presenting with right lower quadrant pain 4. A meta-analysis of six studies from 1994 to 2005 found that CT has better sensitivity and specificity (91% and 90%, respectively) than ultrasonography (78% and 83%, respectively) for detecting acute appendicitis 5. CT also provides more consistent results than ultrasonography 4, because ultrasonography is a highly operator-dependent technique that varies based on the skill and experience level of the technologist and radiologist. Routine use of CT for evaluation of appendicitis has reduced the negative-finding appendectomy rate from 24% to 3%,16 and it has been shown to decrease overall costs by $447 per patient by preventing unnecessary appendectomies and hospital admissions 4.
Left Lower Quadrant Pain
Acute sigmoid diverticulitis is the most common cause of left lower quadrant pain in adults and is the focus of imaging recommendations for this quadrant. Diverticulitis is often diagnosed clinically without radiologic examination, but imaging should be considered if the diagnosis is unclear or if complications (e.g., abscess, fistula, obstruction, perforation) are suspected. The American College of Radiology recommends CT as the initial imaging test for the evaluation of left lower quadrant pain 6. CT has a sensitivity of greater than 95% for detecting diverticulitis,18 and it can provide information about the extent of disease and the presence of abscess formation 6. In addition, CT can reveal disease processes other than diverticulitis that have a similar clinical presentation.
Ultrasonography has also been studied for evaluation of suspected diverticulitis. Although some studies have shown similar sensitivity of ultrasonography compared with CT for detecting diverticulitis, others have shown significantly lower sensitivity with ultrasonography 7. Variation in ultrasonography results may be due to the highly operator-dependent technique and the limitations of patient body habitus, compared with other imaging modalities. Preliminary data on the use of MRI for the evaluation of diverticulitis suggest that it may be useful, with sensitivity of 86% to 94% and specificity of 88% to 92% 6.
Nonlocalized Abdominal Pain
Although certain disease processes such as cholecystitis, appendicitis, and diverticulitis commonly present with pain localized to a specific quadrant of the abdomen, diffuse abdominal pain is also a common clinical presentation. The differential diagnosis of acute nonlocalized abdominal pain is broad. CT is typically the imaging modality of choice if there is significant concern for serious pathology or if the diagnosis is unclear from history, physical examination, and laboratory testing 8. A prospective study of 584 patients with nontraumatic abdominal pain in an emergency department setting found that CT results altered the leading diagnosis in 49% of patients and changed the management plan in 42% of patients 9.
What relieves the pain ?
Whether the pain is new or has been recurring for some time, most people will try to relieve it or will notice what makes the pain feel better. Belching is a common maneuver used to relieve upper abdominal discomfort. The belch is created by swallowing air and immediately expelling it. It is a learned response which can become a habit. Belching does not provide much, if any, clue to the origins of upper abdominal pain. Flatus, the expulsion of gas from the rectum, may relieve crampy abdominal pains due to distension or stretching of the colon and rectum. Some individuals naturally have more gas than others which may cause discomfort, create cramps, and be relieved by the passage of flatus. Certain foods, such as beans, can create excess gas and cramping which is relieved by the passage of flatus.
The pain of peptic ulcer disease has been commonly referred to as hunger or gnawing pain which is typically relieved by eating. This pain may awaken a person from sleep. These individuals will often keep antacids, water or crackers on their bed stand to help relieve the night time pain.
More serious pain will cause restlessness, the need to be still, or to assume a certain position. An obstructed organ such as the intestine or gallbladder typically causes restlessness with a need for movement such as rocking or pacing. A perforation or leakage of intestinal contents will cause one to be very still to minimize irritation of the abdominal cavity and outer lining of the intestines. With inflammation in the lower abdomen, such as appendicitis, the pain may be relieved by lying down with the legs drawn up.
Deep inflammation of the upper abdomen, as can occur with inflammation of the pancreas, may feel better by leaning forward or curling up in a ball on one side or the other.
What other symptoms are associated with the pain ?
Severe pain of any kind may be associated with sweating. This is not a specific observation. Nausea and vomiting may be important responses to pain and may indicate a blocked organ such as the stomach, intestine or gallbladder. Nausea and vomiting are common symptoms associated with inflammation of the pancreas.
The abdomen may become swollen or distended with gas when there is blockage of the large intestine. Blocked large intestines may also be associated with loud grumbling sounds which usually occur at the same time as the crampy waves of pain. These grumbling sounds may also occur normally and most often between meals. Blockage of the stomach may be due to an ulcer at the very end of the stomach. In addition to the steady pain of an ulcer, the individual may be aware of a sloshing sound of fluid in the blocked stomach. This is most noticeable when lying down and changing positions.
Fever with or without shaking chills can accompany intestinal infections, blockage of the bile ducts, and localized areas of infection called abscesses. The presence of shaking chills suggests serious infection with passage of bacteria into the bloodstream.
A change in the color of the urine and stool may accompany the pain from a blocked bile duct. In this setting, the urine becomes very dark, like strong tea and the stool becomes light in color. With a prolonged blockage of the bile duct, the eyes and skin will turn yellow which is called jaundice.
- Crampy pain accompanied by black or bloody stool is a combination of symptoms indicating severe bleeding which requires prompt attention.
Pain arising from the esophagus may be due to irritation and blockage. Individuals with this type of pain problem will describe difficulty swallowing foods, especially solids. When there is a complete blockage of swallowed food, the individual will have trouble swallowing saliva.
Causes of abdominal pain
Many different conditions can cause abdominal pain. The key is to know when you need to get medical care right away. Sometimes you may only need to call a health care provider if your symptoms continue.
Less serious causes of abdominal pain include:
- Constipation
- Irritable bowel syndrome
- Food allergies or intolerance (such as lactose intolerance)
- Food poisoning
- Stomach flu
Other possible causes include:
- Appendicitis
- Abdominal aortic aneurysm (bulging and weakening of the major artery in the body)
- Bowel blockage or obstruction
- Cancer of the stomach, colon (large bowel), and other organs
- Cholecystitis (inflammation of the gallbladder) with or without gallstones
- Decreased blood supply to the intestines (ischemic bowel)
- Diverticulitis (inflammation and infection of the colon)
- Heartburn, indigestion, or gastroesophageal reflux (GERD)
- Inflammatory bowel disease (Crohn disease or ulcerative colitis)
- Kidney stones
- Pancreatitis (swelling or infection of the pancreas)
- Ulcers
Sometimes, abdominal pain may occur due to a problem somewhere else in your body, such as your chest or pelvic area. For example, you may have abdominal pain if you have:
- Severe menstrual cramps
- Endometriosis
- Muscle strain
- Pelvic inflammatory disease (PID)
- Tubal (ectopic) pregnancy
- Urinary tract infections.
- Trowbridge RL, Rutkowski NK, Shojania KG. Does this patient have acute cholecystitis? [published correction appears in JAMA. 2009;302(7):739]. JAMA. 2003;289(1):80–86.[↩]
- Yarmish GM, Smith MP, Rosen MP, et al. ACR appropriateness criteria. Right upper quadrant pain. https://acsearch.acr.org/docs/69474/Narrative/[↩]
- Kiewiet JJ, Leeuwenburgh MM, Bipat S, Bossuyt PM, Stoker J, Boermeester MA. A systematic review and meta-analysis of diagnostic performance of imaging in acute cholecystitis. Radiology. 2012;264(3):708–720.[↩]
- Smith MP, Katz DS, Rosen MP, et al. ACR appropriateness criteria. Right lower quadrant pain—suspected appendicitis. https://acsearch.acr.org/docs/69357/Narrative/[↩][↩][↩][↩]
- van Randen A, Bipat S, Zwinderman AH, Ubbink DT, Stoker J, Boermeester MA. Acute appendicitis: meta-analysis of diagnostic performance of CT and graded compression US related to prevalence of disease. Radiology. 2008;249(1):97–106.[↩]
- McNamara MM, Lalani T, Camacho MA, et al. ACR appropriateness criteria. Left lower quadrant pain—suspected diverticulitis. https://acsearch.acr.org/docs/69356/Narrative/[↩][↩][↩]
- van Randen A, Laméris W, van Es HW, et al.; OPTIMA Study Group. A comparison of the accuracy of ultrasound and computed tomography in common diagnoses causing acute abdominal pain. Eur Radiol. 2011;21(7):1535–1545.[↩]
- Yaghmai V, Rosen MP, Lalani T, et al. ACR appropriateness criteria. Acute (nonlocalized) abdominal pain and fever or suspected abdominal abscess. https://acsearch.acr.org/docs/69467/Narrative/[↩]
- Abujudeh HH, Kaewlai R, McMahon PM, et al. Abdominopelvic CT increases diagnostic certainty and guides management decisions: a prospective investigation of 584 patients in a large academic medical center. AJR Am J Roentgenol. 2011;196(2):238–243.[↩]





{kind=link}