Contents
What is meningioma
Meningioma is a type of slow-growing tumor that forms in the meninges (thin layers of tissue that cover and protect the brain and spinal cord) (see Figures 1 and 2 below). Meningiomas begin in the meninges, the layers of tissue that surround the outer part of the brain and spinal cord. Meningiomas account for about 1 out of 3 primary brain and spinal cord tumors. They are the most common brain tumors in adults (although strictly speaking, they are not actually brain tumors).
Most meningiomas grow very slowly, often over many years without causing symptoms. But in some instances, their effects on adjacent brain tissue, nerves or vessels may cause serious disability. Meningiomas are usually found in the cerebrum and cerebellum.
The risk of these meningiomas increases with age. Meningiomas occur about twice as often in women and are often discovered at older ages, but a meningioma may occur at any age. Sometimes these meningiomas run in families, especially in those with neurofibromatosis, a syndrome in which people develop many benign tumors of nerve tissue.
Because most meningiomas grow slowly, often without any significant signs and symptoms, they do not always require immediate treatment and may be monitored over time.
Meningiomas are often assigned a grade, based on how the cells look under the microscope.
- Grade I (Benign) meningiomas have cells that look the most like normal cells. They account for about 8 of 10 meningiomas. Most of these can be cured by surgery, but some grow very close to vital structures in the brain or cranial nerves and cannot be cured by surgery alone.
- Grade II (Atypical or Invasive) meningiomas usually have cells that look slightly more abnormal. They make up about 15% to 20% of meningiomas. They can grow directly into nearby brain tissue and bone and are more likely to come back (recur) after surgery.
- Grade III (Anaplastic or Malignant) meningiomas have cells that look the most abnormal. They make up only about 1% to 3% of meningiomas. They tend to grow quickly, can grow into nearby brain tissue and bone, and are the most likely to come back after treatment. Some may even spread to other parts of the body.
The meninges
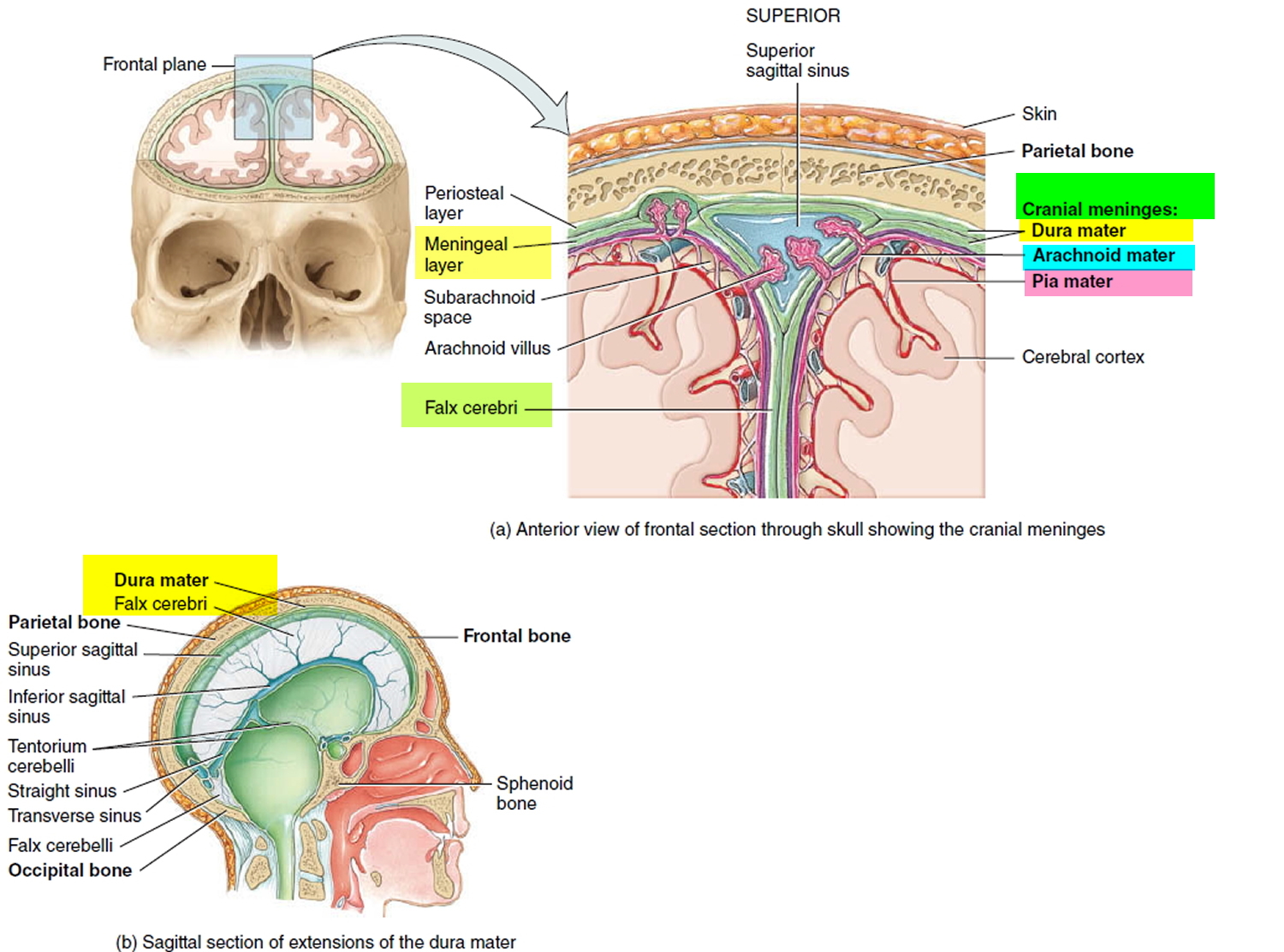
The meninges are three protective, connective tissue coverings that encircle the spinal cord and brain. From superficial to deep they are the (1) Dura mater, (2) Arachnoid mater, and (3) Pia mater.
The spinal meninges surround the spinal cord and are continuous with the cranial meninges, which encircle the brain. All three spinal meninges cover the spinal nerves up to the point where they exit the spinal column through the intervertebral foramina. The spinal cord is also protected by a cushion of fat and connective tissue located in the epidural space, a space between the dura mater and the wall of the vertebral canal.
Following is a description of each meningeal layer.
1. Dura mater
The most superficial of the three spinal meninges is a thick strong layer composed of dense irregular connective tissue. The dura mater forms a sac from the level of the foramen magnum in the occipital bone, where it is continuous with the meningeal dura mater of the brain, to the second sacral vertebra. The dura mater is also continuous with the epineurium, the outer covering of spinal and cranial nerves.
2. Arachnoid mater
This layer, the middle of the meningeal membranes, is a thin, avascular covering comprised of cells and thin, loosely arranged collagen and elastic fibers. It is called the arachnoid mater because of its spider’s web arrangement of delicate collagen fibers and some elastic fibers. It is deep to the dura mater and is continuous through the foramen magnum with the arachnoid mater of the brain. Between the dura mater and the arachnoid mater is a thin subdural space, which contains interstitial fluid.
3. Pia mater
This innermost meninx is a thin transparent connective tissue layer that adheres to the surface of the spinal cord and brain. It consists of thin squamous to cuboidal cells within interlacing bundles of collagen fibers and some fine elastic fibers. Within the pia mater are many blood vessels that supply oxygen and nutrients to the spinal cord. Triangular-shaped membranous extensions of the pia mater suspend the spinal cord in the middle of its dural sheath. These extensions, called denticulate ligaments, are thickenings of the pia mater. They project laterally and fuse with the arachnoid mater and inner surface of the dura mater between the anterior and posterior nerve roots of spinal nerves on either side. Extending along the entire length of the spinal cord, the denticulate ligaments protect the spinal cord against sudden displacement that could result in shock. Between the arachnoid mater and pia mater is a space, the subarachnoid space, which contains shock-absorbing cerebrospinal fluid.
Figure 1. Meninges – spinal cord
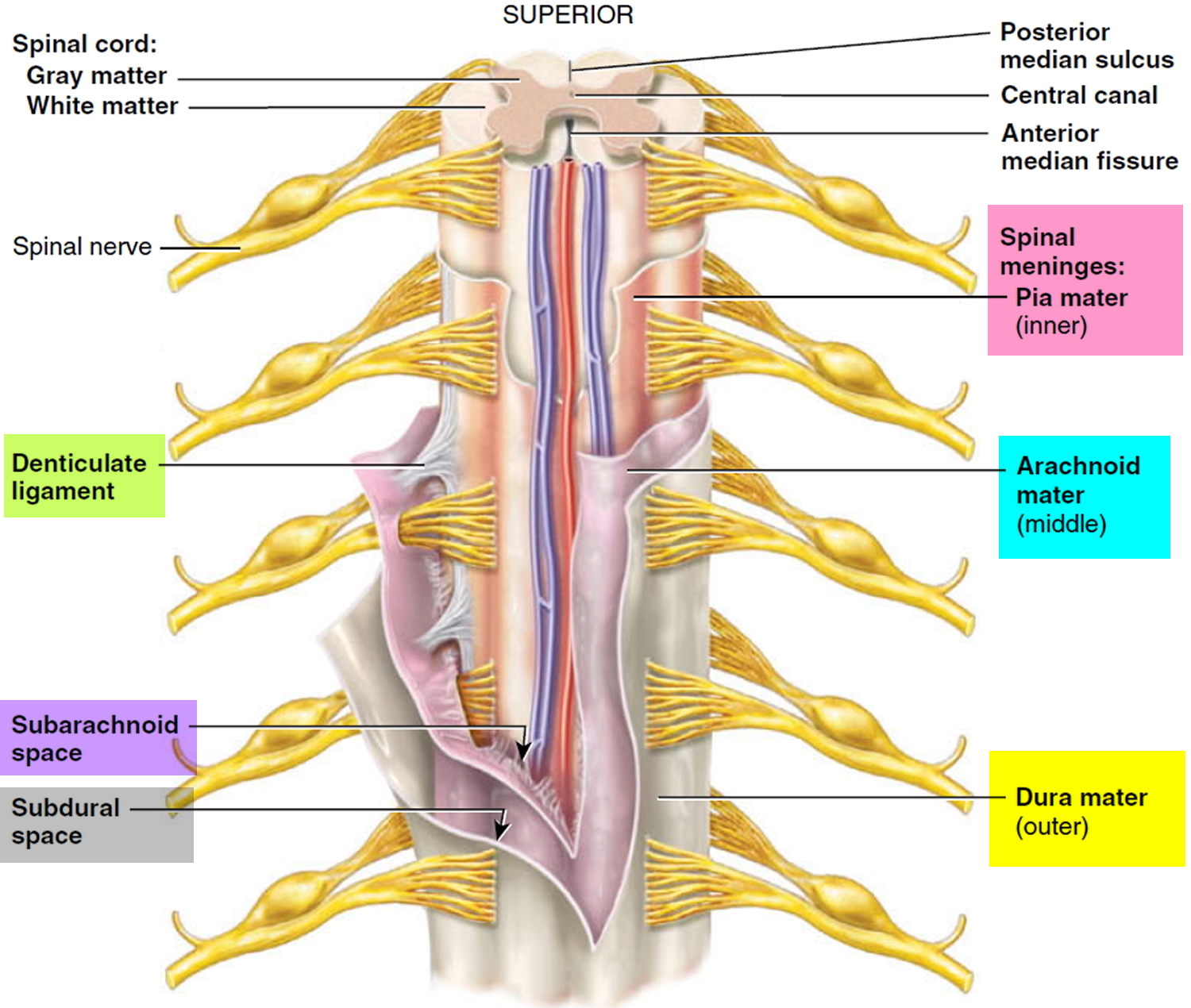
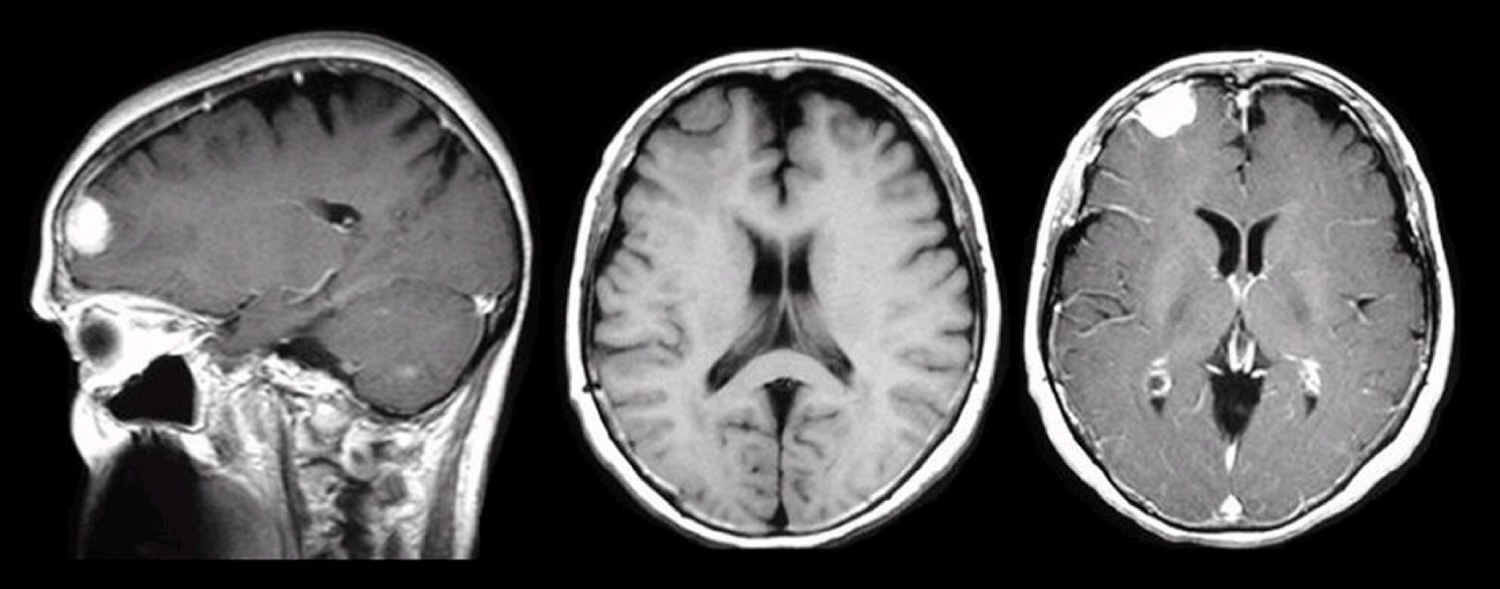
Figure 2. Meninges – brain
Meningioma brain
Meningioma of the brain is a slow-growing tumor of the meninges of the brain.
The meninges are protective membranes which cover the brain. They are in 2 layers; 1 layer is applied closely to the brain and the other layer applied to the skull. The space between the 2 membranes is filled with cerebro-spinal fluid (CSF).
Meningioma brain tumors are relatively uncommon. More than 90% of meningiomas arise within the cranial fossa and occurs with highest incidence in patients aged 40 to 70 years with sex incidence being 3:1 female to males, except when the tumor occurs in children where the sex incidence is approximately equal. Meningiomas tend to increase in size during pregnancy.
The only proven risk factor in the development of meningioma is exposure to ionizing radiation – with tumors commonly developing following a 10 to 20 year lag time from exposure. Patients with neurofibromatosis type 2 (genetic defect on chromosome 22) are at an increased risk of developing meningioma.
Meningioma brain tumor spreads by local invasion and erosion of surrounding bony structures through pressure effects. Meningioma brain tumors are very rarely malignant but occasionally meningioma brain tumors may show a tendency to recur.
The much rarer aggressive form of meningioma can invade adjacent bone structures and very rarely the brain. General investigations may show erosion of bone on a plain skull xray.
Meningioma brain treatment
The prime treatments of meningioma are surgical (this is usually curative) and radiotherapy.
Corticosteroids and antiepileptic drugs are given pre- and post-operatively.
Chemotherapy does not have a significant role.
Improvement in symptoms is an important measurement. Specific monitoring may be by serial imaging of the brain, e.g. with CT scans or MRI.
The symptoms that may require attention are headache which can be treated with standard analgesics. Headaches should be considered as a visceral pain.
Problems with function can be assisted greatly by physiotherapists and occupational therapists.
A variety of equipment is available for the neurologically impaired to make life a little easier. Talk to your doctor about whether it is advisable to drive.
Meningioma spinal cord
Meningioma of the spinal cord is a slow-growing tumor of the meninges of the spinal cord. Meningioma of the spinal cord is rare with less than 1.5 per 100,000 primary spinal cord tumors and of these only approximately 1/4 are meningiomas. More than 90% of meningiomas arise within the cranial fossa (see above description – meningioma of the brain) and occurs with highest incidence in patients aged 40 to 70 years with sex incidence being 3:1 female to males, except when the tumor occurs in children where the sex incidence is approximately equal. Meningiomas tend to increase in size during pregnancy.
The spinal cord forms part of the central nervous system. It is a cylindrical continuation of the brainstem, commencing from the medulla (at the level of the foramen magnum at the base of the skull) and extending to the conus medullaris at the level of the L2 vertebra. It is located within the vertebral canal – the bony tube formed by the vertebral foramina. Below the level of L2 the remaining contents of the spinal canal are known as the cauda equina – the bundle of nerve rootlets in the subarachnoid space. Within the vertebral canal run the spinal cord, the spinal meninges, the cerebrospinal fluid, associated vessels and loose connective and fatty tissue. The spinal meninges – the dura, arachnoid and pia mater – are membranes surrounding and supporting the spinal cord.
Arising from the spinal cord are 31 pairs of spinal nerves that are the neural connections between the peripheries and the central nervous system. They attach to the spinal cord through ventral and dorsal roots and have both afferent and efferent properties. That is, the spinal cord acts as the main pathway for communication between the brain and the rest of the body.
Tumors of the spinal cord can be either primary or metastatic. The vast majority of spinal cord tumors are metastatic deposits from other primary sites. Tumors of the spinal cord can be divided into three groups, based on the anatomical location of the tumor mass. Firstly, they are divided by their relationship to the spinal meninges, with tumors being classified as intradural or extradural. Furthermore, intradural tumors can be subdivided into those arising within the substance of the spinal cord itself – intramedullary tumors – or those arising in the subarachnoid space (extramedullary).
Extradural tumors most commonly represent metastases and usually arise within the vertebral bodies. These tumors most commonly cause spinal compression through extrinsic mass effect but can on occasion do so through intradural invasion. Symptoms from these tumors tend to be the slowly progressing features of spinal cord compression with initial predominantly motor loss followed by progressive sphincter dysfunction and ascending sensory loss. Extradural tumors represent the vast majority of spinal cord tumors.
Intradural extramedullary tumors tend to be nerve sheath tumors (neurofibromas) or meningiomas. They commonly present with nerve root involvement consisting of pain and progressive dysfunction due to spinal cord compression from the expanding tumor mass.
Intramedullary tumours usually represent gliomas – ependymomas or astrocytomas – but metastatic deposits within the spinal cord itself are increasingly recognised. These tumours result in a diffuse swelling of the spinal cord, often over several segments, characterized by loss of local function, pain and eventual loss of spinal cord function below the level of the lesion. A cyst may form in the spinal medulla, giving rise to a clinical picture of syringomyelia (predominant loss of spinothalamic function – pain and temperature sensation – and blunted reflexes at the level of the lesion). Sacral sparing is a very late feature of intramedullary tumors but is pathognomonic.
The only proven risk factor in the development of meningioma is exposure to ionizing radiation – with tumors commonly developing following a 10 to 20 year lag time from exposure. Patients with neurofibromatosis type 2 (genetic defect on chromosome 22) are at increased risk of developing meningioma.
This type of tumor spreads by local invasion and erosion of surrounding bony structures through pressure effects. Meningiomas are very rarely malignant but occasionally tumors may show a tendency to recur.
Meningioma of spinal cord treatment
Initial treatment of patients with suspected spinal cord compression is with corticosteroids.
Surgical resection is the mainstay of treatment in meningiomas of the spinal cord and the degree to which a tumor can be resected has great bearing on prognosis. Unfortunately, the recovery of previously lost neurological function post-operatively is unlikely.
Where complete resection is not possible, post-operative radiotherapy is limited to the area of the tumor and the margin of potential spread is advocated in preference to more radical surgical approaches which are associated with significant increases in post-operative morbidity without any clear survival benefit. Tumor recurrence is usually treated with further surgery.
Improvement in symptoms is an important measurement. Specific monitoring may be done by serial neurological examination and imaging of the spinal cord.
The symptoms that may require attention are those resulting from the neurological deficits associated with the tumor and the neurogenic pain from compressed nerve tissue. Patients with significant neurological deficits are best managed by a specialized neurological team, using a multidisciplinary approach including physiotherapy, occupational therapy, nursing and medical practitioners.
Meningioma survival rate
Benign meningiomas are associated with a very good survival prognosis with approximately 100% 5 year survival. Morbidity relates to the location of the tumor and the degree of neurological dysfunction at diagnosis. Malignant meningiomas have a poor prognosis with median survival of between one and three years even with treatment.
Meningioma complications
A meningioma and its treatment, typically surgery and radiation therapy, can cause long-term complications, including:
- Difficulty concentrating
- Memory loss
- Personality changes
- Seizures
Your doctor can treat some complications and refer you to specialists to help you cope with other complications.
Meningioma symptoms
Signs and symptoms of a meningioma typically begin gradually and may be very subtle at first. Depending on where in the brain or, rarely, spine the tumor is situated, signs and symptoms may include:
- Changes in vision, such as seeing double or blurriness
- Headaches that worsen with time
- Hearing loss or ringing in the ears
- Memory loss
- Loss of smell
- Seizures
- Weakness in your arms or legs
Make an appointment to see your doctor if you have persistent signs and symptoms that concern you, such as headaches that worsen over time.
In many cases, because meningiomas do not cause any noticeable signs or symptoms, they are only discovered as a result of imaging scans done for reasons that turn out to be unrelated to the tumor, such as a head injury, stroke or headaches.
Meningioma causes
It isn’t clear what causes a meningioma. Doctors know that something alters some cells in your meninges to make them multiply out of control, leading to a meningioma tumor.
Whether this occurs because of genes you inherit, hormones (which may be related to the more frequent occurrence in women), the rare instance of prior exposure to radiation or other factors remains largely unknown. There is no solid evidence to support the assertion that meningiomas occur in association with cellphone use.
Risk factors for meningioma
Risk factors for a meningioma include:
- Radiation treatment. Radiation therapy that involves radiation to the head may increase the risk of a meningioma.
- Female hormones. Meningiomas are more common in women, leading doctors to believe that female hormones may play a role. Some studies have also suggested a link between breast cancer and meningioma risk related to the role of hormones.
- An inherited nervous system disorder. The rare disorder neurofibromatosis 2 increases the risk of meningioma and other brain tumors.
- Obesity. A high BMI (body mass index) is an established risk factor for many types of cancers, and a higher prevalence of meningiomas among obese persons has been observed in several large studies. But the relationship between obesity and meningiomas is not clear.
Meningioma diagnosis
A meningioma can be difficult to diagnose because the tumor is often slow growing. Symptoms of a meningioma may also be subtle and mistaken for other health conditions or written off as normal signs of aging.
If your primary care provider suspects a meningioma, you may be referred to a doctor who specializes in neurological conditions (neurologist).
To diagnose a meningioma, a neurologist will conduct a thorough neurological exam followed by an imaging test, such as:
- Computerized tomography (CT) scan. CT scans take X-rays that create cross-sectional images of a full picture of your brain. Sometimes an iodine-based dye is used to augment the picture.
- Magnetic resonance imaging (MRI). With this imaging study, a magnetic field and radio waves are used to create cross-sectional images of the structures within your brain. MRI scans provide a more-detailed picture of the brain and meningiomas.
In some cases, examination of a sample of the tumor (biopsy) may be needed to rule out other types of tumors and confirm a meningioma diagnosis.
Meningioma treatment
The treatment you receive for a meningioma depends on many factors, including:
- The size and location of your meningioma
- The rate of growth or aggressiveness of the tumor
- Your age and overall health
- Your goals for treatment
Wait-and-see approach
Immediate treatment isn’t necessary for everyone with a meningioma. A small, slow-growing meningioma that isn’t causing signs or symptoms may not require treatment.
If the plan is not to undergo treatment for your meningioma, you’ll likely have brain scans periodically to evaluate your meningioma and look for signs that it’s growing.
If your doctor determines your meningioma is growing and needs to be treated, you have several treatment options.
Meningioma surgery
If your meningioma causes signs and symptoms or shows signs that it’s growing, your doctor may recommend surgery.
Surgeons work to remove the meningioma completely. But because a meningioma may occur near many delicate structures in the brain or spinal cord, it isn’t always possible to remove the entire tumor. In those cases, surgeons remove as much of the meningioma as possible.
The type of treatment, if any, you need after surgery depends on several factors.
- If no visible tumor remains, then no further treatment may be necessary. However, you will have periodic follow-up scans.
- If the tumor is benign and only a small piece remained, then your doctor may recommend periodic follow-up scans only. In some cases, small leftover tumors may be treated with a form of radiation treatment called stereotactic radiosurgery.
- If the tumor is atypical or malignant, you’ll likely need radiation.
Surgery may pose risks including infection and bleeding. The specific risks of your surgery will depend on where your meningioma is located. For instance, surgery to remove a meningioma that occurs around the optic nerve can lead to vision loss. Ask your surgeon about the specific risks of your surgery.
Radiation therapy
If your meningioma can’t be completely removed surgically, your doctor may recommend radiation therapy following surgery.
The goal of radiation therapy is to destroy any remaining meningioma cells and reduce the chance that your meningioma may recur. Radiation therapy uses a large machine to aim high-powered energy beams at the tumor cells.
Advances in radiation therapy increase the dose of radiation to the meningioma while reducing radiation to healthy tissue. Radiation therapy options for meningiomas include:
- Stereotactic radiosurgery is a type of radiation treatment that aims several beams of powerful radiation at a precise point. Contrary to its name, radiosurgery doesn’t involve scalpels or incisions. Radiosurgery typically is done in an outpatient setting in a few hours. Radiosurgery may be an option for people with meningiomas that can’t be removed with conventional surgery or for meningiomas that recur despite treatment.
- Fractionated stereotactic radiotherapy delivers radiation in small fractions over time, such as one treatment a day for 30 days. This approach may be used for tumors too large for radiosurgery or those in an area that can’t tolerate the high intensity of radiosurgery — such as near the optic nerve.
- Intensity-modulated radiation therapy uses computer software to modify the intensity of radiation directed at the meningioma site. This may be used for meningiomas located near sensitive brain structures or those with a complex shape.
- Proton beam radiation uses radioactive protons precisely targeted at the tumor, reducing damage to the surrounding tissue.
Chemotherapy
Drug therapy (chemotherapy) is rarely used to treat meningiomas, but it may be used in cases that don’t respond to surgery and radiation.
There isn’t a widely accepted chemotherapy approach to the treatment of meningiomas, but researchers are currently studying molecularly targeted approaches.
Alternative medicine
Alternative medicine treatments can’t treat meningiomas, but some may help provide relief from treatment side effects or help you cope with the stress of having a meningioma.
Alternative medicine therapies that may be helpful include:
- Acupuncture
- Hypnosis
- Massage
- Meditation
- Music therapy
- Relaxation exercises
Discuss options with your doctor.
Coping and support
Being diagnosed with a meningioma can be overwhelming. Coping with a diagnosis of cancer can be difficult, both practically and emotionally. As you come to terms with your diagnosis, your life can be turned upside down with visits to doctors and surgeons as you prepare for your treatment.
Being well informed about your cancer and its treatment can make it easier to make decisions and cope with what happens.
To help you cope, try to:
- Learn everything you can about meningiomas. Ask your health care team where you can get more information about meningiomas and your treatment options. Visit your local library and ask a librarian to help you track down reliable resources for more information, including online sources. Write down your questions so that you’ll remember to ask them at your next appointment with your doctor. The more you know about your condition, the better prepared you’ll be to make decisions about your treatment.
- Build a support network. Having friends and family supporting you can be valuable. You may find it helps to have someone to talk to about your emotions. Other people who may provide support include social workers and psychologists — ask your doctor for a referral if you feel that you need someone else to talk to. Talk with your pastor, rabbi or other spiritual leader. Other people with meningiomas can offer a unique perspective, so consider joining a support group — whether it’s in your community or online. Ask your health care team about brain tumor or meningioma support groups in your area, or contact the American Brain Tumor Association.
- Take care of yourself. Try to stay healthy during your treatment for a meningioma by taking care of yourself. Eat a diet rich in fruits and vegetables, and get moderate exercise daily if your doctor allows it. Get enough sleep so that you wake feeling rested. Reduce stress in your life by focusing on what’s important to you. These measures won’t cure your meningioma, but they may help you feel better as you recover from surgery or help you to cope during radiation therapy.





{kind=link}