Contents
What is measles
Measles (also called Rubeola) is a highly infectious disease caused by a virus, RNA paramyxovirus, that is spread via the respiratory route from person to person through droplets in the air. Over 90% of people who haven’t been vaccinated for measles will get it if they are near an infected person. A person who is exposed to the virus might not show symptoms until 8-10 days later. Early symptoms of measles include fever, cough, runny nose and conjunctivitis (redness and irritation in membranes of the eyes). A rash appears after the third or fourth day. The spots are red and slightly raised. Measles affects the skin and respiratory tract.
- Measles can lead to serious complications. For every 1,000 children who get measles, one or two will die from it.
- Measles may cause pregnant woman to give birth prematurely, or have a low-birth-weight baby.
Anyone can get measles if they haven’t been vaccinated or had it before, although it’s most common in young children and young unvaccinated adults.
People with measles are contagious (can spread the disease) from 4 days before the rash appears until about 4 days after it does, and are most contagious while they have a fever, runny nose, and cough. Those with weakened immune systems due to other conditions (like HIV and AIDS) may be contagious until they recover from measles.
People who are at increased risk of potentially fatal measles complications include:
- anyone with a chronic illness
- children younger than five years
- adults.
Measles is a vaccine preventable disease and vaccination against the disease is recommended as part of routine childhood immunization.
Someone with measles is infectious for 4 days before and 2 days after the rash appears.
Measles has an incubation period of 8-14 days with 2 distinct phases:
- The pre-eruptive and catarrhal stage: Signs of a general viral illness.
- The eruptive or exanthematous stage: The classic measle rash then occurs.
Measles is highly communicable and occurs world-wide. Since the introduction of immunization, the incidence of measles has fallen dramatically in the United States. However, measles is still one of the most common childhood infections in resource-deprived countries with about 20 million cases of measles still happen worldwide every year.
Measles Outbreaks
Measles is very rare in the United States. Before measles vaccination became available in 1963, an estimated 3 to 4 million people got measles each year in the United States. Of these, approximately 500,000 cases were reported each year to the Centers for Disease Control and Prevention (CDC); of these, 400 to 500 died, 48,000 were hospitalized, and 1,000 developed encephalitis (brain swelling) from measles 1. Since then, widespread use of measles vaccine has led to a greater than 99% reduction in measles cases compared with the pre-vaccine era. The number of U.S. measles cases declined steadily to a low of 37 people in 2004. From 2000 to 2007, only about 63 cases per year were reported. However, measles is still common in other countries. But recent years have seen spikes in measles outbreaks, including 131 cases in the first half of 2008 and 644 cases in 2014. Most U.S. outbreaks begin with people who were infected outside of the country, with the disease spreading quickly in areas where too few people have received the vaccine. About 85% of people infected with measles were not immunized or their immunization status was unknown, although they were eligible to receive the vaccine.
The people at highest risk of getting measles during these outbreaks are infants (who aren’t old enough to get the vaccine), pregnant women, and people with poor nutrition or weakened immune systems.
During a measles outbreak, an injection of measles antibodies (called immune globulin) can help protect people who haven’t been vaccinated if they come into contact with an infected person (called “exposure”). The injection is most effective if it’s given within 6 days of exposure. These antibodies can either prevent measles or make symptoms less severe.
For women who are not pregnant and people not in one of the other at-risk groups, the measles vaccine may offer some protection if given within 72 hours of measles exposure.
Unvaccinated people who are exposed to measles and show symptoms of the virus should seek medical care. Otherwise, they should stay home and not return to childcare, school, or work until 21 days after they were exposed.
Could measles ever re-establish itself in the United States?
Yes, measles could become endemic (constant presence of a disease in an area) in the United States again, especially if vaccine coverage levels drop. This can happen when people:
- forget to get vaccinated on time,
- don’t know that they need a vaccine dose (this is most common among adults), or
- refuse vaccines for religious, philosophical or personal reasons.
Research shows that people who refuse vaccines tend to group together in communities. When measles gets into communities with pockets of unvaccinated people, outbreaks are more likely to occur. These communities make it difficult to control the spread of the disease. And these communities make us vulnerable to having the virus re-establish itself in our country.
Is measles contagious
Measles is highly contagious, and spread by respiratory droplets. Measles is usually spread when a person breathes in the measles virus that has been coughed or sneezed into the air by an infectious person. Measles is one of the most easily spread of all human infections. Just being in the same room as someone with measles can result in infection.
People with measles are usually infectious from just before the symptoms begin until four days after the rash appears. The time from exposure to becoming sick is usually about 10 days. The rash usually appears around 14 days after exposure.
Isolation. Because measles is highly contagious from about four days before to four days after the rash breaks out, people with measles shouldn’t return to activities in which they interact with other people during this period.
It may also be necessary to keep nonimmunized people — siblings, for example — away from the infected person.
Measles is preventable with vaccination. Hence the main risk factors for infection are:
- Unvaccinated children coming into contact with a (adult or another child) carrier or an infected case;
- Immunosuppressed individuals not developing immunity after vaccination.
- People with a weak immune system (e.g., people who are receiving chemotherapy or radiotherapy for cancer or people who take high-dose steroid medications) even if they have been fully immunized or have had past measles infection.
Rubeola vs Rubella
Rubella is also commonly known as German measles or 3-day measles — is an infection that mostly affects the skin and lymph nodes. It is caused by the rubella virus (not the same virus that causes measles).
Rubella spreads when people breathe in virus-infected tiny drops of fluid, such as the droplets sprayed into the air when a person with rubella sneezes or coughs, or share food or drink with someone who’s infected. It also can pass through a pregnant woman’s bloodstream to infect her unborn child.
People who have rubella are most contagious from 1 week before to 1 week after the rash appears. Someone who is infected but has no symptoms can still spread the virus.
The rubella rash usually lasts 3 days. Lymph nodes may remain swollen for a week or more, and joint pain can last for more than 2 weeks. Children who have rubella usually recover within 1 week, but adults may take longer.
Infants who have congenital rubella syndrome can shed the virus in urine and fluid from the nose and throat for a year or more and may pass the virus to people who have not been immunized.
- It’s a generally mild disease in children; the primary medical danger of rubella is the infection of pregnant women because it can cause congenital rubella syndrome in developing babies.
Before a vaccine against rubella became available in 1969, rubella epidemics happened every 6-9 years, usually among kids 5 to 9 years old, along with many cases of congenital rubella. Thanks to immunization, there are far fewer cases of rubella and congenital rubella.
Most rubella infections today appear in young, non-immunized adults rather than in kids. In fact, experts estimate that 10% of young adults are currently susceptible to rubella, which could pose a danger to any children they might have someday.
Rubella Incubation Period
The incubation period for rubella is 14–23 days, with an average incubation period of 16–18 days. This means that it can take 2–3 weeks for a child to get rubella after being exposed to someone with the disease.
Rubella Signs and Symptoms
Rubella infection may begin with 1-2 days of mild fever (99-100°F, 37.2–37.8°C) and swollen, tender lymph nodes, usually in the back of the neck or behind the ears. A rash then begins on the face and spreads downward. As it spreads, it usually clears on the face.
The rubella rash is often the first sign of illness that a parent notices. It can look like many other viral rashes, appearing as either pink or light red spots, which may merge to form evenly colored patches. The rash can itch and lasts up to 3 days. As the rash clears, the affected skin might shed in very fine flakes.
Other symptoms of rubella (these are more common in teens and adults) can include headache, loss of appetite, mild conjunctivitis (inflammation of the lining of the eyelids and eyeballs), a stuffy or runny nose, swollen lymph nodes in other parts of the body, and pain and swelling in the joints (especially in young women). Many people with rubella have few or no symptoms.
Rubella in a pregnant woman can cause congenital rubella syndrome, with potentially devastating consequences for the developing fetus. Children who are infected with rubella before birth are at risk for growth problems; intellectual disability; defects of the heart and eyes; deafness; and liver, spleen, and bone marrow problems.
Rubella Prevention
Rubella can be prevented by the rubella vaccine. Widespread immunization against rubella is critical to controlling the spread of the disease, thereby preventing birth defects caused by congenital rubella syndrome.
The vaccine is usually given to children at 12–15 months of age as part of the scheduled measles-mumps-rubella (MMR) immunization. A second dose of MMR usually is given at 4–6 years of age. As with all immunization schedules, there are important exceptions and special circumstances. For example, if your child will be traveling outside the United States, the vaccine can be given as early as 6 months of age. Talk to your child’s doctor to see when the vaccine is needed.
The rubella vaccine should not be given to pregnant women or to a woman who may become pregnant within 1 month of receiving the vaccine. If you are thinking about becoming pregnant, make sure that you’re immune to rubella through a blood test or proof of immunization. If you’re not immune, you should receive the vaccine at least 1 month before you become pregnant.
Pregnant women who are not immune should avoid anyone who has the illness and should be vaccinated after delivery so that they will be immune during any future pregnancies.
Rubella Treatment
Rubella cannot be treated with antibiotics because they do not work against viral infections. Unless there are complications, rubella will get better on its own.
Any pregnant woman who has been exposed to rubella should contact her obstetrician immediately.
Rubella usually is mild in kids, who often can be cared for at home. Monitor your child’s temperature and call the doctor if the fever climbs too high.
To ease minor discomfort, you can give your child acetaminophen or ibuprofen. Remember, you should never give aspirin to a child who has a viral illness, as its use in such cases has been associated with the development of Reye syndrome.
What does measles look like
Figure 1. Measles rash


Figure 2. Measles rash

Figure 3. Koplik’s spots (inside mouth)
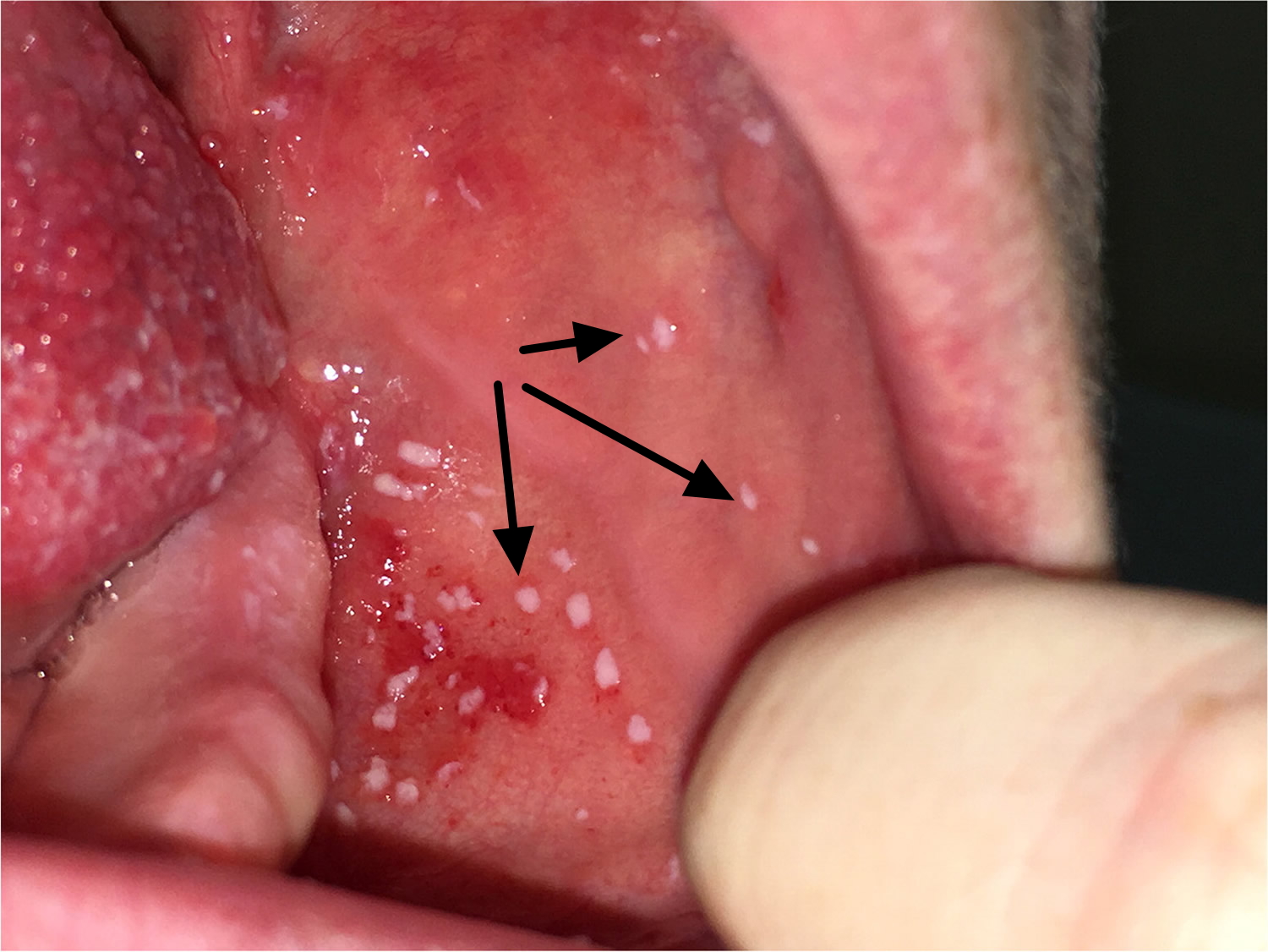
Figure 4. Measles conjunctivitis

What causes measles
Measles is caused by a type of virus called a paramyxovirus. This kind of virus spreads from person to person via ‘droplets’ from coughing or sneezing.
You can catch measles by breathing in these droplets or, if the droplets have settled on a surface, infection can also occur if someone touches contaminated surfaces or objects and then touches their own mouth or nose or eats before washing their hands. The measles virus can survive on surfaces for a few hours.
Once inside your body, the virus multiplies in the back of your throat and lungs before spreading throughout your body, including your respiratory system and the skin. Symptoms usually occur about 10 to 12 days after infection.
Estimates suggest that a person with measles will infect about nine in every 10 people they have contact with who have not been immunized or previously infected with measles.
Measles (Rubeola) Prevention
The disease can be prevented by immunizing children with measles-mumps-rubella vaccine (MMR) or measles-mumps-rubella-varicella vaccine (MMRV) given when they’re 12 to 15 months old and again when they’re 4 to 6 years old.
The Centers for Disease Control and Prevention (CDC) 1 recommends children get two doses of MMR vaccine, starting with the first dose at 12 through 15 months of age, and the second dose at 4 through 6 years of age. Teens and adults should also be up to date on their MMR vaccination.
The measles-mumps-rubella vaccine (MMR) vaccine is very safe and effective. Two doses of MMR vaccine are about 97% effective at preventing measles; one dose is about 93% effective.
Children may also get measles-mumps-rubella-varicella vaccine (MMRV), which protects against measles, mumps, rubella, and varicella (chickenpox). This vaccine is only licensed for use in children who are 12 months through 12 years of age.
Infants are generally protected from measles for 6 months after birth due to immunity passed on by their mothers. Measles vaccine usually is not given to infants younger than 12 months old. But if there’s a measles outbreak, or a child will be traveling outside the United States, the vaccine may be given when a child is 6-11 months old, followed by the usual measles-mumps-rubella vaccine (MMR) immunization at 12-15 months and 4-6 years of age.
The measles vaccine sometimes causes side effects in kids who don’t have underlying health problems. The most common reactions are fever 6-12 days after vaccination (in about 15% of kids vaccinated) and a measles-like rash, which isn’t contagious and fades on its own (in about 5% of vaccinated kids).
As with all immunization schedules, there are important exceptions and special circumstances. Your doctor will have the most current information about vaccine recommendations.
Who Should Get MMR (measles-mumps-rubella) Vaccine?
Children
CDC recommends all children get two doses of MMR (measles-mumps-rubella) vaccine, starting with the first dose at 12 through 15 months of age, and the second dose at 4 through 6 years of age. Children can receive the second dose earlier as long as it is at least 28 days after the first dose.
MMR vaccine is given later than some other childhood vaccines because antibodies transferred from the mother to the baby can provide some protection from disease and make the MMR vaccine less effective until about 1 year of age.
Measles-mumps-rubella-varicella vaccine (MMRV), which protects against measles, mumps, rubella, and varicella (chickenpox). This vaccine is only licensed for use in children who are 12 months through 12 years of age. CDC recommends that children get one dose of MMRV vaccine at 12 through 15 months of age, and the second dose at 4 through 6 years of age. A doctor can help parents decide whether to use this MMRV vaccine or MMR vaccine. MMRV is given by shot and may be given at the same time as other vaccines.
Students at post-high school educational institutions
Students at post-high school educational institutions who do not have evidence of immunity need two doses of MMR vaccine, separated by at least 28 days.
Adults
Adults who do not have evidence of immunity should get at least one dose of MMR vaccine.
International travelers
People 6 months of age and older who will be traveling internationally should be protected against measles. Before any international travel:
- Infants 6 through 11 months of age should receive one dose of MMR vaccine. Infants who get one dose of MMR vaccine before their first birthday should get two more doses (one dose at 12 through 15 months of age and another dose separated by at least 28 days).
- Children 12 months of age and older should receive two doses of MMR vaccine, separated by at least 28 days.
- Teenagers and adults who do not have evidence of immunity against measles should get two doses of MMR vaccine separated by at least 28 days.
Women of Childbearing Age
Women of childbearing age should check with their doctor to make sure they are vaccinated before they get pregnant. Women of childbearing age who do not have evidence of immunity should get at least one dose of MMR vaccine.
It is safe for breastfeeding women to receive MMR vaccination. Breastfeeding does not interfere with the response to MMR vaccine, and the baby will not be affected by the vaccine through breast milk.
How Well Does the MMR Vaccine Work?
MMR vaccine is very effective at protecting people against measles, mumps, and rubella, and preventing the complications caused by these diseases. People who received two doses of MMR vaccine as children according to the U.S. vaccination schedule are considered protected for life.
Two doses of MMR vaccine are 97% effective against measles and 88% effective against mumps. One dose of MMR vaccine is 93% effective against measles, 78% effective against mumps, and 97% effective against rubella.
MMR is an attenuated (weakened) live virus vaccine. This means that after injection, the viruses cause a harmless infection in the vaccinated person with very few, if any, symptoms before they are eliminated from the body. The person’s immune system fights the infection caused by these weakened viruses, and immunity (the body’s protection from the virus) develops.
A few people who get two doses of MMR vaccine may still get measles, mumps, or rubella if they are exposed to the viruses that cause these diseases. Experts aren’t sure why; it could be that their immune systems didn’t respond as well as they should have to the vaccine.
- About 3 out of 100 people who get two doses of MMR vaccine will get measles if exposed to the virus. However, they are more likely to have a milder illness, and are also less likely to spread the disease to other people.
- Two doses of MMR vaccine are 88% (range 31% to 95%) effective at preventing mumps. Mumps outbreaks can still occur in highly vaccinated U.S. communities, particularly in close-contact settings such as schools, colleges, and camps. However, high vaccination coverage helps limit the size, duration, and spread.
- While there are not many studies available, most people who do not respond to the rubella component of the first MMR dose would be expected to respond to the second dose.
Could I still get measles if I am fully vaccinated?
The measles vaccine is very effective. One dose of measles vaccine is about 93% effective at preventing measles if exposed to the virus. Two doses are about 97% effective.
Very few people—about three out of 100—who get two doses of measles vaccine will still get measles if exposed to the virus. Experts aren’t sure why. It could be that their immune systems didn’t respond as well as they should have to the vaccine. But the good news is, fully vaccinated people who get measles are much more likely to have a milder illness. And fully vaccinated people are also less likely to spread the disease to other people, including people who can’t get vaccinated because they are too young or have weakened immune systems.
Do I ever need a booster vaccine?
No. The CDC considers people who received two doses of measles vaccine as children according to the U.S. vaccination schedule protected for life, and they do not ever need a booster dose.
Adults need at least one dose of measles vaccine, unless they have evidence of immunity. Adults who are going to be in a setting that poses a high risk for measles transmission should make sure they have had two doses separated by at least 28 days. These adults include students at post-high school education institutions, healthcare personnel, and international travelers.
Who Should NOT Get MMR Vaccine?
Some people should NOT get MMR vaccine or should wait:
- Anyone who has ever had a life-threatening allergic reaction to the antibiotic neomycin, or any other component of MMR vaccine, should not get the vaccine. Tell your doctor if you have any severe allergies.
- Anyone who had a life-threatening allergic reaction to a previous dose of MMR or MMRV vaccine should not get another dose.
- Some people who are sick at the time the shot is scheduled may be advised to wait until they recover before getting MMR vaccine.
- Pregnant women should not get MMR vaccine. Pregnant women who need the vaccine should wait until after giving birth. Women should avoid getting pregnant for 4 weeks after vaccination with MMR vaccine.
- Tell your doctor if the person getting the vaccine:
- Has HIV/AIDS, or another disease that affects the immune system
- Is being treated with drugs that affect the immune system, such as steroids
- Has any kind of cancer
- Is being treated for cancer with radiation or drugs
- Has ever had a low platelet count (a blood disorder)
- Has gotten another vaccine within the past 4 weeks
- Has recently had a transfusion or received other blood products
- Any of these might be a reason to not get the vaccine, or delay vaccination until later.
A minor illness, such as a cold or chickenpox, should not delay anyone from receiving the benefits of MMR or any other vaccine. In addition, it is safe for people around a pregnant woman to be vaccinated. Measles, mumps, and rubella vaccine viruses are not transmitted from the vaccinated person, so a recently vaccinated person would not pose a risk to a pregnant woman.
Because certain people cannot receive the measles vaccine for health reasons, it’s all the more important to make sure that children who can get the vaccine get it on schedule. At-risk children depend on “herd immunity.” This means a high percentage of people have been immunized against a disease, which prevents the disease from spreading in a population and helps prevent outbreaks.
Who Does Not Need MMR Vaccine?
You do not need measles, mumps, and rubella (MMR) vaccine if you meet any of these criteria for evidence of immunity:
- You have written documentation of adequate vaccination:
- at least one dose of a measles-, mumps-, and rubella-containing vaccine administered on or after the first birthday for preschool-age children and adults not at high risk for exposure and transmission
- two doses of measles- and mumps-containing vaccine for school-age children and adults at high risk for exposure and transmission, including college students, healthcare personnel, and international travelers
- You had blood tests that show you are immune to measles, mumps, and rubella.
- You have laboratory confirmation of past measles, mumps, or rubella infection.
- You were born before 1957.*
If you do not have evidence of immunity against measles, mumps, and rubella, talk with your doctor about getting vaccinated. If you’re unsure whether you’ve been vaccinated, you should first try to find your vaccination records. If you do not have written documentation of MMR vaccine, you should get vaccinated. The MMR vaccine is safe, and there is no harm in getting another dose if you may already be immune to measles, mumps, or rubella.
If you received a measles vaccine in the 1960s, you may not need to be revaccinated. People who have documentation of receiving LIVE measles vaccine in the 1960s do not need to be revaccinated. People who were vaccinated prior to 1968 with either inactivated (killed) measles vaccine or measles vaccine of unknown type should be revaccinated with at least one dose of live attenuated measles vaccine. This recommendation is intended to protect those who may have received killed measles vaccine, which was available in 1963-1967 and was not effective.
* Birth before 1957 provides only presumptive evidence for measles, mumps, and rubella. Before vaccines were available, nearly everyone was infected with measles, mumps, and rubella viruses during childhood. The majority of people born before 1957 are likely to have been infected naturally and therefore are presumed to be protected against measles, mumps, and rubella.
Contact with someone with measles
If you’ve been in contact with someone with measles and you are not immune to measles (have not been immunized or have not had a measles infection), there are different treatment options. If you do not have immunity against measles, mumps, or rubella and are exposed to someone with one of these diseases, talk with your doctor about getting MMR vaccine. It is not harmful to get MMR vaccine after being exposed to measles, mumps, or rubella, and doing so may possibly prevent later disease.
During outbreaks, everyone without evidence of immunity should be brought up to date on their MMR vaccination. Sometimes during measles and mumps outbreaks, an additional dose of MMR may be given.
Depending on your situation, these may include:
- Contact in the last 72 hours – have a measles immunization immediately.
- Contact in the last three to seven days – immunoglobulin can be given for interim protection. This is known as passive immunization. Measles vaccination, or active immunization, should be given later to prevent further risk of infection, but not until five months after you received the immunoglobulin. Normal human immunoglobulin is given as an injection.
If you get MMR vaccine within 72 hours of initially being exposed to measles, you may get some protection against the disease, or have milder illness. Also, if you are given a medicine called immunoglobulin within six days of being exposed to measles, you may get some protection against the disease, or have milder illness. Except in healthcare settings, unvaccinated people who get their first dose of MMR vaccine within 72 hours after being exposed to measles may return to childcare, school, or work.
Measles complications
Up to a third of people with measles have complications. About one in every 1000 people with measles develops encephalitis (swelling of the brain).
- Early complications:
- otitis media (inflammation of the middle ear),
- respiratory infections – such as bronchitis, croup or laryngitis,
- pneumonia – a type of lung inflammation. As many as one out of every 20 children with measles gets pneumonia that causes about 60 per cent of measles deaths in young children.
- diarrhea and vomiting – may cause further complications such as dehydration
- encephalitis or brain inflammation – affects about one person with measles in every 1000. About 10 to 15 per cent of people with encephalitis die and 15 to 40 per cent of survivors have permanent brain damage to varying degrees.
- pregnancy problems – if a pregnant woman contracts measles, she risks miscarriage or preterm labor
- Late complications:
- Subacute Sclerosing Panencephalitis (SSPE): a central nervous system disorder developing many months or years after clinical measles with the patient developing abnormalities in personality, behavior, and memory, as well as blindness, muscle jerks, and spasticity. Subacute sclerosing panencephalitis usually begins about seven to ten years after the measles infection, even though the person seems to have fully recovered from the illness. Subacute sclerosing panencephalitis occurs in about one in every 100,000 cases of measles. Subacute sclerosing panencephalitis is an extremely rare progressive inflammation of the brain that causes brain degeneration and is always fatal. The risk of developing SSPE may be higher for a person who gets measles before they are two years of age. Since measles was eliminated in 2000, SSPE is rarely reported in the United States.
Measles (Rubeola) Prognosis
The probable outcome is excellent in uncomplicated cases. Complications such as pneumonia and encephalitis can be severe, however. Pneumonia accounts for 60% of deaths due to measles, because it is more common than encephalitis. Encephalitis has a mortality of 15%.
Measles signs and symptoms
- Measles begins like a bad cold, runny nose and dry cough with sore and red eyes (conjunctivitis)
- Your child will become gradually more unwell, with a temperature.
- You might notice tiny white marks, known as ‘Koplik’s spots’, on the inside of your child’s cheek and at the back of her mouth.
- A rash appears after the third or fourth day. The spots are red and slightly raised. They may be blotchy, but not itchy. The rash begins behind the ears and spreads to the face and neck, then the rest of the body.
- The illness usually lasts about a week.
The measles rash breaks out 3-5 days after symptoms start, and can coincide with high fevers up to 104°F (40°C). The red or reddish-brown rash usually first shows up as flat red spots on the forehead. It spreads to the rest of the face, then down the neck and torso to the arms, legs, and feet. The fever and rash gradually go away after a few days.
Measles is usually much more serious than chickenpox, German measles (rubella) or mumps. Serious complications include infections of the lungs (pneumonia), brain (encephalitis) and ear, which can lead to brain damage and death. Measles has been virtually eliminated in the US due to the MMR vaccination, though it can still be brought into the country by people coming from overseas.
The infection occurs in sequential stages over a period of two to three weeks.
- Infection and incubation. For the first 10 to 14 days after you’re infected, the measles virus incubates. You have no signs or symptoms of measles during this time.
- Nonspecific signs and symptoms. Measles typically begins with a mild to moderate fever, often accompanied by a persistent cough, runny nose, inflamed eyes (conjunctivitis) and sore throat. This relatively mild illness may last two or three days.
- Acute illness and rash. The rash consists of small red spots, some of which are slightly raised. Spots and bumps in tight clusters give the skin a splotchy red appearance. The face breaks out first, particularly behind the ears and along the hairline. Over the next few days, the rash spreads down the arms and trunk, then over the thighs, lower legs and feet. At the same time, fever rises sharply, often as high as 104 to 105.8 F (40 to 41 C). The measles rash gradually recedes, fading first from the face and last from the thighs and feet.
- Communicable period. A person with measles can spread the virus to others for about eight days, starting four days before the rash appears and ending when the rash has been present for four days.
Measles diagnosis
Your doctor will usually be able to diagnose measles from the combination of symptoms you may have, such as the characteristic rash and the small spots inside the mouth.
- A per-nasal aspirate and chest x-ray may be needed – the latter if pneumonia complicates the illness.
- Encephalitis requires a CT scan of the head for diagnosis.
Doctors must notify the Centers for Disease Prevention and Control (CDC) of all reported and suspected cases of measles. They will also notify the child’s school if necessary.
Your doctor might give your child a blood test to confirm whether it’s measles.
Measles treatment
Since measles is caused by a virus, there is no specific medical treatment for it and the virus has to run its course. A case of measles without complications usually lasts about 14 days and most people make a full recovery. But a child who is sick should drink plenty of fluids, get lots of rest, and be kept from spreading the infection to others.
Kids with measles should have their condition closely monitored by a doctor. In some cases, measles can lead to other complications, such as otitis media, croup, diarrhea, pneumonia, and encephalitis, which may require antibiotics or hospitalization.
In developing countries, vitamin A has been found to decrease complications and death associated with measles infections. In the U.S., vitamin A supplementation should be considered for children between 6 months and 2 years old who are hospitalized with measles and its complications.
Also, all kids over 6 months old with certain risk factors — such as vitamin A deficiency, a weakened immune system, or malnutrition — might benefit from vitamin A supplementation.
- Treatment is mainly supportive – people with measles infection are normally advised to rest, drink plenty of fluids, and take acetaminophen or ibuprofen or naproxen (Aleve) to help relieve the fever that accompanies measles.
- Antibiotics should only be used if secondary bacterial infection occurs. If a bacterial infection, such as pneumonia or an ear infection, develops while you or your child has measles, your doctor may prescribe an antibiotic.
- Immunity is conferred after the first measles disease and second attacks are uncommon.
- Vitamin A. People with low levels of vitamin A are more likely to have a more severe case of measles. Giving vitamin A may lessen the severity of the measles. It’s generally given as a large dose of 200,000 international units (IU) for two days.
Remember, you should never give aspirin to a child who has a viral illness, as its use in such cases has been associated with the development of Reye syndrome.
If you have measles, you should stay home for four days after you develop the rash. Staying home is an important way to not spread measles to other people.
Some measures can be taken to protect vulnerable individuals who have been exposed to the virus.
- Post-exposure vaccination. Nonimmunized people, including infants, may be given the measles vaccination within 72 hours of exposure to the measles virus to provide protection against the disease. If measles still develops, the illness usually has milder symptoms and lasts for a shorter time.
- Immune serum globulin. Pregnant women, infants and people with weakened immune systems who are exposed to the virus may receive an injection of proteins (antibodies) called immune serum globulin. When given within six days of exposure to the virus, these antibodies can prevent measles or make symptoms less severe.
Lifestyle and home remedies
If you or your child has measles, keep in touch with your doctor as you monitor the progress of the disease and watch for complications. Also try these comfort measures:
- Take it easy. Get rest and avoid busy activities.
- Sip something. Drink plenty of water, fruit juice and herbal tea to replace fluids lost by fever and sweating.
- Seek respiratory relief. Use a humidifier to relieve cough and sore throat.
- Rest your eyes. If you or your child finds bright light bothersome, as do many people with measles, keep the lights low or wear sunglasses. Also avoid reading or watching television if light from a reading lamp or from the television is bothersome.
Occasionally, measles develops into a serious disease that requires urgent treatment and can even be life threatening. Sometimes, people can die from complications even if they receive prompt medical attention.
Treatment depends on the complication but may include:
- hospitalization
- supportive care – for example, to maintain hydration, and to check for fever and infection
- antibiotics – to treat bacterial infection.





{kind=link}