Contents
- What is left ventricular hypertrophy
What is left ventricular hypertrophy
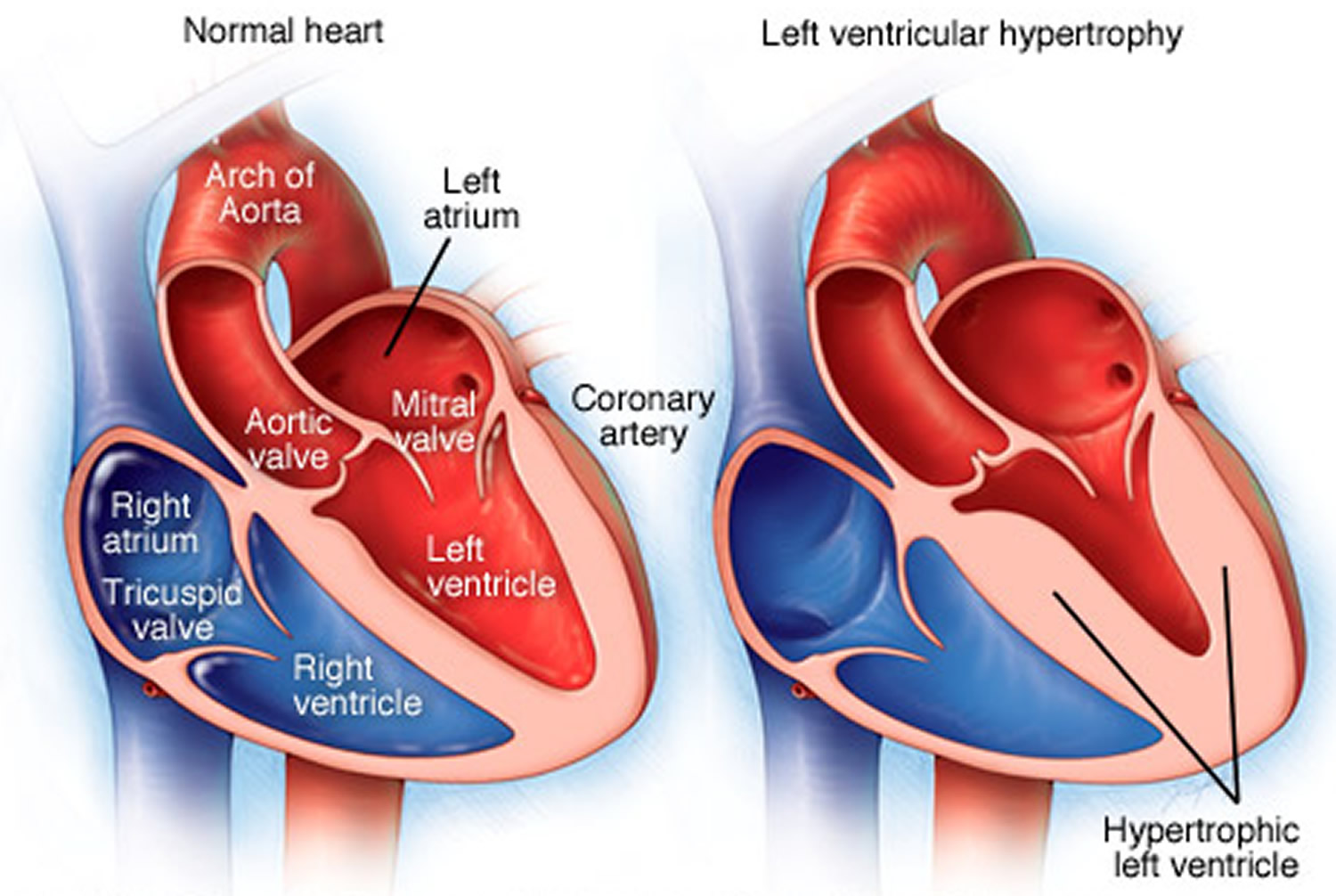
Left ventricular hypertrophy is enlargement and thickening (hypertrophy) of the muscle wall of the left pumping chamber of the heart (left ventricle) which is walls of your heart’s main pumping chamber. Left ventricular hypertrophy can develop in response to some factor — such as high blood pressure or aortic stenosis — that causes the left ventricle muscle to work harder. In response to this pressure overload inside the left ventricle, heart muscle cells may respond by getting thicker along the inner walls of the heart. This thickened wall can cause the left ventricle chamber to weaken, stiffen and lose elasticity, which may prevent healthy blood flow. The enlarged heart muscle loses elasticity and eventually may fail to pump with as much force as needed. Left ventricular hypertrophy is a strong independent predictor of cardiovascular deaths and events and is even worse than triple vessel coronary heart disease [coronary artery disease] 1. The reason why left ventricular hypertrophy is so adverse is because it predates so many different cardiovascular events i.e. left ventricular hypertrophy is intrinsically arrhythmogenic and causes sudden death, left ventricular hypertrophy impedes left ventricular filling and leads to diastolic heart failure, it reduces coronary perfusion reserve and causes ischemia and it causes left atrial enlargement leading to atrial fibrillation and cardio-embolic strokes 2.
Left ventricular hypertrophy affects 1% to 5% of the population, about one third of patients with hypertension 3 and is more prevalent among African-Americans, Caribbean and Mexican-origin Hispanic 4. Left ventricular hypertrophy prevalence ranges from 20% in mildly hypertensive patients to almost 100% in those with severe or complicated hypertension. Findings from prior studies have demonstrated that baseline and serial changes in ECG (electrocardiogram) left ventricular hypertrophy independently predict subsequent cardiovascular events, despite having low sensitivity compared with echocardiographically derived left ventricular hypertrophy.
Left ventricular hypertrophy is more common in people who have uncontrolled high blood pressure. But left ventricular hypertrophy is thought to be present in up to 70% of patients with type 2 diabetes and about 44% of those patients with type 2 diabetes are normotensive (normal blood pressure) patients with left ventricular hypertrophy 5. Thus normotensive left ventricular hypertrophy is very common 6. Indeed, high blood pressure contributes 25% to 70% left ventricular hypertrophy based on the population studied and the criteria used 7. Despite a “normal” blood pressure, normotensive left ventricular hypertrophy is just as risky as is hypertensive left ventricular hypertrophy 8. The lack of association between left ventricular mass and blood pressure in patients with metabolic syndrome suggests other factors such as insulin resistance and hyperinsulinemia, sodium retention, sympathetic activation, and adipose tissue peptides such as leptin may be responsible 9. https://www.ncbi.nlm.nih.gov/pubmed/17684462
Nevertheless, scientists do know that regressing left ventricular hypertrophy irrespective of blood pressure changes is an effective way to reduce the incidence of all major cardiovascular events including specifically sudden deaths, heart failure hospitalizations, new onset atrial fibrillation and strokes 10. The LIFE trial 11 provides conclusive proof that in diabetes, left ventricular hypertrophy regression per se reduces future cardiovascular events [by 24%], reduces cardiovascular deaths [by 37%] and reduces total deaths [by 41%] irrespective of blood pressure.
Treating high blood pressure and losing weight if overweight/obese can help ease your symptoms and may reverse left ventricular hypertrophy.
Can left ventricular hypertrophy be cured?
Treatment for left ventricular hypertrophy depends on the underlying cause, and may involve medication or surgery. For some people, yes. There are a number of studies pointing to improved outcomes for people who are treated for left ventricular hypertrophy. Controlling high blood pressure and using a drug that blocks the renin-angiotensin system are the standard approaches to the management of left ventricular hypertrophy and can help ease your symptoms and may reverse left ventricular hypertrophy. Data from the large Losartan Intervention for Endpoint Reduction (LIFE) study 12 indicate that angiotensin II receptor blockers (ARBs) appear to have a specific effect on left ventricular hypertrophy, independent of blood pressure reduction, and this is associated with more favorable cardiovascular outcomes. More complete blockade of the renin-angiotensin system, using a combination of renin-angiotensin system antihypertensive agents, may offer additional target organ protection.
In a meta-analysis of studies reporting echocardiographic left ventricular hypertrophy before and during antihypertension therapy, left ventricular hypertrophy regression was associated with a 59% reduction in the risk of cardiovascular events when compared with persistence or new development of left ventricular hypertrophy 13. The large Losartan Intervention for Endpoint Reduction (LIFE) study clearly demonstrated that regression of ECG-determined left ventricular hypertrophy with antihypertension treatment improved prognosis, independent of blood pressure 12. A prospective study of 436 hypertensive subjects by Muiesan et al. 14 indicates that the response of left ventricle geometry to treatment may also have prognostic significance. In this study, the persistence or development of concentric geometry was associated with an increased cardiovascular risk after adjusting for other covariates, even in those with follow-up left ventricular hypertrophy index values that were considered to be in the normal range.
Human heart
Your heart is a strong muscle about the size of the palm of your hand. Your body depends on the heart’s pumping action to deliver oxygen- and nutrient-rich blood to the body’s cells. When the cells are nourished properly, the body can function normally. Just like an engine makes a car go, the heart keeps your body running. The heart has two pumps. The stronger pump uses arteries to send blood with oxygen away from the heart, throughout the body. The other pump uses veins to bring blood back to the heart and sends it to the lungs to get more oxygen. An electrical system in the heart controls the heart’s pumps (the heart beat or pulse).
How the Heart Works
Figure 1. The anatomy of the heart
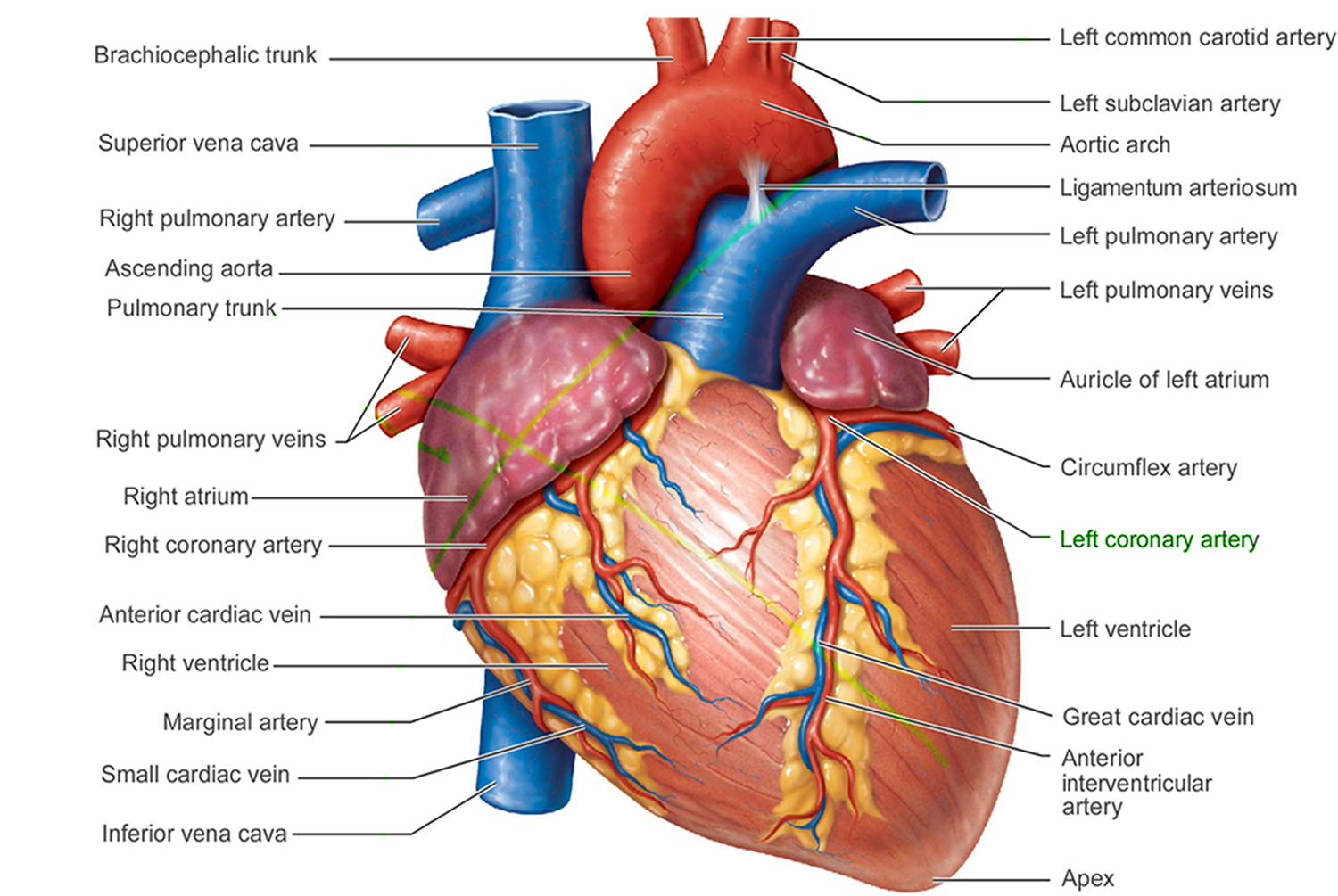
Figure 2. The anatomy of the heart chambers

Figure 3. Normal heart blood flow

The heart has two sides, separated by an inner wall called the septum. The right side of the heart pumps blood to the lungs to pick up oxygen. The left side of the heart receives the oxygen-rich blood from the lungs and pumps it to the body.
The heart has four chambers 15, two on the right and two on the left:
- Two upper chambers are called atrium (two is called an atria). The atria collect blood as it flows into the heart.
- Two lower chambers are called ventricles. The ventricles pump blood out of the heart to the lungs or other parts of the body.
The heart also has four valves that open and close to let blood flow from the atria to the ventricles and from the ventricles into the two large arteries connected to the heart in only one direction when the heart contracts (beats). The four heart valves are:
- Tricuspid valve, located between the right atrium and right ventricle
- Pulmonary or pulmonic valve, between the right ventricle and the pulmonary artery. This artery carries blood from the heart to the lungs.
- Mitral valve, between the left atrium and left ventricle
- Aortic valve, between the left ventricle and the aorta. This aorta carries blood from the heart to the body.
Each valve has a set of flaps (also called leaflets or cusps). The mitral valve has two flaps; the others have three. Valves are like doors that open and close. They open to allow blood to flow through to the next chamber or to one of the arteries. Then they shut to keep blood from flowing backward. Blood flow occurs only when there’s a difference in pressure across the valves, which causes them to open. Under normal conditions, the valves permit blood to flow in only one direction.
The heart four chambers and four valves and is connected to various blood vessels. Veins are blood vessels that carry blood from the body to the heart. Arteries are blood vessels that carry blood away from the heart to the body.
The heart pumps blood to the lungs and to all the body’s tissues by a sequence of highly organized contractions of the four chambers. For the heart to function properly, the four chambers must beat in an organized way.
When the heart’s valves open and close, they make a “lub-DUB” sound that a doctor can hear using a stethoscope 16.
- The first sound—the “lub”—is made by the mitral and tricuspid valves closing at the beginning of systole. Systole is when the ventricles contract, or squeeze, and pump blood out of the heart.
- The second sound—the “DUB”—is made by the aortic and pulmonary valves closing at the beginning of diastole. Diastole is when the ventricles relax and fill with blood pumped into them by the atria.
Figure 4. Left ventricular hypertrophy
Left ventricular hypertrophy ECG
The ECG criteria for diagnosing right or left ventricular hypertrophy are very insensitive (i.e., sensitivity ~50%, which means that ~50% of patients with ventricular hypertrophy cannot be recognized by ECG criteria). However, the criteria are very specific (i.e., specificity >90%, which means if the criteria are met, it is very likely that ventricular hypertrophy is present).
General left ventricular hypertrophy ECG features include:
- ≥ QRS amplitude (voltage criteria; i.e., tall R-waves in LV leads, deep S-waves in RV leads)
- Delayed intrinsicoid deflection in V6 (i.e., time from QRS onset to peak R is ≥ 0.05 sec)
- Widened QRS/T angle (i.e., left ventricular strain pattern, or ST-T oriented opposite to QRS direction)
- Leftward shift in frontal plane QRS axis
- Evidence for left atrial enlargement
Figure 5. Left ventricular hypertrophy ECG
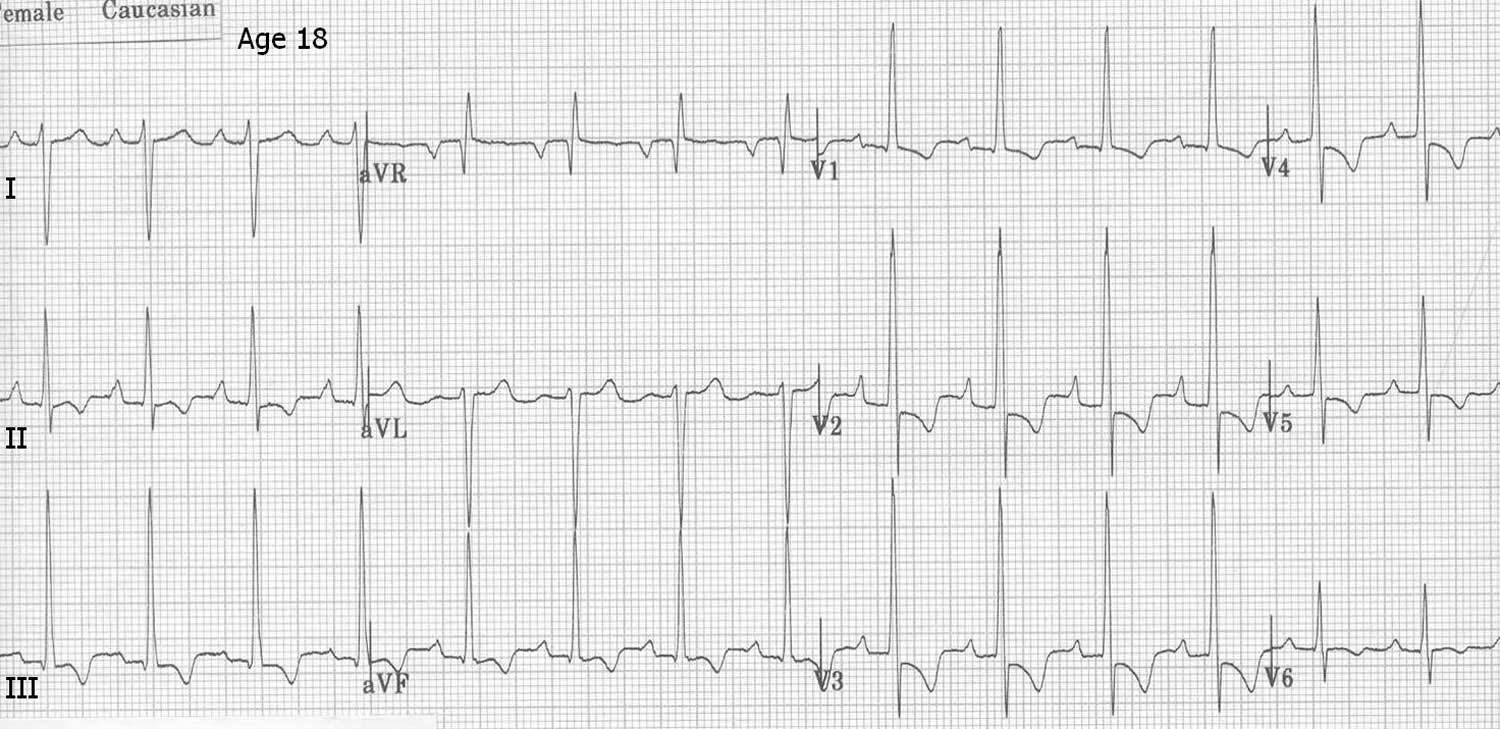
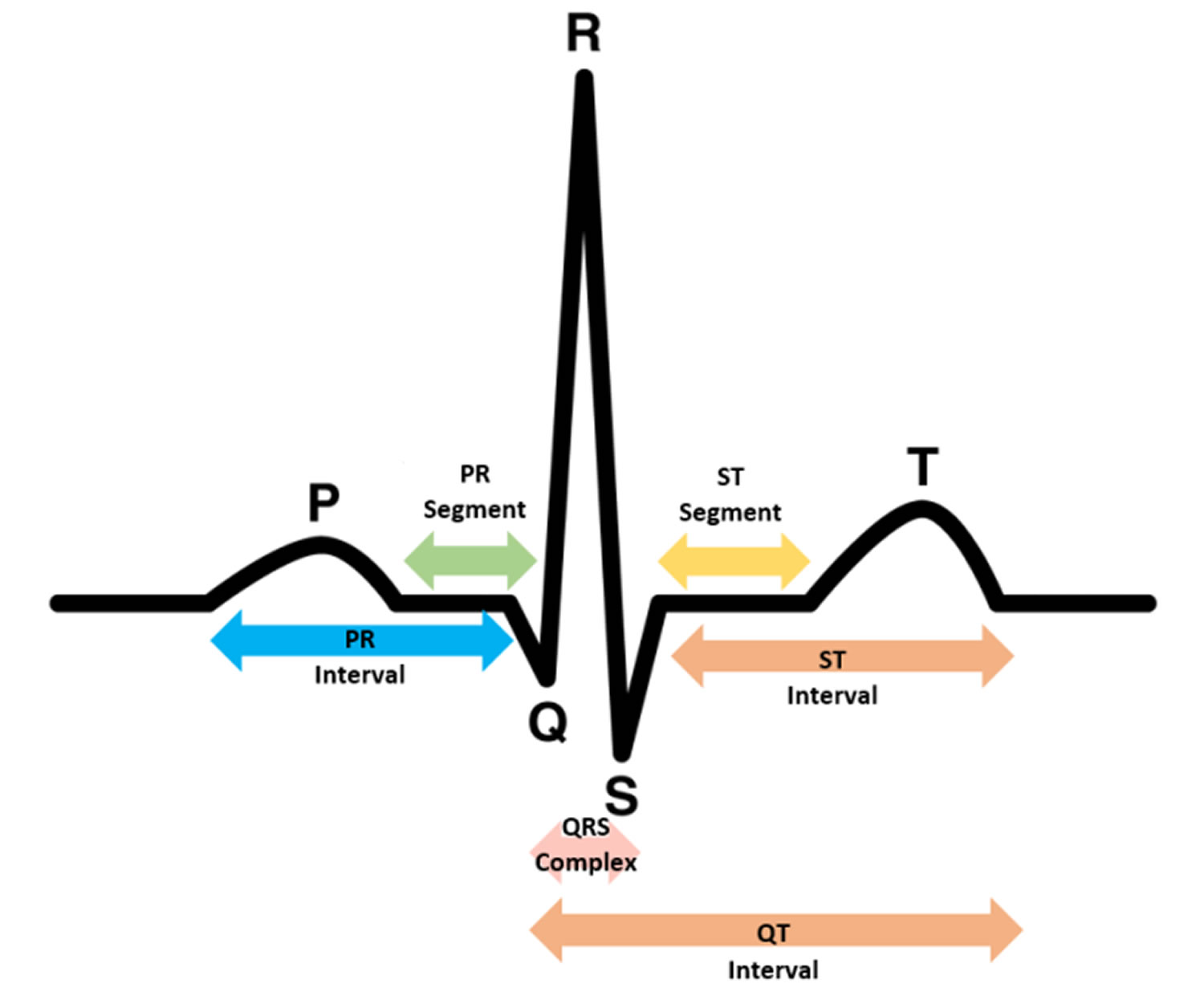
Figure 6. ECG pattern
Left ventricular hypertrophy prognosis
Left ventricular hypertrophy is the heart’s adaptive response to a chronically increased workload, with systemic hypertension being a common cause. It is a recognized intermediate marker of hypertension-related target organ damage, and a strong predictor of congestive heart failure, coronary heart disease, and stroke 17. Left ventricular hypertrophy is, to a great extent, a reversible risk factor; its regression in response to antihypertensive treatment significantly improves the cardiovascular outcome and long-term prognosis.
Left ventricular hypertrophy complications
Left ventricular hypertrophy changes the structure and working of the heart. The enlarged left ventricle can:
- Weaken
- Stiffen and lose elasticity, preventing the chamber from filling properly and increasing pressure in the heart
- Compress the chamber’s blood vessels (coronary arteries) and restrict its supply of blood
As a result of these changes, complications of left ventricular hypertrophy include:
- Interruption of blood supply to the heart
- Inability of the heart to pump enough blood to your body (heart failure)
- Abnormal heart rhythm (arrhythmia)
- Irregular, often rapid heartbeat (atrial fibrillation) that decreases blood flow to the body
- Insufficient supply of oxygen to the heart (ischemic heart disease)
- Enlargement of a section of the aorta (aortic root dilation)
- Stroke
- Sudden, unexpected loss of heart function, breathing and consciousness (sudden cardiac arrest).
Left ventricular hypertrophy causes
Left ventricular hypertrophy can occur when some factor makes your heart work harder than normal to pump blood to your body.
Factors that can cause your heart to work harder include:
- High blood pressure (hypertension). This is the most common cause of left ventricular hypertrophy. More than one-third of people show evidence of left ventricular hypertrophy at the time of their diagnosis with hypertension.
- Diabetes
- Heart valve problems like stenosis or regurgitation.
- Aortic valve stenosis. This disease is a narrowing of the tissue flap (aortic valve) that separates the left ventricle from the large blood vessel leaving your heart (aorta). The narrowing of the aortic valve requires the left ventricle to work harder to pump blood into the aorta.
- Arrhythmia
- Atrial fibrillation (AF)
- Enlargement of the aorta
- Hypertrophic cardiomyopathy. This genetic disease occurs when the heart muscle becomes abnormally thick, making it harder for the heart to pump blood.
- Athletic training. Intense, prolonged endurance and strength training can cause the heart to adapt to handle the extra workload. It’s unclear whether this athletic type of left ventricle hypertrophy can lead to stiffening of the heart muscle and disease.
Factors promoting left ventricular hypertrophy 18:
- Hypertension
- Neurohumoral factors (growth stimulation)
- Angiotensin II
- Aldosterone
- Norepinephrine
- Insulin and other growth factors
- Genetic influences
It is now appreciated that left ventricular hypertrophy is mediated not only by the mechanical stress of pressure overload, but also by various neurohormonal substances that independently exert trophic effects on myocytes and nonmyocytes in the heart 19. As shown in the list of factors promoting left ventricular hypertrophy above, trophic factors include angiotensin II, aldosterone, norepinephrine, and insulin which directly promote myocyte hypertrophy and matrix deposition independent of their effects on systemic arterial pressure 20. These trophins stimulate the production of a series of cytokines and growth factors including transforming growth factor beta, fibroblast growth factor, and insulin growth factor that directly stimulate cardiac protein synthesis and hypertrophy. While elevated systemic arterial pressure plays a role in the pathogenesis of left ventricular hypertrophy, the extent of cardiac growth and response to increased pressure loading is not uniform among patients suggesting genetic mechanisms in cardiac hypertrophy 21. Thus, patients with moderate arterial hypertension present with a wide range of left ventricular mass, ranging from normal heart to severe hypertrophy. In addition, the remodeling of the left ventricle may take a concentric or an eccentric form independent of the extent of blood pressure elevation.
It is important to treat the causes of left ventricular hypertrophy early because it can lead to severe problems like heart failure, sudden cardiac arrest and ischemic stroke.
Risk factors for left ventricular hypertrophy
In addition to hypertension and aortic valve stenosis, factors that increase your risk for left ventricular hypertrophy include:
- Age. Left ventricular hypertrophy is more common in older people.
- Being overweight / obesity increases your risk of high blood pressure and left ventricular hypertrophy.
- Family history. Certain genetic conditions are associated with developing hypertrophy.
- Diabetes.
- Race. African-Americans are at higher risk of left ventricular hypertrophy than are white people with similar blood pressure measurements.
- Sex. Women with hypertension are at higher risk of left ventricular hypertrophy than are men with similar blood pressure measurements.
Left ventricular hypertrophy prevention
The best way to prevent left ventricular hypertrophy is to maintain healthy blood pressure. To better manage your blood pressure:
- Monitor high blood pressure. Purchase a home blood pressure measuring device and check your blood pressure frequently. Schedule regular checkups with your doctor.
- Make time for exercise. Regular exercise helps to lower blood pressure and keep it at normal levels. Aim for 30 minutes of moderate activity most days of the week.
- Watch your diet. Avoid foods that are high in fat and salt, and eat more fruits and vegetables. Avoid alcoholic beverages or drink them in moderation.
- Quit smoking. Giving up smoking improves your blood pressure and overall health.
Left ventricular hypertrophy symptoms
Left ventricular hypertrophy may be present gradually for many years without any noticeable symptoms at all. As the condition worsens, symptoms may develop, such as:
- Shortness of breath
- Fatigue
- Chest pain (especially with exercise)
- Sensation of rapid, fluttering or pounding heartbeats (palpitations)
- Dizziness or fainting
If you are experiencing some or all of these symptoms, speak to your doctor right away. This cluster of symptoms can have several causes and should always be discussed with your healthcare provider so that prompt attention can be given to identify the reasons.
If you have high blood pressure or another condition that increases your risk of left ventricular hypertrophy, your doctor is likely to recommend regular appointments to monitor your heart. Even if you feel well, you need to have your blood pressure checked annually, or more often if you:
- Smoke
- Are overweight
- Have other conditions that increase the risk of high blood pressure
Left ventricular hypertrophy diagnosis
Your doctor will start with a health history, family history and thorough physical examination including checking your blood pressure and heart function.
Your doctor might then recommend screening tests:
- Electrocardiogram (ECG or EKG). Electrical signals are recorded as they travel through your heart. Your doctor can look for patterns that indicate abnormal heart function and increased left ventricle muscle tissue.
- Echocardiogram. Sound waves produce live-action images of your heart. Echocardiogram can reveal thickened muscle tissue in the left ventricle, blood flow through the heart with each beat, and heart abnormalities related to left ventricular hypertrophy, such as aortic valve stenosis.
- MRI. Images of your heart can be used to diagnose left ventricular hypertrophy.
Left ventricular hypertrophy treatment
Left ventricular hypertrophy can often be corrected by treating the underlying problem causing the heart to work too hard. Depending on the type of damage that has occurred, treatment measures may include medications and heart-healthy lifestyle changes to help reduce the load on the heart. If left ventricular hypertrophy is caused by a heart valve problem, surgery may be needed to repair the valve.
Treating high blood pressure
Your doctor is likely to recommend lifestyle changes, including:
- Regular exercise
- Low-sodium, low-fat diet
- Smoking cessation
Blood pressure medication might also help prevent further enlargement of the left ventricle and even shrink your hypertrophic muscles. Your doctor might recommend:
- Angiotensin-converting enzyme (ACE) inhibitors. These medications widen blood vessels to lower blood pressure, improve blood flow and decrease the heart’s workload. Examples include Captopril, Enalapril and Lisinopril. Side effects might include an irritating dry cough.
- Angiotensin II receptor blockers (ARBs). Medications such as losartan (Cozaar) have benefits similar to ACE inhibitors but don’t cause a persistent cough.
- Beta blockers. Medications such as atenolol (Tenormin) can lower your heart rate, reduce blood pressure and prevent some of the harmful effects of stress hormones. Beta blockers aren’t usually given as an initial treatment for hypertension. Your doctor might recommend adding a beta blocker if another type of medication isn’t effective alone.
- Calcium channel blockers. These medications prevent calcium from entering cells of the heart and blood vessel walls, resulting in lower blood pressure. Examples include amlodipine (Norvasc) and diltiazem (Cardizem).
- Diuretics. Medications known as thiazide-type diuretics can facilitate blood flow, lowering hypertension. Examples include chlorthalidone and hydrochlorothiazide.
Treating sleep apnea
If you’ve already been diagnosed with sleep apnea, treating this sleep disorder can lower your blood pressure and help reverse left ventricular hypertrophy.
If you haven’t been diagnosed with sleep apnea, but your partner tells you that you snore or that you stop breathing momentarily while you sleep, talk with your doctor about getting tested for sleep apnea.
Sleep apnea treatment involves using a machine that provides continuous positive airway pressure (CPAP) while you sleep. CPAP keeps your airways open, allowing you to get the oxygen you need to keep your blood pressure at a normal level.
Aortic valve repair or replacement
Left ventricular hypertrophy that is caused by aortic valve stenosis might require surgery to repair the narrow valve or to replace it with an artificial or tissue valve.
Home remedies
Lifestyle changes can help lower your blood pressure and improve left ventricular hypertrophy signs. Consider:
- Weight loss. Left ventricular hypertrophy is often found in obese people regardless of blood pressure. Losing weight has been shown to reverse left ventricular hypertrophy.
- Limiting salt in your diet. Too much salt can increase your blood pressure. Choose low sodium or no-salt-added foods, and don’t add salt to your meals.
- Drinking alcohol in moderation, if at all. Alcohol can also raise your blood pressure, especially if consumed in large amounts.
- Regular exercise. Aim for at least 30 minutes of physical activity, such as walking, most days of the week. Ask your doctor if you need to restrict certain physical activities, such as weightlifting, which may temporarily raise your blood pressure.
- Liao Y, Cooper RS, McGee DL, Mensah GA, Ghali JK. The relative effects of left ventricular hypertrophy, coronary artery disease, and ventricular dysfunction on survival among black adults. JAMA. 1995;273(20):1592–1597. doi: 10.1001/jama.1995.03520440046035. https://www.ncbi.nlm.nih.gov/pubmed/7745772[↩]
- Artham SM, Lavie CJ, Milani RV, Patel DA, Verma A, Ventura HO. Clinical impact of left ventricular hypertrophy and implications for regression. Prog Cardiovasc Dis. 2009;52(2):153–167. doi: 10.1016/j.pcad.2009.05.002. https://www.ncbi.nlm.nih.gov/pubmed/19732607[↩]
- Mathew J, Sleight P, Lonn E, Johnstone D, Pogue J, Yi Q, Bosch J, Sussex B, Probstfield J, Yusuf S; Heart Outcomes Prevention Evaluation (HOPE) Investigators . Reduction of cardiovascular risk by regression of electrocardiographic markers of left ventricular hypertrophy by the angiotensin‐converting enzyme inhibitor ramipril. Circulation. 2001;104:1615–1621. http://circ.ahajournals.org/content/104/14/1615.long[↩]
- Verdecchia P, Schillaci G, Borgioni C, Ciucci A, Gattobigio R, Zampi I, Reboldi G, Porcellati C. Prognostic significance of serial changes in left ventricular mass in essential hypertension. Circulation. 1998;97:48–54. http://circ.ahajournals.org/content/97/1/48.long[↩]
- Dawson A, Morris AD, Struthers AD. The epidemiology of left ventricular hypertrophy in type 2 diabetes mellitus. Diabetologia. 2005;48(10):1971–1979. doi: 10.1007/s00125-005-1896-y. https://www.ncbi.nlm.nih.gov/pubmed/16094529[↩]
- Mancia G, Carugo S, Grassi G, Lanzarotti A, Schiavina R, Cesana G, et al. Prevalence of left ventricular hypertrophy in hypertensive patients without and with blood pressure control: data from the PAMELA population. Pressioni Arteriose Monitorate E Loro Associazioni. Hypertension. 2002;39(3):744–749. doi: 10.1161/hy0302.104669. http://hyper.ahajournals.org/content/39/3/744.long[↩]
- Left ventricular hypertrophy and clinical outcomes in hypertensive patients. Ruilope LM, Schmieder RE. Am J Hypertens. 2008 May; 21(5):500-8. https://www.ncbi.nlm.nih.gov/pubmed/18437140/[↩]
- Brown DW, Giles WH, Croft JB. Left ventricular hypertrophy as a predictor of coronary heart disease mortality and the effect of hypertension. Am Heart J. 2000;140(6):848–856. doi: 10.1067/mhj.2000.111112. https://www.ncbi.nlm.nih.gov/pubmed/11099987[↩]
- Mulé G, Nardi E, Cottone S, et al. Impact of the metabolic syndrome on total arterial compliance in essential hypertension patients. Journal of the Cardiometabolic Syndrome. 2007;2(2):84–90.[↩]
- Wachtell K, Okin PM, Olsen MH, Dahlof B, Devereux RB, Ibsen H, et al. Regression of electrocardiographic left ventricular hypertrophy during antihypertensive therapy and reduction in sudden cardiac death: the LIFE study. Circulation. 2007;116(7):700–705. doi: 10.1161/CIRCULATIONAHA.106.666594. http://circ.ahajournals.org/content/116/7/700.long[↩]
- Lindholm LH, Ibsen H, Dahlof B, Devereux RB, Beevers G, de Faire U, et al. Cardiovascular morbidity and mortality in patients with diabetes in the Losartan intervention for endpoint reduction in hypertension study [LIFE]: a randomised trial against atenolol. Lancet [London, England] 2002;359(9311):1004–1010. doi: 10.1016/S0140-6736(02)08090-X. https://www.ncbi.nlm.nih.gov/pubmed/11937179[↩]
- Okin PM, Devereux RB, Jern S, Kjeldsen SE, Julius S, Nieminen MS, Snapinn S, Harris KE, Aurup P, Edelman JM, Dahlof B; LIFE Study Investigators. Regression of electrocardiographic left ventricular hypertrophy during antihypertensive treatment and the prediction of major cardiovascular events. JAMA 2004;292:2343–2349. https://jamanetwork.com/journals/jama/fullarticle/199807[↩][↩]
- Verdecchia P, Angeli F, Borgioni C, Gattobigio R, de Simone G, Devereux RB, Porcellati C: Changes in cardiovascular risk by reduction of left ventricular mass in hypertension: a meta-analysis. Am J Hypertens 2003;16:895–859. https://www.ncbi.nlm.nih.gov/pubmed/14573325[↩]
- Muiesan ML, Salvetti M, Monteduro C, Bonzi B, Paini A, Viola S, Poisa P, Rizzoni D, Castellano M, Agabitei-Rosei E: Left ventricular concentric geometry during treatment adversely affects cardiovascular prognosis in hypertensive patients. Hypertension 2004;43:731–738. http://hyper.ahajournals.org/content/43/4/731.long[↩]
- American Heart Association. About Arrhythmia. http://www.heart.org/HEARTORG/Conditions/Arrhythmia/AboutArrhythmia/About-Arrhythmia_UCM_002010_Article.jsp[↩]
- Centers for Disease Control and Prevention. Division of Birth Defects and Developmental Disabilities. Congenital Heart Defects (CHDs). https://www.cdc.gov/ncbddd/heartdefects/index.html[↩]
- ESH/ESC Task Force. 2007 Guidelines for the Management of Arterial Hypertension. European Heart Journal Advance Access published on June 14, 2007.[↩]
- Katholi RE, Couri DM. Left Ventricular Hypertrophy: Major Risk Factor in Patients with Hypertension: Update and Practical Clinical Applications. International Journal of Hypertension. 2011;2011:495349. doi:10.4061/2011/495349. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3132610/[↩]
- Post WS, Larson MG, Levy D. Impact of left ventricular structure on the incidence of hypertension: the Framingham Heart Study. Circulation. 1994;90(1):179–185. https://www.ncbi.nlm.nih.gov/pubmed/8025994[↩]
- Johnson DB, Dell’Italia LJ. Cardiac hypertrophy and failure in hypertension. Current Opinion in Nephrology and Hypertension. 1996;5(2):186–191. https://www.ncbi.nlm.nih.gov/pubmed/8744544[↩]
- Simpson TE, Dansky HM, Buttrick PM. Molecular genetic mechanisms of cardiac hypertrophy. Cardiovascular Risk Factors. 1995;5(2):93–108.[↩]





{kind=link}