Contents
What is microcephaly
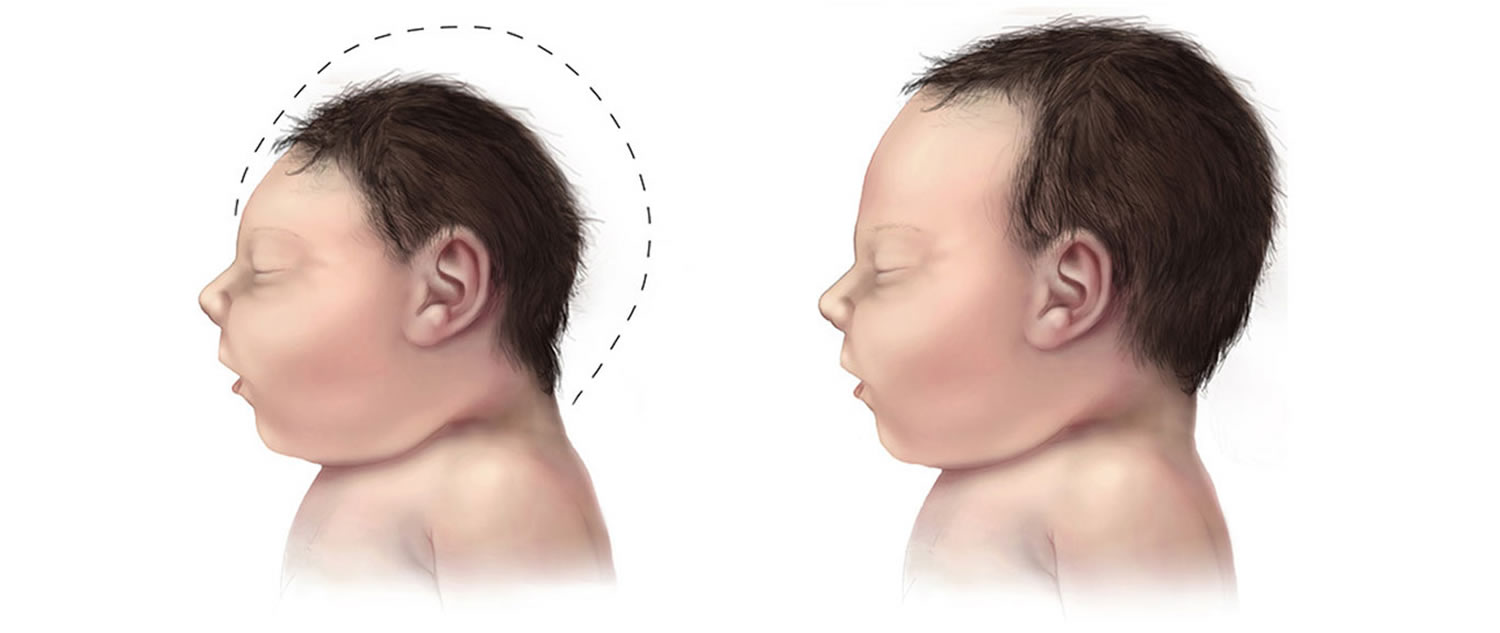
Microcephaly is a birth defect where a baby’s head is smaller than expected when compared to babies of the same sex and age. Babies with microcephaly often have smaller brains that might not have developed properly. Microcephaly is not a common condition. The Unites States birth defects tracking systems have estimated that microcephaly ranges from 2 babies per 10,000 live births to about 12 babies per 10,000 live births 1.
During pregnancy, a baby’s head grows because the baby’s brain grows. Microcephaly can occur because a baby’s brain has not developed properly during pregnancy or has stopped growing after birth, which results in a smaller head size. Microcephaly can be an isolated condition, meaning that it can occur with no other major birth defects, or it can occur in combination with other major birth defects.
Birth defects are health conditions that are present at birth. Birth defects change the shape or function of one or more parts of the body. They can cause problems in overall health, how the body develops or in how the body works. Some babies have microcephaly along with other birth defects.
Figure 1. Microcephaly
 There are many different causes for this problem, including:
There are many different causes for this problem, including:
- infections during pregnancy, such as rubella, cytomegalovirus or the Zika virus
- exposure to substances that might harm the baby, such as alcohol, drugs or chemicals
- genetic problems, such as Down syndrome
- malnutrition during pregnancy
- problems with blood supply to the baby’s brain during pregnancy.
Microcephaly can affect a baby in different ways, including:
- delayed development or speech
- intellectual disability
- problems with coordination or balance
- seizures
- agitation or aggression
- problems with hearing or vision.
Microcephaly is a rare condition associated with mild to severe developmental delays and disability. Babies can be born with microcephaly or it can develop in their first few years.
Microcephaly is a lifelong condition. There is no known cure or standard treatment for microcephaly. There are early childhood intervention services and support available to help.
Mild microcephaly
Babies with mild microcephaly often don’t have problems other than small head size.
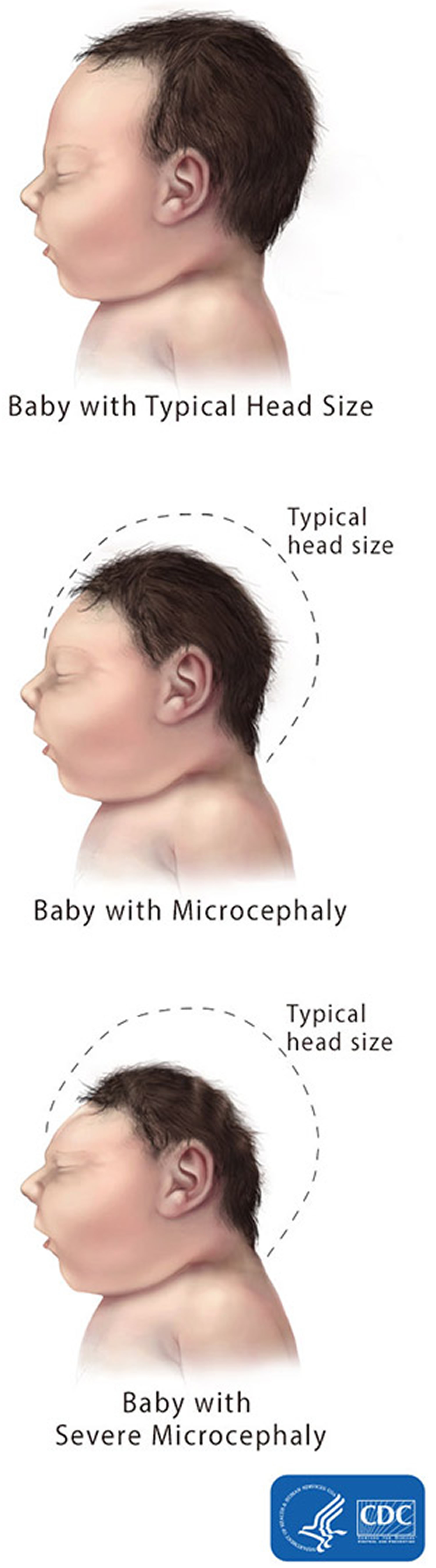
Severe microcephaly
Severe microcephaly is a more serious, extreme form of microcephaly where a baby’s head is much smaller than expected. Severe microcephaly can happen because a baby’s brain has not developed properly during pregnancy, or the brain started to develop correctly and then was damaged at some point during pregnancy.
A baby with severe microcephaly may have more serious health problems than babies with mild microcephaly.
Microcephaly baby
Microcephaly is a birth defect in which a baby’s head is smaller than expected, compared to babies of the same sex and age.
Some babies with microcephaly have no health complications other than having a small head and being short. But some babies with microcephaly may have lifelong health problems, including:
- Cerebral palsy. This is a group of conditions that affects the parts of the brain that control muscles. This can cause problems with movement, posture (standing up straight) and balance.
- Congenital Zika syndrome. This is a group of health conditions present at birth associated with Zika infection during pregnancy. Congenital Zika syndrome includes birth defects (like microcephaly) and other health and development problems. Zika Care Connect is a website that offers information about caring for babies and children with congenital Zika syndrome. It also offers a database of providers who care for these babies and children. You can search the database by things like location, kind of provider, the language the provider speaks and the insurance the provider takes.
- Dwarfism or short height. Dwarfism (being a “little person”) is a condition in which a person is very short, less than 4 feet, 10 inches tall as an adult.
- Face deformities
- Feeding problems, like trouble swallowing
- Problems with movement and balance
- Problems with hearing (hearing loss) or vision
- Hyperactivity (being very active)
- Seizures
- Intellectual and developmental disabilities. These are problems with how the brain works that can cause a person to have trouble or delays in physical development, learning, communicating, taking care of himself, decreased ability to learn and function in daily life or getting along with others. Some babies with microcephaly don’t reach developmental milestones when expected. A developmental milestone is a skill (like sitting, standing, and walking) or activity that most children can do at a certain age. Milestones include sitting, walking, talking, having social skills and having thinking skills.
These problems can range from mild to severe and are often lifelong. Because the baby’s brain is small and underdeveloped, babies with severe microcephaly can have more of these problems, or have more difficulty with them, than babies with milder microcephaly. Severe microcephaly also can be life-threatening. Because it is difficult to predict at birth what problems a baby will have from microcephaly, babies with microcephaly often need close follow-up through regular check-ups with a healthcare provider to monitor their growth and development.
Microcephaly complications
Some children with microcephaly are of normal intelligence and development, even though their heads will always be small for their age and sex. But depending on the cause and severity of the microcephaly, complications may include:
- Developmental delays, such as in speech and movement
- Difficulties with coordination and balance
- Dwarfism or short stature
- Facial distortions
- Hyperactivity
- Intellectual disabilities
- Seizures.
Coping and support
When you learn your child has microcephaly, your emotions might include anger, fear, worry, sorrow and guilt. You may not know what to expect, and you may worry about your child’s future. The best antidote for fear and worry is information and support.
Prepare yourself:
- Find a team of trusted professionals. You’ll need to make important decisions about your child’s education and treatment. Create a team of doctors, teachers and therapists and other professionals who can help you evaluate the resources in your area and explain state and federal programs for children with disabilities. Medical specialties your child might require include pediatrics and developmental pediatrics, infectious diseases, neurology, ophthalmology, genetics and psychology.
- Seek other families who are dealing with the same issues. Your community might have support groups for parents of children with developmental disabilities. You might also find online support groups.
Microcephaly prognosis
Some children with microcephaly will have normal intelligence and a head that will grow bigger, but they may track below the normal growth curves for head circumference. Some children may have only mild disability, while those with more severe cases may face significant learning disabilities, cognitive delays, or develop other neurological disorders. Many, if not most, cases if Zika microcephaly will be very severe, possibly requiring lifelong intensive care.
Microcephaly causes
What causes microcephaly
The causes of microcephaly in most babies are unknown. During pregnancy, your baby’s head grows as her brain grows. Microcephaly can happen when a baby’s brain doesn’t develop properly during pregnancy or stops growing after birth.
Some babies have microcephaly because of changes in their genes.
Scientists know that these things may cause microcephaly in some babies:
Genes and chromosomes
- Changes in genes (also called mutations) that affect the brain’s growth and development. This is the most common cause of microcephaly. Genes are part of your body’s cells. They store instructions for the way your body grows and works. Genes are passed from parents to children.
- Chromosomal conditions, like Down syndrome. Chromosomes are the structures that hold genes. Babies with chromosomal conditions have a problem in one or more of their chromosomes.
- Untreated maternal phenylketonuria (PKU). This is a condition passed through genes in which a woman’s body can’t break down an amino acid called phenylalanine. Most women with phenylketonuria (PKU) can have healthy babies if they follow a special meal plan that’s low in phenylalanine.
If your baby’s microcephaly is caused by a gene change or chromosomal condition, you may want to see a genetic counselor. This is a person who is trained to help you understand about genes, birth defects and other medical conditions that run in families, and how they can affect your health and your baby’s health.
Other causes of microcephaly, including severe microcephaly, can include the following exposures during pregnancy:
- Being exposed to certain infections in the womb, including Zika virus, chickenpox (also called varicella), rubella (also called German measles), toxoplasmosis or cytomegalovirus
- Being exposed to harmful substances, such as alcohol or certain drugs or chemicals in the womb
- Severe malnutrition, meaning a lack of nutrients or not getting enough food
- Interruption of the blood supply to the baby’s brain during development (cerebral anoxia). Certain complications of pregnancy or delivery can impair oxygen delivery to the fetal brain.
Brain problems
- Cerebral anoxia. This is when a baby’s brain doesn’t get enough oxygen. Complications during pregnancy, birth or after birth can cause problems with oxygen flow to a baby’s brain.
- Craniosynostosis. This is a birth defect in which the joints (also called sutures) between the bones in a baby’s skull fuse together too early, before the brain stops growing. This can cause problems with brain development. Treating craniosynostosis usually means your infant needs surgery to separate the fused bones. If there are no underlying problems in the brain, this surgery allows the brain adequate space to grow and develop.
- Traumatic brain injury. This happens when a head injury causes brain damage.
Metabolism or nutrition problems
- Metabolic disorders. These are health conditions that affect a body’s metabolism. Metabolism is the way your body changes food into the energy it needs to use oxygen, digest food and grow.
- Severe malnutrition in the womb. This means a baby doesn’t get enough food or nutrients during pregnancy.
Microcephaly prevention
You can’t always prevent microcephaly in your baby. But there are things you can do to help reduce your baby’s chances of having it. Here’s how:
- Don’t drink alcohol. Alcohol includes beer, wine and liquor.
- Don’t use street drugs or abuse prescription drugs. Tell your provider if you need help to quit using drugs.
- Protect yourself from harmful chemicals. Wear gloves or a face mask if you have to use them. Open a window or door to let clean air in.
- If you have phenylketonuria (PKU), get treatment and follow your meal plan.
- Protect yourself from infections.
Here’s what you can do to help protect yourself from infections before and during pregnancy:
- Protect yourself from Zika. Don’t travel to a Zika-affected area unless absolutely necessary. Protect yourself from mosquito bites. If your male or female partner may be infected with Zika, don’t have sex. If you do have sex, use a condom. If you work in a health care setting, follow safety rules to protect yourself from exposure.
- Talk to your provider to make sure your vaccinations are up to date.
- Have safe sex to protect you against sexually transmitted diseases (also called STDs) and other infections, including Zika. Safe sex means using a condom if you have sex with more than one partner. If your male or female partner may be infected with Zika, use a condom every time you have sex or don’t have sex at all.
- Wash your hands often, especially after using the bathroom, sneezing or coughing, changing a diaper or preparing food.
- Don’t eat raw or undercooked food, including lunch meats. Cook meat, chicken and fish until done. Wash food before you cook or eat it.
- Don’t touch cat poop or change a cat’s litter box to help protect you from toxoplasmosis.
- Get regular dental checkups to help prevent gum infections.
Microcephaly symptoms
After birth, a baby with microcephaly may have these signs and symptoms:
- Small head size
- Failure to thrive (slow weight gain and growth)
- High-pitched crying
- Little appetite or problems with feeding
- Muscle spasms
To diagnose microcephaly after birth, your baby’s provider measures your baby’s head circumference during a physical exam. Head circumference is the distance around your baby’s head. Your baby’s provider then compares your baby’s measurement to that of other babies of the same sex and age.
Microcephaly diagnosis
You may find out your baby has microcephaly during pregnancy or after he’s born. During pregnancy, your health care provider may diagnose microcephaly using ultrasound late in the second trimester or early in the third trimester. Ultrasound is a prenatal test that uses sound waves and a computer screen to show a picture of your baby inside the womb.
Microcephaly during pregnancy
If you are pregnant, your doctor or midwife will discuss the health of both yourself and your baby at your antenatal visits. They might not talk specifically about microcephaly, but they will have good ideas about how to increase your chances of having a healthy baby.
During your pregnancy, you are likely to have an ultrasound and other tests to check on your baby’s health. If there are any signs of a problem, your doctor will discuss this with you. Microcephaly can generally only be diagnosed during an ultrasound late in the 2nd trimester or early in the third trimester because a smaller than expected head size will not be obvious before this time.
If your baby is suspected of having microcephaly, further tests will be performed to identify the cause. Your doctor, obstetrician, midwife or a genetic counselor will be able to answer any questions that you might have, including how it might impact your pregnancy and what your options are. You can also ask about how this might affect your child in the future.
Diagnosis of microcephaly after birth
A diagnosis of microcephaly is made simply by measuring the distance around a newborn baby’s head, also called the head circumference, during a physical exam. Your healthcare provider then compares this measurement to population standards by sex and age. Microcephaly is defined as a head circumference measurement that is smaller than a certain value for babies of the same age and sex. This measurement value for microcephaly is usually less than 2 standard deviations (SDs) below the average. The measurement value also may be designated as less than the 3rd percentile. This means the baby’s head is extremely small compared to babies of the same age and sex.
- Head circumference growth charts for newborns, infants, and children up to age 20 years in the United States can be found on CDC’s growth charts website here: https://www.cdc.gov/growthcharts/clinical_charts.htm
Microcephaly can be determined by measuring head circumference after birth. Although head circumference measurements may be influenced by molding and other factors related to delivery, the measurements should be taken on the first day of life because commonly-used birth head circumference reference charts by age and sex are based on measurements taken before 24 hours of age. The most important factor is that the head circumference is carefully measured and documented. If measurement within the first 24 hours of life is not done, the head circumference should be measured as soon as possible after birth.
It can be more difficult to work out why the baby’s head is smaller than usual, and that might need a number of tests.
If your healthcare provider suspects the baby has microcephaly, he or she can request one or more tests to help confirm the diagnosis. For example, special tests like like magnetic resonance imaging can provide critical information on the structure of the baby’s brain that can help determine if the newborn baby had an infection during pregnancy. They also can help the healthcare provider look for other problems that might be present.
Your healthcare provider also may do these tests:
- Blood tests
- Computed tomography scan (also called CT or CAT scan). CT scan uses special X-ray equipment and powerful computers to make pictures of the inside of your baby’s brain.
- Magnetic resonance imaging (also called MRI). MRI is a medical test that makes a detailed picture of the inside of your body.
Microcephaly treatment
There’s no cure for microcephaly. Because microcephaly can range from mild to severe, treatment options can range as well. Treatment options depend on how severe your baby’s condition is. Babies with mild microcephaly often don’t have other health problems besides small head size, but they still need regular check-ups so their health care provider can monitor their growth and development.
Babies with severe microcephaly may need special care and treatment. Babies with craniosynostosis may need to have surgery to help separate the fused bones in their heads and give the skull the ability to expand as the brain grows and develops. Some babies need to take medicines to treat seizures or other health problems. If your baby has microcephaly and has developmental delays, he/she should see a child neurologist. This is a doctor who treats the brain, spine and nerves in children.
Developmental services early in life will often help babies with microcephaly to improve and maximize their physical and intellectual abilities. These services, known as early intervention, can include speech, occupational, and physical therapies. Sometimes medications also are needed to treat seizures or other symptoms. Getting early intervention services as soon as possible can help improve your child’s development. These services can help children from birth through 3 years old learn important skills. Services include therapy to help a child talk, walk, learn self-help skills and interact with others.
Overview of Early Intervention
Early intervention is a system of services that helps babies and toddlers with developmental delays or disabilities. Early intervention is available in every state and territory of the United States. Early intervention focuses on helping eligible babies and toddlers learn the basic and brand-new skills that typically develop during the first three years of life, such as:
- physical (reaching, rolling, crawling, and walking);
- cognitive (thinking, learning, solving problems);
- communication (talking, listening, understanding);
- social/emotional (playing, feeling secure and happy); and
- self-help (eating, dressing).
Examples of early intervention services
If an infant or toddler has a disability or a developmental delay in one or more of these developmental areas, that child will likely be eligible for early intervention services. Those services will be tailored to meet the child’s individual needs and may include:
- Assistive technology (devices a child might need)
- Audiology or hearing services
- Speech and language services
- Counseling and training for a family
- Medical services
- Nursing services
- Nutrition services
- Occupational therapy
- Physical therapy
- Psychological services
Services may also be provided to address the needs and priorities of the child’s family. Family-directed services are meant to help family members understand the special needs of their child and how to enhance his or her development.
Who’s eligible for early intervention?
Early intervention is intended for infants and toddlers who have a developmental delay or disability. Eligibility is determined by evaluating the child (with parents’ consent) to see if the little one does, in fact, have a delay in development or a disability. Eligible children can receive early intervention services from birth through the third birthday (and sometimes beyond).
- For some children, from birth. Sometimes it is known from the moment a child is born that early intervention services will be essential in helping the child grow and develop. Often this is so for children who are diagnosed at birth with a specific condition or who experience significant prematurity, very low birth weight, illness, or surgery soon after being born. Even before heading home from the hospital, this child’s parents may be given a referral to their local early intervention office.
- For others, because of delays in development. Some children have a relatively routine entry into the world, but may develop more slowly than others, experience set backs, or develop in ways that seem very different from other children. For these children, a visit with a developmental pediatrician and a thorough evaluation may lead to an early intervention referral.
Parents DON’T have to wait for a referral to early intervention. If you’re concerned about your child’s development, you may contact your local program directly and ask to have your child evaluated. That evaluation is provided free of charge. They are funded by state and federal monies.
If you’re not sure how to locate the early intervention program in your community, here is how to get in touch with your community’s early intervention program:
Try any of these suggestions:
- Contact the Pediatrics branch in a local hospital and ask where you should call to find out about early intervention services in your area.
- Ask your pediatrician for a referral to the local early intervention system.
- Visit the Early Childhood Technical Assistance Center (ECTA) early intervention “contacts” page at: http://ectacenter.org/contact/ptccoord.asp
However a child comes to be referred, evaluated, and determined eligible, early intervention services provide vital support so that children with developmental needs can thrive and grow.
It’s important to note that an evaluation of your child won’t be necessary if he or she is automatically eligible due to a diagnosed physical or mental condition that has a high probability of resulting in a developmental delay. Such conditions include but aren’t limited to microcephaly, chromosomal abnormalities; genetic or congenital disorders; sensory impairments; inborn errors of metabolism; disorders reflecting disturbance of the development of the nervous system; congenital infections; severe attachment disorders; and disorders secondary to exposure to toxic substances, including fetal alcohol syndrome. Many states have policies that further specify what conditions automatically qualify an infant or toddler for early intervention (e.g., Down syndrome, Fragile X syndrome).
- National Birth Defects Prevention Network. Major birth defects data from population-based birth defects surveillance programs in the United States, 2006-2010. Birth Defects Research (Part A): Clinical and Molecular Teratology. 2013;97:S1-S172.[↩]





{kind=link}