
Contents
What is Lassa fever
Lassa fever is an animal-borne, or zoonotic, acute viral illness. Lassa fever is part of a group of conditions known as viral hemorrhagic fevers. Lassa fever is caused by infection with the Lassa virus, the virus is named after the town in Nigeria where the first identified cases occurred. The natural reservoir of the Lassa virus is the “multimammate rat” (Mastomys natalensis), a rodent found commonly in rural areas of tropical Africa that often colonizes in or around human homes where food is stored.
Lassa fever is endemic in parts of West Africa including Sierra Leone, Liberia, Guinea and Nigeria. Neighboring countries are also at risk, as the animal vector for Lassa virus, the “multimammate rat” (Mastomys natalensis) is distributed throughout the region.
In West Africa, Lassa virus is carried by rats and spread to humans through contact with urine or droppings of infected rats. In rare cases Lassa fever can be spread from person to person through direct contact with a sick person’s blood or body fluids. Lassa fever virus is not transmitted through casual contact, and patients are not believed to be infectious before the onset of symptoms.
Lassa fever was discovered in 1969 and is named after the town in Nigeria where the first cases occurred.
An estimated 100,000 to 300,000 infections of Lassa fever occur annually, with approximately 5,000 deaths related to Lassa fever, occur in West Africa each year. Surveillance for Lassa fever is not standardized; therefore, these estimates are crude. In some areas of Sierra Leone and Liberia, it is known that 10-16% of people admitted to hospitals annually have Lassa fever, demonstrating the serious impact the disease has on the region.
While viral hemorrhagic fevers, like Lassa fever, are very serious, they are not common in the U.S. 1.
Lassa fever what you need to know 2:
- Lassa fever is a viral hemorrhagic fever endemic in West Africa
- Lassa fever is predominantly asymptomatic or results in mild febrile symptoms (about 80% of cases). Severe symptoms (such as haemorrhage, respiratory distress, repeated vomiting, facial swelling, shock) occur in around 20% of cases. Overall mortality is around 1%, but observed case fatality rate among hospitalized patients is reported to be up to 70%
- Symptoms of Lassa fever can be difficult to distinguish from malaria and typhoid; therefore, other potentially serious illnesses should be considered in an individual returning from an endemic area with an appropriate history
- Diagnosis is entirely dependent on an accurate history and an understanding of the geography of the disease, supported by laboratory investigations
- Management involves early recognition of infection, effective isolation and infection control, early initiation of the antiviral drug ribavirin, and supportive care in hospital
- Ribavirin is occasionally used as post-exposure prophylaxis for high risk exposure to Lassa virus
Figure 1. Mastomys natalensis rat
Lassa fever outbreak
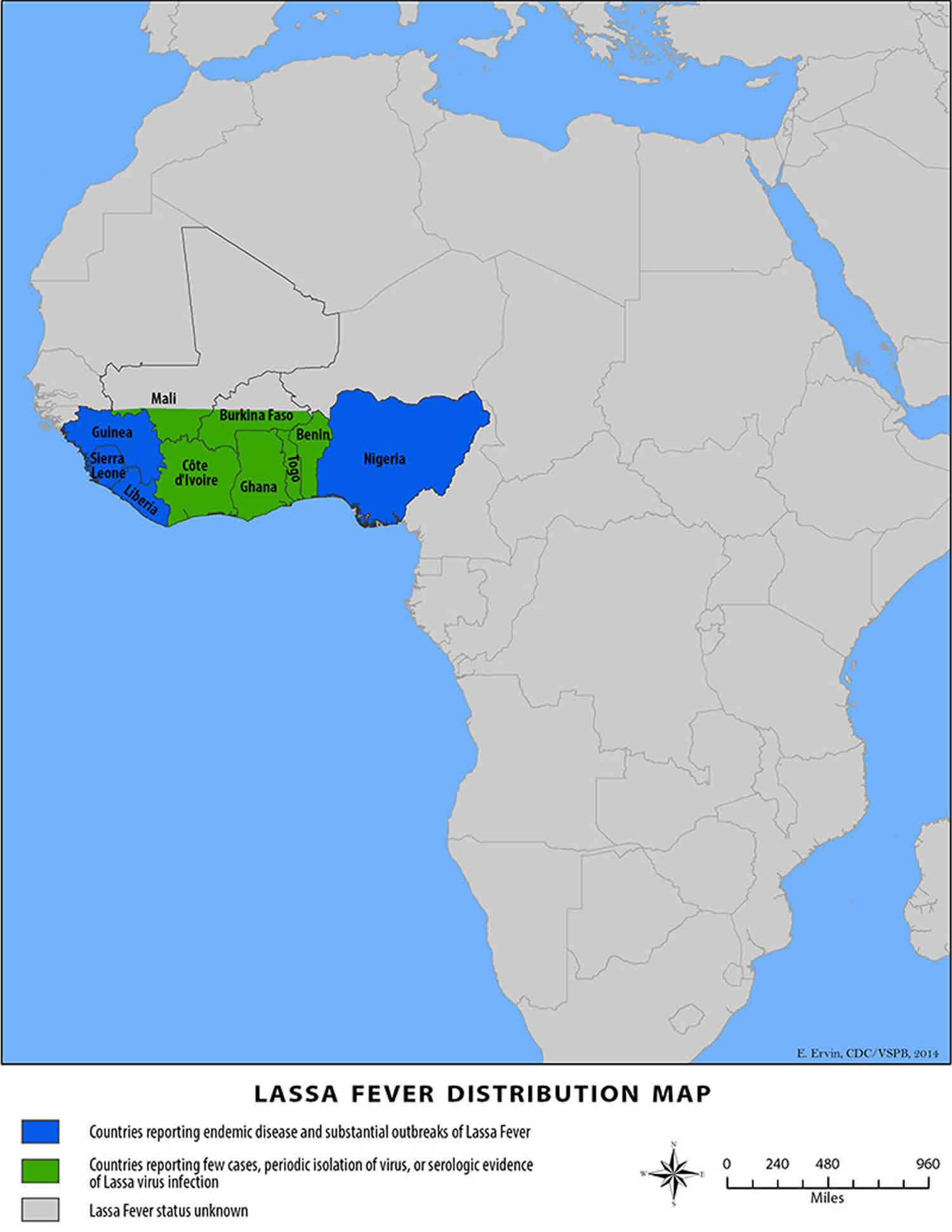
Lassa Fever Outbreak Distribution Map
Countries reporting endemic disease and substantial outbreaks of Lassa fever:
- Guinea,
- Liberia,
- Nigeria,
- Sierra Leone
Countries reporting few cases, periodic isolation of virus, or serological evidence of Lassa virus infection:
- Benin,
- Burkina Faso,
- Cote d’Ivoire,
- Ghana,
- Mali,
- Togo
Figure 2. Lassa fever outbreak distribution map
Lassa fever transmission
The reservoir, or host of Lassa virus is a rodent known as the “multimammate rat” (Mastomys natalensis). Once infected, this rodent is able to excrete virus in urine for an extended time period, maybe for the rest of its life. Mastomys rodents breed frequently, produce large numbers of offspring, and are numerous in the savannas and forests of west, central, and east Africa. In addition, Mastomys readily colonize human homes and areas where food is stored. All of these factors contribute to the relatively efficient spread of Lassa virus from infected rodents to humans.
Transmission of Lassa virus to humans occurs most commonly through ingestion or inhalation. Mastomys rodents shed the virus in urine and droppings and direct contact with these materials, through touching soiled objects, eating contaminated food, or exposure to open cuts or sores, can lead to infection.
Because Mastomys rodents often live in and around homes and scavenge on leftover human food items or poorly stored food, direct contact transmission is common. Mastomys rodents are sometimes consumed as a food source and infection may occur when rodents are caught and prepared. Contact with the virus may also occur when a person inhales tiny particles in the air contaminated with infected rodent excretions. This aerosol or airborne transmission may occur during cleaning activities, such as sweeping.
Direct contact with infected rodents is not the only way in which people are infected; person-to-person transmission may occur after exposure to virus in the blood, tissue, secretions, or excretions of a Lassa virus-infected individual. Casual contact (including skin-to-skin contact without exchange of body fluids) does not spread Lassa virus. Person-to-person transmission is common in health care settings (called nosocomial transmission) where proper personal protective equipment is not available or not used. Lassa virus may be spread in contaminated medical equipment, such as reused needles.
Risk factors for Lassa fever
Individuals at greatest risk of Lassa virus infection are those who live in or visit endemic regions, including Sierra Leone, Liberia, Guinea, and Nigeria and have exposure to the multimammate rat. Risk of exposure may also exist in other west African countries where Mastomys rodents exist. Hospital staff are not at great risk for infection as long as protective measures and proper sterilization methods are used.
Lassa fever prevention
Primary transmission of the Lassa virus from its host to humans can be prevented by avoiding contact with Mastomys rodents, especially in the geographic regions where outbreaks occur. Putting food away in rodent-proof containers and keeping the home clean help to discourage rodents from entering homes. Using these rodents as a food source is not recommended. Trapping in and around homes can help reduce rodent populations; however, the wide distribution of Mastomys in Africa makes complete control of this rodent reservoir impractical.
If you travel to West Africa, the best way to prevent Lassa fever is to avoid rats.
You can also:
- Put food away in rat-proof containers and keep the home clean to discourage rat from entering homes.
- Avoid using these rats as a food source.
- Trap rats in and around homes to reduce rat population.
When caring for patients with Lassa fever, further transmission of the disease through person-to-person contact or nosocomial routes can be avoided by taking preventive precautions against contact with patient secretions (called VHF isolation precautions or barrier nursing methods). Such precautions include wearing protective clothing, such as masks, gloves, gowns, and goggles; using infection control measures, such as complete equipment sterilization; and isolating infected patients from contact with unprotected persons until the disease has run its course.
Further, educating people in high-risk areas about ways to decrease rodent populations in their homes will aid in the control and prevention of Lassa fever. Other challenges include developing more rapid diagnostic tests and increasing the availability of the only known drug treatment, ribavirin.
Lassa fever vaccine
Research is presently under way to develop a vaccine for Lassa fever.
Symptoms of Lassa fever
Signs and symptoms of Lassa fever typically occur 1-3 weeks after the patient comes into contact with the Lassa fever virus. For the majority of Lassa fever virus infections (approximately 80%), symptoms are mild and are undiagnosed.
Mild symptoms include:
- slight fever,
- general malaise,
- weakness,
- headache.
In 20% of infected individuals, however, disease may progress to more serious symptoms including hemorrhaging (in gums, eyes, or nose, as examples), respiratory distress, repeated vomiting, facial swelling, pain in the chest, back, and abdomen, and shock. Neurological problems have also been described, including hearing loss, tremors, and encephalitis.
Death may occur within two weeks after symptom onset due to multi-organ failure.
The most common complication of Lassa fever is deafness. Various degrees of deafness occur in approximately one-third of infections, and in many cases hearing loss is permanent. As far as is known, severity of the disease does not affect this complication: deafness may develop in mild as well as in severe cases.
Approximately 15%-20% of patients hospitalized for Lassa fever die from the illness. However, only 1% of all Lassa virus infections result in death. The death rates for women in the third trimester of pregnancy are particularly high. Spontaneous abortion is a serious complication of infection with an estimated 95% mortality in fetuses of infected pregnant mothers.
Because the symptoms of Lassa fever are so varied and nonspecific, clinical diagnosis is often difficult. Lassa fever is also associated with occasional epidemics, during which the case-fatality rate can reach 50% in hospitalized patients.
Lassa fever diagnosis
Lassa fever is most often diagnosed by using enzyme-linked immunosorbent serologic assays (ELISA), which detect IgM and IgG antibodies as well as Lassa antigen. Reverse transcription-polymerase chain reaction (RT-PCR) can be used in the early stage of disease. The virus itself may be cultured in 7 to 10 days, but this procedure should only be done in a high containment laboratory with good laboratory practices. Immunohistochemistry, performed on formalin-fixed tissue specimens, can be used to make a post-mortem diagnosis.
Lassa fever treatment
Ribavirin, an antiviral drug, has been used with success in Lassa fever patients. Ribavirin has been shown to be most effective when given early in the course of the illness. Patients should also receive supportive care consisting of maintenance of appropriate fluid and electrolyte balance, oxygenation and blood pressure, as well as treatment of any other complicating infections.





{kind=link}