Contents
- What is lymphoma
- The Lymphatic System
- Signs and symptoms of lymphoma
- What Causes lymphoma
- Diagnosis of lymphoma
- Treatment of lymphoma
- Coping and support
- Hodgkin’s lymphoma
- Non hodgkin’s lymphoma
- How Many People Survive 5 Years Or More after Being Diagnosed with non-Hodgkin Lymphoma?
- Types of Non-Hodgkin Lymphoma
- B-cell lymphomas
- Diffuse large B-cell lymphoma (DLBCL)
- Follicular lymphoma
- Chronic lymphocytic leukemia (CLL) /small lymphocytic lymphoma (SLL)
- Mantle cell lymphoma (MCL)
- Marginal zone lymphomas
- Burkitt lymphoma
- Lymphoplasmacytic lymphoma (Waldenstrom macroglobulinemia)
- Hairy cell leukemia
- Primary central nervous system (CNS) lymphoma
- T-cell lymphomas
- B-cell lymphomas
- Non hodgkin’s lymphoma signs and symptoms
- What Causes non-Hodgkin’s lymphoma
- Risk Factors non-Hodgkin’s lymphoma
- How non-Hodgkin lymphoma is diagnosed
- Non-Hodgkin’s lymphoma Staging
- Non-Hodgkin’s lymphoma Subtypes
- Non-Hodgkin’s lymphoma Treatment
- Treatment for Aggressive Non-Hodgkin’s lymphoma Subtypes
- Treatment for Indolent Non-Hodgkin’s lymphoma Subtypes
What is lymphoma
Lymphoma is a cancer of the lymphatic system 1, which is part of the body’s germ-fighting network (see Figures 1, 2 and 3). Lymphomas are cancers that start in white blood cells called lymphocytes.
The lymphatic system includes the lymph nodes (lymph glands), spleen, thymus gland and bone marrow. Lymphoma can affect all those areas as well as other organs throughout the body.
There are many types of lymphoma. The main categories of lymphoma are:
- Hodgkin’s lymphoma (Hodgkin disease)
- Non-Hodgkin’s lymphoma
They behave, spread, and respond to treatment differently, so it’s important for you to know which one you have. Knowing which type of lymphoma you have is important because it affects your treatment options and your outlook (prognosis). If you aren’t sure which type you have, ask your doctor so you can get the right information.
What lymphoma treatment is best for you depends on your lymphoma type and its severity. Lymphoma treatment may involve chemotherapy, immunotherapy medications, radiation therapy or a bone marrow transplant.
The Lymphatic System
To understand what lymphoma is, it helps to know about the lymph system (also known as the lymphatic system). The lymph system is part of the immune system, which helps fight infections and some other diseases. It also helps the flow of fluids in the body.
The lymph system is made up mainly of cells called lymphocytes, a type of white blood cell. There are 2 main types of lymphocytes:
- B lymphocytes (B cells): B cells make proteins called antibodies to help protect the body from germs (bacteria and viruses).
- T lymphocytes (T cells): There are several types of T cells. Some T cells destroy germs or abnormal cells in the body. Other T cells help boost or slow the activity of other immune system cells.
The lymphatic system is a vast collection of cells and biochemicals that travel in lymphatic vessels, and the organs and glands that produce them. The lymphatic system includes a network of vessels that assist in circulating body fluids, so it is closely associated with the cardiovascular system. Lymphatic vessels transport excess fluid away from interstitial spaces in most tissues and return it to the bloodstream (Figure 3). Without the lymphatic system, this fluid would accumulate in tissue spaces. Special lymphatic capillaries, called lacteals, are located in the lining of the small intestine. They absorb digested fats and transport them to the venous circulation.
The major sites of lymphoid tissue are:
Lymph nodes: Lymph nodes are bean-sized collections of lymphocytes and other immune system cells throughout the body, including inside the chest, abdomen, and pelvis. They are connected to each other by a system of lymphatic vessels.
Spleen: The spleen is an organ under the lower ribs on your left side. The spleen makes lymphocytes and other immune system cells. It also stores healthy blood cells and filters out damaged blood cells, bacteria, and cell waste.
Bone marrow: The bone marrow is the spongy tissue inside certain bones. New blood cells (including some lymphocytes) are made there.
Thymus: The thymus is a small organ behind the upper part of the breastbone and in front of the heart. It is important for T lymphocyte development..
Adenoids and tonsils: These are collections of lymphoid tissue in the back of your throat. They help make antibodies against germs that are breathed in or swallowed.
Digestive tract: The stomach, intestines, and many other organs also have lymph tissue.
The lymphatic system has a second major function— it enables you to live in a world with different types of organisms. Some of them live in or on the human body and in some circumstances may cause infectious diseases. Cells and biochemicals of the lymphatic system launch both generalized and targeted attacks against “foreign” particles, enabling the body to destroy infectious agents. This immunity against disease also protects against toxins and cancer cells. When the immune response is abnormal, persistent infection, cancer, allergies, and autoimmune disorders may result.
The larger lymphatic vessels lead to specialized organs called lymph nodes. After leaving the lymph nodes, the vessels merge to form still larger lymphatic trunks.
Figure 1. Locations of major lymph nodes
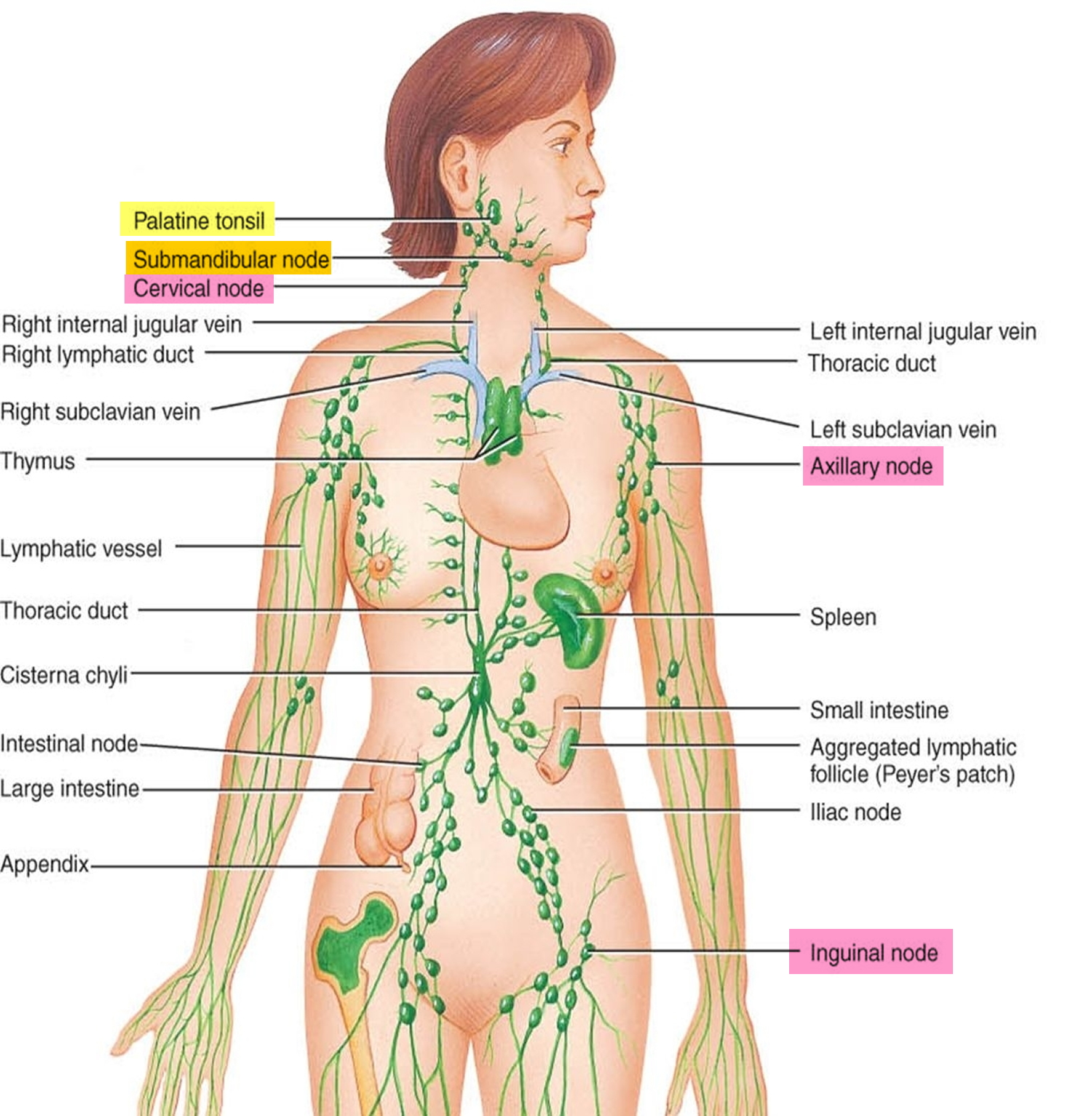
Figure 2. Functions of lymph nodes in the lymphatic system
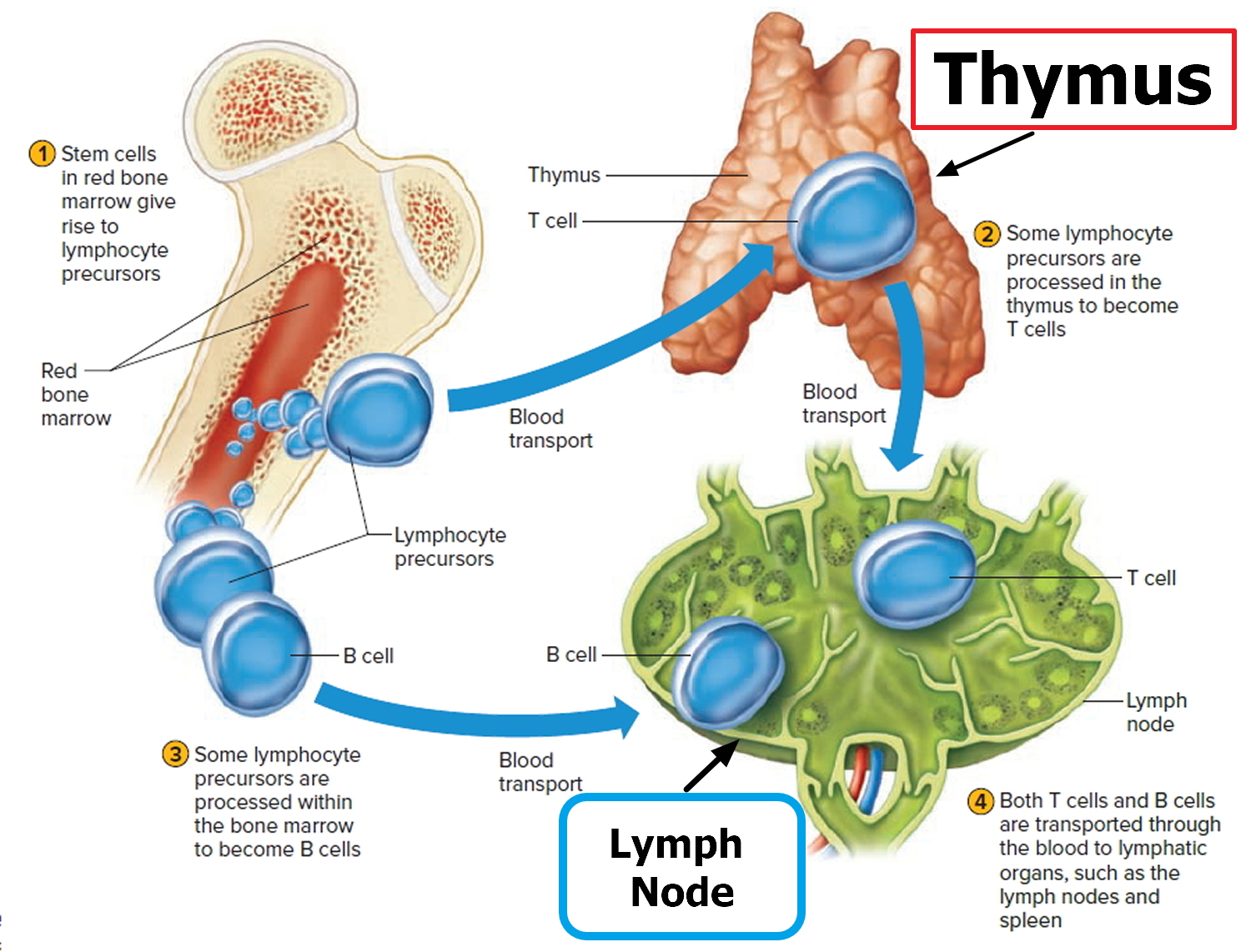
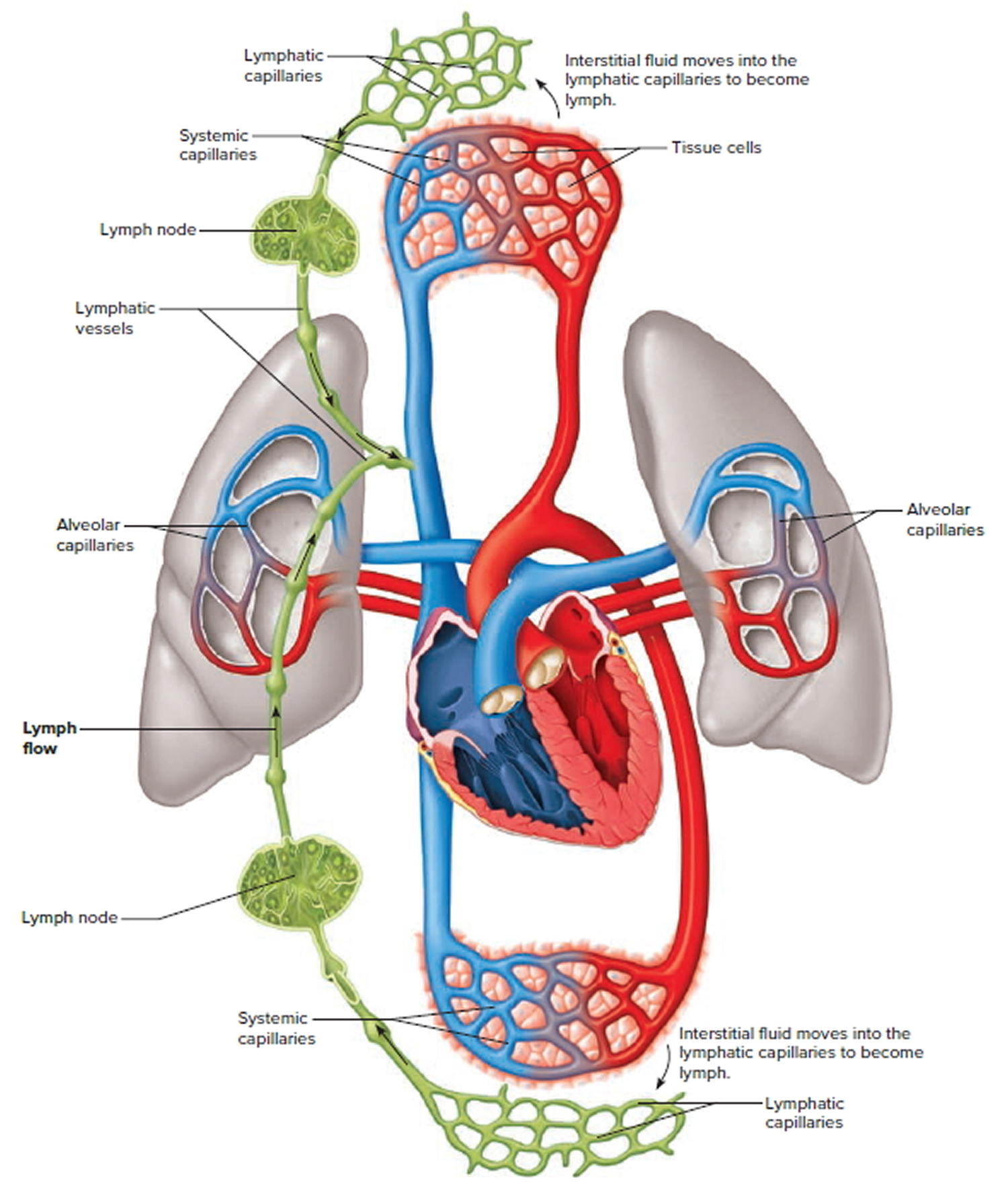
Figure 3. Schematic representation of lymphatic vessels transporting fluid from interstitial spaces to the bloodstream. Depending on its origin, lymph enters the right or left subclavian vein.
Signs and symptoms of lymphoma
Signs and symptoms of lymphoma include:
- Enlarged lymph nodes that can occur in any part of the body but most often occur in the neck, armpit or groin
- Fatigue
- Fever
- Night sweats
- Shortness of breath
- Weight loss
What Causes lymphoma
Doctors aren’t sure what causes lymphoma.
Lymphoma begins when a disease-fighting white blood cell called a lymphocyte develops a mutation in its genetic code. The mutation tells the cell to multiply rapidly, causing many diseased lymphocytes that continue multiplying.
The mutations also allow the cells to go on living when other cells would die. This causes too many diseased and ineffective lymphocytes in your lymph nodes and causes the lymph nodes to swell.
Risk factors for lymphoma
Factors that may increase your risk of lymphoma include:
- Increasing age. Your risk of lymphoma increases as you age, though it can occur at any age. Some types of lymphoma are more common in young adults.
- Being male. Lymphoma is more common in men than it is in women.
- Having an impaired immune system. Lymphoma is more common in people with immune system diseases or in people who take drugs that suppress their immune systems.
- Developing certain infections. Some infections are associated with an increased risk of lymphoma, including Epstein-Barr virus and Helicobacter pylori infection.
Diagnosis of lymphoma
Tests and procedures used to diagnose lymphoma include:
- Physical exam. Your doctor may examine your body to look for signs of enlarged lymph nodes.
- Removing a lymph node for testing. Your doctor may recommend a lymph node biopsy procedure to remove all or part of a lymph node for laboratory testing. Advanced tests can determine if lymphoma cells are present and what types of cells are involved.
- Blood tests. Blood tests to count the number of cells in a sample of your blood can give your doctor clues about your diagnosis.
- Removing a sample of bone marrow for testing. A bone marrow biopsy and aspiration procedure involves inserting a needle into your hipbone to remove a sample of bone marrow. The sample is analyzed to look for lymphoma cells.
- Imaging tests. Imaging tests may be used to look for signs of lymphoma in other areas of your body. Tests may include CT, MRI and positron emission tomography (PET).
Treatment of lymphoma
Your lymphoma treatment options will depend on your type of lymphoma, its aggressiveness and your treatment goals.
Lymphoma treatments include:
- Active surveillance. Some forms of lymphoma are very slow growing. You and your doctor may decide to wait to treat your lymphoma when it causes signs and symptoms that interfere with your daily activities. Until then, you may undergo periodic tests to monitor your condition.
- Chemotherapy. Chemotherapy is a drug treatment that uses chemicals to kill cancer cells. Chemotherapy is usually administered through a vein, but can also be taken as a pill, depending on the specific drugs you receive.
- Other drug therapy. Other drugs used to treat lymphoma include targeted drugs that focus on specific abnormalities within your cancer cells that allow them to survive. Immunotherapy drugs use your immune system to kill cancer cells.
- Radiation therapy. Radiation therapy uses powerful beams of energy, such as X-rays and protons, to kill cancer cells.
- Bone marrow transplant. Bone marrow transplant, also known as a stem cell transplant, involves using high doses of chemotherapy and radiation to suppress your bone marrow. Then healthy bone marrow stem cells from your body or from a donor are infused into your blood where they travel to your bones and rebuild your bone marrow.
Coping and support
A lymphoma diagnosis can be overwhelming and scary. With time you’ll find ways to cope with the distress and uncertainty of cancer. Until then, you may find it helps to:
- Learn enough about lymphoma to make decisions about your care. Ask your doctor about your lymphoma, including your type, your treatment options and, if you like, your prognosis. As you learn more about lymphoma, you may become more confident in making treatment decisions.
- Keep friends and family close. Keeping your close relationships strong will help you deal with your lymphoma. Friends and family can provide the practical support you’ll need, such as helping take care of your house if you’re in the hospital. And they can serve as emotional support when you feel overwhelmed by cancer.
Find someone to talk with. Find a good listener with whom you can talk about your hopes and fears. This may be a friend or family member. The concern and understanding of a counselor, medical social worker, clergy member or cancer support group also may be helpful.
Ask your doctor about support groups in your area. You might also contact a cancer organization such as the National Cancer Institute 2 or the Leukemia and Lymphoma Society 3.
Hodgkin’s lymphoma
Hodgkin lymphoma usually starts in B lymphocytes. Hodgkin lymphoma is an uncommon cancer that develops in the lymphatic system.
Hodgkin lymphoma named after Dr. Thomas Hodgkin who, in 1832, described several cases of people with symptoms of a cancer involving the lymph nodes. The disease was called “Hodgkin’s disease” until it was officially renamed “Hodgkin lymphoma” in the late 20th century.
Although Hodgkin lymphoma can start almost anywhere, most often it starts in lymph nodes in the upper part of the body. The most common sites are in the chest, neck, or under the arms.
Hodgkin lymphoma starts when an abnormal change to the DNA of a white blood cell (called a lymphocyte) causes it to become a lymphoma cell that, if untreated, results in the uncontrolled growth of cancerous lymphocytes.
- These cancerous cells crowd out normal white cells, and the immune system can’t guard against infection effectively.
- Lymphoma cells grow and form masses, usually in the lymph nodes, located throughout our bodies in the lymphatic system.
- Lymphoma cells can also gather in other areas of the body where lymphoid tissue is found.
- Hodgkin lymphoma is distinguished from other types of lymphoma by the presence of Reed-Sternberg cells (named for the scientists who first identified them). Other cells associated with the disease are called Hodgkin cells.
Hodgkin lymphoma most often spreads through the lymph vessels from lymph node to lymph node. Rarely, late in the disease, it can invade the bloodstream and spread to other parts of the body, such as the liver, lungs, and/or bone marrow.
The American Cancer Society’s estimates for Hodgkin disease (Hodgkin’s lymphoma) in the United States for 2017 are:
- About 8,260 new cases (3,610 in females and 4,650 in males)
- About 1,070 deaths (440 females, 630 males) from this cancer
Both children and adults can develop Hodgkin lymphoma, but it is most common in early adulthood (especially in a person’s 20s). The risk of Hodgkin lymphoma rises again in late adulthood (after age 55). Overall, the average age at the time of diagnosis is 39.
Hodgkin lymphoma is rare in children younger than 5 years of age. About 10% to 15% of cases are diagnosed in children and teenagers.
Survival rates have improved in the past few decades, largely due to advances in treatment. The 5-year relative survival rate for all patients diagnosed with Hodgkin lymphoma is now about 86%, and the 10-year relative survival rate is about 80%. Certain factors such as the stage (extent) of Hodgkin lymphoma and a person’s age affect these rates.
Survival rates for Hodgkin’s lymphoma
The numbers below come from the National Cancer Institute’s Surveillance, Epidemiology, and End Results Program 4 database, looking at more than 8,000 people diagnosed with Hodgkin lymphoma between 1988 and 2001.·
- The 5-year survival rate for people with stage I Hodgkin lymphoma is about 90%.·
- For stage II Hodgkin lymphoma, the 5-year survival rate is about 90%.
- The 5-year survival rate for stage III Hodgkin lymphoma is about 80%.
- Stage IV Hodgkin lymphoma has a 5-year survival rate of about 65%.
Based on data from SEER 18 2007-2013, percent surviving 5 Years is 86.4% 5
Hodgkin’s lymphoma Survival by Stage
Cancer stage at diagnosis, which refers to extent of a cancer in the body, determines treatment options and has a strong influence on the length of survival. In general, if the cancer is found only in the part of the body where it started it is localized (sometimes referred to as stage 1). If it has spread to a different part of the body, the stage is regional or distant. For Hodgkin lymphoma, 15.6% are diagnosed at the local stage. The 5-year survival for localized Hodgkin lymphoma is 92.2%.
Remember, these survival rates are only estimates – they can’t predict what will happen to any individual person. We understand that these statistics can be confusing and may lead you to have more questions. Talk to your doctor to better understand your specific situation.
Other prognostic factors
Along with the stage of the Hodgkin lymphoma, other factors can affect a person’s prognosis (outlook). For example, having some factors means the lymphoma is likely to be more serious:
- Having B symptoms or bulky disease
- Being older than 45
- Being male
- Having a high white blood cell count (above 15,000)
- Having a low red blood cell count (hemoglobin level below 10.5)
- Having a low blood lymphocyte count (below 600)
- Having a low blood albumin level (below 4)
- Having a high erythrocyte sedimentation rate, or ESR (over 30 in someone with B symptoms, or over 50 for someone without B symptoms)
Some of these factors are used to help divide stage I or II Hodgkin lymphoma into favorable and unfavorable groups, which can affect how intense the treatment needs to be (see Hodgkin’s lymphoma staging below).
Types of Hodgkin lymphoma
The World Health Organization (WHO) divides Hodgkin lymphoma into two main subtypes. They are:
- Classical Hodgkin lymphoma (cHL)
- Nodular lymphocyte-predominant Hodgkin lymphoma (NLPHL)
Classical Hodgkin lymphoma is characterized by the presence of Reed-Sternberg cells. Nodular lymphocyte-predominant Hodgkin lymphoma is characterized by the presence of lymphocyte-predominant cells, sometimes termed “popcorn cells,” and Reed-Sternberg cells are not found.
It’s important to know your subtype since it plays a large part in determining the type of treatment you’ll receive.
Classic Hodgkin’s lymphoma
Classic Hodgkin’s lymphoma (cHL) accounts for about 95% of all cases of Hodgkin’s lymphomas in developed countries 6.
The cancer cells in cHL are called Reed-Sternberg cells. These cells are usually an abnormal type of B lymphocyte. Enlarged lymph nodes in people with cHL usually have a small number of Reed-Sternberg cells and a large number of surrounding normal immune cells. These other immune cells make up most of the enlarged lymph nodes.
Classic Hodgkin’s lymphoma has 4 subtypes:
Nodular sclerosis Hodgkin lymphoma: This is the most common type of Hodgkin disease in developed countries. It is most common in teens and young adults, but it can occur in people of any age. It tends to start in lymph nodes in the neck or chest.
Mixed cellularity Hodgkin lymphoma: This is the second most common type and is seen mostly in older adults (although it can occur at any age). It can start in any lymph node but most often occurs in the upper half of the body.
Lymphocyte-rich Hodgkin lymphoma: This subtype usually occurs in the upper half of the body and is rarely found in more than a few lymph nodes.
Lymphocyte-depleted Hodgkin lymphoma: This is the least common form of Hodgkin disease. It is seen mainly in older people. It is more likely to be advanced when first found, in lymph nodes in the abdomen as well as in the spleen, liver, and bone marrow.
| Subtype | Characteristics |
|---|---|
| Nodular sclerosis |
|
| Mixed cellularity |
|
| Lymphocyte-rich |
|
| Lymphocyte-depleted |
|
Nodular lymphocyte predominant Hodgkin lymphoma
Nodular lymphocyte predominant Hodgkin lymphoma (NLPHL) accounts for about 5% of cases. The cancer cells in Nodular lymphocyte predominant Hodgkin lymphoma (NLPHL) are large cells called popcorn cells (because they look like popcorn), which are variants of Reed-Sternberg cells.
Nodular lymphocyte predominant Hodgkin lymphoma usually starts in lymph nodes in the neck and under the arm. It can occur in people of any age, and is more common in men than in women. This type of Hodgkin’s lymphoma is treated differently from the classic types.
The following are some characteristics of NLPHL:
- Most common in 30 to 50 year-old age group
- More common in male than in female patients
- NLPHL is slow growing (indolent) and highly curable.
- Small risk (3-5 percent of cases) of transformation to aggressive non-Hodgkin lymphoma.
What Causes Hodgkin Lymphoma?
Scientists have found some risk factors that make a person more likely to get Hodgkin disease, but it’s not always clear exactly how these factors might increase risk.
For example, some researchers think that infection with the Epstein-Barr virus may sometimes cause DNA changes in B lymphocytes, leading to the development of Reed-Sternberg cells, which are the cancer cells in Hodgkin lymphoma.
DNA is the chemical in our cells that makes up our genes, which control how our cells function. We look like our parents because they are the source of our DNA. But DNA affects more than just how we look.
Some genes control when cells grow, divide into new cells, and die:
- Genes that help cells grow, divide, and stay alive are called oncogenes.
- Genes that slow down cell division or cause cells to die at the right time are called tumor suppressor genes.
Cancers can be caused by DNA changes that turn on oncogenes or turn off tumor suppressor genes.
Scientists have found many gene changes in Reed-Sternberg cells that help the cells grow and divide or live longer than they should. Reed-Sternberg cells also make substances called cytokines, which attract many other cells into the lymph node, enlarging it. In turn, these non-cancerous cells release substances that further help Reed-Sternberg cells grow.
Despite these advances, scientists do not yet know what sets off these processes. An abnormal reaction to infection with EBV or to other infections may be the trigger in some cases. But more research is needed to understand what causes Hodgkin lymphoma.
Hodgkin Lymphoma Risk Factors
The following risk factors may increase a person’s likelihood of developing Hodgkin lymphoma:
- The Epstein-Bar virus (EBV), known for causing infectious mononucleosis, is associated with the development of Hodgkin lymphoma. The exact role of EBV in the development of Hodgkin lymphoma is not clear. Many people are infected with EBV, but very few develop Hodgkin lymphoma. Parts of the virus are found in Reed-Sternberg cells in about 1 out of 3 people with Hodgkin lymphoma. But most people with Hodgkin lymphoma have no signs of EBV in their cancer cells.
- People infected with human immunodeficiency virus (HIV) the virus that causes AIDS, have increased probability of developing Hodgkin lymphoma.
- There are occasional cases of Hodgkin lymphoma in families-having a parent or a sibling with Hodgkin lymphoma may increase the risk of developing the disease. These cases are uncommon, but some experts are studying whether some people have a genetic predisposition to Hodgkin lymphoma.
- Family history: Brothers and sisters of young people with this disease have a higher risk for Hodgkin lymphoma. The risk is very high for an identical twin of a person with Hodgkin lymphoma. But a family link is still uncommon – most people with Hodgkin lymphoma do not have a family history of it. It’s not clear why family history might increase risk. It might be because family members have similar childhood exposures to certain infections (such as Epstein-Barr virus), because they share inherited gene changes that make them more likely to get Hodgkin lymphoma, or some combination of these factors.
- Age: People can be diagnosed with Hodgkin lymphoma at any age, but it is most common in early adulthood (especially in a person’s 20s) and in late adulthood (after age 55).
- Gender: Hodgkin lyphoma occurs slightly more often in males than in females.
- Geography: Hodgkin lymphoma is most common in the United States, Canada, and Europe, and is least common in African and Asian countries.
- Socioeconomic status: The risk of Hodgkin disease is greater in people with a higher socioeconomic background. The reason for this is not clear. One theory is that children from more affluent families might be exposed to some type of infection (such as Epstein-Barr virus) later in life than children from less affluent families, which might somehow increase their risk.
You can not catch the disease from someone else.
Signs and Symptoms of Hodgkin’s lymphoma
The most common early sign of Hodgkin lymphoma is painless swelling (enlargement) of one or more lymph nodes. Most people have affected lymph nodes in the upper part of their body, usually the neck or upper chest. Sometimes the affected lymph nodes are in the armpit, stomach area or groin.
Hodgkin’s lymphoma doesn’t usually hurt, but the area may become painful after drinking alcohol. The lump might grow larger over time, or new lumps might appear near it (or even in other parts of the body).
But Hodgkin lymphoma is not the most common cause of lymph node swelling. Most enlarged lymph nodes, especially in children, are caused by an infection. Lymph nodes that grow because of infection are called reactive or hyperplastic nodes. These often hurt when they are touched. If an infection is the cause, the node should return to its normal size within a few weeks after the infection goes away.
Other cancers can also cause swollen lymph nodes. If you have an enlarged lymph node, especially if you haven’t had a recent infection, it’s best to see your doctor so that the cause can be found and treated without delay, if needed.
In addition to swollen lymph nodes, other signs and symptoms of Hodgkin lymphoma may include:
- Unexplained fever
- Persistent fatigue
- Persistent cough
- Shortness of breath during normal activity
- Drenching sweats, especially at night
- Unexplained weight loss
- Decreased appetite
- Itchy skin
- Abdominal pain or swelling and feeling of fullness (due to an enlarged spleen)
- Lymph node pain after drinking alcohol
B symptoms. Fever, drenching night sweats and loss of more than 10 percent of body weight over six months are sometimes termed “B symptoms.” These symptoms are significant to the prognosis and staging of the disease.
Some Hodgkin lymphoma symptoms are associated with other, less serious illnesses. However, if you’re troubled by any of the above symptoms, see your doctor.
Hodgkin’s lymphoma diagnosis
Hodgkin lymphoma can be a difficult disease to diagnose because it can be confused with some types of non-Hodgkin lymphoma. Having the correct diagnosis is important for getting the right treatment. You may want to get a second medical opinion by an experienced hematopathologist before you begin treatment. A hematopathologist is a specialist who studies blood and bone marrow cells and other tissues to help diagnose diseases of the blood, bone marrow and lymph system.
If a person has signs or symptoms that suggest Hodgkin lymphoma, exams and tests will be done to find out for sure and, if so, to determine the exact type.
Medical history and physical exam
Your doctor will want to get a thorough medical history, including information about symptoms, possible risk factors, family history, and other medical conditions.
Next, the doctor will examine you, paying special attention to the lymph nodes and other areas of the body that might be affected, including the spleen and liver. Because infections are the most common cause of enlarged lymph nodes, especially in children, the doctor will look for an infection in the part of the body near any swollen lymph nodes.
The doctor also might order blood tests to look for signs of infection or other problems. If the doctor suspects that Hodgkin lymphoma might be causing the symptoms, he or she might recommend a biopsy of a swollen lymph node.
Lymph Node Biopsy
Diagnosing Hodgkin lymphoma usually involves performing a lymph node biopsy. The entire lymph node or part of the lymph node is surgically removed using a special needle. A hematopathologist examines the sample of the lymph node under a microscope to look for the identifying characteristics of Hodgkin lymphoma. If the biopsy confirms that you have Hodgkin lymphoma, the hematopathologist will categorize the Hodgkin lymphoma into one of several subtypes. .
The lymph node biopsy’s purpose is to confirm a diagnosis and:
- Identify your Hodgkin lymphoma subtype
- Develop a treatment plan
Immunophenotyping
The hematopathologist may use a lab test called immunophenotyping to distinguish Hodgkin lymphoma from other types of lymphoma or other cancerous or noncancerous conditions based on the antigens or markers on the surface of the cells.
Staging Tests
Once your hematologist-oncologist confirms a Hodgkin lymphoma diagnosis, he or she orders more tests to stage your disease. Staging identifies the extent of your disease and where it’s located in your body.
Staging tests include:
- Imaging tests
- Blood tests
- Bone marrow tests
Imaging Tests
Imaging tests help the doctor evaluate:
- The location and distribution of enlarged lymph nodes
- Whether organs other than lymph nodes are involved
- Whether there are very large masses of tumors in one site or another
Imaging tests may include:
- Chest X-ray
- CT (computed tomography) scan of the neck, chest, pelvis and abdomen (stomach area)
- FDG-PET (fluorodeoxyglucose [FDG] positron emission tomography [PET]) of the entire body with a radioactive tracer
- Combination PET-CT scan
- MRI (magnetic resonance imaging)
Blood Tests
Blood tests are used to:
- Assess blood counts including red blood cells, white blood cells and platelets;
- Determine whether lymphoma cells are present in the blood;
- Determine whether the immunoglobulins (proteins that fight infection) made by lymphocytes are deficient or abnormal;
- Check indicators of inflammation and disease severity such as blood protein levels, uric acid levels and erythrocyte sedimentation rate ;
- Assess kidney and liver functions.
Bone Marrow Tests
Your doctor may decide to examine your bone marrow to see whether the disease has spread to the bone marrow. Your doctor will decide if this procedure is necessary based on certain features such as the location of the disease in your body. Bone marrow testing may not be required for patients with early-stage disease and low-risk clinical features.
- Bone marrow testing involves two steps usually done at the same time in a doctor’s office or a hospital:
- A bone marrow aspiration to remove a liquid sample of bone marrow
Hodgkin Lymphoma Staging
Doctors use physical examinations, imaging tests, blood test and, sometimes, bone marrow tests to determine the extent of the disease. This determination is called “staging.” Staging provides important information for treatment planning.
Staging for Hodgkin lymphoma is based on the Ann Arbor staging system. Each stage is subdivided and assigned to category A, B or E.
Categories A, B and E
Each stage of Hodgkin lymphoma is subdivided and assigned to category A, B or E. :
- Category A indicates no symptoms are present
- Category B indicates the presence of “B symptoms:”
- Unexplained fevers
- Drenching night sweats
- Unexpected weight loss of more than 10 percent of body weight
- Category E indicates involvement of organs or tissues beyond the lymph system.
A vs. B
Each stage may also be assigned a letter (A or B). B is added (stage IIIB, for example) if a person has any of these B symptoms:
- Loss of more than 10% of body weight over the previous 6 months (without dieting)
- Unexplained fever of at least 100.4°F (38°C)
- Drenching night sweats
If a person has any B symptoms, it usually means the lymphoma is more advanced, and more intensive treatment is often recommended. If no B symptoms are present, the letter A is added to the stage.
For example, staging for Hodgkin lymphoma based on the Ann Arbor staging system means that a patient with stage IIB Hodgkin lymphoma has:
Involvement of two lymph node sites near each other (for example, enlarged lymph nodes in the neck and near the collarbone, or in the neck and the armpit)
Fever, excessive sweating and weight loss.
- Your treatment depends on your stage and category. Patients who fall into the B category usually need more aggressive treatment than A category patients do.
| Stage I | Involvement of one lymph node group or a group of adjacent nodes |
| Stage II | Involvement of two or more lymph node regions on the same side of the diaphragm (a thin muscle below the lungs) |
| Stage III | Involvement of lymph node groups on both sides of the diaphragm (for example, neck, chest and abdomen) |
| Stage IV | Involvement of lymph nodes on both sides of the diaphragm and/or involvement of one or more organs such as the lungs, spleen, liver, bones or bone marrow |
Figure 4. Hodgkin Lymphoma Stages
Resistant or recurrent Hodgkin lymphoma
Resistant or recurrent Hodgkin lymphoma is not part of the formal staging system, but doctors or nurses might use these terms to describe what is going on with the lymphoma in some cases.
The terms resistant or progressive disease are used when the lymphoma does not go away or progresses (grows) while you are still being treated.
Recurrent or relapsed disease means that Hodgkin lymphoma initially went away with treatment, but it has now come back. If the lymphoma returns, it may be in the same place where it started or in another part of the body. This may occur shortly after treatment or years later.
Hodgkin’s lymphoma Treatment
Treatment for Hodgkin lymphoma is changing due to new drugs and research findings from clinical trials. Therefore, before treatment begins, it is important to consider getting a second opinion at a center with a Hodgkin lymphoma expert.
It’s important that your doctor is experienced in treating patients with Hodgkin lymphoma or works in consultation with a Hodgkin lymphoma specialist. This type of specialist is called a hematologist-oncologist.
For many people with Hodgkin lymphoma, starting treatment helps them focus on moving ahead and looking forward to recovery. Hodgkin lymphoma is considered one of the most curable forms of cancer.
Types of Treatment
Doctors use several types of approaches and treatment combinations for adults and children with Hodgkin lymphoma, some at different stages:
- Chemotherapy
- Radiotherapy also known as “radiation therapy”
- Stem cell transplantation
- Your doctor may suggest that you participate in a clinical trial. Clinical trials can involve therapy with new drugs and new drug combinations or new approaches to stem cell transplantation.
Pretreatment Considerations
Adults of childbearing age and parents of children diagnosed with Hodgkin lymphoma should ask their doctors for information that may lessen the risk of infertility.
Finding the Best Treatment Approach
The goal of Hodgkin lymphoma treatment is to cure the disease.
- The treatment your doctor recommends is based on several factors, including:
- Your disease subtype
- Your disease stage and category
- Whether your disease is either refractory (the disease does not respond to treatment) or relapsed (the disease has recurred after treatment)
- Your age
- Whether you have coexisting diseases or conditions (for example, heart disease, kidney disease, diabetes)
As you develop a treatment plan with your doctor, be sure to discuss:
- The results you can expect from treatment
- The potential side effects, including long-term effects and late-term effects
- The possibility of participating in a clinical trial, where you may have access to advanced medical treatment that may be more beneficial to you than standard treatment
You may find it helpful to bring a loved one with you to your doctor’s visits for support, to take notes and to ask follow-up questions. It’s a good idea to prepare questions you’d like to ask when you visit your doctor. You can also record your conversations with your doctor and listen more closely when you get home.
Chemotherapy Drug Combinations
Children and young adults with Hodgkin lymphoma are usually treated with combination chemotherapy and involved field radiation therapy.
Common chemotherapy drug combinations used to treat children and young adults include:
- ABVD: doxorubicin (Adriamycin®), bleomycin (Blenoxane®), vinblastine (Velban®), dacarbazine (DTIC-Dome®)
- AV-PC: doxorubicin (Adriamycin®), vincristine (Oncovin®), prednisone and cyclophosphamide (Cytoxan®)
- ABVE: doxorubicin (Adriamycin®), bleomycin (Blenoxane®), vincristine (Oncovin®), and etoposide (Etopophos®, Toposar®, VePesid®, VP-16)
- ABVE-PC: doxorubicin (Adriamycin®), bleomycin (Blenoxane®), vincristine (Oncovin®), etoposide (Etopophos®, Toposar®, VePesid®, VP-16), prednisone and cyclophosphamide (Cytoxan®)
- BEACOPP: bleomycin (Blenoxane®), etoposide (Etopophos®, Toposar®, VePesid®, VP-16), doxorubicin (Adriamycin®), cyclophosphamide (Cytoxan®), vincristine (Oncovin®), procarbazine (Matulane®) and prednisone
- OEPA: vincristine (Oncovin®), etoposide (Etopophos®, Toposar®, VePesid®, VP-16), prednisone, and doxorubicin (Adriamycin®)
Clinical Trials
A clinical trial may be an option when it comes to finding the right treatment for your child’s cancer. Your child may have access to new or improved therapies under study and not yet on the market. Discuss with your child’s doctor the possibility of taking part in a clinical trial, where treatment is administered in a safe, closely monitored environment.
Advances in treating childhood Hodgkin lymphoma, which have improved the cure rate and quality of life for survivors, are due, in large part, to the research of pediatric cooperative groups. The focus of ongoing research and clinical trials is to
- Further improve the cure rate, especially for children with advanced Hodgkin’s lymphoma
- Minimize the risk of long-term and late effects associated with treatment (for example, infertility, impaired cardiac function and secondary cancers).
Survivorship and Special Healthcare Needs
After treatment, most children can expect to have full and productive lives. Many survivors return to school, attend college, enter the workforce, marry and become parents.
You may want to consider a survivorship program for your child that focuses on life after cancer. Many comprehensive cancer centers around the country offer these programs.
Follow-Up Care
Your child should visit his or her pediatrician or doctor at least once a year for a complete physical exam and any additional needed tests. Your child’s oncologist should also regularly examine your child.
Regular doctor visits are encouraged to:
- Enable doctors to assess the full effect of therapy
- Detect and treat disease recurrence
- Identify and manage long-term and late effects of treatment
Your pediatrician should recommend a schedule for having your child’s learning skills assessed. If your child appears to be experiencing learning disabilities, special education methods can help.
Coordination between your child’s pediatrician and oncologist is important for the best care possible. Some treatment centers offer comprehensive follow-up care clinics for childhood cancer survivors.
Long-Term and Late Effects of Treatment
Some side effects of cancer treatment, such as fatigue, can linger for months or years after therapy. Some medical conditions like heart disease and other cancers may not appear until years after treatment ends. Long-term and late effects can affect your child’s physical, mental and cognitive (brain function) health.
Most childhood survivors of lymphoma don’t develop significant long-term or late effects of treatment. However, for some patients the effects can be severe.
Long-Term and Late Effects of Chemotherapy
Children treated for lymphoma may be at increased risk for:
- Fatigue
- Growth delays
- Thyroid dysfunction
- Hearing loss
- A secondary cancer
Some long-term and late effects become evident with maturation (puberty), growth and the normal aging process. Early intervention and healthy lifestyle practices (not smoking, good nutrition, exercise, regular screenings and follow-up) may have a positive effect on the occurrence and/or severity of long-term and late effects.
Long-Term and Late Effects of Radiation Therapy
Girls (as well as women under age 30) who had radiation to the breast area are at risk for developing breast cancer 15 to 20 years after treatment. Male survivors of childhood cancer are at risk for developing secondary cancers, but they don’t have as high a risk for developing breast cancer as female childhood cancer survivors do.
Girls who had radiation therapy in the chest (mediastinal) area should:
- Perform monthly breast self-examinations
- Have yearly breast examinations by a healthcare professional
- Have early baseline mammograms within 8 to 10 years after therapy or by age 40, whichever occurs earlier.
- Have breast MRIs in addition to mammography for women who received irradiation of the chest when they were between 10 and 30 years of age.
Both girls and boys who’ve undergone mediastinal radiation therapy should have baseline testing for heart function. This should be followed by testing every three to five years after treatment or more regularly if any abnormalities are found.
Returning to School
Learning disabilities can begin during treatment or appear months or years after treatment. Educate family members, friends, school personnel and healthcare providers about your child’s possible long-term and late effects of treatment. Talk with teachers about your child’s needs before he or she returns to school. Work with your child’s teachers and medical providers to develop a program tailored to his or her needs that features baseline testing, special accommodations and long-term planning.
Non hodgkin’s lymphoma
Non-Hodgkin lymphomas begin when a type of white blood cell, called a T cell or B cell, becomes abnormal. The cell divides again and again, making more and more abnormal cells. These abnormal cells can spread to almost any other part of the body. Most of the time, doctors don’t know why a person gets non-Hodgkin lymphoma. You are at increased risk if you have a weakened immune system or have certain types of infections.
Non-Hodgkin lymphoma (NHL) is one of the most common cancers in the United States, accounting for about 4% of all cancers. The American Cancer Society’s most recent estimates for non-Hodgkin’s lymphoma are for 2017:
- About 72,240 people (40,080 males and 32,160 females) will be diagnosed with NHL. This includes both adults and children.
- About 20,140 people will die from this cancer (11,450 males and 8,690 females).
The average American’s risk of developing non-Hodgkin’s lymphoma during his or her lifetime is about 1 in 50. But each person’s risk can be affected by a number of risk factors.
Non-Hodgkin’s lymphoma can occur at any age. In fact, it is one of the more common cancers among children, teens, and young adults. Still, the risk of developing non-Hodgkin’s lymphoma increases throughout life, and more than half of patients are 65 or older at the time of diagnosis. The aging of the American population is likely to lead to an increase in non-Hodgkin’s lymphoma cases during the coming years.
How Many People Survive 5 Years Or More after Being Diagnosed with non-Hodgkin Lymphoma?
Based on data from SEER 18 2007-2013, percent surviving 5 Years is 71.0% 8
Non-Hodgkin’s lymphoma Survival by Stage
Cancer stage at diagnosis, which refers to extent of a cancer in the body, determines treatment options and has a strong influence on the length of survival. In general, if the cancer is found only in the part of the body where it started it is localized (sometimes referred to as stage 1). If it has spread to a different part of the body, the stage is regional or distant. For non-Hodgkin lymphoma, 27.6% are diagnosed at the local stage. The 5-year survival for localized non-Hodgkin lymphoma is 82.9%.
Types of Non-Hodgkin Lymphoma
There are many different types of non-Hodgkin lymphoma (NHL), so classifying it can be quite confusing (even for doctors). Several different systems have been used, but the most recent system is the World Health Organization (WHO) classification. The WHO system groups lymphomas based on:
- The type of lymphocyte the lymphoma starts in
- How the lymphoma looks under a microscope
- The chromosome features of the lymphoma cells
- The presence of certain proteins on the surface of the cells
The more common types of lymphoma are listed below according to whether they start in B lymphocytes (B cells) or T lymphocytes (T cells). Some rarer forms of non-Hodgkin lymphoma are not listed here.
B-cell lymphomas
B-cell lymphomas make up most (about 85%) of NHL in the United States.
Diffuse large B-cell lymphoma (DLBCL)
This is the most common type of NHL in the United States, accounting for about 1 out of every 3 lymphomas. The lymphoma cells look fairly large when seen with a microscope.
Diffuse large B-cell lymphoma can affect people of any age, but it occurs mostly in older people. (The average age at the time of diagnosis is mid-60s.) It usually starts as a quickly growing mass in a lymph node deep inside the body, such as in the chest or abdomen, or in a lymph node you can feel, such as in the neck or armpit. It can also start in other areas such as the intestines, bones, or even the brain or spinal cord.
Diffuse large B-cell lymphoma tends to be a fast-growing (aggressive) lymphoma, but it often responds well to treatment. Overall, about 3 out of 4 people will have no signs of disease after the initial treatment, and many are cured.
A common subtype of diffuse large B-cell lymphoma is primary mediastinal B-cell lymphoma. This type of lymphoma occurs mostly in young women. It starts in the mediastinum (the area in the middle of the chest behind the breastbone). It can grow quite large and can cause trouble breathing because it often presses on the windpipe (trachea) leading into the lungs. It can also block the superior vena cava (the large vein that returns blood to the heart from the arms and head), which can make the arms and face swell. This is a fast-growing lymphoma, but it usually responds well to treatment.
There are several other subtypes of diffuse large B-cell lymphoma, but these are rare.
Follicular lymphoma
About 1 out of 5 lymphomas in the United States is a follicular lymphoma. This is usually a slow-growing (indolent) lymphoma, although some follicular lymphomas can grow quickly.
The average age for people with this lymphoma is about 60. It’s rare in very young people. Usually, this lymphoma occurs in many lymph node sites throughout the body, as well as in the bone marrow.
Follicular lymphomas often respond well to treatment, but they are hard to cure. These lymphomas may not need to be treated when they are first diagnosed. Instead, treatment may be delayed until the lymphoma starts causing problems. Over time, some follicular lymphomas turn into a fast-growing diffuse large B-cell lymphoma.
Chronic lymphocytic leukemia (CLL) /small lymphocytic lymphoma (SLL)
Chronic lymphocytic leukemia (CLL) and small lymphocytic lymphoma (SLL) are closely related diseases. In fact, many doctors consider them different versions of the same disease. The same type of cancer cell (known as a small lymphocyte) is seen in both chronic lymphocytic leukemia (CLL) and small lymphocytic lymphoma (SLL) . The only difference is where the cancer cells are found. In chronic lymphocytic leukemia, most of the cancer cells are in the blood and bone marrow. In small lymphocytic lymphoma, the cancer cells are mainly in the lymph nodes and spleen.
Both chronic lymphocytic leukemia and small lymphocytic lymphoma are usually slow-growing (indolent) diseases, although chronic lymphocytic leukemia, which is much more common, tends to grow more slowly. Treatment is the same for chronic lymphocytic leukemia and small lymphocytic lymphoma. They are usually not curable with standard treatments, but many people can live a long time (even decades) with them. Sometimes, these can turn into a more aggressive (fast-growing) type of lymphoma over time.
Mantle cell lymphoma (MCL)
About 5% of lymphomas are mantle cell lymphomas. Mantle cell lymphoma is much more common in men than in women, and it most often appears in people older than 60. When mantle cell lymphoma is diagnosed, it is usually widespread in the lymph nodes, bone marrow, and often the spleen.
Mantle cell lymphoma can be challenging to treat. It tends to grow faster than indolent (slow-growing) lymphomas, but it doesn’t usually respond to treatment as well as aggressive (fast-growing) lymphomas. But newer treatments might offer a better chance for long-term survival for patients now being diagnosed.
Marginal zone lymphomas
Marginal zone lymphomas account for about 5% to 10% of lymphomas. They tend to be slow-growing (indolent). The cells in these lymphomas look small under the microscope. There are 3 main types of marginal zone lymphomas:
Extranodal marginal zone B-cell lymphoma, also known as mucosa-associated lymphoid tissue (MALT) lymphoma: This is the most common type of marginal zone lymphoma. It starts in places other than the lymph nodes (extranodal). Most MALT lymphomas start in the stomach and are linked to infection by Helicobacter pylori (the bacteria that causes many stomach ulcers). MALT lymphoma might also start in the lung, skin, thyroid, salivary glands, or tissues surrounding the eye. Usually the lymphoma stays in the area where it begins and is not widespread. Many of these other MALT lymphomas have also been linked to infections with bacteria or viruses.
The average age of people with MALT lymphoma at the time of diagnosis is about 60. This lymphoma tends to grow slowly and is often curable if found early. Doctors often use antibiotics as the first treatment for MALT lymphoma of the stomach, because treating the Helicobacter pylori infection often cures the lymphoma.
Nodal marginal zone B-cell lymphoma: This is a rare disease, found mainly in older women. It starts and usually stays in the lymph nodes, although lymphoma cells can also sometimes be found in the bone marrow.
This lymphoma tends to be slow-growing (although not usually as slow as MALT lymphoma), and is often curable if found early.
Splenic marginal zone B-cell lymphoma: This is a rare lymphoma. Most often the lymphoma is found only in the spleen and bone marrow.
It is most common in older men, and often causes fatigue and discomfort due to an enlarged spleen. Because the disease is slow-growing, it might not need to be treated unless the symptoms become troublesome. This type of lymphoma has been linked to infection with the hepatitis C virus.
Burkitt lymphoma
This fast-growing lymphoma is named after the doctor who first described this disease in African children and young adults. It makes up about 1% to 2% of all lymphomas. It is rare in adults, but is more common in children. It’s also much more common in males than in females.
The cells in Burkitt lymphoma are medium-sized. A similar kind of lymphoma, Burkitt-like lymphoma, has slightly larger cells. Because it is hard to tell these lymphomas apart, the WHO classification combines them.
Different varieties of this lymphoma are seen in different parts of the world:
- In the African (or endemic) variety, Burkitt lymphoma often starts as a tumor of the jaw or other facial bones. It is often linked to infection with the Epstein-Barr virus (EBV, which can also cause infectious mononucleosis or “mono”). This type of Burkitt lymphoma is rare in the United States.
- In the type seen more often in the United States, the lymphoma usually starts in the abdomen (belly), where it forms a large tumor. It can also start in the ovaries, testicles, or other organs, and can spread to the brain and spinal fluid. It is not usually linked to EBV infection.
Burkitt lymphoma grows very quickly, so it needs to be treated right away. But more than half of patients can be cured by intensive chemotherapy.
Lymphoplasmacytic lymphoma (Waldenstrom macroglobulinemia)
This slow-growing lymphoma is not common, accounting for only 1% to 2% of lymphomas. The lymphoma cells are small and found mainly in the bone marrow, lymph nodes, and spleen.
Hairy cell leukemia
Despite the name, hairy cell leukemia (HCL) is sometimes considered to be a type of lymphoma. It is rare – about 700 people in the United States are diagnosed with it each year. Men are much more likely to get HCL than women, and the average age at diagnosis is around 50.
The cells are small B lymphocytes with projections coming off them that give them a “hairy” appearance. They are typically found in the bone marrow and spleen and in the blood.
Hairy cell leukemia is slow-growing, and some people may never need treatment. An enlarging spleen or low blood cell counts (due to cancer cells invading the bone marrow) are the usual reasons to begin treatment. If treatment is needed, it’s usually very effective.
Primary central nervous system (CNS) lymphoma
This lymphoma involves the brain or spinal cord (the central nervous system, or CNS). The lymphoma is also sometimes found in tissues around the spinal cord or the eye. Over time, it tends to become widespread in the central nervous system.
Primary CNS lymphoma is rare overall, but it’s more common in older people and in people with immune system problems, such as those who have had an organ transplant or who have AIDS. Most people develop headaches and confusion. They can also have vision problems; weakness or altered sensation in the face, arms, or legs; and in some cases, seizures.
Historically, the outlook for patients with primary CNS lymphoma has not been as good as for many other lymphomas, but this is at least partly because people with CNS lymphoma tend to be older or have other serious health problems. Still, some people do well with treatment.
T-cell lymphomas
T-cell lymphomas make up less than 15% of non-Hodgkin lymphomas in the United States. There are many types of T-cell lymphoma, but they are all fairly rare.
Precursor T-lymphoblastic lymphoma/leukemia
This disease accounts for about 1% of all lymphomas. It can be considered either a lymphoma or a type of acute lymphoblastic leukemia (ALL), depending on how much of the bone marrow is involved (leukemias have more bone marrow involvement). The cancer cells are very early forms of T cells.
This lymphoma often starts in the thymus (a small organ behind the breastbone and in front of the heart, which is where many T cells are made), and can grow into a large tumor in the mediastinum (the area between the lungs). This can cause trouble breathing and swelling in the arms and face.
This lymphoma is most common in teens or young adults, with males being affected more often than females.
This lymphoma is fast-growing, but if it hasn’t spread to the bone marrow when it is first diagnosed, the chance of cure with chemotherapy is quite good.
Often, the lymphoma form of this disease is treated in the same way as the leukemia form. For more information, see Acute Lymphocytic Leukemia (Adults).
Peripheral T-cell lymphomas
These uncommon types of lymphomas develop from more mature forms of T cells.
Cutaneous T-cell lymphomas (mycosis fungoides, Sezary syndrome, and others): These lymphomas start in the skin. Skin lymphomas account for about 5% of all lymphomas. They are described in Lymphoma of the Skin.
Adult T-cell leukemia/lymphoma: This lymphoma is caused by infection with a virus called HTLV-1. It is rare in the United States, and much more common in Japan, the Caribbean, and parts of Africa – where infection with HTLV-1 is more common. It can affect the bone marrow (where new blood cells are made), lymph nodes, spleen, liver, skin, and other organs. There are 4 subtypes:
- The smoldering subtype tends to grow slowly and has a good prognosis.
- The chronic subtype also grows slowly and has a good prognosis.
- The acute subtype is the most common. It grows quickly like acute leukemia, so it needs to be treated right away.
- The lymphoma subtype grows more quickly than the chronic and smoldering types, but not as fast as the acute type.
Angioimmunoblastic T-cell lymphoma: This lymphoma accounts for about 4% of all lymphomas. It is more common in older adults. It tends to involve the lymph nodes as well as the spleen or liver, which can become enlarged. People with this lymphoma usually have fever, weight loss, and skin rashes and often develop infections. This lymphoma often progresses quickly. Treatment is often effective at first, but the lymphoma tends to come back (recur).
Extranodal natural killer/T-cell lymphoma, nasal type: This rare type often involves the upper airway passages, such as the nose and upper throat, but it can also invade the skin, digestive tract, and other organs. It is much more common in parts of Asia and South America. Cells of this lymphoma are similar in some ways to natural killer (NK) cells, another type of lymphocyte.
Enteropathy-associated intestinal T-cell lymphoma (EATL): EATL is a lymphoma that occurs in the lining of the intestine. This lymphoma is most common in the small intestine, but can also occur in the colon. Symptoms can include severe abdominal (belly) pain, nausea, and vomiting. There are 2 subtypes of this lymphoma:
- Type I EATL occurs in some people with celiac disease (also called gluten-sensitive enteropathy). Celiac disease is an autoimmune disease in which eating gluten, a protein found mainly in wheat and barley, causes the immune system to attack the lining of the intestine and other parts of the body. Type I EATL is rare among people who have had celiac disease since childhood, and is more common in people diagnosed as older adults. This lymphoma is more common in men than women.
- Type II EATL is not linked to celiac disease and is less common than type I.
Anaplastic large cell lymphoma (ALCL): About 2% of lymphomas are of this type. It is more common in young people (including children), but it can also affect older adults. This type of lymphoma tends to be fast-growing, but many people with this lymphoma can be cured.
There are different forms of ALCL:
- Primary cutaneous ALCL only affects the skin. This is discussed in more detail in Lymphoma of the Skin.
- Systemic ALCL can affect the lymph nodes and other organs, including the skin. Systemic ALCL is divided into 2 types based on whether the lymphoma cells have a change in the ALK gene. ALK-positive ALCL is more common in younger people and tends to have a better prognosis (outlook) than the ALK-negative type.
- Breast implant-associated ALCL is a rare type of ALCL that can develop in the breasts of women who have had implants. It seems to be more likely to occur if the implant surfaces are textured (as opposed to smooth).
Peripheral T-cell lymphoma, not otherwise specified (PTCL, NOS): This name is given to T-cell lymphomas that don’t readily fit into any of the groups above. Most people diagnosed with these lymphomas are in their 60s. These lymphomas often involve the lymph nodes, but they can affect the skin, bone marrow, spleen, liver, and digestive tract, as well. As a group, these lymphomas tend to be widespread and grow quickly. Some patients respond well to chemotherapy, but over time these lymphomas tend to become harder to treat.
Non hodgkin’s lymphoma signs and symptoms
The most common symptom of non-Hodgkin lymphoma is a painless swelling in a lymph node, usually in the neck, armpit or groin.
Some people have no symptoms and the disease may only be discovered during a routine medical examination or while the patient is under care for an unrelated condition.
B Symptoms. Fever, drenching night sweats and loss of more than 10 percent of body weight over six months are sometimes termed “B symptoms” and are significant to the prognosis and staging of the disease. Other non-Hodgkin’s lymphoma symptoms, such as itching and fatigue, do not have the same prognostic importance as the symptoms designated as B symptoms. Further, they are not considered to be B symptoms.
Non-Hodgkin lymphoma can cause many symptoms, such as:
- Painless swelling in one or more lymph node(s)
- Unexplained weight loss
- Fever
- Soaking night sweats
- Coughing, trouble breathing or chest pain
- Weakness and tiredness that don’t go away
- Loss of appetite
- Pain, swelling or a feeling of fullness in the abdomen (due to an enlarged spleen)
- Itchy skin
- Enlargement of the spleen or liver
- Rashes or skin lumps
What Causes non-Hodgkin’s lymphoma
Non-Hodgkin’s lymphoma usually starts with an abnormal change in a white cell in a lymph node or lymphoid tissue called a lymphocyte. It can start in one of three major types of lymphocytes:
- B lymphocytes (B cells), which produce antibodies to help combat infections
- T lymphocytes (T cells), which have several functions, including helping B lymphocytes make antibodies
- Natural killer (NK) cells, which attack virus-infected cells or tumor cells
About 85 percent of non-Hodgkin’s lymphoma cases start in the B cells. Your doctor plans your treatment according to the type of cell your non-Hodgkin’s lymphoma developed in.
The abnormal lymphocyte grows out of control and produces more abnormal cells like it.
- These abnormal lymphocytes (lymphoma cells) accumulate and form masses (tumors). If non-Hodgkin’s lymphoma isn’t treated, the cancerous cells crowd out normal white cells, and the immune system can’t guard against infection effectively.
- Non-Hodgkin’s lymphoma that develops in or spreads to other areas of the body where lymphoid tissue is found, such as the spleen, digestive tract and bone marrow, is called primary extranodal lymphoma.
- Non-Hodgkin’s lymphoma is classified into more than 30 different subtypes. Doctors classify the non-Hodgkin’s lymphoma subtypes into categories that describe how rapidly or slowly the disease is progressing:
- Aggressive non-Hodgkin’s lymphoma
- Indolent (slow-growing) non-Hodgkin’s lymphoma
Risk Factors non-Hodgkin’s lymphoma
The exact cause of non-Hodgkin’s lymphoma is not known but there are risk factors that may increase a person’s likelihood of developing the disease.
Immune suppression is one of the most clearly established risk factors for non-Hodgkin’s lymphoma. People with autoimmune disease, acquired immunodeficiencies including human immunodeficiency virus infection and acquired immune deficiency syndrome (HIV/AIDS), and organ transplant recipients have an elevated risk for non-Hodgkin’s lymphoma. In addition, factors that suppress the immune system, such as chemical exposures or treatments for autoimmune diseases, may contribute to the development of non-Hodgkin’s lymphoma.
Farming communities have a higher incidence of non-Hodgkin’s lymphoma. Some studies suggest that specific ingredients in herbicides and pesticides such as organochlorine, organophosphate and phenoxy acid compounds, are linked to lymphoma. The number of lymphoma cases caused by such exposures has not been determined. More studies are needed to understand these associations.
Exposure to certain viruses and bacteria is associated with non-Hodgkin’s lymphoma. It is thought that infection with either a virus or a bacterium can lead to intense lymphoid cell proliferation, increasing the probability of a cancer-causing event in a cell. Here are some examples:
- Epstein-Barr virus (EBV) infection
- Human T-cell lymphotropic virus-1 (HTLV-1)
- Human immunodeficiency virus infection and acquired immune deficiency syndrome (HIV/AIDS)
- The bacterium Helicobacter Pylori (H Pylori)
- Hepatitis C
Other conditions, such as Sjögren syndrome, Wiskott-Aldrich syndrome and Klinefelter syndrome can predispose individuals to later development of non-Hodgkin’s lymphoma.
How non-Hodgkin lymphoma is diagnosed
The only way to confirm a diagnosis of non-Hodgkin lymphoma is by carrying out a biopsy.
This is a minor surgical procedure where a sample of affected lymph node tissue is removed and studied in a laboratory.
Lymph Node Biopsy
Diagnosing non-Hodgkin lymphoma usually involves performing a lymph node biopsy. If the biopsy confirms that you have the disease, your doctor performs additional tests to stage the lymphoma.
A lymph node biopsy’s purpose is to confirm a diagnosis and:
- Identify your non-Hodgkin’s lymphoma subtype
- Develop a treatment plan
Lab Tests to Confirm a Diagnosis
After your doctor takes samples of your lymph node and tissues, a hematopathologist examines them under a microscope to look for identifying characteristics of NHL. He or she confirms a diagnosis and identifies the NHL subtype. A hematopathologist is a specialist who studies blood cell diseases by looking at samples of blood and bone marrow cells and other tissues.
The hematopathologist uses one or more lab tests such as those below to examine your cells:
- Immunophenotyping
- Flow cytometry
- Cytogenetic analysis
- Gene expression profiling and microarray analysis
- Polymerase chain reaction (PCR)
Since NHL is a difficult disease to diagnose, you may want to get a second medical opinion by an experienced hematopathologist before you begin treatment. Some types of NHL can be confused with each other. The appropriate treatment depends on having the correct diagnosis.
Staging Tests
Once your doctor confirms an NHL diagnosis, he or she runs more tests to stage your disease. Staging identifies the extent of your disease and where it’s located in your body.
Staging tests include:
- A physical exam
- Imaging tests
- Blood tests
- Bone marrow tests
Imaging Tests
Your doctor conducts one or more imaging tests (also called diagnostic radiology), along with a physical exam, to look for:
- The location and distribution of lymph node enlargement
- Whether organs other than the lymph nodes are involved
- If there are very large masses of tumors in one site or another.
Imaging tests may include:
- Chest x-rays
- CT (computed tomography) scan
- FDG-PET (fluorodeoxyglucose (FDG) positron emission tomography) scan
- Magnetic resonance imaging (MRI)
- PET-CT scan
Blood Tests
After your blood is taken, it’s sent to a lab for a complete blood count (CBC) and more blood work. Blood tests are used to:
- Determine whether lymphoma cells are present in the blood and if the special proteins (called “immunoglobulins”) made by lymphocytes are either deficient or abnormal
- Check indicators of disease severity by examining blood protein levels, uric acid levels and erythrocyte sedimentation rate (ESR)
- Assess kidney and liver functions
- Measure two important biological markers, lactate dehydrogenase (LDH) and beta2-microglobulin which are helpful prognostic indicators for several NHL subtypes
A complete blood count (CBC) may show:
- Anemia (low red blood cell counts)
- Neutropenia (low levels of neutrophils, a type of white blood cells)
- Thrombocytopenia (low platelet levels)
Bone Marrow Biopsy
Most patients diagnosed with NHL undergo a bone marrow biopsy to make sure there is no spread of the disease to the bone marrow and to evaluate the use of specific therapies including radioimmunotherapy (a combination of radiation therapy and immunotherapy). A bone marrow biopsy may not always be required for patients with early-stage disease who also have low-risk features, for example, NHL with no B symptoms and no large masses.
Other Tests for Specific Subtypes
Certain tests are performed for specific subtypes only and not necessary for all patients with NHL. They include:
- Full evaluation of the gastrointestinal (GI) tract, including upper and lower endoscopies for patients who have disease involving the GI tract, such as MALT lymphoma
- Colonoscopy for patients with mantle cell lymphoma (routine colonoscopy is important for all persons beginning at age 50, or earlier if there is a family history of colon cancer)
- Testicular ultrasound for patients who have a testicular mass
- Spinal tap (lumbar puncture) and/or MRI of the brain or spinal column may be required for patients with certain subtypes or symptoms that suggest central nervous system involvement.
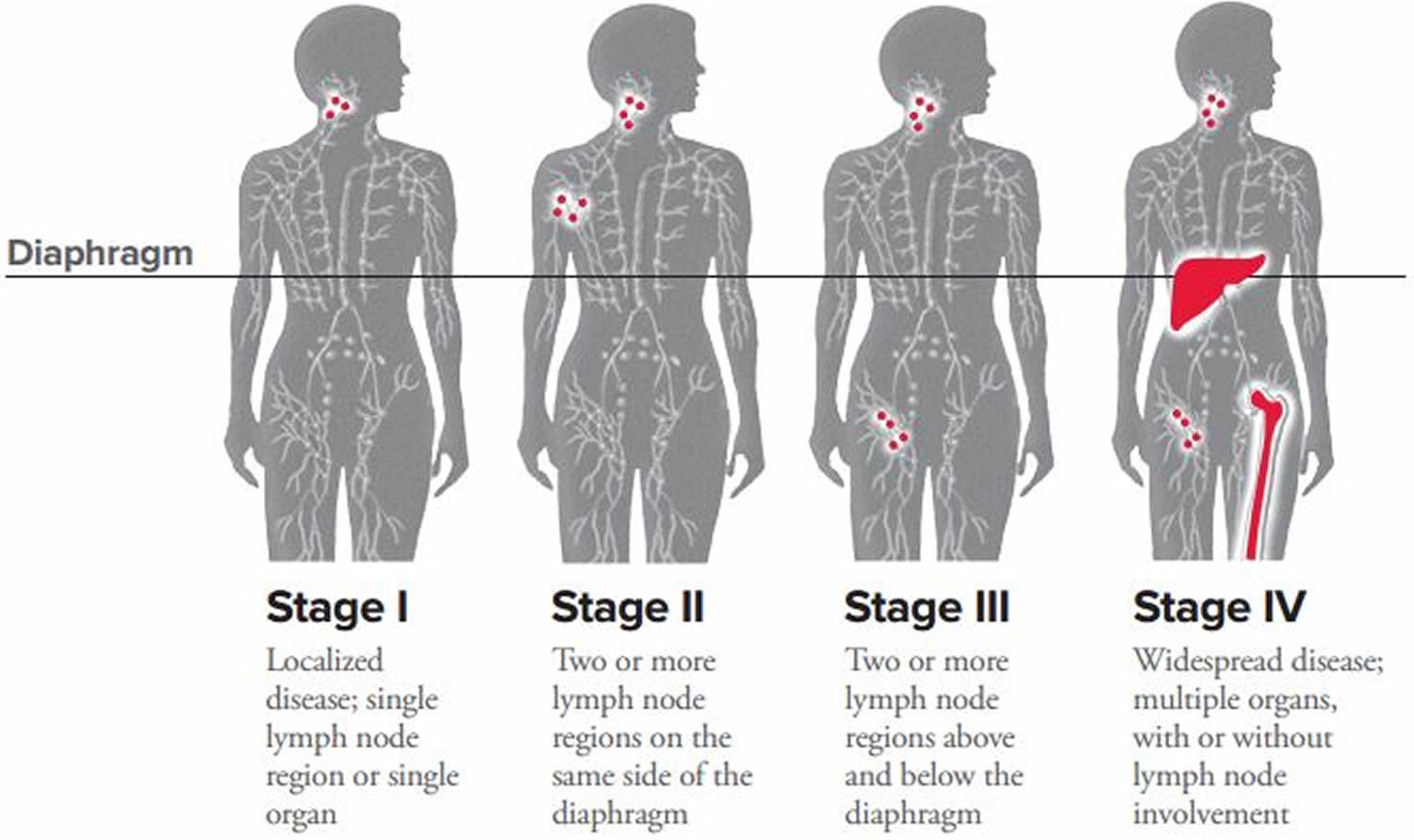
Non-Hodgkin’s lymphoma Staging
Your doctor will determine the extent of your disease’s progression by staging. Staging helps your doctor predict the disease’s progression and develop a treatment plan.
NHL doesn’t always begin in stage I and spread to more advanced stages. More than half of all patients with intermediate or aggressive disease and more than 80 percent of all patients with indolent disease are diagnosed with stage III or IV NHL. And if someone is diagnosed in stage IV, it doesn’t mean that the disease is incurable – it may be highly curable depending on the subtype. “Stage IV” does not have the same implications in NHL as it does for many other cancers.
| Stage | Number and Location of Affected Lymph Nodes and Organs |
|---|---|
| Stage I | Involvement of one lymph node or a group of adjacent nodes |
| Stage II | Involvement of two or more lymph node regions on the same side of the diaphragm |
| Stage III | Involvement of two or more lymph node regions above and below the diaphragm (for example, neck, chest and abdomen) |
| Stage IV | Involvement of lymph node regions on both sides of the diaphragm and involvement of organs such as the lungs, liver or bones |
Categories A, B, X and E
The four stages of NHL can be divided into categories:
- A Category: No symptoms
- B Category: Presence of fever, drenching sweats, loss of more than 10 percent of body weight over the previous six months (without dieting)
- X Category: Bulky disease. This is a nodal mass whose greatest size is usually more than 10 cm or more than onethird of the chest diameter by x-ray
- E Category: Involvement of organs or tissues beyond the lymph system
For example, stage IIB indicates that the patient has
- Two lymph node sites near each other with disease involvement (for example, enlarged lymph nodes in the neck and near the collarbone, or in the neck and the armpit)
- Fever, excessive sweating and/or weight loss (any one of these symptoms).
When all the diagnostic and staging tests are completed, the doctor will evaluate the information, identify the NHL subtype, determine which areas of the body are involved and begin to discuss treatment options with the patient.
Non-Hodgkin’s lymphoma Subtypes
More than 60 specific NHL subtypes have been identified and assigned names by the World Health Organization (WHO). NHL subtypes are categorized by the characteristics of the lymphoma cells, including their appearance, the presence of proteins on the surface of the cells and their genetic features. It’s important to know your subtype since it plays a large part in determining the type of treatment you’ll receive. A hematopathologist, a doctor who specializes in the diagnosis of blood disorders and blood cancers, should review your biopsy specimens.
Specialists further characterize the NHL subtypes according to how the disease progresses:
- Aggressive lymphomas are fast-moving and account for about 60 percent of all NHL cases. Diffuse large B-cell lymphoma (DLBCL) is the most common aggressive NHL subtype.
- Indolent lymphomas are slow-moving and tend to grow more slowly and have fewer signs and symptoms when first diagnosed. Slow-growing or indolent subtypes represent about 40 percent of all NHL cases. Follicular lymphoma (FL) is the most common subtype of indolent NHL.
The treatments for aggressive and indolent lymphomas are different. When a patient’s rate of disease progression is between indolent and aggressive, he or she is considered to have “intermediate grade” disease. Some cases of indolent NHL can transform into aggressive NHL.
| Most Common Subtypes of Non-Hodgkin Lymphoma |
|---|
Aggressive
|
Indolent
|
Below are the NHL diagnostic designations of the subtypes for non-Hodgkin lymphoma. The descriptive part of the names (eg, follicular, mantle cell or marginal zone) in some disease subtypes refers to the specific areas of the lymph nodes (the follicle, mantle and marginal zones) where the lymphoma appears to have originated.
| Diagnostic Designations for Non-Hodgkin Lymphoma (NHL): Subtypes |
|---|
Mature B-cell lymphomas
|
Mature T-cell and NK-cell lymphomas
|
Non-Hodgkin’s lymphoma Treatment
It’s important that your doctor is experienced in treating patients with non-Hodgkin lymphoma (NHL) or works in consultation with an NHL specialist. This type of specialist is usually called a hematologist oncologist.
Types of Treatment
Doctors use several types of approaches and treatment combinations for NHL, some at different stages:
- Chemotherapy and other drug therapy
- Radiation therapy, usually combined with chemotherapy
- Stem cell transplantation
- Watch-and-wait
- Your doctor may suggest that you participate in a clinical trial. Clinical trials can involve therapy with new drugs and new drug combinations or new approaches to stem cell transplantation.
There can also be vast differences between treatment for aggressive NHL and treatment for indolent NHL.
Pretreatment Considerations
Adults of childbearing age and parents of children diagnosed with HL should ask their doctors for information that may lessen the risk for infertility.
Finding the Best Treatment Approach
The goal of non-Hodgkin’s lymphoma treatment is to destroy as many lymphoma cells as possible to induce a complete remission (no trace of the disease). Patients who go into remission are sometimes cured of the disease.
Treatment can keep non-Hodgkin’s lymphoma in check for many years, even if tests show some lingering lymphoma cells. This is called partial remission.
The treatment your doctor recommends is based on several factors, including:
- Your disease subtype
- Whether your disease is aggressive (fast growing) or indolent (slow growing)
- Your disease stage and category
- Whether the lymphoma is in areas of your body other than your lymph nodes (extranodal involvement)
- Your overall health and whether you have any conditions like heart disease, kidney disease, lung disease, diabetes or anemia
As you develop a treatment plan with your doctor, be sure to discuss:
- The results you can expect from treatment
- Potential side effects, including long-term and late-term effects
- The possibility of participating in a clinical trial, where you’ll have access to advanced medical treatment that may be more beneficial to you than standard treatment
You may find it helpful to bring a loved one with you to your doctor’s visits for support, to take notes and ask follow-up questions. It’s a good idea to prepare questions you’d like to ask when you visit your doctor. You can also record your conversations with your doctor and listen more closely when you get home.
Treatment for Aggressive Non-Hodgkin’s lymphoma Subtypes
Aggressive non-Hodgkin lymphoma (NHL) progresses rapidly. It makes up about 60 percent of all NHL cases in the United States. Aggressive subtypes include:
- AIDS-associated lymphoma
- Burkitt lymphoma
- Central nervous system (CNS) lymphoma
- Diffuse large B-cell lymphoma (DLBCL)
- Mantle cell lymphoma
- Peripheral T-cell lymphoma (PTCL)
Patients with fast-growing NHL are frequently treated with chemotherapy that consists of four or more drugs. In most cases, this is the combination therapy called R-CHOP (rituximab [Rituxan®], cyclophosphamide [Cytoxan®], doxorubicin [hydroxydoxorubicin], Oncovin® [vincristine] and prednisone). This intensive, multidrug chemotherapy can be very effective for aggressive lymphoma, and cures have been achieved. Chemotherapy can be supplemented by radiation therapy in select cases, for instance, when large NHL masses are found during the diagnostic and staging process.
Treating Specific Aggressive Subtypes
AIDS-Associated Lymphoma
The types of NHL that are most often seen in people with acquired immune deficiency syndrome (AIDS) are diffuse large B-cell lymphoma, Burkitt lymphoma and primary central nervous system (CNS) lymphoma. Treatment outcomes depend on how well the patient with AIDS responds to therapy and manages the effects of chemotherapy on blood counts. Because AIDS already leads to low blood cell counts, chemotherapy must be carefully considered to determine whether the chemotherapy’s additional effects on blood levels can be managed. The number of people developing AIDS-associated NHL has decreased in the last several years because of improved treatment of HIV, the virus that can lead to AIDS.
Burkitt Lymphoma
This B-cell subtype is considered to be highly aggressive. It may involve the jaw, bones of the face, bowel, kidneys, ovaries, bone marrow, blood, central nervous system (CNS) and other organs. Burkitt lymphoma was named after Dr. Dennis Burkitt, a surgeon who first identified the disease in children in Africa. In Africa, the disease usually appears in children as a mass in a facial bone, especially the jaw.
Doctors typically use highly aggressive chemotherapy to treat this subtype of NHL. Commonly used regimens include:
- CODOX-M/IVAC (cyclophosphamide, vincristine, doxorubicin and high-dose methotrexate) alternating with IVAC (ifosfamide, etoposide and high-dose cytarabine)
- Hyper-CVAD (hyperfractionated cyclophosphamide, vincristine, doxorubicin and dexamethasone) alternating with methotrexate and cytarabine
- DA-EPOCH-R (dose-adjusted etoposide, prednisone, vincristine, cyclophosphamide, doxorubicin plus rituximab)
Participation in clinical trials is recommended for all patients with Burkitt lymphoma.
Central Nervous System Lymphoma
There are two types of central nervous system (CNS) lymphoma: primary and secondary. Primary CNS lymphoma starts in the brain and/or the spinal cord. It is often a feature of AIDS-associated lymphoma, although it may be related to other NHL subtypes as well. Secondary CNS lymphoma starts in another area of the body and spreads to the brain and/or spinal cord.
Both primary and secondary CNS lymphomas are uncommon. Standard treatment may include chemotherapy, glucocorticoid drugs and/or radiation therapy. Immunotherapy and high-dose chemotherapy with stem cell transplantation are being studied in clinical trials. Read more>>
Diffuse Large B-Cell Lymphoma
Diffuse large B-cell lymphoma (DLBCL) is the most common NHL subtype, making up about 30 percent of all NHL cases in the United States. It affects mostly middle-aged and older adults. DLBCL usually starts in lymph nodes in the neck or abdomen and is characterized by masses of large B cells (lymphocytes). DLBCL grows rapidly and frequently involves the spleen, liver, bone marrow or other organs.
For some patients, DLBCL may be the initial diagnosis. For other patients, their indolent lymphomas such as small lymphocytic lymphoma or follicular lymphoma transform and become DLBCL.
DLBCL is frequently treated with a chemotherapy regimen that is made up of four or more drugs. One regimen is R-CHOP. Another more intense regimen is DA-EPOCH-R, which is a combination of dose-adjusted etoposide (Etopophos®, VePesid®, Toposar®), prednisone, vincristine (Oncovin®), cyclophosphamide, hydroxydoxorubicin (doxorubicin) plus rituximab.
Mantle Cell Lymphoma
Mantle cell lymphoma begins in the lymph nodes and spreads to the spleen, blood, bone marrow and sometimes the esophagus, stomach and intestines. This subtype originates from a lymphocyte in the mantle zone of the lymph node. This subtype usually occurs in people over age 50 and is found in more frequently in men than in women. Standard treatment is combination chemotherapy, either with or without autologous stem cell transplantation.
Peripheral T-Cell Lymphoma
Peripheral T-cell lymphoma (PTCL) refers to a group of aggressive NHL subtypes that originate in mature T-cell lymphocytes. PTCL generally affects people age 60 and older. The most common subtypes include:
- Peripheral T-cell, not otherwise specified (PTCL NOS) – This is the most common subtype of PTCL. It often involves lymph node sites but can also involve other areas such as the liver, bone marrow, gastrointestinal track and skin.
- Anaplastic Large Cell Lymphoma (ALCL) – This subtype usually starts in the lymph nodes and can spread to the skin. There are two main subtypes of ALCL:
- Systemic ALCL ALK-1 positive anaplastic large cell lymphoma – About 80 percent of patients with this subtype are cured. This disease is more common in young people.
- Systemic ALCL ALK-1 negative anaplastic large cell lymphoma – This subtype occurs mainly in older patients. Treatment with chemotherapy or radiation therapy is often less successful and a stem cell transplant may be discussed.
- Primary cutaneous anaplastic large cell lymphoma – This subtype mostly affects the skin, but other parts of the body may be involved.
- Hepatosplenic T-cell lymphoma – This subtype of PTCL starts in the liver and spleen and usually affects young men.
- Angioimmunoblastic T-cell lymphoma – This type of T-cell lymphoma often involves lymph nodes and the bone marrow. Many patients have “paraneoplastic symptoms” including fevers, rashes and abnormal protein levels in their blood.
- Extranodal natural killer/T-cell lymphoma – This subtype of lymphoma can occur in the nasal sinuses or in other parts of the body. It is usually a very aggressive lymphoma that requires both chemotherapy and radiation.
- Enteropathy-type intestinal T-cell lymphoma – This subtype develops in the small bowel of patients with untreated celiac disease.
Peripheral T-cell lymphoma is commonly treated with the regimens used for diffuse large B-cell lymphoma. Chemotherapy with CHOP is the standard treatment for newly diagnosed peripheral T-cell lymphoma. However, clinical trials are under way to develop more effective treatment approaches, and patients are encouraged to seek out these clinical trials.
Treatment for Indolent Non-Hodgkin’s lymphoma Subtypes
Indolent non-Hodgkin lymphoma (NHL) subtypes progress slowly. They make up about 40 percent of all NHL cases in the United States. Indolent subtypes include:
- Cutaneous T-cell lymphoma (mycosis fungoides and Sézary syndrome)
- Follicular lymphoma (FL)
- Lymphoplasmacytic lymphoma and Waldenström macroglobulinemia
- Marginal zone lymphoma and mucosa-associated lymphoid tissue (MALT) lymphoma
- Small cell lymphocytic lymphoma (SLL) and chronic lymphocytic leukemia (CLL)
Treatment for indolent NHL ranges from observation with careful monitoring (the watch-and-wait approach) to aggressive therapy. Indolent NHL management or treatment is highly individual. Your doctor considers a number of factors such as:
- Prognostic factors
- Stage of disease
- Age and other medical conditions.
Treating Specific Indolent Subtypes
Cutaneous T-Cell Lymphoma (Mycosis Fungoides and Sézary Syndrome)
Cutaneous T-cell lymphomas (CTCLs) are a group of NHLs that develop primarily in the skin and may grow to involve lymph nodes, blood and other organs. This type of lymphoma originates in a T-cell. Mycosis fungoides is the most common type of CTCL, and is characterized by prominent skin involvement. When the malignant lymphocytes enter and accumulate in the blood, the disease is called Sézary syndrome.
Therapy for CTCL depends on the nature of the skin lesions and whether disease is present in the lymph nodes. Topical therapies are among the approaches used to treat the skin lesions. These include drugs applied directly to the skin combined with either ultraviolet light therapy or electron beam therapy. Ultraviolet light is used in conjunction with psoralen (a drug that becomes active when it is exposed to light); the combination therapy is often referred to as “PUVA” (psoralen and ultraviolet A) therapy.
If there is widespread involvement of lymph nodes and other sites, single- or multi-drug chemotherapy or extracorporeal photopheresis can be used. Extracorporeal photopheresis (ECP) is a method of removing blood from the body and treating it with ultraviolet light before returning it to the body. This treatment is recommended for patients either with, or at risk for, blood involvement such as that seen in Sézary syndrome.
Follicular Lymphoma (FL)
Follicular lymphoma (FL) is the second most common subtype of non-Hodgkin lymphoma (NHL), making up about 20 percent of all NHL cases. Most patients with FL are age 50 or older at diagnosis. Most follicular lymphoma cells have a specific chromosomal abnormality (a translocation between parts of chromosomes 14 and 18) that causes the production (overexpression) of the gene, BCL-2, which can make the cells resistant to therapy.
FL is a very slow-growing disease. Some patients may not need treatment for several years, whereas others may have extensive lymph node or organ involvement and need treatment right away. In a small percentage of patients, FL may transform into a more aggressive disease.
Stage I or stage II FL may be treated with:
- Watch-and-wait approach; patients with less advanced disease can be observed with periodic examinations and imaging tests.
- Radiation therapy
- Chemotherapy with rituximab (Rituxan®) followed by radiation therapy
- For patients with stage II FL who have large lymph nodes, stage III or stage IV FL or advanced-stage relapsed FL, treatment will be based on symptoms, the patient’s age and health status and the extent of the patient’s disease. Taking part in a clinical trial can also be a good treatment option. Other treatment options include:
- Radiation therapy to lymph nodes that are causing symptoms, or to a large localized mass, if one is present
- Single chemotherapy drugs in combination with rituximab. Examples of drugs used for treatment include cyclophosphamide (Cytoxan®), chlorambucil (Leukeran®) or bendamustine (Bendeka™)
- Chemotherapy combinations plus rituximab, such as R-CVP (rituximab plus cyclophosphamide, vincristine [Oncovin®], and prednisone) or R-CHOP (rituximab plus cyclophosphamide, hydroxydoxorubicin [doxorubicin], vincristine and prednisone)
- A radioactive monoclonal antibody, such as yttrium-90+ibritumomab tiuxetan (Zevalin®)
- Stem cell transplantation for some patients
- Idelalisib (Zydelig®) to treat patients who have relapsed FL and who have received at least two prior therapies
- Copanlisib (AliqopaTM) to treat adult patients with relapsed follicular lymphoma (FL) who have received at least two prior systemic therapies.
Doctors have created a scoring system called the Follicular Lymphoma International Prognostic Index that is used to predict which patients have a higher risk of the disease returning (recurring). Doctors design a treatment plan based upon the patients’ score. Factors that raise the risk for FL patients include:
- Older than 60
- Stage III or IV disease
- More than five lymph nodes involved
- An elevated level of lactic dehydrogenase (a type of protein) in the blood
- Hemoglobin concentration less than 12 g/dL.
Lymphoplasmacytic Lymphoma and Waldenström Macroglobulinemia
Lymphoplasmacytic lymphoma and Waldenström macroglobulinemia are both slow-growing types of lymphoma that originate in a B-lymphocyte precursor. Both subtypes can become more advanced and involve the lungs, the gastrointestinal tract and other organs.
One option for patients without symptoms is to take a watch-and-wait approach. Active treatment begins for patients only if symptoms develop. Therapy regimens may then include a combination of biological agents (monoclonal antibodies such as rituximab), signaling inhibitors (drugs that block cell growth and survival signals), and chemotherapy with alkylating agents such as chlorambucil (Leukeran®), melphalan (Alkeran®) and cyclophosphamide (Cytoxan®). The Bruton tyrosine kinase (BTK) inhibitor ibrutinib (Imbruvica®) has been approved by the FDA for the treatment of patients with symptomatic Waldenström macroglobulinemia.
A serious complication of both diseases is called hyperviscosity syndrome. Hyperviscosity syndrome may occur when the malignant cells secrete an abnormal protein that can thicken the blood. This leads to inadequate blood flow, causing such symptoms as headache, blurred vision and mental confusion. Hyperviscosity syndrome can be treated with plasmapheresis, a process of removing plasma from the blood. This is followed by treatment to control the lymphoma.
Marginal Zone Lymphoma and Mucosa-Associated Lymphoid Tissue (MALT) Lymphoma
Marginal zone lymphoma can develop in either the lymph nodes (nodal) or outside the lymph nodes (extranodal). It begins in B lymphocytes in a part of the lymph tissue called the “marginal zone.” The disease tends to remain localized.
Marginal zone lymphoma includes several subtypes, each categorized by the type of tissue where the lymphoma forms.
- Gastric mucosa-associated lymphoid tissue (MALT) lymphoma usually develops in the stomach. Patients with MALT lymphoma may have a history of an autoimmune disease such as Hashimoto thyroiditis or Sjögren syndrome. A higher incidence of MALT lymphoma involving the stomach is seen in patients who have been infected with the bacterium H. pylori. Bacteria have also been implicated in other forms of MALT lymphoma. Treatment often includes potent combinations of antibiotics, which both eradicate the H. pylori infection and cause the lymphoma to regress. Many patients with H. pylori have been cured of MALT lymphoma without radiation or chemotherapy. For a small subset of patients, MALT lymphoma can transform into diffuse large B-cell lymphoma (DLBCL). These patients can benefit from treatments used for Diffuse Large B-cell Lymphoma.
- Extragastric MALT lymphoma begins outside the stomach and may form in almost any part of the body including other areas of the GI tract, salivary glands, thyroid, lung, skin and around the eye.
- Monocytoid B-cell lymphoma, also known as “nodal marginal zone B-cell lymphoma,” may be found in the spleen and blood. This form of NHL is generally treated like follicular lymphoma.
- Splenic marginal zone lymphoma (SMZL) begins in the spleen and may spread to the blood and bone marrow. One of the first signs of SMZL is an enlarged spleen; however, symptoms can be slow to develop. Splenic marginal zone lymphoma has been associated with hepatitis C infection. Treatment for hepatitis C with interferon (either alone or in combination with ribavirin) may result in a remission of the patient’s lymphoma.
For patients with splenic marginal zone lymphoma who do not have hepatitis C or any symptoms of lymphoma, the first treatment may be the watch-and-wait approach. Treatment is generally started when an enlarged spleen starts to cause symptoms or produces low white blood cell counts. For symptomatic patients who are hepatitis-C negative, treatment may include:
- Removal of the spleen
- Single-agent chemotherapy
- Combination chemotherapy
- Immunotherapy with rituximab
- Rituximab combined with chemotherapy.
Small Cell Lymphocytic Lymphoma (SLL) and Chronic Lymphocytic Leukemia (CLL)
Small cell lymphocytic lymphoma (SLL) and chronic lymphocytic leukemia (CLL) are similar NHL subtypes. They tend to affect the same age groups (median age of patients is 65 years), have common signs and symptoms and be slow-growing. The differences lie in where they develop: SLL mostly affects the lymph nodes and lymphoid tissue; CLL mostly affects blood and bone marrow but can spread to the lymph nodes.
Rituximab or a rituximab-containing regimen is used as first-line therapy for CLL/SLL . The Bruton’s tyrosine kinase (BTK) inhibitor ibrutinib (Imbruvica®) has also been approved as first-line therapy. The PI3K inhibitor idelalisib (Zydelig®) in combination with rituximab and the BCL-2 inhibitor venetoclax (Venclexta®) have been approved for use in patients with relapsed CLL/SLL. Bendamustine hydrochloride is a chemotherapy agent that has been approved for the treatment of CLL patients who have progressed during or within six months of treatment with rituximab or a rituximab-containing regimen.
- Lymphoma. https://www.cancer.org/cancer/lymphoma.html[↩]
- National Cancer Institute. https://www.cancer.org/[↩]
- Leukemia and Lymphoma Society. http://www.lls.org/[↩]
- Surveillance, Epidemiology, and End Results Program. https://seer.cancer.gov/[↩]
- Cancer Stat Facts: Hodgkin Lymphoma. https://seer.cancer.gov/statfacts/html/hodg.html[↩]
- Hodgkin Lymphoma Subtypes. http://www.lls.org/lymphoma/hodgkin-lymphoma/diagnosis/hodgkin-lymphoma-subtypes[↩][↩]
- Hodgkin Lymphoma Staging. http://www.lls.org/lymphoma/hodgkin-lymphoma/diagnosis/hodgkin-lymphoma-staging[↩][↩]
- Cancer Stat Facts: Non-Hodgkin Lymphoma. https://seer.cancer.gov/statfacts/html/nhl.html[↩]





{kind=link}