What is Muscle
Muscles constitute nearly half of your body’s weight and occupy a place of central interest in several fields of health care and fitness. Life without muscle tissue mean you couldn’t sit, stand, walk, speak, or grasp objects. Blood would not circulate because the heart couldn’t propel it through the vessels. The lungs couldn’t empty and fill, nor could food move along the digestive tract.
The muscular system of the human body has more than 700 skeletal muscles and includes all the skeletal muscles that are under voluntary control.
Many of your physiological processes and virtually all your dynamic interactions with the environment, involve muscle tissue. There are three types of muscle tissue: skeletal muscle, cardiac muscle, and smooth muscle.
Skeletal muscle tissue moves the body by pulling on bones of the skeleton, making it possible for us to walk, dance, or play a musical instrument.
Cardiac muscle tissue pushes blood through the blood vessels of the cardiovascular system.
Smooth muscle tissue pushes fluid and solids along the digestive tract and performs varied functions in other systems. These muscle tissues share four properties:
- Excitability: The ability to respond to stimulation. For example, skeletal muscles respond to stimulation by the nervous system, and some smooth muscles respond to circulating hormones.
- Contractility: The ability to shorten actively and exert a pull or tension that is harnessed by connective tissues.
- Extensibility: The ability to contract over a range of resting lengths. For example, a smooth muscle cell can be stretched to several times its original length and still contract when stimulated.
- Elasticity: The ability of a muscle to return to its original length after a contraction.
The Functions of Muscles
Collectively, the three types of muscle serve the following functions:
- Movement. Muscles enable us to move from place to place and to move individual body parts; they move body contents in the course of breathing, blood circulation, feeding and digestion, defecation, urination, and childbirth; and they serve various roles in communication—speech, writing, cial expressions, and other body language.
- Stability. Muscles maintain posture by preventing unwanted movements. Some are called antigravity muscles because, at least part of the time, they resist the pull of gravity and prevent us from falling or slumping over. Many muscles also stabilize the joints by maintaining tension on tendons and bones.
- Control of body openings and passages. Muscles encircling the mouth serve not only for speech but also for food intake and retention of food while chewing. In the eyelid and pupil, they regulate the admission of light to the eye. Internal muscular rings control the movement of food, bile, blood, and other materials within the body. Muscles encircling the urethra and anus control the elimination of waste. Some of these muscles are called sphincters, but not all.
- Heat production. The skeletal muscles produce as much as 85% of one’s body heat, which is vital to the functioning of enzymes and therefore to all metabolism.
- Glycemic control. This means the regulation of blood glucose concentration within its normal range. The skeletal muscles absorb, store, and use a large share of one’s glucose and play a highly significant role in stabilizing its blood concentration. In old age, in obesity, and when muscles become deconditioned and weakened, people suffer an increased risk of type 2 diabetes mellitus because of the decline in this glucose-buffering function.
Skeletal muscle
Skeletal muscles are organs composed mainly of skeletal muscle, but a skeletal muscle consists of more than muscular tissue. It also contains connective tissue, nerves, and blood vessels. The connective tissue components, from the smallest to largest and from deep to superficial, are as follows:
• Endomysium. This is a thin sleeve of loose connective tissue that surrounds each muscle fiber. It creates room for blood capillaries and nerve fibers to reach every muscle fiber, ensuring that no muscle cell is without stimulation and nourishment. The endomysium also provides the extracellular chemical environment for the muscle fiber and its associated nerve ending. Excitation of a muscle fiber is based on the exchange of calcium, sodium, and potassium ions between the endomysial tissue fluid and the nerve and muscle fibers.
• Perimysium. This is a thicker connective tissue sheath that wraps muscle fibers together in bundles called fascicles. Fascicles are visible to the naked eye as parallel strands—the grain in a cut of meat; if you pull apart “fork-tender” roast beef, it separates along these fascicles. The perimysium carries the larger nerves and blood vessels as well as stretch receptors called muscle spindles.
• Epimysium. This is a fibrous sheath that surrounds the entire muscle. On its outer surface, the epimysium grades into the fascia, and its inner surface issues projections between the fascicles to form the perimysium.
• Fascia. This is a sheet of connective tissue that separates neighboring muscles or muscle groups from each other and from the subcutaneous tissue. Muscles are grouped in compartments separated from each other by fasciae. The fascicles defined by the perimysium are oriented in a variety of ways that determine the strength of a muscle and the direction in which it pulls.
The muscular system, like the skeletal system, is divided into axial and appendicular divisions. The axial musculature originates on the axial skeleton. It positions the head and vertebral column and helps breathing by moving the rib cage. The appendicular musculature inserts onto and stabilizes or moves the appendicular skeleton.
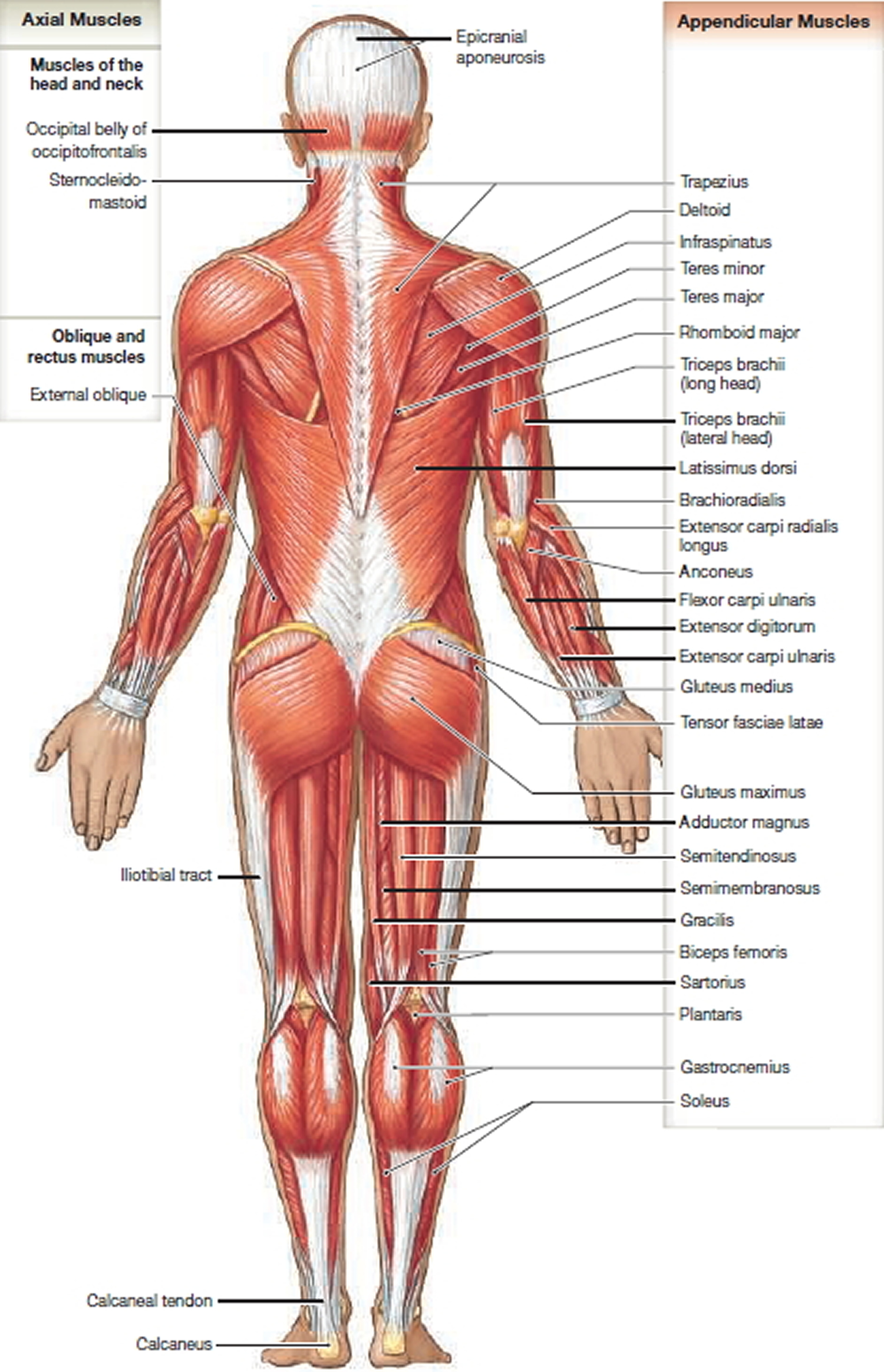
Figures 1 illustrate the major axial and appendicular muscles of the human body. These are the superficial muscles, which are relatively large. Superficial muscles cover deeper, smaller muscles that cannot be seen unless the overlying muscles are cut and pulled out of the way.
Figure 1. Muscle anatomy (front or anterior view)
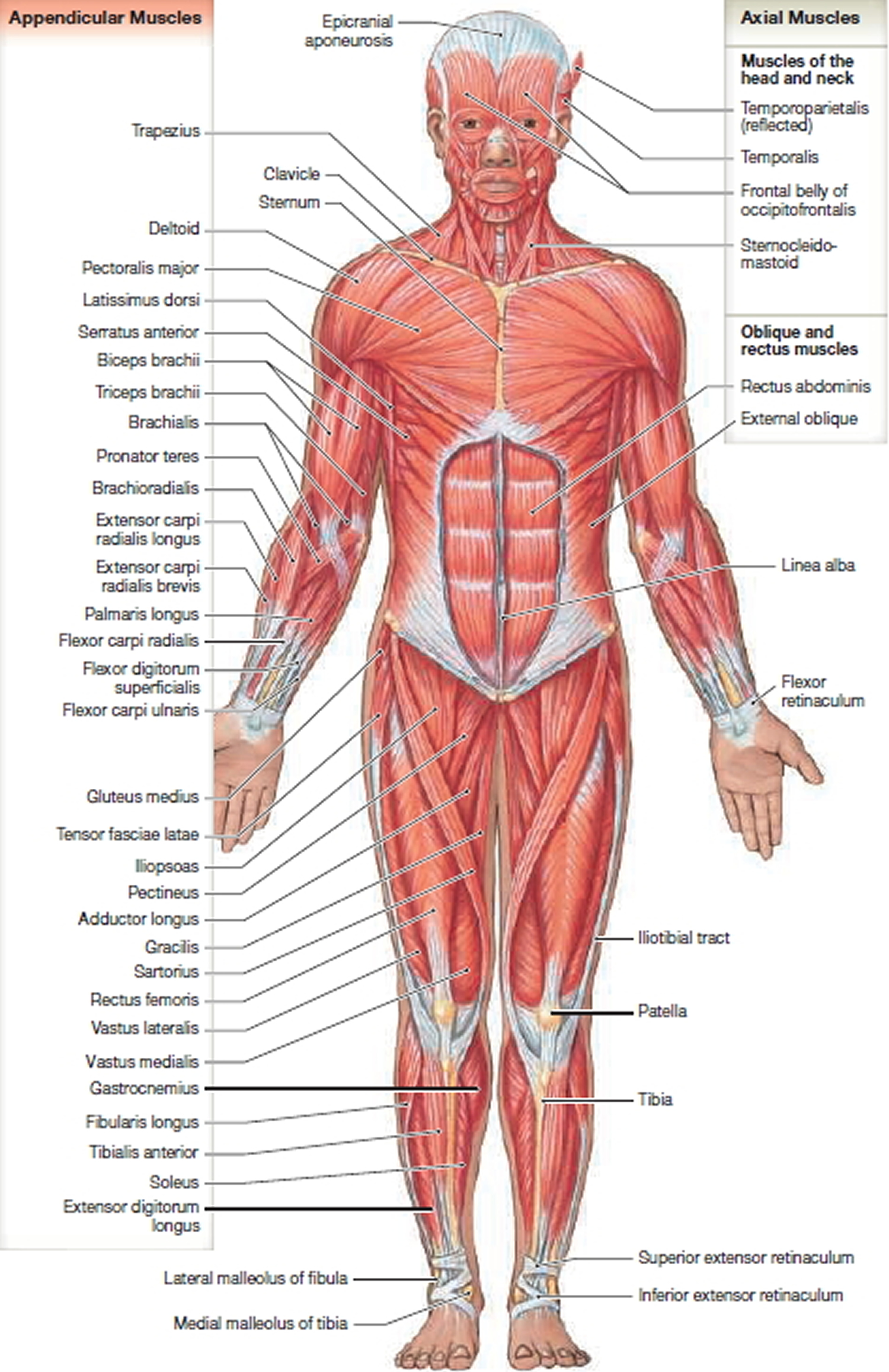
Figure 2. Muscle anatomy (back or posterior view)
There are four groups of axial muscles:
- Muscles of the head and neck. These muscles include those that move the face, tongue, larynx, and eyes. They are responsible for verbal and nonverbal communication, such as laughing, talking, frowning, smiling, and whistling. This group is also involved in chewing, swallowing, and moving the eyes.
- Muscles of the vertebral column. This group includes flexors and extensors of the axial skeleton.
- Muscles that form the walls of the abdominal and pelvic cavities. This group, the oblique and rectus muscles, is located between the first thoracic vertebra and the pelvis. These muscles move the chest wall during breathing (inspiration and expiration), compress the abdominal cavity, and rotate the vertebral column. In the thoracic area, the ribs separate these muscles, but over the abdominal surface, the muscles form broad muscular sheets. There are also oblique and rectus muscles in the neck. Although they do not form a muscular wall, they are included in this group because they share a common embryological origin. The diaphragm is within this group because it is embryologically linked to other muscles of the chest wall.
- Muscles of the perineal region and pelvic diaphragm. These muscles extend between the sacrum and pelvic girdle to support organs of the pelvic cavity, flex joints of the sacrum and coccyx, and control movement of materials through the urethra and anus.
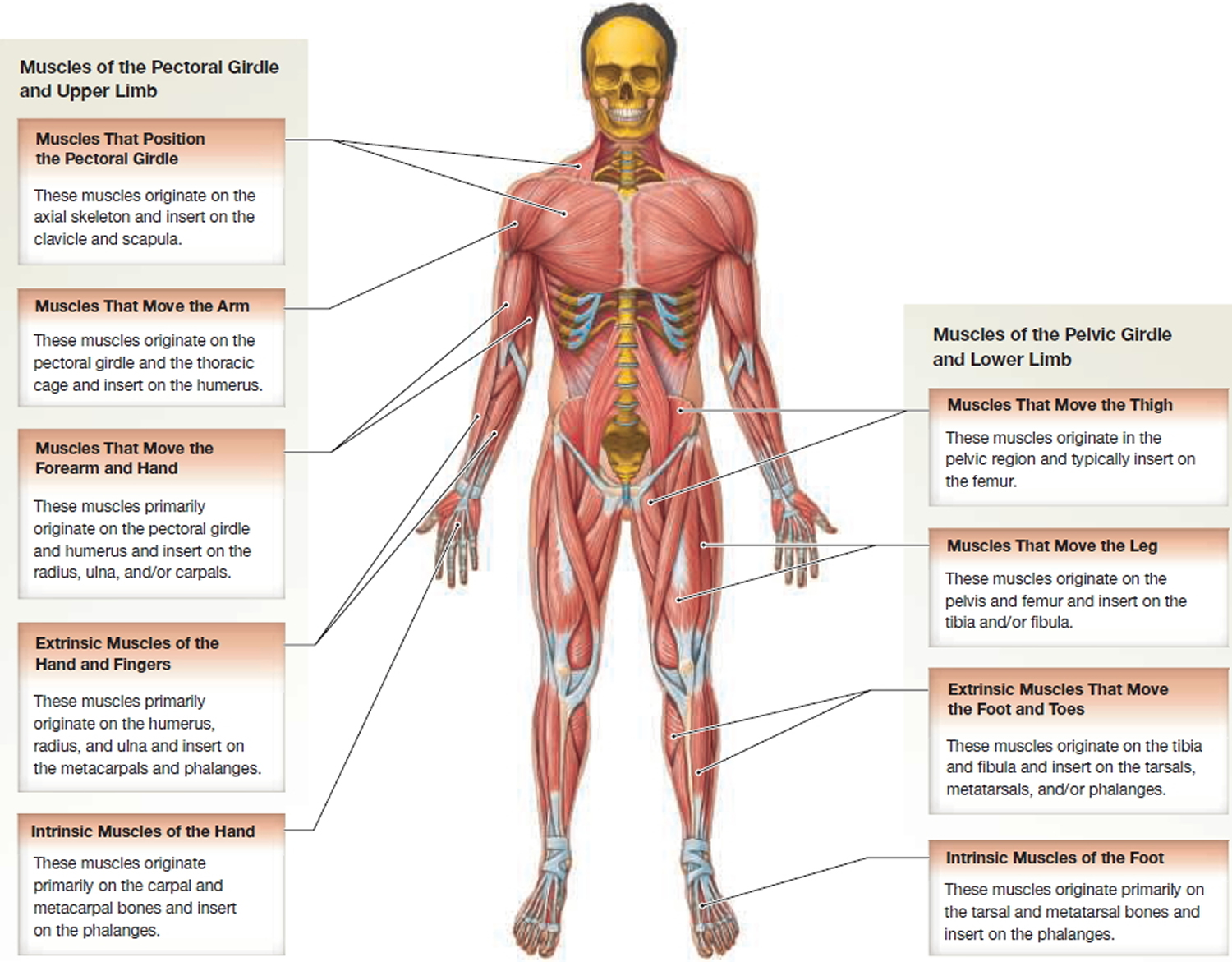
The Appendicular Musculature
There are two major groups of appendicular muscles: (1) the muscles of the pectoral girdle and upper limb and (2) the muscles of the pelvic girdle and lower limb. The upper limb has a large range of motion (amount of movement that occurs at a joint) because of the muscular connections between the pectoral girdle and the axial skeleton. These muscular connections also act as shock absorbers. For example, when you jog, you can perform delicate hand movements at the same time because the appendicular muscles absorb the shocks and bounces in your stride. In contrast, the pelvic girdle transfers weight from the axial skeleton to the lower limb. The emphasis is on strength rather than mobility, and the anatomical features that strengthen the joints limit the range of movement of the lower limbs.
Figure 3. Appendicular muscles
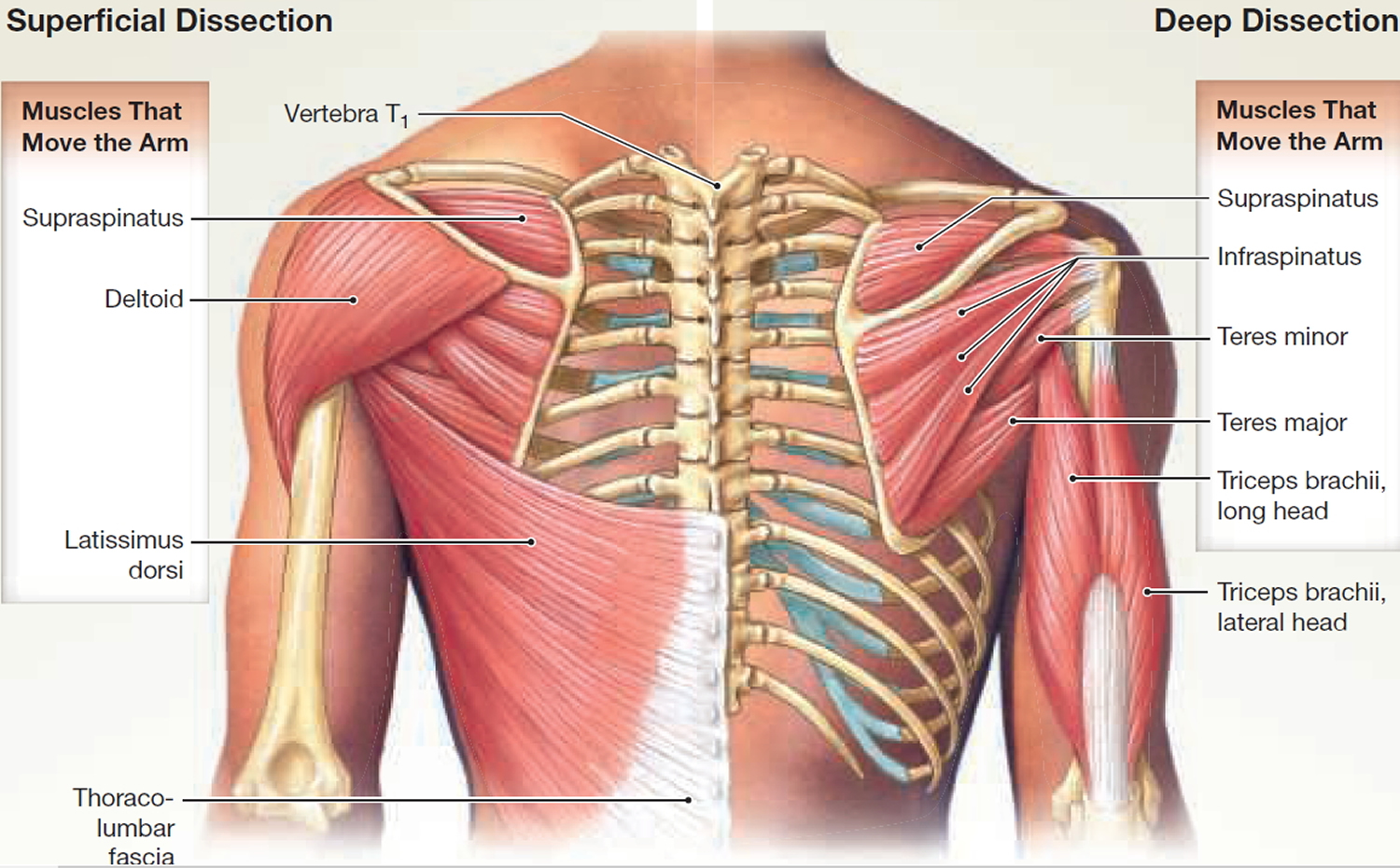
Muscles That Move the Arm
The deltoid is the prime mover for abducting the arm, but the supraspinatus is a synergist at the start of this movement. The subscapularis and teres major rotate the arm medially, whereas the infraspinatus and teres minor are antagonistic to that action, rotating the arm laterally. All of these muscles originate on the scapula. The coracobrachialis is the only muscle attached to the scapula that flexes and adducts the arm at the shoulder joint.
The pectoralis major originates from the cartilages of ribs 2 to 6 and inserts onto the crest of the greater tubercle of the humerus. The pectoralis major flexes, adducts, and medially rotates the humerus at the shoulder joint. The latissimus dorsi has a wide variety of origins and inserts onto the intertubercular sulcus of the humerus. The latissimus dorsi flexes, adducts, and medially rotates the humerus at the shoulder joint.
The shoulder is a mobile but weak joint. The tendons of the supraspinatus, infraspinatus, subscapularis, and teres minor join with the connective tissue of the shoulder joint capsule and form the rotator cuff. The rotator cuff supports and strengthens the joint capsule of the shoulder. Powerful, repetitive arm movements common in many sports (such as pitching a fastball for many innings) place considerable strain on the muscles of the rotator cuff, often causing tendon damage, muscle strains, bursitis, and other painful injuries.
Figure 4. Muscles that move the arm (front or anterior view)
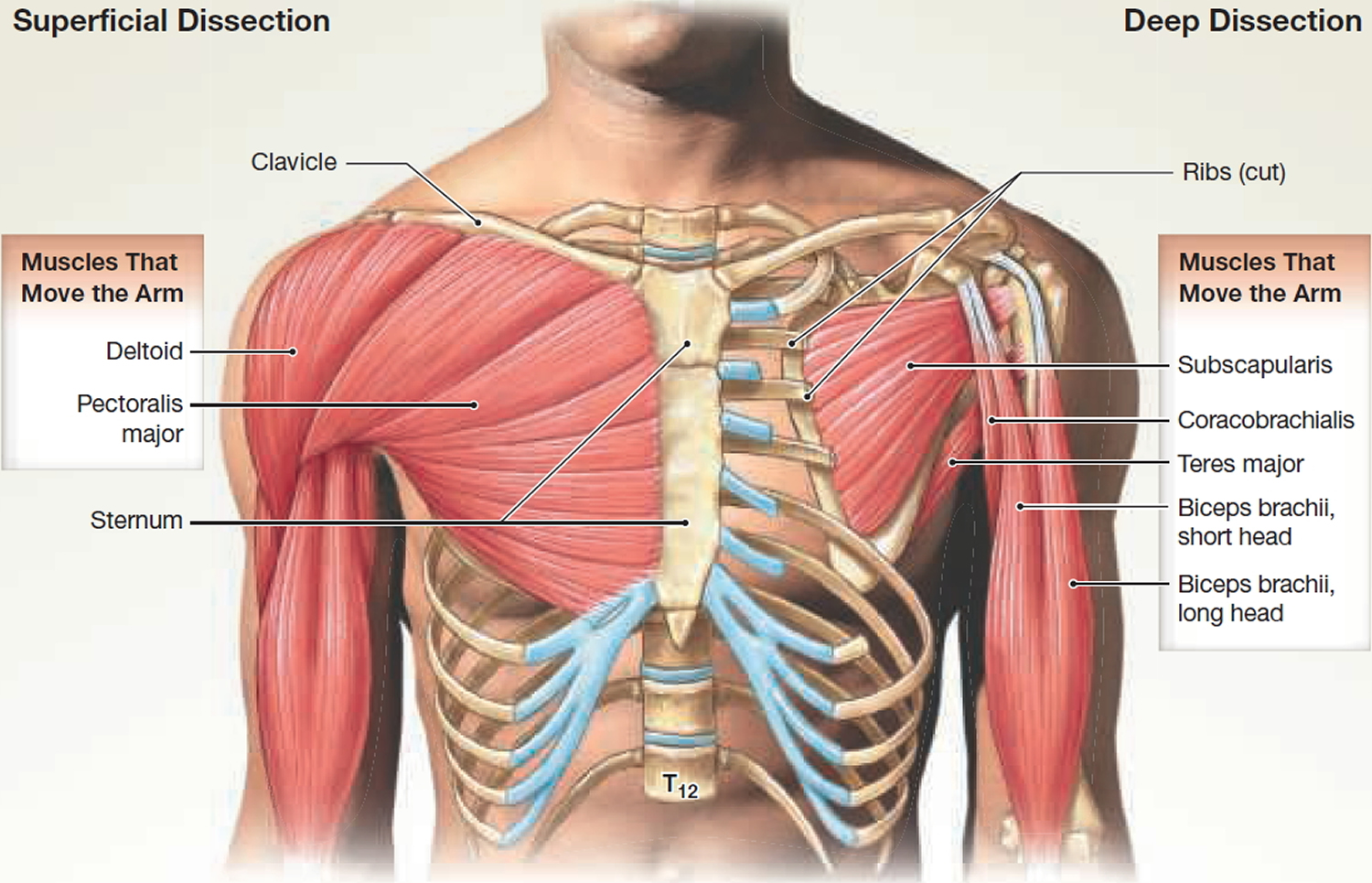
Figure 5. Muscles that move the arm (back or posterior view)
Muscles That Move the Forearm and Hand
Most of the muscles that move the forearm and hand originate on the humerus and insert on the forearm and wrist. There are two noteworthy exceptions:
- The long head of the triceps brachii originates on the scapula and inserts on the olecranon.
- The long head of the biceps brachii originates on the scapula and inserts on the radial tuberosity of the radius.
The triceps brachii and biceps brachii are examples of muscles of the arm that exert actions at more than one joint. Contracting the triceps brachii extends and adducts the shoulder and also extends the elbow. Contracting the biceps brachii flexes the shoulder and also flexes the elbow and supinates the forearm. Although these muscles exert an action at the shoulder, their primary (most important) actions are at the elbow.
The biceps brachii is also an example of how the position of the body affects the action of a muscle: When the forearm is pronated, the biceps brachii cannot contract as forcefully as when the forearm is supinated due to the position of the muscle’s insertion.
The brachialis and brachioradialis also flex the elbow. The anconeus and the triceps brachii are antagonists to this action. The flexor carpi ulnaris, flexor carpi radialis, and palmaris longus are superficial muscles that work together to flex the wrist. The flexor carpi radialis also abducts the wrist, while the flexor carpi ulnaris adducts the wrist. The extensor carpi radialis and the extensor carpi ulnaris also have an antagonistic action: The extensor carpi radialis extends and abducts the wrist, and the extensor carpi ulnaris extends and adducts the wrist.
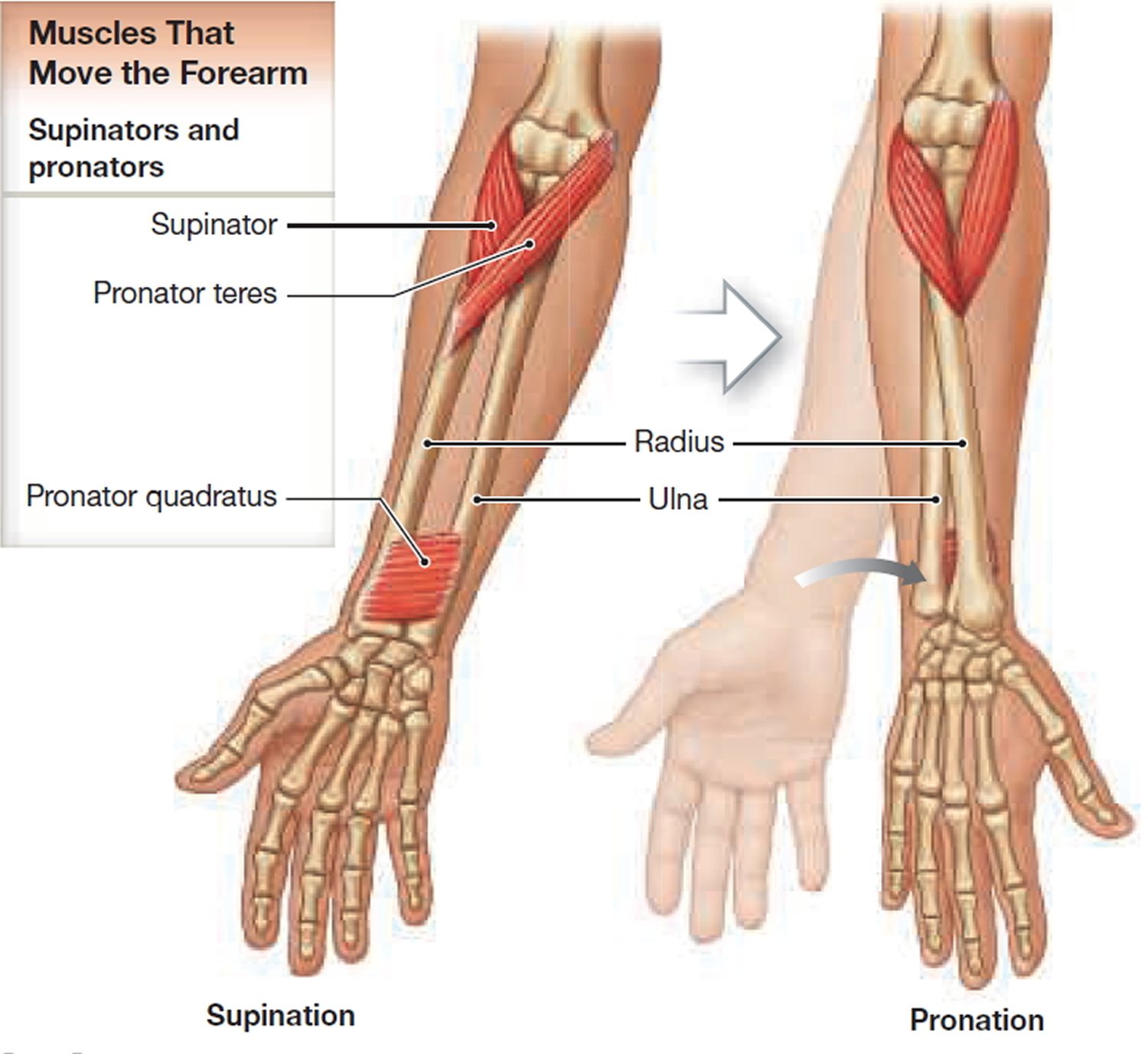
The pronator teres and the supinator muscle are antagonistic muscles that originate on the humerus and the ulna. They insert on the radius and rotate the forearm without flexing or extending the elbow. The pronator quadratus originates on the ulna and assists the pronator teres in opposing the supination actions of the supinator muscle and the biceps brachii. Figure 7 shows the muscles involved in pronation and supination (medial and lateral rotation). Note how the radius changes position as the pronator teres and pronator quadratus contract. A bursa prevents abrasion against the tendon as the tendon of the biceps brachii rolls under the radius during pronation.
Figure 6. Muscles that move forearm and hand
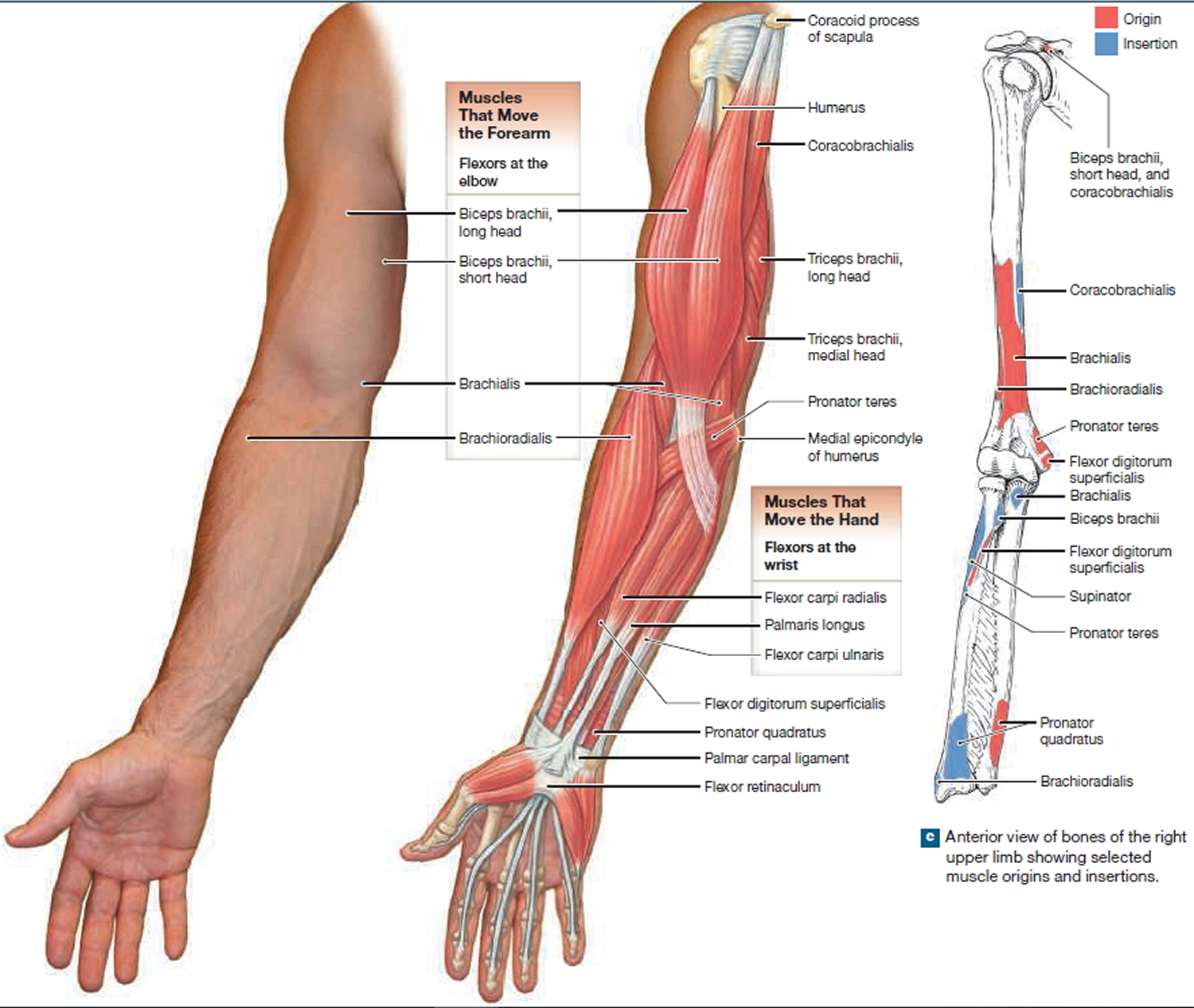
Figure 7. Muscles that pronate and supinate the forearm
Muscles That Move the Hands and Fingers
Several superficial and deep muscles of the forearm flex and extend the joints of the fingers. These muscles provide strength and gross motor control of the hand and fingers and are called extrinsic muscles of the hand.
Only the tendons of the extrinsic muscles of the hand cross the wrist joint. These are large muscles, so to ensure maximum mobility of the wrist and hand, the tendons of these muscles must be kept clear of the wrist joints. The tendons crossing the posterior and anterior surfaces of the wrist pass through synovial tendon sheaths, elongated bursae that reduce friction. Figures 8 show these muscles in an anterior view and Figures 9 show them in a posterior view.
The fascia of the forearm thickens on the posterior surface of the wrist to form a wide band of connective tissue, the extensor retinaculum. The extensor retinaculum holds the tendons of the extensor muscles in place. The fascia also thickens on the anterior surface, forming another wide band of connective tissue, the flexor retinaculum, which holds the tendons of the flexor muscles in place Inflammation of the retinacula and tendon sheaths restricts movement and irritates the median nerve, a sensory and motor nerve that innervates the hand. This condition, known as carpal tunnel syndrome, causes chronic pain.
Figure 8. Muscles that move the hands and fingers (front view)

Figure 9. Muscles that move the hands and fingers (back view)

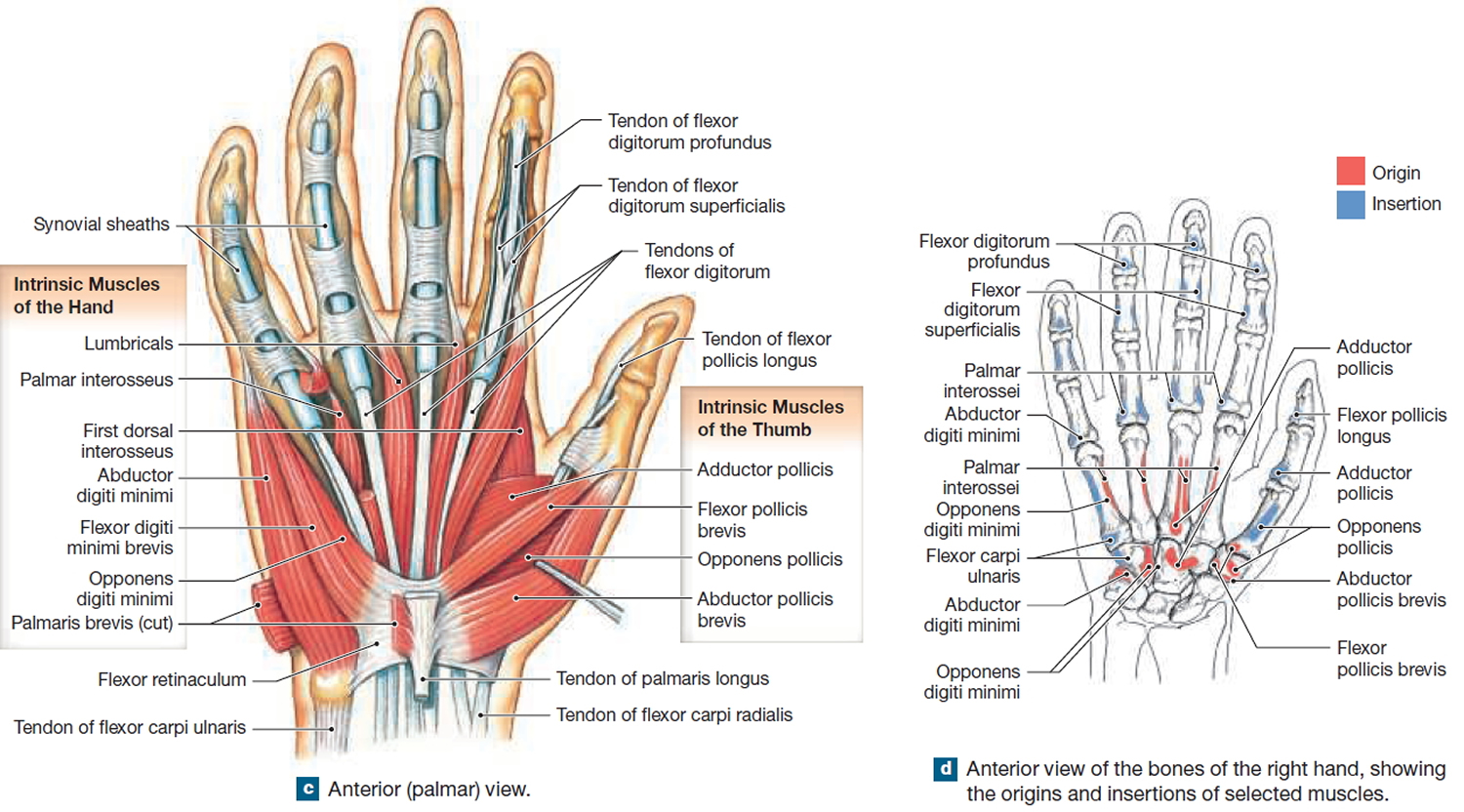
Intrinsic Muscles of the Hand
Fine motor control of the hand involves small intrinsic muscles of the hand that originate on the carpal and metacarpal bones (Figures 10 and 11). These intrinsic muscles are responsible for (1) flexion and extension of the fingers at the metacarpophalangeal joints, (2) abduction and adduction of the the fingers at the metacarpophalangeal joints, and (3) opposition and reposition of the thumb. No muscles originate on the phalanges, and only tendons extend across the distal joints of the fingers.
The four lumbricals originate on the tendons of the flexor digitorum profundus muscle in the palm of the hand. They insert onto the tendons of the extensor digitorum muscle. These muscles flex the metacarpophalangeal joints and extend the interphalangeal joints of the fingers.
The four dorsal interossei abduct the fingers. The abductor digiti minimi abducts the little finger, and the abductor pollicis brevis abducts the thumb. The adductor pollicis adducts the thumb, and the four palmar interossei adduct the fingers at the metacarpophalangeal joints.
Opposition of the thumb refers to flexing and medially rotating the thumb at the carpometacarpal joint and touching any other digit on the same hand.
The opponens pollicis allows this action. Two extrinsic muscles of the hand, the extensor pollicis longus and the abductor pollicis longus reposition the thumb.
Figure 10. Muscles of the hand (front view)
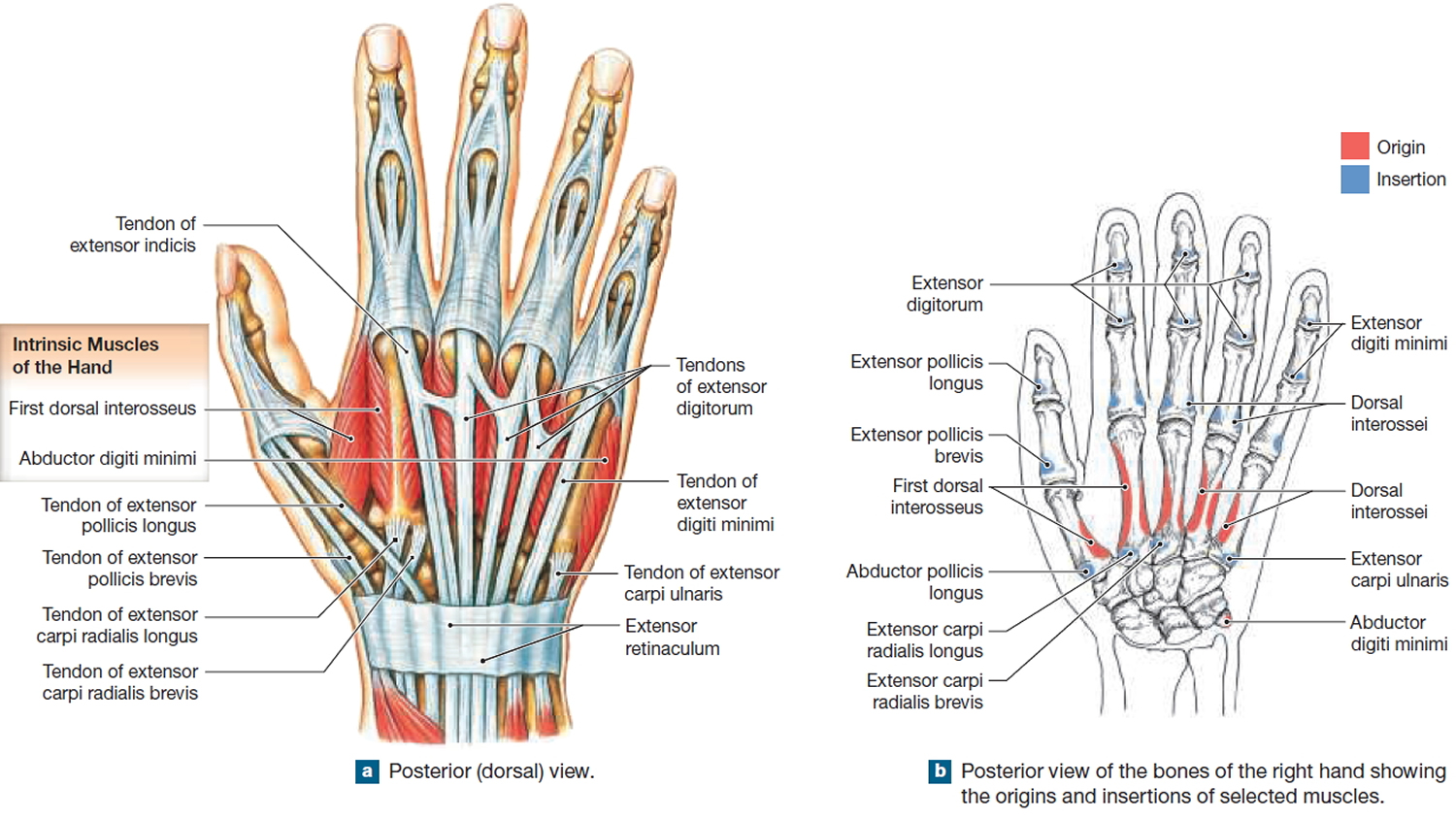
Figure 11. Muscles of the hand (back view)
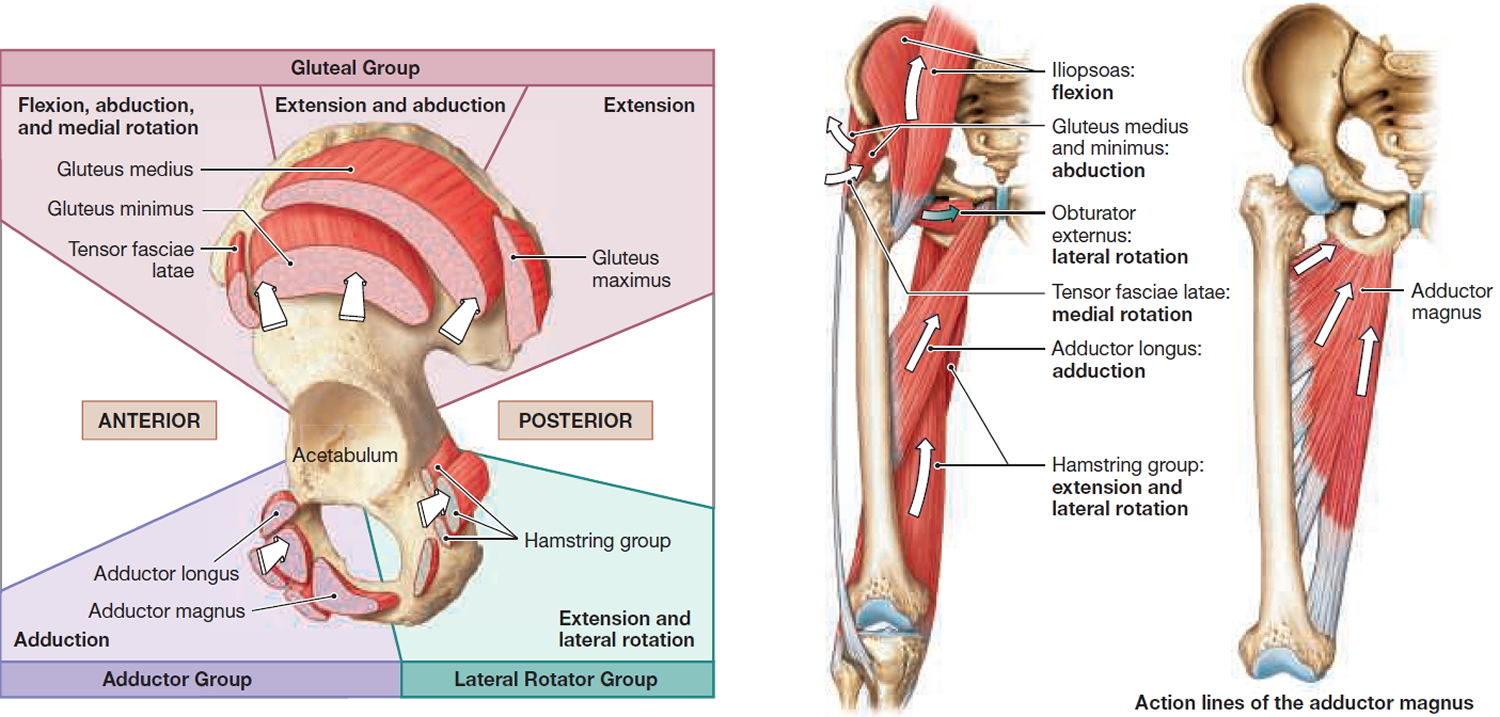
Muscles That Move the Thigh – Groin muscles
The hip joint, like the shoulder joint, is a multiaxial synovial joint that flexes, extends, adducts, abducts, medially rotates, and laterally rotates. The movement at the joint depends on the anatomy of the joint and its axes of movement. The large, powerful muscles that move the thigh originate on the pelvis. These muscles include the gluteal group, lateral rotator group, adductor group, and iliopsoas group. Three gluteal muscles cover the lateral surface of the ilium. The gluteus maximus is the largest and most superficial of the gluteal muscles. It originates on the posterior gluteal line and parts of the iliac crest; the sacrum, coccyx, and associated ligaments; and the thoracolumbar fascia. This muscle extends and laterally rotates the thigh at the hip. The gluteus maximus shares an insertion with the tensor fasciae latae, which originates on the iliac crest and lateral surface of the anterior superior iliac spine. Together, these muscles pull on the iliotibial tract, a band of collagen fibers that extends along the lateral surface of the thigh and inserts on the tibia. This tract braces the lateral surface of the knee and stabilizes the knee when a person balances on one foot.
The gluteus medius and gluteus minimus originate anterior to the gluteus maximus and insert on the greater trochanter of the femur. Both abduct and medially rotate the thigh at the hip. The anterior gluteal line on the lateral surface of the ilium marks the boundary between the gluteus medius and gluteus minimus.
The lateral rotators laterally rotate the thigh at the hip. In addition, the piriformis obturator muscles and the gemelli muscles abduct the thigh at the hip. The dominant lateral rotators of this group are the piriformis, obturator externus, and obturator internus.
The adductors are found inferior to the acetabulum. The adductor magnus, adductor brevis, adductor longus, pectineus and gracilis all originate on the pubis. Except for the gracilis, all of these muscles insert on the linea aspera, a ridge along the posterior surface of the femur. The gracilis inserts on the tibia. Their actions are varied. All of the adductors except the adductor magnus originate both anterior and inferior to the hip, so they are flexors, adductors, and medial rotators of the thigh at the hip. The adductor magnus adducts, flexes, and medially rotates, or extends and laterally rotates, the thigh at the hip, depending on which region of the muscle is stimulated.
When an athlete pulls a groin muscle, he or she has torn one of these adductor muscles.
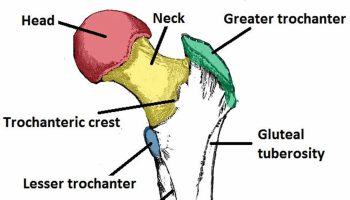
The medial surface of the pelvis is dominated by a single pair of muscles: the psoas major and iliacus. The psoas major originates on the inferior thoracic and lumbar vertebrae and inserts onto the lesser trochanter of the femur. The tendon of the psoas major muscle joins with the tendon of the iliacus, which originates on the iliac fossa. These two muscles are powerful flexors of the hip, and they pass deep to the inguinal ligament. They are often referred to together as the iliopsoas. One way to organize the diverse muscles is to group them by their orientation around the hip. Muscles that originate on the pelvis and insert on the femur produce characteristic movements determined by their position relative to the acetabulum.
Figure 12. Muscles that move the thigh
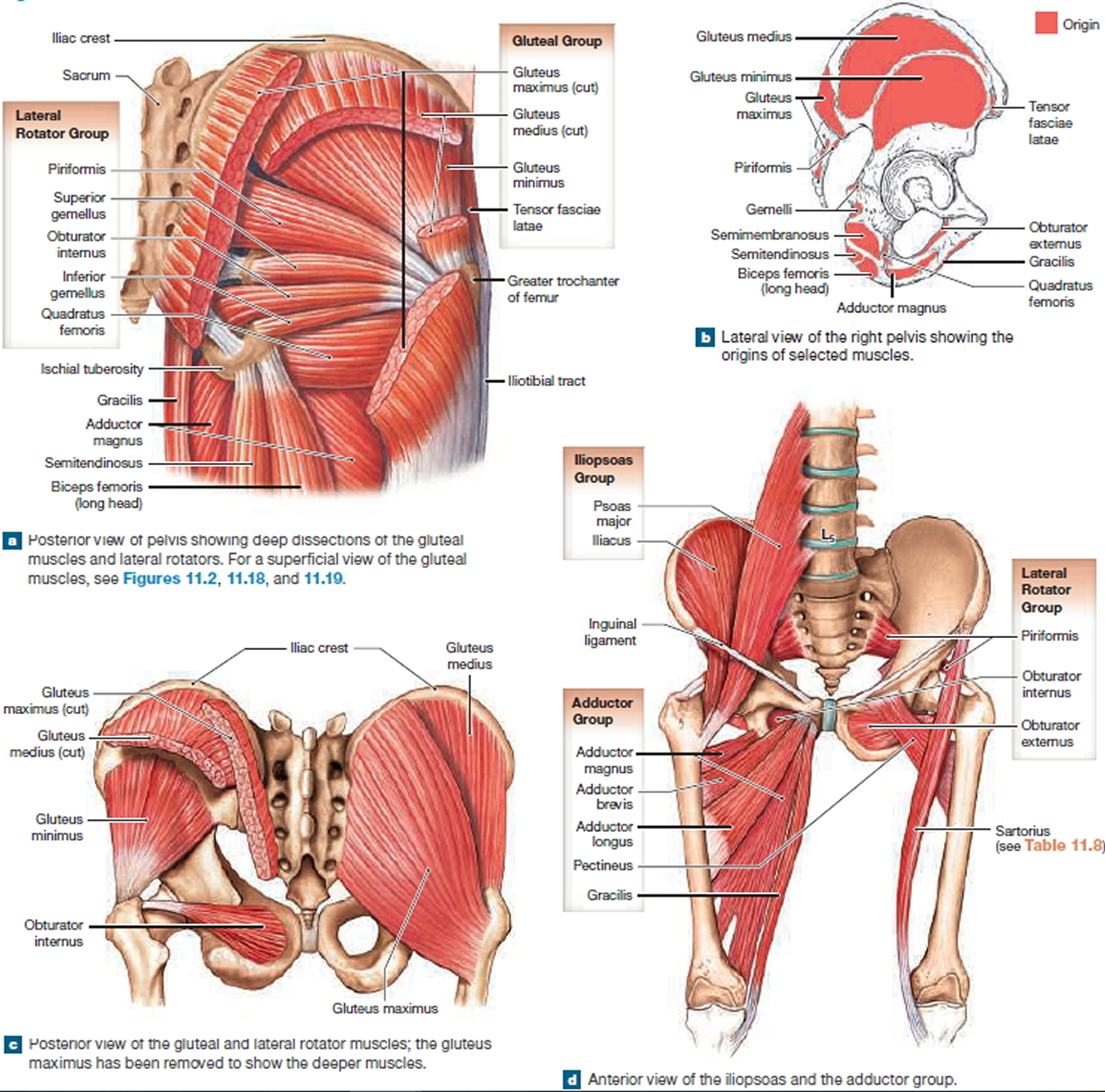
Figure 13. Groin (hip joint) muscles and actions at the hip and thigh
Muscles That Move the Leg
Muscles that move the leg are detailed in Figure 14. You can use the relationships between the action lines and the axis of the knee joint to predict the actions of the muscles that move the leg at the knee. However, the anterior/posterior orientation of the muscles that move the leg is reversed. This is related to the rotation of the limb during embryological development. Therefore: Muscles that have action lines passing anteriorly to the axis of the knee joint, such as the quadriceps femoris, extend the knee. Muscles that have action lines passing posteriorly to the axis of the knee joint, such as the hamstrings, flex the knee. Most of the extensor muscles originate on the femur and extend along the anterior and lateral surfaces of the thigh. Flexor muscles originate on the pelvis and extend along the posterior and medial surfaces of the thigh.
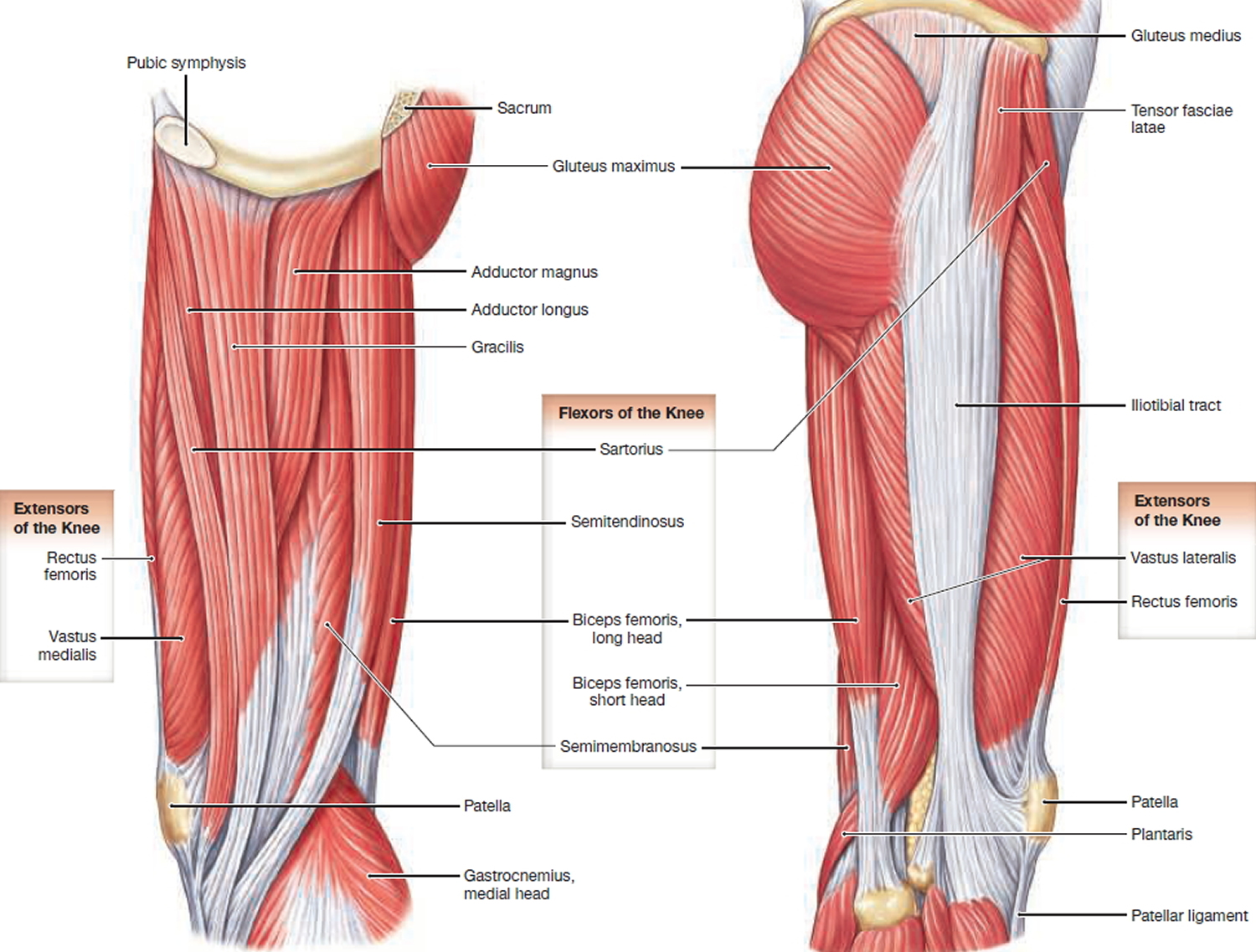
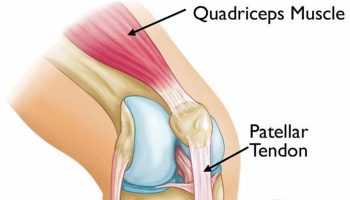
Collectively, the knee extensors are called the quadriceps femoris, or the quadriceps muscles. Three of the quadriceps muscles, the vastus muscles (vastus lateralis, vastus medialis, and vastus intermedius), originate on the femur, and the rectus femoris originates on the anterior inferior iliac spine. All of these muscles insert onto the tibial tuberosity by the quadriceps tendon, patella, and patellar ligament. The three vastus muscles surround the rectus femoris the same way a bun surrounds a hot dog. The vastus lateralis, vastus medialis, and vastus intermedius extend the knee. Because the rectus femoris originates on the anterior inferior iliac spine of the pelvis, it crosses the hip and the knee joints, so it flexes the hip and extends the knee.
The flexors of the knee are the biceps femoris, semimembranosus, semitendinosus and sartorius. These muscles originate on the pelvis and insert on the tibia and fibula. Because the long head of the biceps femoris and the semimembranosus and semitendinosus originate on the pelvis inferior and posterior to the acetabulum, they also cross the hip joint and, therefore, extend the hip. These muscles are often called the “hamstrings.” The sartorius is the only knee flexor that originates superior to the acetabulum. It inserts on the medial aspect of the tibia. The sartorius flexes, abducts, and laterally rotates the hip and also flexes the knee.
the knee joint can be locked at full extension by a slight lateral rotation of the tibia. The small popliteus originates on the femur near the lateral condyle and inserts on the posterior tibial shaft. When the knee starts to flex, this muscle contracts and medially rotates the tibia, unlocking the knee joint.
Figure 14. Muscles that move the leg (front view)
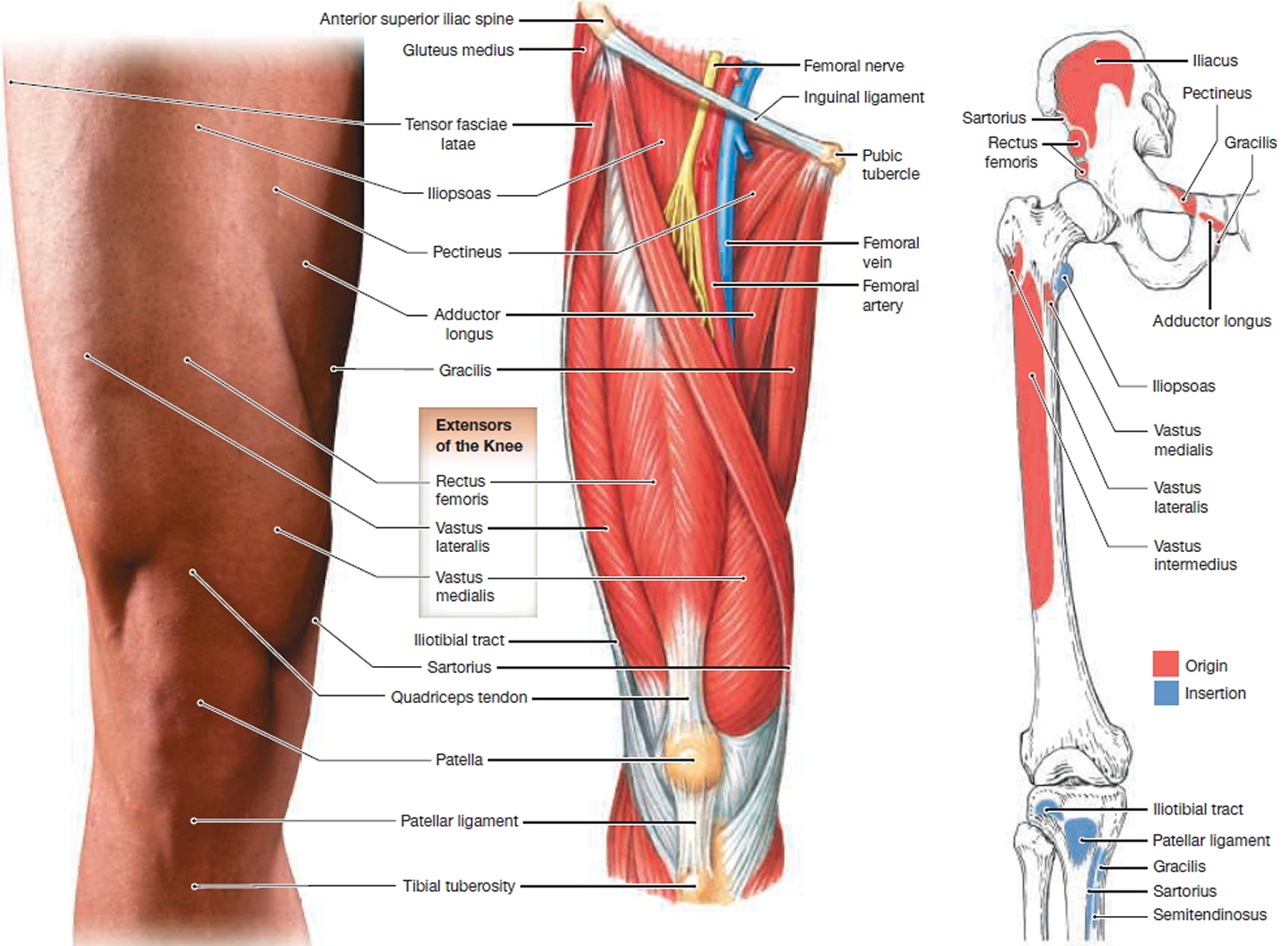
Figure 15. Muscles that move the leg (back view)
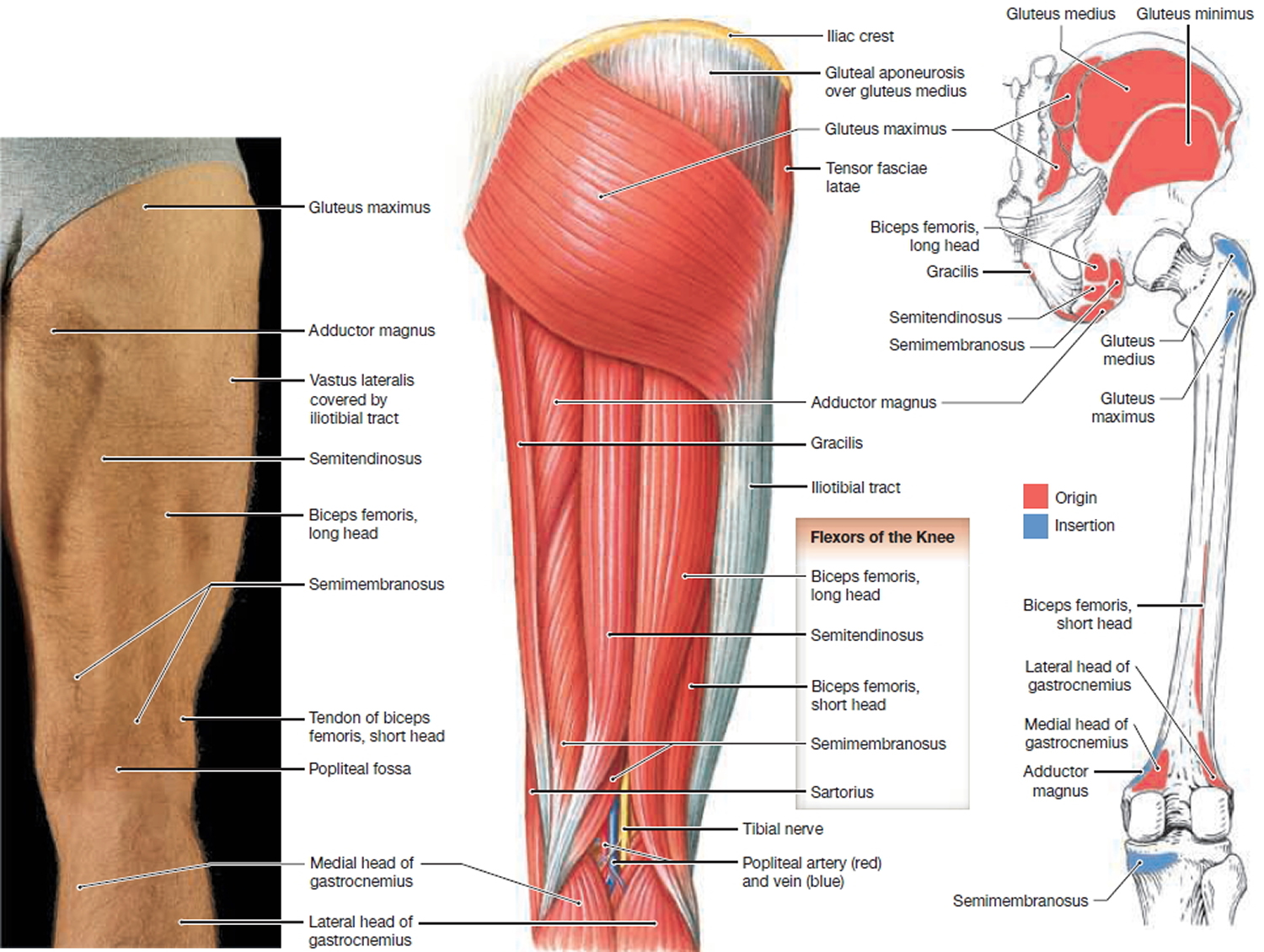
Figure 16. Muscles that move the leg (side view)
Calf muscles – Muscles That Move the Foot and Toes
Extrinsic muscles of the foot move the foot and toes. Figure 16 show the extrinsic muscles of the foot. The large gastrocnemius and the underlying soleus are plantar flexors of the foot. The soleus is a synergist to the gastrocnemius, increasing the speed and force of the plantar flexion. The gastrocnemius originates on the medial and lateral condyles of the femur. A sesamoid bone, called the fabella, is sometimes found in the tendon of the lateral head of the gastrocnemius. The gastrocnemius and soleus insert onto the calcaneal tendon (commonly called the “Achilles tendon”).
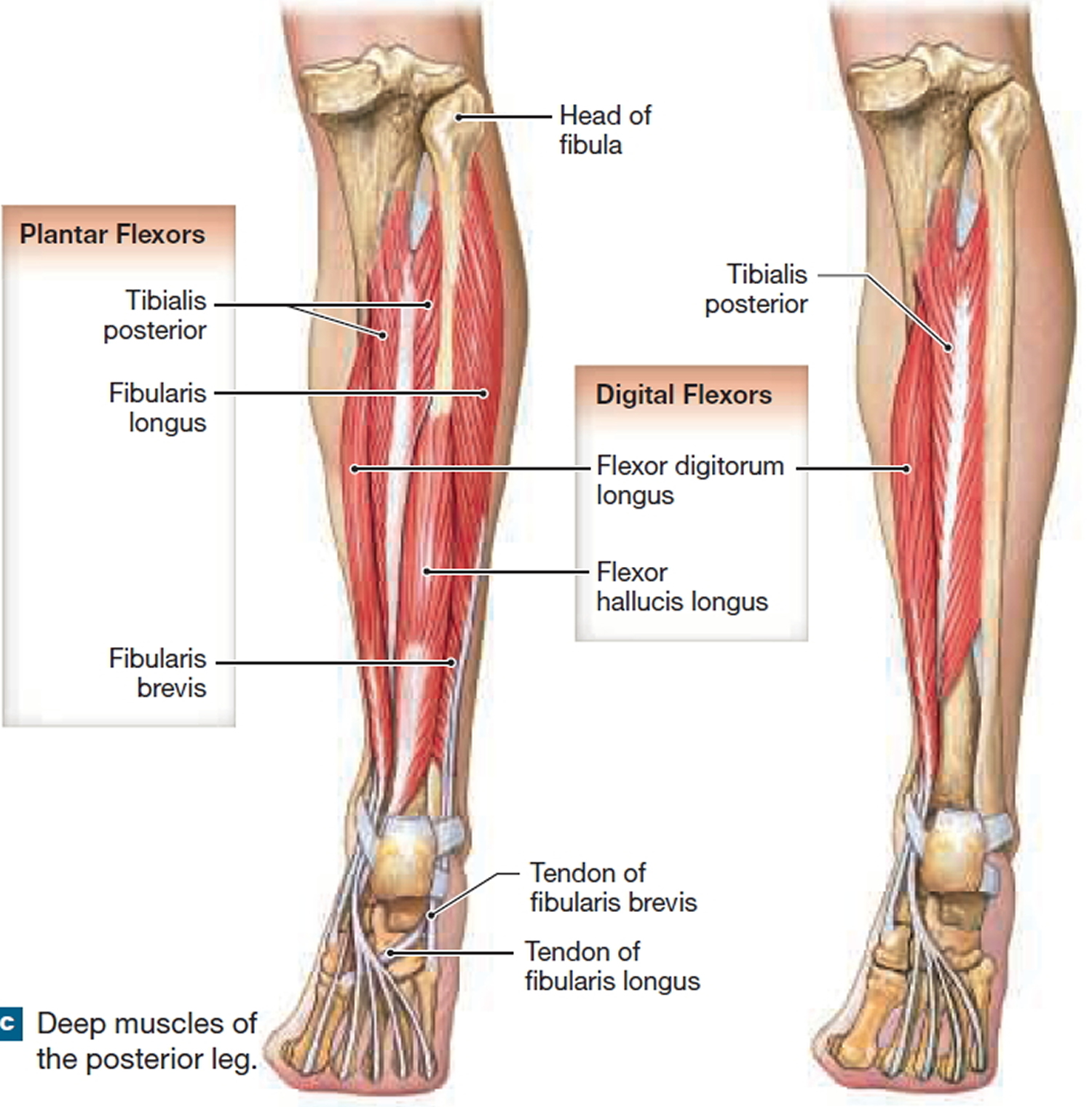
The two fibularis longus and fibularis brevis (peroneus longus and peroneus brevis) lie partially deep to the gastrocnemius and soleus. These muscles plantar flex and evert the ankle. The tibialis anterior dorsiflexes and inverts the foot and is an antagonist to the gastrocnemius. Muscles that flex or extend the toes originate on the tibia, the fibula, or both. Large tendon sheaths surround the tendons of the tibialis anterior, extensor digitorum longus, and extensor hallucis longus where they cross the ankle joint. The superior extensor retinaculum and inferior extensor retinaculum stabilize these tendon sheaths.
Figure 17. Calf muscles that move the leg and foot – superficial muscles
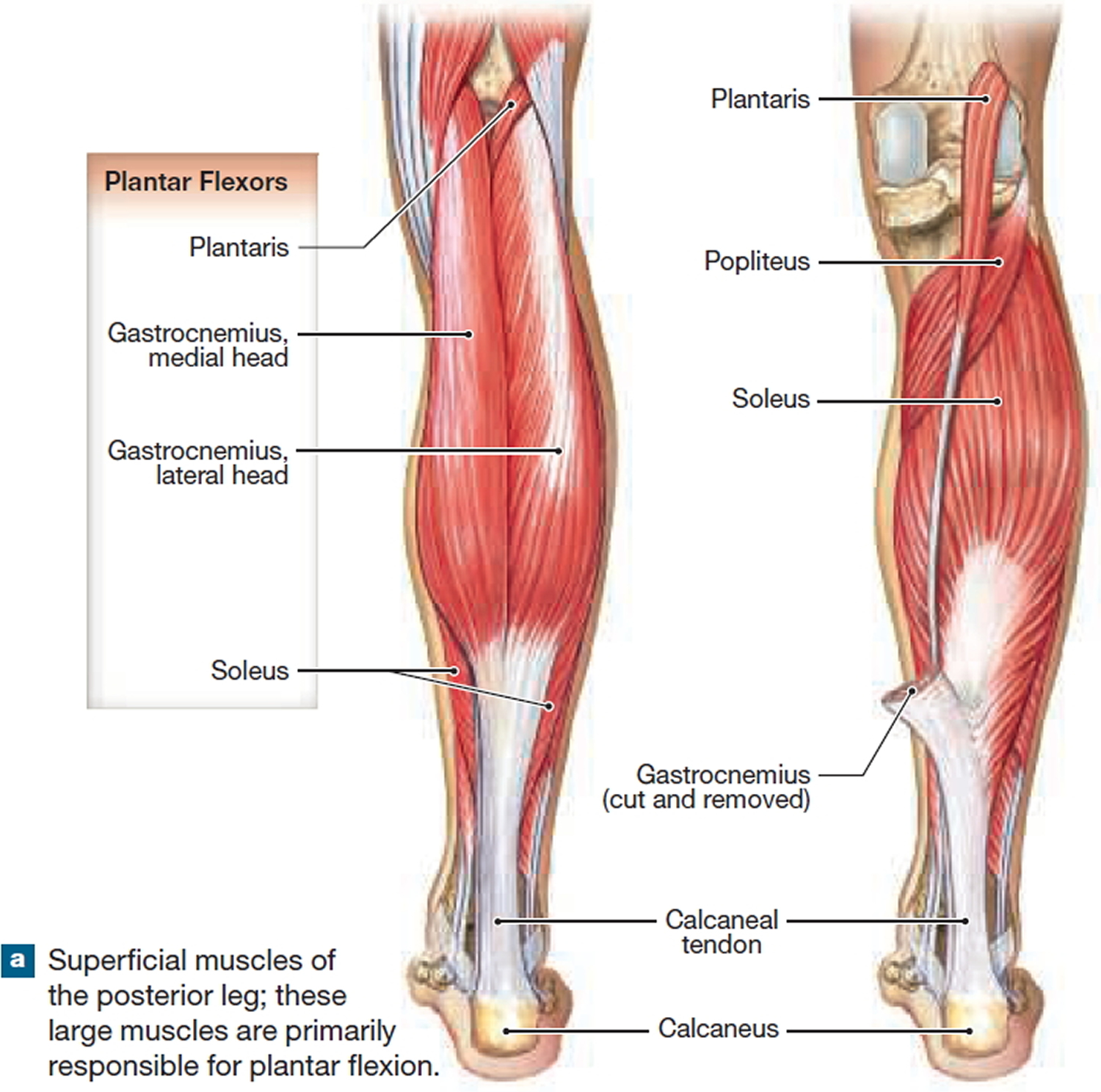
Figure 18. Calf muscles that move the leg and foot – deep muscles

{kind=link}