Contents
What are moles
Moles are common non-cancerous overgrowths of pigment-producing cells called melanocytes (cells that make a substance called melanin, which gives color to skin and eyes). Moles happen when pigment cells in the skin, called melanocytes, grow in clusters. Almost all of us have moles. Moles are not normally present at birth but appear in childhood and early teenage years. By the age of fifteen years, American children have an average of 10 to 40 common moles. A person may develop new moles from time to time, usually until about age 40 1. Early in their life cycle, moles tend to be flat and dark. As the patient ages, moles tend to raise up and lose their color. Late in life, moles may disappear altogether. In older people, moles tend to fade away. Moles are usually found above the waist on areas exposed to the sun. Moles are seldom found on the scalp, breast, or buttocks. Moles have a very small risk of developing into melanoma.
The number of moles that develop in an individual is predominately determined by genetic (inherited) factors and to a lesser extent by sunlight exposure. Childhood and early teenage years are the times when sunlight influences the development of new moles most strongly. In a study of white children in Colorado, the total number of moles increased with both chronic sun exposure and number of sunburns 2.
Moles are usually pink, tan or brown. They can be flat or raised. They are usually round or oval and no larger than a pencil eraser.
The typical mole is a brown spot. But moles come in different colors, shapes and sizes:
- Color and texture. Moles can be brown, tan, black, red, blue or pink. They can be smooth, wrinkled, flat or raised. They may have hair growing from them.
- Shape. Most moles are oval or round.
- Size. Moles are usually less than 1/4 inch (about 6 millimeters) in diameter — the size of a pencil eraser. Rarely, moles present at birth (congenital nevi) can be much bigger, covering wide areas of the face, torso or a limb.
The medical term for a mole is a melanocytic nevus. Nevi are the plural of nevus. A brown or black mole contains the pigment melanin, so may also be called a pigmented nevus. About one out of every ten people has at least one abnormal mole or “atypical mole” that looks different from an ordinary mole. They are called dysplastic nevi. A dysplastic nevus is more likely than ordinary moles to develop into malignant melanoma, a type of skin cancer that starts in pigment cells. A dysplastic nevus is often large (more than 5 millimeters) and have borders that are not easy to see, that is a dysplastic nevus does not have a round or oval shape or a distinct edge. A dysplastic nevus color is usually uneven and can range from pink, tan to dark brown. People who have many dysplastic nevi have a greater chance than others of developing melanoma, a dangerous form of skin cancer. Although, most dysplastic nevi do not turn into melanoma, people with dysplastic nevi should get their skin examined by a doctor 3.
- You should have a health care professional check your moles if they look unusual, grow larger, change in color or outline, or in any other way.
If you have a large number of moles or multiple dysplastic moles, you may need to have regular skin checks. Your dermatologist may photograph your skin so that changes in your moles can be detected at follow-up visits. Since many melanomas arise as new spots (on normal skin), it is necessary to observe all of the skin, not only the moles.
You should self-examine your skin at least every 3 to 4 months for moles that are new, growing or changing and report any significant changes to your doctor or dermatologist. It is important to avoid excessive sun exposure and protect your skin from the sun by wearing tightly woven longer sleeved clothing, broad brimmed hats and sunglasses and applying sunscreens regularly.
See a doctor immediately if you notice a change in a mole!
It’s important to get a new or existing mole checked out if it:
- changes shape or looks uneven
- changes color, gets darker or has more than 2 colors
- starts itching, crusting, flaking or bleeding
- gets larger or more raised from the skin
These changes can happen over weeks or months. They’re sometimes a sign of malignant melanoma, a type of potentially deadly form of skin cancer that is diagnosed in about 70,000 Americans each year.
Melanoma is a form of cancer that begins in melanocytes (cells that make the pigment melanin). It may begin in a mole (skin melanoma), but infrequently can also begin in other pigmented tissues, such as in the eye or the intestines. Melanoma is potentially dangerous because it can spread to nearby tissues and other parts of the body, such as the lung, liver, bone, or brain. The earlier that melanoma is detected and removed, the more likely that treatment will be successful.
Unusual moles that may indicate melanoma
This ABCDE guide can help you determine if a mole or a spot may indicate melanoma or other skin cancers:
- A is for asymmetrical shape. One half is unlike the other half.
- B is for border. Look for moles with irregular, notched or scalloped borders.
- C is for color. Look for growths that have changed color, have many colors or have uneven color.
- D is for diameter. Look for new growth in a mole larger than 1/4 inch (about 6 millimeters).
- E is for evolving. Watch for moles that change in size, shape, color or height, especially if part or all of a mole turns black. Moles may also evolve to develop new signs and symptoms, such as itchiness or bleeding.
Cancerous (malignant) moles vary greatly in appearance. Some may show all of the features listed above. Others may have only one or two.
Congenital nevi are moles present at birth (see Figure 4); acquired nevi develop anytime later. Nevi are made up of a particular type of cell, and the name is used to distinguish them from other, similar appearing fleshy growths.
Surgical excision should be done where cancer is a reasonable concern. Improving cosmetic appearance is another reason for excision, but all surgery leaves some scarring. Smaller nevi can be “shaved off”. Larger ones can be cut out directly and the wound edges sewn together. Much larger nevi may be excised in stages by taking a little more out each time until the entire nevus is removed. This is called “serial excision.” Cutting out very large nevi will leave behind a raw area that is too big to be sewn together and must be covered. This can be done with a split thickness skin graft from some other normal area of the body. The skin-grafted area will have varying degrees of scarring and will usually be thinner and more fragile than normal skin.
There have been several reported cases of melanoma developing underneath a skin graft from nevus cells left behind. Occasionally, thickened scars called keloids may appear. Laser treatment, chemical peels and dermabrasion, also destroy nevus cells before they can be checked for cancer under a microscope. They also leave nevus cells behind and the pigment often seems to reappear.
While it may seem more convenient to shave off or cut out a mole yourself, there are 3 very good reasons a dermatologist should remove it:
- Skin cancer: If the mole contains skin cancer, some of the cancer cells can stay in the skin and even spread.
- Scarring: You can disfigure your skin causing a scar.
- Infection: A dermatologist uses sterile equipment to prevent infection.
Figure 1. Skin structure

Figure 2. Structure and skin cells of the Epidermis
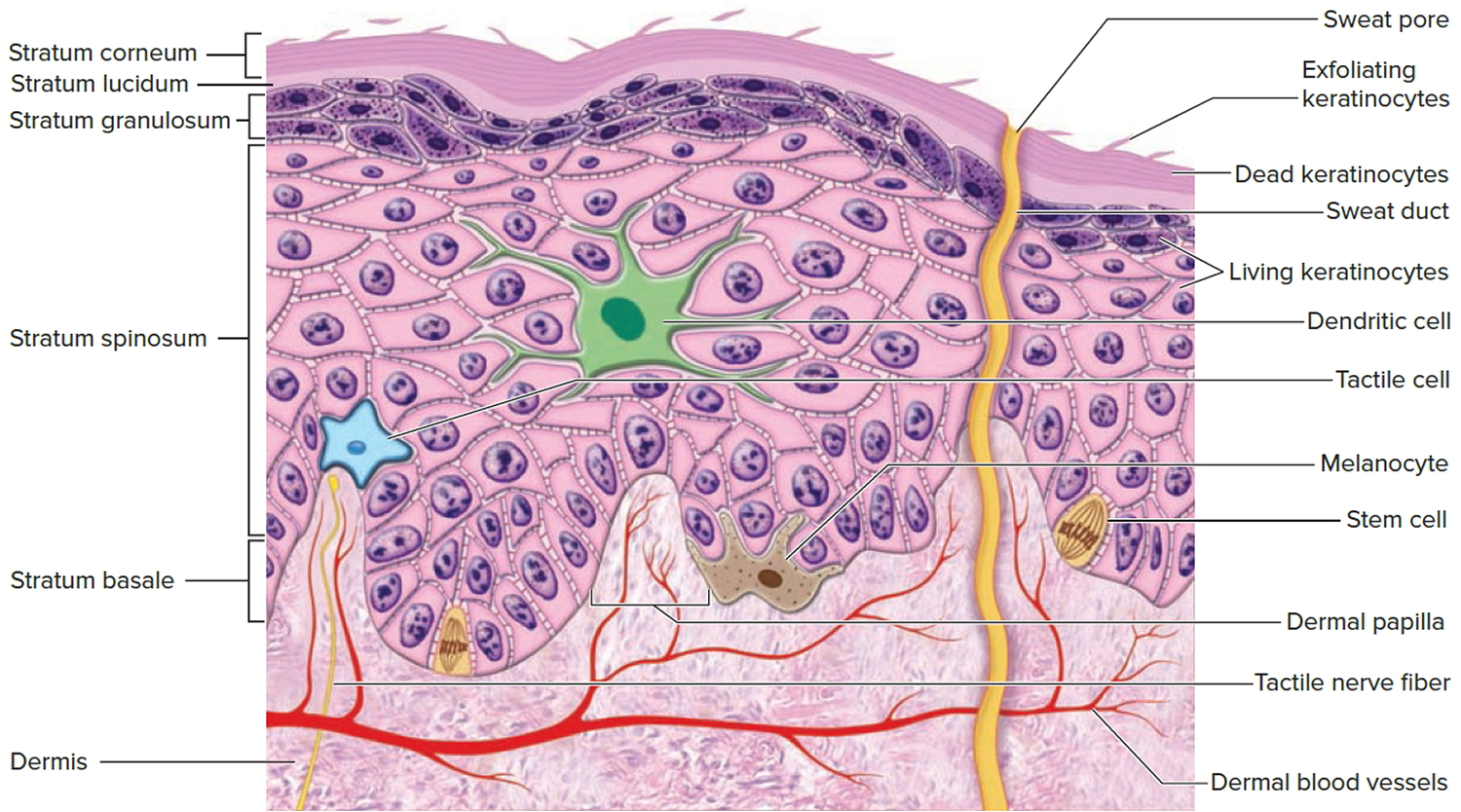
Figure 3. A mole (melanocytic nevus) – most harmless moles are round or oval-shaped, with a smooth edge


Figure 4. Congenital mole (congenital nevus)

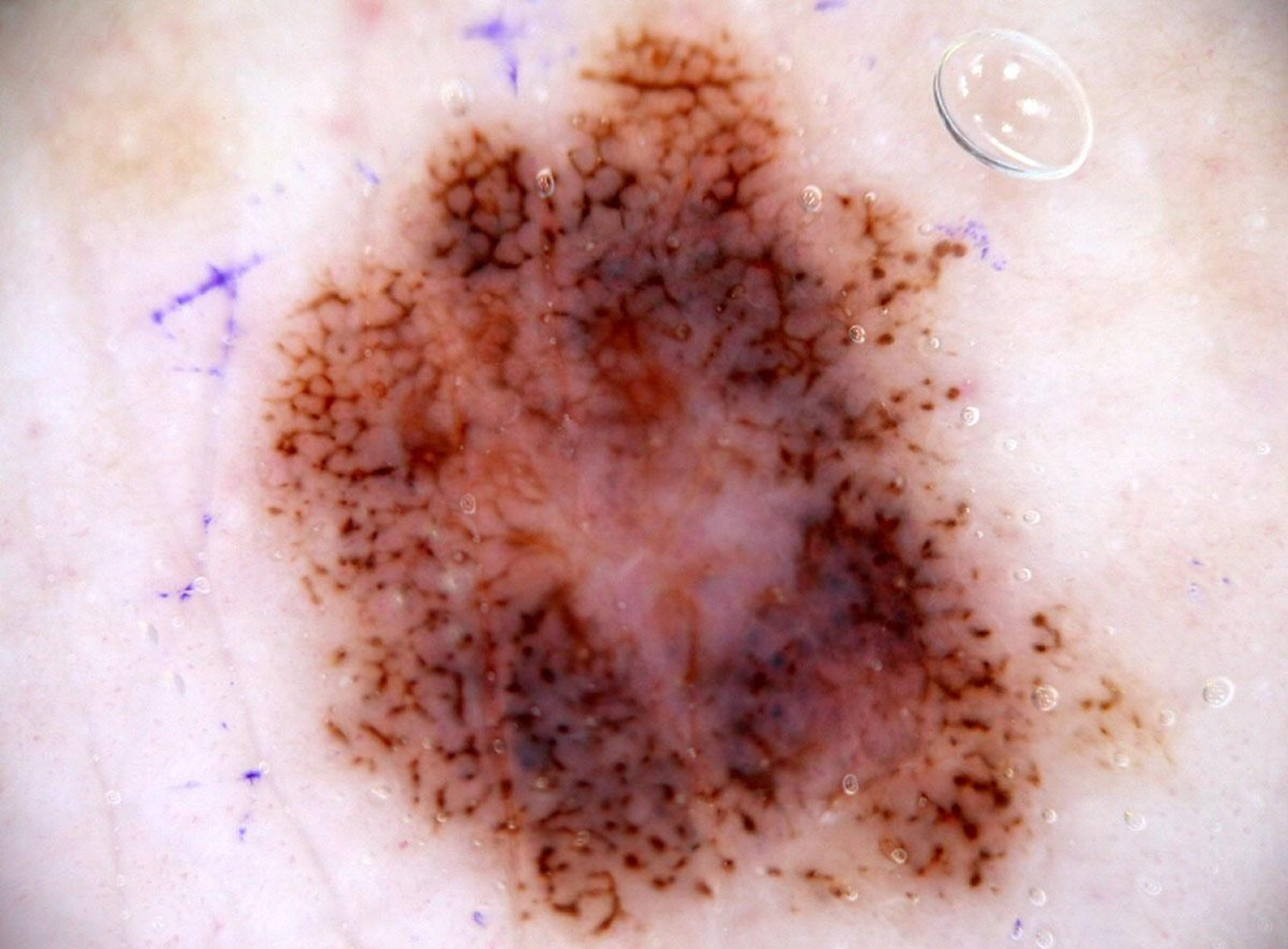
Figure 5. Abnormal moles (dysplastic nevus)



Figure 6. Cancerous moles (melanoma)

Figure 7. Cancerous moles (melanoma)

What do normal moles look like?
Moles are generally medium to dark brown in color, though they range from even skin color, tan, brown or pink to black. People who have dark skin or hair tend to have darker moles than people with fair skin or blonde hair. A common mole is round or oval, usually smaller than about 5 millimeters wide (about 1/4 inch, the width of a pencil eraser). The majority of moles are flat, relatively even in color, smooth surface and regular in shape with a distinct edge. Some moles are raised and these are usually soft to touch and lighter in color.
Moles can develop anywhere on your body, including your scalp, armpits, under your nails, and between your fingers and toes. Most people have 10 to 40 moles. Many of these develop by age 50. Moles may change in appearance or fade away over time. Hormonal changes of adolescence and pregnancy may cause moles to become darker and larger.
Moles need to be distinguished from freckles that occur on the faces of red-headed and fair-skinned children or on the shoulders following sunburns. Moles can appear anywhere including palms and soles, nails, genitals, scalp and eyes.
Can a common mole turn into melanoma?
Yes, but a common mole rarely turns into melanoma, which is the most serious type of skin cancer.
Although common moles are not cancerous, people who have more than 50 common moles have an increased chance of developing melanoma 4.
People should tell their doctor if they notice any of the following changes in a common mole 3:
- The color changes
- The mole gets unevenly smaller or bigger (unlike normal moles in children, which get evenly bigger)
- The mole changes in shape, texture, or height
- The skin on the surface becomes dry or scaly
- The mole becomes hard or feels lumpy
- It starts to itch
- It bleeds or oozes
Types of moles
Acquired nevi
Most moles that are acquired during life are usually less than 1/4 inch in size. Many of those that form in childhood and early adult life are now thought to be due to sun damage. Most people think of a mole as being a dark brown spot, but moles have a much wider range of appearance. They can be raised from the skin and very noticeable, or they may contain dark hairs. Having hairs in a mole doesn’t make it more dangerous. Moles can appear anywhere on the skin, alone or grouped. They usually are brown in color and can be various sizes and shapes. Special cells that contain the pigment melanin cause the brown color.
Facial moles are probably are determined before a person is born. Some may not appear until later in life, but moles that appear after age 50 should be regarded with suspicion. Moles may darken, which can happen after exposure to the sun, pregnancy and sometimes during therapy with certain steroid drugs. There is little risk of melanoma cancer developing in these moles.
Atypical moles (Dysplastic nevi or Clarks nevi)
An estimated one out of every 10 Americans has at least one atypical mole. These moles are larger than common moles (e.g. > 6 mm), with borders that are irregular and poorly defined (features suggesting melanoma). Atypical moles also vary in color, ranging from tan to dark brown shades on a pink background. They have irregular borders that may include notches. They may fade into surrounding skin and include a flat portion level with the skin. These are some of the features that one sees when looking at a melanoma. When a pathologist looks at an atypical mole under the microscope, it has features that are in-between a normal mole and a melanoma.
While atypical moles are considered to be pre-cancerous (more likely to turn into melanoma than regular moles), not everyone who has atypical moles gets melanoma. In fact, most moles — both ordinary and atypical ones — never become cancerous. There is ongoing debate amongst dermatologists on whether atypical moles should be removed or left alone. Some doctors argue for removal due to the risk of atypical moles developing into melanoma in some people. It is now known that about half of the people with melanoma have numerous atypical moles on their bodies. The risk is greatest in people who also have extremely fair skin and heavy freckling, a sign of excessive sun exposure.
While atypical moles are considered to be pre-cancerous (more likely to turn into melanoma than regular moles), not everyone who has atypical moles gets melanoma. In fact, most moles — both ordinary and atypical ones — never become cancerous. Thus the removal of all atypical nevi is unnecessary. In fact, most of the melanomas found on people with atypical moles arise from normal skin and not an atypical mole.
Still, there is potentially great benefit in identifying persons at increased risk of melanoma. Individuals and family members with atypical moles from melanoma-prone families should be closely checked for melanomas. This has resulted in the diagnosis of a substantial number of curable melanomas.
People without a family history of atypical moles or melanoma have an increased risk of melanoma, but it is not as high as the risk observed in members of melanoma-prone families. Individuals with a single atypical mole on their bodies have a twofold risk of developing melanoma. The risk rises to 14-fold in those with 10 or more abnormal moles.
If there are a great many atypical moles and several family members have had melanoma, you need to be very careful. Still, it has not been shown that removing all the moles (sometimes in the hundreds) decreases the lifetime risk for melanoma. Melanoma usually arises de novo, i.e. not in a pre-existing benign mole. Also people with atypical moles should have annual eye exams, as ocular melanoma is also a big risk in these cases. One should be followed closely with a very low threshold to biopsy any lesion remotely suspicious. Getting detailed body photographs are an excellent way to follow moles to see if any are changing.
Although a physician bases the initial diagnosis of atypical moles on a physical examination, removing several moles and examining them under a microscope must confirm the diagnosis. This procedure, called a biopsy, is usually performed in your doctor’s office using local anesthesia.
A pathologist will examine the tissue under a microscope and make the precise diagnosis. Diagnosis by biopsy is not exact, and in difficult cases doctors may split 50/50 down the middle as to whether a mole is melanoma or benign. If the pathologist uses the term “severely dysplastic” or “atypical melanocytic hyperplasia” or offers a long descriptive narrative it means he really is concerned about melanoma, but does not want to call it that.
Most dermatologists usually recommend that all patients with these severely dysplastic moles have them removed with a margin (5 mm clear margins-about a quarter inch) of clinically normal skin. Also many dermatologists recommend removing “moderate dysplasia” moles, if the biopsy didn’t get all of it. Those with “mild dysplasia” can usually be left alone or watched.
If the pathology report describes some amount of atypia, the following have been recommended 5:
- Dysplastic moles with mild or moderate histologic atypia with clear margins do not need reexcision.
- Dysplastic moles with mild histologic atypia with positive margins but without clinical residual pigmentation may be safely observed rather than reexcised.
Once the diagnosis of atypical moles is established, additional biopsies are performed only if melanoma is suspected, or if a new mole appears. Just as women who regularly examine their own breast are much more likely to be cured of breast cancer if it appears, self-exam of your skin once a month is the best defense against melanoma. Be sure to insist on a biopsy of any mole that is changing or growing.
Can a dysplastic nevus turn into melanoma?
Yes, but most dysplastic nevi do not turn into melanoma 6. Most remain stable over time. Researchers estimate that the chance of melanoma is about ten times greater for someone with more than five dysplastic nevi than for someone who has none, and the more dysplastic nevi a person has, the greater the chance of developing melanoma 6.
Congenital nevi
Only a few babies, about 1 in 100, are born with a mole, the congenital nevus. These can vary in size from being less than 1/4 inch to covering almost the entire body. Large nevi can vary greatly in size, shape, color, surface texture, and hairiness. Some are reddish-tan; others are almost black. Most are shades of brown. Some have fine downy hair; many have long, thick, darker hair. Some have a permanent “goose bump” appearance.
Nevi measuring 4 inches (10 cm) or more at birth occur in about one in every 20,000 children. Giant congenital nevi involving much of the body surface are less common, possibly around one in every 200,000 to 500,000 births. Many people with a giant nevus will have anywhere from several to hundreds of smaller “satellite” nevi. In a very few persons with giant moles, nevus cells can also be found in the spinal cord and near the brain, a condition called neurocutaneous melanosis.
The exact risk of melanoma developing in a giant congenital nevus is not known but is thought to be at least 6%. There has not been any melanoma in the satellite nevi, and those on the arms and legs are also less dangerous in general.
Small and medium sized congenital nevi have a much lower risk, perhaps 1/10%. Small congenital nevi rarely turn malignant before puberty. Congenital moles will grow in proportion to body growth. Their color may stay the same, lighten slowly, or darken slowly over time. Changes in growth, in color, in surface texture, pain, bleeding, or itching are all of concern. Any such changes should be evaluated medically if they last longer than a few weeks.
Spitz nevus
A Spitz nevus (Epithelioid and Spindle-Cell Nevus) is an uncommon, benign type of mole (melanocytic naevus) that is usually acquired and has histologic features that overlap with those of melanoma, so they are often excised as a precaution. Spitz nevi were previously diagnosed as melanomas due to their similar appearance under a microscope, until it was found that they did not show malignant behavior. They tend to grow very rapidly, reaching a size of approximately 1 cm within 6 months and thereafter remaining static, which may be worrisome to patients. These lesions are more common in the younger population, with 70% of cases diagnosed during the first two decades of life. Both sexes are affected equally with fair skinned individuals being most frequently affected.
The cause of the Spitz nevus is currently unknown. Some cases of Spitz nevi have a unique aberration of genes on chromosome 11p which is not observed in melanomas.
Patients with Spitz nevus may present with possible bleeding and itching of the lesion, although these symptoms are not common as most patients are asymptomatic. On physical examination, the Spitz nevus appears as a symmetric, well-circumscribed, smooth-surfaced or warty, firm, <1 cm, dome-shaped papule or nodule. The Spitz nevus is usually a solitary lesion but may rarely be in clusters or present as eruptive widespread lesions. Most Spitz nevi are pink, raised, and dome-shaped. Spitz nevi are uniform in color and may also be pink, red, red-brown, tan, blue-black, or even non-pigmented. They are most commonly located on the face, neck, and legs, although the upper extremities and trunk may be affected. Palms, soles, and mucous membranes are usually spared.
A complete medical history including a family history of skin cancers should be performed on all patients. If a dermatoscope is available, a characteristic “starburst pattern” is observed where pigmented streaks radiate symmetrically at the periphery of the lesion. A biopsy should be performed to determine malignant potential. The management of the Spitz nevus is controversial as some dermatologists recommend conservative treatment with a partial biopsy as they are benign. On the other hand, due to the histologic overlap with melanomas and the possible recurrence, some dermatologists recommend a biopsy with complete excision with a clear margin of normal skin whenever possible. Due to the possible disfigurement of excisions and the benign nature of the Spitz nevus, each patient should be evaluated individually with the best interest of the patient kept in mind. Certain atypical features of the Spitz nevus such as a diameter greater than 1 cm, asymmetry, or ulceration warrant a wider margin of normal skin during the initial excision. All patients should have regular follow-ups with a dermatologist to check for any changes or recurrences of the Spitz nevus regardless of the treatment plan.
Figure 8. Spitz nevus


What are the differences between a common mole, a dysplastic nevus and a melanoma?
Common moles, dysplastic nevi, and melanoma vary by size, color, shape, and surface texture. The list below summarizes some differences between moles and cancer. Another important difference is that a common mole or dysplastic nevus will not return after it is removed by a full excisional biopsy from the skin, but melanoma sometimes grows back. Also, melanoma can spread to other parts of the body.
Common Mole (Nevus)
- Is it cancer? No. Common moles rarely become cancer.
- How many people have common moles? Most American adults—about 300 million people—have common moles.
- How big are they? Usually less than 5 millimeters wide, or about 1/4 inch (not as wide as a new pencil eraser).
- What color are they? May be pink, tan, brown, black (in people with dark skin), or a color that is very close to a person’s normal skin tone. The color is usually even throughout.
- What shape are they? Usually round or oval. A common mole has a distinct edge that separates it from the rest of the skin.
- What is the surface texture? Begins as a flat, smooth spot on the skin. May become raised and form a smooth bump.
Dysplastic Nevus
- Is it cancer? No. A dysplastic nevus is more likely than a common mole to become cancer, but most do not become cancer.
- How many people have dysplastic nevi? About 1 in 10 American adults—about 30 million people—have at least one dysplastic nevus 6.
- How big are they? Often wider than 5 millimeters (wider than a new pencil eraser).
- What color are they? May be a mixture of tan, brown, and red or pink shades.
- What shape are they? Have irregular or notched edges. May fade into the rest of the skin.
- What is the surface texture? May have a smooth, slightly scaly, or rough, irregular, and pebbly appearance.
Melanoma
- Is it cancer? Yes.
- How many people have melanoma? Melanoma is much less common than other kinds of skin cancer. But every year, about 2 in 10,000 Americans—more than 70,000 people—develop melanoma. More than 800,000 Americans alive today have been diagnosed with melanoma 7.
- How big are they? Usually wider than 6 millimeters (wider than a new pencil eraser).
- What color are they? Usually uneven in color. May have shades of black, brown, and tan. May also have areas of white, gray, red, pink, or blue.
- What shape are they? Often irregular and asymmetrical (the shape of one half does not match the other half). Edges may be ragged, notched, or blurred. May fade into the rest of the skin.
- What is the surface texture? May break down and look scraped, become hard or lumpy, or ooze or bleed.
ABCDE Criteria of Melanoma
The “ABCDE” criteria describes the features of early melanoma 8:
- A is for Asymmetric shape. One half is unlike the other half.
- B is for Irregular Border. Look for moles with irregular, notched or scalloped borders.
- C is for Multiple Colors or dark black. Look for growths that have changed color, have many colors or have uneven color.
- D is for Diameter > 6 mm. Look for new growth in a mole larger than 1/4 inch (about 6 millimeters).
- E is for Evolving, changing (e.g., present for years unchanged and then suddenly grows). Watch for moles that change in size, shape, color or height, especially if part or all of a mole turns black. Moles may also evolve to develop new signs and symptoms, such as itchiness or bleeding.
Cancerous (malignant) moles vary greatly in appearance. Some may show all of the features listed above. Others may have only one or two.
Some melanomas don’t fit these rules.
- It’s important to tell your doctor about any changes or new spots on the skin, or growths that look different from the rest of your moles.
Figure 9. Asymmetric shape (melanoma in-situ)

Figure 10. Irregular Border (melanoma)

Figure 11. Multiple Colors or dark black (melanoma)

Figure 12. Diameter > 6 mm (melanoma)

Figure 13. Evolving, changing (melanoma)

What factors increase the chance of melanoma?
People with the following risk factors have an increased chance of melanoma 4:
- Having a dysplastic nevus
- Having more than 50 common moles
- Sunlight: Sunlight is a source of UV radiation, which causes skin damage that can lead to melanoma and other skin cancers.
- Severe, blistering sunburns: People who have had at least one severe, blistering sunburn have an increased chance of melanoma. Although people who burn easily are more likely to have had sunburns as a child, sunburns during adulthood also increase the chance of melanoma.
- Lifetime sun exposure: The greater the total amount of sun exposure over a lifetime, the greater the chance of melanoma.
- Tanning: Although having skin that tans well lowers the risk of sunburn, even people who tan well without sunburning increase their chance of melanoma by spending time in the sun without protection.
Sunlight can be reflected by sand, water, snow, ice, and pavement. The sun’s rays can get through clouds, windshields, windows, and light clothing.
In the United States, skin cancer is more common where the sun is strong. For example, a larger proportion of people in Texas than Minnesota get skin cancer. Also, the sun is strong at higher elevations, such as in the mountains.
- Sunlamps and tanning booths: UV radiation from artificial sources, such as sunlamps and tanning booths, can cause skin damage and melanoma. Health care providers strongly encourage people, especially young people, to avoid using sunlamps and tanning booths. The risk of skin cancer is greatly increased by using sunlamps and tanning booths before age 30.
- Personal history: People who have had melanoma have an increased risk of developing other melanomas.
- Family history: Melanoma sometimes runs in families. People who have two or more close relatives (mother, father, sister, brother, or child) with melanoma have an increased chance of melanoma. In rare cases, members of a family will have an inherited disorder, such as xeroderma pigmentosum, that makes the skin extremely sensitive to the sun and greatly increases the chance of melanoma.
- Skin that burns easily: People who have fair (pale) skin that burns easily in the sun, blue or gray eyes, red or blond hair, or many freckles have an increased chance of melanoma.
- Certain medical conditions or medicines: Medical conditions or medicines (such as some antibiotics, hormones, or antidepressants) that make skin more sensitive to the sun or that suppress the immune system increase the chance of melanoma.
Moles complications
Melanoma is the main complication of moles. Some people have a higher than average risk of their moles becoming cancerous and developing into melanoma. Factors that increase your risk of melanoma include:
- Being born with large moles. These types of moles are called congenital nevi. On an infant, such moles are classified as large if they’re more than 2 inches (5 centimeters) in diameter. Even a large mole seldom becomes cancerous and almost never before the child reaches puberty.
- Having unusual moles. Moles that are bigger than a common mole and irregular in shape are known as atypical (dysplastic) nevi. They tend to be hereditary. And they often have dark brown centers and lighter, uneven borders.
- Having many moles. Having more than 50 ordinary moles indicates an increased risk of melanoma. Two studies add to the evidence that the number of your moles predict cancer risk. One showed that people under 50 years old who have 20 or more moles on their arms are at increased risk of melanoma. Another showed a relationship between the number of women’s moles and breast cancer risk.
- Having a personal or family history of melanoma. If you’ve had melanoma before, you are at increased risk of a mole becoming cancerous. In addition, some types of atypical moles lead to a genetic form of melanoma.
What causes moles
Moles are caused when cells in the skin (melanocytes) grow in clusters or clumps. Melanocytes are distributed throughout your skin and produce melanin, the natural pigment that gives your skin its color.
Moles prevention
The following measures can help limit the development of moles and the main complication of moles — melanoma.
Watch for changes
Become familiar with the location and pattern of your moles. Regularly examine your skin to look for changes that may signal melanoma. Do self-exams once a month, especially if you have a family history of melanoma. With the help of mirrors, do a head-to-toe check, including your scalp, palms and fingernails, armpits, chest, legs, and your feet, including the soles and the spaces between the toes. Also check your genital area and between your buttocks.
Talk with your doctor about your risk factors for melanoma and whether you need a professional skin exam on a routine basis.
Protect your skin
Take measures to protect your skin from ultraviolet (UV) radiation, such as from the sun or tanning beds. UV radiation has been linked to increased melanoma risk. And children who haven’t been protected from sun exposure tend to develop more moles.
- Avoid peak sun times. For many people in North America, the sun’s rays are strongest between 10 a.m. and 4 p.m. Schedule outdoor activities for other times of the day, even on cloudy days or in winter.
- Use sunscreen year-round. Apply sunscreen about 30 minutes before going outdoors, even on cloudy days. Use a broad-spectrum sunscreen with an SPF of at least 30+. Apply it generously and reapply every two hours — or more often if you’re swimming or sweating. The American Academy of Dermatology recommends using a broad-spectrum, water-resistant sunscreen with an SPF of at least 30+.
- Cover up. Sunglasses, broad-brimmed hats, long sleeves and other protective clothing can help you avoid damaging UV rays. You might also want to consider clothing that’s made with fabric specially treated to block UV radiation.
- Avoid tanning lamps and beds. Tanning lamps and beds emit UV rays and can increase your risk of skin cancer.
Moles diagnosis
Your doctor can identify moles by looking at your skin. You may choose to make a skin examination a regular part of your preventive medical care. Talk to your doctor about a schedule that’s appropriate for you. During a skin exam, your doctor inspects your skin from head to toe.
If your doctor suspects that a mole may be cancerous, he or she may take a tissue sample (biopsy) for microscopic examination.
How to get rid of moles
All pigmented lesions should be evaluated by the ABCDE criteria and removed if abnormal.
People should protect themselves from the sun. Any clinically benign mole removed for cosmetic or functional reasons should be submitted for pathologic examination to exclude cancer. In a study of such lesions, 2.3% were found to represent a malignancy (melanoma, basal cell carcinoma and squamous cell carcinoma) 9. In a study of over a thousand moles, enlargement alone (without signs of atypia) was not a sign of malignancy.
How to remove moles
If your mole is cancerous, your doctor will do a surgical procedure to remove it. If you have a mole that causes irritation when you shave, you may want to have it removed.
Mole removal takes only a short time and is usually done on an outpatient basis. Your doctor numbs the area around the mole and cuts it out, along with a margin of healthy skin if necessary. The procedure may leave a permanent scar.
- If you notice that a mole has grown back, see your doctor promptly.
A dermatologist can usually remove a mole during an office visit. Most removals require only 1 office visit. Occasionally, a patient may need to return for a second visit.
Whether it’s during 1 or 2 visits, a dermatologist can safely and easily remove a mole. A dermatologist will use one of these procedures:
- Surgical excision: The dermatologist cuts out the entire mole and stitches the skin closed if necessary. Your mole will also be looked at under a microscope by a specially trained doctor. This is done to check for cancer cells. If cancer cells are found, your dermatologist will let you know.
- Surgical shave: The dermatologist uses a surgical blade to remove the mole. In most cases, a specially trained doctor will examine your mole under a microscope. If cancer cells are found, your dermatologist will let you know.
Cosmetic care
If you’re self-conscious about a mole, you could try makeup to help conceal it. If you have a hair growing from a mole, you might try clipping it close to the skin’s surface or plucking it. Or talk with your dermatologist about permanently removing the hair and the mole.
Anytime you cut or irritate a mole, keep the area clean. See your doctor if the mole doesn’t heal.
While it may seem more convenient to shave off or cut out a mole yourself, there are 3 very good reasons a dermatologist should remove it:
- Skin cancer: If the mole contains skin cancer, some of the cancer cells can stay in the skin and even spread.
- Scarring: You can disfigure your skin causing a scar.
- Infection: A dermatologist uses sterile equipment to prevent infection.
- BJD 2016;174:312[↩]
- Cancer Epidemiol Biomarkers Prev. 2007;16:2136[↩]
- Goodson AG, Grossman D. Strategies for early melanoma detection: approaches to the patient with nevi. Journal of the American Academy of Dermatology 2009; 60(5):719–738. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2690513/[↩][↩]
- Tucker MA. Melanoma epidemiology. Hematology/Oncology Clinics of North America 2009; 23(3):383–395. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3234163/[↩][↩]
- JAMA Derm 2015;151;212[↩]
- Friedman RJ, Farber MJ, Warycha MA, et al. The “dysplastic” nevus. Clinics in Dermatology 2009; 27(1):103–115. https://www.ncbi.nlm.nih.gov/pubmed/19095156[↩][↩][↩]
- American Cancer Society. Cancer Facts and Figures 2011. https://www.cancer.org/research/cancer-facts-statistics.html[↩]
- Rigel DS, Russak J, Friedman R. The evolution of melanoma diagnosis: 25 years beyond the ABCDs. CA: A Cancer Journal for Clinicians 2010; 60(5):301–316. https://onlinelibrary.wiley.com/doi/pdf/10.3322/caac.20074[↩]
- JAAD 1999;40;567[↩]





{kind=link}