
What is MCT oil
MCT oil is short for medium chain triglyceride oil or medium-chain triacylglycerol or saturated fatty acid with carbon chain lengths ranging from C6, C8, C10 or C12 (C6:0–C12:0) 1, 2, 3,4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16. MCT oil in commercial products are often a mixture of 7.8% caprylic acid (C8), 6.7% capric acid (C10) and approximately 47.5% lauric acid (C12) (100% saturated medium-chain fatty acids) 17, 18, 19, 20. MCT oil is present in natural substances like coconut, coconut oil and palm kernel oil and in small amounts in dairy products such as butter and goat milk 12, 13, 14, 15, 16, 21, 22. Human breast milk is also a natural source of MCT oil 23, 24. MCT supplements are derived from concentrated palm kernel and coconut oils. The U.S. Food and Drug Administration (FDA) has assigned Generally Recognized As Safe (GRAS) status to the use of MCT in food products 25, 26. Most of the reported treatment-related MCT oil side effects were of gastrointestinal such as diarrhea, flatulence and abdominal pain; those occurred in a relatively small proportion of participants, in frequencies that varied from study to study, from 13.5% to 50% 27, 28, 29, 30. Factors such as splitting of the total dose into multiple doses and administration of MCT oil with food might help in controlling the gastrointestinal side effects.
Figure 1. Medium-chain triglyceride (MCT) chemical structure
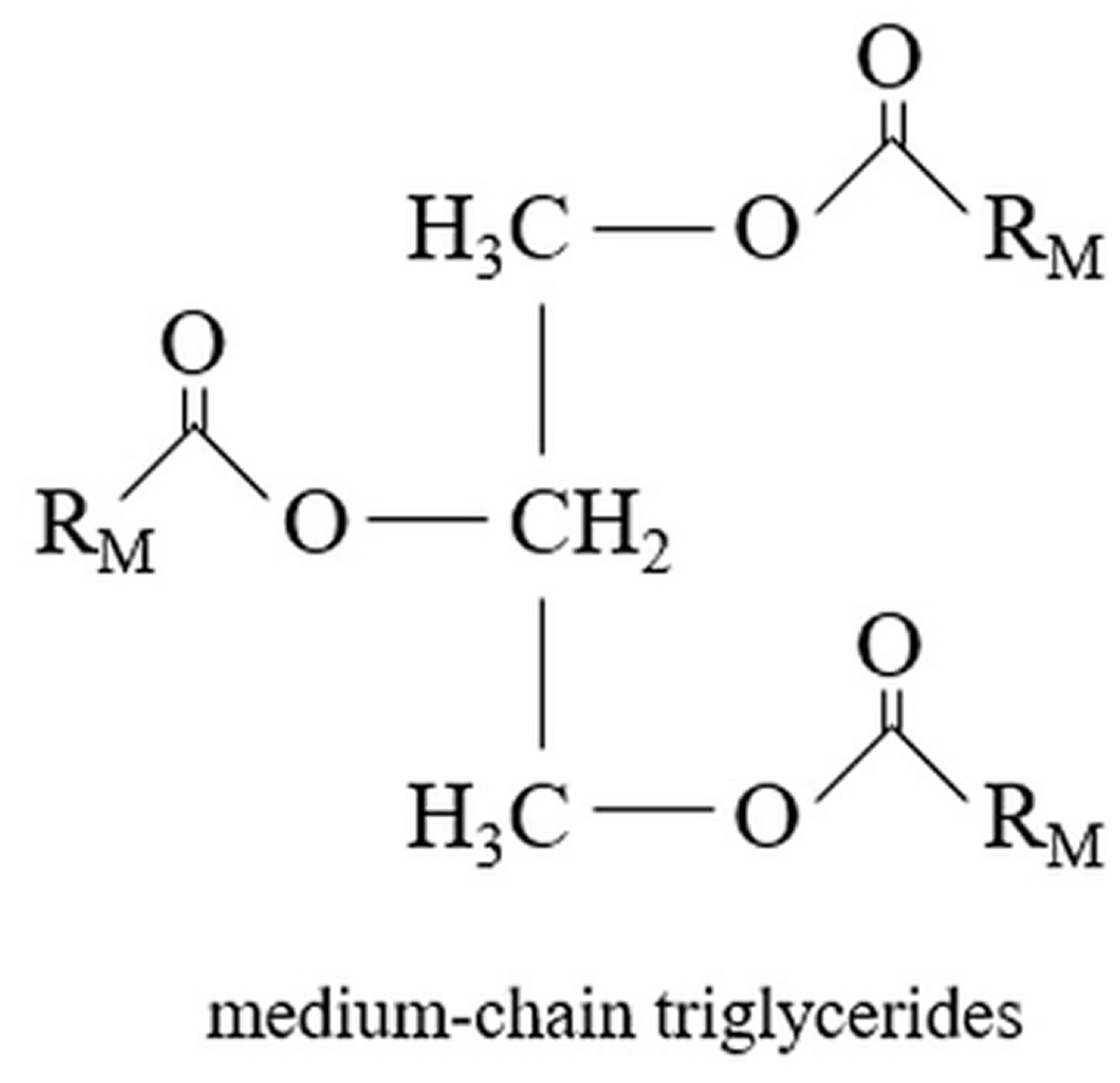
Footnotes: Common structure of a medium-chain triglyceride (MCT), consisting of three saturated fatty acids represented by the “R” groups attached to a glycerol backbone. Carbon atoms number C6 to C12.
[Source 2 ]Table 1. Medium chain fatty acids
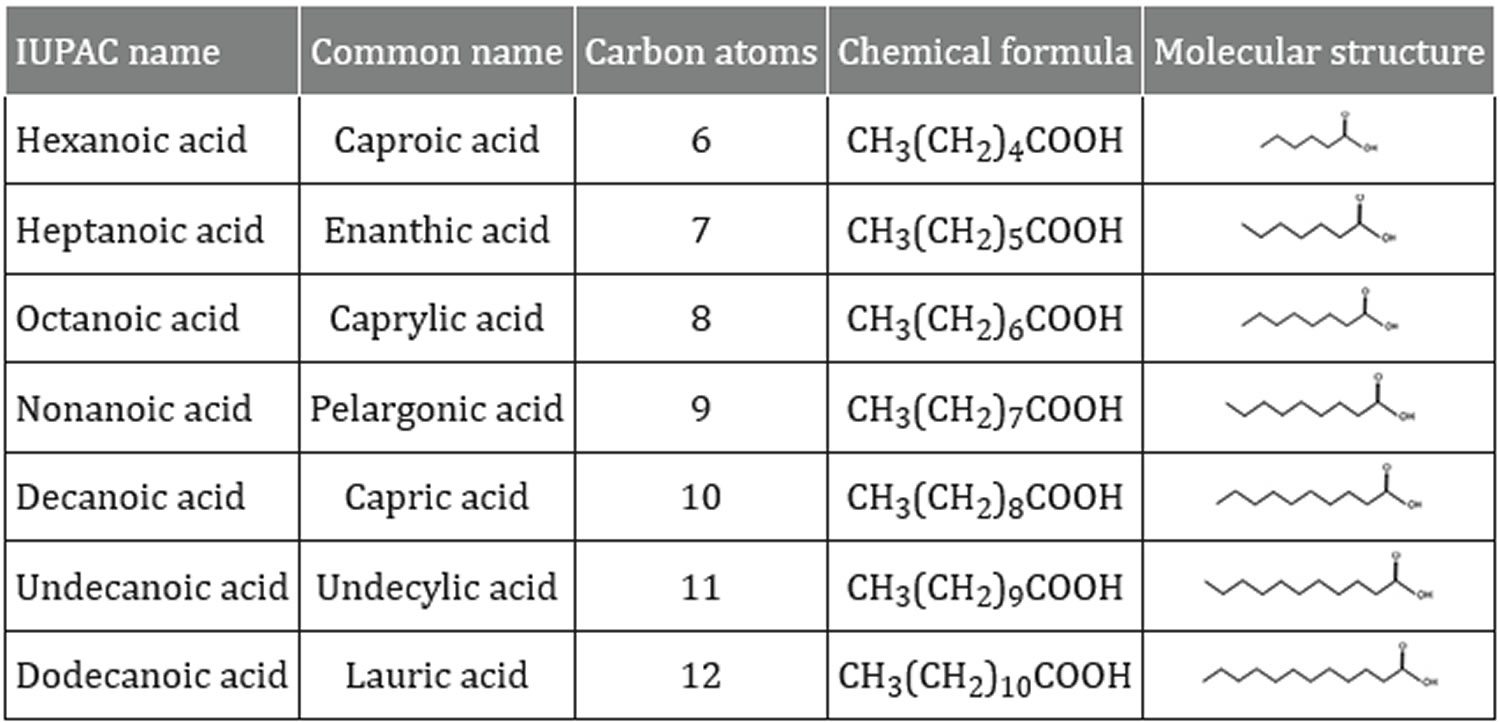
Footnotes: Caprylic acid (Octanoic acid, C8) and Capric acid (decanoic acid, C10) are medium chain fatty acids (MCFAs) and components of the medium chain triglyceride (MCT) ketogenic diet. These medium chain fatty acids (MCFAs) can provide an alternate energy source to glucose for neurones and astrocytes 31.
Source 32 ]
Figure 2. MCT absorption and metabolism
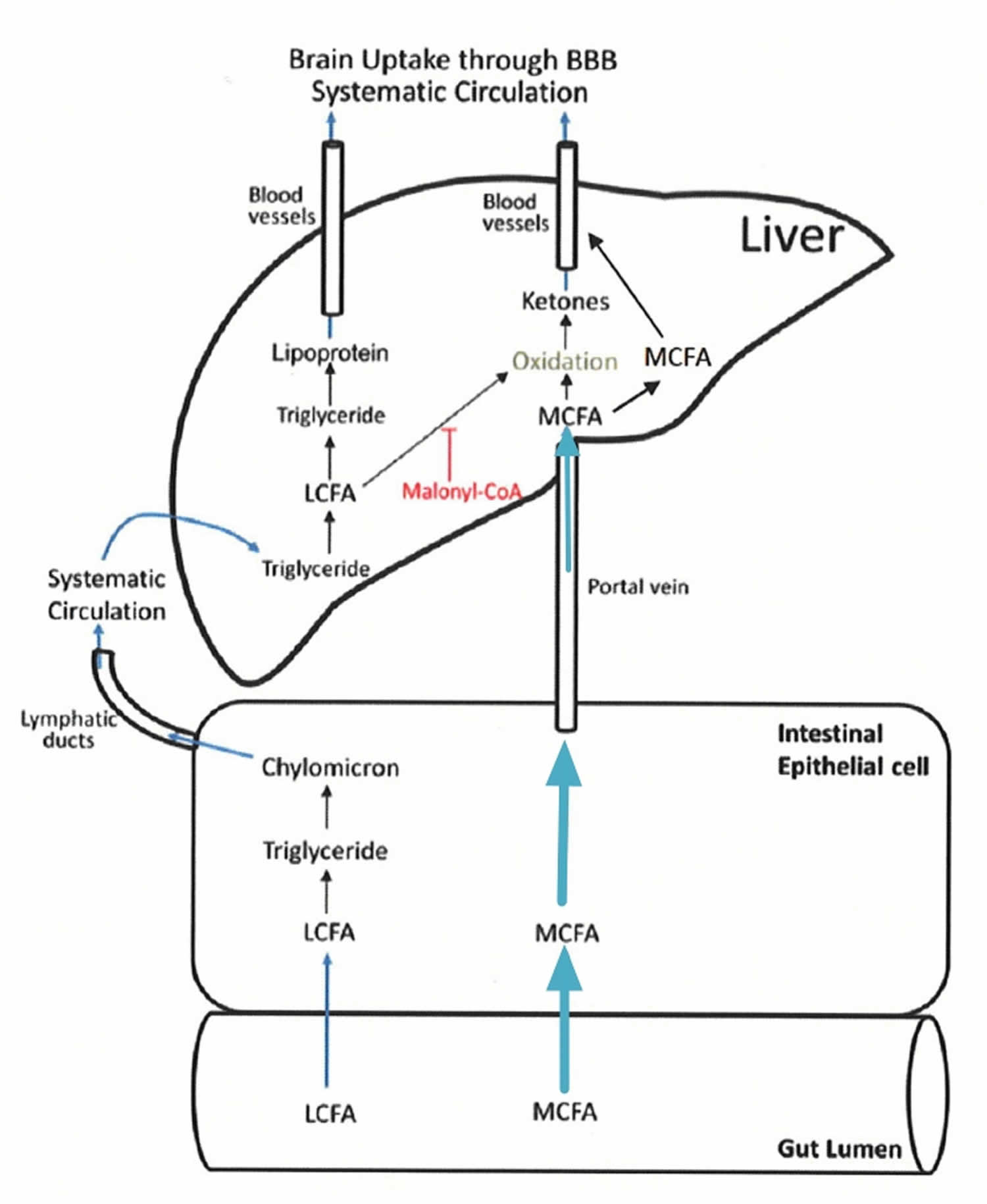
Abbreviations: LCFA = long chain fatty acids; MCFA = medium chain fatty acids; BBB = blood brain barrier
[Source 33 ]Figure 3. MCT mechanism of actions
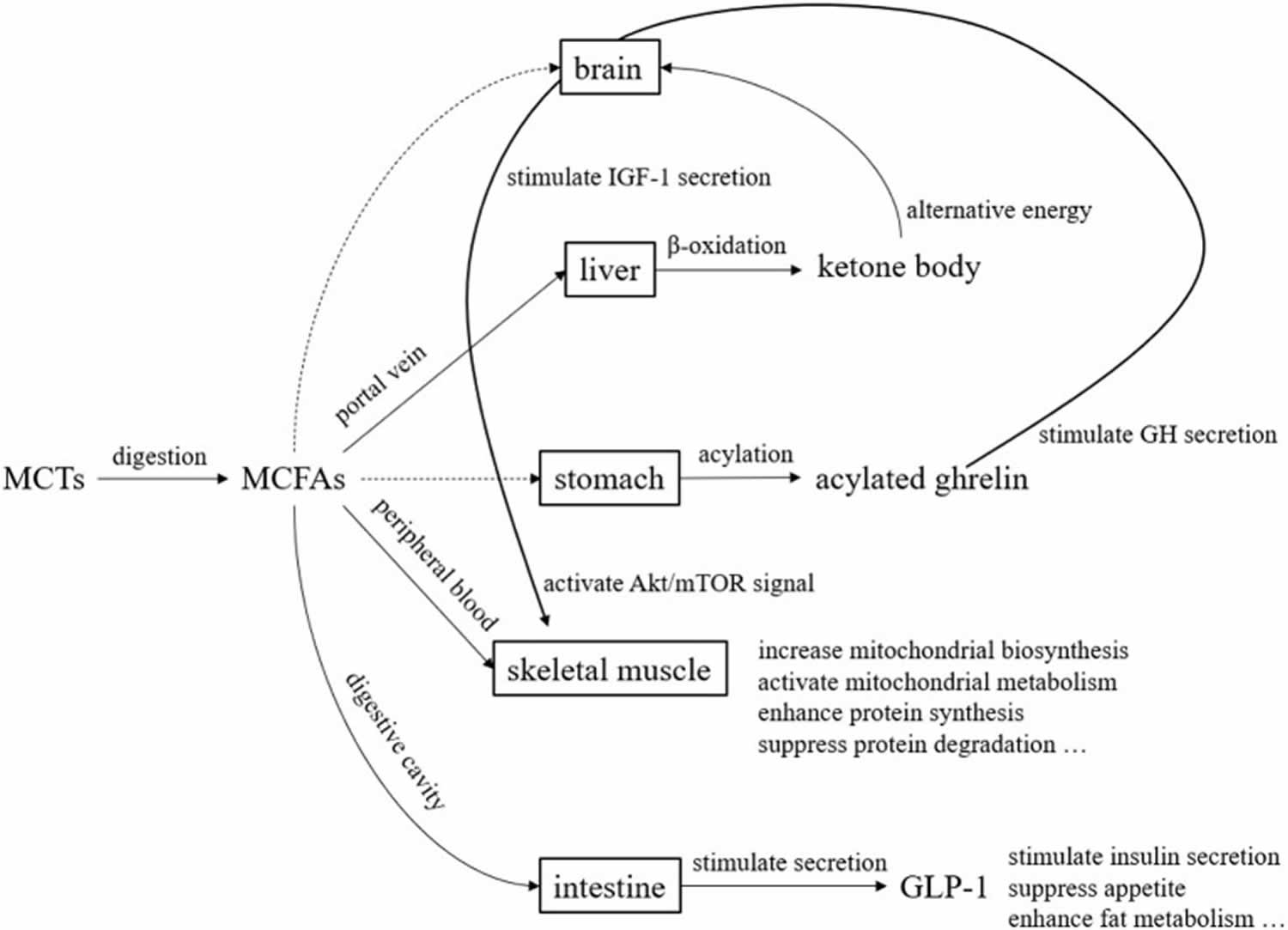
Footnotes: Medium chain triglycerides (MCTs) are mostly transported to the liver via the portal vein after digestion and absorption. Since MCTs do not require carnitine for transfer to the mitochondria, they are quickly beta-oxidized and become energy. During this process, ketone bodies are produced, which serve as an alternative energy source to glucose in the brain. Although the pathway is unknown, acylated ghrelin levels in the blood increase after MCTs ingestion. Acylated ghrelin enhance the secretion of growth hormone (GH), which in turn stimulates the secretion of insulin-like growth factor 1 (IGF-1). Furthermore, IGF-1 enhance protein synthesis and suppress protein degradation by activating Akt/mTOR signaling. Medium-chain fatty acids (MCFAs) transferred to the peripheral blood act on skeletal muscle to enhance mitochondrial biosynthesis and mitochondrial metabolic activity. Medium-chain fatty acids (MCFAs) also stimulates the secretion of glucagon-like peptide 1 (GLP-1) from small intestinal L cells.
[Source 2 ]Dietary fat is the most important source of energy of all the nutrients, supplying 9 kcal/g, about double that contributed by either protein or carbohydrate at 4 kcal/g 34. Fatty acids, stored as triglycerides also called triacylglycerols in the body, are an important reservoir of stored energy. Fatty acids are composed of two major types: saturated and unsaturated fatty acids, and the presence or absence of carbon-carbon double bonds in the hydrocarbon chain is the only difference between them. Saturated fatty acids do not have double bonds in the hydrocarbon chain and unsaturated fatty acids contain at least one double bond. The unsaturated fatty acids are often divided into two subgroups: monounsaturated fatty acids with a single double bond and polyunsaturated fatty acids with two or more double bonds. The basic formulae of saturated and monounsaturated species are CH3(CH2)nCOOH and CH3(CH2)nCH=CH(CH2)nCOOH, respectively. In addition, based on chain length, they are often categorized as short-chain, medium-chain, or long-chain fatty acids. Short-chain fatty acids have aliphatic tails of fewer than eight carbons (<C8). Fatty acids with aliphatic tails of 8–12 carbons (C8-C12) are classified as medium-chain fatty acids, and long-chain fatty acids have aliphatic tails longer than 12 carbons (>C12). Sometimes, fatty acids with aliphatic tails longer than 22 carbons (>C22) are defined as very-long-chain fatty acids 35.
The four major types of fats are 36:
- Monounsaturated fats (Good). Monounsaturated fats have a single carbon-to-carbon double bond. The result is that it has two fewer hydrogen atoms than a saturated fat and a bend at the double bond. This structure keeps monounsaturated fats liquid at room temperature. Eating food that has more monounsaturated fat (or “healthy fat”) instead of saturated fat (like butter) may help lower cholesterol and reduce heart disease risk. Research also shows that monounsaturated fats may benefit insulin levels and blood sugar control, which can be especially helpful if you have type 2 diabetes. However, monounsaturated fat has the same number of calories (9 calories or 37kJ) as other types of fat and may contribute to weight gain if you eat too much of it. Good sources of monounsaturated fats are olive oil, peanut oil, canola oil, avocados, most nuts, as well as high-oleic safflower and sunflower oils. The carbon-carbon double bond found in monounsaturated or polyunsaturated fatty acids can exist in the cis or trans configuration. When the two hydrogen atoms are on opposite sides of the double bond, the configuration is called trans. When the hydrogen atoms are on the same side of the double bond, the configuration is called cis. Monounsaturated fats (monounsaturated fatty acids) are found in high concentrations in olive oil, peanut oil, canola, avocados, almonds, safflower oils, hazelnuts, pecans, pumpkin seeds and sesame seeds and most nuts. Monounsaturated fats also are part of most animal fats such as fats from chicken, pork, beef, and wild game. When you dip your bread in olive oil at an Italian restaurant, you’re getting mostly monounsaturated fat.
- Polyunsaturated fats (Good). Polyunsaturated fats also called polyunsaturated fatty acids (PUFAs) are a type of healthy fat that is essential for bodily functions and should be included in a balanced diet. The two major classes of polyunsaturated fatty acids (PUFAs) are the omega-3 fatty acids and omega-6 fatty acids. Polyunsaturated fats or polyunsaturated fatty acids (PUFAs) are liquid at room temperature and are found in plant and animal-based foods. Examples include fatty fish, plant-based oils, and certain nuts and seeds. Polyunsaturated fats are beneficial for heart health and can help reduce the risk of heart disease and other health problems when consumed in place of saturated and trans fats. Polyunsaturated fats can help reduce bad cholesterol levels in your blood, which can lower your risk of heart disease and stroke. Polyunsaturated fats also provide nutrients to help develop and maintain your body’s cells. Oils rich in polyunsaturated fats also provide vitamin E, an important antioxidant vitamin. Oils rich in polyunsaturated fats also provide essential fats that your body needs but can’t produce itself, including omega-6 and omega-3 fatty acids. You must get essential fats through food. Omega-6 and omega-3 fatty acids are important for many functions in the body. Polyunsaturated fats are distinguished from saturated and monounsaturated fatty acids by the presence of two or more double bonds between carbons within the fatty acid chain.
- Saturated fats (Bad). Saturated fats also called saturated fatty acids (SFA) are fats that are solid at room temperature. Because saturated fats are typically solid at room temperature — think cooled bacon grease, butter, beef tallow, coconut oil, ghee or pork lard, they are sometimes called “solid fats”. The word “saturated” here refers to the number of hydrogen atoms surrounding each carbon atom. The chain of carbon atoms holds as many hydrogen atoms as possible — it’s saturated with hydrogens. Saturated fats are common in the American diet. Saturated fats include margarine, butter, whole fat dairy products, lard, the fat marbling in meats, coconut oil and palm oil. Saturated fats are also found in full-fat milk, yogurt, full-fat cheese, cakes, pastries, cookies, crackers, and biscuits 1. Coconut, palm kernel, and palm oil are called oils because they come from plants. However, they are solid or semi-solid at room temperature due to their high content of short-chain saturated fatty acids. They are considered solid fats for nutritional purposes. They also are found in other animal fats, such as pork and chicken fats and in other plant fats, such as nuts. Saturated fats don’t need to be avoided entirely, but diets high in saturated fats can increase bad LDL (low-density lipoprotein) cholesterol and triglycerides, increasing your risk of heart disease and stroke. The Dietary Guidelines for Americans suggest that less than 10% of calories a day should be from saturated fats. The American Heart Association recommends that saturated fats only make up 5 to 6% of your daily calories. For a 2,000 calorie diet, that is a total of 100 calories, or 11 grams a day. But just replacing saturated fat with refined carbohydrates, like sugary foods and drinks, won’t improve your health either. However, replacing saturated fat with unsaturated fats such as monounsaturated fats or polyunsaturated fats that are found in oily fish, nuts, or vegetable oils like rapeseed or sunflower oil, does seem to reduce your risk of heart attack and stroke.
- Trans fats (Very Bad). Trans fat is also known as trans fatty acid or partially hydrogenated oils, is an unsaturated dietary fat that increases your risk of coronary heart disease (coronary artery disease). There are two broad types of trans fats found in foods: naturally-occurring and artificial trans fats. Naturally-occurring trans fats are produced in the gut of some animals (ruminants) and foods made from these animals (e.g., dairy products like milk, butter, cheese, and meat products) may contain small quantities of trans fats. Artificial trans fats (partially hydrogenated oils) are created in an industrial process that adds hydrogen to liquid vegetable oils to make them more solid, through a process called hydrogenation (a manufacturing process that adds hydrogen to vegetable oil) 37. Foods with industrially produced trans fat include those listing hydrogenated or partially hydrogenated fat on the label, such as crackers, snack foods, commercially produced baked goods, and some stick margarines. The primary dietary source for trans fats in processed food is “partially hydrogenated oils.” Look for them on the ingredient list on food packages.
Monounsaturated and polyunsaturated fats are known as “healthy fats” because they are good for your heart, cholesterol levels, and overall health. Monounsaturated and polyunsaturated fats do not raise LDL “bad” cholesterol and are beneficial when consumed in moderation. These fats tend to be “liquid” at room temperature. Olive oil and canola oil are examples of a type of oil that contains monounsaturated fats.
Monounsaturated fats (MUFAs) can help reduce bad cholesterol levels in your blood which can lower your risk of heart disease and stroke 38. They also provide nutrients to help develop and maintain your body’s cells. Oils rich in monounsaturated fats also contribute vitamin E to the diet, an antioxidant vitamin most Americans need more of.
Polyunsaturated fats (PUFAs) are simply fat molecules that have more than one unsaturated carbon bond in the molecule, this is also called a double bond. Oils that contain polyunsaturated fats are typically liquid at room temperature but start to turn solid when chilled. Soybean oil and flax seed oil are examples of a type of oil that contains polyunsaturated fats. Polyunsaturated fats can help reduce bad cholesterol levels in your blood which can lower your risk of heart disease and stroke 39. They also provide nutrients to help develop and maintain your body’s cells. Oils rich in polyunsaturated fats also contribute vitamin E to the diet, an antioxidant vitamin most Americans need more of.
Oils rich in polyunsaturated fats also provide essential fats that your body needs but can’t produce itself – such as omega-6 and omega-3 fatty acids. You must get essential fats through food. Omega-6 and omega-3 fatty acids are important for many functions in the body.
For good health, the majority of the fats that you eat should be monounsaturated or polyunsaturated. Consider eating more of the beneficial polyunsaturated fats containing Omega-3 fatty acids found in fatty fish, flaxseed, chia seeds and walnuts 39. Eat foods containing monounsaturated fats and/or polyunsaturated fats instead of foods that contain saturated fats and/or trans fats.
The majority of saturated fat comes from animal products such as beef, lamb, pork, poultry with skin, butter, cream, cheese and other dairy products made from whole or 2 percent milk. All of these foods also contain dietary cholesterol. Foods from plants that contain saturated fat include coconut, coconut oil, palm oil and palm kernel oil (often called tropical oils) and cocoa butter. Replacing foods that are high in saturated fat with healthier monounsaturated and polyunsaturated fats (oils) can lower your blood cholesterol levels and improve your blood lipid profiles 40. The American Heart Association recommends you don’t eat more than 5% to 6% of calories from saturated fat 40. For example, if you need about 2,000 calories a day, no more than 120 of them should come from saturated fat. That’s about 13 grams of saturated fat per day.
Trans fats (or trans fatty acids) are created in an industrial process that adds hydrogen to liquid vegetable oils to make them more solid. Another name for trans fats is “partially hydrogenated oils.” Partially hydrogenated oils (trans fats) are used by food manufacturers to improve the texture, shelf life and flavor stability of foods. Partially hydrogenated oils should not be confused with “fully hydrogenated oils,” or saturated fats which are solid fats that contain very low levels of trans fat. Trans fats are found in many fried foods and baked goods such as pastries, pizza dough, pie crust, cookies and crackers. And trans fat are also formed naturally and is found in small amounts in some animal products, such as meats and dairy products 41.
Trans fats raise your bad (LDL) cholesterol levels and lower your good (HDL) cholesterol levels 41. These changes are associated with a higher risk of heart disease.
There are two sources of trans fat:
- Trans fat formed naturally – this type of trans fat is produced in the gut of some grazing animals (such as cattle and sheep).
- Trans fat formed artificially during food processing – this type of trans fat is created during a process called “partial hydrogenation” in which hydrogen is added to liquid vegetable oil to make it more solid, and therefore more resistant to becoming spoiled or rancid. The process generally does not make the oil completely solid, resulting in “partially” hydrogenated oils.
Since 2006, the U.S. Food and Drug Administration (FDA) has required trans fat content to be listed on the Nutrition Facts panel of packaged foods 42. In recent years, many major national fast-food chains and casual-dining restaurant chains have announced they will no longer use trans fats to fry or deep-fry foods. Many smaller local and regional restaurant chains have made similar announcements.
On June 16, 2015, the U.S. Food and Drug Administration (FDA) took action that will significantly reduce the use of partially hydrogenated oils, the major source of artificial trans fats in the food supply. The FDA announcement to eliminate trans fats from processed foods and their action is expected to reduce cardiovascular disease and prevent thousands of fatal heart attacks each year in the U.S. 43. According to the FDA, “On June 18, 2018, manufacturers must ensure that their products no longer contain partially hydrogenated oils (trans fats) for uses that have not been otherwise authorized by FDA.”
To find the amount of trans fats in a particular packaged food, look at the Nutrition Facts panel. Companies must list any measurable amount of trans fat (0.5 grams or more per serving) in a separate line in the “Total Fat” section of the panel, directly beneath the line for “Saturated Fat.” This means if a food package states 0 gram of trans fats, it might still have some trans fats if the amount per serving is less than 0.5 g. Make sure to check the ingredients list for “partially hydrogenated oil.”
Saturated fats are considered to be unhealthy and several health authorities recommend limiting their intake in the diet 44. These recommendations stem from studies linking higher intakes of saturated fat and heart disease 45. Replacing saturated fat with healthier fat could lower cardiovascular risks 46. However, saturated fats are quite heterogeneous in nature and potentially also in their health effects. In fact, based on their structure, saturated fats can be sub-classified into short chain, medium chain, and long chain fats whereas mono- and polyunsaturated fats are all long chain fats. Short chain fatty acids are considered to have 6 or fewer carbon atoms, medium chain fatty acids (MCFA) have 8–10 carbons, and long chain fatty acids (LCFA) generally have 12 or more carbon chains. In the US, the average consumption of medium chain fatty acids (MCFA) is approximately 2% of total fat intake 47.
Most studies comparing the effects of saturated fats to unsaturated fats have focused on fats that contained a large proportion of their fatty acids as long chain fatty acids (LCFA). Very few clinical studies have examined the impact of medium chain fatty acids (MCFA) on cardiovascular disease risk factors 48, 49. Some of those studies have found that medium chain fatty acids (MCFA) consumption increased total cholesterol and low-density lipoprotein cholesterol (LDL-C) to the same extent as palm oil 50 and led to higher levels of triglycerides (TG) than palm oil and sunflower oil 50, an other diet rich in long chain fatty acids (LCFA) 51, or soybean oil 52. Reductions in HDL-C “good” cholesterol 51 and absence of effects on total cholesterol, LDL-C “bad” cholesterol, and HDL-C “good” cholesterol have also been noted with medium chain fatty acids (MCFA) soybean oil consumption 52. Previous studies with medium chain triglyceride (MCT) oil showed reductions in total cholesterol and LDL-C “bad” cholesterol and no change in HDL-C “good” cholesterol or triglycerides 49, 48 but the MCT oil was fed along with plant sterols, which are known to reduce total cholesterol and “bad” cholesterol 53, 54 and safflower oil, an oil rich in n-3 polyunsaturated fats (omega 3 fatty acids). Hu et al. 55, however, have found that MCT oil did not increase the risk of coronary heart disease in the Nurses’ Health Study whereas consumption of long chain saturated fats did. Therefore, whether MCT oil truly has a negative impact on cardiovascular disease risk remains to be firmly established. This is particularly important since MCT oil has been taunted as a potential weight-lowering agent 56.
What does MCT oil do?
Medium-chain triglycerides (MCT) contain medium-chain fatty acid (MCFA) attached to glycerol molecule 1. Medium-chain fatty acid (MCFA) includes caprylic acid (C8), capric acid (C10) and lauric acid (C12) 1. MCT oil is a source of ketone bodies and are hydrolyzed to produce medium chain fatty acids (MCFAs) by the enzyme lipase 57. The metabolism, digestion and absorption of medium-chain triglycerides (MCT) is different than that of long-chain triglycerides (LCT). Human endogenous enzyme lipase brings about hydrolysis of medium-chain triglycerides (MCT). After hydrolysis the medium-chain fatty acid (MCFA) are released from glycerol backbone and because of its hydrophilic nature (tendency to mix with or dissolve in water) and shorten carbon chain these medium-chain fatty acid (MCFA) are directly transported via hepatic portal vein to liver and it is not dependent on the transporter protein for mitochondrial entry 58, 59, 60. This quick metabolism of MCFA results in formation of ketone bodies. These ketone bodies act as an immediate energy source to body. The hydrolysed medium chain fatty acid does not go to lymphatic system for re-synthesis of triglyceride molecule which has ability to be stored in the form of adipose tissue as fat, leading to obesity 61.
Medium chain triglyceride (MCT, C6 to C12) are rapidly absorbed from the gastrointestinal tract, and unlike long chain fatty acids (C13 to C22) and move directly into the liver via the portal vein and do not promote triglyceride synthesis 62, 63, 64, 65, 66. Some of the medium chain triglyceride (MCT) consumed is converted into ketone bodies in the liver (ie. beta-hydroxybutyrate), but some also remains as medium chain fatty acids (MCFA, saturated fatty acids of 6–12 carbons in chain length) in the blood, the relative amount of which depends on the MCT consumed 67, 68. For example, C8 medium chain triglyceride (caprylic acid) produces more ketone bodies than C10 medium chain triglyceride (capric acid) 69. Beta-hydroxybutyrate is one of the three ketone bodies, along with acetoacetate and acetone, that serve as an alternative fuel source for your body when glucose is scarce, particularly during fasting, prolonged exercise, or on a ketogenic diet 70. Ketones or ketone bodies in your blood or urine indicate that your body is burning fats instead of glucose for energy. Having ketones means your body is using its backup energy source — fats. For people on a ketogenic diet, MCT oil can help the body enter and stay in a state of ketosis by increasing the production of ketone bodies 71, 72, 73. The degree of ketosis induced by MCT oil is not as large as with exogenous ketone ester intake (CJ et al., 2018; Stubbs et al., 2018), but it is comparable to that of ketogenic diets 74, 75 and is greater than ketosis occurring after a 12-hour fasting period (Boden et al., 2005; CJ et al., 2018). Medium chain triglyceride (MCT) oil has the potential to produce a nutritional source of ketones for an alternative brain fuel to glucose or by the consumption of MCT oil or esterases in freeze‐dried form 21, 76, 77, 30, 78, 27, 79. This is independent of the fasting state or carbohydrate intake. The brain can use ketones from MCTs as an alternative fuel source to glucose 80, 81, 82, 83. This has led to research on its potential to improve cognitive function in individuals with conditions like Alzheimer’s disease 84. No clinical studies have yet found that MCT oil can prevent dementia, but some evidence suggests that there may be short-term cognitive benefits from taking MCT oil, including for patients with dementia 63, 7, 76, 21, 77, 30, 78, 27. Improvements in cognitive functions in patients with Alzheimer’s disease and mild cognitive impairment (MCI) were seen in the general 85, 27, 7, 86, 87, 79, 88, memory (n = 3) 89, 88, 90, language 86, 89, 88, and attention domains, after MCT treatments 86, 89, 88; and hyperketonemia induced by MCT intake might be responsible for the changes in cognitive function 91. The increase in blood ketone levels following MCT oil administration was seen in seven of the studies 90, 27, 89, 79, 88, 92. Correlating blood ketone levels to cognitive function assessment scores found a significant positive correlation, and hence, improvement in cognitive function assessment score is directly related to an increased blood ketone level 93.
Several clinical trials have tested MCT oil in patients with and without dementia and reported benefits 63, 7, 76, 21, 77, 30, 78, 27. Some meta-analyses and systematic reviews of these studies overall suggest potential cognitive benefits of MCT usage, though not all do 94, 95, 93, 60. Many of the studies had design issues. For instance, some studies were small, or did not compare medium chain triglyceride (MCT) to a placebo, or were not blinded – that is, the participants knew they were receiving medium chain triglyceride (MCT) – which means results could be biased. Studies also used very different kinds and doses of MCTs. Some of the studies found no benefit of MCTs, including one Phase 3 study 92. Overall, the evidence suggests that MCT oil might have benefits in patients with Alzheimer’s disease or those at higher risk of Alzheimer’s disease (i.e., individuals with mild cognitive impairment), but larger and better controlled studies are needed to determine whether these benefits are real. It is also not known what the long term effects are of taking MCT oil, as no identified trial lasted longer than six months 96. The use of MCT oil remains controversial due to the concern of increased cardiovascular disease risk. MCT is a type of saturated fatty acid (SFA), and intakes of saturated fats have been shown to increase total cholesterol and LDL cholesterol levels (bad cholesterol) 97. Therefore, the potential harmful health effects on long-term consumption of MCT oil remain a concern for its use in the treatment of Alzheimer’s disease 93.
Although some laboratory studies provide a biological rationale of how MCT oil might benefit brain health such as improving brain cell function, preventing Alzheimer’s-like pathology, and enhancing learning in older animals 98, 99, 32, there are no clinical data that showed MCT oil promotes long-term brain health. Despite potential cognitive benefits for patients with dementia have been reported, larger and longer studies looking specifically at individuals with dementia are needed 94, 93. No human studies have examined whether MCT oil can prevent or delay dementia. Some preclinical laboratory studies suggest that MCT oil may improve some measures of cognition and prevent amyloid plaque formation in animals, but these results have not been confirmed in humans 32, 100, 99.
Medium chain triglycerides (MCT) of 8 and 10 carbons (C8 to C10) are ketogenic. Some of the medium chain triglyceride (MCT) consumed is converted into ketone bodies in the liver (ie. acetone, acetoacetate and beta-hydroxybutyrate), but some also remains as medium chain fatty acids (MCFA, saturated fatty acids of 6 to 12 carbons in chain length) in the blood, the relative amount of which depends on the MCT consumed 101, 26, 67, 68. For example, according to Vandenberghe et al. 102, the ketogenic effect of MCT oil depends on the percentage of caprylic acid (C8) and capric acid (C10). The ketogenic effect of C8 medium chain triglyceride (caprylic acid) is two-fold that of C10 medium chain triglyceride (capric acid) 69. Fatty acids with carbon chain lengths≤8 can cross the inner mitochondria membrane in the absence of carnitine palmitoyl transferase I 103. Moreover, C8 medium chain triglyceride (caprylic acid) appears to experience beta-oxidation in astrocytes more easily than C10 medium chain triglyceride (capric acid), hence more readily induces ketogenesis 104. This could suggest that MCT oil may have different effects on blood lipid profile due to difference in C8 and C10 levels. MCT oil transiently raise plasma ketone bodies to 0.5 to 1.0 mmol/L when taken as a 10 to 15 g dietary supplement at meals 105, 73, 102. Plasma ketones increase in a direct dose-response relationship to the oral dose of MCT oil consumed 106. Emulsifying (the process of dispersing two or more immiscible liquids together to form a semistable mixture) or consuming MCT oil without a meal increases their ketogenic effect 106, 102. Moreover, 20 g of medium chain triglyceride C8 produced a significantly stronger ketogenic response than 10 g of medium chain triglyceride C8 107.
Clinical studies have shown that consumption of Medium chain triglycerides (MCTs) leads to greater energy expenditure than does consumption of long-chain triacylglycerols (LCTs) 108, 109, 110, 111, 112. Such studies suggest that MCT oil consumption may be useful for weight management. MCT oil based diet has also been shown to reverse hypertrophic cardiomyopathy in a patient with very long chain acyl-coA dehydrogenase deficiency 113. Very long chain acyl-CoA dehydrogenase (VLCAD) deficiency is one of the genetic defects of mitochondrial fatty acid beta-oxidation presenting in early infancy or childhood. If undiagnosed and untreated, very long chain acyl-coA dehydrogenase deficiency deficiency may be fatal, secondary to cardiac involvement 113. Treatment is essentially dietary modification, with avoidance of long-chain fatty acids and supplementation with medium chain triglycerides, so that the enzyme-deficient step can be bypassed 114.
MCT oil is thought to lead to increases in triglyceride concentrations and increase LDL “bad” cholesterol with consequent development of cardiovascular diseases 115, 52. Another 2021 review involving six studies on whether MCT oil raises total cholesterol and LDL cholesterol levels found MCT oil increases total cholesterol, LDL cholesterol and triglycerides when compared to unsaturated fatty acids 116. However, this small 2008 study did not observe this in those results 117. Their finding confirms previous findings that MCT do not raise triacylglyceride concentrations when consumed at levels 12–20% of energy intakes 118, 119. Of the 3 studies that looked at the effect of MCT oil on blood lipid profile, 2 showed no change in triglyceride and cholesterol level 7, 120 and 1 showed that MCT oil significantly increased the concentrations of total cholesterol (TC) and high-density lipoprotein cholesterol (HDL-C or “good” cholesterol) 88. This is in consensus with previous studies, which suggested no effect of MCT on cholesterol metabolism 121, 25. Furthermore, a 2018 systematic review and meta-analysis demonstrated that MCT oil consumption could increase high-density lipoprotein cholesterol (HDL or “good” cholesterol) levels without changing non-HDL-cholesterol in comparison with long-chain saturated fatty acids 122.
Asakura et al. 123 did not observe any change in fasting triglyceride concentrations with increasing MCT consumption up to maximum of 24 g/d for periods of 2 weeks each. It is possible that dose may have played a role in the earlier findings that MCT raise triglyceride concentrations. In fact, in the studies by Hill et al. 52 and Swift et al. 51, where triglyceride concentrations increased by 200% and 42%, respectively, subjects consumed 40% of energy in the form of MCT oil. The studies provided either 150% of weight-maintenance energy requirements 52 or 100% of weight-maintenance energy requirements 51. In the study by Cater et al. 50, triglyceride concentrations were higher after 3 weeks of MCT oil consumption at a level of 43% of energy intake compared to equivalent amounts of palm oil and high oleic sunflower oil. Swift et al. 51 had also recognized a potential dose effect when one of their study groups consuming half of the MCT dose of the MCT group (ie. 20% of energy intake) had no significant increase in fasting triacylglyceride. Therefore, it is possible that MCT oil consumption at a level of 20 to 60 g/d, or 12–20% of energy intake, does not result in adverse effects on triglyceride levels.
The data also agree with those of Hill et al. 52 who found that overfeeding men with MCT oil for 6 days did not result in any change in total cholesterol or HDL-C “good” cholesterol. However, that study was very short in duration and potentially not long enough to effect changes in lipid parameters. Similarly, in a weight maintenance setting, the same group did not find any effect of MCT consumption for 6 days on total cholesterol or LDL-C “bad” cholesterol but found reductions in HDL-C “good” cholesterol with MCT oil consumption 51. Data show that MCT oil consumption has a similar effect on plasma total cholesterol and LDL-C “bad” cholesterol as olive oil when consumed at similar levels. This is in contrast with data comparing MCT oil consumption and high oleic sunflower oil 50. In that study 50, MCT oil consumption led to higher total cholesterol and LDL-C “bad” cholesterol concentrations than high oleic sunflower oil consumption after a 3 week period. This may be partly attributed to the higher plant sterol content of sunflower oil compared to olive oil 124; plant sterols being well known for their hypocholesterolemic effect 125.
MCT oil consumption had no effect on glucose or insulin concentrations 117. This is similar to the observations of Hill et al. 52 in their overfeeding study with MCT and soybean oil and in a 12-week weight loss study comparing MCT and rapeseed oil/soybean oil consumption 126. An early study by Yost et al. 127 also found that MCT oil consumption, at a level of 77.5% of total fat intake for 30 days, did not lead to reductions in fasting glucose or insulin concentrations in type 2 diabetics. It therefore appears that MCT oil consumption has little impact on glycemic control.
Olive oil consumption at a level of approximately 12% of energy intake did not have any significant impact on fasting plasma lipid concentrations. This is in agreement with earlier work showing that monounsaturated fatty acids are not as effective as polyunsaturated fatty acids in reducing plasma cholesterol concentrations 128. Studies have, however, shown that olive oil consumption results in lower total cholesterol and LDL-C “bad” cholesterol and triacylglyceride than consumption of an average American diet 129. More recently, studies have shown that olive oil results in higher total cholesterol and LDL-C “bad” cholesterol and triacylglyceride than sunflower oil or rapeseed oil consumption 124 or not different from an average American diet with regards to effects on total cholesterol and LDL-C “bad” cholesterol, HDL-C “good” cholesterol or triacylglyceride 130. MCT oil consumption does not differ from olive oil in its effects on cardiovascular disease risk and may thus be considered to be a neutral dietary fat as well.
MCT oil health benefits
Medium-chain triglyceride (MCT) oil has been reported as a therapeutic aid for Alzheimer’s disease, epilepsy, and malabsorption 131, 132, 133, 134, 135. Moreover, MCT oil has been considered to improve endurance exercise performance by providing a quick source of energy because medium-chain triglycerides (MCTs) can quickly undergo beta-oxidation 133, 136, 137, 138. However, others showed no evidence that supports its use to improve physiological functions in endurance exercise 139, 140, 141, 142, 143, 144, 145, 146. More human studies are needed for MCT oil to confirm many of these effects and potential benefits.
Energy Source: MCT were first launched as a source of energy in 1950. Due to their shorter chain length, MCTs are quickly absorbed and transported directly to the liver, where they are converted into energy. This makes MCT a popular choice for athletes and sports person looking for an immediate energy source and also for humans having inability in metabolizing sugar due to old age.
Weight Management: Some studies suggest that MCT oil can increase the release of hormones that promote a feeling of fullness, potentially leading to a reduction in overall calorie intake 147. Zhang et al. 148 reported that diet rich in MCT can lead to increase in fat oxidation (fat burning) and increase in energy expenditure in healthy adults fed with 2% MCT in diet for 3 months, which can contribute to modest weight loss. For people on a ketogenic diet, MCT oil can help the body enter and stay in a state of ketosis by increasing the production of ketone bodies.
Brain Health and Cognitive Function: The brain can use ketones from MCT oil as an alternative fuel source to glucose. This has led to research on its potential to improve cognitive function in individuals with conditions like Alzheimer’s disease and dementia. A recent study on rats showed that diet rich in MCT can reduces anxiety and leads to improve social behaviour in rats 149, 150. MCT diet containing only caprylic acid (Octanoic acid, C8) and capric acid (decanoic acid, C10) has been shown to improve attention and structural connectivity in the brains of patients with mild cognitive impairment 151. These effects are closely related to metabolism of MCT which generates ketone body namely beta-hydroxybutyrate. Increase in formation of this ketone body results in positive cognitive effects by boosting memory in memory-impaired adults 152.
Antimicrobial and Anti-fungal Properties: Some of the fatty acids in MCT oil, such as lauric acid, have been shown to have antimicrobial effects, which may help fight off certain bacteria and fungi. MCT is also found to be effective against SARS Coronavirus-2 (Covid-19 virus). MCT is able to change the metabolism of lipids in virus. Virus replicates quickly and for this replication energy is needed which is extracted from long chain fatty acids. Long chain fatty acids (LCFA) are also needed for attachment of virus envelope with the host. MCT decreases formation of long chain fatty acid thereby making it unavailable to virus, leading to death of virus. MCFA released from glycerol backbone after lipase hydrolysis are believed to have antimicrobial properties. MCFA destroys the bacterial colony in intestinal tract by decreasing the pH. Recent research reported that 3% MCT supplement results in decreasing the total coliform bacteria present in rectum and colon. MCT can also be used as an effective antibiotics against the bacterial growth 153. But to use MCT as antibiotics needs further study as this is just a single study reported in literature for medium chain fatty acids (MCFA) as potential antimicrobial agent.
Long-chain fatty acid oxidation disorders (LC-FAOD) are a group of rare autosomal recessive genetic conditions where the body has trouble breaking down long-chain fatty acids for energy and accumulation of toxic metabolites 154, 155. This can lead to energy deficiencies and a buildup of harmful fatty acid byproducts, affecting various organs. Common symptoms include muscle weakness, low blood sugar, and heart problems. Treatment includes dietary management, including maximum fasting guidelines (under healthy steady-state conditions and according to age), restricted long-chain triglyceride (LCT) intake and supplementation with medium-chain triglyceride (MCT) oil and sometimes medication 156, 157.
MCT oil may be used to aid in fat absorption issues in people with malabsorption syndromes 26, 158, 159, 160, 161.
MCTs have also been used as a keto diet (modified Atkins diet), as a substitute for carbohydrates in patients with intractable pediatric epilepsy or drug-resistant epilepsy 162. The ketone bodies generated after metabolism of MCT are transported to brain cell shows good results in reduction of seizures as compared to ketone bodies generated by glucose metabolism. Ketogenic diets, which are designed to produce high levels of ketone bodies, decrease seizure frequency in patients with refractory epilepsy. In the 1920s, several papers were published on the effects of fasting on epilepsy 163. Wilder et al. 164 thought that if they could create a state of ketosis, they could achieve the same effect as fasting, so they implemented a dietary regimen and observed a dramatic reduction in epileptic seizures. The diet at that time is referred to as the classic ketone diet 164. Later, Huttenlocher et al. 165 developed a MCT- ketogenic diet that allows efficient ketone production with less lipids by using MCTs. The MCT ketogenic diet allows for an increase in carbohydrate and protein due to the potential to increase ketone levels through the inclusion of MCT fats. Furthermore, the results of randomized controlled trials have reported that the effects of the classical ketone diet and the MCT-ketone diet are equivalent 166.
An oil-based MCT diet has also been used to treat hypertrophic cardiomyopathy in a patient with a deficiency in the gene coding for acyl-coA dehydrogenase 167
Table 2. Commercially available MCT products
| MCT oil brand | Application | Producer |
|---|---|---|
| MCT oil | Act as a fuel to brain and body | Nature way, USA |
| Powdered MCT Oil | Ketogenic diet | Quest Nutrition USA |
| MCT Oil (mixture of C8 and C10) | Food applications like bakery and confectionary | AAK Kamani, India |
| Joymix MCT Oil | For weight management | Malaysia |
| Keto products | Source of energy | 360 Nutrition, USA |
| Keto organic MCT Oil | Used for weight loss | Ancient Nutrition, USA |
| MCT powder | Help to control cardiovascular diseases | Ogranika, Canada |
| Liquid MCT Oil | Supplement to be used in food formulation | Supplement manufacturer, UK |
| Spring valley oil | Management of weight and for athletes | Spring valley, USA |
| Soft gel (MCT Oil) | Improved fat metabolism | Carlson Lab, USA |
| Melrose MCT powder and MCT oil | Energy for brain and body | Melrose, Australia |
| MCT Oil | Source of energy | Bioglan, Australia |
| Max-C8 | Proper metabolism, digestion, energy, weight management | Zenwise health, Germany |
| Pure tricaprylin oil | Weight management | Weight world, UK |
| Diet MCT Oil | Nutraceutical fat and source of energy | Diet works, USA |
MCT oil for weight loss
Dietary fat is often blamed for the rising prevalence of obesity 168. However, all fats are not equal in their metabolic effects. For example, MCT (medium-chain triacylglycerols), which typically contain fatty acids with chain lengths of ≤10 carbon atoms, are processed differently from long-chain triacylglycerols (LCTs) by the body 169. Because of their chain length, medium-chain fatty acids can be absorbed in the gastrointestinal tract and transported to the liver via the portal circulation without incorporation into chylomicrons. As a result, it is hypothesized that MCTs are oxidized to a greater extent than are long-chain triacylglycerols (LCTs) and have less opportunity for deposition into adipose tissue 170. These characteristics of MCTs have been well demonstrated in animal studies, in which rats were shown to have smaller adipose tissue mass if fed MCTs than if fed long-chain triacylglycerides (LCTs) 171, 172. Human studies have also long shown that MCTs increase fat oxidation and thermogenesis compared with LCTs in short-term feeding studies 109, 110, 111, 112. More recently, St Onge et al. showed in women 173 and in men 174 that this remains the case even over prolonged consumption periods of up to 4 weeks. Furthermore, St Onge et al. showed that when men consume a diet rich in MCTs, they lose more fat mass than when they consume an equicaloric diet rich in LCTs from olive oil 174.
As a result of data showing increased thermogenesis and lower fat deposition with MCT consumption, it has been hypothesized that MCT oil may be a useful adjunct to a weight-loss diet.
This very small randomized clinical study with 31 healthy overweight and obese subjects (body mass index: 29.8 ± 0.4, in kg/m2) 117 shows that long-term consumption of moderate amounts of saturated fats, in the form of MCT oil, does not have adverse effects on cardiovascular disease risk factors. In that small study, thirty-one men and women, age 19–50 y and body mass index 27–33 kg/m2, were randomized to a 16-week weight loss program 117. The weight loss program (EatRight program) is a 12-week program that teaches good nutrition habits and provides tips for better weight control and weight loss. Four lessons were added to the basic program to account for the longer duration of this weight-loss study. The sequence and topics for each counseling session are shown in Table 2. The subjects were provided EatRight materials weekly and discussed the weight-loss principles taught with the dietitian.
As part of the weight-loss program, the subjects were counseled to reduce their caloric intakes to 1500 kcal/d for women and 1800 kcal/d for men 18. Within this diet, all subjects received study muffins (either cranberry or blueberry; Krusteaz, Seattle, WA) that contained 10 g of their assigned oil and 8 or 14 g of liquid oil, for women and men, respectively, to incorporate into their foods during cooking. Therefore, all subjects received ≈12% of their prescribed weight-loss energy requirements in the form of the study oil (18 g for women and 24 g for men) in their foods during cooking. This level of oil was chosen because it was found to produce significant increases in energy expenditure 109, which is believed to be the main mechanism of action for weight loss with MCT oil.
The subjects, along with the dietitian and clinical coordinator, were unaware of the oil each person was consuming. Muffins were given to the clinical coordinator in bags labeled with the subject’s study ID code and A or B to designate group. Oil was provided in opaque plastic containers, which were also labeled with the subject’s study ID code and A or B. Neither the dietitian nor the clinical coordinator knew which oil was A and which one was B. The oils did not impart any particular taste to the study muffins. Also, because the subjects were instructed to consume the liquid oil in stir-frying and with foods, it is unlikely that they could identify which study oil they were being provided. Another point of note is that none of the subjects had previously tasted MCT oil and therefore had no point of reference to determine whether it tasted any different from olive oil.
Body weight and waist circumference were measured at each weekly session by the clinical coordinator.
MCT oil consumption resulted in lower endpoint body weight than did olive oil (−1.67 ± 0.67 kg) after the 16 week study [see Table 3] 18. This agrees with the study authors previous data 173 and hypothesis put forth previously concerning the potential for enhanced weight management with MCT consumption 175. Tsuji et al 176 found that overweight subjects consuming a diet containing ≈10 g MCT oil/d for 12 wk lost 1.34 kg more than did a group consuming 10 g of an LCT oil (rapeseed oil–soybean oil blend). Similar results were also obtained with subjects consuming 5 g of MCT or LCT oil/day 177. In that study, weight loss over a 12-week period was enhanced by 1.3 kg, which could extrapolate to 1.7 kg over a 16-week period. Weight-loss data from these 2 studies, extrapolated to 16 week, are similar to those obtained in the present study 18.
The 16 week weight loss study comparing MCT oil and olive oil combined with a weight loss program that includes reduced calories consumption and diet counseling, showed the inclusion of MCT oil in a weight-loss program leads to greater weight loss than does the inclusion of a similar amount of olive oil. The addition of an enhanced thermic effect of food and reduced food intake would result in a lower caloric retention of 107.5 kcal/d. This lower caloric retention, if maintained over a 16-wk period, would lead to an additional loss of 1.55 kg body wt with MCT consumption than with long-chain triacylglyceride (LCT). However, the study was not able to show differences in adipose tissue distribution between the different diets 18.
There was a trend toward greater loss of fat mass and trunk fat mass with MCT oil consumption than with olive oil. Endpoint trunk fat mass, total fat mass, and intraabdominal adipose tissue were all lower with MCT oil consumption than with olive oil consumption 18. The results also show that MCT oil consumption leads to comparable effects on cardiovascular disease risk factors as an equal amount of olive oil, an oil considered to have beneficial health effects 129.
Table 3. Fatty acid profile of MCT oil and Olive oil per 100 g of oil used in the weight loss study
| Fatty acid | MCT oil | Olive oil |
|---|---|---|
| C8:0 | 55 | 0 |
| C10:0 | 45 | 0 |
| C12:0 | 0 | 0 |
| C14:0 | 0 | 0 |
| C16:0 | 0 | 11.29 |
| C16:1 | 0 | 1.255 |
| C17:0 | 0 | 0.022 |
| C17:1 | 0 | 0.125 |
| C18:0 | 0 | 1.953 |
| C18:1 | 0 | 71.269 |
| C18:2 | 0 | 9.761 |
| C18:3 | 0 | 0.761 |
| C20:0 | 0 | 0.414 |
| C20:1 | 0 | 0.311 |
| C22:0 | 0 | 0.125 |
Figure 4. MCT oil versus Olive oil weight loss
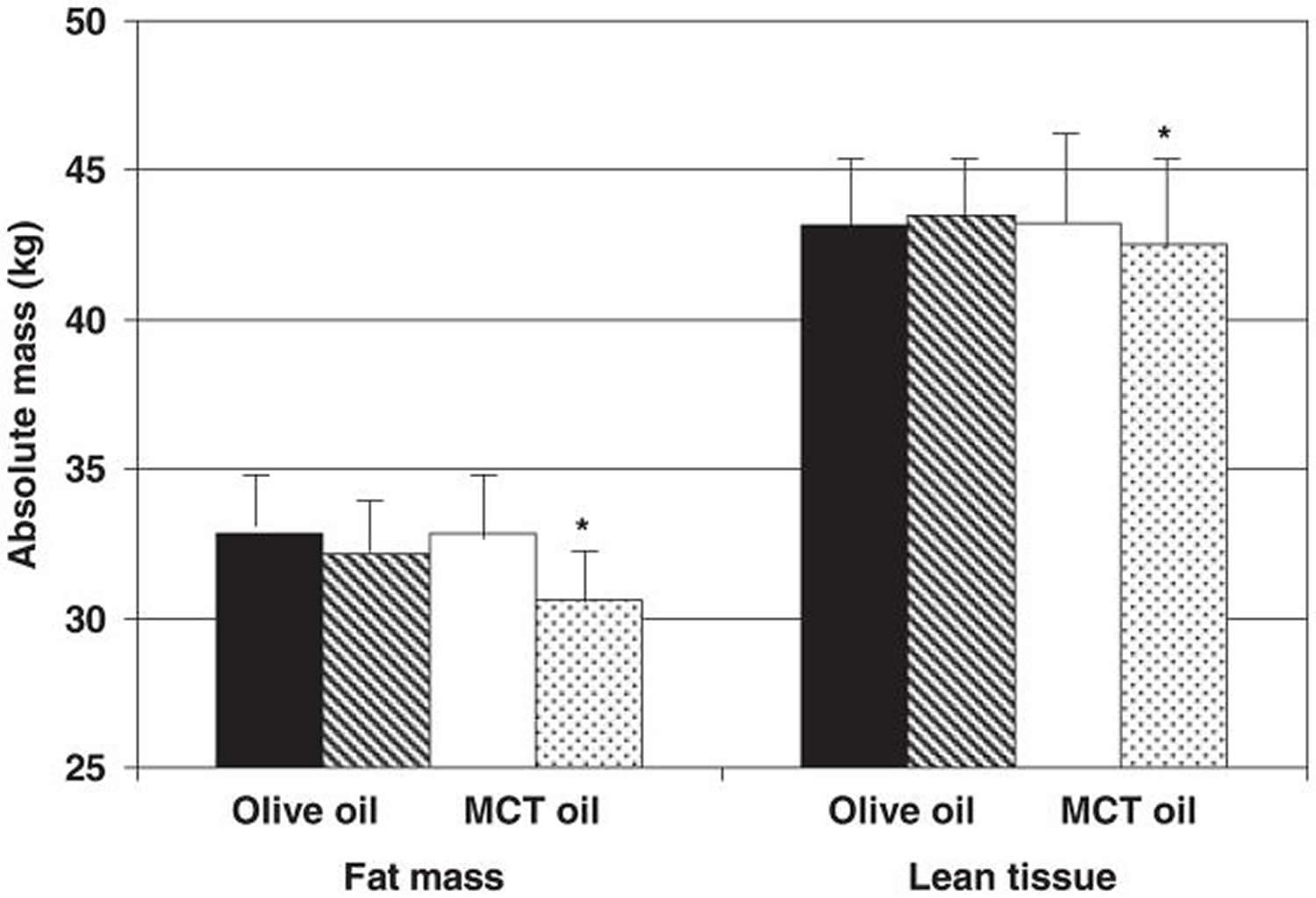
Footnotes: Mean absolute body composition, assessed by dual-energy X-ray absorptiometry, at baseline and at the endpoint of a 16-week weight-loss program that included either olive oil (baseline = black bars; endpoint = dark gray bars; n = 15) or medium-chain triacylglycerol (MCT) oil (baseline = white bars; endpoint = light gray bars; n = 16). There was a trend for a diet-by-week interaction on lean tissue. There was a trend for a diet-by-week interaction on absolute total fat mass and fat massand a trend for a diet effect on fat mass. There was a significant effect of week on fat mass (P = 0.0013).
[Source 18 ]Table 4. Change in adipose tissue compartments, assessed by dual-energy X-ray absorptiometry and computed tomography, during consumption of either olive oil or medium-chain triacylglycerol (MCT) oil as part of a weight-loss diet for 16 week
| Change in body compartment | MCT oil (n = 16) | Olive oil (n = 15) |
|---|---|---|
| Total fat mass (%) | −1.46 ± 0.45 | −0.58 ± 0.46 |
| Total fat mass (kg) | −2.23 ± 0.57 | −0.69 ± 0.58 |
| Trunk fat mass (%) | −1.23 ± 0.73 | −0.49 ± 0.75 |
| Trunk fat mass (kg) | −1.20 ± 0.35 | −0.34 ± 0.36 |
| Intraabdominal adipose tissue (cm2) | −8.85 ± 3.92 | −1.32 ± 4.19 |
| Subcutaneous abdominal adipose tissue (cm2) | −24.76 ± 9.37 | −11.29 ± 10.02 |
Summary
The thought process behind MCT’s is that they are rapidly broken, go straight to the liver and may play a role in weight loss. They are also considered to not adversely affect blood cholesterol levels. Although MCT oil plus weight loss program study 18 cannot distinguish which side of the energy balance equation played a bigger role in weight loss (enhanced suppression of food intake or enhanced thermic effect of food), the data complement the body of literature concluding that MCT oil can be successfully used in a weight-management program to enhance weight loss. However, a recent study 178 looking at MCT oil in adolescents showed no increase in thermogenesis, or a decrease in appetite or satiety. More research is needed into the use of MCT oil as a tool in weight management in overweight and obesity. Furthermore, previous studies have shown that MCT oil can used as a special-purpose food as a supportive nutritional therapy in the management of childhood diarrhea 179. MCT oil may be also used to increase the calorie value, improve the palatability, digestibility, absorption and transport of a diet indicated for diseases with maldigestion/malabsorption 180, 181. The effect of MCT oil on malabsorption states is related to the circumstance that the molecularly small medium chain fatty acids are more easily hydrolyzed by pancreatic lipase and, therefore, more rapidly absorbed than conventional fats 180. In that study on children with dairrhea 179, MCT oil supplemented group was heavier (10.3 kg versus 8.9 kg), had greater proportion of weight gain, lesser proportion of weight loss (14.3% versus 55.6%) and with no weight change (14.3% vs. 22.2%) compared to the non-MCT supplemented group. There was a statistical significant difference in the rate of weight gain among subjects in the MCT group compared to subjects in the non-MCT group (0.22 + 0.22 kg/day vs. -.048 + .26 kg/day). In this childhood diarrhea study 179, MCT oil was administered equally throughout the day, incorporated into the milk formula or meals, with a dosage of 15 ml per day, which was on the average 46.8% of the total fat calorie. During the course of MCT oil administration, no significant clinical symptoms warranted the discontinuation of therapy. These MCT oil studies show that fats have a place in a weight-loss diet and that choosing MCT oil is interesting, especially in light of the effects of MCT oil consumption on energy balance and weight control – MCT oil may provide weight loss or even weight gain benefits wihout the adverse effects of saturated fats.
MCT oil side effects
Therapeutic use of MCT oil at three tablespoons daily (42 g) has been limited due to the occasional occurrence of mild gastrointestinal symptoms, including crampy abdominal pain, nausea, vomiting, and diarrhea 7. Reportedly, these symptoms can be minimized by taking MCT oil with meals 182, 183. MCT oil should be introduced in small amounts, given at room temperature, diluted with an equal volume of water or fruit juice, and taken slowly 184. In this study on healthy subjects (0.5 g MCT oil per kg of body weight with 0.2 g glucose per kg of body weight in 200 mL of still-drinking water), participants experienced 50% fewer side effects when consuming MCT oil with glucose compared to MCT oil alone 185.
MCT oil vs Coconut oil
Coconut oil, extracted from the meat of the coconut is mostly composed of about 92 percent of saturated fat (SFA) with 62–70 percent being MCT 186, 26, 187, 188. Coconut oil also has 6% monounsaturated fat (oleic acid) and 1.7% polyunsaturated fat (linoleic acid). One tablespoon adds up to more than 11 grams of saturated fats, according to the federal National Nutrient Database 188. That’s nearly the total daily limit of 13 grams recommended by the American Heart Association. Replacing saturated fat with healthier fat in the diet lowers cardiovascular disease risk as much as cholesterol-lowering statin drugs, according to an American Heart Association 2017 Presidential Advisory 189. When you look at biomarkers of cardiovascular disease such as serum lipid profiles, studies show that coconut oil consistently raises cholesterol higher than monounsaturated (Oleic acid) and polyunsaturated oils (linoleic acid) 190.
It’s a common misconception that coconut oil and MCT oil are the same. While coconut oil is a rich source of medium-chain triglyceride (MCT, capric and caprylic acid), coconut oils typically have 13 percent to 14 percent of medium-chain triglyceride (MCT). Pure MCT oil has a much higher concentration of medium-chain triglyceride (MCT, capric and caprylic acid). The MCT oil used in the MCT Oil Consumption as Part of a Weight Loss Diet study was a special 100 percent medium-chain coconut oil 117. So, you would need to eat a lot of coconut oil to replicate the results used in the MCT Oil Consumption as Part of a Weight Loss Diet study 117. “No one eats 150 grams (10 tablespoons) of coconut oil in a day,” said the study author 117. Nor should they.
The thought process behind MCT’s is that they are rapidly broken, go straight to the liver and may play a role in weight loss. They are also considered to not adversely affect blood cholesterol levels. However, a recent study looking at MCT in adolescents showed no increase in thermogenesis, or a decrease in appetite or satiety 191. In another study comparing virgin coconut oil to extra virgin olive oil, there was also no difference in metabolism or fat oxidation 192.
The cardiovascular health benefits of coconut oil are cited from the studies looking at indigenous populations from India, Sri Lanka, Philippines, Polynesia and Melanesia. However, most of these populations rely on coconuts and not coconut oil. The remainder of their diet tends to be higher in whole foods and lower in sugar and processed foods. It should be noted that coconuts are a high fiber food. One cup of coconut flesh has 7 grams of fiber. Eating coconuts are not linked to cardiovascular disease.
In the case of the Pukapukans and Tokelauans, their overall diet is very low in sugar and rich in high fiber foods. It consists mainly of coconuts, breadfruit, and fish. There is little, if any, consumption of coconut oil 193.
The Kitava studies examined the Melanesian people in Papua New Guinea. Their overall fat intake is only 21%. In addition, their diet is mostly whole coconuts, tubers, fish, and fruit. Their intake of oils, margarine, and sugar is very little. In other words, mostly whole-food, plant-based diet.
When looking at Samoans, their traditional diet also consists of coconuts along with seafood, low intake of processed foods. Of course, all that has changed now with the widely available processed food, refined sugars and red meat (beef, spam) 193.
The bottom line is that coconut oil increases LDL cholesterol, does not increase thermogenesis or weight loss. Based on all the current research we have so far, regular use of coconut oil should not be advised. As always, a whole foods diet consisting of mainly plants should be the foundation of a healthy eating pattern.
Table 5. Coconut oil nutrition facts
| Nutrient | Unit | Value per 100 g | Tablespoon 13.6 g | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Approximates | |||||||||
| Water | g | 0.03 | 0 | ||||||
| Energy | kcal | 892 | 121 | ||||||
| Protein | g | 0 | 0 | ||||||
| Total lipid (fat) | g | 99.06 | 13.47 | ||||||
| Carbohydrate, by difference | g | 0 | 0 | ||||||
| Fiber, total dietary | g | 0 | 0 | ||||||
| Sugars, total | g | 0 | 0 | ||||||
| Minerals | |||||||||
| Calcium, Ca | mg | 1 | 0 | ||||||
| Iron, Fe | mg | 0.05 | 0.01 | ||||||
| Magnesium, Mg | mg | 0 | 0 | ||||||
| Phosphorus, P | mg | 0 | 0 | ||||||
| Potassium, K | mg | 0 | 0 | ||||||
| Sodium, Na | mg | 0 | 0 | ||||||
| Zinc, Zn | mg | 0.02 | 0 | ||||||
| Vitamins | |||||||||
| Vitamin C, total ascorbic acid | mg | 0 | 0 | ||||||
| Thiamin | mg | 0 | 0 | ||||||
| Riboflavin | mg | 0 | 0 | ||||||
| Niacin | mg | 0 | 0 | ||||||
| Vitamin B-6 | mg | 0 | 0 | ||||||
| Folate, DFE | µg | 0 | 0 | ||||||
| Vitamin B-12 | µg | 0 | 0 | ||||||
| Vitamin A, RAE | µg | 0 | 0 | ||||||
| Vitamin A, IU | IU | 0 | 0 | ||||||
| Vitamin E (alpha-tocopherol) | mg | 0.11 | 0.01 | ||||||
| Vitamin D (D2 + D3) | µg | 0 | 0 | ||||||
| Vitamin D | IU | 0 | 0 | ||||||
| Vitamin K (phylloquinone) | µg | 0.6 | 0.1 | ||||||
| Lipids | |||||||||
| Fatty acids, total saturated | g | 82.475 | 11.217 | ||||||
| Fatty acids, total monounsaturated | g | 6.332 | 0.861 | ||||||
| Fatty acids, total polyunsaturated | g | 1.702 | 0.231 | ||||||
| Fatty acids, total trans | g | 0.028 | 0.004 | ||||||
| Cholesterol | mg | 0 | 0 | ||||||
| Other | |||||||||
| Caffeine | mg | 0 | 0 | ||||||
MCT oil keto
Keto diet also known as ketogenic diet or ketone diet is a very low-carb, high-fat diet that shares many similarities with the Atkins diet and low-carb diets that is designed to produce ketones or the state of ketosis mimicking the metabolic state of fasting. The Atkins diet is a low-carbohydrate diet developed by Dr. Atkins for weight loss in obese individuals. Based on this diet, a modified Atkins diet was developed for patients who cannot continue to consume the classic ketogenic diet 194. Keto diet lowers blood sugar and insulin levels, and shifts the body’s metabolism away from carbs and towards fat and ketones. Keto diet involves drastically reducing carbohydrate intake, and replacing it with fat. Ketogenic diets are characterized by a reduction in carbohydrates (usually to less than 50 g/day) and a relative increase in the proportions of protein and fat 195. The reduction in carbs puts your body into a metabolic state called ketosis. When this happens, your body becomes incredibly efficient at burning fat for energy. It also turns fat into ketones in the liver, which can supply energy for the brain.
Ketogenic diets have been shown to be effective, at least in the short to medium term, as a tool to fight obesity including people with diabetes who are obese 196, hyperlipidemia and some cardiovascular risk factors 197, 198, 199. Clinical studies have shown significant improvements in weight loss, glycemic control, and lipid profiles among patients following a ketogenic diet 200. Keto diet’s ability to significantly lower blood glucose levels and improve insulin sensitivity is particularly beneficial for cardiovascular health 201. However, ketogenic diets also raise some concerns among physicians 202. Many of the concerns about the use of ketogenic diet as therapeutic tools could be attributed to a broad lack of knowledge about the physiological mechanisms involved. Ketogenic diets induce a metabolic condition named “physiological ketosis” by Hans Krebs, to distinguish it from the pathological diabetic ketosis 203.
Under normal diet with average amount of carbohydrates and fat, insulin activates key enzymes in the glucose metabolic pathways, which store energy derived from carbohydrates, and when there is an absence or scarcity of dietary carbohydrates the resulting reduced insulin level leads to a reduction in lipogenesis and fat accumulation. After a few days of fasting, or of drastically reduced carbohydrate consumption (below 20 g/day), glucose reserves become insufficient both for normal fat oxidation via the supply of oxaloacetate in the Krebs cycle (which gave origin to the phrase ‘fat burns in the flame of carbohydrate’) and for the supply of glucose to the central nervous system 204, 205, 206, 207.
Medium-chain triglycerides (MCTs) are rapidly metabolized into ketone bodies, providing a quick source of beta-hydroxybutyrate. Supplementation with MCT oil increases ketone levels and improves metabolic parameters associated with cardiovascular health 208. Studies have shown that MCT oil can enhance mitochondrial biogenesis and reduce inflammation, further supporting cardiovascular health 73. Beta-hydroxybutyrate is one of the three ketone bodies, along with acetoacetate and acetone, that serve as an alternative fuel source for your body when glucose is scarce, particularly during fasting, prolonged exercise, or on a ketogenic diet 70. Ketones or ketone bodies in your blood or urine indicate that your body is burning fats instead of glucose for energy. Having ketones means your body is using its backup energy source — fats. For people on a ketogenic diet, MCT oil can help the body enter and stay in a state of ketosis by increasing the production of ketone bodies. Medium chain triglyceride (MCT) oil has the potential to produce a nutritional source of ketones for an alternative brain fuel to glucose or by the consumption of MCT oil or esterases in freeze‐dried form 21, 76, 77, 30, 78, 27, 79. This is independent of the fasting state or carbohydrate intake. The brain can use ketones from MCTs as an alternative fuel source to glucose 80, 81, 82, 83. Multiple studies have suggested that increased ketone bodies, obtained through the consumption of MCT supplementation or coconut oil may provide an alternative energy source in Alzheimer’s disease, and alleviate the severity of symptoms in patients 91, 209, 90.
The question of why such a keto diet is effective for epileptic seizures has not yet been fully clarified. One of the hypotheses proposed is that acetoacetic acid, a type of ketone body, promotes the conversion of glutamate to glutamine, a cerebral neuroexcitatory transmitter, and then effectively converts glutamine to GABA, thereby suppressing neural excitation 210. It is also thought that a keto diet may suppress the intracellular glycolytic system and reduce the ATP concentration in neurons, thereby inhibiting electrical neuronal membrane excitation 211.
In 2016, new findings showed that capric acid (C10) inhibits neuronal excitation by binding to alpha-amino-3-hydroxy-5-methyl-4-isoxazolepropionic acid (AMPA) receptors at neuronal synapses 212. Other reports on the function of capric acid (C10) in suppressing epilepsy 213, 214. There are in vivo data supporting this hypothesis that capric acid (C10) crosses the blood-brain barrier 215. This study suggests a role for capric acid (C10) in the suppression of epileptic seizures through a ketogenic diet. A recent systematic review of 932 subjects (711 children aged 4 months to 18 years, and 221 adults aged 16 years and older) and 13 clinical studies on the efficacy of a ketogenic diet in drug-resistant epilepsy has been reported 216. In conclusion, all 13 studies were rated as high risk for detecting efficacy because they were not blinded and were conducted in small study populations. The systematic review stated that evidence for the use of a ketogenic diet, especially for adults, remains unclear, but did suggest that a ketogenic diet may have efficacy in children with drug-resistant epilepsy 216.
Figure 5. Metabolic pathway of ketosis and tissues ketolysis.
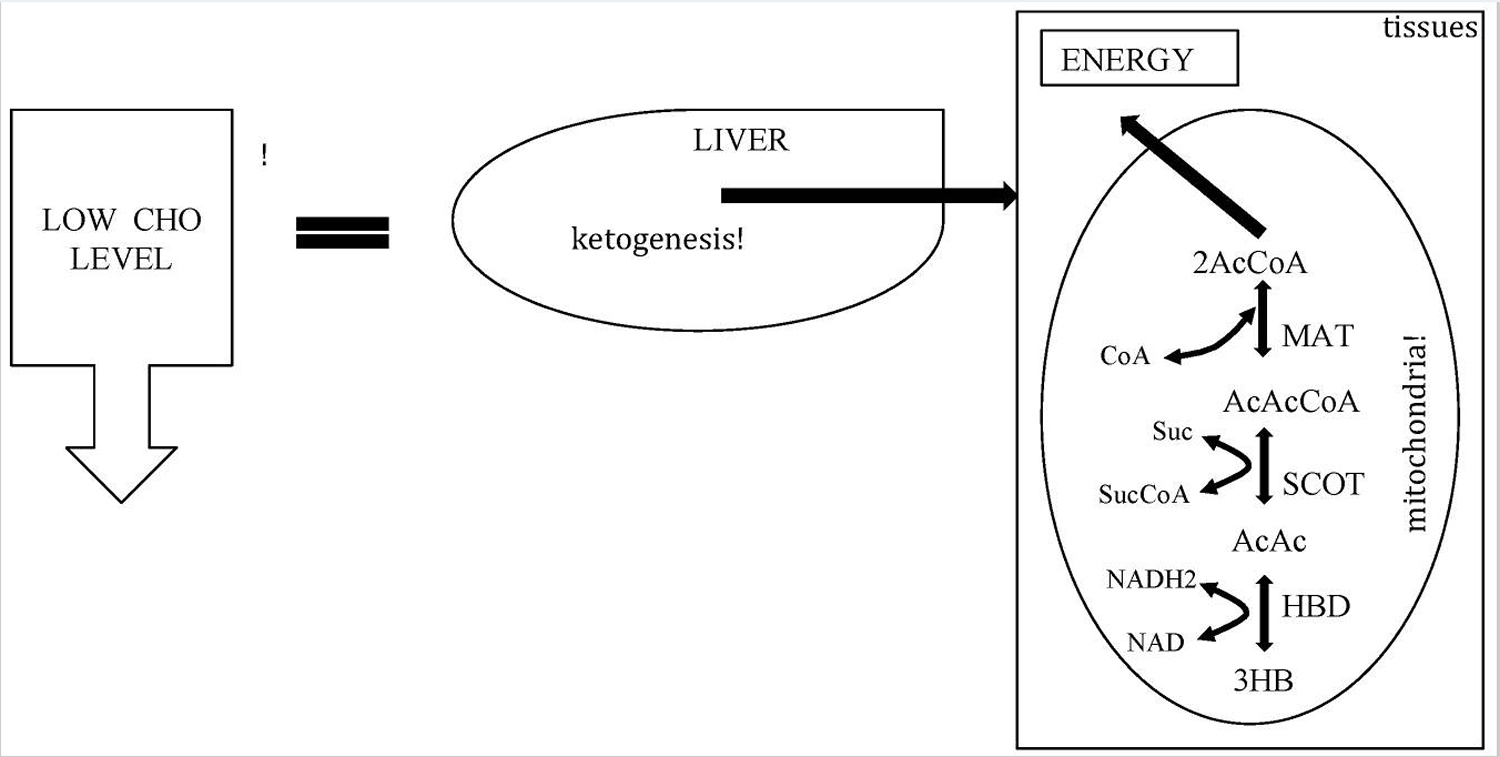
Figure 6. Ketone bodies formation from acetyl-CoA (acetyl coenzyme A).
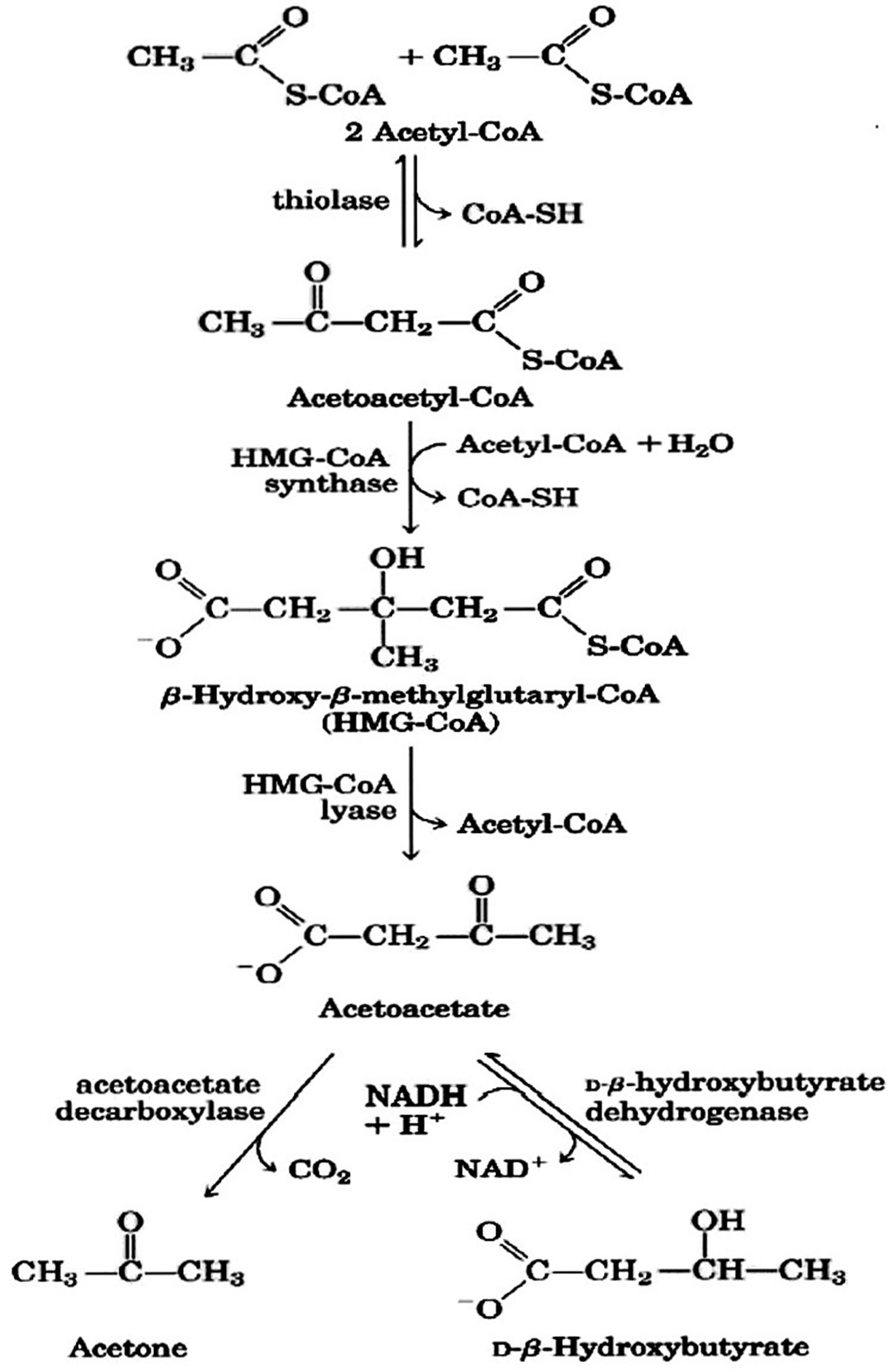
Footnotes: Ketone bodies are used by tissues as a source of energy through a pathway that involves firstly that bea-hydroxybutyric acid is converted back to acetoacetate (AcAc) this is then transformed into acetoacetyl-CoA and, finally, two molecules of acetyl-CoA are formed from acetoacetyl-CoA which are used in the Krebs cycle or Citric Acid cycle.
[Source 217]Different Types of Keto Diets
There are several versions of the keto diet, the standard keto diet (SKD) is the most researched and most recommended.
- Standard keto diet (SKD): This is a very low-carb, moderate-protein and high-fat diet. It typically contains 75% fat, 20% protein and only 5% carbs. A standard keto diet is an effective way to lose weight and lower risk factors for disease.
- Cyclical keto diet (CKD): This diet involves periods of higher-carb refeeds, such as 5 keto days followed by 2 high-carb days.
- Targeted keto diet (TKD): This diet allows you to add carbs around workouts.
- High-protein keto diet: This is similar to a standard ketogenic diet, but includes more protein. The ratio is often 60% fat, 35% protein and 5% carbs.
However, only the standard and high-protein ketogenic diets have been studied extensively. Cyclical or targeted ketogenic diets are more advanced methods, and primarily used by bodybuilders or athletes. The information in this article mostly applies to the standard ketogenic diet, although many of the same principles also apply to the other versions.
**The keto diet can boost insulin sensitivity and cause fat loss, leading to drastic improvement for type 2 diabetes and prediabetes.
Studies have now shown that the diet can have benefits for a wide variety of different health conditions. However, keep in mind that research into many of these areas is far from conclusive:
- Heart disease: The keto diet can improve risk factors like body fat, HDL levels, blood pressure and blood sugar.
- Cancer: The diet is currently being used to treat several types of cancer and slow tumor growth.
- Alzheimer’s disease: The diet may reduce symptoms of Alzheimer’s and slow down the disease’s progression.
- Epilepsy: Research has shown that the ketogenic diet can cause massive reductions in seizures in epileptic children.
- Parkinson’s disease: One study found that the diet helped improve symptoms of Parkinson’s disease.
- Polycystic ovary syndrome: The ketogenic diet can help reduce insulin levels, which may play a key role in polycystic ovary syndrome.
- Brain injuries: One animal study found that the diet can reduce concussions and aid recovery after brain injury.
- Acne: Lower insulin levels and eating less sugar or processed foods may help improve acne.
Summary
A keto diet may provide many health benefits, especially with metabolic, neurological or insulin-related diseases. You should check with your physician if you have any concerns about starting a ketogenic diet plan with pre-existing health conditions, especially if those conditions involve kidney, bone or heart problems. People with kidney disease should definitely consult with their physician about starting a ketogenic diet.
Talk to your doctor about implementing a ketogenic diet if you have any of these conditions:
- History of pancreatitis
- Active gall bladder disease
- Impaired liver function
- Impaired fat digestion
- Poor nutritional status
- Gastric bypass surgery
- Abdominal tumors
- Decreased gastrointestinal motility; this may be in conjunction with conventional cancer treatment and associated drugs
- History of kidney failure
- Pregnancy and lactation
A period of low carbohydrate ketogenic diet may help to control hunger and may improve fat oxidative metabolism and therefore reduce body weight. Furthermore new kinds of ketogenic diets using meals that mimic carbohydrate rich foods could improve the compliance to the diet. Attention should be paid to patient’s renal function and to the transition phase from ketogenic diet to a normal diet that should be gradual and well controlled. The duration of ketogenic diet may range from a minimum (to induce the physiological ketosis) of 2–3 weeks to a maximum (following a general precautionary principle) of many months (6–12 months). Correctly understood the ketogenic diet can be a useful tool to treat obesity in the hands of the physician.
MCT oil for dementia
Medium chain triglyceride (C6 to C12) are rapidly absorbed from the gastrointestinal tract, and unlike long chain fatty acids (C13 to C22) and move directly into the liver via the portal vein and do not promote triglyceride synthesis 62, 63, 64, 65, 66. Some of the medium chain triglyceride (MCT) consumed is converted into ketone bodies in the liver (ie. beta-hydroxybutyrate), but some also remains as medium chain fatty acids (MCFA, saturated fatty acids of 6–12 carbons in chain length) in the blood, the relative amount of which depends on the MCT consumed 67, 68. For example, C8 medium chain triglyceride (caprylic acid) produces more ketone bodies than C10 medium chain triglyceride (capric acid) 69. Beta-hydroxybutyrate is one of the three ketone bodies, along with acetoacetate and acetone, that serve as an alternative fuel source for your body when glucose is scarce, particularly during fasting, prolonged exercise, or on a ketogenic diet 70. Ketones or ketone bodies in your blood or urine indicate that your body is burning fats instead of glucose for energy. Having ketones means your body is using its backup energy source — fats. For people on a ketogenic diet, MCT oil can help the body enter and stay in a state of ketosis by increasing the production of ketone bodies. Medium chain triglyceride (MCT) oil has the potential to produce a nutritional source of ketones for an alternative brain fuel to glucose or by the consumption of MCT oil or esterases in freeze‐dried form 21, 76, 77, 30, 78, 27, 79. This is independent of the fasting state or carbohydrate intake. The brain can use ketones from MCTs as an alternative fuel source to glucose 80, 81, 82, 83. This has led to research on its potential to improve cognitive function in individuals with conditions like Alzheimer’s disease. No clinical studies have yet found that MCT oil can prevent dementia, but some evidence suggests that there may be short-term cognitive benefits from taking MCT oil, including for patients with dementia 63, 7, 76, 21, 77, 30, 78, 27.
Several clinical trials have tested MCT oil in patients with and without dementia and reported benefits 63, 7, 76, 21, 77, 30, 78, 27. Some meta-analyses and systematic reviews of these studies overall suggest potential cognitive benefits of MCT usage, though not all do 94, 95, 93, 60. Many of the studies had design issues. For instance, some studies were small, or did not compare medium chain triglyceride (MCT) to a placebo, or were not blinded – that is, the participants knew they were receiving medium chain triglyceride (MCT) – which means results could be biased. Studies also used very different kinds and doses of MCTs. Some of the studies found no benefit of MCTs, including one Phase 3 study 92. Overall, the evidence suggests that MCT oil might have benefits in patients with Alzheimer’s disease or those at higher risk of Alzheimer’s disease (i.e., individuals with mild cognitive impairment), but larger and better controlled studies are needed to determine whether these benefits are real. It is also not known what the long term effects are of taking MCT oil, as no identified trial lasted longer than six months 96. The use of MCT oil remains controversial due to the concern of increased cardiovascular disease risk. MCT is a type of saturated fatty acid (SFA), and intakes of saturated fats have been shown to increase total cholesterol and LDL cholesterol levels (bad cholesterol) 97. Therefore, the potential harmful health effects on long-term consumption of MCT oil remain a concern for its use in the treatment of Alzheimer’s disease 93.
One of the major genetic risk factors associated with Alzheimer’s disease is the presence of APOE (apolipoprotein E) gene in individuals 218. There are three types of the APOE (apolipoprotein E) gene, called alleles: APOE2, E3 and E4. Everyone has two copies of the APOE (apolipoprotein E) gene and the combination determines your APOE “genotype”—E2/E2, E2/E3, E2/E4, E3/E3, E3/E4, or E4/E4. The APOE E2 allele is the rarest form of APOE and carrying even one copy appears to reduce the risk of developing Alzheimer’s disease by up to 40%. APOE3 is the most common allele and doesn’t seem to influence risk. The APOE4 allele, present in approximately 10 to 15% of people, increases the risk for Alzheimer’s disease and lowers the age of onset. Having one copy of E4 (E3/E4) can increase your risk by 2 to 3 times while two copies (E4/E4) can increase the risk by 12 times 219. APOE E4 allele carriers were found to have decreased ability to metabolize glucose and lipids, and thus potentially affecting therapeutics targeting these pathways in the management of Alzheimer’s disease 220. Studies suggest that MCT oil supplementation might improve cognitive function only in, or to a greater extent in, patients who do not have an APOE4 allele 93. Subgroup analysis conducted found significant cognitive improvements in APOE E4 negative individuals in response to MCT treatment, while APOE E4 positive showed no benefit 88, 27, 79. It is suggested that APOE E4 carriers may have a different dose-response pattern compared to non-carriers, and hence differences in pathophysiology 79. In some other Alzheimer’s disease therapies, APOE E4 negative patients have shown to have greater benefits compared to APOE E4 positive patients, such as in glucose and insulin 221, nasal insulin 222, and insulin sensitizing agent rosiglitazone therapies 223 . One possible explanation could be that APOE E4 positive patients have lower mitochondrial enzyme function compared to APOE E4 negative patients as seen in Alzheimer’s disease brain tissue samples 224, 225. Reduced mitochondrial function is associated with reduced ability in ketone utilization, which could explain the unresponsiveness to MCT treatment in APOE E4 positive patients despite a significant increase in blood ketone 79. Further studies examining the role of APOE gene on the pharmacokinetic response patterns in Alzheimer’s disease patients may provide better explanations to the observed phenomenon.
Although some laboratory studies provide a biological rationale of how MCT oil might benefit brain health such as improving brain cell function, preventing Alzheimer’s-like pathology, and enhancing learning in older animals 98, 99, 32, there are no clinical data that showed MCT oil promotes long-term brain health. Despite potential cognitive benefits for patients with dementia have been reported, larger and longer studies looking specifically at individuals with dementia are needed 94, 93. No human studies have examined whether MCT oil can prevent or delay dementia. Some preclinical laboratory studies suggest that MCT oil may improve some measures of cognition and prevent amyloid plaque formation in animals, but these results have not been confirmed in humans 32, 100, 99.
- Jadhav HB, Annapure US. Triglycerides of medium-chain fatty acids: a concise review. J Food Sci Technol. 2023 Aug;60(8):2143-2152. doi: 10.1007/s13197-022-05499-w[↩][↩][↩][↩]
- Watanabe S, Tsujino S. Applications of Medium-Chain Triglycerides in Foods. Front Nutr. 2022 Jun 2;9:802805. doi: 10.3389/fnut.2022.802805[↩][↩][↩]
- Nimbkar S, Leena MM, Moses JA, Anandharamakrishnan C. Medium chain triglycerides (MCT): State-of-the-art on chemistry, synthesis, health benefits and applications in food industry. Compr Rev Food Sci Food Saf. 2022 Mar;21(2):843-867. doi: 10.1111/1541-4337.12926[↩]
- Hoang TD, Hatfield JS, Nadolsky K, Bonsu O, Nath PV, Tuamokumo FO, Shakir MK. The Effects of Medium-Chain Triglyceride Oil and Butter on Lipid Profiles. Cureus. 2024 Jun 17;16(6):e62556. doi: 10.7759/cureus.62556[↩]
- Subih HS, Qudah RA, Janakat S, Rimawi H, Elsahoryi NA, Alyahya L. Medium-Chain Triglyceride Oil and Dietary Intervention Improved Body Composition and Metabolic Parameters in Children with Glycogen Storage Disease Type 1 in Jordan: A Clinical Trial. Foods. 2024 Apr 2;13(7):1091. doi: 10.3390/foods13071091[↩]
- Abe T. Timing of Medium-Chain Triglyceride Consumption Modulates Effects in Mice with Obesity Induced by a High-Fat High-Sucrose Diet. Nutrients. 2022 Dec 1;14(23):5096. doi: 10.3390/nu14235096[↩]
- Juby AG, Blackburn TE, Mager DR. Use of medium chain triglyceride (MCT) oil in subjects with Alzheimer’s disease: A randomized, double-blind, placebo-controlled, crossover study, with an open-label extension. Alzheimers Dement (N Y). 2022 Mar 14;8(1):e12259. doi: 10.1002/trc2.12259[↩][↩][↩][↩][↩][↩][↩][↩]
- Dutta K, Satishchandra P, Borkotokey M. Medium-chain Triglyceride Ketogenic Diet as a Treatment Strategy for Adult Super-refractory Status Epilepticus. Indian J Crit Care Med. 2022 Jan;26(1):139-140. doi: 10.5005/jp-journals-10071-24073[↩]
- Neudorf H, Jackson G, Little JP. Examining the Effect of Consuming C8 Medium-Chain Triglyceride Oil for 14 Days on Markers of NLRP3 Activation in Healthy Humans. J Nutr Metab. 2022 Apr 6;2022:7672759. doi: 10.1155/2022/7672759[↩]
- Lichtenstein AH, Appel LJ, Vadiveloo M, Hu FB, Kris-Etherton PM, Rebholz CM, Sacks FM, Thorndike AN, Van Horn L, Wylie-Rosett J. 2021 Dietary Guidance to Improve Cardiovascular Health: A Scientific Statement From the American Heart Association. Circulation. 2021 Dec 7;144(23):e472-e487. https://doi.org/10.1161/CIR.0000000000001031[↩]
- Vandenberghe C., St-Pierre V., Pierotti T., Fortier M., Castellano C.-A., Cunnane S. C. Tricaprylin alone increases plasma ketone response more than coconut oil or other medium-chain triglycerides: an acute crossover study in healthy adults. Current Developments in Nutrition . 2017;1(4) doi: 10.3945/cdn.116.000257.e000257[↩]
- Babayan V.K. Medium chain triglycerides and structured lipids. Lipids. 1987;22:417–420. doi: 10.1007/BF02537271[↩][↩]
- Bodkowski R., Czyż K., Kupczyński R., Patkowska-Sokoła B., Nowakowski P., Wiliczkiewicz A. Lipid complex effect on fatty acid profile and chemical composition of cow milk and cheese. J. Dairy Sci. 2016;99:57–67. doi: 10.3168/jds.2015-9321[↩][↩]
- Edem D.O. Palm oil: Biochemical, physiological, nutritional, hematological, and toxicological aspects: A review. Plant Foods Hum. Nutr. 2002;57:319–341. doi: 10.1023/A:1021828132707[↩][↩]
- Traul K.A., Driedger A., Ingle D.L., Nakhasi D. Review of the toxicologic properties of medium-chain triglycerides. Food Chem. Toxicol. 2000;38:79–98. doi: 10.1016/S0278-6915(99)00106-4[↩][↩]
- Marten B., Pfeuffer M., Schrezenmeir J. Medium-chain triglycerides. Int. Dairy J. 2006;16:1374–1382. doi: 10.1016/j.idairyj.2006.06.015[↩][↩]
- Bach A.C., Babayan V.K. Medium-chain triglycerides: An update. Am. J. Clin. Nutr. 1982;36:950–962. doi: 10.1093/ajcn/36.5.950[↩]
- St-Onge M-P, Bosarge A. Weight-loss diet that includes consumption of medium-chain triacylglycerol oil leads to a greater rate of weight and fat mass loss than does olive oil. The American journal of clinical nutrition. 2008;87(3):621-626. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2874190/[↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Ulrich H, Pastores SM, Katz DP, Kvetan V. Parenteral use of medium-chain triglycerides: a reappraisal. Nutrition. 1996 Apr;12(4):231-8. doi: 10.1016/s0899-9007(96)00089-6[↩]
- Joshi S, Kaushik V, Gode V, Mhaskar S. Coconut Oil and Immunity: What do we really know about it so far? J Assoc Physicians India. 2020 Jul;68(7):67-72.[↩]
- Fernando WM, Martins IJ, Goozee KG, Brennan CS, Jayasena V, Martins RN. The role of dietary coconut for the prevention and treatment of Alzheimer’s disease: potential mechanisms of action. Br J Nutr. 2015 Jul 14;114(1):1-14. doi: 10.1017/S0007114515001452[↩][↩][↩][↩][↩][↩][↩][↩]
- Takeuchi H, Sekine S, Kojima K, Aoyama T. The application of medium-chain fatty acids: edible oil with a suppressing effect on body fat accumulation. Asia Pac J Clin Nutr. 2008;17 Suppl 1:320-3. [↩]
- Dai X., Yuan T., Zhang X., Zhou Q., Bi H., Yu R., Wei W., Wang X. Short-chain fatty acid (SCFA) and medium-chain fatty acid (MCFA) concentrations in human milk consumed by infants born at different gestational ages and the variations in concentration during lactation stages. Food Funct. 2020;11:1869–1880. doi: 10.1039/C9FO02595B[↩]
- Andreas NJ, Kampmann B, Mehring Le-Doare K. Human breast milk: A review on its composition and bioactivity. Early Hum Dev. 2015 Nov;91(11):629-35. doi: 10.1016/j.earlhumdev.2015.08.013[↩]
- Traul KA, Driedger A, Ingle DL, Nakhasi D. Review of the toxicologic properties of medium-chain triglycerides. Food Chem Toxicol. 2000 Jan;38(1):79-98. doi: 10.1016/s0278-6915(99)00106-4[↩][↩]
- Bach AC, Babayan VK. Medium-chain triglycerides: an update. Am J Clin Nutr. 1982 Nov;36(5):950-62. doi: 10.1093/ajcn/36.5.950[↩][↩][↩][↩]
- Henderson ST, Vogel JL, Barr LJ, Garvin F, Jones JJ, Costantini LC. Study of the ketogenic agent AC-1202 in mild to moderate Alzheimer’s disease: a randomized, double-blind, placebo-controlled, multicenter trial. Nutr Metab (Lond). 2009 Aug 10;6:31. doi: 10.1186/1743-7075-6-31[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Maynard SD, Gelblum J. Retrospective cohort study of the efficacy of caprylic triglyceride in patients with mild-to-moderate alzheimer’s disease. Neuropsychiatr Dis Treat. 2013;9:1619-27. doi: 10.2147/NDT.S52331[↩]
- Ohnuma T, Toda A, Kimoto A, Takebayashi Y, Higashiyama R, Tagata Y, Ito M, Ota T, Shibata N, Arai H. Benefits of use, and tolerance of, medium-chain triglyceride medical food in the management of Japanese patients with Alzheimer’s disease: a prospective, open-label pilot study. Clin Interv Aging. 2016 Jan 8;11:29-36. doi: 10.2147/CIA.S95362[↩]
- Taylor MK, Sullivan DK, Mahnken JD, Burns JM, Swerdlow RH. Feasibility and efficacy data from a ketogenic diet intervention in Alzheimer’s disease. Alzheimers Dement (N Y). 2017 Dec 6;4:28-36. doi: 10.1016/j.trci.2017.11.002[↩][↩][↩][↩][↩][↩][↩][↩]
- Cunnane S. C., Trushina E., Morland C., Prigione A., Casadesus G., Andrews Z. B., et al. (2020). Brain energy rescue: An emerging therapeutic concept for neurodegenerative disorders of ageing. Nat. Rev. 19 609–633. 10.1038/s41573-020-0072-x[↩]
- Dunn E, Zhang B, Sahota VK, Augustin H. Potential benefits of medium chain fatty acids in aging and neurodegenerative disease. Front Aging Neurosci. 2023 Aug 23;15:1230467. doi: 10.3389/fnagi.2023.1230467[↩][↩][↩][↩][↩]
- Juby AG, Cunnane SC, Mager DR. Refueling the post COVID-19 brain: potential role of ketogenic medium chain triglyceride supplementation: an hypothesis. Front Nutr. 2023 Jun 21;10:1126534. doi: 10.3389/fnut.2023.1126534[↩]
- Regulation of intestinal cholesterol absorption. Wang DQ. Annu Rev Physiol. 2007; 69():221-48. https://www.ncbi.nlm.nih.gov/pubmed/17002594/[↩]
- Wang TY, Liu M, Portincasa P, Wang DQ-H. New insights into the molecular mechanism of intestinal fatty acid absorption. European journal of clinical investigation. 2013;43(11):1203-1223. doi:10.1111/eci.12161. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3996833[↩]
- U.S. Department of Health and Human Services. What Are the Types of Fat ? https://www.move.va.gov/docs/NewHandouts/Nutrition/N09_WhatAreTheTypesOfFat.pdf[↩]
- Uauy R, Aro A, Clarke R, L’Abbé MR, Mozaffarian D, Skeaff CM,, et al. WHO scientific update on trans fatty acids: summary and conclusions. Eur J Clin Nutr. 2009;63:S68–75. doi:10.1038/ejcn.2009.15[↩]
- American Heart Association. Monounsaturated Fat. https://healthyforgood.heart.org/Eat-smart/Articles/Monounsaturated-Fats[↩]
- American Heart Association. Polyunsaturated Fat. https://healthyforgood.heart.org/Eat-smart/Articles/Polyunsaturated-Fats[↩][↩]
- American Heart Association. Saturated Fat. https://healthyforgood.heart.org/Eat-smart/Articles/Saturated-Fats[↩][↩]
- U.S. Food and Drug Administration. Trans Fat. https://www.accessdata.fda.gov/scripts/interactivenutritionfactslabel/trans-fat.html[↩][↩]
- U.S. Food and Drug Administration. Trans Fat Now Listed With Saturated Fat and Cholesterol. https://www.fda.gov/food/ingredientspackaginglabeling/labelingnutrition/ucm274590.htm[↩]
- U.S. Food and Drug Administration. Final Determination Regarding Partially Hydrogenated Oils (Removing Trans Fat). https://www.fda.gov/food/ingredientspackaginglabeling/foodadditivesingredients/ucm449162.htm[↩]
- Lichtenstein AH, Appel LJ, Brands M, Carnethon M, Daniels S, Franch HA, Franklin B, Kris-Etherton P, Harris WS, Howard B, Karanja N, Lefevre M, Rudel L, Sacks F, Van Horn L, Winston M, Wylie-Rosett J. Diet and lifestyle recommendations revision 2006: a scientific statement from the American Heart Association Nutrition Committee. Circulation. 2006;114:82–96. http://circ.ahajournals.org/content/114/1/82.long[↩]
- Hu FB, Stampfer MJ, Manson JE, Rimm E, Colditz GA, Rosner BA, Hennekens CH, Willett WC. Dietary fat intake and the risk of coronary heart disease in women. N Engl J Med. 1997;337:1491–1499. https://www.nejm.org/doi/10.1056/NEJM199711203372102[↩]
- Dietary Fats and Cardiovascular Disease: A Presidential Advisory From the American Heart Association. Circulation June 15, 2017 http://circ.ahajournals.org/content/early/2017/06/15/CIR.0000000000000510[↩]
- U.S. Department of Agriculture ARS. Nutrient Intakes from Foods: Mean Amounts Consumed per Individual, One Day, 2003–2004. 2007.[↩]
- Bourque C, St-Onge MP, Papamandjaris AA, Cohn JS, Jones PJ. Consumption of an oil composed of medium chain triacyglycerols, phytosterols, and N-3 fatty acids improves cardiovascular risk profile in overweight women. Metabolism. 2003;52:771–777. https://www.ncbi.nlm.nih.gov/pubmed/12800105[↩][↩]
- St-Onge MP, Lamarche B, Mauger JF, Jones PJ. Consumption of a functional oil rich in phytosterols and medium-chain triglyceride oil improves plasma lipid profiles in men. J Nutr. 2003;133:1815–1820. https://www.ncbi.nlm.nih.gov/pubmed/12771322[↩][↩]
- Cater NB, Heller HJ, Denke MA. Comparison of the effects of medium-chain triacylglycerols, palm oil, and high oleic acid sunflower oil on plasma triacylglycerol fatty acids and lipid and lipoprotein concentrations in humans. Am J Clin Nutr. 1997;65:41–45. https://www.ncbi.nlm.nih.gov/pubmed/8988911[↩][↩][↩][↩][↩]
- Swift LL, Hill JO, Peters JC, Greene HL. Plasma lipids and lipoproteins during 6 d of maintenance feeding with long-chain, medium-chain, and mixed-chain triglycerides. Am J Clin Nutr. 1992;56:881–886. https://www.ncbi.nlm.nih.gov/pubmed/1415007[↩][↩][↩][↩][↩][↩]
- Hill JO, Peters JC, Swift LL, Yang D, Sharp T, Abumrad N, Greene HL. Changes in blood lipids during six days of overfeeding with medium or long chain triglycerides. J Lipid Res. 1990;31:407–416. http://www.jlr.org/content/31/3/407.long[↩][↩][↩][↩][↩][↩][↩]
- Jones PJ, Raeini-Sarjaz M, Ntanios FY, Vanstone CA, Feng JY, Parsons WE. Modulation of plasma lipid levels and cholesterol kinetics by phytosterol versus phytostanol esters. J Lipid Res. 2000;41:697–705. http://www.jlr.org/content/41/5/697.long[↩]
- St-Onge MP, Jones PJ. Phytosterols and human lipid metabolism: efficacy, safety, and novel foods. Lipids. 2003;38:367–375. https://www.ncbi.nlm.nih.gov/pubmed/12848281[↩]
- Hu FB, Stampfer MJ, Manson JE, Ascherio A, Colditz GA, Speizer FE, Hennekens CH, Willett WC. Dietary saturated fats and their food sources in relation to the risk of coronary heart disease in women. Am J Clin Nutr. 1999;70:1001–1008. https://www.ncbi.nlm.nih.gov/pubmed/10584044[↩]
- St-Onge MP. Dietary fats, teas, dairy, and nuts: potential functional foods for weight control? Am J Clin Nutr. 2005;81:7–15. St-Onge MP. Dietary fats, teas, dairy, and nuts: potential functional foods for weight control? Am J Clin Nutr. 2005;81:7–15. https://www.ncbi.nlm.nih.gov/pubmed/15640454[↩]
- Chatterjee P, Fernando M, Fernando B, Dias CB, Shah T, Silva R, Williams S, Pedrini S, Hillebrandt H, Goozee K, Barin E, Sohrabi HR, Garg M, Cunnane S, Martins RN. Potential of coconut oil and medium chain triglycerides in the prevention and treatment of Alzheimer’s disease. Mech Ageing Dev. 2020 Mar;186:111209. doi: 10.1016/j.mad.2020.111209[↩]
- Fukao T, Lopaschuk GD, Mitchell GA. Pathways and control of ketone body metabolism: on the fringe of lipid biochemistry. Prostaglandins Leukot Essent Fatty Acids. 2004 Mar;70(3):243-51. doi: 10.1016/j.plefa.2003.11.001[↩]
- DeLany JP, Windhauser MM, Champagne CM, Bray GA. Differential oxidation of individual dietary fatty acids in humans. Am J Clin Nutr. 2000 Oct;72(4):905-11. doi: 10.1093/ajcn/72.4.905[↩]
- Castro CB, Dias CB, Hillebrandt H, Sohrabi HR, Chatterjee P, Shah TM, Fuller SJ, Garg ML, Martins RN. Medium-chain fatty acids for the prevention or treatment of Alzheimer’s disease: a systematic review and meta-analysis. Nutr Rev. 2023 Aug 10;81(9):1144-1162. doi: 10.1093/nutrit/nuac104[↩][↩][↩]
- Babayan VK. Medium-chain triglycerides-their composition, preparation, and application. J Am Oil Chem Soc. 1968;45:23–25. doi: 10.1007/BF02679040[↩]
- Schonfeld P, Wojtczak L. Short- and medium-chain fatty acids in energy metabolism: the cellular perspective. J Lipid Res. (2016) 57:943–54. 10.1194/jlr.R067629[↩][↩]
- Cunnane SC, Courchesne-Loyer A, St-Pierre V, Vandenberghe C, Pierotti T, Fortier M, et al. Can ketones compensate for deteriorating brain glucose uptake during aging? implications for the risk and treatment of Alzheimer’s disease. Ann N Y Acad Sci. (2016) 1367:12–20. 10.1111/nyas.12999[↩][↩][↩][↩][↩][↩]
- Seaton TB, Welle SL, Warenko MK, Campbell RG. Thermic effect of medium-chain and long-chain triglycerides in man. Am J Clin Nutr. (1986) 44:630–4. 10.1093/ajcn/44.5.630[↩][↩]
- Papamandjaris AA, MacDougall DE, Jones PJ. Medium chain fatty acid metabolism and energy expenditure: obesity treatment implications. Life Sci. (1998) 62:1203–15. 10.1016/S0024-3205(97)01143-0[↩][↩]
- Lei E, Vacy K, Boon WC. Fatty acids and their therapeutic potential in neurological disorders. Neurochem Int. (2016) 95:75–84. doi: 10.1016/j.neuint.2016.02.014[↩][↩]
- Juby AG, Brocks DR, Jay DA, Davis CMJ, Mager DR. Assessing the impact of factors that influence the ketogenic response to varying doses of medium chain triglyceride (MCT) oil. J Prev Alz Dis. (2021) 1:19–28. doi: 10.14283/jpad.2020.53[↩][↩][↩]
- Vandenberghe C, St-Pierre V, Pierotti T, Fortier M, Castellano CA, Cunnane SC. Tricaprylin alone increases plasma ketone response more than coconut oil or other medium-chain triglycerides: an acute crossover study in healthy adults. Curr Dev Nutr. (2017) 1:e000257. 10.3945/cdn.116.000257[↩][↩][↩]
- St-Pierre V, Vandenberghe C, Lowry CM, Fortier M, Castellano CA, Wagner R, Cunnane SC. Plasma Ketone and Medium Chain Fatty Acid Response in Humans Consuming Different Medium Chain Triglycerides During a Metabolic Study Day. Front Nutr. 2019 Apr 16;6:46. doi: 10.3389/fnut.2019.00046[↩][↩][↩]
- Li K, Wang WH, Wu JB, Xiao WH. β-hydroxybutyrate: A crucial therapeutic target for diverse liver diseases. Biomed Pharmacother. 2023 Sep;165:115191. https://doi.org/10.1016/j.biopha.2023.115191[↩][↩][↩]
- Bach A., Schirardin H., Weryha A., Bauer M. Ketogenic response to medium-chain triglyceride load in the rat. Journal of Nutrition. 1977;107(10):1863–1870. doi: 10.1093/jn/107.10.1863[↩]
- Yeh Y. Y., Zee P. Relation of ketosis to metabolic changes induced by acute medium-chain triglyceride feeding in rats. Journal of Nutrition. 1976;106(1):58–67. doi: 10.1093/jn/106.1.58[↩]
- St-Onge MP, Ross R, Parsons WD, Jones PJ. Medium-chain triglycerides increase energy expenditure and decrease adiposity in overweight men. Obes Res. 2003 Mar;11(3):395-402. doi: 10.1038/oby.2003.53[↩][↩][↩]
- D C Harvey CJ, Schofield GM, Williden M, McQuillan JA. The Effect of Medium Chain Triglycerides on Time to Nutritional Ketosis and Symptoms of Keto-Induction in Healthy Adults: A Randomised Controlled Clinical Trial. J Nutr Metab. 2018 May 22;2018:2630565. doi: 10.1155/2018/2630565[↩]
- Stubbs BJ, Cox PJ, Evans RD, Cyranka M, Clarke K, de Wet H. A Ketone Ester Drink Lowers Human Ghrelin and Appetite. Obesity (Silver Spring). 2018 Feb;26(2):269-273. doi: 10.1002/oby.22051[↩]
- Lei E, Vacy K, Boon WC. Fatty acids and their therapeutic potential in neurological disorders. Neurochem Int. 2016 May;95:75-84. doi: 10.1016/j.neuint.2016.02.014[↩][↩][↩][↩][↩][↩][↩]
- Newport MT, VanItallie TB, Kashiwaya Y, King MT, Veech RL. A new way to produce hyperketonemia: use of ketone ester in a case of Alzheimer’s disease. Alzheimers Dement. 2015 Jan;11(1):99-103. doi: 10.1016/j.jalz.2014.01.006[↩][↩][↩][↩][↩][↩][↩]
- Rebello CJ, Keller JN, Liu AG, Johnson WD, Greenway FL. Pilot feasibility and safety study examining the effect of medium chain triglyceride supplementation in subjects with mild cognitive impairment: A randomized controlled trial. BBA Clin. 2015 Jan 16;3:123-5. doi: 10.1016/j.bbacli.2015.01.001[↩][↩][↩][↩][↩][↩][↩]
- Reger MA, Henderson ST, Hale C, Cholerton B, Baker LD, Watson GS, Hyde K, Chapman D, Craft S. Effects of beta-hydroxybutyrate on cognition in memory-impaired adults. Neurobiol Aging. 2004 Mar;25(3):311-4. doi: 10.1016/S0197-4580(03)00087-3[↩][↩][↩][↩][↩][↩][↩][↩]
- Owen OE, Morgan AP, Kemp HG, Sullivan JM, Herrera MG, Cahill GF Jr. Brain metabolism during fasting. J Clin Invest. 1967 Oct;46(10):1589-95. https://pmc.ncbi.nlm.nih.gov/articles/instance/292907/pdf/jcinvest00272-0077.pdf[↩][↩][↩]
- Drenick EJ, Alvarez LC, Tamasi GC, Brickman AS. Resistance to symptomatic insulin reactions after fasting. J Clin Invest. 1972 Oct;51(10):2757-62. https://pmc.ncbi.nlm.nih.gov/articles/instance/332976/pdf/jcinvest00637-0253.pdf[↩][↩][↩]
- Hasselbalch SG, Madsen PL, Hageman LP, Olsen KS, Justesen N, Holm S, Paulson OB. Changes in cerebral blood flow and carbohydrate metabolism during acute hyperketonemia. Am J Physiol. 1996 May;270(5 Pt 1):E746-51. doi: 10.1152/ajpendo.1996.270.5.E746[↩][↩][↩]
- Courchesne-Loyer A, Croteau E, Castellano CA, St-Pierre V, Hennebelle M, Cunnane SC. Inverse relationship between brain glucose and ketone metabolism in adults during short-term moderate dietary ketosis: A dual tracer quantitative positron emission tomography study. J Cereb Blood Flow Metab. 2017 Jul;37(7):2485-2493. doi: 10.1177/0271678X16669366[↩][↩][↩]
- Croteau E, Castellano CA, Richard MA, Fortier M, Nugent S, Lepage M, Duchesne S, Whittingstall K, Turcotte ÉE, Bocti C, Fülöp T, Cunnane SC. Ketogenic Medium Chain Triglycerides Increase Brain Energy Metabolism in Alzheimer’s Disease. J Alzheimers Dis. 2018;64(2):551-561. doi: 10.3233/JAD-180202[↩]
- Gandotra S, Kour J, Van der Waag A (2014) Efficacy of adjunctive extra virgin coconut oil use in moderate to severe Alzheimer’s disease. Int J Sch Cog Psychol 1, 2.[↩]
- De la Rubia Ortí JE, Sánchez Álvarez C, Selvi Sabater P, Bueno Cayo AM, Sancho Castillo S, Rochina MJ, Hu Yang I. Influencia del aceite de coco en enfermos de alzhéimer a nivel cognitivo [How does coconut oil affect cognitive performance in alzheimer patients?]. Nutr Hosp. 2017 Mar 30;34(2):352-356. Spanish. doi: 10.20960/nh.780[↩][↩][↩]
- Hu Yang I, De la Rubia Ortí JE, Selvi Sabater P, Sancho Castillo S, Rochina MJ, Manresa Ramón N, Montoya-Castilla I. ACEITE DE COCO: TRATAMIENTO ALTERNATIVO NO FARMACOLÓGICO FRENTE A LA ENFERMEDAD DE ALZHEIMER [COCONUT OIL: NON-ALTERNATIVE DRUG TREATMENT AGAINST ALZHEIMER´S DISEASE]. Nutr Hosp. 2015 Dec 1;32(6):2822-7. Spanish. doi: 10.3305/nh.2015.32.6.9707[↩]
- Xu Q, Zhang Y, Zhang X, Liu L, Zhou B, Mo R, Li Y, Li H, Li F, Tao Y, Liu Y, Xue C. Medium-chain triglycerides improved cognition and lipid metabolomics in mild to moderate Alzheimer’s disease patients with APOE4-/-: A double-blind, randomized, placebo-controlled crossover trial. Clin Nutr. 2020 Jul;39(7):2092-2105. doi: 10.1016/j.clnu.2019.10.017[↩][↩][↩][↩][↩][↩][↩]
- Fortier M, Castellano CA, St-Pierre V, Myette-Côté É, Langlois F, Roy M, Morin MC, Bocti C, Fulop T, Godin JP, Delannoy C, Cuenoud B, Cunnane SC. A ketogenic drink improves cognition in mild cognitive impairment: Results of a 6-month RCT. Alzheimers Dement. 2021 Mar;17(3):543-552. doi: 10.1002/alz.12206[↩][↩][↩][↩]
- Ota M, Matsuo J, Ishida I, Takano H, Yokoi Y, Hori H, Yoshida S, Ashida K, Nakamura K, Takahashi T, Kunugi H. Effects of a medium-chain triglyceride-based ketogenic formula on cognitive function in patients with mild-to-moderate Alzheimer’s disease. Neurosci Lett. 2019 Jan 18;690:232-236. doi: 10.1016/j.neulet.2018.10.048[↩][↩][↩]
- Augustin K, Khabbush A, Williams S, Eaton S, Orford M, Cross JH, Heales SJR, Walker MC, Williams RSB. Mechanisms of action for the medium-chain triglyceride ketogenic diet in neurological and metabolic disorders. Lancet Neurol. 2018 Jan;17(1):84-93. doi: 10.1016/S1474-4422(17)30408-8[↩][↩]
- Henderson ST, Morimoto BH, Cummings JL, Farlow MR, Walker J. A Placebo-Controlled, Parallel-Group, Randomized Clinical Trial of AC-1204 in Mild-to-Moderate Alzheimer’s Disease. J Alzheimers Dis. 2020;75(2):547-557. doi: 10.3233/JAD-191302[↩][↩][↩]
- Sun L, Ye KX, Wong HLK, Wang L, Lim SL, Chao YX, Zhang C, Yap KZ, Feng L. The Effects of Medium Chain Triglyceride for Alzheimer’s Disease Related Cognitive Impairment: A Systematic Review and Meta-Analysis. J Alzheimers Dis. 2023;94(2):441-456. doi: 10.3233/JAD-230406[↩][↩][↩][↩][↩][↩][↩][↩]
- Avgerinos KI, Egan JM, Mattson MP, Kapogiannis D. Medium Chain Triglycerides induce mild ketosis and may improve cognition in Alzheimer’s disease. A systematic review and meta-analysis of human studies. Ageing Res Rev. 2020 Mar;58:101001. doi: 10.1016/j.arr.2019.101001[↩][↩][↩][↩]
- Giannos P, Prokopidis K, Lidoriki I, Triantafyllidis KK, Kechagias KS, Celoch K, Candow DG, Ostojic SM, Forbes SC. Medium-chain triglycerides may improve memory in non-demented older adults: a systematic review of randomized controlled trials. BMC Geriatr. 2022 Oct 23;22(1):817. doi: 10.1186/s12877-022-03521-6[↩][↩]
- Page KA, Williamson A, Yu N, McNay EC, Dzuira J, McCrimmon RJ, Sherwin RS. Medium-chain fatty acids improve cognitive function in intensively treated type 1 diabetic patients and support in vitro synaptic transmission during acute hypoglycemia. Diabetes. 2009 May;58(5):1237-44. doi: 10.2337/db08-1557[↩][↩]
- Mensink RP, Katan MB. Effect of dietary fatty acids on serum lipids and lipoproteins. A meta-analysis of 27 trials. Arterioscler Thromb. 1992 Aug;12(8):911-9. doi: 10.1161/01.atv.12.8.911[↩][↩]
- Pan Y, Larson B, Araujo JA, Lau W, de Rivera C, Santana R, Gore A, Milgram NW. Dietary supplementation with medium-chain TAG has long-lasting cognition-enhancing effects in aged dogs. Br J Nutr. 2010 Jun;103(12):1746-54. doi: 10.1017/S0007114510000097[↩][↩]
- Kashiwaya Y, Bergman C, Lee JH, Wan R, King MT, Mughal MR, Okun E, Clarke K, Mattson MP, Veech RL. A ketone ester diet exhibits anxiolytic and cognition-sparing properties, and lessens amyloid and tau pathologies in a mouse model of Alzheimer’s disease. Neurobiol Aging. 2013 Jun;34(6):1530-9. doi: 10.1016/j.neurobiolaging.2012.11.023[↩][↩][↩][↩]
- Yin JX, Maalouf M, Han P, Zhao M, Gao M, Dharshaun T, Ryan C, Whitelegge J, Wu J, Eisenberg D, Reiman EM, Schweizer FE, Shi J. Ketones block amyloid entry and improve cognition in an Alzheimer’s model. Neurobiol Aging. 2016 Mar;39:25-37. doi: 10.1016/j.neurobiolaging.2015.11.018[↩][↩]
- Schönfeld P, Wojtczak L. Short- and medium-chain fatty acids in energy metabolism: the cellular perspective. J Lipid Res. 2016 Jun;57(6):943-54. doi: 10.1194/jlr.R067629[↩]
- Vandenberghe C, St-Pierre V, Pierotti T, Fortier M, Castellano CA, Cunnane SC. Tricaprylin Alone Increases Plasma Ketone Response More Than Coconut Oil or Other Medium-Chain Triglycerides: An Acute Crossover Study in Healthy Adults. Curr Dev Nutr. 2017 Mar 22;1(4):e000257. doi: 10.3945/cdn.116.000257[↩][↩][↩]
- Khabbush A, Orford M, Tsai YC, Rutherford T, O’Donnell M, Eaton S, Heales SJR. Neuronal decanoic acid oxidation is markedly lower than that of octanoic acid: A mechanistic insight into the medium-chain triglyceride ketogenic diet. Epilepsia. 2017 Aug;58(8):1423-1429. doi: 10.1111/epi.13833[↩]
- Thevenet J, De Marchi U, Domingo JS, Christinat N, Bultot L, Lefebvre G, Sakamoto K, Descombes P, Masoodi M, Wiederkehr A. Medium-chain fatty acids inhibit mitochondrial metabolism in astrocytes promoting astrocyte-neuron lactate and ketone body shuttle systems. FASEB J. 2016 May;30(5):1913-26. doi: 10.1096/fj.201500182[↩]
- Fortier M, Castellano CA, Croteau E, Langlois F, Bocti C, St-Pierre V, Vandenberghe C, Bernier M, Roy M, Descoteaux M, Whittingstall K, Lepage M, Turcotte ÉE, Fulop T, Cunnane SC. A ketogenic drink improves brain energy and some measures of cognition in mild cognitive impairment. Alzheimers Dement. 2019 May;15(5):625-634. doi: 10.1016/j.jalz.2018.12.017[↩]
- Courchesne-Loyer A, Lowry CM, St-Pierre V, Vandenberghe C, Fortier M, Castellano CA, Wagner JR, Cunnane SC. Emulsification Increases the Acute Ketogenic Effect and Bioavailability of Medium-Chain Triglycerides in Humans: Protein, Carbohydrate, and Fat Metabolism. Curr Dev Nutr. 2017 Jun 21;1(7):e000851. doi: 10.3945/cdn.117.000851[↩][↩]
- Vandenberghe C, St-Pierre V, Fortier M, Castellano CA, Cuenoud B, Cunnane SC. Medium Chain Triglycerides Modulate the Ketogenic Effect of a Metabolic Switch. Front Nutr. 2020 Jan 31;7:3. doi: 10.3389/fnut.2020.00003[↩]
- Hill JO, Peters JC, Yang D, Sharp T, Kaler M, Abumrad NN, Greene HL. Thermogenesis in humans during overfeeding with medium-chain triglycerides. Metabolism. 1989;38:641–648. http://www.jlr.org/content/31/3/407.long[↩]
- Dulloo AG, Fathi M, Mensi N, Girardier L. Twenty-four-hour energy expenditure and urinary catecholamines of humans consuming low-to-moderate amounts of medium-chain triglycerides: a dose-response study in a human respiratory chamber. Eur J Clin Nutr. 1996;50:152–8. https://www.ncbi.nlm.nih.gov/pubmed/8654328[↩][↩][↩]
- Scalfi L, Coltorti A, Contaldo F. Postprandial thermogenesis in lean and obese subjects after meals supplemented with medium-chain and long-chain triglycerides. Am J Clin Nutr. 1991;53:1130–3. https://www.ncbi.nlm.nih.gov/pubmed/2021124[↩][↩]
- White MD, Papamandjaris AA, Jones PJ. Enhanced postprandial energy expenditure with medium-chain fatty acid feeding is attenuated after 14 d in premenopausal women. Am J Clin Nutr. 1999;69:883–9. https://www.ncbi.nlm.nih.gov/pubmed/10232626[↩][↩]
- Seaton TB, Welle SL, Warenko MK, Campbell RG. Thermic effect of medium-chain and long-chain triglycerides in man. Am J Clin Nutr. 1986;44:630–4. https://www.ncbi.nlm.nih.gov/pubmed/3532757[↩][↩]
- Pervaiz MA, Kendal F, Hegde M, Singh RH. MCT oil-based diet reverses hypertrophic cardiomyopathy in a patient with very long chain acyl-coA dehydrogenase deficiency. Indian Journal of Human Genetics. 2011;17(1):29-32. doi:10.4103/0971-6866.82190. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3144685[↩][↩]
- Reversal of severe hypertrophic cardiomyopathy and excellent neuropsychologic outcome in very-long-chain acyl-coenzyme A dehydrogenase deficiency. Cox GF, Souri M, Aoyama T, Rockenmacher S, Varvogli L, Rohr F, Hashimoto T, Korson MS. J Pediatr. 1998 Aug; 133(2):247-53. https://www.ncbi.nlm.nih.gov/pubmed/9709714/[↩]
- Maki KC, Dicklin MR, Kirkpatrick CF. Saturated fats and cardiovascular health: Current evidence and controversies. J Clin Lipidol. 2021 Nov-Dec;15(6):765-772. doi: 10.1016/j.jacl.2021.09.049[↩]
- McKenzie KM, Lee CM, Mijatovic J, Haghighi MM, Skilton MR. Medium-Chain Triglyceride Oil and Blood Lipids: A Systematic Review and Meta-Analysis of Randomized Trials. J Nutr. 2021 Oct 1;151(10):2949-2956. https://doi.org/10.1093/jn/nxab220[↩]
- St-Onge M-P, Bosarge A, Goree LLT, Darnell B. Medium Chain Triglyceride Oil Consumption as Part of a Weight Loss Diet Does Not Lead to an Adverse Metabolic Profile When Compared to Olive Oil. Journal of the American College of Nutrition. 2008;27(5):547-552. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2874191/[↩][↩][↩][↩][↩][↩][↩][↩]
- Bourque C, St-Onge MP, Papamandjaris AA, Cohn JS, Jones PJ. Consumption of an oil composed of medium chain triacyglycerols, phytosterols, and N-3 fatty acids improves cardiovascular risk profile in overweight women. Metabolism. 2003;52:771–777.[↩]
- St-Onge MP, Lamarche B, Mauger JF, Jones PJ. Consumption of a functional oil rich in phytosterols and medium-chain triglyceride oil improves plasma lipid profiles in men. J Nutr. 2003;133:1815–1820.[↩]
- Fortier M, Castellano CA, St-Pierre V, Myette-Côté É, Langlois F, Roy M, Morin MC, Bocti C, Fulop T, Godin JP, Delannoy C, Cuenoud B, Cunnane SC. A ketogenic drink improves cognition in mild cognitive impairment: Results of a 6-month RCT. Alzheimers Dement. 2021 Mar;17(3):543-552. doi: 10.1002/alz.1220[↩]
- Courchesne-Loyer A, Fortier M, Tremblay-Mercier J, Chouinard-Watkins R, Roy M, Nugent S, Castellano CA, Cunnane SC. Stimulation of mild, sustained ketonemia by medium-chain triacylglycerols in healthy humans: estimated potential contribution to brain energy metabolism. Nutrition. 2013 Apr;29(4):635-40. doi: 10.1016/j.nut.2012.09.009[↩]
- Panth N, Abbott KA, Dias CB, Wynne K, Garg ML. Differential effects of medium- and long-chain saturated fatty acids on blood lipid profile: a systematic review and meta-analysis. Am J Clin Nutr. 2018 Oct 1;108(4):675-687. doi: 10.1093/ajcn/nqy167. Erratum in: Am J Clin Nutr. 2018 Dec 1;108(6):1356. doi: 10.1093/ajcn/nqy319[↩]
- Asakura L, Lottenberg AM, Neves MQ, Nunes VS, Rocha JC, Passarelli M, Nakandakare ER, Quintao EC. Dietary medium-chain triacylglycerol prevents the postprandial rise of plasma tri-acylglycerols but induces hypercholesterolemia in primary hyper-triglyceridemic subjects. Am J Clin Nutr. 2000;71:701–705. https://www.ncbi.nlm.nih.gov/pubmed/10702162[↩]
- Pedersen A, Baumstark MW, Marckmann P, Gylling H, Sandstrom B. An olive oil-rich diet results in higher concentrations of LDL cholesterol and a higher number of LDL subfraction particles than rapeseed oil and sunflower oil diets. J Lipid Res. 2000;41:1901–1911. http://www.jlr.org/content/41/12/1901.long[↩][↩]
- Vanstone CA, Raeini-Sarjaz M, Parsons WE, Jones PJ. Unesterified plant sterols and stanols lower LDL-cholesterol concentrations equivalently in hypercholesterolemic persons. Am J Clin Nutr. 2002;76:1272–1278. https://www.ncbi.nlm.nih.gov/pubmed/12450893[↩]
- Nosaka N, Maki H, Suzuki Y, Haruna H, Ohara A, Kasai M, Tsuji H, Aoyama T, Okazaki M, Igarashi O, Kondo K. Effects of margarine containing medium-chain triacylglycerols on body fat reduction in humans. J Atheroscler Thromb. 2003;10:290–298. https://www.jstage.jst.go.jp/article/jat/10/5/10_5_290/_pdf/-char/en[↩]
- Yost TJ, Erskine JM, Gregg TS, Podlecki DL, Brass EP, Eckel RH. Dietary substitution of medium chain triglycerides in subjects with non-insulin-dependent diabetes mellitus in an ambulatory setting: impact on glycemic control and insulin-mediated glucose metabolism. J Am Coll Nutr. 1994;13:615–622. https://www.ncbi.nlm.nih.gov/pubmed/7706596[↩]
- Kris-Etherton PM, Derr J, Mitchell DC, Mustad VA, Russell ME, McDonnell ET, Salabsky D, Pearson TA. The role of fatty acid saturation on plasma lipids, lipoproteins, and apolipoproteins: I. Effects of whole food diets high in cocoa butter, olive oil, soybean oil, dairy butter, and milk chocolate on the plasma lipids of young men. Metabolism. 1993;42:121–129. https://www.ncbi.nlm.nih.gov/pubmed/8446039[↩]
- Kris-Etherton PM, Pearson TA, Wan Y, Hargrove RL, Moriarty K, Fishell V, Etherton TD. High-monounsaturated fatty acid diets lower both plasma cholesterol and triacylglycerol concentrations. Am J Clin Nutr. 1999;70:1009–1015. https://www.ncbi.nlm.nih.gov/pubmed/10584045[↩][↩]
- Binkoski AE, Kris-Etherton PM, Wilson TA, Mountain ML, Ni-colosi RJ. Balance of unsaturated fatty acids is important to a cholesterol-lowering diet: comparison of mid-oleic sunflower oil and olive oil on cardiovascular disease risk factors. J Am Diet Assoc. 2005;105:1080–1086. https://www.ncbi.nlm.nih.gov/pubmed/15983524[↩]
- Croteau E, Castellano CA, Richard MA, Fortier M, Nugent S, Lepage M, et al. Ketogenic medium chain triglycerides increase brain energy metabolism in Alzheimer’s disease. J Alzheimers Dis. 2018;64:551–61. doi: 10.3233/JAD-180202[↩]
- Lambrechts DA, de Kinderen RJ, Vles HS, de Louw AJ, Aldenkamp AP, Majoie MJ. The MCT-ketogenic diet as a treatment option in refractory childhood epilepsy: a prospective study with 2-year follow-up. Epilepsy Behav. 2015;51:261–6. doi: 10.1016/j.yebeh.2015.07.023[↩]
- MacDonald A, Webster R, Whitlock M, Gerrard A, Daly A, Preece MA, et al. The safety of Lipistart, a medium-chain triglyceride based formula, in the dietary treatment of long-chain fatty acid disorders: a phase I study. J Pediatr Endocrinol Metab. 2018;31:297–304. doi: 10.1515/jpem-2017-0426[↩][↩]
- Neal EG, Chaffe H, Schwartz RH, Lawson MS, Edwards N, Fitzsimmons G, et al. A randomized trial of classical and medium-chain triglyceride ketogenic diets in the treatment of childhood epilepsy. Epilepsia. 2009;50:1109–17. doi: 10.1111/j.1528-1167.2008.01870.x[↩]
- Xu Q, Zhang Y, Zhang X, Liu L, Zhou B, Mo R, et al. Medium-chain triglycerides improved cognition and lipid metabolomics in mild to moderate Alzheimer’s disease patients with APOE4-/-: a double-blind, randomized, placebo-controlled crossover trial. Clin Nutr. 2020;39:2092–105. doi: 10.1016/j.clnu.2019.10.017[↩]
- McKenzie KM, Lee CM, Mijatovic J, Haghighi MM, Skilton MR. Medium-chain triglyceride oil and blood lipids: a systematic review and meta-analysis of randomized trials. J Nutr. 2021;151:2949–56. doi: 10.1093/jn/nxab220[↩]
- Maher T, El-Chab A, Shafat A, Clegg ME. Effect of mediumchain TAG and exercise on satiety, energy intake and energy balance. Br J Nutr. 2019;122:1313–20. doi: 10.1017/S0007114519002186[↩]
- Thomas DD, Stockman MC, Yu L, Meshulam T, McCarthy AC, Ionson A, et al. Effects of medium chain triglycerides supplementation on insulin sensitivity and beta cell function: a feasibility study. PLoS One. 2019;14:e0226200. doi: 10.1371/journal.pone.0226200[↩]
- Angus DJ, Hargreaves M, Dancey J, Febbraio MA. Effect of carbohydrate or carbohydrate plus medium-chain triglyceride ingestion on cycling time trial performance. J Appl Physiol (1985) 2000;88:113–9. doi: 10.1152/jappl.2000.88.1.113[↩]
- Jeukendrup AE, Saris WH, Brouns F, Halliday D, Wagenmakers JM. Effects of carbohydrate (CHO) and fat supplementation on CHO metabolism during prolonged exercise. Metabolism. 1996;45:915–21. doi: 10.1016/S0026-0495(96)90169-9[↩]
- Jeukendrup AE, Saris WH, Van Diesen R, Brouns F, Wagenmakers AJ. Effect of endogenous carbohydrate availability on oral medium-chain triglyceride oxidation during prolonged exercise. J Appl Physiol (1985) 1996;80:949–54. doi: 10.1152/jappl.1996.80.3.949[↩]
- Jeukendrup AE, Thielen JJ, Wagenmakers AJ, Brouns F, Saris WH. Effect of medium-chain triacylglycerol and carbohydrate ingestion during exercise on substrate utilization and subsequent cycling performance. Am J Clin Nutr. 1998;67:397–404. doi: 10.1093/ajcn/67.3.397[↩]
- Massicotte D, Péronnet F, Brisson GR, Hillaire-Marcel C. Oxidation of exogenous medium-chain free fatty acids during prolonged exercise: comparison with glucose. J Appl Physiol (1985) 1996;73:1334–9. doi: 10.1152/jappl.1992.73.4.1334[↩]
- Nosaka N, Tsujino S, Honda K, Suemitsu H, Kato K. Enhancement of fat oxidation during submaximal exercise in sedentary persons: variations by medium-chain fatty acid composition and age group. Lipids. 2020;55:173–83. doi: 10.1002/lipd.12222[↩]
- Van Zyl CG, Lambert EV, Hawley JA, Noakes TD, Dennis SC. Effects of medium-chain triglyceride ingestion on fuel metabolism and cycling performance. J Appl Physiol (1985) 1996;80:2217–25. doi: 10.1152/jappl.1996.80.6.2217[↩]
- Chapman-Lopez TJ, Koh Y. The Effects of Medium-Chain Triglyceride Oil Supplementation on Endurance Performance and Substrate Utilization in Healthy Populations: A Systematic Review. J Obes Metab Syndr. 2022 Sep 30;31(3):217-229. doi: 10.7570/jomes22028[↩]
- Kinsella R, Maher T, Clegg ME. Coconut oil has less satiating properties than medium chain triglyceride oil. Physiol Behav. 2017 Oct 1;179:422-426. doi: 10.1016/j.physbeh.2017.07.007[↩]
- Zhang Y, Xu Q, Liu YH, et al. Medium-chain triglyceride activated brown adipose tissue and induced reduction of fat mass in C57BL/6J mice fed high-fat diet. Biomed Environ Sci. 2015;28:97–104. doi: 10.3967/bes2015.012[↩]
- Hollis F, Mitchell ES, Canto C, et al. Medium chain triglyceride diet reduces anxiety-like behaviors and enhances social competitiveness in rats. Neuropharmacology. 2018;138:245–256. doi: 10.1016/j.neuropharm.2018.06.017[↩]
- Ashton JS, Roberts JW, Wakefield CJ, et al. The effects of medium chain triglyceride (MCT) supplementation using a C8:C10 ratio of 30:70 on cognitive performance in healthy young adults. Physiol Behav. 2021;229:113252. doi: 10.1016/j.physbeh.2020.113252[↩]
- Roy M, Edde M, Fortier M, Croteau E, Castellano CA, St-Pierre V, Vandenberghe C, Rheault F, Dadar M, Duchesne S, Bocti C, Fulop T, Cunnane SC, Descoteaux M. A ketogenic intervention improves dorsal attention network functional and structural connectivity in mild cognitive impairment. Neurobiol Aging. 2022 Jul;115:77-87. doi: 10.1016/j.neurobiolaging.2022.04.005[↩]
- Reger MA, Henderson ST, Hale C, et al. Effects of β-hydroxybutyrate on cognition in memory-impaired adults. Neurobiol Aging. 2004;25:311–314. doi: 10.1016/S0197-4580(03)00087-3[↩]
- Yen HC, Lai WK, Lin CS, Chiang SH. Medium-chain triglyceride as an alternative of in-feed colistin sulfate to improve growth performance and intestinal microbial environment in newly weaned pigs. Anim Sci J. 2015;86:99–104. doi: 10.1111/asj.12248[↩]
- Knottnerus SJG, Bleeker JC, Wüst RCI, Ferdinandusse S, IJlst L, Wijburg FA, Wanders RJA, Visser G, Houtkooper RH. Disorders of mitochondrial long-chain fatty acid oxidation and the carnitine shuttle. Rev Endocr Metab Disord. 2018 Mar;19(1):93-106. doi: 10.1007/s11154-018-9448-1[↩]
- Merritt JL 2nd, Norris M, Kanungo S. Fatty acid oxidation disorders. Ann Transl Med. 2018 Dec;6(24):473. doi: 10.21037/atm.2018.10.57[↩]
- Spiekerkoetter U, Lindner M, Santer R, Grotzke M, Baumgartner MR, Boehles H, Das A, Haase C, Hennermann JB, Karall D, de Klerk H, Knerr I, Koch HG, Plecko B, Röschinger W, Schwab KO, Scheible D, Wijburg FA, Zschocke J, Mayatepek E, Wendel U. Treatment recommendations in long-chain fatty acid oxidation defects: consensus from a workshop. J Inherit Metab Dis. 2009 Aug;32(4):498-505. doi: 10.1007/s10545-009-1126-8[↩]
- Vockley J. Long-chain fatty acid oxidation disorders and current management strategies. Am J Manag Care. 2020 Aug;26(7 Suppl):S147-S154. doi: 10.37765/ajmc.2020.88480[↩]
- Murphy JL, Badaloo AV, Chambers B, Forrester TE, Wootton SA, Jackson AA. Maldigestion and malabsorption of dietary lipid during severe childhood malnutrition. Arch Dis Child. 2002 Dec;87(6):522-5. doi: 10.1136/adc.87.6.522[↩]
- Brinson RR, Hanumanthu SK, Pitts WM. A reappraisal of the peptide-based enteral formulas: clinical applications. Nutr Clin Pract. 1989 Dec;4(6):211-7. doi: 10.1177/0115426589004006211[↩]
- Holt PR. Medium chain triglycerides. A useful adjunct in nutritional therapy. Gastroenterology. 1967 Dec;53(6):961-6.[↩]
- Smart KM, Alex G, Hardikar W. Feeding the child with liver disease: a review and practical clinical guide. J Gastroenterol Hepatol. 2011 May;26(5):810-5. doi: 10.1111/j.1440-1746.2011.06687.x[↩]
- Löscher W, Potschka H, Sisodiya SM, Vezzani A. Drug Resistance in Epilepsy: Clinical Impact, Potential Mechanisms, and New Innovative Treatment Options. Pharmacol Rev. 2020 Jul;72(3):606-638. doi: 10.1124/pr.120.019539[↩]
- Helmholz HF. The treatment of epilepsy in childhood: five years’ experience with the ketogenic dieT. J Am Med Assoc. (1927) 88:2028–32. 10.1001/jama.1927.0268052001800825996397[↩]
- Wilder RM . The effects of ketonemia on the course of epilepsy. Mayo Clin Proc. (1921) 2:307–8.[↩][↩]
- Huttenlocher PR, Wilbourn AJ, Signore JM. Medium-chain triglycerides as a therapy for intractable childhood epilepsy. Neurology. (1971) 21:1097–103. 10.1212/WNL.21.11.1097[↩]
- Neal EG, Chaffe H, Schwartz RH, Lawson MS, Edwards N, Fitzsimmons G, et al. A randomized trial of classical and medium-chain triglyceride ketogenic diets in the treatment of childhood epilepsy. Epilepsia. (2009) 50:1109–17. 10.1111/j.1528-1167.2008.01870.x[↩]
- Pervaiz MA, Kendal F, Hegde M, Singh RH. MCT oil-based diet reverses hypertrophic cardiomyopathy in a patient with very long chain acyl-coA dehydrogenase deficiency. Indian J Hum Genet. 2011 Jan;17(1):29-32. doi: 10.4103/0971-6866.82190[↩]
- Bray GA, Paeratakul S, Popkin BM. Dietary fat and obesity: a review of animal, clinical and epidemiological studies. Physiol Behav. 2004;83:549–55. https://www.ncbi.nlm.nih.gov/pubmed/15621059[↩]
- Babayan VK. Medium chain triglycerides and structured lipids. Lipids. 1987;22:417–20 https://www.ncbi.nlm.nih.gov/pubmed/3112486[↩]
- St-Onge MP. Dietary fats, teas, dairy, and nuts: potential functional foods for weight control? Am J Clin Nutr. 2005;81:7–15. https://www.ncbi.nlm.nih.gov/pubmed/15640454[↩]
- Baba N, Bracco EF, Hashim SA. Enhanced thermogenesis and diminished deposition of fat in response to overfeeding with diet containing medium chain triglyceride. Am J Clin Nutr. 1982;35:678–82.[↩]
- Crozier G, Bois-Joyeux B, Chanez M, Girard J, Peret J. Metabolic effects induced by long-term feeding of medium-chain triglycerides in the rat. Metabolism. 1987;36:807–14.[↩]
- St-Onge MP, Bourque C, Jones PJ, Ross R, Parsons WE. Medium-versus long-chain triglycerides for 27 days increases fat oxidation and energy expenditure without resulting in changes in body composition in overweight women. Int J Obes Relat Metab Disord. 2003;27:95–102. https://www.ncbi.nlm.nih.gov/pubmed/12532160[↩][↩]
- St-Onge MP, Ross R, Parsons WD, Jones PJ. Medium-chain triglycerides increase energy expenditure and decrease adiposity in overweight men. Obes Res. 2003;11:395–402. https://www.ncbi.nlm.nih.gov/pubmed/12634436[↩][↩]
- St-Onge MP, Jones PJ. Physiological effects of medium-chain triglycerides: potential agents in the prevention of obesity. J Nutr. 2002;132:329–32. https://www.ncbi.nlm.nih.gov/pubmed/11880549[↩]
- Dietary medium-chain triacylglycerols suppress accumulation of body fat in a double-blind, controlled trial in healthy men and women. Tsuji H, Kasai M, Takeuchi H, Nakamura M, Okazaki M, Kondo K. J Nutr. 2001 Nov; 131(11):2853-9. https://www.ncbi.nlm.nih.gov/pubmed/11694608/[↩]
- Effects of margarine containing medium-chain triacylglycerols on body fat reduction in humans. Nosaka N, Maki H, Suzuki Y, Haruna H, Ohara A, Kasai M, Tsuji H, Aoyama T, Okazaki M, Igarashi O, Kondo K. J Atheroscler Thromb. 2003; 10(5):290-8. https://www.jstage.jst.go.jp/article/jat/10/5/10_5_290/_pdf/-char/en[↩]
- Abstract P285: Small Dose of Medium Chain Fatty Acids From Coconut Oil Does Not Enhance Thermogenesis in Overweight Adolescents. Circulation March 7, 2017, Volume 135, Issue Suppl 1. http://circ.ahajournals.org/content/135/Suppl_1/AP285[↩]
- Diet supplemented with MCT oil in the management of childhood diarrhea. Asia Pac J Clin Nutr 2007;16 (2):286-292. http://apjcn.nhri.org.tw/server/APJCN/16/2/286.pdf[↩][↩][↩]
- Kaunitz H. Biological and therapeutic effects of ‘MCT’ (Medium Chain Triglycerides) from coconut oil. Coconuts Today, October 2001 Special Issue, 18-21.[↩][↩]
- Babayan VK. Medium chain length fatty acid esters and their medical and nutritional applications. J Am Oil Chem Soc. 1981; 58: 49A-51A.[↩]
- Shcherbakova K., Schwarz A., Apryatin S., Karpenko M., Trofimov A. Supplementation of Regular Diet With Medium-Chain Triglycerides for Procognitive Effects: A Narrative Review. Front. Nutr. 2022;9:934497. doi: 10.3389/fnut.2022.934497[↩]
- Henderson S.T., Vogel J.L., Barr L.J., Garvin F., Jones J.J., Costantini L.C. Study of the ketogenic agent AC-1202 in mild to moderate Alzheimer’s disease: A randomized, double-blind, placebo-controlled, multicenter trial. Nutr. Metab. 2009;6:1–25. doi: 10.1186/1743-7075-6-31[↩]
- Ledeboer M, Masclee AA, Jansen JB, Lamers CB. Effect of equimolar amounts of long-chain triglycerides and medium-chain triglycerides on small bowel transit time in humans. J Parenter Enteral Nutr 1995; 19:5-8.[↩]
- Heidt C, Fobker M, Newport M, Feldmann R, Fischer T, Marquardt T. Beta-Hydroxybutyrate (BHB), Glucose, Insulin, Octanoate (C8), and Decanoate (C10) Responses to a Medium-Chain Triglyceride (MCT) Oil with and without Glucose: A Single-Center Study in Healthy Adults. Nutrients. 2023 Feb 24;15(5):1148. doi: 10.3390/nu15051148[↩]
- Gopala, KAG, Gaurav, R, Ajit, SB, et al. (2010) Coconut oil: chemistry, production and its applications – a review. Indian Coconut J 73, 15–27.[↩]
- Chandrashekar, P, Lokesh, BR & Gopala, KAG (2010) Hypolipidemic effect of blends of coconut oil with soybean oil or sunflower oil in experimental rats. Food Chem 123, 728–733.[↩]
- United States Department of Agriculture. Agricultural Research Service. National Nutrient Database for Standard Reference Legacy Release. https://ndb.nal.usda.gov/ndb/search/list[↩][↩][↩]
- Dietary Fats and Cardiovascular Disease: A Presidential Advisory From the American Heart Association. Circulation. June 15, 2017. http://circ.ahajournals.org/content/early/2017/06/15/CIR.0000000000000510[↩]
- Effects of saturated fatty acids on serum lipids and lipoproteins: a systematic review and regression analysis. World Health Organization. http://apps.who.int/iris/bitstream/handle/10665/246104/9789241565349-eng.pdf[↩]
- Abstract P285: Small Dose of Medium Chain Fatty Acids From Coconut Oil Does Not Enhance Thermogenesis in Overweight Adolescents. Circulation March 7, 2017, Volume 135, Issue Suppl 1. https://doi.org/10.1161/circ.135.suppl_1.p285[↩]
- Effects of coconut oil consumption on energy metabolism, cardiometabolic risk markers, and appetitive responses in women with excess body fat. European Journal of Nutrition Eur J Nutr (2018) 57: 1627. https://link.springer.com/article/10.1007/s00394-017-1448-5[↩]
- How healthy is Coconut Oil? https://www.selfprinciple.org/healthy-coconut-oil/[↩][↩]
- Kossoff EH, Dorward JL. The modified Atkins diet. Epilepsia. 2008 Nov;49 Suppl 8:37-41. doi: 10.1111/j.1528-1167.2008.01831.x[↩]
- Prostaglandins Leukot Essent Fatty Acids. 2004 Mar;70(3):309-19. The therapeutic implications of ketone bodies: the effects of ketone bodies in pathological conditions: ketosis, ketogenic diet, redox states, insulin resistance, and mitochondrial metabolism. http://www.plefa.com/article/S0952-3278(03)00221-7/fulltext[↩]
- Very-low-carbohydrate ketogenic diet v. low-fat diet for long-term weight loss: a meta-analysis of randomised controlled trials. Bueno NB, de Melo IS, de Oliveira SL, da Rocha Ataide T. Br J Nutr. 2013 Oct; 110(7):1178-87. https://www.ncbi.nlm.nih.gov/pubmed/23651522/[↩]
- Therapeutic role of low-carbohydrate ketogenic diet in diabetes. Al-Khalifa A, Mathew TC, Al-Zaid NS, Mathew E, Dashti HM. Nutrition. 2009 Nov-Dec; 25(11-12):1177-85. https://www.ncbi.nlm.nih.gov/pubmed/19818281/[↩]
- Beneficial effects of ketogenic diet in obese diabetic subjects. Dashti HM, Mathew TC, Khadada M, Al-Mousawi M, Talib H, Asfar SK, Behbahani AI, Al-Zaid NS. Mol Cell Biochem. 2007 Aug; 302(1-2):249-56. https://www.ncbi.nlm.nih.gov/pubmed/17447017/[↩]
- A ketogenic diet favorably affects serum biomarkers for cardiovascular disease in normal-weight men. Sharman MJ, Kraemer WJ, Love DM, Avery NG, Gómez AL, Scheett TP, Volek JS. J Nutr. 2002 Jul; 132(7):1879-85. https://www.ncbi.nlm.nih.gov/pubmed/12097663/[↩]
- Bueno N.B., de Melo I.S., de Oliveira S.L., da Rocha Ataide T. Very-low-carbohydrate ketogenic diet v. low-fat diet for long-term weight loss: A meta-analysis of randomised controlled trials. Br. J. Nutr. 2013;110:1178–1187. doi: 10.1017/S0007114513000548[↩]
- Paoli A., Rubini A., Volek J.S., Grimaldi K.A. Beyond weight loss: A review of the therapeutic uses of very-low-carbohydrate (ketogenic) diets. Eur. J. Clin. Nutr. 2013;67:789–796. doi: 10.1038/ejcn.2013.116[↩]
- Popular diets: a scientific review. Freedman MR, King J, Kennedy E. Obes Res. 2001 Mar; 9 Suppl 1():1S-40S. https://www.ncbi.nlm.nih.gov/pubmed/11374180/[↩]
- The regulation of the release of ketone bodies by the liver. Krebs HA. Adv Enzyme Regul. 1966; 4():339-54. https://www.ncbi.nlm.nih.gov/pubmed/4865971/[↩]
- Brain metabolism during fasting. Owen OE, Morgan AP, Kemp HG, Sullivan JM, Herrera MG, Cahill GF Jr. J Clin Invest. 1967 Oct; 46(10):1589-95. https://www.ncbi.nlm.nih.gov/pubmed/6061736/[↩]
- Amino acid metabolism during prolonged starvation. Felig P, Owen OE, Wahren J, Cahill GF Jr. J Clin Invest. 1969 Mar; 48(3):584-94. https://www.ncbi.nlm.nih.gov/pubmed/5773094/[↩]
- Owen O.E. Ketone bodies as a fuel for the brain during starvation. Biochem. Mol. Biol. Educ. 2005;33:246–251. doi: 10.1002/bmb.2005.49403304246.[↩]
- Liver and kidney metabolism during prolonged starvation. Owen OE, Felig P, Morgan AP, Wahren J, Cahill GF Jr. J Clin Invest. 1969 Mar; 48(3):574-83. https://www.ncbi.nlm.nih.gov/pubmed/5773093/[↩]
- St-Onge M.P., Bosarge A. Weight-loss diet that includes consumption of medium-chain triacylglycerol oil leads to a greater rate of weight and fat mass loss than does olive oil. Am. J. Clin. Nutr. 2008;87:621–626. doi: 10.1093/ajcn/87.3.621[↩]
- de la Rubia Ortí JE, García-Pardo MP, Drehmer E, Sancho Cantus D, Julián Rochina M, Aguilar MA, Hu Yang I. Improvement of Main Cognitive Functions in Patients with Alzheimer’s Disease after Treatment with Coconut Oil Enriched Mediterranean Diet: A Pilot Study. J Alzheimers Dis. 2018;65(2):577-587. doi: 10.3233/JAD-180184[↩]
- Yudkoff M, Daikhin Y, Melø TM, Nissim I, Sonnewald U, Nissim I. The ketogenic diet and brain metabolism of amino acids: relationship to the anticonvulsant effect. Annu Rev Nutr. (2007) 27:415–30. 10.1146/annurev.nutr.27.061406.093722[↩]
- Ma W, Berg J, Yellen G. Ketogenic diet metabolites reduce firing in central neurons by opening K(ATP) channels. J Neurosci. (2007) 27:3618–25. 10.1523/JNEUROSCI.0132-07.2007[↩]
- Chang P, Augustin K, Boddum K, Williams S, Sun M, Terschak JA, et al. Seizure control by decanoic acid through direct AMPA receptor inhibition. Brain. (2016) 139:431–43. 10.1093/brain/awv325[↩]
- Chang P, Terbach N, Plant N, Chen PE, Walker MC, Williams RSB. Seizure control by ketogenic diet-associated medium chain fatty acids. Neuropharmacology. (2013) 69:105–114. 10.1016/j.neuropharm.2012.11.004[↩]
- Wlaz P, Socała K, Nieoczym D, Zarnowski T, Zarnowska I, Czuczwar SJ, Gasior M. Acute anticonvulsant effects of capric acid in seizure tests in mice. Prog Neuropsychopharmacol Biol Psychiatry. (2015) 57:110–6. 10.1016/j.pnpbp.2014.10.013[↩]
- Oldendorf WH. Carrier-mediated blood-brain barrier transport of short-chain monocarboxylic organic acids. Am J Physiol. (1973) 224:1450–3. 10.1152/ajplegacy.1973.224.6.1450[↩]
- Martin-McGill KJ, Bresnahan R, Levy RG, Cooper PN. Ketogenic diets for drug-resistant epilepsy. Cochrane Database Syst Rev. 2020 Jun 24;6(6):CD001903. doi: 10.1002/14651858.CD001903.pub5[↩][↩]
- Paoli A. Ketogenic Diet for Obesity: Friend or Foe? International Journal of Environmental Research and Public Health. 2014;11(2):2092-2107. doi:10.3390/ijerph110202092. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3945587/[↩]
- Kim J, Basak JM, Holtzman DM. The role of apolipoprotein E in Alzheimer’s disease. Neuron. 2009 Aug 13;63(3):287-303. doi: 10.1016/j.neuron.2009.06.026[↩]
- Michaelson DM. APOE ε4: the most prevalent yet understudied risk factor for Alzheimer’s disease. Alzheimers Dement. 2014 Nov;10(6):861-8. doi: 10.1016/j.jalz.2014.06.015[↩]
- Brandon JA, Farmer BC, Williams HC, Johnson LA. APOE and Alzheimer’s Disease: Neuroimaging of Metabolic and Cerebrovascular Dysfunction. Front Aging Neurosci. 2018 Jun 14;10:180. doi: 10.3389/fnagi.2018.00180[↩]
- Craft S, Asthana S, Schellenberg G, Baker L, Cherrier M, Boyt AA, Martins RN, Raskind M, Peskind E, Plymate S. Insulin effects on glucose metabolism, memory, and plasma amyloid precursor protein in Alzheimer’s disease differ according to apolipoprotein-E genotype. Ann N Y Acad Sci. 2000 Apr;903:222-8. doi: 10.1111/j.1749-6632.2000.tb06371.x[↩]
- Reger MA, Watson GS, Frey WH 2nd, Baker LD, Cholerton B, Keeling ML, Belongia DA, Fishel MA, Plymate SR, Schellenberg GD, Cherrier MM, Craft S. Effects of intranasal insulin on cognition in memory-impaired older adults: modulation by APOE genotype. Neurobiol Aging. 2006 Mar;27(3):451-8. doi: 10.1016/j.neurobiolaging.2005.03.016[↩]
- Risner ME, Saunders AM, Altman JF, Ormandy GC, Craft S, Foley IM, Zvartau-Hind ME, Hosford DA, Roses AD; Rosiglitazone in Alzheimer’s Disease Study Group. Efficacy of rosiglitazone in a genetically defined population with mild-to-moderate Alzheimer’s disease. Pharmacogenomics J. 2006 Jul-Aug;6(4):246-54. doi: 10.1038/sj.tpj.6500369[↩]
- Liang WS, Reiman EM, Valla J, Dunckley T, Beach TG, Grover A, Niedzielko TL, Schneider LE, Mastroeni D, Caselli R, Kukull W, Morris JC, Hulette CM, Schmechel D, Rogers J, Stephan DA. Alzheimer’s disease is associated with reduced expression of energy metabolism genes in posterior cingulate neurons. Proc Natl Acad Sci U S A. 2008 Mar 18;105(11):4441-6. doi: 10.1073/pnas.0709259105[↩]
- Gibson, G.E., Haroutunian, V., Zhang, H., Park, L.C.H., Shi, Q., Lesser, M., Mohs, R.C., Sheu, R.K.-F. and Blass, J.P. (2000), Mitochondrial damage in Alzheimer’s disease varies with apolipoprotein E genotype. Ann Neurol., 48: 297-303. https://doi.org/10.1002/1531-8249(200009)48:3<297::AID-ANA3>3.0.CO;2-Z[↩]
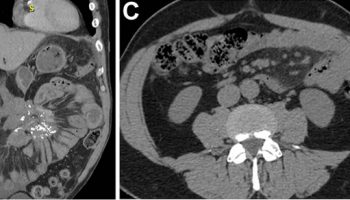


{kind=link}