
Contents
- What is lyme disease
- Can Lyme disease be prevented or avoided ?
- Is Lyme disease contagious
- Untreated Lyme disease signs and symptoms
- How is Lyme disease diagnosed ?
- Lyme disease treatment
- I am pregnant and just found out I have Lyme disease. What should I do ?
- Where can I get a test to make sure that I am cured ?
- I heard that if I get Lyme disease I will always have it. Is that true ?
- If I have been diagnosed with Lyme disease, do I need to get tested for other tickborne diseases (coinfections) ?
- What is Chronic Lyme Disease ?
What is lyme disease
Lyme disease is a bacterial (Borrelia burgdorferi) infection that is spread by black-legged ticks (sometimes called deer ticks) 1. It was first recognized in 1975. Large numbers of children around the town of Lyme, Connecticut, were being diagnosed with juvenile rheumatoid arthritis. Researchers investigated and found that tick bites were causing the illnesses.
Lyme disease, is the most common tick-borne illness in the United States. Many types of ticks bite people in the U.S., but only blacklegged ticks transmit the bacteria that cause Lyme disease 2. Furthermore, only blacklegged ticks in the highly endemic areas of the northeastern and north central U.S. are commonly infected 2. Finally, blacklegged ticks need to be attached for at least 24 hours before they can transmit Lyme disease, but in most cases, the tick must be attached for 36 to 48 hours or more before the Lyme disease bacterium can be transmitted 3. This is why it’s so important to remove them promptly and to check your body daily for ticks if you live in an endemic area.
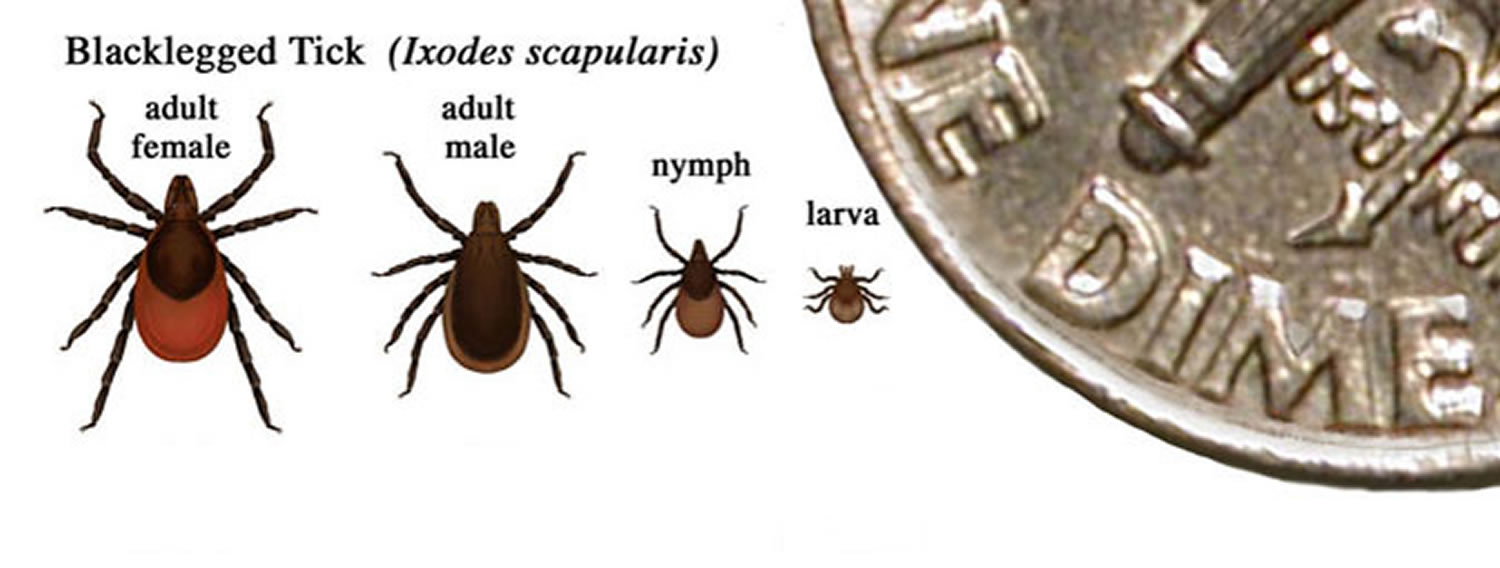
Figure 1. Blacklegged tick (Ixodes scapularis)

The Lyme disease ticks can attach to any part of the human body but are often found in hard-to-see areas such as the groin, armpits, and scalp. Most humans are infected through the bites of immature ticks called nymphs. Nymphs are tiny (less than 2 mm) and difficult to see; they feed during the spring and summer months. Adult ticks can also transmit Lyme disease bacteria, but they are much larger and are more likely to be discovered and removed before they have had time to transmit the bacteria. Adult Ixodes ticks are most active during the cooler months of the year. In general, adult ticks are approximately the size of a sesame seed and nymphal ticks are approximately the size of a poppy seed.
Figure 2. Relative sizes of blacklegged ticks at different life stages
Each year, approximately 30,000 cases of Lyme disease are reported to CDC by state health departments and the District of Columbia and around 300,000 in the United States 4. However, this number does not reflect every case of Lyme disease that is diagnosed in the United States every year.
These ticks are typically about the size of a sesame seed. They live only in certain areas of the country:
- Northeast and mid-Atlantic (northeast Virginia to Maine)
- North central states (mostly Wisconsin and Minnesota)
- West Coast (mostly northern California)
Lyme disease can also be found in other parts of the United States. But it is rare to get it outside of where the black-legged tick lives. The disease is also found in Europe, Asia, and Australia.
Is it true that you can get Lyme disease anywhere in the U.S. ?
No. Lyme disease is spread through the bite of a blacklegged tick (Ixodes scapularis or Ixodes pacificus) that is infected with Borrelia burgdorferi. In the United States, most infections occur in the following endemic areas:
- Northeast and mid-Atlantic, from northeastern Virginia to Maine
- North central states, mostly in Wisconsin and Minnesota
- West Coast, particularly northern California
Maps showing the distribution of human cases are based on where people live, which because of travel, is not necessarily where they became infected. Cases are sometimes diagnosed and reported from an area where Lyme disease is not expected, but they are almost always travel-related.
Most people with Lyme disease develop a characteristic skin rash around the area of the bite. The rash may feel hot to touch and vary in size, shape, and color, but it will often have a “bull’s eye” appearance (a red ring with a clear center) 5. However, there are those who will not develop the rash, which can make Lyme disease hard to diagnose because its symptoms and signs mimic those of many other diseases 5.
Figure 3. Bull’s eye rash of Lyme disease (Erythema migrans rash)

Figure 4. Expanding Lyme disease rash with central crust

Figure 5. Multiple rashes of Lyme disease

Figure 6. Lyme disease rash – bluish rash with no central clearing

Figure 7. Lyme disease red-blue rash with central clearing

Anywhere from 7 to 14 days (or in some cases, 30 days) following an infected tick’s bite, the first stage of Lyme disease may begin with flu-like symptoms such as fever, chills, swollen lymph nodes, headaches, fatigue, muscle aches, and joint pain.
Neurological complications most often occur in the second stage of Lyme disease, with numbness, pain, weakness, Bell’s palsy (paralysis of the facial muscles), visual disturbances, and meningitis symptoms such as fever, stiff neck, and severe headache. Other problems, which may not appear until weeks, months, or years after a tick bite, include decreased concentration, irritability, memory and sleep disorders, and nerve damage in the arms and legs.
Most individuals with Lyme disease respond well to antibiotics and have full recovery. Early-stage Lyme disease responds very well to treatment. In most cases, taking an antibiotic for 2 to 4 weeks kills the bacteria and clears up the infection. Your doctor will tell you how long to take the antibiotic. It’s important to take all the medicine your doctor prescribes. This will prevent the spread of Lyme disease to your joints, nervous system, or heart. If you have problems with the medicine, do not quit taking it. See your doctor and talk to him or her about your side effects.
In a small percentage of individuals, symptoms may continue or recur, requiring additional antibiotic treatment. Varying degrees of permanent joint or nervous system damage may develop in individuals with late-stage Lyme disease.
Late-stage Lyme disease is also treated with antibiotics 1. It may be necessary to give the antibiotics intravenously (through an IV) at this stage. Medicine that reduces swelling and pain can ease arthritis associated with late-stage Lyme disease. If necessary, excess fluid can be drained from any affected joints.
Can Lyme disease be prevented or avoided ?
The best way to prevent Lyme disease is to avoid being bitten by ticks. When you are outdoors, follow these guidelines:
- Avoid areas that are wooded, brushy, or have tall grass.
- Walk in the center of trails.
- Use an insect repellent with at least 20% DEET. It can be put on clothing or sparingly on the skin. Don’t apply it to the face or hands of children.
- Treat clothing, tents, or other gear with repellents containing 0.5% permethrin.
- Wear light-colored clothing. This makes it easier to see and remove ticks from your clothes.
- Wear a long-sleeved shirt and long pants. Tuck your pant legs into your socks or boots for added protection.
After you get home, check everything and everyone for ticks.
- Bathe or shower as soon as you can to wash off any ticks that have not attached to you.
- Check your entire body for ticks. Use a mirror for places you can’t see. Check your children and your pets. Common tick locations include the back of the knees, groin area, underarms, ears, scalp, and the back of the neck.
- Check any gear you used, including coats, backpacks, or tents.
- Tumble dry clothes or blankets on high heat in the dryer for 10 to 15 minutes. This should kill any ticks. If clothes are dirty, wash them in hot water and dry on high heat for 60 minutes.
What to do if you find a tick on your skin ?
Don’t panic. Use fine-tipped tweezers to grasp the tick as close to the skin’s surface as possible. Pull up with steady, even pressure. Be careful not to squeeze or twist the tick body. Sometimes parts of the tick remain in the skin. You can leave them alone or carefully remove them the same way you would a splinter. Do not use heat (such as a lit match), petroleum jelly, or other methods to try to make the tick “back out” on its own. These methods are not effective.
- Your goal is to remove the tick as quickly as possible–do not wait for it to detach.
Wash the area where the tick was attached thoroughly with soap and water. Keep an eye on the area for a few weeks and note any changes. Call your doctor if you develop a rash around the area where the tick was attached. Be sure to tell your doctor that you were bitten by a tick and when it happened.
I live in the southeastern U.S. and get a lot of lone star tick bites. Can you can get “southern Lyme disease” ?
The lone star tick is primarily found in the southeastern and eastern United States. Lone star ticks do not transmit Lyme disease. However, you are correct to be concerned about this very aggressive species. The lone star tick (Amblyomma americanum) can spread human ehrlichiosis, tularemia, and Southern Tick-Associated Rash Illness.
The rash of Southern Tick-Associated Rash Illness is a red, expanding “bull’ s eye” lesion that develops around the site of a lone star tick bite. The rash usually appears within seven days of tick bite and expands to a diameter of 8 centimeters (3 inches) or more. The rash should not be confused with much smaller areas of redness and discomfort that can occur commonly at tick bite sites. Unlike Lyme disease, Southern Tick-Associated Rash Illness has not been linked to arthritis, neurological problems, or chronic symptoms. Nevertheless, the similarity between the Southern Tick-Associated Rash Illness bull’s eye rash and the Lyme disease bull’s eye rash has created much public confusion. The pathogen responsible for Southern Tick-Associated Rash Illness has not been identified.
In contrast, Lyme disease in North America is caused by a specific type of bacteria, Borrelia burgdorferi, which is transmitted by two species of blacklegged ticks, Ixodes scapularis and Ixodes pacificus. While blacklegged ticks exist in the southern U.S., their feeding habits in this region make them much less likely to maintain, sustain, and transmit Lyme disease.
Is Lyme disease contagious
- There is no evidence that Lyme disease is transmitted from person-to-person. For example, a person cannot get infected from touching, kissing, or having sex with a person who has Lyme disease.
- Lyme disease acquired during pregnancy may lead to infection of the placenta and possible stillbirth; however, no negative effects on the fetus have been found when the mother receives appropriate antibiotic treatment. There are no reports of Lyme disease transmission from breast milk.
- Although no cases of Lyme disease have been linked to blood transfusion, scientists have found that the Lyme disease bacteria can live in blood that is stored for donation. Individuals being treated for Lyme disease with an antibiotic should not donate blood. Individuals who have completed antibiotic treatment for Lyme disease may be considered as potential blood donors.
- Although dogs and cats can get Lyme disease, there is no evidence that they spread the disease directly to their owners. However, pets can bring infected ticks into your home or yard. Consider protecting your pet, and possibly yourself, through the use of tick control products for animals.
- You will not get Lyme disease from eating venison or squirrel meat, but in keeping with general food safety principles, always cook meat thoroughly. Note that hunting and dressing deer or squirrels may bring you into close contact with infected ticks.
- There is no credible evidence that Lyme disease can be transmitted through air, food, water, or from the bites of mosquitoes, flies, fleas, or lice.
- Ticks not known to transmit Lyme disease include Lone star ticks (Amblyomma americanum), the American dog tick (Dermacentor variabilis), the Rocky Mountain wood tick (Dermacentor andersoni), and the brown dog tick (Rhipicephalus sanguineus).
Can Lyme disease be transmitted sexually ?
There is no credible scientific evidence that Lyme disease is spread through sexual contact. Published studies in animals do not support sexual transmission 6, and the biology of the Lyme disease spirochete is not compatible this route of exposure 7. The ticks that transmit Lyme disease are very small and easily overlooked. Consequently, it is possible for sexual partners living in the same household to both become infected through tick bites, even if one or both partners doesn’t remember being bitten.
Can Lyme disease be transmitted through breast milk ?
There are no reports of Lyme disease being spread to infants through breast milk. If you are diagnosed with Lyme disease and are also breastfeeding, make sure that your doctor knows this so that he or she can prescribe an antibiotic that’s safe for use when breastfeeding.
Can Lyme disease be transmitted during a blood transfusion ?
Although no cases of Lyme disease have been linked to blood transfusion, scientists have found that the Lyme disease bacteria can live in blood from a person with an active infection that is stored for donation. Individuals being treated for Lyme disease with an antibiotic should not donate blood. Individuals who have completed antibiotic treatment for Lyme disease may be considered as potential blood donors. The Red Cross 8 provides additional information on the most recent criteria for blood donation.
Untreated Lyme disease signs and symptoms
Untreated Lyme disease can produce a wide range of symptoms, depending on the stage of infection. These include fever, rash, facial paralysis, and arthritis. Seek medical attention if you observe any of these symptoms and have had a tick bite, live in an area known for Lyme disease, or have recently traveled to an area where Lyme disease occurs.
Early Signs and Symptoms (3 to 30 days after tick bite)
- Fever, chills, headache, fatigue, muscle and joint aches, and swollen lymph nodes
Erythema migrans rash:
- Occurs in approximately 70 to 80 percent of infected persons
- Begins at the site of a tick bite after a delay of 3 to 30 days (average is about 7 days)
- Expands gradually over a period of days reaching up to 12 inches or more (30 cm) across
- May feel warm to the touch but is rarely itchy or painful
- Sometimes clears as it enlarges, resulting in a target or “bull’s-eye” appearance
- May appear on any area of the body.
Later Signs and Symptoms (days to months after tick bite)
- Severe headaches and neck stiffness
- Additional erythema migrans rashes on other areas of the body
- Arthritis with severe joint pain and swelling, particularly the knees and other large joints.
- Facial palsy (loss of muscle tone or droop on one or both sides of the face) – Bell’s palsy
- Intermittent pain in tendons, muscles, joints, and bones
- Heart palpitations or an irregular heart beat (Lyme carditis)
- Episodes of dizziness or shortness of breath
- Inflammation of the brain and spinal cord
- Nerve pain
- Shooting pains, numbness, or tingling in the hands or feet
- Problems with short-term memory.
Lyme disease can progress to a late stage months to years after the initial tick bite, which may result in substantial morbidity, primarily from chronic arthritis 9. These complications are distinct from what have recently been named “post–Lyme disease syndrome,” which refers to the nonspecific symptoms (e.g., fatigue) that may persist after successful treatment, and “chronic Lyme disease,” which refers more broadly to chronic symptoms occurring in patients who may or may not have Lyme disease 10.
What is Lyme carditis ?
Lyme carditis occurs when Lyme disease bacteria enter the tissues of the heart 11. This can interfere with the normal movement of electrical signals from the heart’s upper to lower chambers, a process that coordinates the beating of the heart. The result is something physicians call “heart block,” which can be mild, moderate, or severe. Heart block from Lyme carditis can progress rapidly.
Cardiac involvement usually occurs within one to two months after infection (range of less than one week to seven months) 12. Lyme carditis is a less common complication of systemic disease, occurring in approximately 4 to 10 percent of patients 13. It may present as chest pain, light-headedness, fainting, shortness of breath on exertion, heart palpitations, fatigue, heart palpitations or syncope, and often includes some form of atrioventricular block. A study of 105 patients with Lyme carditis reported that 49 percent had third-degree atrioventricular block, 28 percent had some form of second- or first-degree atrioventricular block, and 23 percent had no conduction abnormalities 14. Other less common manifestations include myopericarditis, bundle branch block, and heart failure 12.
Patients with Lyme carditis usually have other symptoms such as fever and body aches, and they may have more specific symptoms of Lyme disease, such as the erythema migrans rash.
How is Lyme carditis treated ?
Lyme carditis can be treated with oral or intravenous (IV) antibiotics, depending on how severe it is. Some patients might need a temporary pacemaker.
Can Lyme carditis be fatal ?
Yes. Between 1985 and 2008, medical journals reported four deaths, worldwide, as a result of Lyme carditis 11.
What is a Heart Block ?
Heart block is a problem in the electrical signals in the heart 15.
Normally, the heart beat starts in an area in the top chambers of the heart (atria). This area is the heart’s pacemaker. The electrical signals travel to the lower chambers of the heart (ventricles). This keeps the heart beat steady and regular.
Heart block occurs when the electrical signal is slowed down or does not reach the bottom chambers of the heart. Your heart may beat slowly, or it may skip beats. Heart block may resolve on its own, or it may be permanent and require treatment.
The symptoms and severity of heart block depend on which type you have. First-degree heart block may not cause any severe symptoms.
Second-degree heart block may result in the heart skipping a beat or beats. This type of heart block also can make you feel dizzy or faint.
Third-degree heart block limits the heart’s ability to pump blood to the rest of the body. This type of heart block may cause fatigue (tiredness), dizziness, and fainting. Third-degree heart block requires prompt treatment because it can be fatal.
A medical device called a pacemaker is used to treat third-degree heart block and some cases of second-degree heart block. This device uses electrical pulses to prompt the heart to beat at a normal rate. Pacemakers typically are not used to treat first-degree heart block.
All types of heart block may increase your risk for other arrhythmias, such as atrial fibrillation. Talk with your doctor to learn more about the signs and symptoms of a heart block.
How long does it take for a person to recover from Lyme carditis ?
Typically the patient receives antibiotic treatment for 14-21 days. Most symptoms are gone within 1-6 weeks.
How is Lyme disease diagnosed ?
Lyme disease is diagnosed based on:
- Signs and symptoms
- A history of possible exposure to infected blacklegged ticks
Laboratory blood tests are helpful if used correctly and performed with validated methods. Laboratory tests are not recommended for patients who do not have symptoms typical of Lyme disease. Just as it is important to correctly diagnose Lyme disease when a patient has it, it is important to avoid misdiagnosis and treatment of Lyme disease when the true cause of the illness is something else.
Two-step Laboratory Testing Process for Lyme Disease
The Centers for Disease Control and Prevention (CDC) currently recommends a two-step process when testing blood for evidence of antibodies against the Lyme disease bacteria. Both steps can be done using the same blood sample.
The first step uses a testing procedure called “EIA” (enzyme immunoassay) or rarely, an “IFA” (indirect immunofluorescence assay). If this first step is negative, no further testing of the specimen is recommended. If the first step is positive or indeterminate (sometimes called “equivocal”), the second step should be performed. The second step uses a test called an immunoblot test, commonly, a “Western blot” test. Results are considered positive only if the EIA/IFA and the immunoblot are both positive.
The two steps of Lyme disease testing are designed to be done together. The Centers for Disease Control and Prevention does not recommend skipping the first test and just doing the Western blot. Doing so will increase the frequency of false positive results and may lead to misdiagnosis and improper treatment.
New tests may be developed as alternatives to one or both steps of the two-step process. Before CDC will recommend new tests, their performance must be demonstrated to be equal to or better than the results of the existing procedure, and they must be FDA approved.
Figure 8. Two-Tiered Testing for Lyme Disease
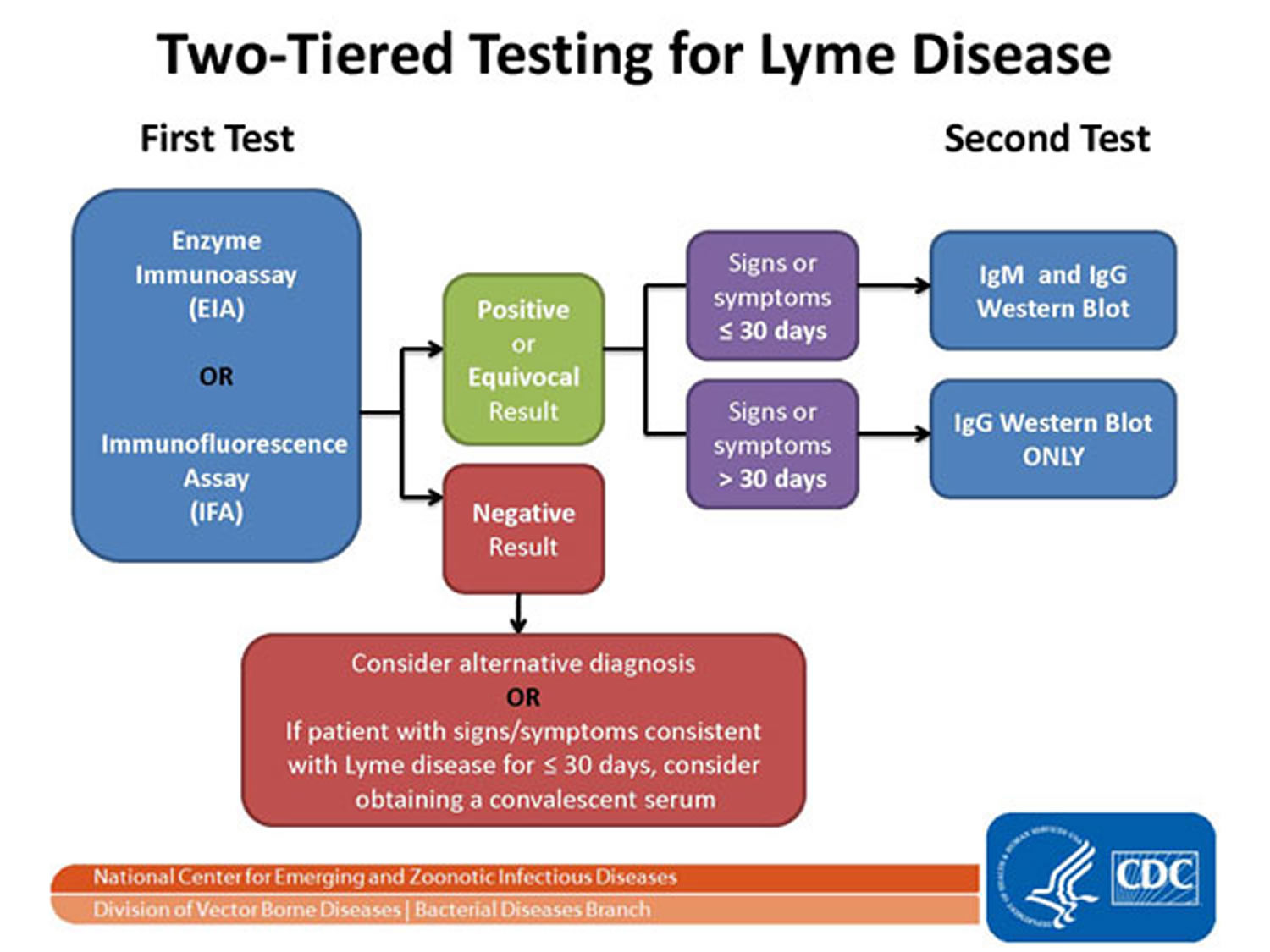
Notes: The Two-tier Testing Decision Tree describes the steps required to properly test for Lyme disease. The first required test is the Enzyme Immunoassay (EIA) or Immunofluorescence Assay (IFA). If this test yields negative results, the provider should consider an alternative diagnosis. Or in cases where the patient has had symptoms for less than or equal to 30 days, the provider may treat the patient and follow up with a convalescent serum. If the first test yields positive or equivocal results, two options are available: 1) if the patient has had symptoms for less than or equal to 30 days, an IgM Western Blot is performed; 2) if the patient has had symptoms for more than 30 days, the IgG Western Blot is performed. The IgM should not be used if the patient has been ill for more than 30 days.
[Source 16]Understanding the EIA Test
Several types of EIA tests exist. Validated and FDA-approved EIAs include “ELISA” (enzyme-linked immunosorbent assay) and “ELFA” (enzyme-linked fluorescent immunoassay). Lyme disease testing measures a person’s antibody (or immune response) to the bacteria that cause Lyme disease. EIA tests are designed to be very “sensitive”, meaning that when they are used properly, almost everyone with Lyme disease will test positive. It is also possible, however, to test positive with an EIA test even when you do not have Lyme disease. This can occur because of other medical conditions, including:
- Tick-borne relapsing fever
- Syphilis
- Anaplasmosis (formerly known as granulocytic ehrlichiosis)
- Leptospirosis
- Some autoimmune disorders (e.g., lupus)
- Bacterial endocarditis
- Infection with Helicobacter pylori, Epstein Barr virus, or Treponema denticola (bacteria found in the mouth that can cause gum disease and/or infection after dental procedures)
For this reason, doctors want to verify any “positive” or “equivocal” (indeterminate) EIA results by performing an immunoblot test such as a Western blot. The Western blot or other FDA-approved type of immunoblot can help distinguish patients who have Lyme disease from those with other conditions.
Understanding the Immunoblot Test
The immunoblot is a laboratory test that looks for antibodies the body makes against different molecules, or “antigens,” that are part of the Borrelia burgdorferi bacteria. Western Blots were the first type of immunoblot developed for Lyme disease testing. Later, a striped type of immunoblot was approved by the FDA that does not require human interpretation of bands.
Practically speaking, the test produces something that looks like a bar code used on grocery items, with several lines or “bands”. Each line represents antibodies to a different component of the bacteria. As with bar codes, the presence of any one or two lines is not particularly meaningful. Instead, it is the combination of multiple, specific lines that identifies the infection as being due to Borrelia burgdorferi.
Immunoblot tests for Lyme disease testing can detect two different classes of antibodies: IgM and IgG. IgM antibodies are made sooner, so testing for them can be helpful for identifying patients during the first few weeks of infection. The downside of testing for IgM antibodies is that they are more likely to give false positive results. Tests for IgG antibodies are more reliable, but can take 4-6 weeks for the body to produce in large enough quantities for the test to detect them.
If this sounds complex, that’s because it is. Just remember the following:
- The immunoblot should not be run without first performing an EIA or IFA.
- The immunoblot should not be run if the EIA or IFA tests are negative.
- A positive IgM immunoblot is only meaningful during the first 4 weeks of illness
- If you’ve been ill for longer than 4-6 weeks and the IgG immunoblot test is negative, it is unlikely that you have Lyme disease, even if the IgM immunoblot is positive.
Note on test result interpretation: It is not correct to interpret a test result that has only some bands that are positive as being “mildly” or “somewhat” positive for Lyme disease. The criterion that requires at least 5 IgG bands reflects the fact that people with Lyme disease have at least 5 antigens (specific molecules) detectable.
Lyme disease treatment
The treatment of Lyme disease is determined mainly by the clinical manifestations of the disease. In general, oral regimens are recommended for early localized disease. Intravenous regimens are reserved for patients with neurologic symptoms (e.g., meningitis), symptomatic cardiac disease, or, in a few cases, refractory Lyme arthritis. Many experts recommend doxycycline as the preferred agent for oral treatment because of its activity against other tick-borne illnesses (e.g., human granulocytic anaplasmosis), which can occur in up to 10 percent of patients with Lyme disease 10.
Patients treated with appropriate antibiotics in the early stages of Lyme disease usually recover rapidly and completely. Antibiotics commonly used for oral treatment include doxycycline, amoxicillin, or cefuroxime axetil. Patients with certain neurological or cardiac forms of illness may require intravenous treatment with drugs such as ceftriaxone or penicillin.
Table 1. Treatment options for Lyme disease
| Clinical symptoms | Treatment | ||||||
|---|---|---|---|---|---|---|---|
| Adults | Children | Duration | Comments | ||||
Early localized | |||||||
| Doxycycline, 100 mg orally twice per day | Doxycycline, 4 mg per kg orally per day in two divided doses (maximum of 100 mg twice per day) in children eight years or older | 14 days (range of seven to 10 days for azithromycin; 10 to 21 days for doxycycline; and14 to 21 days for amoxicillin or cefuroxime axetil) |
| |||
or | or | ||||||
Amoxicillin, 500 mg orally three times per day | Amoxicillin, 50 mg per kg orally per day in three divided doses (maximum of 500 mg per dose) | ||||||
or | or | ||||||
Cefuroxime axetil (Ceftin), 500 mg orally twice per day | Cefuroxime axetil, 30 mg per kg orally per day in two divided doses (maximum of 500 mg per dose) | ||||||
or | or | ||||||
Azithromycin (Zithromax), 500 mg orally once per day | Azithromycin, 10 mg per kg orally per day (maximum of 500 mg per day) | ||||||
Early disseminated | |||||||
| Ceftriaxone (Rocephin), 2 g intravenously per day | Ceftriaxone, 50 to 75 mg per kg intravenously per day (maximum of 2 g per dose) | 14 days (range of 14 to 21 days for ceftriaxone or cefotaxime and 10 to 28 days for oral doxycycline) |
| |||
or | or | ||||||
Cefotaxime (Claforan), 2 g intravenously every eight hours | Cefotaxime, 150 to 200 mg per kg intravenously per day in three or four divided doses (maximum of 6 g per day) | ||||||
or | or | ||||||
Doxycycline, 200 to 400 mg orally in two divided doses per day | Doxycycline, 4 to 8 mg per kg intravenously in two divided doses per day in children eight years or older (maximum of 100 to200 mg per dose) | ||||||
Late | |||||||
| Same oral antibiotics as used for erythema migrans | Same oral antibiotics as used for erythema migrans | 28 days |
| |||
| Same intravenous antibiotics as used for neurologic symptoms of early disseminated disease | Same intravenous antibiotics as used for neurologic symptoms of early disseminated disease | 14 to 28 days | ||||
Note: Treatments are listed in order of most to least preferred.
I am pregnant and just found out I have Lyme disease. What should I do ?
If you are pregnant and suspect you have contracted Lyme disease, contact your physician immediately. Untreated Lyme disease during pregnancy may lead to infection of the placenta and possible stillbirth.
Thankfully, no serious effects on the fetus have been found in cases where the mother receives appropriate antibiotic treatment for her Lyme disease. In general, treatment for pregnant women with Lyme disease is similar to that of non-pregnant adults, although certain antibiotics, such as doxycycline, are not used because they can affect fetal development.
Additionally, there are no reports of Lyme disease transmission from breast milk.
Where can I get a test to make sure that I am cured ?
As with many infectious diseases, there is no test that can “prove” cure. Tests for Lyme disease detect antibodies produced by the human immune system to fight off the bacteria (Borrelia burgdorferi) that cause Lyme disease. These antibodies can persist long after the infection is gone. This means that if your blood tests positive, then it will likely continue to test positive for months or even years even though the bacteria are no longer present.
A research tool called PCR can detect bacterial DNA in some patients. Unfortunately, this is also not helpful as a test of whether the antibiotics have killed all the bacteria. Studies have shown that DNA fragments from dead bacteria can be detected for many months after treatment. Studies have also shown that the remaining DNA fragments are not infectious. Positive PCR test results are analogous to a crime scene – – just because a robbery occurred and the robber left his DNA, it doesn’ t mean that the robber is still in the house. Similarly, just because DNA fragments from an infection remain, it doesn’ t mean the bacteria are alive or viable.
I heard that if I get Lyme disease I will always have it. Is that true ?
No. Patients treated with antibiotics in the early stages of the infection usually recover rapidly and completely. Most patients who are treated in later stages of the disease also respond well to antibiotics, although some may have suffered long-term damage to the nervous system or joints. It is not uncommon for patients treated for Lyme disease with a recommended 2 to 4 week course of antibiotics to have lingering symptoms of fatigue, pain, or joint and muscle aches at the time they finish treatment. In a small percentage of cases, these symptoms can last for more than 6 months. These symptoms cannot be cured by longer courses of antibiotics, but they generally improve on their own, over time.
If I have been diagnosed with Lyme disease, do I need to get tested for other tickborne diseases (coinfections) ?
Maybe. The blacklegged ticks that transmit Lyme disease can sometimes also transmit babesiosis and anaplasmosis. Fortunately, Lyme disease and anaplasmosis are treated with the same antibiotics, so if you are receiving treatment for Lyme disease, anaplasmosis will be treated at the same time 17. Babesiosis is a parasitic disease that is treated with different medications. If your Lyme disease symptoms do not seem to be going away after taking antibiotics, see your health care provider.
There is, however, a great deal of misinformation regarding tickborne coinfections on the internet. The possibility of having three or more tickborne infections or having pathogens such Bartonella or Mycoplasma (which have not been shown to be tickborne), is extremely unlikely.
The chance of having multiple tickborne infections depends on your location. Several studies have looked at the prevalence of these different organisms in ticks, though methods and locations are very different. Studies have shown that the rate of coinfection in blacklegged ticks varies by region from 1 to 28%. The most common coinfection in ticks is Borrelia burgdorferi (Lyme disease) and Anaplasma phagocytophilum (anaplasmosis). The frequency of tickborne coinfections in Lyme disease patients from endemic areas ranges from 4 to 45% 18. From 2 to 12% of patients with early Lyme disease may also have anaplasma infection, and 2 to 40% of patients with early Lyme disease may also have babesia infection, depending on the region 19.
What is Chronic Lyme Disease ?
Chronic lyme disease also known as “Post-treatment Lyme Disease Syndrome”, is lingering symptoms of fatigue, pain, or joint and muscle aches at the time patients finish their treatment for Lyme disease. In a small percentage of cases, these symptoms can last for more than 6 months 20.
Table 2. Categories to Describe Symptoms Attributed to Chronic Lyme Disease
Category 1: Patients have nonspecific signs and symptoms suggestive of Lyme disease, but no objective clinical or laboratory evidence of infection |
Category 2: Patients may have a history of tick exposure, with symptoms suggestive of Lyme disease, but have an alternative identifiable illness to explain symptoms |
Category 3: Patients have serologic evidence suggestive of Lyme disease, but do not have clinical symptoms consistent with Lyme disease |
Category 4: Patients have clinical and laboratory evidence of previous Lyme disease, but have persistent symptoms for longer than six months despite appropriate antibiotic therapy; also referred to as Post-treatment Lyme Disease Syndrome. |
[Source 21]
The exact cause of chronic lyme disease or Post-treatment Lyme Disease Syndrome is not yet known. Most medical experts believe that the lingering symptoms are the result of residual damage to tissues and the immune system that occurred during the infection. Similar complications and “auto–immune” responses are known to occur following other infections, including Campylobacter (Guillain-Barre syndrome), Chlamydia (Reiter’s syndrome), and Strep throat (rheumatic heart disease). In contrast, some health care providers tell patients that these symptoms reflect persistent infection with Borrelia burgdorferi. Recent animal studies have given rise to questions that require further research. Clinical studies are ongoing to determine the cause of chronic lyme disease in humans.
Although controversy exists regarding post–Lyme disease syndrome and chronic Lyme disease treatment, four randomized clinical trials found no evidence that prolonged antibiotic therapy is of benefit 22, 23, 24. Regardless of the cause of chronic lyme disease, studies have not shown that patients who received prolonged courses of antibiotics do better in the long run than patients treated with placebo. Therefore, the American Academy of Pediatrics, American Academy of Neurology, American College of Rheumatology, and Infectious Disease Society of America do not recommend prolonged antibiotic therapy 25. A recent survey concluded that 97 percent of primary care physicians in Lyme disease–endemic areas did not diagnose or treat patients for chronic Lyme disease 26. Furthermore, long-term antibiotic treatment for Lyme disease has been associated with serious complications. The good news is that patients with chronic lyme disease almost always get better with time; the bad news is that it can take months to feel completely well.
If you have been treated for Lyme disease and still feel unwell, see your doctor to discuss how to relieve your suffering. Your doctor may want to treat you in ways similar to patients who have fibromyalgia or chronic fatigue syndrome. This does not mean that your doctor is dismissing your pain or saying that you have these conditions. It simply means that the doctor is trying to help you cope with your symptoms using the best tools available.
It is normal to feel overwhelmed by your ongoing symptoms. Some things that may help you manage your chronic lyme disease include:
- Check with your doctor to make sure that Lyme disease is not the only thing affecting your health.
- Become well-informed. A lot of inaccurate information is available, especially on the internet. Learn how to sort through this maze.
- Track your symptoms. It can be helpful to keep a diary of your symptoms, sleep patterns, diet, and exercise to see how these influence your well-being.
- Maintain a healthy diet and get plenty of rest.
- Share your feelings. If your family and friends can’t provide the support you need, talk with a counselor who can help you find ways of managing your life during this difficult time. As with any illness, Lyme disease can affect you and your loved ones. It doesn’t mean that your symptoms are not real. It means that you are a human being who needs extra support in a time of need.
- Lyme Disease. American Academy of Family Physicians. https://familydoctor.org/condition/lyme-disease/[↩][↩]
- Lyme Disease Frequently Asked Questions (FAQ). Centers for Disease Control and Prevention. https://www.cdc.gov/lyme/faq/[↩][↩]
- Lyme Disease. Centers for Disease Control and Prevention. https://www.cdc.gov/lyme/transmission/index.html[↩][↩]
- How many people get Lyme disease ? Centers for Disease Control and Prevention. https://www.cdc.gov/lyme/stats/index.html[↩]
- Lyme disease. National Institute of Allergy and Infectious Diseases. https://www.ninds.nih.gov/Disorders/All-Disorders/Neurological-Complications-Lyme-Disease-Information-Page[↩][↩]
- Woodrum JE, Oliver JH, Jr., 1999. Investigation of venereal, transplacental, and contact transmission of the Lyme disease spirochete, Borrelia burgdorferi, in Syrian hamsters. J Parasitol 85: 426-30. https://www.ncbi.nlm.nih.gov/pubmed/10386432[↩]
- Porcella SF, Schwan TG, 2001. Borrelia burgdorferi and Treponema pallidum: a comparison of functional genomics, environmental adaptations, and pathogenic mechanisms. J Clin Invest 107: 651-6. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC208952/[↩]
- Eligibility Requirements. American National Red Cross. http://www.redcrossblood.org/donating-blood/eligibility-requirements[↩]
- Marques A. Chronic Lyme disease: a review. Infect Dis Clin North Am. 2008;22(2):341–360, viiviii.[↩]
- Wormser GP, Dattwyler RJ, Shapiro ED, et al. The clinical assessment, treatment, and prevention of lyme disease, human granulocytic anaplasmosis, and babesiosis: clinical practice guidelines by the Infectious Diseases Society of America [published correction appears in Clin Infect Dis. 2007;45(7):941]. Clin Infect Dis. 2006;43(9):1089–1134.[↩][↩][↩]
- What you need to know about Lyme carditis. Centers for Disease Control and Prevention. https://www.cdc.gov/lyme/signs_symptoms/lymecarditis.html[↩][↩]
- Steere AC. Lyme disease. N Engl J Med. 2001;345(2):115–125.[↩][↩]
- Sigal LH. Early disseminated Lyme disease: cardiac manifestations. Am J Med. 1995;98(4A):25S–28S, discussion 28S–29S.[↩]
- van der Linde MR. Lyme carditis: clinical characteristics of 105 cases. Scand J Infect Dis Suppl. 1991;77:81–84.[↩]
- Heart Block. National Heart, Lung and Blood Institute. https://www.nhlbi.nih.gov/health/health-topics/topics/hb/[↩]
- Two-step Laboratory Testing Process. Centers for Disease Control and Prevention. https://www.cdc.gov/lyme/diagnosistesting/labtest/twostep/index.html[↩]
- Wormser et al. The clinical assessment, treatment, and prevention of Lyme disease, human granulocytic anaplasmosis, and babesiosis: Clinical practice guidelines by the Infectious Diseases Society of America. Clin Infect Dis. 2006;43:1089-1134. https://academic.oup.com/cid/article/43/9/1089/422463/The-Clinical-Assessment-Treatment-and-Prevention[↩]
- Swanson, et al. Coinfections acquired from Ixodes ticks. Clin Microbiol Rev. 2006 Oct;19(4):708-27. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1592693/[↩]
- Wormser, Gary. Clinical practice. Early Lyme disease. N Engl J Med. 2006 Jun 29;354(26):2794-801.[↩]
- Post-Treatment Lyme Disease Syndrome. Centers for Disease Control and Prevention. https://www.cdc.gov/lyme/postlds/index.html[↩]
- Diagnosis and Management of Lyme Disease. Am Fam Physician. 2012 Jun 1;85(11):1086-1093. http://www.aafp.org/afp/2012/0601/p1086.html[↩]
- Klempner MS, Hu LT, Evans J, et al. Two controlled trials of antibiotic treatment in patients with persistent symptoms and a history of Lyme disease. N Engl J Med. 2001;345 (2):85–92.[↩]
- Krupp LB, Hyman LG, Grimson R, et al. Study and treatment of post Lyme disease (STOP-LD): a randomized double masked clinical trial. Neurology. 2003;60(12):1923–1930.[↩]
- Fallon BA, Keilp JG, Corbera KM, et al. A randomized, placebo-controlled trial of repeated IV antibiotic therapy for Lyme encephalopathy. Neurology. 2008;70(13):992–1003.[↩]
- Appropriateness of parenteral antibiotic treatment for patients with presumed Lyme disease. A joint statement of the American College of Rheumatology and the Council of the Infectious Diseases Society of America. Ann Intern Med. 1993;119(6):518.[↩]
- Johnson M, Feder HM Jr. Chronic Lyme disease: a survey of Connecticut primary care physicians J Pediatr. 2010;157(6):1025–1029e1–e2.[↩]





{kind=link}