
Contents
- What is hypogonadism in male
- Men’s Health and Testosterone Hormone
- Pathophysiology of Testosterone and Male Hypogonadism
- Male hypogonadism complications
- Male hypogonadism causes
- Hypogonadism symptoms male
- Male hypogonadism diagnosis
- Male hypogonadism treatment
What is hypogonadism in male
Male hypogonadism is a condition in which your body does not produce enough of the testosterone hormone; the hormone that plays a key role in masculine growth and development during puberty, mental cognition or has an impaired ability to produce sperm or both. Clinically low testosterone levels can lead to the absence of secondary sex characteristics, infertility, muscle wasting, and other abnormalities.
You may be born with male hypogonadism, or it can develop later in life, often from injury or infection. Low testosterone levels may be due to testicular, hypothalamic, or pituitary abnormalities. The effects of male hypogonadism and what you can do about them — depend on the cause and at what point in your life male hypogonadism occurs. Some types of male hypogonadism can be treated with testosterone replacement therapy.
Male hypogonadism can significantly reduce the quality of your life and has resulted in the loss of livelihood and separation of couples, leading to divorce. It is also important for you to recognize that testosterone is not just a sex hormone. There is an important research being published to demonstrate that testosterone may have key actions on metabolism, on the vasculature, and on brain function, in addition to its well-known effects on bone and body composition.
Male hypogonadism is a common condition in the male population, with a higher prevalence in older men, obese men, and men with type 2 diabetes. If you are concerned about your testosterone levels It is important to talk to doctor about ways to manage.
Men’s Health and Testosterone Hormone
The pituitary gland is a tiny organ, the size of a pea, found at the base of the brain and is often referred to as the “master gland.” As the “master gland” of the body, the pituitary gland produces and stores many different hormones that travel throughout your body, directing certain processes or stimulating other glands to produce other hormones.
The following hormones are made in the anterior (front part) of the pituitary gland:
- Growth hormone (GH): This hormone promotes growth in childhood. For adults, it helps to maintain healthy muscle and bone mass.
- Prolactin: In women, it stimulates milk production. In males, low levels are linked to sexual problems; however, most males make no use of the hormone.
- Adrenocorticotropic (ACTH): This hormone promotes the production of cortisol, which helps to reduce stress, maintain healthy blood pressure and more.
- Thyroid-stimulating hormone (TSH): Just as the name implies, this hormone helps to regulate the body’s thyroid, which is crucial in maintaining a healthy metabolism.
- Luteinizing hormone (LH): stimulates testosterone production in men and egg release (ovulation) in women.
- Follicle-stimulating hormone (FSH): Found in both men and women. Follicle stimulating hormone promotes sperm production in men and stimulates the ovaries to produce estrogen and develop eggs in women. Luteinizing hormone (LH) and follicle stimulating hormone (FSH) work together to enable normal function of the ovaries and testes
The back part of the pituitary gland is called the posterior pituitary. It produces the following two hormones:
- Oxytocin: This hormone causes pregnant women to start having contractions (labor) at the appropriate time and also promotes milk flow in nursing mothers.
- Antidiuretic hormone (ADH): Commonly referred to as vasopressin, this hormone helps to regulate water balance in the body. It conserves body water by reducing the amount of water lost in urine.
When the pituitary gland doesn’t operate in a healthy manner, this can lead to pituitary disorders.
Male Reproductive Health Problems
Hormones are essential to reproductive health in all aspects of a man’s sexual life. The hypothalamus and pituitary gland are located at the base of the brain, and they work together to release hormones— luteinizing hormone (LH) and follicle stimulating hormone (FSH) —that stimulate the testes to produce testosterone and sperm. Testosterone, the main male hormone, helps maintain sex drive; vitality; sperm production; facial, pubic, and body hair; muscle; and bone.
In men, important health issues related to hormonal imbalances or deficiencies include:
- Male hypogonadism—effects (symptoms) of low testosterone and consistently lower than normal levels of testosterone in the blood
- Male infertility—inability to produce sperm adequate for reproduction
- Sexual dysfunction
- Erectile dysfunction—inability to get or keep an erection firm enough for sexual intercourse
- Decreased libido—reduced sexual desire or interest
These conditions are often, but not always, related to each other.
Role of Testosterone in Men’s Health
Testosterone is the most important sex hormone that men have. Throughout men’s lifespan, testosterone plays a critical role in sexual, cognitive, and body development. During fetal development, testosterone aids in the determination of sex. The most visible effects of rising testosterone levels begin in the prepubertal stage. During this time, body odor develops, oiliness of the skin and hair increase, acne develops, accelerated growth spurts occur, and pubic, early facial, and axillary hair grows. In men, the pubertal effects include enlargement of the sebaceous glands, penis enlargement, increased libido, increased frequency of erections, increased muscle mass, deepening of voice, increased height, bone maturations, loss of scalp hair, and growth of facial, chest, leg, and axillary hair. Even as adults, the effects of testosterone are visible as libido, penile erections, aggression, and mental and physical energy.
Testosterone also helps maintain sex drive, sperm production, and bone health. The brain and pituitary gland (a small gland at the base of the brain) control the production of testosterone by the testes.
In the short term, low testosterone (also called hypogonadism) can cause:
- A drop in sex drive
- Poor erections
- Low sperm count
- Enlarged breasts
Over time, low testosterone may cause a man to lose body hair, muscle bulk, and strength and to gain body fat. Chronic (long-term) low testosterone may also cause weak bones (osteoporosis), mood changes, less energy, and smaller testes. Signs and symptoms (what you see and feel) vary from person to person.
Testosterone Facts For Men
- Low testosterone comes with age — Testosterone levels naturally decrease by 1% each year after age 30, though don’t severely deplete, even in advanced age
- Testosterone production may be disrupted by disorders of the testicles, pituitary gland, or brain
- Testosterone levels change from hour to hour — highest in the morning; lowest at night
- Testosterone levels can temporarily lower due to too much exercise, poor nutrition, severe illness, and with certain medications
- Normal Testosterone levels should be between 300–1,000 ng/dL (nanograms per deciliter), depending on age and lab used
- Testosterone must be measured more than once for accurate assessment
Testosterone therapy is only recommended for hypogonadism patients. Boosting testosterone is NOT approved by the US Food and Drug Administration (FDA) to help improve your strength, athletic performance, physical appearance, or to treat or prevent problems associated with aging. Using testosterone for these purposes may be harmful to your health.
You should NOT receive testosterone therapy if you have:
- Prostate or breast cancer (or suspected)
- Enlarged prostate causing difficulty with urination
- Elevated prostate specific antigen (PSA) levels
- High number of red blood cells
- Untreated sleep apnea (obstructed breathing during sleep)
- Planning to have children
- Heart attack or stroke within the last 6 months
- Blood clots
What causes low testosterone?
Low testosterone can result from:
- Testicular injury (trauma, castration) or infection
- Radiation or chemotherapy treatment for cancer
- Some medications, such as opiate painkillers Hormone disorders (pituitary tumors or diseases, high levels of prolactin)
- Chronic diseases, such as liver and kidney disease, obesity, type 2 diabetes, and HIV/AIDS
- A genetic condition (Klinefelter syndrome, hemochromatosis, Kallmann syndrome, Prader-Willi syndrome, myatonic dystrophy)
Low testosterone is common in older men. In many cases, the cause is not known.
How is low testosterone diagnosed?
During a physical exam, your doctor will examine your body hair, size of your breasts and penis, and the size and consistency of the testes and scrotum. Your doctor may check for loss of side vision, which could indicate a pituitary tumor, a rare cause of low testosterone.
Your doctor will also use blood tests to see if your total testosterone level is low. The normal range is generally 300 to 1,000 ng/dL, but this depends on the lab that conducts the test. To get a diagnosis of low testosterone, you may need more than one early morning (7–10 AM) blood test and, sometimes, tests of pituitary gland hormones.
If you have symptoms of low testosterone, your doctor may suggest that you talk with an endocrinologist. This expert in hormones can help find the cause. Be open with your doctor about your medical history, all prescription and nonprescription drugs you are now taking, sexual problems, and any major changes in your life.
How is low testosterone treated?
Testosterone replacement therapy can improve sexual interest, erections, mood and energy, body hair growth, bone density, and muscle mass. There are several ways to replace testosterone:
- Gel or patches that you put on your skin
- Injections (shots)
- Tablets that stick to the gums
- Pellets inserted under the skin or pills (in some countries outside the United States)
The best method will depend on your preference and tolerance, and the cost.
There are risks with long-term use of testosterone. The most serious possible risk is prostate cancer. African American men, men over 40 years of age who have close relatives with prostate cancer, and all men over 50 years of age need monitoring for prostate cancer during testosterone treatment. Men with known or suspected prostate cancer, or with breast cancer, should not receive testosterone treatment.
Other possible risks of testosterone treatment include:
- A high red blood cell count
- Acne
- Breast enlargement
- An increase in prostate enlargement
- Sleep apnea—the occasional stopping of breathing during sleep (rarely)
- Fluid buildup (edema) in ankles, feet and legs (rarely)
Figure 1. The pituitary gland location

Figure 2. The hypothalamus and pituitary gland (anterior and posterior) endocrine pathways and target organs

Figure 3. Male reproductive system
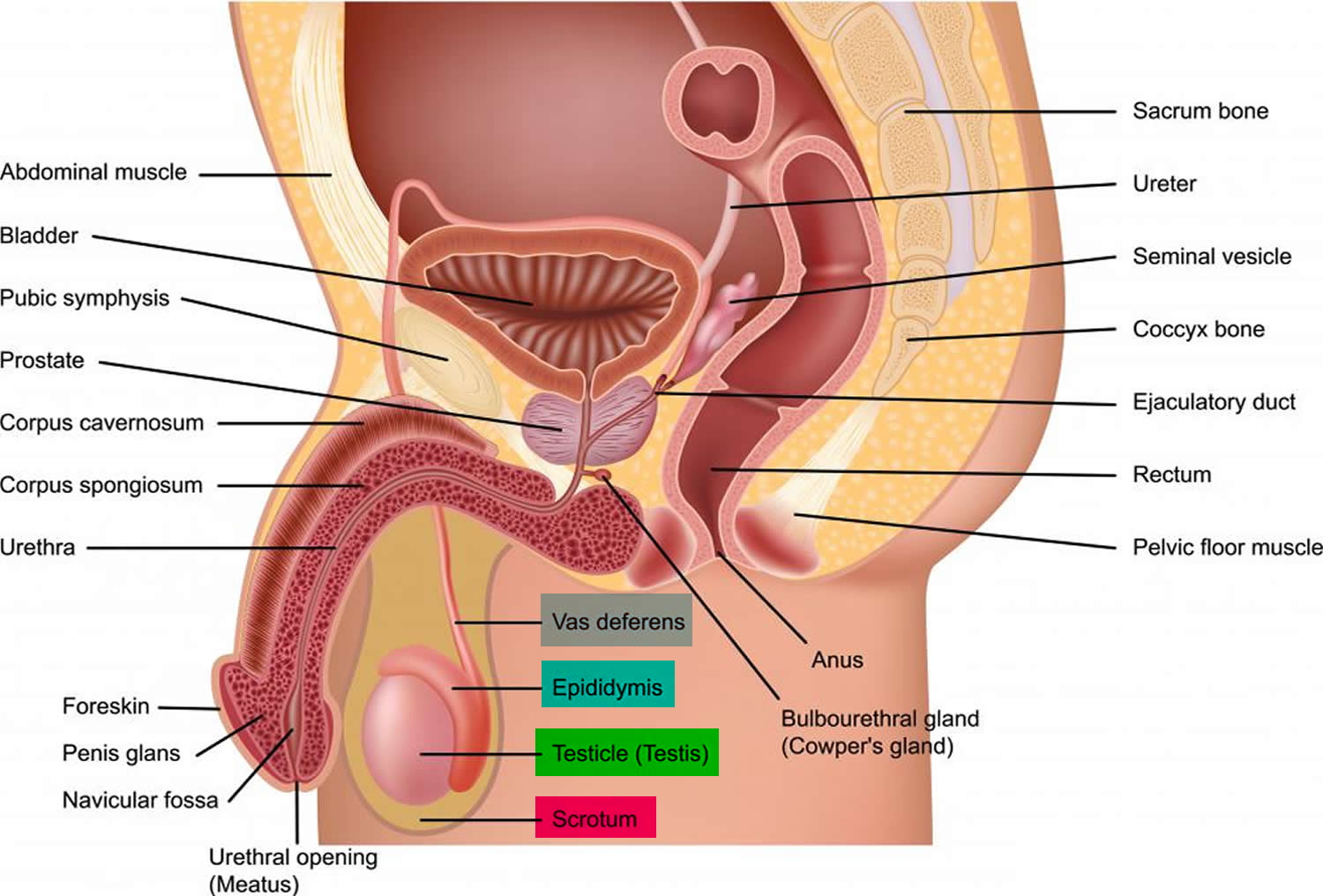
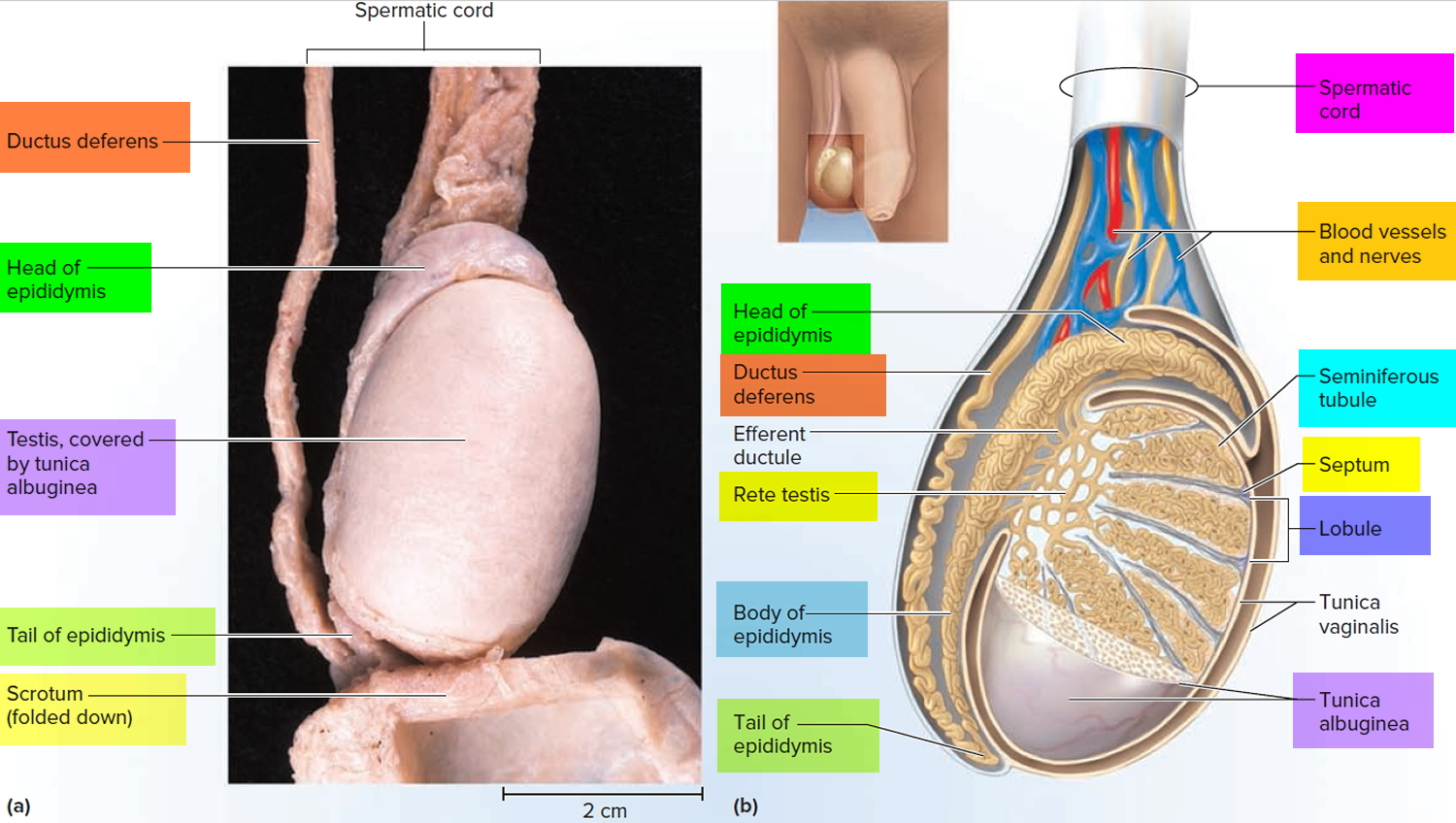
Figure 4. Testicle anatomy (normal)
Pathophysiology of Testosterone and Male Hypogonadism
The cerebral cortex – the layer of the brain often referred to as the gray matter – is the most highly developed portion of the human brain. This portion of the brain, encompassing about two-thirds of the brain mass, is responsible for the information processing in the brain. It is within this portion of the brain that testosterone production begins. The cerebral cortex signals the hypothalamus to stimulate production of testosterone. To do this, the hypothalamus releases the gonadotropin-releasing hormone (GnRH) in a pulsatile fashion, which stimulates the pituitary gland – the portion of the brain responsible for hormones involved in the regulation of growth, thyroid function, blood pressure, and other essential body functions. Once stimulated by the gonadotropin-releasing hormone (GnRH), the pituitary gland produces the follicle-stimulating hormone (FSH) and the luteinizing hormone (LH). Once released into the bloodstream, the luteinizing hormone (LH) triggers activity in the Leydig cells in the testes. In the Leydig cells, cholesterol is converted to testosterone. When the testosterone levels are sufficient, the pituitary gland slows the release of the luteinizing hormone via a negative feedback mechanism, thereby, slowing testosterone production. With such a complex process, many potential problems can lead to low testosterone levels. Any changes in the testicles, hypothalamus or pituitary gland can result in hypogonadism. Such changes can be congenital or acquired, temporary, or permanent.
Recent studies have found that testosterone production slowly decreases as a result of aging, although the rate of decline varies. Unlike women who experience a rapid decline in hormone levels during menopause, men experience a slow, continuous decline over time. The Baltimore Longitudinal Study of Aging reported that approximately 20% of men in their 60s and 50% of men in their 80s are hypogonadal 1. The New Mexico Aging Process Study showed a decrease in serum testosterone of 110 ng/dL every 10 years 2. As testosterone hormone levels decline slowly, this type of hypogonadism is sometimes referred to as the partial androgen deficiency of the aging male (PADAM). With the growing elderly population, the incidence of partial androgen deficiency of the aging male may increase over the next few decades.
Regardless of the age or comorbid conditions, obesity is associated with hypogonadism 1. The Baltimore Longitudinal Study of Aging found that testosterone decreased by 10 ng/dL per 1-kg/m2 increase in body mass index 1. Another study also showed reduced testosterone levels in men with increased total abdominal adiposity 3. The proposed causes for the effects of obesity on testosterone level include increased clearance or aromatization of testosterone in the adipose tissue and increased formation of inflammatory cytokines, which hinder the secretion of the gonadotropin-releasing hormone 4. Similar to the projections for an aging population, the increasing incidence of obesity may lead to an increased incidence of secondary male hypogonadism. When the risk factors of obesity and age are removed, diabetes mellitus still remains an independent risk factor for male hypogonadism. Although diabetes mellitus–related hypogonadism was previously thought to be associated with testicular failure, study results show one-third of diabetic men had low testosterone levels, but also had low pituitary hormone levels 5. Population projections expect the number of cases of diabetes mellitus to rise from 171 million in 2000 to 366 million in 2030 6. This drastic increase in cases will impact the prevalence of male hypogonadism as well. Certain medications are shown to reduce testosterone production. Among the medications known to alter the hypothalamic-pituitary-gonadal axis are spironolactone, corticosteroids, ketoconazole, ethanol, anticonvulsants, immunosuppressants, opiates, psychotropic medications, and hormones 7.
Male hypogonadism complications
The complications of untreated hypogonadism differ depending on what age it first develops — during fetal development, puberty or adulthood.
Fetal development
A baby may be born with:
- Ambiguous genitalia
- Abnormal genitalia
Puberty
Pubertal development can be delayed or incomplete, resulting in:
- Diminished or lack of beard and body hair
- Impaired penis and testicle growth
- Unproportional growth, usually increased length of arms and legs compared with the trunk
- Enlarged male breasts (gynecomastia)
Adulthood
Complications may include:
- Infertility
- Erectile dysfunction
- Decreased sex drive
- Fatigue
- Muscle loss or weakness
- Enlarged male breasts (gynecomastia)
- Decreased beard and body hair growth
- Osteoporosis
Male hypogonadism causes
Male hypogonadism means the testicles don’t produce enough of the male sex hormone testosterone.
There are two basic types of male hypogonadism that exist:
- Primary male hypogonadism: This type of hypogonadism – also known as primary testicular failure – originates from a problem in the testicles.
- Secondary male hypogonadism: This type of hypogonadism indicates a problem in the hypothalamus or the pituitary gland – parts of the brain that signal the testicles to produce testosterone. The hypothalamus produces the gonadotropin releasing hormone, which signals the pituitary gland to make the follicle-stimulating hormone (FSH) and luteinizing hormone (LH). The luteinizing hormone then signals the testes to produce testosterone. Either type of hypogonadism may be caused by an inherited (congenital) trait or something that happens later in life (acquired), such as an injury or an infection.
Primary Hypogonadism
Common causes of primary hypogonadism include:
Klinefelter’s Syndrome
This condition results from a congenital abnormality of the sex chromosomes, X and Y. A male normally has one X and one Y chromosome. In Klinefelter’s syndrome, two or more X chromosomes are present in addition to one Y chromosome (46,XXY). The Y chromosome contains the genetic material that determines the sex of a child and the related development. The extra X chromosome that occurs in Klinefelter’s syndrome causes abnormal development of the testicles, which in turn results in the underproduction of testosterone.
Undescended testicles (cryptorchidism)
Before birth, the testicles develop inside the abdomen and normally move down into their permanent place in the scrotum. Sometimes, one or both of the testicles may not descend at birth. This condition often corrects itself within the first few years of life without treatment. If not corrected in early childhood, it may lead to malfunction of the testicles and reduced production of testosterone.
Mumps orchitis
If a mumps infection involving the testicles in addition to the salivary glands (mumps orchitis) occurs during adolescence or adulthood, long-term testicular damage may occur. This may affect normal testicular function and testosterone production.
Hemochromatosis
Too much iron in the blood can cause testicular failure or pituitary gland dysfunction, affecting testosterone production.
Injury to the Testicles
Because of their location outside the abdomen, the testicles are prone to injury. Damage to normally developed testicles can cause male hypogonadism. Damage to one testicle may not impair testosterone production.
Cancer treatment
Chemotherapy or radiation therapy for the treatment of cancer can interfere with testosterone and sperm production. The effects of both treatments are often temporary, but permanent infertility may occur. Although many men regain their fertility within a few months after the treatment ends, preserving sperm before starting cancer therapy is an option that many men consider. Howell et al. 8 reported that hypogonadism was seen in 30% of the men with cancer and 90% of these gentlemen had germinal epithelial failure.
Normal aging
Older men generally have lower testosterone levels than younger men do. As men age, there’s a slow and continuous decrease in testosterone production. The rate that testosterone declines varies greatly among men. As many as 30% of men older than 75 have a testosterone level that is below normal, according to the American Association of Clinical Endocrinologists. Whether or not treatment is necessary remains a matter of debate 9.
Secondary Hypogonadism
In secondary hypogonadism, the testicles are normal, but function improperly due to a problem with the pituitary or hypothalamus. A number of conditions can cause secondary hypogonadism, including:
Kallmann syndrome
Abnormal development of the hypothalamus – the area of the brain that controls the secretion of pituitary hormones – can cause hypogonadism. This abnormality is also associated with the impaired development of the ability to smell (anosmia) and red-green color blindness.
Pituitary disorders
An abnormality in the pituitary gland can impair the release of hormones from the pituitary gland to the testicles, affecting normal testosterone production. A pituitary tumor or other type of brain tumor located near the pituitary gland may cause testosterone or other hormone deficiencies. Also, the treatment for a brain tumor such as surgery or radiation therapy may impair pituitary function and cause hypogonadism.
Inflammatory disease
Certain inflammatory diseases such as sarcoidosis, histiocytosis, and tuberculosis involve the hypothalmus and pituitary gland and can affect testosterone production, causing hypogonadism.
HIV/AIDS
This virus can cause low levels of testosterone by affecting the hypothalamus, the pituitary, and the testes.
Medications
The use of certain drugs, such as, opiate pain medications and some hormones, can affect testosterone production 10.
Obesity
Being significantly overweight at any age may be linked to hypogonadism.
Stress-induced Hypogonadism
Stress, excessive physical activity, and weight loss have all been associated with hypogonadism. Some have attributed this to stress-induced hypercortisolism, which would suppress hypothalamic function 11.
Risk factors for male hypogonadism
Risk factors for hypogonadism include:
- Kallmann syndrome
- Undescended testicles as an infant
- Mumps infection affecting your testicles
- Injury to your testicles
- Testicular or pituitary tumors
- HIV/AIDS
- Klinefelter syndrome
- Hemochromatosis
- Previous chemotherapy or radiation therapy
- Untreated sleep apnea
Hypogonadism can be inherited. If any of these risk factors are in your family health history, tell your doctor.
Hypogonadism symptoms male
Male hypogonadism is characterized by serum testosterone levels < 300 ng/dL in combination with at least one clinical sign or symptom 7. Signs of hypogonadism include absence or regression of secondary sex characteristics, anemia, muscle wasting, reduced bone mass or bone mineral density, oligospermia, and abdominal adiposity. Symptoms of post pubescent hypogonadism include sexual dysfunction (erectile dysfunction, reduced libido, diminished penile sensation, difficulty attaining orgasm, and reduced ejaculate), reduced energy and stamina, depressed mood, increased irritability, difficulty concentrating, changes in cholesterol levels, anemia, osteoporosis, and hot flushes. In the prepubertal male, if treatment is not initiated, signs and symptoms include sparse body hair and delayed epiphyseal closure.
Adulthood Male hypogonadism is a combination of low testosterone levels and the presence of any of these symptoms:
- Drop in sex drive (libido)
- Erectile dysfunction (ED — inability to get or keep an erection) and loss of spontaneous erections
- Lowered sperm count and infertility (inability to have children)
- Breast enlargement (gynecomastia) or tenderness
- Reduced energy
- Reduced muscle mass
- Shrinkage of testes
- Increased irritability, inability to concentrate, and depressed mood
- Hot flashes (when testosterone levels are very low)
- Loss of bone mass (osteoporosis)
Hypogonadism can also cause mental and emotional changes. As testosterone decreases, some men may experience symptoms similar to those of menopause in women. These may include:
- Fatigue
- Decreased sex drive
- Difficulty concentrating
Hypogonadism can also begin during fetal development or before puberty. Signs and symptoms depend on when the condition develops.
Fetal development
If the body doesn’t produce enough testosterone during fetal development, the result may be impaired growth of the external sex organs. Depending on when hypogonadism develops and how much testosterone is present, a child who is genetically male may be born with:
- Female genitals
- Ambiguous genitals — genitals that are neither clearly male nor clearly female
- Underdeveloped male genitals
Puberty
Male hypogonadism may delay puberty or cause incomplete or lack of normal development. It can cause:
- Decreased development of muscle mass
- Lack of deepening of the voice
- Impaired growth of body hair
- Impaired growth of the penis and testicles
- Excessive growth of the arms and legs in relation to the trunk of the body
- Development of breast tissue (gynecomastia)
Male hypogonadism diagnosis
Your doctor will conduct a physical exam during which he or she will note whether your sexual development, such as your pubic hair, muscle mass and size of your testes, is consistent with your age. Your doctor may test your blood level of testosterone if you have any of the signs or symptoms of male hypogonadism.
Early detection in boys can help prevent problems from delayed puberty. Early diagnosis and treatment in men offer better protection against osteoporosis and other related conditions.
Doctors base a diagnosis of male hypogonadism on symptoms and results of blood tests that measure testosterone levels. Because testosterone levels vary and are generally highest in the morning, blood testing is usually done early in the day, before 10 a.m.
If tests confirm you have low testosterone, further testing can determine if a testicular disorder or a pituitary abnormality is the cause. Based on specific signs and symptoms, additional studies can pinpoint the cause. These studies may include:
- Hormone testing
- Semen analysis
- Pituitary imaging
- Genetic studies
- Testicular biopsy
Testosterone testing also plays an important role in managing male hypogonadism. This helps your doctor determine the right dosage of medication, both initially and over time.
Male hypogonadism treatment
Treatment for adults
Treatment for male hypogonadism depends on the cause and whether you’re concerned about fertility.
Hormone replacement. For hypogonadism caused by testicular failure, doctors use male hormone replacement therapy (testosterone replacement therapy). Testosterone replacement therapy can restore muscle strength and prevent bone loss. In addition, men receiving testosterone replacement therapy may experience an increase in energy, sex drive, erectile function and sense of well-being. Testosterone replacement therapy is safe and can be effective for men who are diagnosed with consistently abnormal low testosterone production and symptoms that are associated with this type of androgen (hormone) deficiency.
While testosterone replacement therapy is the primary treatment option some conditions that cause hypogonadism are reversible without testosterone therapy. These should be addressed before testosterone therapy is contemplated. If testosterone therapy is needed, goal of treatment is to improve symptoms associated with testosterone deficiency and maintain sex characteristics. There are many different types of testosterone therapy. You should discuss the different options with your physician “your partner in care” to find out which therapy is right for you.
If a pituitary problem is the cause, pituitary hormones may stimulate sperm production and restore fertility. Testosterone replacement therapy can be used if fertility isn’t an issue. A pituitary tumor may require surgical removal, medication, radiation or the replacement of other hormones.
Assisted reproduction. Although there’s often no effective treatment to restore fertility in a man with primary hypogonadism, assisted reproductive technology may be helpful. This technology covers a variety of techniques designed to help couples who have been unsuccessful in achieving conception.
Treatment for boys
In boys, testosterone replacement therapy can stimulate puberty and the development of secondary sex characteristics, such as increased muscle mass, beard and pubic hair growth, and growth of the penis. Pituitary hormones may be used to stimulate testicle growth. An initial low dose of testosterone with gradual increases may help to avoid adverse effects and more closely mimic the slow increase in testosterone that occurs during puberty.
Types of testosterone replacement therapy
Testosterone replacement therapy is the primary treatment option for hypogonadism. Ideally, the therapy should provide physiological testosterone levels, typically in the range of 300 to 800 ng/dL. According to the guidelines from the American Association of Clinical Endocrinologists 12, the goals of therapy are to:
- Restore sexual function, libido, well-being, and behavior
- Produce and maintain virilization
- Optimize bone density and prevent osteoporosis
- In elderly men, possibly normalize growth hormone levels
- Potentially affect the risk of cardiovascular disease
- In cases of hypogonadotropic hypogonadism, restore fertility 13
To achieve these goals, several testosterone delivery systems are currently available in the market. Clinical guidelines published in 2006, by the Endocrine Society 13, recommend reserving treatment for those patients with clinical symptoms, rather than for those with just low testosterone levels.
Method of treatment depends on the cause of low testosterone, the patient’s preferences, cost, tolerance, and concern about fertility.
- Injections. Testosterone injections sold as Depo-Testosterone (testosterone cypionate) and Delatestryl (testosterone enanthate) are safe and effective. Injections are given in a muscle. Your symptoms might fluctuate between doses depending on the frequency of injections. Self or doctor administered in a muscle every 1–2 weeks; administered at a clinic every 10 weeks for longer-acting. Testosterone undecanoate (Aveed), an injection recently approved by the Food and Drug Administration, is injected less frequently but must be administered by a health care provider and can have serious side effects. The testosterone is suspended in oil to prolong absorption. Peak levels occur within 72 hours of administration, but intramuscular administration is associated with the most variable pharmacokinetics of all the formulations. In the first few days after administration, supraphysiological testosterone levels are achieved, followed by subphysiological levels near the end of the dosing interval. Such fluctuations, are often associated with wide variations in mood, energy, and sexual function, and prove distressing to many patients. To reduce fluctuations, lower doses and shorter dosing intervals (two weeks) are often used. Injection site reactions are also common, but are rarely the reason for discontinuation of therapy. Despite the fluctuations in testosterone levels, intramuscular injections provide a cost-effective option and the convenience of two- to four-week dosing intervals. Disadvantages associated with injections include visits to the doctor’s office, visits for dose administration, and lack of physiological testosterone patterns.
Side effects: uncomfortable, fluctuating symptoms. - Gels/Solutions. There are several gel preparations available with different ways of applying them. Depending on the brand, you either rub testosterone gel into your skin on your upper arm or shoulder (AndroGel, Testim, Vogelxo), apply with an applicator under each armpit (Axiron) or pump on your front and inner thigh (Fortesta). As the gel dries, your body absorbs testosterone through your skin. Gel application of testosterone replacement therapy appears to cause fewer skin reactions than patches do. Don’t shower or bathe for several hours after a gel application, to be sure it gets absorbed. Application in the morning allows for testosterone concentrations that follow the normal circadian pattern. Topical testosterone gels also provide longer-lasting elevations in serum testosterone, compared to transdermal patches 14. Similar to patches, testosterone delivered via gels does not undergo first-pass metabolism. Adverse effects associated with therapy include headache, hot flushes, insomnia, increased blood pressure, acne, emotional labiality, and nervousness. Although application site reactions occur, skin irritation is approximately 10 times less frequent with gels than with transdermal patches 15. Advantages associated with topical gel include maintenance of normal diurnal testosterone levels and documented increases in bone density 16. Potential problems associated with the gel are the potential for transfer of the gel from person to person and the cost.A potential side effect of the gel is the possibility of transferring the medication to another person and must wait to absorb completely into skin. Avoid skin-to-skin contact until the gel is completely dry or cover the area after an application.
- Patches. A patch containing testosterone (Androderm) is applied each night to your back, abdomen, upper arm or thigh. The site of the application is rotated to maintain seven-day intervals between applications to the same site, to lessen skin reactions.
- Side effects: skin redness and rashes. Application site reactions account for the majority of adverse effects associated with transdermal patches, with elderly men proving particularly prone to skin irritation. Local reactions include pruritus, blistering under the patch, erythema, vesicle formation, indurations, and allergic contact dermatitis. Approximately 10% of the patients discontinue patch therapy due to skin reactions 17. In one study, 60% of the subjects discontinued the patch between weeks four and eight due to skin irritation 18. A small percentage of patients may also experience headache, depression, and gastrointestinal (GI) bleeding. Some patients report that the patch easily falls off and is difficult to remove from the package without good dexterity. Transdermal patches are more expensive than injections, but the convenience of use and maintenance of normal diurnal testosterone levels are advantageous. Some patients report that the patch is noisy and therefore they feel stigmatized by its presence.
- Buccal Tablets. A small putty-like substance, gum and cheek testosterone replacement (Striant) delivers testosterone through the natural depression above your top teeth where your gum meets your upper lip (buccal cavity). This product quickly sticks to your gumline and allows testosterone to be absorbed into your bloodstream. Sticky pill applied to gums twice a day, absorbs quickly into bloodstream through gums. With this route, the peak testosterone levels are rapidly achieved and a steady state is reached by the second dose following twice-daily dosing. Similar to gel and transdermal products, buccal administration avoids first-pass metabolism. Food and beverage do not alter drug absorption. Although well-tolerated, transient gum irritation and a bitter taste are the chief adverse effects associated with this route. Gum irritation tends to resolve within the first week. Other adverse effects include dry mouth, toothache, and stomatitis. Some patients find the buccal tablet uncomfortable and report concern about the tablet shifting in the mouth while talking. Side effects: gum irritation.
- Pellets. Testosterone-containing pellets (Testopel) are implanted under skin surgically every 3–6 months for consistent and long-term dosages. Side effects: pellet coming out through skin, site infection/ bleeding (rare), scarring, dose decreasing over time and male hypogonadism symptoms possibly returning towards the end of dose period.
- Nasal Gel. Testosterone can be pumped into the nostrils as a gel. This option reduces the risk that medication will be transferred to another person through skin contact. Nasal-delivered testosterone must be applied twice in each nostril, three times daily, which may be more inconvenient than other delivery methods. Side effects: nasal irritation or congestion.
Oral Tablets
Oral testosterone tablets, under the brand name Andriol, are available in other countries. Android and Testroid – both methyl testosterone products are FDA approved oral formulations.
- Oral testosterone isn’t recommended for long-term hormone replacement because it might cause liver problems.
Although relatively inexpensive, oral products undergo extensive first-pass metabolism and therefore require multiple daily doses. Oral products are associated with elevated liver enzymes, GI intolerance, acne, and gynecomastia. Regardless of the treatment option, patients should be aware of the risks associated with testosterone therapy, including:
- Worsening of the prostatic hypertrophy
- Increased risk of prostate cancer
- Lower sperm count with large doses
- Swelling of ankles, feet, or body, with or without heart failure
- Gynecomastia
- Sleep apnea
- Blood clots
Patients should be educated on the signs and symptoms of these adverse effects and instructed to notify their doctor if any of these occur.
Risks of Testosterone Therapy
- Elevated red blood cell count
- Blood clots forming in the veins
- Acne
- Sleep apnea
- Possible prostate and/or breast enlargement
There is no firm scientific evidence that long-term testosterone replacement is associated with either prostate cancer or cardiovascular events. Recent research also suggests testosterone therapy might increase your risk of a heart attack. The FDA requires that you are made aware that the possibility of cardiovascular events may exist during treatment. Prostate cells are stimulated by testosterone, so be extra vigilant about cancer screenings. African American men over age 45 — especially those with family history of cancer — are already at risk for prostate cancer.
Coping and support
- Prevent osteoporosis. If hypogonadism occurs during adulthood, make lifestyle and dietary changes to prevent osteoporosis. Regular exercise and adequate amounts of calcium and vitamin D to maintain bone strength are important to reduce the risk of osteoporosis. The Institute of Medicine recommends 1,000 milligrams (mg) of calcium and 600 international units (IUs) of vitamin D a day for men ages 19 to 70. That recommendation increases to 1,200 mg of calcium and 800 IUs of vitamin D a day for men age 71 and older. Talk to your doctor about dietary guidelines that are appropriate for you.
- Learn about erectile dysfunction or infertility. The conditions caused by hypogonadism can cause psychological and relationship problems. Know what to expect from these conditions and what to do if new or uncomfortable feelings develop between you and your partner.
- Reduce stress. Talk with your doctor about how you can reduce the anxiety and stress that often accompany these conditions. Many men benefit from psychological or family counseling. Support groups can help people with hypogonadism and related conditions cope with similar situations and challenges. Helping your family understand the diagnosis of hypogonadism also is important.
- Allow time to adjust. Adolescents with hypogonadism may feel as if they don’t fit in. Testosterone replacement therapy will trigger puberty. When given at a slow pace that allows time for adjustment to physical changes and new feelings, the therapy decreases the chance of social or emotional problems.
- Harman SM, Metter EJ, Tobin JD, Pearson J, Blackman MR. Longitudinal effects of aging on serum total and free testosterone levels in healthy men.Baltimore Longitudinal Study of Aging. J Clin Endocrinol Metab. 2001;86:724–31. https://academic.oup.com/jcem/article/86/2/724/2841070[↩][↩][↩]
- Morley JE, Kaiser FE, Perry HM. Longitudinal changes in testosterone, luteinizing hormone, and follicle-stimulating hormone in healthy older men. Metabolism. 1997;46:410–3[↩]
- Haffner SM, Valdez RA, Stern MP, Katz MS. Obesity, body fat distribution and sex hormones in men. Int J Obes Relat Metab Disord. 1993;17:643–9. https://www.ncbi.nlm.nih.gov/pubmed/8281222[↩]
- Zumoff B, Strain GW, Miller LK. Plasma free and non-sex-hormone-binding globulin-bound testosterone are decreased in obese men in proportion to their degree of obesity. J Clin Endocrinol Metab. 1990;71:929–31. https://www.ncbi.nlm.nih.gov/pubmed/2401718[↩]
- Dhindsa S, Prabhaker S, Sethi M, Bandyopadhyay A, Chaudhari A, Dandona P. Frequent occurrence of hypogonadotropic hypogonadism in type 2 diabetes. J Clin Endocrinol Metab. 2004;89:5462–8. https://www.ncbi.nlm.nih.gov/pubmed/15531498[↩]
- Wild S, Roglic G, Green A, Sicree R, King H. Global prevalence of diabetes: Estimates for the year 2000 and projections for 2030. Diabetes Care. 2004;27:1047–53 https://www.ncbi.nlm.nih.gov/pubmed/15111519[↩]
- Kumar P, Kumar N, Thakur DS, Patidar A. Male hypogonadism: Symptoms and treatment. Journal of Advanced Pharmaceutical Technology & Research. 2010;1(3):297-301. doi:10.4103/0110-5558.72420. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3255409/[↩][↩]
- Howell SJ, Radford JA, Ryder WD, Shalet SM. Testicular function after cytotoxic chemotherapy: Evidence of leydig cell insufficiency. J Clin Oncol. 1999;17:1493–8. https://www.ncbi.nlm.nih.gov/pubmed/10334536[↩]
- Harman SM. Longitudinal effects of aging on serum total and free testosterone levels in healthy men.Baltimore Longitudinal Study of Aging. J Clin Endocrinol Metab. 2001;86:724–31. https://academic.oup.com/jcem/article/86/2/724/2841070[↩]
- Daniell HW. Hypogonadism in men consuming sustained-action oral opioids. J Pain. 2002;3:377–84. https://www.ncbi.nlm.nih.gov/pubmed/14622741[↩]
- Cumming DC, Quigley ME, Yen SS. Acute suppression of circulating testosterone levels by cortisol in men. J Clin Endocrinol Metab. 1983;57:671–3. https://www.ncbi.nlm.nih.gov/pubmed/6348068[↩]
- AACE Hypogonadism Task Force. Medical guidelines for clinical practice for the evaluation and treatment of hypogonadism in adult male patients -2002 updated. Endocr Pract. 2002;8:434–56. https://www.ncbi.nlm.nih.gov/pubmed/15260010[↩]
- Bhasin S, Cunningham GR, Hayes FJ. Testosterone therapy in adult men with androgen deficiency syndromes: An endocrine society clinical practice guideline. J Clin Endocrinol Metab. 2006;91:1995–2010 https://academic.oup.com/jcem/article/91/6/1995/2843294[↩][↩]
- Swerdloff RS, Wang C, Cunningham G. Long-term pharmacokinetics of transdermal testosterone gal in hypogonadal men. J Clin Endocrinol Metab. 2000;85:4500–10 https://www.ncbi.nlm.nih.gov/pubmed/11134099[↩]
- Wang C, Swedloff RS, Iranmanesh A. Testosterone Gel Study Group.Transdermal testosterone gel improves sexual function, mood, muscle strength, and body composition parameters in hypgonadal men. J Clin Endocrinol Metab. 2000;85:2839–53 https://www.ncbi.nlm.nih.gov/pubmed/10946892[↩]
- Wang C, Swerdloff RS, Iranmanesh A. Effects of transdermal testosterone gel on bone turnover makers and bone mineral density in hypogonadal men. Clin Endocrinol (Oxf) 2001;54:739–50 https://www.ncbi.nlm.nih.gov/pubmed/11422108[↩]
- Jordan JR. Allergy and topical irritation associated with transdermal testosterone administration: A comparison of scrotal and nonscrotal transdermal systems. Am J Contact Dermatol. 1997;8:108–13. https://www.ncbi.nlm.nih.gov/pubmed/9153333[↩]
- Parker S, Armitage M. Experience with transdermal testosterone replacement therapy for hypogonadal men. Clin Endocrinol (Oxf) 1999;50:57–62. https://www.ncbi.nlm.nih.gov/pubmed/10341856[↩]





{kind=link}