Contents
What are liver enzymes
Your liver is the largest organ inside your body. You cannot live without your liver.
The liver has several important functions:
- Picks up glucose from nutrient-rich blood returning from the alimentary canal and stores this carbohydrate as glycogen for subsequent use by the body.
- Processes fats and amino acids and stores certain vitamins.
- Detoxifies many poisons and drugs in the blood.
- Makes the blood proteins.
- It breaks down and stores many of the nutrients absorbed from the intestine that your body needs to function. Some nutrients must be changed (metabolized) in the liver before they can be used for energy or to build and repair body tissues.
- It makes most of the clotting factors that keep you from bleeding too much when you are cut or injured.
- It secretes bile into the intestines to help absorb nutrients (especially fats).
- It breaks down alcohol, drugs, and toxic wastes in the blood, which then pass from the body through urine and stool.
Almost all of these functions are carried out by a type of cell called a hepatocyte or simply a liver cell.
Amazingly versatile, your liver performs over 500 functions. Its digestive function is to produce bile, a green alkaline liquid that is stored in the gallbladder and secreted into the duodenum. Bile salts emulsify fats in the small intestine; that is, they break up fatty nutrients into tiny particles, just as dish detergent breaks up a pool of fat drippings in a roasting pan. These smaller particles are more accessible to digestive enzymes from the pancreas.
The liver carries on many important metabolic activities. The liver plays a key role in carbohydrate metabolism by helping maintain concentration of blood glucose within the normal range. Liver cells responding to the hormone insulin lower the blood glucose level by polymerizing glucose to glycogen. Liver cells responding to the hormone glucagon raise the blood glucose level by breaking down glycogen to glucose or by converting noncarbohydrates into glucose.
The liver’s effects on lipid metabolism include oxidizing (breaking down) fatty acids at an especially high rate; synthesizing lipoproteins, phospholipids, and cholesterol; and converting excess portions of carbohydrate molecules into fat molecules. The blood transports fats synthesized in the liver to adipose tissue for storage.
Other liver functions concern protein metabolism. They include deaminating amino acids; forming urea; synthesizing plasma proteins such as clotting factors; and converting certain amino acids into other amino acids.
The liver also stores many substances, including glycogen, iron, and vitamins A, D, and B12. In addition, macrophages in the liver help destroy damaged red blood cells and phagocytize foreign antigens. The liver also removes toxic substances such as alcohol and certain drugs from blood (detoxification).
A liver function important to digestion is bile secretion. Table 1 summarizes the major functions of the liver.
Table 1. Major Functions of the Liver
General Function | Specific Function |
| Carbohydrate metabolism | Polymerizes glucose to glycogen; breaks down glycogen to glucose; converts noncarbohydrates to glucose |
| Lipid metabolism | Oxidizes fatty acids; synthesizes lipoproteins, phospholipids, and cholesterol; converts excess portions of carbohydrate molecules into fats |
| Protein metabolism | Deaminates amino acids; forms urea; synthesizes plasma proteins; converts certain amino acids into other amino acids |
| Storage | Stores glycogen, iron, and vitamin A, vitamin D and vitamin B12 |
| Blood filtering | Removes damaged red blood cells and foreign substances by phagocytosis |
| Detoxification | Removes toxins from blood |
| Secretion | Produces and secretes bile |
Many of these biosynthetic functions use the products of digestion. With the exception of most lipids, absorbed food products pass directly from the gut to the liver through the hepatic portal vein.
Figure 1. Location of the human liver
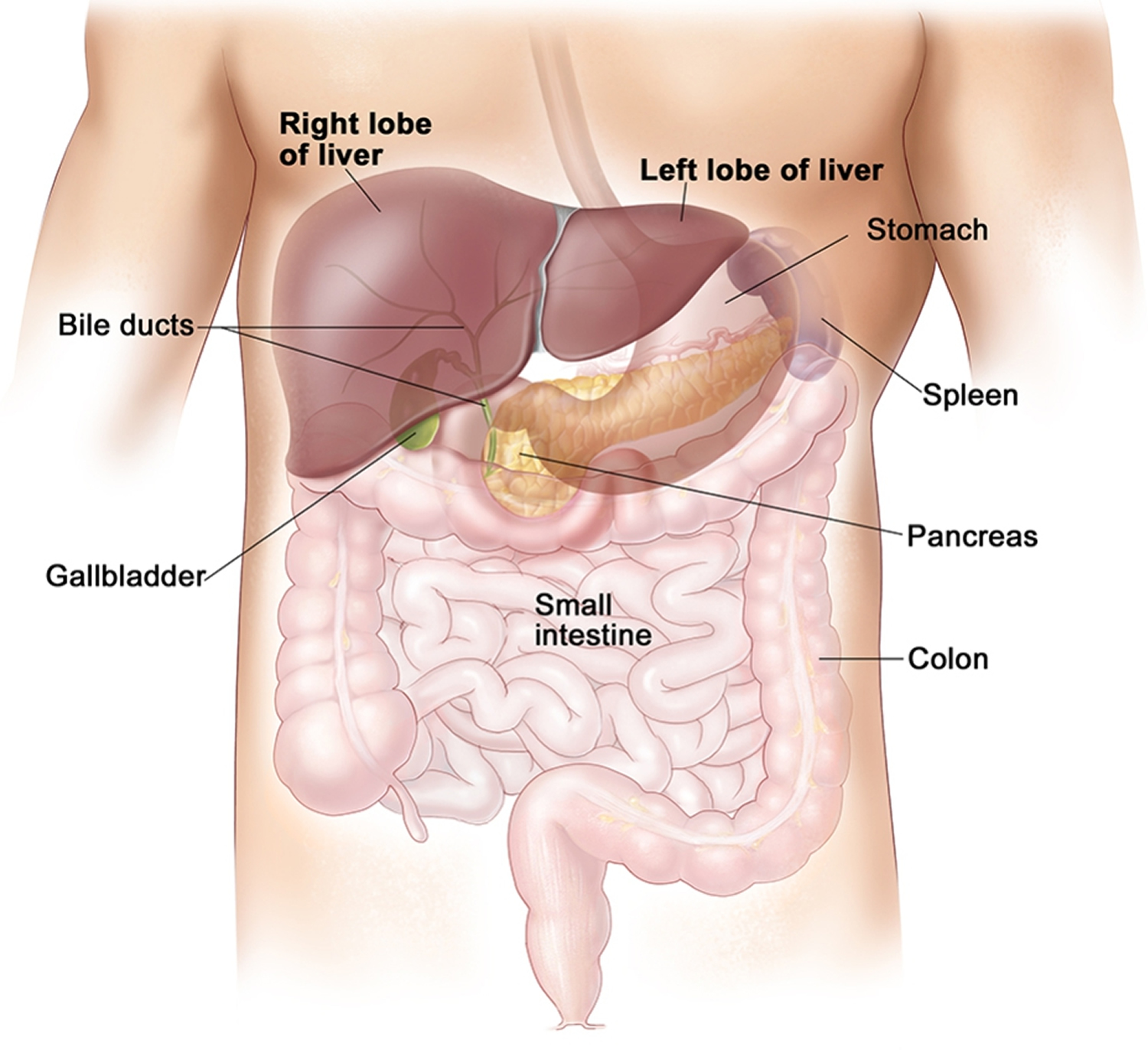
Figure 2. Liver anatomy
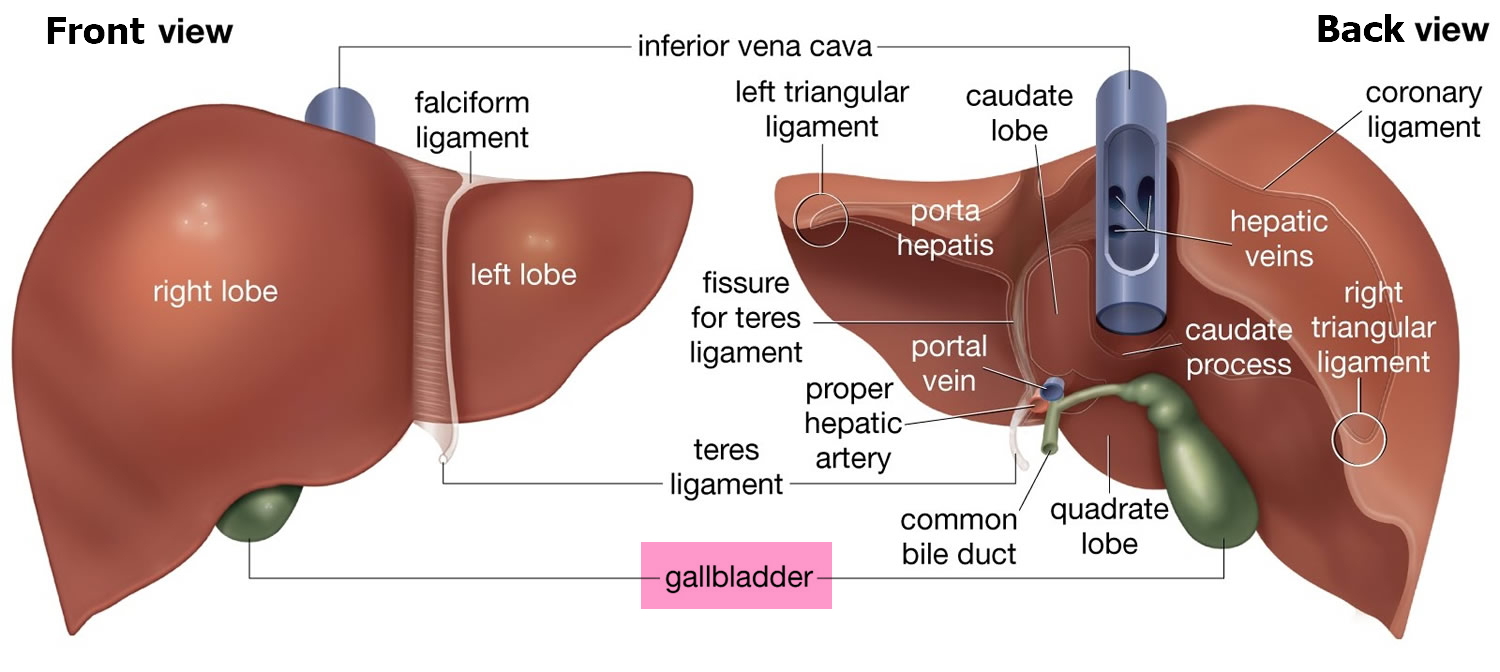
Figure 3. Liver lobule
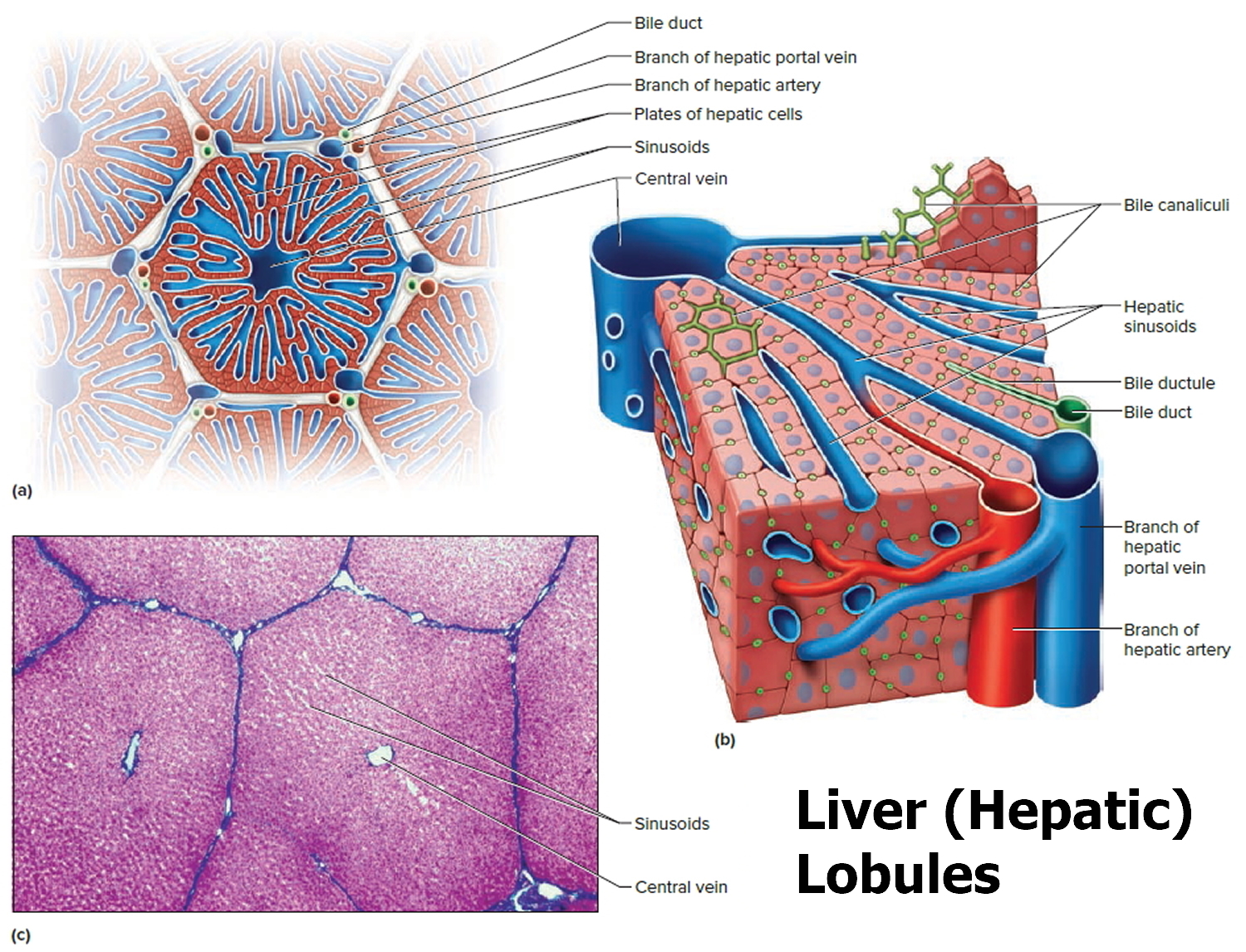
Note: (a) Cross section of a hepatic lobule. (b) Enlarged longitudinal section of a hepatic lobule. (c) Light micrograph of hepatic lobules in cross section.
Your doctor will order liver enzymes and a function test to screen for, detect, evaluate, and monitor acute and chronic liver inflammation (hepatitis), liver infection, liver disease and/or and damage.
Liver function test (LFT) measures the concentrations of various different proteins and enzymes in the blood that are either produced by liver cells or released when liver cells are damaged. Liver function tests are very common investigations carried out in people with suspected liver disease. Specific patterns of results can tell your doctor the likely type of liver disease so they can decide whether any further tests are required. Liver function tests can also help tell how severely the liver is damaged and help monitor your response to drugs and other treatments.
Your doctor will periodically to evaluate your liver function; whenever you are at risk for liver injury; when you are taking medications that may affect your liver; when you have a liver disease; when you have symptoms associated with liver damage, such as jaundice.
Alanine Aminotransferase (ALT) also called SGPT (Serum Glutamic-Pyruvic Transaminase) or GPT (Glutamic-Pyruvic Transaminase): ALT (Alanine Transaminase) is an enzyme produced in hepatocytes (the major type of liver cells). ALT level in the blood is increased when hepatocytes are damaged or die — all types of hepatitis (viral, alcoholic, drug-induced etc) cause hepatocyte damage. Levels of ALT may equate to the degree of cell damage but this is not always the case, particularly with hepatitis C. An accurate estimate of liver cell damage can only be made by liver biopsy. Reference values for ALT are less than 36U/L.
Aspartate Amino Transferase (AST) also called SGOT (Serum Glutamic-Oxaloacetic Transaminase) or GOT (Glutamic-Oxaloacetic Transaminase): AST (Aspartate Transaminase) is similar to ALT above, but less specific for liver disease because it is also produced in body muscle cells. It does tend to be higher than ALT in cases of alcohol-related liver disease.Reference values for AST are less than 42U/L.
Alkaline Phosphatase (ALP): This enzyme is mainly implicated in the diagnosis of biliary obstruction and is normally found in small bile tracts in the liver. There are many different types of this enzyme found in the body in the liver, bone and placenta so elevated levels may be due to a problem outside the liver such as a malignancy (cancer). A normal ALP is between 35-50 g/L.
Gamma Glutamyl Transpeptidase (GGT): GGT enzyme is found in certain liver cells and bile duct cells. It is also elevated in diseases that decrease or obstruct the flow of bile. Alcohol abuse, warfarin (a blood-thinner) and drugs used for epilepsy can increase GGT levels. GGT has been used to detect chronic alcohol abuse but it is increased in a range of conditions so it is not always correct. GGT should be less than 60U/L in a normal individual.
Doctors often request these liver function tests for people who:
- have liver disease or damage
- are, or might be, infected with hepatitis viruses
- are heavy drinkers
- have a family history of liver disease
- take drugs that can damage the liver.
Your doctor might order liver function tests if you have:
- jaundice
- dark urine
- weakness or tiredness
- loss of appetite
- nausea and vomiting
- abdominal pain or swelling
- itching.
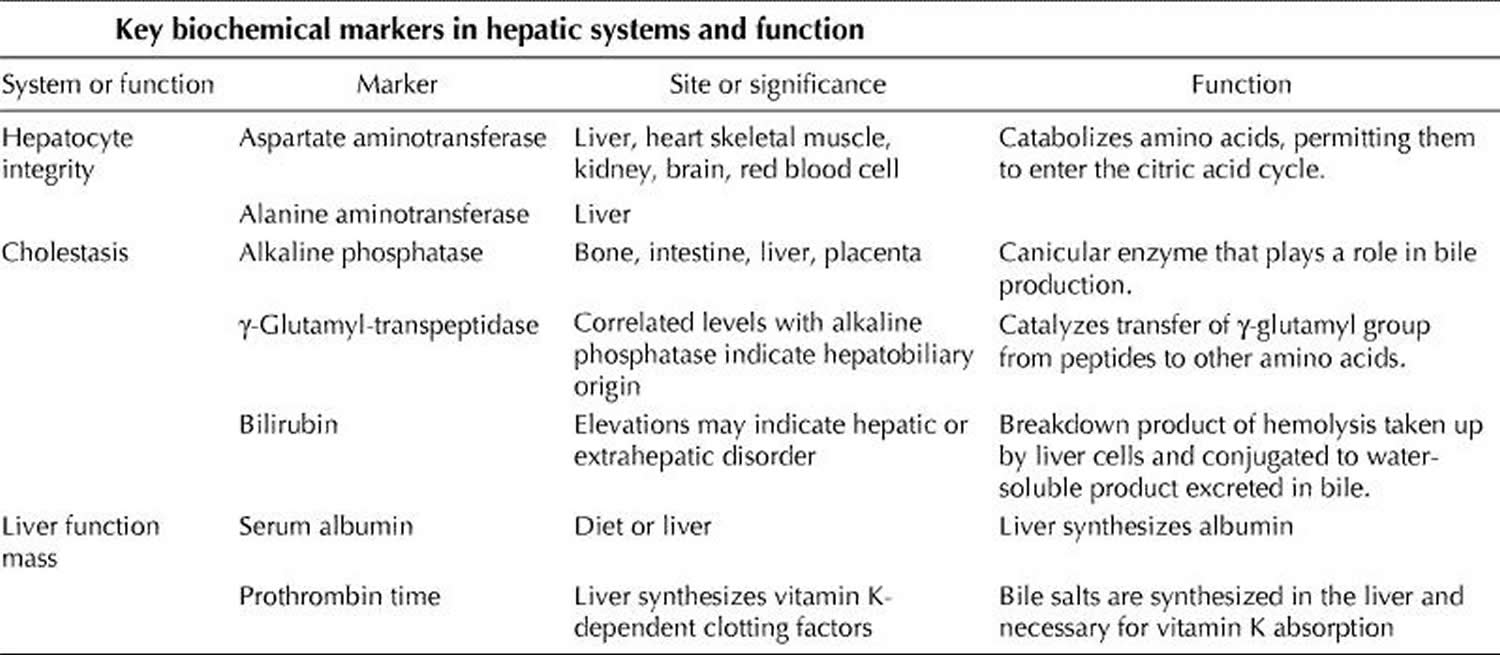
Liver disease is often reflected by biochemical abnormalities of 1 of 2 different hepatic systems or of liver function (Table 2). Although tests that measure the level of serum liver enzymes are commonly referred to as liver function tests, they usually reflect hepatocyte integrity or cholestasis rather than liver function 1. A change in serum albumin level or prothrombin time may be associated with a decrease in liver functioning mass, although neither is specific for liver disease 1.
An abnormal level is usually defined as a value exceeding the upper reference limit, since there is no clinical significance to the occurrence of low levels of biochemical markers, except for serum albumin 1. Because the reference limits for each test often vary among laboratories, specific ranges will not be provided here, in order to avoid generating confusion.
Table 2. Key liver enzymes
It is common practice when establishing laboratory parameters to define the “normal” range as the mean value within ± 2 standard deviations observed in the reference, “normal” population. Accordingly, as many as 2.5% of normal patients have “abnormal” aminotransferase levels. Moreover, at least 16% of patients with chronic hepatitis C infection and 13% of patients with nonalcoholic fatty liver disease have varying degrees of histological damage despite showing persistently normal aminotransferase levels 2, 3. This apparent discrepancy may be explained by the fact that the healthy population that was recruited to establish the normal range could have included a small subset of patients with subclinical liver disease.
As well, aminotransferase levels vary according to age and sex, so care must be taken to use age- and sex-appropriate reference limits 4. The clinical context of patient presentation is also important when interpreting reference limits. Levels of both aspartate aminotransferase (AST) and alanine aminotransferase (ALT) may increase with strenuous exercise 5, 6, and hospital admission has been observed to induce a 5% increase in AST levels and a 17.5% increase in ALT levels in healthy subjects 7; restricted physical activity and hospital diet have been suggested as possible explanations for these increases 1.
Liver enzymes
Alanine Aminotransferase (ALT) or SGPT
Alanine aminotransferase (ALT) also called SGPT (Serum Glutamic-Pyruvic Transaminase) or GPT (Glutamic-Pyruvic Transaminase), is an enzyme found mostly in the cells of the liver and kidney. Much smaller amounts of it are also found in the heart and muscles. This test measures the level of ALT in the blood.
The function of ALT is to convert alanine, an amino acid found in proteins, into pyruvate, an important intermediate in cellular energy production. In healthy individuals, ALT levels in the blood are low. When the liver is damaged, ALT is released into the blood, usually before more obvious signs of liver damage occur, such as jaundice. This makes ALT a useful test for early detection of liver damage.
The liver is a vital organ located in the upper right-hand side of the abdominal area, just beneath the rib cage. It is involved in many important functions in the body. The liver helps to process the body’s nutrients, manufactures bile to help digest fats, produces many important proteins such as blood clotting factors and albumin, and breaks down potentially toxic substances into harmless ones that the body can use or eliminate.
A number of conditions can cause damage to liver cells, resulting in an increase in ALT. The test is most useful in detecting damage due to hepatitis or as a result of drugs or other substances that are toxic to the liver.
ALT is commonly tested in conjunction with aspartate aminotransferase (AST), another liver enzyme, as part of a liver panel. Both ALT and AST levels usually rise whenever the liver is being damaged, although ALT is more specific for the liver and, in some cases, may be the only one of the two to be increased. An AST/ALT ratio may be calculated to aid in distinguishing between different causes and severity of liver injury and to help distinguish liver injury from damage to heart or muscles.
When is ALT (alanine aminotransferase) ordered?
ALT may be ordered as part of a comprehensive metabolic panel when a person has a routine health examination.
A healthcare practitioner usually orders an ALT test (and several others) to evaluate a person who has signs and symptoms of a liver disorder. Some of these signs and symptoms may include:
- Weakness, fatigue
- Loss of appetite
- Nausea, vomiting
- Abdominal swelling and/or pain
- Jaundice
- Dark urine, light-colored stool
- Itching (pruritus)
ALT may also be ordered, either by itself or with other tests, for people who are at an increased risk for liver disease since many people with mild liver damage will have no signs or symptoms. Even without other symptoms, ALT will be increased with mild liver damage. Some examples include:
- Persons who have a history of known or possible exposure to hepatitis viruses
- Those who are heavy drinkers
- Individuals whose families have a history of liver disease
- Persons who take drugs that might damage the liver
- Persons who are overweight and/or have diabetes
A shot or injection of medicine into the muscle tissue, or strenuous exercise, may increase ALT levels.
Many drugs may raise ALT levels by causing liver damage in a very small percentage of patients taking the drug. This is true of both prescription drugs and some “natural” health products. Be sure to tell your healthcare provider about all of the drugs and/or health supplements you are taking.
When ALT is used to monitor the treatment of people who have liver disease, it may be ordered on a regular basis during the course of treatment to determine whether the therapy is effective.
How is ALT (alanine aminotransferase) used?
The alanine aminotransferase (ALT) test is typically used to detect liver injury. It is often ordered in conjunction with aspartate aminotransferase (AST) as part of a liver panel or comprehensive metabolic panel to screen for and/or help diagnose liver disease.
ALT is an enzyme found mostly in the cells of the liver and kidney. When the liver is damaged, ALT is released into the blood. This makes ALT a useful test for early detection of liver damage.
AST and ALT are considered to be two of the most important tests to detect liver injury, although ALT is more specific to the liver than is AST. Sometimes AST is compared directly to ALT and an AST/ALT ratio is calculated. This ratio may be used to distinguish between different causes of liver damage and to help recognize heart or muscle injury.
ALT values are often compared to the results of other tests such as alkaline phosphatase (ALP), total protein, and bilirubin to help determine which form of liver disease is present.
ALT is often used to monitor the treatment of persons who have liver disease, to see if the treatment is working, and may be ordered either by itself or along with other tests for this purpose.
What does abnormal ALT test result mean?
A low level of ALT in the blood is normal. Liver disease is the most common reason for higher than normal levels of ALT.
Very high levels of ALT (more than 10 times normal) are usually due to acute hepatitis, sometimes due to a viral infection. In acute hepatitis, ALT levels usually stay high for about 1-2 months but can take as long as 3-6 months to return to normal. Levels of ALT may also be markedly elevated (sometimes over 100 times normal) as a result of exposure to drugs or other substances that are toxic to the liver or in conditions that cause decreased blood flow (ischemia) to the liver.
ALT levels are usually not as high in chronic hepatitis, often less than 4 times normal. In this case, ALT levels often vary between normal and slightly increased, so the test may be ordered frequently to see if there is a pattern. Other causes of moderate increases in ALT include obstruction of bile ducts, cirrhosis (usually the result of chronic hepatitis or bile duct obstruction), heart damage, alcohol abuse, and with tumors in the liver.
ALT is often performed together with a test for AST or as part of a liver panel. For more about ALT results in relation to other liver tests, see the Liver Panel article.
In most types of liver diseases, the ALT level is higher than AST and the AST/ALT ratio will be low (less than 1). There are a few exceptions; the AST/ALT ratio is usually greater than 1 in alcoholic hepatitis, cirrhosis, and with heart or muscle injury and may be greater than 1 for a day or two after onset of acute hepatitis.
What conditions other than liver problems can cause increased ALT?
ALT is more specific for the liver than AST and so is much less affected by conditions affecting other parts of the body. Nevertheless, injury to organs other than the liver, such as the heart and skeletal muscle, can cause elevations of ALT. For example, small increases may be seen with skeletal muscle damage or heart attacks.
What other tests may be performed to help determine the cause of liver damage?
After a thorough physical exam and evaluation of a person’s medical history, there are several other tests that may be performed as follow up depending on what is suspected to be the cause of liver damage. Some of these include:
- Tests for hepatitis A, hepatitis B, and hepatitis C
- Testing for exposure to drugs and other substances toxic to the liver (see Drug Abuse Testing and Emergency and Overdose Drug Testing)
- Ethanol level
- Copper and ceruloplasmin for Wilson disease
- Iron tests and genetic tests for hereditary hemochromatosis
A liver biopsy may be performed to help determine the cause of liver injury and to evaluate the extent of liver damage.
How is the sample collected for testing?
A blood sample is drawn from a vein in the arm.
Is any test preparation needed to ensure the quality of the sample?
No test preparation is needed.
Aspartate Aminotransferase (AST) or SGOT
Aspartate aminotransferase (AST) also called SGOT (Serum Glutamic-Oxaloacetic Transaminase) or GOT (Glutamic-Oxaloacetic Transaminase), is an enzyme found in cells throughout your body but mostly in your heart and liver and, to a lesser extent, in the kidneys and muscles. In healthy individuals, levels of AST in the blood are low. When liver or muscle cells are injured, they release AST into the blood. This makes AST a useful test for detecting or monitoring liver damage.
A number of conditions can cause injury to liver cells and may cause increases in AST. The test is most useful in detecting liver damage due to hepatitis, drugs toxic to the liver, cirrhosis, or alcoholism. AST, however, is not specific for the liver and may be increased in conditions affecting other parts of the body.
An aspartate aminotransferase (AST) test is often performed along with an alanine aminotransferase (ALT) test. Both are enzymes found in the liver that become elevated in the blood when the liver is damaged. A calculated AST/ALT ratio is useful for differentiating between different causes of liver injury and in recognizing when the increased levels may be coming from another source, such as heart or muscle injury.
When is AST (aspartate aminotransferase) ordered?
AST may be ordered as part of a comprehensive metabolic panel when someone has a routine health examination.
An AST test may be ordered along with several other tests when a person has signs and symptoms of a liver disorder. Some of these may include:
- Weakness, fatigue
- Loss of appetite
- Nausea, vomiting
- Abdominal swelling and/or pain
- Jaundice
- Dark urine, light-colored stool
- Itching (pruritus)
- Swelling in the legs and ankles
- Tendency to bruise easily
AST may also be ordered, either by itself or with other tests, for people who are at an increased risk for liver disease since many people with mild liver damage will have no signs or symptoms. Some examples include:
- Persons who might have been exposed to hepatitis viruses
- Persons who are heavy drinkers
- Persons who have a history of liver disease in their family
- Persons taking drugs that can damage the liver
- Persons who are overweight and/or have diabetes
Pregnancy, a shot or injection of medicine into muscle tissue, or even strenuous exercise may increase AST levels. Acute burns, surgery, and seizures may raise AST levels as well.
In rare instances, some drugs can damage the liver or muscle, increasing AST levels. This is true of both prescription drugs and some “natural” health products. Be sure to tell your healthcare practitioner about all of the drugs and/or health supplements that you are taking.
When AST is used to monitor treatment of persons with liver disease, it may be ordered on a regular basis during the course of treatment to determine whether the therapy is effective.
What does abnormal AST test result mean?
Low levels of AST in the blood are normal.
Very high levels of AST (more than 10 times normal) are usually due to acute hepatitis, sometimes due to a viral infection. With acute hepatitis, AST levels usually stay high for about 1-2 months but can take as long as 3-6 months to return to normal. Levels of AST may also be markedly elevated (often over 100 times normal) as a result of exposure to drugs or other substances that are toxic to the liver as well as in conditions that cause decreased blood flow (ischemia) to the liver.
With chronic hepatitis, AST levels are usually not as high, often less than 4 times normal, and are more likely to be normal than are ALT levels. AST often varies between normal and slightly increased with chronic hepatitis, so the test may be ordered frequently to determine the pattern. Such moderate increases may also be seen in other diseases of the liver, especially when the bile ducts are blocked, or with cirrhosis or certain cancers of the liver. AST may also increase after heart attacks and with muscle injury, usually to a much greater degree than ALT.
AST is often performed together with the ALT test or as part of a liver panel. For more about AST results in relation to other liver tests, see the Liver Panel article.
In most types of liver disease, the ALT level is higher than AST and the AST/ALT ratio will be low (less than 1). There are a few exceptions; the AST/ALT ratio is usually increased in alcoholic hepatitis, cirrhosis, hepatitis C virus-related chronic liver disease, and in the first day or two of acute hepatitis or injury from bile duct obstruction. With heart or muscle injury, AST is often much higher than ALT (often 3-5 times as high) and levels tend to stay higher than ALT for longer than with liver injury.
What conditions other than liver problems can cause increased AST?
Conditions that affect other organs, such as the heart and skeletal muscle, can cause elevations of AST. Mild to moderate increases may be seen with vigorous exercise and skeletal muscle injury or in conditions such as acute pancreatitis and heart attacks.
What other tests may be used to help determine the cause of liver damage?
After a thorough physical exam and evaluation of a person’s medical history, there are several other tests that may be performed as follow up depending on what is suspected to be the cause of liver damage. Some of these include:
- Tests for hepatitis A, hepatitis B, and hepatitis C
- Testing for exposure to drugs and other substances toxic to the liver
- Ethanol level
- Copper and ceruloplasmin for Wilson disease
- Iron tests and genetic tests for hereditary hemochromatosis
A liver biopsy may be performed to help determine the cause of liver injury and to evaluate the extent of liver damage.
How is the sample collected for testing?
A blood sample is drawn by needle from a vein in the arm.
Is any test preparation needed to ensure the quality of the sample?
No test preparation is needed.
Alkaline Phosphatase (ALP)
Alkaline phosphatase (ALP) is an enzyme found in several tissues throughout the body. The highest concentrations of ALP are present in the cells that comprise bone and the liver. Elevated levels of ALP in the blood are most commonly caused by liver disease or bone disorders. This test measures the level of ALP in the blood.
In the liver, ALP is found on the edges of cells that join to form bile ducts, tiny tubes that drain bile from the liver to the bowels, where it is needed to help digest fat in the diet. ALP in bone is produced by special cells called osteoblasts that are involved in the formation of bone. Each of the various tissue types produces distinct forms of ALP called isoenzymes.
Alkaline phosphatase (ALP) blood levels can be greatly increased, for example, in cases where one or more bile ducts are blocked. This can occur as a result of inflammation of the gallbladder (cholecystitis) or gallstones. Smaller increases of blood ALP are seen in liver cancer and cirrhosis, with use of drugs toxic to the liver, and in hepatitis.
Any condition causing excessive bone formation, including bone disorders such as Paget’s disease, can cause increased ALP levels. Children and adolescents typically have higher blood ALP levels because their bones are still growing. As a result, the ALP test must be interpreted with different reference (normal) values for children and for adults.
It is possible to distinguish between the different forms (isoenzymes) of ALP produced by different types of tissues in the body. If it is not apparent from clinical signs and symptoms whether the source of a high ALP test result is from liver or bone disease, then a test may be performed to determine which isoenzyme is increased in the blood.
When is ALP (alkaline phosphatase) ordered?
An ALP test may be ordered as part of routine laboratory testing, often with a group of other tests called a liver panel. It is also usually ordered along with several other tests when a person has symptoms of a liver or bone disorder.
Signs and symptoms of liver involvement may include:
- Weakness, fatigue
- Loss of appetite
- Nausea, vomiting
- Abdominal swelling and/or pain
- Jaundice
- Dark urine, light-colored stool
- Itching (pruritus)
Some examples of the signs and symptoms suggesting a bone disorder include:
- Bone and/or joint pain
- Increased frequency of fractures
- Deformed bones
How is ALP (alkaline phosphatase) used?
The alkaline phosphatase test (ALP) is used to help detect liver disease or bone disorders.
- In conditions affecting the liver, damaged liver cells release increased amounts of ALP into the blood. This test is often used to detect blocked bile ducts because ALP is especially high in the edges of cells that join to form bile ducts. If one or more of them are obstructed, for example by a tumor, then blood levels of ALP will often be high.
- Any condition that affects bone growth or causes increased activity of bone cells can affect ALP levels in the blood. An ALP test may be used, for example, to detect cancers that have spread to the bones or to help diagnose Paget’s disease, a condition that causes malformed bones. This test may also sometimes be used to monitor treatment of Paget’s disease or other bone conditions, such as vitamin D deficiency.
Pregnancy can increase ALP levels. Temporary elevations are also seen with healing fractures.
Children and adolescents normally have higher ALP levels than adults because their bones are growing, and ALP is often very high during a growth spurt, which occurs at different ages in boys and girls.
Some drugs may affect ALP levels. For example, oral contraceptives may decrease ALP levels while anti-epileptics may increase ALP levels.
If ALP results are increased but it is not clear whether this is due to liver or bone disease, tests for ALP isoenzyme may be done to determine the cause. A GGT test and/or a test for 5′-nucleotidase may also be done to differentiate between liver and bone disease. GGT and 5′-nucleotidase levels are increased in liver disease but not in bone disorders.
What does abnormal ALP test result mean?
High ALP usually means that either the liver has been damaged or a condition causing increased bone cell activity is present.
If other liver tests such as bilirubin, aspartate aminotransferase (AST), or alanine aminotransferase (ALT) are also high, usually the increased ALP is coming from the liver. If GGT or 5′-nucleotidase is also increased, then the high ALP is likely due to liver disease. If either of these two tests is normal, then the high ALP is likely due to a bone condition. Likewise, if calcium and/or phosphorus measurements are abnormal, usually the ALP is coming from bone.
If it is not clear from signs and symptoms or from other routine tests whether the high ALP is from liver or bone, then a test for ALP isoenzymes may be necessary to distinguish between bone and liver ALP.
- ALP in liver disease
ALP results are usually evaluated along with other tests for liver disease. In some forms of liver disease, such as hepatitis, ALP is usually much less elevated than AST and ALT. When the bile ducts are blocked (usually by gallstones, scars from previous gallstones or surgery, or by cancers), ALP and bilirubin may be increased much more than AST or ALT. ALP may also be increased in liver cancer.
- ALP in bone disease
In some bone diseases, such as Paget’s disease, where bones become enlarged and deformed, or in certain cancers that spread to bone, ALP may be increased.
If a person is being successfully treated for Paget’s disease, then ALP levels will decrease or return to normal over time. If someone with bone or liver cancer responds to treatment, ALP levels should decrease.
Moderately elevated ALP may result from other conditions, such as Hodgkin’s lymphoma, congestive heart failure, ulcerative colitis, and certain bacterial infections.
Low levels of ALP may be seen temporarily after blood transfusions or heart bypass surgery. A deficiency in zinc may cause decreased levels. A rare genetic disorder of bone metabolism called hypophosphatasia can cause severe, protracted low levels of ALP. Malnutrition or protein deficiency as well as Wilson disease could also be possible causes for lowered ALP.
What other tests are used to evaluate liver disorders?
There are other commonly used liver tests that measure other enzymes found in liver cells, such as alanine aminotransferase (ALT) and aspartate aminotransferase (AST). A test for bilirubin, a substance produced by the breakdown of red blood cells and removed from the body by the liver, may also be performed. Sometimes these tests (along with albumin and total protein testing) are run together as a liver panel. Other tests that may be performed individually or as part of a liver panel to detect or monitor liver disease include gamma-glutamyl transferase (GGT), lactate dehydrogenase (LDH), and prothrombin time (PT).
How is the sample collected for testing?
A blood sample is drawn by needle from a vein in the arm.
Is any test preparation needed to ensure the quality of the sample?
Fasting is preferred but not required for ALP test. Eating a meal can increase the ALP level slightly for a few hours in some people. It is usually better to do the test after fasting overnight. In this case, only water is permitted.
Gamma-Glutamyl Transferase (GGT)
Gamma-glutamyl transferase (GGT) is an enzyme found in many organs throughout your body, with the highest concentrations found in the liver. GGT is elevated in the blood in most diseases that cause damage to the liver or bile ducts. This test measures the level of GGT in a blood sample.
Normally, GGT is present in low levels, but when the liver is injured, the GGT level can rise. Gamma-glutamyl transferase (GGT) is usually the first liver enzyme to rise in the blood when any of the bile ducts that carry bile from the liver to the intestines become obstructed, for example, by tumors or stones. This makes it the most sensitive liver enzyme test for detecting bile duct problems.
However, the GGT test is not very specific and is not useful in differentiating between various causes of liver damage because it can be elevated with many types of liver diseases, such as liver cancer and viral hepatitis, as well as other non-hepatic conditions, such as acute coronary syndrome. For this reason, the GGT test is not recommended for routine use by itself. However, it can be useful in conjunction with other tests and in determining the cause of a high alkaline phosphatase (ALP) level, another enzyme found in the liver.
Both GGT and ALP are increased in liver diseases, but only ALP will be increased with diseases affecting bone tissue. Therefore, GGT can be used as a follow up to an elevated ALP to help determine if the high ALP result is due to liver or bone disease.
GGT levels are sometimes increased with consumption of even small amounts of alcohol. Higher levels are found more commonly in chronic heavy drinkers than in people who consume less than 2 to 3 drinks per day or who only drink heavily on occasion (binge drinkers). The GGT test may be used in evaluating someone for acute or chronic alcohol abuse.
When is GGT ordered?
A GGT test may be ordered when someone has an elevated ALP level. An ALP test may be ordered alone or as part of a routine liver panel to screen for liver damage, even if no symptoms are present. A GGT test may be ordered when results of the ALP test are high but other tests that are part of the liver panel (such as AST and ALT) are not increased.
GGT may be ordered along with or as a follow up to other liver function tests when a person has signs or symptoms that suggest liver disease. Some signs and symptoms of liver damage include:
- Weakness, fatigue
- Loss of appetite
- Nausea and vomiting
- Abdominal swelling and/or pain
- Jaundice
- Dark urine, light-colored stool
- Itching (pruritus)
GGT may also be ordered when someone with a history of alcohol abuse has completed alcohol treatment in order to monitor compliance with the treatment program.
Even small amounts of alcohol within 24 hours of a GGT test may cause a temporary increase in the GGT.
Smoking can also increase GGT.
Elevated GGT levels may be an indicator of cardiovascular disease and/or hypertension. Some studies have shown that people with increased GGT levels have an elevated risk of dying from heart disease, but the reason for this association is not yet known.
Drugs that may cause an elevated GGT level include phenytoin, carbamazepine, and barbiturates such as phenobarbital. Use of many other prescription and non-prescription drugs, including nonsteroidal anti-inflammatory drugs (NSAIDs), lipid-lowering drugs, antibiotics, histamine receptor blockers (used to treat excess stomach acid production), antifungal agents, antidepressants, and hormones such as testosterone, can increase GGT levels. Clofibrate and oral contraceptives can decrease GGT levels.
Levels of GGT increase with age in women, but not in men, and are always somewhat higher in men than in women.
How is GGT used?
The gamma-glutamyl transferase (GGT) test may be used to determine the cause of elevated alkaline phosphatase (ALP). Both ALP and GGT are elevated in disease of the bile ducts and in some liver diseases, but only ALP will be elevated in bone disease. Therefore, if the GGT level is normal in a person with a high ALP, the cause of the elevated ALP is most likely bone disease.
The GGT test is sometimes used to help detect liver disease and bile duct obstructions. It is usually ordered in conjunction with or as follow up to other liver tests such as ALT, AST, ALP, and bilirubin. (Read also about the Liver Panel.) In general, an increased GGT level indicates that a person’s liver is being damaged but does not specifically point to a condition that may be causing the injury.
GGT can be used to screen for chronic alcohol abuse (it will be elevated in about 75% of chronic drinkers) and to monitor for alcohol use and/or abuse in people who are receiving treatment for alcoholism or alcoholic hepatitis.
What does abnormal GGT test result mean?
An elevated GGT level suggests that a condition or disease is damaging the liver but does not indicate specifically what. In general, the higher the level, the greater the damage to the liver. Elevated GGT levels may be due to liver diseases, such as hepatitis or cirrhosis, but they may also be due to other conditions, such as congestive heart failure, diabetes, or pancreatitis. They may also be caused by alcohol abuse or use of drugs that are toxic to the liver.
A low or normal GGT test result indicates that it is unlikely that a person has liver disease or has consumed any alcohol.
A high GGT level can help rule out bone disease as the cause of an increased ALP level, but if GGT is low or normal, then an increased ALP is more likely due to bone disease.
Can my GGT level be elevated if I don’t have any symptoms?
Yes, GGT is very sensitive and can be increased when you don’t have symptoms. This elevation may be temporary, perhaps due to medications that you are taking or alcohol ingested within 24 hours of the test. If other liver enzymes are normal, your healthcare practitioner may just wait and then repeat the GGT test. If the GGT is very high and/or your other liver enzymes are elevated, it may be necessary to have more extensive testing to identify the cause.
I am an alcoholic, but I have quit drinking. Will my GGT ever go back to normal?
Over time, your GGT level will fall from whatever level it was at when you stopped drinking alcohol to within the normal range. This can take several weeks to more than a month. Abstaining from alcohol will decrease your chances of further damaging your liver and should allow your liver function to improve.
How is the sample collected for testing?
A blood sample is obtained by inserting a needle into a vein in the arm.
Is any test preparation needed to ensure the quality of the sample?
GGT levels fall after meals. You may be instructed to fast (have nothing to eat or drink except water) for at least 8 hours prior to the test. Alcohol and certain prescription medications can affect GGT levels, so you may be asked to abstain from them prior to the test as well.
Bilirubin
Bilirubin is an orange-yellow pigment, a waste product primarily produced by the normal breakdown of heme. Heme is a component of hemoglobin, which is found in red blood cells (RBCs). Bilirubin is ultimately processed by the liver to allow its elimination from the body. This test measures the amount of bilirubin in the blood to evaluate a person’s liver function or to help diagnose anemias caused by red blood cell destruction (hemolytic anemia).
Red blood cells normally degrade after about 120 days in circulation. As heme is released from hemoglobin, it is converted to bilirubin. This form of bilirubin is also called unconjugated bilirubin. Unconjugated bilirubin is carried by proteins to the liver; there, sugars are attached (conjugated) to bilirubin to form conjugated bilirubin. Conjugated bilirubin enters the bile and passes from the liver to the small intestines; there, it is further broken down by bacteria and eventually eliminated in the stool. Thus, the breakdown products of bilirubin give stool its characteristic brown color.
A small amount (approximately 250 to 350 milligrams) of bilirubin is produced daily in a normal, healthy adult. Most (85%) of bilirubin is derived from damaged or degraded red blood cells (RBCs), with the remaining amount derived from the bone marrow or liver. Normally, small amounts of unconjugated bilirubin are released into the blood, but virtually no conjugated bilirubin is present. Both forms can be measured or estimated by laboratory tests, and a total bilirubin result (a sum of these) may also be reported.
If the bilirubin level increases in the blood, a person may appear jaundiced, with a yellowing of the skin and/or whites of the eyes. The pattern of bilirubin test results can give the health practitioner information regarding the condition that may be present. For example, unconjugated bilirubin may be increased when there is an unusual amount of red blood cell destruction destruction (hemolysis) or when the liver is unable to process bilirubin (i.e., with liver diseases such as cirrhosis or inherited problems). Conversely, conjugated bilirubin can increase when the liver is able to process bilirubin but is not able to pass the conjugated bilirubin to the bile for removal; when this happens, the cause is often acute hepatitis or blockage of the bile ducts.
Increased total and unconjugated bilirubin levels are relatively common in newborns in the first few days after birth. This finding is called “physiologic jaundice of the newborn” and occurs because the newborn’s liver is not mature enough to process bilirubin yet. Usually, physiologic jaundice of the newborn resolves itself within a few days. However, in hemolytic disease of the newborn, red blood cell destructions may be destroyed because of blood incompatibilities between the baby and the mother; in these cases, treatment may be required because high levels of unconjugated bilirubin can damage the newborn’s brain.
A rare (about 1 in 10,000 births) but life-threatening congenital condition called biliary atresia can cause increased total and conjugated bilirubin levels in newborns. This condition must be quickly detected and treated, usually with surgery, to prevent serious liver damage that may require liver transplantation within the first few years of life. Some children may require liver transplantation despite early surgical treatment.
When is bilirubin test ordered?
A health practitioner usually orders a bilirubin test in conjunction with other laboratory tests (alkaline phosphatase [ALP], aspartate aminotransferase [AST], alanine aminotransferase [ALT]) when someone shows signs of abnormal liver function. A bilirubin level may be ordered when a person:
- Shows evidence of jaundice
- Has a history of drinking excessive amounts of alcohol
- Has suspected drug toxicity
- Has been exposed to hepatitis-causing viruses
Other symptoms that may be present include:
- Dark, amber-colored urine
- Nausea/vomiting
- Abdominal pain and/or swelling
- Fatigue and general malaise that often accompany chronic liver disease
Measuring and monitoring bilirubin in newborns with jaundice is considered standard medical care.
Tests for bilirubin may also be ordered when someone is suspected of having (or known to have) hemolytic anemia as a cause of anemia. In this case, it is often ordered along with other tests used to evaluate hemolysis, such as complete blood count, reticulocyte count, haptoglobin, and lactate dehydrogenase (LDH).
How is bilirubin test used?
A bilirubin test is used to detect an increased level in the blood. It may be used to help determine the cause of jaundice and/or help diagnose conditions such as liver disease, hemolytic anemia, and blockage of the bile ducts.
Bilirubin is an orange-yellow pigment, a waste product primarily produced by the normal breakdown of heme. Heme is a component of hemoglobin, which is found in red blood cells (RBCs). Bilirubin is ultimately processed by the liver to allow its elimination from the body. Any condition that accelerates the breakdown of RBCs or affects the processing and elimination of bilirubin may cause an elevated blood level.
Two forms of bilirubin can be measured or estimated by laboratory tests:
- Unconjugated bilirubin—when heme is released from hemoglobin, it is converted to unconjugated bilirubin. It is carried by proteins to the liver. Small amounts may be present in the blood.
- Conjugated bilirubin—formed in the liver when sugars are attached (conjugated) to bilirubin. It enters the bile and passes from the liver to the small intestines and is eventually eliminated in the stool. Normally, no conjugated bilirubin is present in the blood.
Usually, a chemical test is used to first measure the total bilirubin level (unconjugated plus conjugated bilirubin). If the total bilirubin level is increased, the laboratory can use a second chemical test to detect water-soluble forms of bilirubin, called “direct” bilirubin. The direct bilirubin test provides an estimate of the amount of conjugated bilirubin present. Subtracting direct bilirubin level from the total bilirubin level helps estimate the “indirect” level of unconjugated bilirubin. The pattern of bilirubin test results can give the healthcare provider information regarding the condition that may be present.
Though unconjugated bilirubin may be toxic to brain development in newborns (up to 2-4 weeks of age), it does not pose the same threat to older children and adults. In older children and adults, the “blood-brain barrier” is more developed and prevents bilirubin from gaining access to brain cells. Nevertheless, elevated bilirubin strongly suggests that a medical condition is present that must be evaluated and treated.
Bilirubin is not normally present in the urine. However, conjugated bilirubin is water-soluble and may be eliminated from the body through the urine if it cannot pass into the bile. Measurable bilirubin in the urine usually indicates blockage of liver or bile ducts, hepatitis, or some other form of liver damage and may be detectable early in disease; for this reason, bilirubin testing is integrated into common dipstick testing used for routine urinalysis.
Bilirubin concentrations tend to be slightly higher in males than females. African Americans routinely show lower bilirubin concentrations than non-African Americans. Strenuous exercise may increase bilirubin levels.
Drugs that can decrease total bilirubin include barbiturates, caffeine, penicillin, and high doses of salicylates (e.g. aspirin). The drug atazanavir increases unconjugated (indirect) bilirubin.
In adults and older children, bilirubin is measured to:
- Diagnose and/or monitor diseases of the liver and bile duct (e.g., cirrhosis, hepatitis, or gallstones)
- Evaluate people with sickle cell disease or other causes of hemolytic anemia; these people may have episodes called crises when excessive RBC destruction increases bilirubin levels.
In newborns with jaundice, bilirubin is used to distinguish the causes of jaundice.
- In both physiologic jaundice of the newborn and hemolytic disease of the newborn, only unconjugated (indirect) bilirubin is increased.
- In much less common cases, damage to the newborn’s liver from neonatal hepatitis and biliary atresia will increase conjugated (direct) bilirubin concentrations as well, often providing the first evidence that one of these less common conditions is present.
It is important that an elevated level of bilirubin in a newborn be identified and quickly treated because excessive unconjugated bilirubin damages developing brain cells. The consequences of this damage include mental retardation, learning and developmental disabilities, hearing loss, eye movement problems, and death.
What does abnormal bilirubin test result mean?
Adults and children
Increased total bilirubin that is mainly unconjugated (indirect) bilirubin may be a result of:
- Hemolytic or pernicious anemia
- Transfusion reaction
- Cirrhosis
- A relatively common inherited condition called Gilbert syndrome, due to low levels of the enzyme that produces conjugated bilirubin
If conjugated (direct) bilirubin is elevated more than unconjugated (indirect) bilirubin, there typically is a problem associated with decreased elimination of bilirubin by the liver cells. Some conditions that may cause this include:
- Viral hepatitis
- Drug reactions
- Alcoholic liver disease
Conjugated (direct) bilirubin is also elevated more than unconjugated (indirect) bilirubin when there is blockage of the bile ducts. This may occur, for example, with:
- Gallstones present in the bile ducts
- Tumors
- Scarring of the bile ducts
Rare inherited disorders that cause abnormal bilirubin metabolism such as Rotor, Dubin-Johnson, and Crigler-Najjar syndromes, may also cause increased levels of bilirubin.
Low levels of bilirubin are generally not concerning and are not monitored.
Newborns
An elevated bilirubin level in a newborn may be temporary and resolve itself within a few days to two weeks. However, if the bilirubin level is above a critical threshold or increases rapidly, an investigation of the cause is needed so appropriate treatment can be initiated. Increased bilirubin concentrations may result from the accelerated breakdown of red blood cells due to:
- Blood type incompatibility between the mother and her newborn
- Certain congenital infections
- Lack of oxygen (hypoxia)
- Diseases that can affect the liver
In most of these conditions, only unconjugated (indirect) bilirubin is increased. An elevated conjugated (direct) bilirubin is seen in the rare conditions of biliary atresia and neonatal hepatitis. Biliary atresia requires surgical intervention to prevent liver damage.
Are some people more at genetic risk of abnormal bilirubin levels?
Several inherited chronic conditions increase bilirubin levels in the blood and include Gilbert syndrome, Dubin-Johnson syndrome, Rotor syndrome, and Crigler-Najjar syndrome. The first three are usually mild, chronic conditions that can be aggravated under certain conditions but in general cause no significant health problems. For example, Gilbert syndrome is very common; about 1 in every 6 people has this genetic abnormality, but usually people with Gilbert syndrome do not have elevated bilirubin. Crigler-Najjar syndrome is the most serious inherited condition listed; this disorder is relatively rare, and some people with it may die.
How do you treat abnormal bilirubin levels and/or jaundice?
Treatment depends on the cause of the jaundice. In newborns, phototherapy (special light therapy), blood exchange transfusion, and/or certain drugs may be used to reduce the bilirubin level. In Gilbert, Rotor, and Dubin-Johnson syndromes, no treatment is usually necessary. Crigler-Najjar syndrome may respond to certain enzyme drug therapy or may require a liver transplant. Jaundice caused by an obstruction is often resolved by surgery. Jaundice due to cirrhosis is a result of long-term liver damage and does not respond well to any type of therapy other than liver transplantation.
How is the sample collected for testing?
In adults, blood is typically collected from a vein in the arm using a needle. In newborns, blood is often collected from a heelstick. Heelstick is a technique that uses a small, sharp blade to cut the skin on the infant’s heel so that a few drops of blood can be collected in a small tube. Non-invasive technology that measures bilirubin through the skin is available in some healthcare facilities; this instrument is called a transcutaneous bilirubin meter.
Is any test preparation needed to ensure the quality of the sample?
You may need to fast (nothing but water) for several hours before the test; fasting requirements vary by laboratory. Ask your lab or healthcare provider for instructions.
Lactate Dehydrogenase (LDH)
Lactate dehydrogenase (LDH or LD) is an enzyme involved in energy production that is found in almost all of the body’s cells, with the highest levels found in the cells of the heart, liver, muscles, kidneys, lungs, and in blood cells; bacteria also produce lactate dehydrogenase. This test measures the level of LDH in the blood or sometimes other body fluids.
Blood LDH (lactate dehydrogenase)
Only a small amount of lactate dehydrogenase (LDH) is usually detectable in the fluid portion of the blood (serum or plasma). Lactate dehydrogenase (LDH) is released from the cells into the serum when cells are damaged or destroyed. Thus, an lactate dehydrogenase (LDH) blood level is a non-specific marker for the presence of tissue damage somewhere in the body. By itself, it cannot be used to identify the underlying cause or location of the cellular damage. However, it may be used, in conjunction with other blood tests, to help evaluate for and/or monitor conditions that lead to tissue damage, such as liver or blood diseases or cancer.
Fluid LDH (lactate dehydrogenase)
Sometimes when there is injury, inflammation, or infection within a specific area of the body, such as the brain, heart or lungs, fluid will accumulate or constituents of the fluid present will change. The level of lactate dehydrogenase present in the fluid may be useful in determining the cause. For example, lactate dehydrogenase is typically high in cerebrospinal fluid when an individual has bacterial meningitis. The lactate dehydrogenase test can also be used, along with other tests, to determine whether fluid accumulation, for example around the heart or lungs or in the abdominal cavity, is due to injury or inflammation (exudate) or due to an imbalance of fluid pressure inside blood vessels and the protein level in blood (transudate).
When is LDH (lactate dehydrogenase) ordered?
Blood test
An lactate dehydrogenase level may be ordered, along with other tests such as a comprehensive metabolic panel, when a health practitioner suspects that a disease or condition is causing some degree of cellular or tissue damage. If lactate dehydrogenase is elevated, then more specific tests, such as ALT, AST or ALP, may help diagnose the condition and help determine which organs are involved. Once the acute or chronic problem is diagnosed, total lactate dehydrogenase levels may be ordered at regular intervals to monitor its progress and/or resolution.
Lactate dehydrogenase levels may also occasionally be ordered when an individual has experienced muscle trauma or injury or when a person has signs and symptoms of hemolytic anemia.
Lactate dehydrogenase testing may be ordered on a regular basis when an individual has been diagnosed with cancer.
Body fluid test
This test may be ordered, for example, when a person has signs and symptoms of meningitis or when someone has a buildup of fluid around the heart, lungs or in the abdomen.
How is LDH (lactate dehydrogenase) test used?
A lactate dehydrogenase test is a non-specific test that may be used in the evaluation of a number of diseases and conditions. Lactate dehydrogenase is an enzyme that is found in almost all of the body’s cells (as well as in bacteria) and is released from cells into the fluid portion of blood (serum or plasma) when cells are damaged or destroyed. Thus, the blood level of lactate dehydrogenase is a general indicator of tissue and cellular damage. The level of lactate dehydrogenase may also rise in other types of body fluids (e.g., cerebrospinal fluid, pleural fluid, etc.) in the presence of certain diseases.
A lactate dehydrogenase blood test may be used:
- As a general indicator of the existence and severity of acute or chronic tissue damage
- To detect and monitor progressive conditions such as anemia, including hemolytic anemia and megaoloblastic anemia, or severe infections
- To help stage, determine prognosis, and/or monitor treatment (i.e., chemotherapy) of cancers, such as germ cell tumors (e.g., some types of testicular cancer and ovarian cancer), lymphoma, leukemia, melanoma, and neuroblastoma
An lactate dehydrogenase test is performed on body fluids for a few different reasons:
- To help evaluate cerebrospinal fluid and distinguish between bacterial or viral meningitis
- To evaluate other body fluids such as pleural, peritoneal or pericardial fluid and help determine whether the accumulation of fluid is due to injury and inflammation (exudate) or due to an imbalance of pressure within blood vessels and the amount of protein in the blood (transudate). This information is helpful in guiding treatment.
What does abnormal LDH (lactate dehydrogenase) test result mean?
Blood test
Elevated levels of lactate dehydrogenase usually indicate some type of tissue damage. lactate dehydrogenase levels typically will rise as the cellular destruction begins, peak after some time period, and then begin to fall. lactate dehydrogenase levels are elevated in a wide variety of conditions, reflecting its widespread tissue distribution.
An elevated level of lactate dehydrogenase may be seen with:
- Hemolytic anemia
- Pernicious anemia (megaloblastic anemia)
- Infections such as infectious mononucleosis (mono), meningitis, encephalitis, HIV
- Sepsis
- Intestinal and lung (pulmonary) infarction
- Acute kidney disease
- Acute liver disease
- Acute muscle injury
- Pancreatitis
- Bone fractures
- Testicular cancer, lymphoma or other cancers
A high lactate dehydrogenase in the blood may indicate that treatment for cancer (e.g., chemotherapy) has not been successful. A high level is predictive of a poorer outlook for survival for those with cancer. With some chronic and progressive conditions, moderately elevated lactate dehydrogenase blood levels may persist. Low and normal levels of lactate dehydrogenase do not usually indicate a problem. Low levels are sometimes seen when someone ingests large amounts of ascorbic acid (vitamin C).
Many things can affect blood lactate dehydrogenase results that are not necessarily a cause for concern. For example:
- Strenuous exercise can cause temporary elevations in lactate dehydrogenase.
- Hemolysis of the blood specimen can cause falsely elevated results. This may happen if the specimen is handled roughly, stored in extreme temperatures, or if the sample was difficult to collect.
- If a person’s platelet count is increased, serum lactate dehydrogenase can be artificially high and not reflective of the lactate dehydrogenase actually present in the circulation.
Historically, the lactate dehydrogenase test was used to help diagnose and monitor a heart attack, but the test for troponin has largely replaced lactate dehydrogenase in this role. lactate dehydrogenase is not specific for damage to the heart and is no longer recommended for evaluating people with suspected acute coronary syndrome.
Body fluids:
- Cerebrospinal fluid—a high lactate dehydrogenase indicates that meningitis is likely caused by bacteria, while a low or normal level indicates viral meningitis is more likely.
- A high lactate dehydrogenase indicates that pericardial fluid, peritoneal or pleural fluid is an exudate, while a low level indicates it is transudate. Transudates are usually caused by congestive heart failure or cirrhosis. Exudates have several possible causes and usually require additional testing to determine the cause. Read more about these tests by accessing the specific fluid article listed under Related Tests (above).
If the lactate dehydrogenase test is not specific, then how can it be clinically useful?
The lactate dehydrogenase test can be useful to a health practitioner as a warning because it indicates that cellular injury is occurring. In a similar fashion, tests such as a C-reactive protein (CRP) warn that inflammation is occurring somewhere in the body.
Is there anything I can do to lower my lactate dehydrogenase level?
No, LDH is an indicator of injury that will typically return to normal when the underlying condition resolves. If someone has a chronic condition with ongoing tissue damage, such as may occur with liver disease, then increased lactate dehydrogenase concentrations may persist.
What is an lactate dehydrogenase isoenzymes test?
A test for lactate dehydrogenase isoenzymes is rarely ordered and not widely available nowadays. In the past, the test was used to help diagnose and monitor heart attacks, but it has been replaced by the test for troponin. Though not a routine test, it may be used in differential diagnosis to help determine which organs are likely affected by tissue damage when the cause of an elevated total lactate dehydrogenase is not clear and cannot be determined using other specific tests.
Lactate dehydrogenase exists in five different forms called isoenzymes. Although there is some overlap, each of the five lactate dehydrogenase isoenzymes tends to be concentrated in specific body tissues. In general, the isoenzyme locations tend to be:
- LD-1: heart, red cells, kidneys, germ cells
- LD-2: heart, red blood cells, kidneys (lesser amounts than LD-1)
- LD-3: lungs and other tissues
- LD-4: white blood cells, lymph nodes, muscles, liver (lesser amounts than LD-5)
- LD-5: liver, skeletal muscle
Determining which isoenzyme is elevated in the blood may give clues to where tissue damage is occurring in the body and/or which organs may be affected.
How is the sample collected for testing?
A blood sample is obtained by inserting a needle into a vein in the arm. Sometimes a special procedure may be performed to collect body fluid from the site affected (e.g., cerebrospinal fluid, pleural fluid, peritoneal fluid, etc.).
Is any test preparation needed to ensure the quality of the sample?
No test preparation is needed.
What does elevated liver enzymes mean
Elevated liver enzymes may indicate inflammation or damage to cells in the liver 8. Inflamed or injured liver cells leak higher than normal amounts of certain chemicals, including liver enzymes, into the bloodstream, which can result in elevated liver enzymes on blood tests.
The specific elevated liver enzymes most commonly found are:
- Alanine aminotransferase (ALT)
- Aspartate aminotransferase (AST)
- Alkaline phosphatase (ALP)
- Gamma-glutamyl transpeptidase (GGT)
Elevated liver enzymes may be discovered during routine blood testing. In most cases, liver enzyme levels are only mildly and temporarily elevated. Most of the time, elevated liver enzymes don’t signal a chronic, serious liver problem.
Many diseases and conditions can contribute to elevated liver enzymes. Your doctor determines the specific cause of your elevated liver enzymes by reviewing your medications, your signs and symptoms and, in some cases, other tests and procedures.
If a blood test reveals you have elevated liver enzymes, ask your doctor about what your test results might mean. Your doctor may suggest you undergo other tests and procedures to determine what’s causing your elevated liver enzymes.
Causes of elevated liver enzymes
Many diseases and conditions can contribute to elevated liver enzymes. Your doctor determines the specific cause of your elevated liver enzymes by reviewing your medications, your signs and symptoms and, in some cases, other tests and procedures.
The most common alterations in enzyme levels encountered in clinical practice can be divided into 2 major subgroups:
- Hepatocellular predominant: Arising from liver cells (hepatocytes).
- Cholestatic predominant: Cholestasis is any condition in which the flow of bile from the liver is slowed or blocked.
Although certain liver diseases may display a mixed biochemical picture — usually elevated AST and ALT levels with mild abnormalities of alkaline phosphatase (ALP) and γ-glutamyl transpeptidase (GGT) levels — the ability to distinguish between the 2 subgroups is fundamental to narrowing down the differential diagnosis.
More common causes of elevated liver enzymes include:
- Over-the-counter pain medications, particularly acetaminophen (Tylenol, others)
- Certain prescription medications, including statin drugs used to control cholesterol
- Drinking alcohol
- Heart failure
- Hepatitis A
- Hepatitis B
- Hepatitis C
- Nonalcoholic fatty liver disease
- Obesity
Other causes of elevated liver enzymes may include:
- Alcoholic hepatitis (severe liver inflammation caused by excessive alcohol consumption)
- Autoimmune hepatitis (liver inflammation caused by an autoimmune disorder)
- Celiac disease (small intestine damage caused by gluten)
- Cytomegalovirus (CMV) infection
- Epstein-Barr virus
- Hemochromatosis (too much iron stored in your body)
- Irritable bowel syndrome
- Mononucleosis
- Polymyositis (inflammatory disease that causes muscle weakness)
- Sepsis
- Thyroid disorders
- Toxic hepatitis (liver inflammation caused by drugs or toxins)
- Wilson’s disease (too much copper stored in your body)
Table 3. Common causes of marked elevated aminotransferase levels
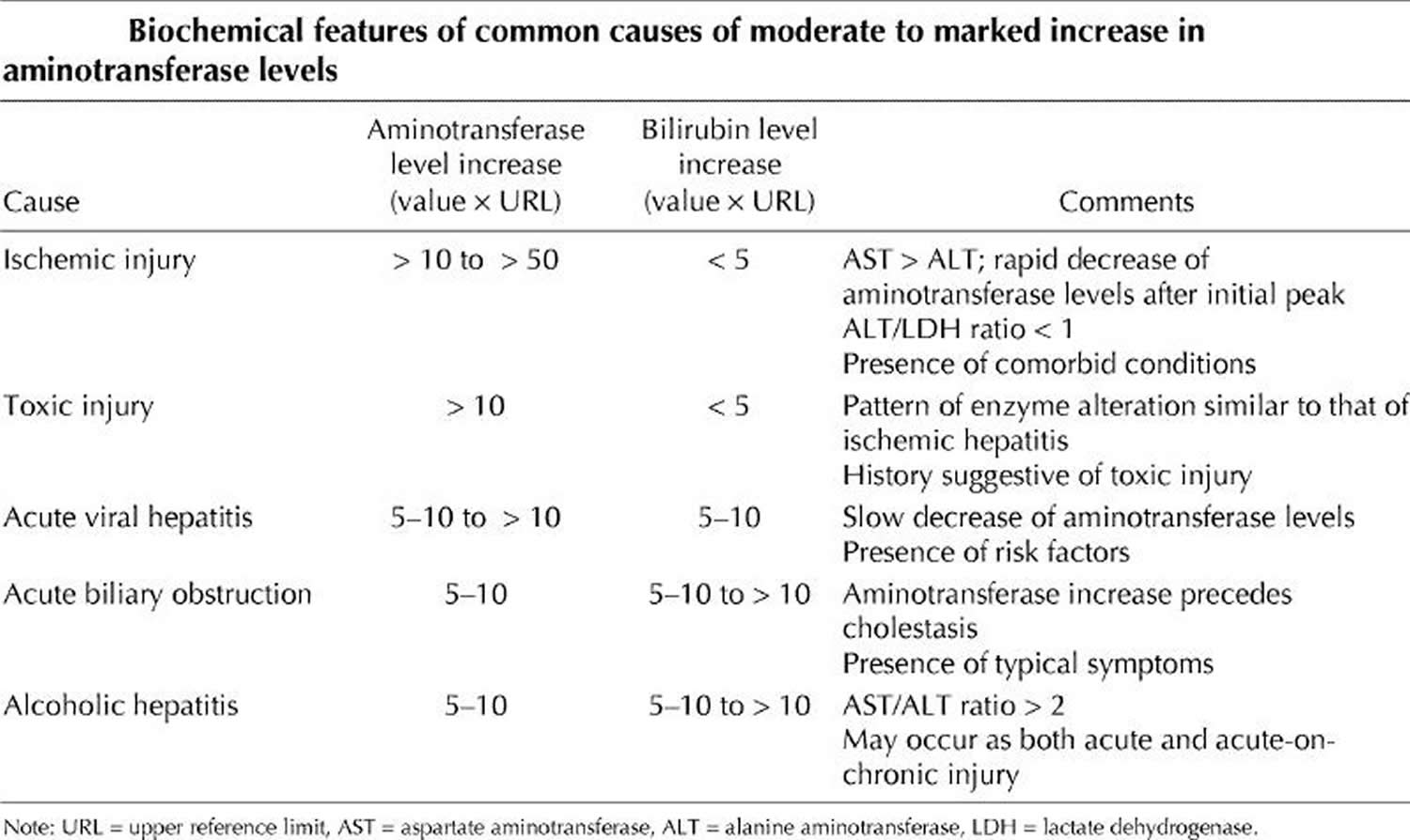
Figure 1. Serum aminotransferase levels in various liver diseases
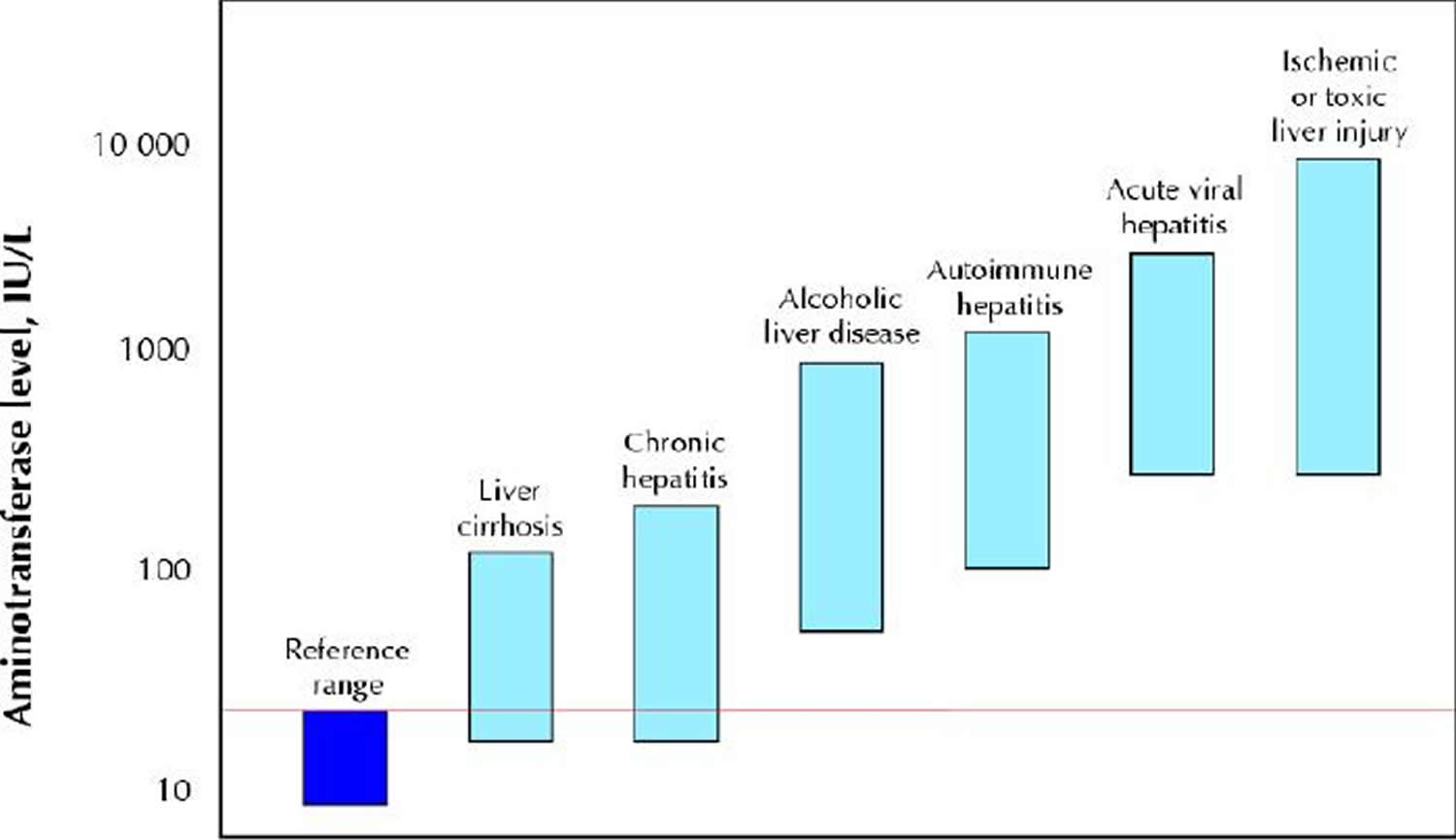
Note: Patients with acute viral or ischemic or toxic liver injury reach the highest aminotransferase levels, but there is a broad overlap in aminotransferase values between patients with acute alcoholic hepatitis and autoimmune hepatitis as well as between patients with chronic hepatitis and liver cirrhosis. Both chronic hepatitis and cirrhotic patients may have aminotransferase levels within the reference range. The red line indicates the upper limit of the reference range.
[Source 1]Hepatocellular (Liver cell) predominance
Injury to the liver, whether acute or chronic, eventually results in an increase in serum concentrations of aminotransferases. Aspartate aminotransferase (AST) and alanine aminotransferase (ALT) are enzymes that catalyze the transfer of α-amino groups from aspartate and alanine to the α-keto group of ketoglutaric acid to generate oxalacetic and pyruvic acids respectively, which are important contributors to the citric acid cycle. Both enzymes require pyridoxal-5′-phosphate (vitamin B6) in order to carry out this reaction, although the effect of pyridoxal-5′-phosphate deficiency is greater on alanine aminotransferase (ALT) activity than on that of aspartate aminotransferase (AST) 9. This has clinical relevance in patients with alcoholic liver disease, in whom pyridoxal-5′-phosphate deficiency may decrease ALT serum activity and contribute to the increase in the AST/ALT ratio that is observed in these patients 10.
Both aminotransferases are highly concentrated in the liver. Aspartate aminotransferase (AST) is also diffusely represented in the heart, skeletal muscle, kidneys, brain and red blood cells, and Alanine aminotransferase (ALT) has low concentrations in skeletal muscle and kidney 11; an increase in Alanine aminotransferase (ALT) serum levels is, therefore, more specific for liver damage. In the liver, Alanine aminotransferase (ALT) is localized solely in the cellular cytoplasm, whereas Aspartate aminotransferase (AST) is both cytosolic (20% of total activity) and mitochondrial (80% of total activity) 12. Zone 3 of the hepatic acinus has a higher concentration of AST, and damage to this zone, whether ischemic or toxic, may result in greater alteration to AST levels. Aminotransferase clearance is carried out within the liver by sinusoidal cells 13. The half-life in the circulation is about 47 hours for ALT, about 17 hours for total AST and, on average, 87 hours for mitochondrial AST 5.
The magnitude of aminotransferase (ALT and AST) alteration can be classified as:
- “Mild” (< 5 times the upper reference limit),
- “Moderate” (5–10 times the upper reference limit) or
- “Marked” (> 10 times the upper reference limit).
This classification is somewhat arbitrary, since no uniform definition exists and various reviews of the subject use different cut-off points 14. Marked and moderate increases are discussed together because the clinical distinction between them is especially grey.
Mild increase in aminotransferase levels (ALT and AST)
A minimal or mild increase in aminotransferase level is the most common biochemical alteration encountered in everyday clinical practice. In addition to considering the when and where of the alterations, there is a series of first-line tests that can be performed on all patients because of their clinical relevance and the high prevalence of the diseases screened by these tests. Extrahepatic causes of aminotransferase alteration (especially in patients with isolated AST elevation) should be ruled out by considering the clinical context of enzyme abnormality. Although some reviews dealing with liver enzyme alteration suggest repeating tests as a first measure in order to rule out laboratory error and a first-line, clinically guided screening for the most prevalent causes of chronic liver disease be started together with repetition of the test. In fact, chronic hepatitis C infection is characterized by a pattern of aminotransferase levels fluctuating around the upper reference value. For patients who are taking drugs known to cause liver injury or who have evidence of alcohol abuse, a second, confirmatory check of aminotransferase levels after alcohol or the medication has been stopped can be a suitable option; patients who have evidence of alcohol abuse also need to be carefully assessed for the risk of underlying chronic damage.
As in the case of acute damage, the pharmacologic history of the patient is of particular importance. All nonessential and over-the-counter medications should be discontinued, and discontinuation of an essential medication should be considered in a risk–benefit perspective. The use of dedicated scales or scores may help the clinician assess the likelihood of the hepatic drug reaction 15. Liver biopsy may represent a suitable diagnostic option in particular cases.
Nonalcoholic fatty liver disease (NAFLD) is the most common cause of mild alteration of liver enzyme levels in the western world, and, according to the National Health and Nutritional Survey, point-prevalence is about 23% among American adults 16. The biochemical picture includes mildly raised aminotransferase levels, and GGT levels can be elevated up to 3 times the upper reference value in nearly half of patients in the absence of ethanol consumption 17. As with chronic viral hepatitis, an AST/ALT ratio greater than 1, which is observed in 61% of patients with advanced fibrosis and 24% of patients with no or initial fibrosis, is highly suggestive of advanced liver disease 18. Suspicion of nonalcoholic fatty liver disease is increased by the presence of conditions linked to the metabolic syndrome and insulin resistance (increased body mass index, diabetes, hyperlipemia, hypertension), although the disease may occur in patients without these associated factors 16. The diagnostic approach to suspected nonalcoholic fatty liver disease is aimed at ruling out other causes of liver disease since there is no specific blood test for diagnosis. Distinguishing between simple steatosis with or without minimal inflammation and nonalcoholic steatohepatitis with fibrosis with confidence is not possible on clinical grounds alone, and therefore liver biopsy should be performed in order to confirm diagnosis and assess prognosis 19.
All patients presenting with mild increases in aminotransferase levels should be questioned about risk factors for hepatitis B or C infection (intravenous drug use, exposure to nonsterile needles or sexual exposure to an infected person). However, since these 2 diseases have a high prevalence worldwide 20 and infected people may lack or under report specific risk factors for infection 21, testing for Hepatitis C virus antibodies and hepatitis B surface antigens is advisable for all patients presenting with a mild increase in aminotransferase levels. If the patient tests positive for Hepatitis C virus antibodies, then qualitative Hepatitis C virus RNA testing should follow. In subjects who are seropositive for hepatitis B, the successive diagnostic work-up may depend upon the clinical situation (e.g., e-minus v. wild-type strands). It is important to emphasize that the degree of aminotransferase alteration is a poor guide to the severity of the disease in patients with established chronic viral hepatitis, unless an AST/ALT ratio greater than 1 is found 22. An AST/ALT ratio greater than 1 can be found in 4% of patients with chronic hepatitis C infection and in 79% of patients who also have liver cirrhosis 23. Among patients with cirrhosis of viral cause, an AST/ALT ratio greater than 1.17 was found to prognosticate 1-year survival with 87% sensitivity and 52% specificity 22. Patients may benefit from ultrasound examination of the liver in order to evaluate the presence of signs of advanced disease or liver masses. In patients with viral hepatitis, liver biopsy is needed to assess progression, evaluate the need for therapy and establish a prognosis.
HFE-related hereditary hemochromatosis is a fairly common autosomal recessive condition (homozygote frequency 1:200-1:400) 24 that is characterized by pathological deposition of iron in the liver, pancreas and heart. Serum ferritin, iron and transferrin saturation index (serum iron/total iron binding capacity) should routinely be measured in patients with altered aminotransferase levels.60 High ferritin levels and, most importantly, a transferrin saturation index greater than 45% are strongly suggestive of the disease 25. The presence of diabetes, heart disease or arthritis is also suggestive, and mutation analysis for the HFE gene may confirm the diagnosis, especially if the patient is of northern European descent 24. Nevertheless, other, rarer forms of non-HFE-related hereditary hemochromatosis are being characterized more frequently, and liver biopsy remains a fundamental diagnostic tool in the presence of strong clinical suspicion and a negative result for HFE gene mutation analysis 25.
The presence of a mild elevation in aminotransferase levels in female patients with concomitant autoimmune disorders (e.g., autoimmune thyroiditis, connective tissue diseases) is suggestive of autoimmune hepatitis. The prevalence of the disease is about 1:6000 to 1:7000, and as many as 80% of patients may have hypergammaglobulinemia even in the absence of liver cirrhosis 26. Patients with suspected autoimmune hepatitis should have autoantibodies tested (antinuclear, anti-smooth muscle and anti-liver–kidney microsomes), although the criteria for diagnosis are complex and include liver biopsy 26. Patients may have a dramatic therapeutic response to corticosteroids, but the course of the disease may be long and can fluctuate between phases of remission and relapses that may mimic acute hepatitis 26.
Wilson’s disease (homozygote frequency 1:30 000– 1:300 000) should be suspected in young patients with signs of hemolysis or concomitant psychiatric or neurologic symptoms, and serum ceruloplasmin levels and copper metabolism (serum and 24-hour urinary copper) should be tested. Diagnosis in patients showing low serum ceruloplasmin levels and increased urinary copper excretion can be confirmed by slit-lamp examination for Kayser–Fleischer rings, although liver biopsy with quantitative copper measurement may be needed where no clear clinical diagnosis is possible 27.
Although α-1-antitripsin deficiency is not a rare disease, affecting 1:1600–1:2800 newborns in Europe and the United States, it is an unusual cause of aminotransferase alteration among adults since the disease is usually identified in childhood.62 It can be suspected in adult patients with concomitant pulmonary disease (emphysema), although low serum α-1-antitripsin levels and phenotype determination provide definite diagnosis 28.
Finally, it has been reported that up to 10% of patients with unexplained hypertransaminasemia actually have celiac disease, and minimal or mild alteration of aminotransferase levels may be the only visible part of the “celiac iceberg” 29. In these patients, screening by measuring tissue transglutaminase antibodies and confirmation and grading of the disease by small bowel biopsy are required for diagnosis 30.
Marked and moderate aminotransferase increase (ALT and AST)
Patients with a marked increase in aminotransferase levels (> 10 times the upper reference limit) typically have acute hepatic injury. However, data from a series of patients with acute hepatic injury due to viral hepatitis suggest that the most sensitive and specific aminotransferase threshold level to identify acute injury lies within the moderate range of increase (5–10 times the upper reference limit, at 200 IU/L for AST and 300 IU/L for ALT) 31. Thus, the academic attribution of cause and “severity” of acute damage on the basis of the magnitude of enzyme elevation may sometimes be misleading, since there can be grey areas in which a range of causes overlap (Figure 1). Moreover, the degree of elevation varies during the course of injury and depends on when the enzyme levels were tested (see Figure. 2).
Figure 2. Schematic representation of the rate of change of aminotransferase and bilirubin levels in a patient with acute ischemic hepatitis and and acute viral hepatitis
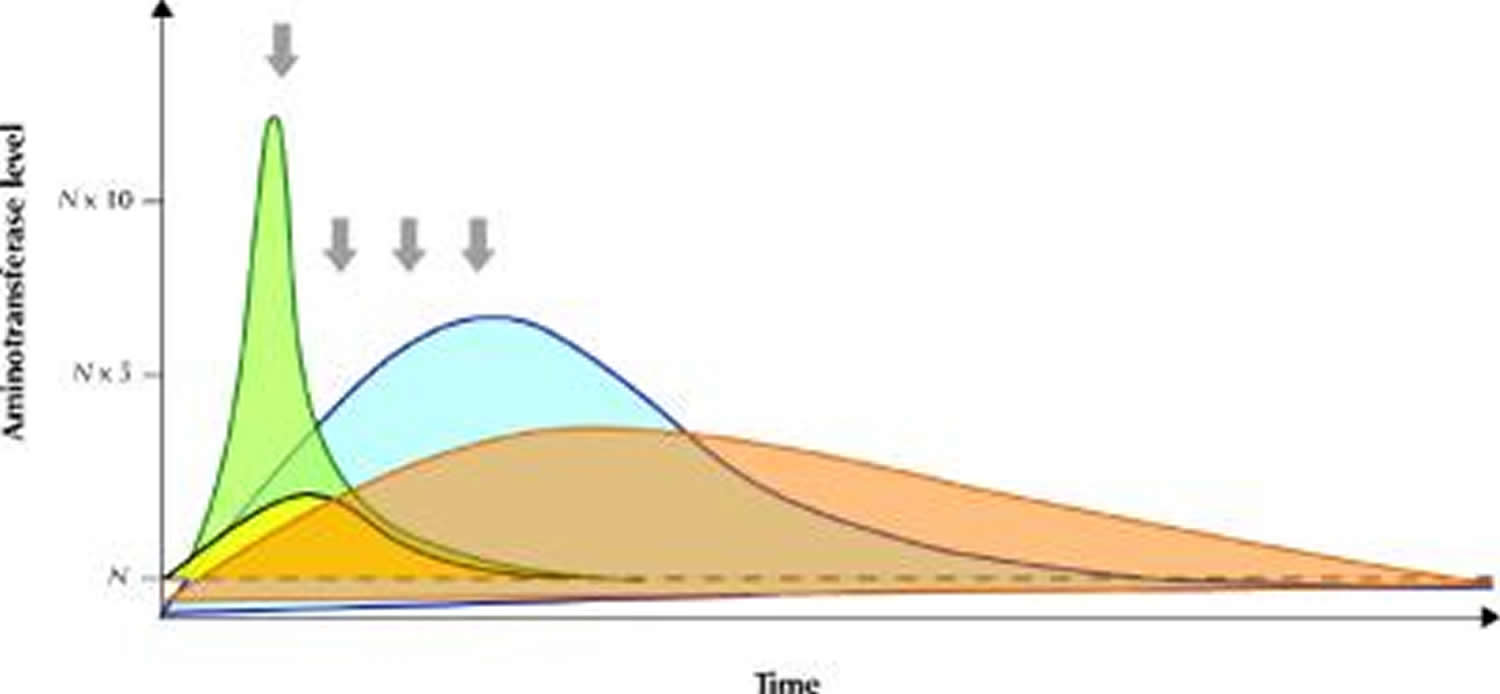
Note: Schematic representation of the rate of change of aminotransferase and bilirubin levels in a patient with acute ischemic hepatitis (green area, yellow area respectively) and acute viral hepatitis (blue area, orange area respectively). It is important to underscore that the pattern of enzyme alteration may vary and occasionally appear similar if a single observation point is taken into consideration (arrows).
[Source 1]Despite these ambiguities, the magnitude and rate of change of aminotransferase alteration may provide initial insight into a differential diagnosis. Very high aminotransferase levels (> 75 times the upper reference limit) indicate ischemic or toxic liver injury in more than 90% of cases of acute hepatic injury, whereas they are less commonly observed with acute viral hepatitis 5. In ischemic or toxic liver injury, AST levels usually peak before those of ALT because of the enzyme’s peculiar intralobular distribution 32. Zone 3 of the acinus is more vulnerable to both hypoxic (hepatocytes are exposed to an already oxygen-poor milieu) and toxic (hepatocytes are richer in microsomal enzymes) damage. Furthermore, in ischemic injury aminotransferase levels tend to decrease rapidly after peaking (Figure 2). In about 80% of patients with ischemic injury, the serum bilirubin level is lower than 34 μmol/L, and lactate dehydrogenase (LDH), a marker of ischemic damage, may reach very high concentrations (ALT/LDH ratio < 1) 33. It is important to stress that a decrease in aminotransferase levels alone after a marked increase does not have prognostic meaning, since both resolution and massive hepatic necrosis may draw a similar biochemical picture. In this setting, patients with high bilirubin serum levels and prolonged prothrombin time should be closely monitored for the risk of hepatic failure.
In cases of acute viral hepatitis, aminotransferase levels usually peak before jaundice appears and have a more gradual decrease thereafter, and there is a greater increase in serum bilirubin levels (Figure 2) 34. Jaundice occurs in about 70% of cases of acute hepatitis A infection, 33%–50% of cases of acute hepatitis B infection and 20%–33% of cases of acute hepatitis C infection 4. Lactate dehydrogenase (LDH) concentration is altered in about 50% of the patients, with values typically only slightly above the reference limit 35. The entire alphabet of viral hepatitis (A, B, C, D and E) may be responsible for a marked increase in aminotransferase levels, although the increase associated with hepatitis C infection tends to be more modest than that associated with hepatitis A or B 36. Patients with acute viral hepatitis may lack a history of exposure to risk factors and may have nonspecific (fatigue, arthralgias, low-grade fever) or specific (jaundice) symptoms of liver disease; the diagnosis may be made following routine analysis with asymptomatic hypertransaminasemia. The presence of symptoms is more common in patients with acute hepatitis A (70%–80% of infected adults) or B (30%–50% of infected adults) infection than in patients with acute hepatitis C (20% of patients) infection 37. Obviously, the presence of risk factors such as travel to areas endemic for viral hepatitis or parenteral exposure may help identify the cause and should drive the subsequent investigation. Patients with suspected acute viral hepatitis should be tested for IgM antibodies to hepatitis A and hepatitus B core virus, hepatitis B surface antigens and hepatitis C virus (HCV) antibodies. Testing for hepatitis D infection should be limited to patients with evidence of hepatitis B surface antigens. If test results for HCV antibodies are negative and there is no evidence of acute hepatitis A or B infection, testing for HCV RNA may be a useful strategy since a recent study has demonstrated that, although these patients are rarely at risk of acute liver failure, they may benefit from early antiviral treatment 38.
Ischemic and hypoxic acute liver damage is more likely in patients with concomitant clinical conditions such as sepsis or low-flow hemodynamic state 33. Careful investigation of the patient’s pharmacologic history is essential in order to identify medications and herbal products associated with hepatotoxicity 39. Acetaminophen-induced hepatic damage causes 54% and 16% of the cases of acute liver failure in the United Kingdom and United States respectively 40. Although ischemic damage can be suspected on a clinical basis alone, and the patient history may suggest drug- or toxin-induced liver damage, there are no specific serologic tests for either condition, except in the case of acetaminophen poisoning, in which plasma acetaminophen levels may also represent a helpful guide to therapy. Alcohol-induced acute hepatic damage represents a distinct situation. It can be encountered in clinical practice both as acute and as acute-on-chronic liver injury. The biochemical picture is characteristic (e.g., GGT/ALP ratio > 2.5; jaundice may occur in more than 60% of patients 41. In a landmark study by Cohen and Kaplan, the increase in AST levels was less than 6–7 times the upper reference value in 98% of the patients with alcoholic liver disease, and the AST/ALT ratio was greater than 1 in 92% and greater than 2 in 70% of the patients 42. The presence of physical signs of chronic liver disease and the patient’s history may help distinguish between acute and acute-on-chronic damage.
After the most common causes of acute liver injury have been excluded, consideration should be given to minor hepatitis viruses (e.g., Epstein–Barr virus, cytomegalovirus) and to autoimmune, extrahepatic and congenital causes 43. Autoimmune hepatitis may present with a mild increase in aminotransferase levels or with a moderate to marked increase in aminotransferase levels (up to 49% of patients) with jaundice 44. Finally, as many as 25% of the patients with AST levels greater than 10 times the upper reference limit may have acute extrahepatic biliary tract obstruction, which can be heralded by a peak in aminotransferase levels (> 50 times the upper reference value in 1%–2% of patients) that rapidly subsides once the obstruction has been removed 27. The patient’s history, presence of symptoms such as biliary pain and the ultrasound evidence of dilated bile ducts can provide a definitive diagnosis.
Cholestatic (Bile flow problem) predominance
Presentation of liver injury with a prevalent cholestatic pattern is less frequently encountered in clinical practice than the pattern of hepatocellular damage. ALP and bilirubin levels are routinely assessed, and the level of GGT is often measured as an additional aid toward diagnosis in particular situations because of its high sensitivity but low specificity.
Alkaline phosphatase (ALP)
ALP is an enzyme that transports metabolites across cell membranes. Liver and bone diseases are the most common causes of pathological elevation of ALP levels, although ALP may originate from other tissue, such as the placenta, kidneys or intestines, or from leukocytes 45. The third trimester of pregnancy (placenta origin) and adolescence (bone origin) are associated with an isolated increase in serum ALP levels 5. Hepatic ALP is present on the surface of bile duct epithelia. Cholestasis enhances the synthesis and release of ALP, and accumulating bile salts increase its release from the cell surface 46. ALP half-life in the circulation is about 1 week 5. These characteristics explain why ALP levels usually rise late in bile duct obstruction and decrease slowly after resolution.
In some patients (e.g., pregnant women, adolescents) the reason for increased ALP levels may be straightforward, but in other patients it is necessary to identify the origin of the enzyme. This task can be accomplished in 2 ways: assessment of GGT levels or dosage of ALP isoenzymes. From a practical point of view, measurement of GGT is preferred since it relies on automated analysis rather than on more sophisticated and expensive techniques.
The degree and rate of enzyme alteration may provide minor and nonspecific clues to diagnosis, but the presence of symptoms and the patient’s history, with particular emphasis on comorbid conditions, may provide fundamental clues. Liver ultrasound may reveal the presence of bile duct dilation, demonstrate signs of chronic liver disease or even liver cirrhosis, and identify hepatic masses.
Drug-induced liver injury may present with a cholestatic pattern (preferential increase in ALP or ALT/ALP ratio < 2), although the degree of ALP alteration is variable and may be accompanied by hyperbilirubinemia.68 Commonly used drugs such as antihypertensives (e.g., angiotensin-converting enzyme inhibitors) or hormones (e.g., estrogen) may cause cholestasis and can be overlooked. Liver ultrasound in these patients is often unremarkable.
Varying degrees of ALP alteration in patients with inflammatory bowel disease (most commonly ulcerative colitis) suggest the presence of primary sclerosing cholangitis, since about 70% of these cases are associated with inflammatory bowel disease 47. The same biochemical abnormality observed in middle-aged women with a history of itching and autoimmune disease raises the suspicion of primary biliary cirrhosis 48. Further diagnostic work-up of patients with suspected autoimmune cholestatic liver disease includes testing antineutrophil cytoplasmic antibodies and cholangiography for primary sclerosing cholangitis and antimitochondria antibodies and total IgM levels for primary biliary cirrhosis. In these diseases, ALP and GGT levels may be slightly or markedly raised, whereas aminotransferase levels are often minimally altered or within the upper reference limit, unless overlapping features of autoimmune cholestatic diseases and autoimmune hepatitis occur 49. In patients with primary sclerosing cholangitis or primary biliary cirrhosis, serum bilirubin levels have prognostic meaning 50, and liver ultrasound may reveal an echotexture suggestive of diffuse disease or even liver cirrhosis.
ALP alteration due to common bile duct obstruction may be heralded by a peak in aminotransferase levels, typical symptoms and conjugated hyperbilirubinemia, especially in the acute setting, or the ALP levels may have a fluctuating pattern (± GGT alteration) with normal serum bilirubin in “valve” choledocholithiasis 51. In these patients, liver ultrasound may show dilated bile ducts, and endoscopic retrograde cholangiopancreatography can be used to remove the obstacle.
Abnormal ALP levels may also be a sign of metastatic cancer of the liver, lymphoma or infiltrative diseases such as sarcoidosis. In some of these situations ALP levels may be markedly elevated and the only sign of liver involvement. In these cases, liver ultrasound examination is extremely important when the patient history is not suggestive of disease, although some patients may require liver biopsy in order to obtain a definitive diagnosis 14.
The clinical work-up should help to establish a diagnosis in the majority of patients with elevated ALP levels. The degree of elevation seems to have no specific diagnostic relevance. Nevertheless, diagnosis may not be evident even after thorough evaluation in asymptomatic patients with mild increases in ALP levels. As mentioned above, liver biopsy can provide a fundamental clue to some unusual and unsuspected diagnoses.
γ-Glutamyl transpeptidase (GGT)
GGT is an enzyme that is present in hepatocytes and biliary epithelial cells, renal tubules, and the pancreas and intestine. The mechanisms of alteration are similar to those described for alkaline phosphatase. GGT is a microsomal enzyme, and its activity can be induced by several drugs, such as anticonvulsants and oral contraceptives 52. Elevated GGT levels can be observed in a variety of nonhepatic diseases, including chronic obstructive pulmonary disease and renal failure, and may be present for weeks after acute myocardial infarction. Increased serum levels observed in alcoholic liver disease can be the result of enzyme induction and decreased clearance. In these patients, GGT serum levels can be markedly altered (> 10 times the upper reference value), whereas ALP levels may be normal or only slightly altered (GGT/ALP ratio > 2.5). The whole spectrum of liver diseases, regardless of cause, may be responsible for altered GGT serum levels. In particular, GGT levels may be 2–3 times greater than the upper reference value in more than 50% of the patients with nonalcoholic fatty liver disease and above the upper reference value in about 30% of patients with chronic hepatitis C infection 53. Furthermore, an increase in GGT levels in patients with chronic liver disease is associated with bile duct damage and fibrosis 54. Thus, because of its lack of specificity but high sensitivity for liver disease, GGT can be useful for identifying causes of altered ALP levels, or elevated levels, together with other biochemical abnormalities (AST/ALT ratio > 2) 42, may support the diagnosis of alcoholic liver disease.
Bilirubin
Bilirubin is the product of hemoglobin catabolism within the reticuloendothelial system. Heme breakdown determines the formation of unconjugated bilirubin, which is then transported to the liver. In the liver, UDP-glucuronyltransferase conjugates the water-insoluble unconjugated bilirubin to glucuronic acid, and conjugated bilirubin is then excreted into the bile 55.
Table 4. Causes of elevated bilirubin
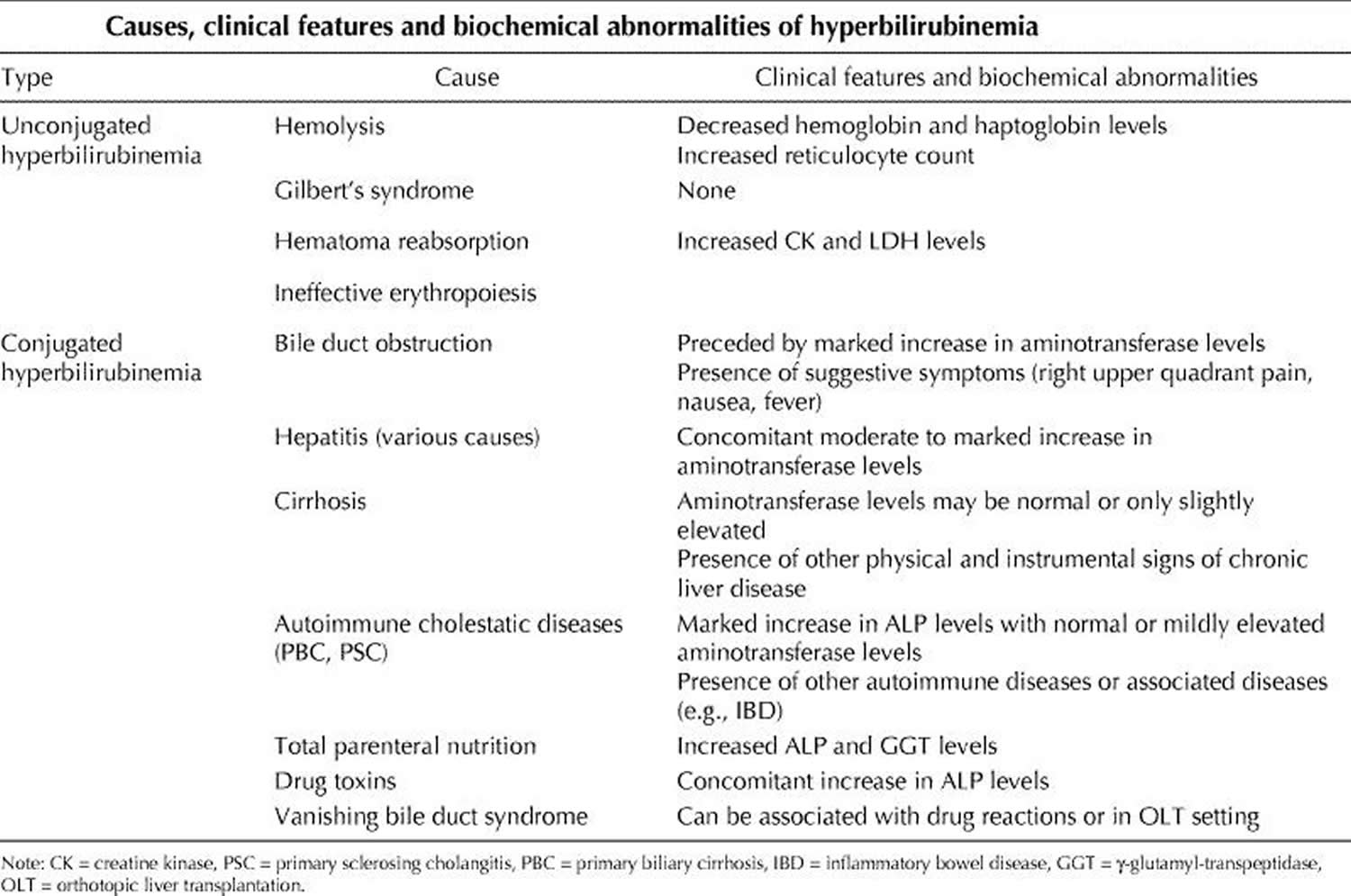
Unconjugated bilirubin may increase because of augmented bilirubin production or decreased hepatic uptake or conjugation or both (Table 4). In adults, the most common conditions associated with unconjugated hyperbilirubinemia are hemolysis and Gilbert’s syndrome 56. Hemolysis can be ruled out by measuring hemoglobin serum levels, reticulocyte count, and haptoglobin levels. Gilbert’s syndrome is determined by a variety of genetic defects in UDP-glucuronyltransferase that affect about 5% of the population 57. In these subjects serum indirect bilirubin usually does not exceed 68 μmol/L, and the remainder of liver chemistry tests and liver ultrasound are unremarkable 58. Although a series of tests has been proposed to confirm the diagnosis, this condition is usually diagnosed on a clinical basis alone, and the patient should be reassured of the benign nature of this enzymatic alteration 58. Other, less frequent causes of unconjugated hyperbilirubinemia include reabsorption of large hematomas and ineffective erythropoiesis 59.
In healthy people, conjugated bilirubin is virtually absent from serum mainly because of the rapid process of bile secretion 43. Levels increase when the liver has lost at least half of its excretory capacity. Therefore, the presence of increased conjugated bilirubin is usually a sign of liver disease. Conjugated hyperbilirubinemia (usually < 34 μmol/L) and concomitant, markedly elevated aminotransferase levels may suggest acute viral hepatitis or toxic or ischemic liver injury. Furthermore, this biochemical picture can be the presenting feature of autoimmune hepatitis 60. On the other hand, a purely cholestatic picture, with conjugated hyperbilirubinemia, an increase in ALP levels and a negligible increase in aminotransferase levels, may be present in cholestatic drug reactions 61. Sometimes, the same biochemical picture may be present in the late presentation of previously unrecognized autoimmune cholestatic diseases (primary biliary cirrhosis, primary sclerosing cholangitis). In these patients, the presence of other signs of chronic liver disease may facilitate diagnosis 48.
Biliary obstruction can cause various degrees of conjugated hyperbilirubinemia. The severity of alteration depends upon the degree and duraction of obstruction and the functional reserve of the liver. Biliary obstruction may have an abrupt onset and be preceded by typical symptoms (right upper quadrant pain, nausea) or may be silent and progressive. With the presence or absence of concomitant aminotransferase alteration, a liver ultrasound is essential to identify and locate the obstacle to bile flow.
Once the causal condition of conjugated hyperbilirubinemia has resolved, whatever the cause, bilirubin serum levels decrease in a bimodal fashion. There is a first, rapid decrease and then a later, slower decrease caused by the binding of bilirubin to albumin and the formation of a complex (δ-bilirubin) that has the same half-life as serum albumin 62.
Other liver function markers
Determining serum albumin levels and assessing prothrombin time are often considered “tests of liver function” 1. This is mainly because hepatic synthesis of albumin tends to decrease in end-stage liver disease, and an increase in prothrombin time depends on the decreased synthesis of liver-derived coagulation factors. In fact, albumin is produced by hepatocytes, and prothrombin time depends on the activity of clotting factors I, II, V, VII and X, which are produced in the liver. However, neither test is specific for liver disease, since albumin serum levels may decrease in patients with nephrotic syndrome, malabsorption or protein-losing enteropathy, or malnutrition, and prothrombin time may be prolonged by warfarin treatment, deficiency in vitamin K (which is needed to activate clotting factors II, VII and X) and consumptive coagulopathy 63. The finding of hypoalbuminemia and no other alterations in liver tests virtually rules out the hepatic origin of this abnormality.
However, when it is certain that the cause of their alteration is liver disease, serum albumin levels and prothrombin time are useful tests for monitoring liver synthetic activity 1. The half-life of albumin in circulation is long (about 20 days), and the half-life of blood clotting factors is quite short (about 1 day) 63. Thus, albumin levels decrease when cirrhosis occurs, and they have prognostic meaning in these patients. On the contrary, patients with acute, massive hepatocellular necrosis (acute toxic or viral hepatitis) may have a brisk increase in prothrombin time (usually < 3 seconds) that tends to plateau, and normal albuminemia. In these patients, prothrombin time can be monitored in order to assess the risk of acute liver failure. On the other hand, prothrombin time is not useful for assessing liver function in patients with mild aminotransferase alteration, since prothrombin time can remain within normal limits for long periods unless a marked decrease in liver function occurs and patients with compensated liver cirrhosis may have normal prothrombin time 62. Thus, it is evident from these data that albumin and prothrombin time alteration should be interpreted within the clinical and biochemical context of the patient.
Obstructive jaundice may decrease the absorption of vitamin K, and therefore increase prothrombin time. In this situation, prothrombin time responds to parenteral administration of vitamin K, which is ineffective when jaundice is caused by decreased liver functioning mass. Finally, prothrombin time values are strictly dependent upon the International Sensitivity Index of the reagent that is used, and this does not allow for easy standardization of results among laboratories. Taking these limitations into account, both serum albumin and prothrombin time can be considered useful tools, alone or combined in clinical scores, for evaluating liver function 64. Nevertheless, tests that involve administering exogenous compounds may be used to evaluate liver function more accurately 65.
- Giannini EG, Testa R, Savarino V. Liver enzyme alteration: a guide for clinicians. CMAJ : Canadian Medical Association Journal. 2005;172(3):367-379. doi:10.1503/cmaj.1040752. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC545762/[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Gholson CF, Morgan K, Catinis G, Favrot D, Taylor B, Gonzalez E, et al. Chronic hepatitis C with normal aminotransferase levels: a clinical histologic study. Am J Gastroenterol 1997;92(10):1788-92. https://www.ncbi.nlm.nih.gov/pubmed/9382037[↩]
- Mofrad P, Contos MJ, Haque M, Sargeant C, Fisher RA, Luketic VA, et al. Clinical and histologic spectrum of nonalcoholic fatty liver disease associated with normal ALT values. Hepatology 2003;37(6):1286-92. https://www.ncbi.nlm.nih.gov/pubmed/12774006[↩]
- Dufour DR, Lott JA, Nolte FS, Gretch DR, Koff RS, Seeff LB. Diagnosis and monitoring of hepatic injury. II. Recommendations for use of laboratory tests in screening, diagnosis, and monitoring. Clin Chem 2000;46(12):2050-68. http://clinchem.aaccjnls.org/content/46/12/2050.long[↩][↩]
- Dufour DR, Lott JA, Nolte FS, Gretch DR, Koff RS, Seeff LB. Diagnosis and monitoring of hepatic injury. I. Performance characteristics of laboratory tests. Clin Chem 2000;46(12):2027-49. http://clinchem.aaccjnls.org/content/46/12/2027.long[↩][↩][↩][↩][↩]
- Dufour DR. Effects of habitual exercise on routine laboratory tests [abstract]. Clin Chem 1998;44 (Suppl 6):A136.[↩]
- Narjes H, Nehmiz G. Effect of hospitalisation on liver enzymes in healthy subjects. Eur J Clin Pharmacol 2000;56(4):329-33. https://www.ncbi.nlm.nih.gov/pubmed/10954348[↩]
- Elevated liver enzymes. Mayo Clinic. http://www.mayoclinic.org/symptoms/elevated-liver-enzymes/basics/definition/sym-20050830[↩]
- Vanderlinde RE. Review of pyridoxal phosphate and the transaminases in liver disease. Ann Clin Lab Sci 1986;16(2):79-93. https://www.ncbi.nlm.nih.gov/pubmed/3008634[↩]
- Diehl AM, Potter J, Boitnott J, Van Duyn MA, Herlong HF, Mezey E. Relationship between pyridoxal 5′-phosphate deficiency and aminotransferase levels in alcoholic hepatitis. Gastroenterology 1984;86(4):632-6. https://www.ncbi.nlm.nih.gov/pubmed/6698365[↩]
- Wroblewski F. The clinical significance of alterations in transaminase activities of serum and other body fluids. Adv Clin Chem 1958;1(2):313-51. https://www.ncbi.nlm.nih.gov/pubmed/13571034[↩]
- Rej R. Aminotransferases in disease. Clin Lab Med 1989;9(4):667-87. https://www.ncbi.nlm.nih.gov/pubmed/2686908[↩]
- Kamimoto Y, Horiuchi S, Tanase S, Morino Y. Plasma clearance of intravenously injected aspartate aminotransferase isozymes: evidence for preferential uptake by sinusoidal liver cells. Hepatology 1985;5(3):367-75. https://www.ncbi.nlm.nih.gov/pubmed/3997068[↩]
- Gopal DV, Rosen HR. Abnormal findings on liver function tests. Postgrad Med 2000;107(2):100-14. https://www.ncbi.nlm.nih.gov/pubmed/10689411[↩][↩]
- Aithal GP, Rawlins MD, Day CP. Clinical diagnostic scale: a useful tool in the evaluation of suspected hepatotoxic adverse drug reactions. J Hepatol 2000;33(6);949-52. https://www.ncbi.nlm.nih.gov/pubmed/11131457[↩]
- Harrison SA, Kadakia S, Lang KA, Schenker S. Nonalcoholic steatohepatitis: what we know in the new millenium. Am J Gastroenterol 2002;97(11):2714-24. https://www.ncbi.nlm.nih.gov/pubmed/12425538[↩][↩]
- Brunt EM. Nonalcoholic steatohepatitis. Semin Liver Dis 2004;24(1):3-20. https://www.ncbi.nlm.nih.gov/pubmed/15085483[↩]
- Angulo P, Keach JC, Batts KP, Lindor KD. Independent predictors of liver fibrosis in patients with nonalcoholic steatohepatitis. Hepatology 1999; 30 (6): 1356-62. https://www.ncbi.nlm.nih.gov/pubmed/10573511[↩]
- Matteoni CA, Younossi ZM, Gramlich T, Boparai N, Liu YC, Mc-Cullogh AJ. Nonalcoholic fatty liver disease: a spectrum of clinical and pathological severity. Gastroenterology 1999;116(6):1413-9. https://www.ncbi.nlm.nih.gov/pubmed/10348825[↩]
- The Global Burden Of Hepatitis C Working Group. Global burden of disease (GBD) for hepatitis C. J Clin Pharmacol 2004;44 (1):20-9. https://www.ncbi.nlm.nih.gov/pubmed/14681338[↩]
- Memon MI, Memon MA. Hepatitis C: An epidemiological review. J Viral Hepat 2002;9(2):84-100. https://www.ncbi.nlm.nih.gov/pubmed/11876790[↩]
- Giannini E, Botta F, Testa E, Romagnoli P, Polegato S, Malfatti F, et al. The 1-year and 3-month prognostic utility of the AST/ALT ratio and model for end-stage liver disease score in patients with viral liver cirrhosis. Am J Gastroenterol 2002;97(11):2855-60. https://www.ncbi.nlm.nih.gov/pubmed/12425560[↩][↩]
- Giannini E, Botta F, Fasoli A, Ceppa P, Risso D, Lantieri PB, et al. Progressive liver functional impairment is associated with an increase in AST/ALT ratio. Dig Dis Sci 1999;44(6):1249-53. https://www.ncbi.nlm.nih.gov/pubmed/10389705[↩]
- Merryweather-Clarke AT, Pointon JJ, Shearman JD, Robson KJ. Global prevalence of putative haemochromatosis mutations. Journal of Medical Genetics. 1997;34(4):275-278. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1050911/[↩][↩]
- Tavill AS. Diagnosis and management of Hemochromatosis. Hepatology 2001; 33 (5):1321-8. https://www.ncbi.nlm.nih.gov/pubmed/11343262[↩][↩]
- Czaja AJ. Natural history, clinical features, and treatment of autoimmune hepatitis. Semin Liver Dis 1984;4(1):1-12. https://www.ncbi.nlm.nih.gov/pubmed/6710168[↩][↩][↩]
- Ferenci P, Caca K, Loudianos G, Mieli-Vergani G, Tanner S, Sternlieb I, et al. Diagnosis and phenotypic classification of Wilson disease. Liver Int 2003; 23 (3):139-42. https://www.ncbi.nlm.nih.gov/pubmed/12955875[↩][↩]
- Morrison ED, Kowdley KV. Genetic liver disease in adults: early recognition of the three most common causes. Postgrad Med 2000;107(2):147-59. https://www.ncbi.nlm.nih.gov/pubmed/10689414[↩]
- Abdo A, Meddings J, Swain M. Liver abnormalities in celiac disease. Clin Gastroenterol Hepatol 2004;2(2):107-12. https://www.ncbi.nlm.nih.gov/pubmed/15017614[↩]
- Farrell RJ, Kelly CP. Diagnosis of celiac sprue. Am J Gastroenterol 2001; 96 (12): 3237-46. https://www.ncbi.nlm.nih.gov/pubmed/11774931[↩]
- Rozen P, Korn RJ, Zimmerman HJ. Computer analysis of liver function tests and their interrelationship in 347 cases of viral hepatitis. Isr Med Sci 1970; 6 (1): 67 -79. https://www.ncbi.nlm.nih.gov/pubmed/5509868[↩]
- Singer AJ, Carracio TR, Mofenson HC. The temporal profile of increased transaminase levels in patients with acetaminophen-induced liver dysfunction. Ann Emerg Med 1995;26(1):49-53. https://www.ncbi.nlm.nih.gov/pubmed/7793720[↩]
- Fuchs S, Bogomolski-Yahalom V, Paltiel O, Ackerman Z. Ischemic hepatitis: clinical and laboratory observations of 34 patients. J Clin Gastroenterol 1998; 26 (3):183-6. https://www.ncbi.nlm.nih.gov/pubmed/9600366[↩][↩]
- Clermont RJ, Chalmers TC. The transaminase tests in liver disease. Medicine 1967; 46(2):197-207. https://www.ncbi.nlm.nih.gov/pubmed/5338702[↩]
- Seeto RK, Fenn B, Rockey DC. Ischemic hepatitis: clinical presentation and pathogenesis. Am J Med 2000;109(2):109-13. https://www.ncbi.nlm.nih.gov/pubmed/10967151[↩]
- Marcellin P. Hepatitis C: the clinical spectrum of the disease. J Hepatol 1999; 31 (Suppl 1):9-16. https://www.ncbi.nlm.nih.gov/pubmed/10622554[↩]
- Geller SA. Hepatitis B and hepatitis C. Clin Liver Dis 2002;6(2):317-34. https://www.ncbi.nlm.nih.gov/pubmed/12122858[↩]
- Wedemeyer H, Jackel E, Wiegand J, Cornberg M, Manns MP. Whom? When? How? Another piece of evidence for early treatment of acute hepatitis C. Hepatology 2004;39(5):1201-3. https://www.ncbi.nlm.nih.gov/pubmed/15122747[↩]
- Shad JA, Chinn CG, Brann OS. Acute hepatitis after ingestion of herbs. South Med J 1999;92(11):1095-7. https://www.ncbi.nlm.nih.gov/pubmed/10586838[↩]
- O’Grady JG. Acute liver failure. In: Comprehensive Clinical Hepatology. O’Grady JG, Lake JR, Howdle PD, editors. Mosby:London, 2000. p. 16.1-16.13.[↩]
- Goldberg S, Mendenhall C, Anderson S, Garcia-Pont P, Kiernan T, Seeff L, et al. VA Cooperative Study on Alcoholic Hepatitis. IV. The significance of clinically mild alcoholic hepatitis-describing the population with minimal hyperbilirubinemia. Am J Gastroenterol 1986;81(11):1029-34. https://www.ncbi.nlm.nih.gov/pubmed/3776948[↩]
- Cohen JA, Kaplan MM. The SGOT/SGPT ratio — an indicator of alcoholic liver disease. Dig Dis Sci 1979;24(11):835-8. https://www.ncbi.nlm.nih.gov/pubmed/520102[↩][↩]
- Green RM, Flamm S. AGA technical review on the evaluation of liver chemistry tests. Gastroenterology 2002;123(4):1367-84. https://www.ncbi.nlm.nih.gov/pubmed/12360498[↩][↩]
- Kessler WR, Cummings OW, Eckert G, Chalasani N, Lumeng L, Kuo PY. Fulminant hepatic failure as the initial presentation of acute autoimmune hepatitis. Clin Gastroenterol Hepatol 2004;2(7):625-31. https://www.ncbi.nlm.nih.gov/pubmed/15224287[↩]
- Fishman WH. Alkaline phosphatase isoenzymes: recent progress. Clin Biochem 1990;23(2):99-104. https://www.ncbi.nlm.nih.gov/pubmed/2197029[↩]
- Moss DW. Physiochemical and pathophysiological factors in the release of membrane-bound alkaline phosphatase from cells. Clin Chim Acta 1997; 257 (1): 133-40. https://www.ncbi.nlm.nih.gov/pubmed/9028630[↩]
- Ponsioen CI, Tytgat GN. Primary sclerosing cholangitis: a clinical review. Am J Gastroenterol 1998;93(4):515-23. https://www.ncbi.nlm.nih.gov/pubmed/9576440[↩]
- Heathcote J. Update on primary biliary cirrhosis. Can J Gastroenterol 2000; 14 (1): 43-8. https://www.ncbi.nlm.nih.gov/pubmed/10655026[↩][↩]
- Poupon R. Autoimmune overlapping syndromes. Clin Liver Dis 2003; 7 (4): 865-78. https://www.ncbi.nlm.nih.gov/pubmed/14594134[↩]
- Kim WR, Therneau TM, Wiesner RH, Poterucha JJ, Benson JT, Malinchoc M, et al. A revised natural history model for primary sclerosing cholangitis. Mayo Clin Proc 2000;75(7):688-94. https://www.ncbi.nlm.nih.gov/pubmed/10907383[↩]
- Anciaux ML, Pelletier AG, Attali P, Meduri B, Liguory C, Etienne JP. Prospective study of clinical and biochemical features of symptomatic choledocolithiasis. Dig Dis Sci 1986;31:449-53. https://www.ncbi.nlm.nih.gov/pubmed/2870885[↩]
- Rosalki SB, Tarlow D, Rau D. Plasma gamma-glutamyl transpeptidase elevation in patients receiving enzyme-inducing drugs. Lancet 1971;2:376-7. https://www.ncbi.nlm.nih.gov/pubmed/4105075[↩]
- McCullough AJ. Update on nonalcoholic fatty liver disease. J Clin Gastroenterol 2002;34(3):255-62. https://www.ncbi.nlm.nih.gov/pubmed/11873108[↩]
- Giannini E, Botta F, Fasoli A, Romagnoli P, Mastracci L, Ceppa P, et al. Increased levels of gammaGT suggest the presence of bile duct lesions in patients with chronic hepatitis C: absence of influence of HCV genotype, HCV-RNA serum levels, and HGV infection on this histological damage. Dig Dis Sci 2001;46(3):524-9. https://www.ncbi.nlm.nih.gov/pubmed/11318526[↩]
- Berk PD, Noyer C. Clinical chemistry and physiology of bilirubin. Semin Liver Dis 1994; 4(4):346-55.[↩]
- Fevery J, Blanckaert N. What can we learn from analysis of serum bilirubin. J Hepatol 1986;2(1):113-21. https://www.ncbi.nlm.nih.gov/pubmed/3081621[↩]
- Bosma PJ, Chowdury JR, Bakker C, Gantla S, de Boer A, Oostra BA, et al. The genetic bases of the reduced expression of bilirubin UDP-glucuronosyltransferase 1 in Gilbert’s syndrome. N Engl J Med 1995;333(18):1171-5. https://www.ncbi.nlm.nih.gov/pubmed/7565971[↩]
- Thomsen HF, Hardt F, Juhl E. Diagnosis of Gilbert’s syndrome. Scand J Gastroenterol 1981;16(5):699-703. https://www.ncbi.nlm.nih.gov/pubmed/7323703[↩][↩]
- Pratt DS, Kaplan MM. Evaluation of abnormal liver-enzyme results in asymptomatic patients. N Engl J Med 2000;342(17): 1266-71. https://www.ncbi.nlm.nih.gov/pubmed/10781624[↩]
- Alvarez F, Berg PA, Bianchi FB, Bianchi L, Burroughs AK, Cancado EL, et al. International Autoimmune Hepatitis Group Report: review of criteria for diagnosis of autoimmune hepatitis. J Hepatol 1999;31(5):929-38. https://www.ncbi.nlm.nih.gov/pubmed/10580593[↩]
- Velayudham LS, Farrell GC. Drug-induced cholestasis. Expert Opin Drug Saf 2003;2(3):287-304. https://www.ncbi.nlm.nih.gov/pubmed/12904107[↩]
- Van Hootegem P, Fevery J, Blanckaert N. Serum bilirubins in hepatobiliary disease: comparison with other liver function tests and changes in the postobstructive period. Hepatology 1985;5(1):112-7. https://www.ncbi.nlm.nih.gov/pubmed/3967852[↩][↩]
- Doumas BT, Peters T. Serum and urine albumin: a progress report on their measurement and clinical significance. Clin Chim Acta 1997;258(1):3-20. https://www.ncbi.nlm.nih.gov/pubmed/9049439[↩][↩]
- Botta F, Giannini E, Romagnoli P, et al. MELD scoring system is useful for predicting prognosis in patients with liver cirrhosis and is correlated with residual liver function: a European study. Gut. 2003;52(1):134-139. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1773509/[↩]
- Jalan R, Hayes PC. Review article: quantitative tests of liver function. Aliment Pharmacol Ther 1995;9(3):263-70. https://www.ncbi.nlm.nih.gov/pubmed/7654888[↩]





{kind=link}