Contents
What is myopia
Myopia also known as nearsightedness or short-sightedness. Myopia occurs when the eyeball grows too long and prevents incoming light from focusing directly on the retina. Myopia (nearsightedness) may also be caused by an abnormal shape of the cornea that is too curved for the length of the eyeball or a lens that is too thick.
Myopia (nearsightedness) develops in eyes that focus images in front of the retina instead of on the retina, which results in blurred vision. This occurs when the eyeball becomes too long
Instead of focusing images on the retina—the light-sensitive tissue in the back of the eye—the lens of the eye focuses the image in front of the retina. People with myopia have good near vision but poor distance vision.
People with myopia can typically see well enough to read a book or computer screen (nearsightedness or short-sightedness), but struggle to see objects farther away. Sometimes people with undiagnosed myopia have headaches and eyestrain from struggling to clearly see things in the distance.
Signs that your child may be nearsighted can include:
- needing to sit near the front of the class at school because they find it difficult to read the whiteboard
- sitting close to the TV
- complaining of headaches or tired eyes
- regularly rubbing their eyes
Myopia (nearsightedness) can range from mild, where treatment may not be required, to severe, where a person’s vision is significantly affected (see high myopia below).
The nearsightedness usually starts around puberty and gets gradually worse until the eye is fully grown, but it can also develop in very young children.
About 42 percent of Americans ages 12-54 are nearsighted, up from 25 percent in 1971 1. A recent review 2 reports that myopia prevalence varies by ethnicity. East Asians show the highest prevalence, reaching 69 percent at 15 years of age. Blacks in Africa had the lowest prevalence at 5.5 percent at 15 years of age. Children from urban environments are more than twice as likely to be myopic as those from rural environments.
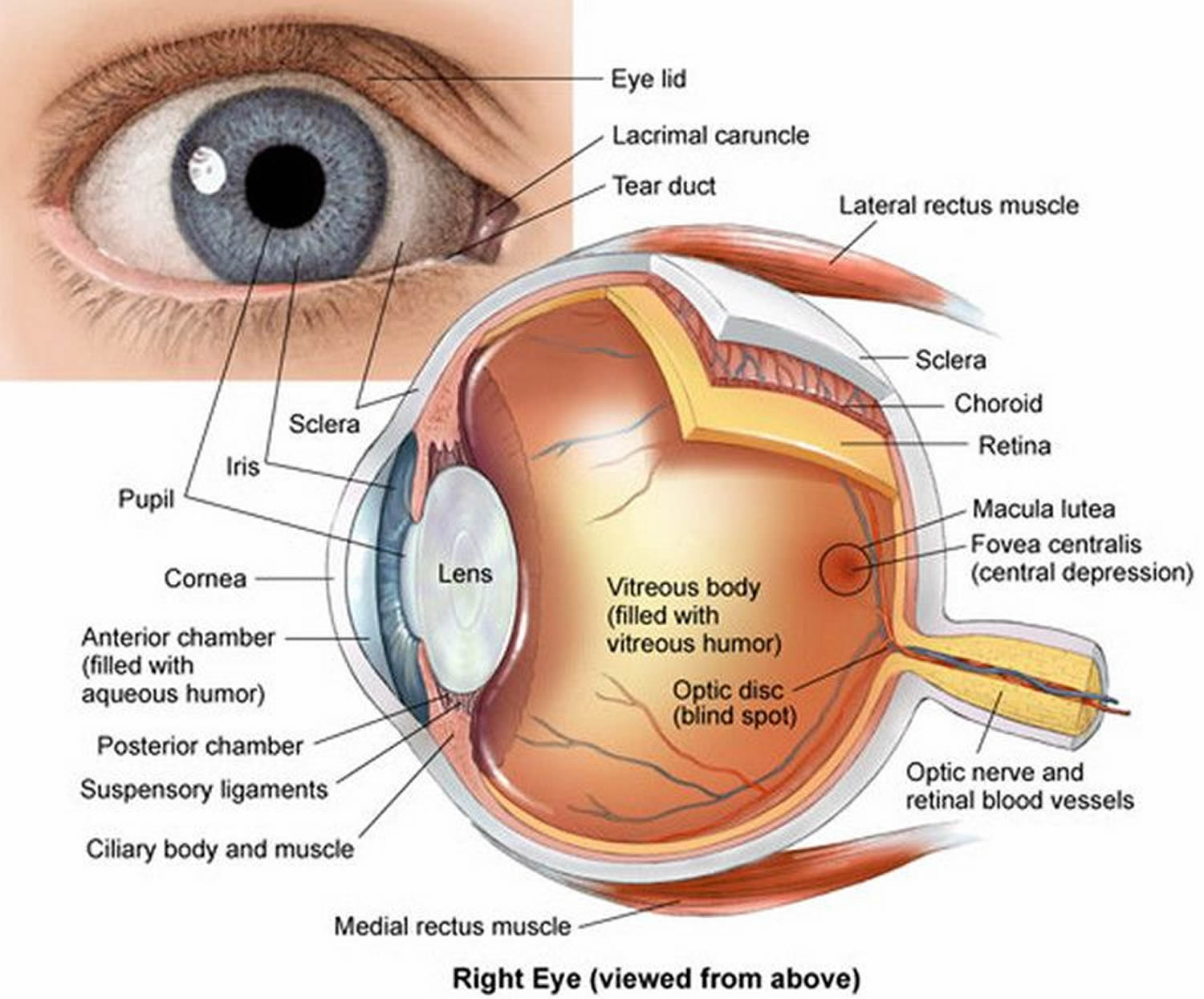
Figure 1. Eye anatomy
Normal vision
To focus the images it sees, your eye relies on two critical parts:
- The cornea, the clear front surface of your eye
- The crystalline lens, a clear structure inside your eye that changes shape to help focus objects
In a normally shaped eye, each of these focusing elements has a perfectly smooth curvature like the surface of a smooth rubber ball. A cornea and lens with such curvature bend (refract) all incoming light in such a way as to make a sharply focused image on the retina, at the back of your eye.
Figure 2. Normal eye refraction (perfect image on the Macula’s Fovea)
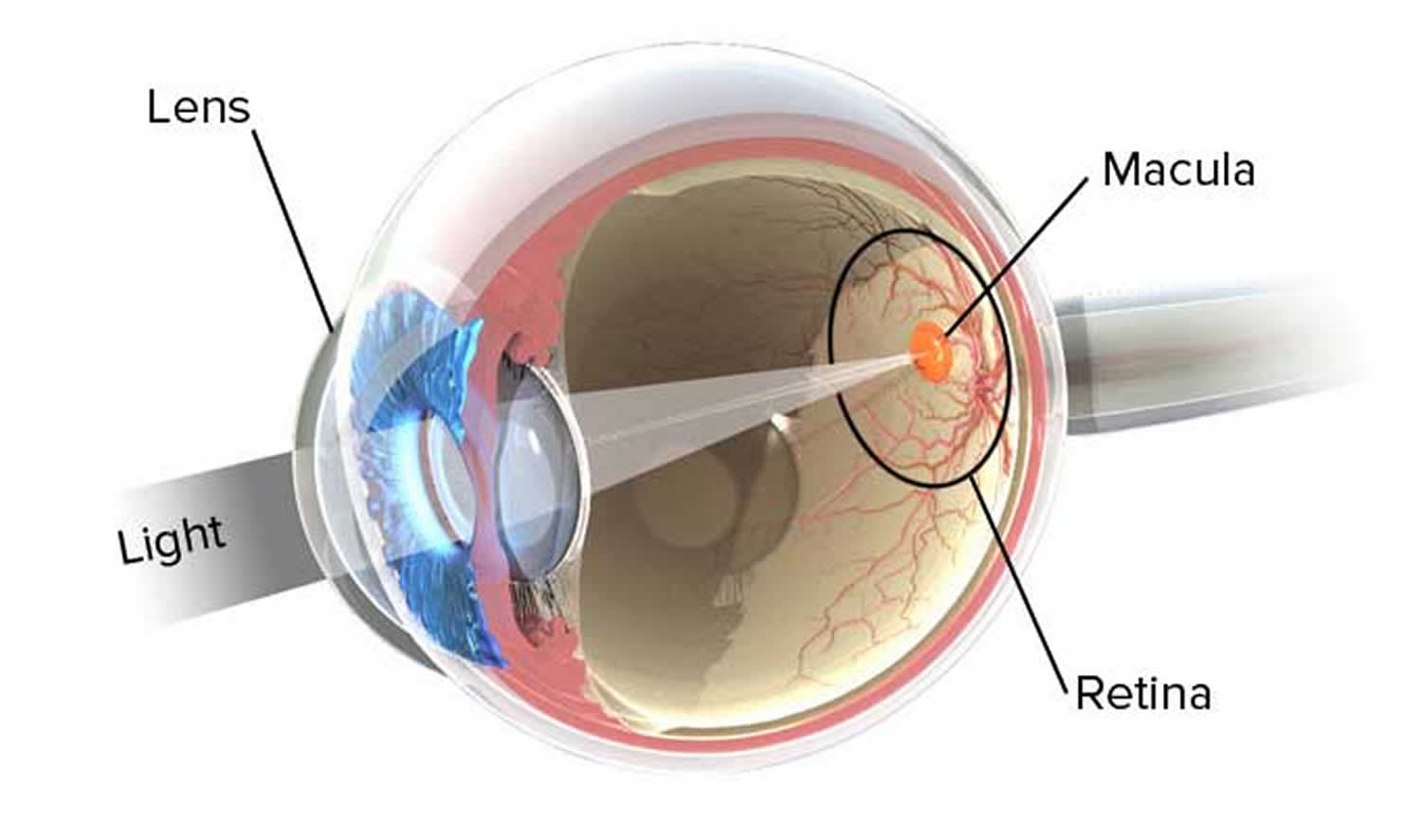
Figure 3. Myopia (nearsightedness)
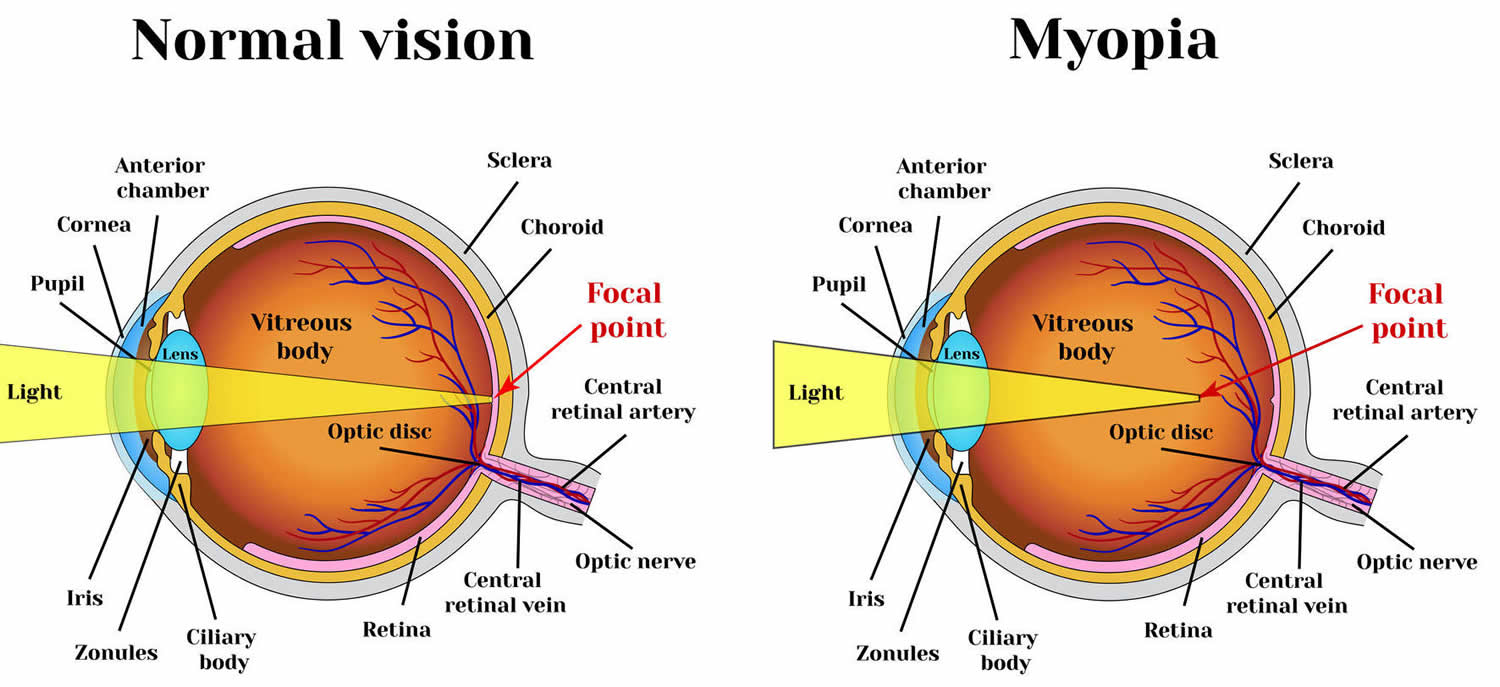 Note: In a normal eye, the light focuses on the retina. With myopia, the eye is too long and focuses light in front of the retina.
Note: In a normal eye, the light focuses on the retina. With myopia, the eye is too long and focuses light in front of the retina.
Myopia causes
Scientists are unsure why the eyeball sometimes grows too long. In 2013, the Consortium for Refractive Error and Myopia 3, an international team of vision scientists, discovered 24 new genetic risk factors for myopia. Some of these genes are involved in nerve cell function, metabolism, and eye development. Alone, each gene has a small influence on myopia risk; however, the researchers found that individuals carrying greater numbers of the myopia-prone versions of the genes have a up to tenfold increased risk of myopia.
Although genetics plays a role in myopia, the recent dramatic increase in the prevalence of myopia documented by several studies in the U.S. and other countries points to environmental causes such as lack of time spent outdoors and greater amount of time spent doing near-work, such as reading, writing, and working on a computer.
In 1999, the Collaborative Longitudinal Evaluation of Ethnicity and Refractive Error 4, a long-term study following the eye development of more than 1,200 children ages 6 to 14, the age range during which myopia typically develops. Collaborative Longitudinal Evaluation of Ethnicity and Refractive Error researchers found that children who spent more time outdoors had a smaller chance of becoming nearsighted 5. The researchers also showed that time spent outside is independent from time spent reading, providing evidence against the assumption that less time outside means more time doing near work.
Researchers are unsure why time outdoors helps prevent the onset of myopia. Some suggest natural sunlight may provide important cues for eye development. Other researchers suggest that normal eye development may require sufficient time looking at distant objects. Curiously, once myopia has begun to develop, time outdoors does not appear to slow its progression, the researchers found.
Risk factors for developing myopia
Certain risk factors may increase the likelihood of developing nearsightedness, such as:
- Family history. Nearsightedness tends to run in families. If one of your parents is nearsighted, your risk of developing the condition is increased. The risk is even higher if both parents are nearsighted.
- Reading. People who do a lot of reading may be at increased risk of myopia.
- Environmental conditions. Some studies support the idea that a lack of time spent outdoors may increase the chances of developing myopia.
High myopia
Conventionally, an eye is considered to have high myopia if it requires -6.0 diopters or more of lens correction. Diopters indicate lens strength. High myopia increases the risk of retinal detachment. The retina is the tissue in the back part of the eye that signals the brain in response to light. When it detaches, it pulls away from the underlying tissue called the choroid. Blood from the choroid supplies the retina with oxygen and nutrients.
High myopia can also increase the risk of cataract and glaucoma. Cataract is the clouding of eye’s lens. Glaucoma is a group of diseases that damage the optic nerve, which carries signals from the retina to the brain. Each of these conditions can cause vision loss.
Pathological myopia
A condition called pathological myopia (also called degenerative or malignant myopia) sometimes occurs in eyes with high myopia when the excessive elongation of the eye causes changes in the retina, choroid, vitreous, sclera, and/or the optic nerve (see Figure 1). The vitreous is the gel-like substance that fills the center of the eye. The sclera is the outer white part of the eye.
Symptoms of pathological myopia typically first appear in childhood and usually worsen during adolescence and adulthood. Treatment cannot slow or stop elongation of the eye; however, complications such as retinal detachment, macular edema (build-up of fluid in the central part of the retina), choroidal neovascularization (abnormal blood vessel growth), and glaucoma usually can be treated.
Myopia Complications
Nearsightedness may be associated with several complications, such as:
- Reduced quality of life. Uncorrected nearsightedness can affect your quality of life. You might not be able to perform a task as well as you wish. And your limited vision may detract from your enjoyment of day-to-day activities.
- Eyestrain. Uncorrected nearsightedness may cause you to squint or strain your eyes to maintain focus. This can lead to eyestrain and headaches.
- Impaired safety. Your own safety and that of others may be jeopardized if you have an uncorrected vision problem. This could be especially serious if you are driving a car or operating heavy equipment.
- Other eye problems. Severe nearsightedness puts you at a slightly increased risk of retinal detachment, glaucoma and cataracts.
Is there a cure for myopia?
Unfortunately, nearsightedness in children tends to get worse as they grow.
The younger they are when they start becoming nearsighted, generally the faster their vision deteriorates and the more severe it is in adulthood. Nearsightedness usually stops getting worse at around 20 years of age.
There’s currently no single treatment available that appears to stop this progression. However, it may be slowed by treatments involving eye drops of a medication called atropine, or special contact lenses
Research has shown that atropine eye drops can slow the progression of nearsightedness, but it can cause side effects at high strengths – such as difficulty reading and sensitivity to bright light.
Orthokeratology and bifocal contact lenses may also slow down short-sight progression in children, but possibly not as much as the eye drops, and they carry small risks.
Myopia symptoms
Nearsightedness symptoms may include:
- Blurry vision when looking at distant objects
- The need to squint or partially close the eyelids to see clearly
- Headaches caused by eyestrain
- Difficulty seeing while driving a vehicle, especially at night (night myopia)
Nearsightedness is often first detected during childhood and is commonly diagnosed between the early school years through the teens. A child with nearsightedness may:
- Persistently squint
- Need to sit closer to the television, movie screen or the front of the classroom
- Seem to be unaware of distant objects
- Blink excessively
- Rub his or her eyes frequently
Regular eye exams
Since it may not always be readily apparent that you’re having trouble with your vision, the American Academy of Ophthalmology recommends the following intervals for regular eye exams:
Adults
If you’re at high risk of certain eye diseases, such as glaucoma, get an eye exam every two to four years up to age 40, then every one to three years between 40 and 54, and every one to two years beginning at age 55.
If you don’t wear glasses or contacts, have no symptoms of eye trouble, and are at a low risk of developing eye diseases, such as glaucoma, get an eye exam at the following intervals.
- An initial exam at 40
- Every two to four years between ages 40 and 54
- Every one to three years between ages 55 and 64
- Every one to two years beginning at age 65
If you wear glasses or contacts, you’ll likely need to have your eyes checked regularly. Ask your eye doctor how frequently you need to schedule your appointments. But, if you notice any problems with your vision, schedule an appointment with your eye doctor as soon as possible, even if you’ve recently had an eye exam. Blurred vision, for example, may suggest you need a prescription change, or it could be a sign of another problem.
Children and adolescents
Children need to be screened for eye disease and have their vision tested by a pediatrician, an ophthalmologist or another trained screener at the following ages and intervals.
- During the newborn period
- At well-child visits until school age
- During school years, every one to two years at well-child visits, or through school or public screenings
Myopia diagnosis
If you think you or your child may be nearsighted, you should book an eye test at a local optometrist (someone who’s been specially trained to examine the eyes).
You should have a routine eye test at least every two years, but you can have a test at any point if you have any concerns about your vision.
An eye test can confirm whether you’re short or long-sighted, and you can be given a prescription for glasses or contact lenses to correct your vision.
Nearsighted test
An eye care professional can diagnose myopia during a comprehensive eye exam, which includes testing vision and examining the eye in detail. When possible, a comprehensive eye exam should include the use of dilating eyedrops to open the pupils wide for close examination of the optic nerve and retina.
An eye care professional can quickly identify lenses that best correct a patient’s vision using a device called a phoropter. In younger children, a technique called retinoscopy helps the eye doctor determine the correction required. The results are written as a prescription.
A number of different tests will usually be carried out as part of your eye test, possibly including:
- measurements of the pressure inside your eyes
- checks to measure how well your eyes work together
- visual acuity tests – where you’re asked to read from a chart that has rows of letters that get smaller on each line
- retinoscopy – where a bright light is shone into your eye to see how your eye reacts to it
If the tests detect a possible problem with your distance vision, you may be asked to repeat the visual acuity tests while different strength lenses are placed in front of your eyes. This will help the optometrist to determine what your glasses prescription should be.
Understanding your glasses prescription
If an eye test finds that you’re nearsighted, you’ll be given a prescription that describes what lenses you need to improve your vision. This can be used to make glasses or contact lenses.
Your prescription will usually consist of three main numbers for each eye. These are:
- Sph (sphere) – a positive number here indicates that you’re long-sighted, while a negative number indicates that you’re short-sighted
- Cyl (cylinder) – this number indicates whether you have astigmatism (where the front of your eye isn’t perfectly curved)
- Axis – this describes the angle of any astigmatism you have
If you’re short-sighted, the Sph number is the most relevant. This is given in a measurement called diopters (D), which describes how severely short-sighted you are.
A score of -0.5D to -3D is usually considered to be mild myopia, while a score of more than -6D (minus 6 diopters) is considered to be severe or “high” myopia.
Myopia treatment
The most common way to treat myopia is with corrective myopia glasses or contact lenses, which refocus light onto the retina. Contact lenses can cause complications (e.g., dry eye, corneal distortion, immunologic reaction, infection), but may be advantageous for activities where glasses are not practical (e.g., certain sports).
Refractive surgery is an option once the optic error of the eye has stabilized, usually by the early 20s. The most common types of refractive surgery are laser-assisted in situ keratomileusis (LASIK) and photorefractive keratectomy (PRK). Both change the shape of the cornea to better focus light on the retina.
LASIK (Laser-Assisted In Situ Keratomileusis) removes tissue from the inner layer of the cornea. To do this, a thin section of the outer corneal surface is cut and folded back to expose the inner cornea. A laser removes a precise amount of tissue to reshape the cornea and then the flap is placed back in position to heal. The correction possible with LASIK is limited by the amount of corneal tissue that can be safely removed.
PRK (photorefractive keratectomy) also removes a layer of corneal tissue, but does so without creating a surface flap. Instead, the corneal surface cells are removed prior to the laser procedure. For this reason, PRK requires a longer healing time, as the surface cells have to grow back to cover the corneal surface. As with LASIK surgery, PRK is limited to how much tissue safely can be removed.
Implanting artificial lenses in the eyes is a fairly new technique that is very occasionally used if laser surgery is ineffective or not possible (such as people with very severe short-sightedness). Phakic intraocular lenses (IOLs) are an option for people who are very nearsighted or whose corneas are too thin to allow the use of laser procedures such as LASIK and PRK. Phakic lenses are surgically placed inside the eye to help focus light onto the retina.
Nearsighted glasses
Nearsightedness can usually be corrected using glasses made specifically to your prescription. See diagnosing nearsightedness for more information about what your prescription means.
Wearing a lens that is made to your prescription will ensure that light is focused onto the back of your eye (retina) correctly, so that distant objects don’t appear as blurry.
The thickness and weight of the lenses you need will depend on how nearsighted you are.
Your eyesight often changes as you get older, which means you may eventually need to use two pairs of glasses – one pair for close vision activities such as reading and the other pair for distance vision activities such as watching television.
Some people prefer to use bifocal lenses that allow them to see objects clearly that are both close up and far away without changing their glasses.
You can also get multifocal lenses that help you see nearby objects and those at middle and long distances (varifocal glasses).
Contact lenses
Contact lenses can also be used to correct vision in the same way as glasses. Some people prefer contact lenses to glasses because they are lightweight and almost invisible, but some people find them more of a hassle than wearing glasses.
Contact lenses can be worn on a daily basis and discarded each day (daily disposables), or they can be disinfected and reused. They can also be worn for a longer period of time, although eye specialists generally recommend that contact lenses are not worn overnight because of the risk of infection.
Some opticians very occasionally use a technique called orthokeratology. This involves wearing a hard contact lens overnight to flatten the curvature of the cornea (transparent layer at the front of the eye) so you can see better without a lens or glasses during the day. It’s not a cure for nearsightedness because the cornea usually returns to its normal shape, but it may reduce reliance on lenses for some people.
Your optician can advise you about the most suitable type of contact lenses for you. If you decide to wear contact lenses, it is very important that you maintain good lens hygiene to prevent eye infections.
Contact lens safety
Cleaning and using your contact lenses properly will help keep your eyes healthy and free from infections.
DO:
- wash, rinse and dry your hands thoroughly before touching your lenses
- only wear your contacts for the recommended time
- always have an up-to-date pair of glasses for when you take your lenses out
- have regular contact lens check-ups, even if everything seems OK
- get advice straight away if you’re having any problems with your contact lenses, such as sore, red or swollen eyes
DON’T:
- wear any contact lenses, including novelty lenses, that haven’t been properly fitted to your eyes
- put water or saliva on your lenses or in your eye when you’re wearing them
- pick up a dropped lens and put it straight back into your eye without cleaning it thoroughly
- carry on wearing your lenses if they don’t look good, feel good or your vision is blurry
- use a lens if it looks damaged
- sleep in your lenses unless your contact lens practitioner says it’s OK to do this
- wear your lenses while swimming or playing water sports
- wear your lenses in the shower or hot tub
- wear someone else’s contact lenses or share your lenses with anyone
- reuse a daily disposable lens
- use eyedrops while wearing your lenses unless your contact lens practitioner or ophthalmologist says it’s safe to do this
Soft, daily disposable contact lenses
Daily disposable lenses don’t need cleaning or disinfecting because they’re only worn once then thrown away.
To keep your eyes healthy if you wear disposable lenses:
- make sure you put them in the right way round
- check them for faults or damage before putting them in
- never re-use them
Reusable contact lenses
There are two types of reusable lenses: soft and hard.
- soft reusable lenses – these can be reused daily for a set period of time, usually one week or one month
- hard reusable lenses – also known as rigid gas permeable (RGP) lenses, these can be reused every day for up to a year
Soft and hard reusable lenses both have to be disinfected with contact lens solution every day to prevent infections. Your contact lens prescriber will tell you how to do this.
To look after your reusable lenses safely:
- clean your lenses after you take them out by rubbing them with your contact lens solution
- rinse your lenses with contact lens solution after cleaning them
- leave them in the disinfecting solution overnight
- never reuse disinfecting solution or top it up – throw it away and use fresh solution every time
- only use the solution recommended by your contact lens practitioner, and follow the instructions carefully
- follow your practitioner’s instructions for cleaning your storage case (don’t use tap water)
- replace your lens case at least once a month
- never decant your solution into smaller travel-size bottles
When to get medical help
If in doubt, take your lenses out and go to your prescriber or local eye casualty department.
Get advice straightaway if you have:
- blurred vision
- painful, red or swollen eyes
- a white or yellow spot over the colored part of your eye
Laser eye surgery
Laser eye surgery involves using a laser to burn away small sections of your cornea to correct the curvature, so light is better focused onto your retina.
There are three main types of laser eye surgery:
- photorefractive keratectomy (PRK) – where a small amount of the cornea’s surface is removed and a laser is used to remove tissue and change the shape of the cornea
- laser epithelial keratomileusis (LASEK) – similar to PRK, but involves using alcohol to loosen the surface of the cornea, so a flap of tissue can be lifted out of the way, while a laser is used to alter the shape of the cornea; the flap is put back in place afterwards
- laser in situ keratectomy (LASIK) – similar to LASEK, but a smaller flap of cornea is created
These procedures are usually carried out on an outpatient basis, so you won’t normally have to stay in hospital overnight. The treatment usually takes less than 30 minutes to complete. A local anesthetic is used to numb your eyes while it’s carried out.
Which procedure is best?
All three laser eye surgery techniques produce similar results, but they tend to have different recovery times.
LASEK or LASIK are usually the preferred methods, as they cause almost no pain and your vision will usually start to recover within a few hours or days. However, your vision may not fully stabilize for up to a month.
PRK can be a bit painful and it can take several months for your vision to stabilize afterwards.
LASIK can only be carried out if your cornea is thick enough. If your cornea is thin, the risk of complications occurring, such as loss of vision, is too high. LASEK and PRK may be possible if your cornea is not thick enough for LASIK.
The results of all three techniques are usually good. While it may not always be possible to completely cure your nearsightedness, around 9 out of 10 people experience a significant improvement in their vision and many are able to meet the minimum vision requirements for driving.
Risks and complications
Laser eye surgery does carry risks, including:
- dry eyes – this will usually last a few months, during which time you can lubricate your eyes with special eye drops
- removal of too much cornea tissue – this occurs in around 1 in 20 cases and could leave you with an eye that is long-sighted
- reduced night vision – this usually passes within six weeks
- a haze effect around bright lights – this will usually pass within 6 to 12 months
There’s also a small risk of potentially serious complications that could threaten your vision, such as the cornea becoming too thin or infected. However, these problems are rare, occurring in less than 1 in every 500 cases.
Make sure you understand all the risks involved before deciding to have laser eye surgery.
In the Patient Reported Outcomes with LASIK study 6, up to 28 percent of people experienced dry eye symptoms after LASIK. In the same study, up to 40 percent of patients undergoing LASIK experienced side effects such as ghosting of images, starbursts, glare, and halos, especially at night. Nevertheless, less than 1 percent of patients experienced difficulty performing their usual activities following LASIK surgery due to any one symptom and 95 percent of participants said they were satisfied with their vision 6.
An important consideration for people considering refractive surgery is that a nearsighted person who can comfortably read without glasses will likely require reading glasses if good distance vision is achieved through refractive surgery, so an individual who gets full distance correction with LASIK or PRK might be trading distance glasses for reading glasses.
Who cannot have laser surgery?
You shouldn’t have any sort of laser eye surgery if you are under the age of 21. This is because your vision may still be developing at this stage.
Even if you’re over 21, laser eye surgery should only be carried out if your glasses or contact lens prescriptions hasn’t changed significantly over the last two years or more.
You may also not be suited to laser surgery if you:
- have diabetes – this can cause abnormalities in the eyes that can be made worse by laser surgery to the cornea
- are pregnant or breastfeeding – your body will contain hormones that cause slight fluctuations in your eyesight, making precise surgery difficult
- have a condition that affects your immune system, such as HIV or rheumatoid arthritis – these conditions may affect your ability to recover after surgery
- have other problems with your eyes, such as glaucoma (increased pressure in the eye), or cataracts (cloudy patches in the lens of the eye)
Laser eye surgery can generally be effective for people with a prescription of up to -10D. If your nearsightedness is more severe, lens implants may be more appropriate.
Lens implant surgery
Lens implant surgery is a relatively new type of surgery for nearsightedness. It involves implanting an artificial lens into your eye through a small cut in your cornea.
The lenses are specially designed to help focus light more clearly on to the retina. They can be helpful in improving the vision of people with very severe short-sightedness or those who have difficulty wearing glasses or contact lenses.
There are two main types of lens implant:
- Phakic implant – where an artificial lens is placed into your eye without removing your natural lens; usually preferred for younger people whose natural reading vision is normal
- Artificial replacement – where the natural lens is removed and replaced with an artificial one, similar to cataract surgery
Both types of implant are usually inserted under a local anesthetic and you’ll be normally be able to return home the same day. Each eye will usually be treated on separate occasions.
Results
Phakic lens implants may achieve better results than lens replacements, in terms of improving vision on a long-term basis. However, the technique carries a higher risk of complications, such as cataracts.
Overall, most people will experience a significant improvement in their vision and around 1 in 4 may have almost completely normal vision (“20/20” vision) afterwards.
A lens replacement may be more suitable for older adults with damage to their eyes or an eye condition other than nearsightedness, such as cataracts or glaucoma.
Also, as both techniques are relatively new, there is little information about whether they are safe or effective in the long term.
Risks and complications
Like all medical procedures, surgery to place artificial lens implants in the eyes carries a risk of complications.
Posterior capsule opacification (PCO) is one of the most common complications of lens implant surgery. This is where part of the artificial lens becomes thickened and cloudy.
Posterior capsule opacification (PCO) usually occurs a few months or years after having surgery. Treatment for posterior capsule opacification (PCO) can involve having laser surgery to remove the thickened part of the lens.
Other possible complications of lens implant surgery include:
- retinal detachment (where the retina begins to pull away from the blood vessels that supply it with oxygen and nutrients)
- cataracts
- seeing a halo of light around objects at night
- reduced night vision
- glaucoma
You should talk to your doctor or surgeon about each procedure so you’re fully aware of any risks involved.
Lifestyle and home remedies
You can’t prevent nearsightedness. Some studies suggest you may be able to slow its progression. You can help protect your eyes and your vision by following these tips:
- Have your eyes checked. Do this regularly even if you see well.
- Control chronic health conditions. Certain conditions, such as diabetes and high blood pressure, can affect your vision if you don’t receive proper treatment.
- Protect your eyes from the sun. Wear sunglasses that block ultraviolet (UV) radiation.
- Prevent eye injuries. Wear protective eyewear when doing certain things, such as playing sports, mowing the lawn, painting or using other products with toxic fumes.
- Eat healthy foods. Try to eat plenty of fruits, leafy greens and other vegetables. And studies show that your eyes benefit if you also include in your diet fish high in omega-3 fatty acids, such as tuna and salmon.
- Don’t smoke. Just as smoking isn’t good for the rest of your body, smoking can adversely affect your eye health as well.
- Use the right corrective lenses. The right lenses optimize your vision. Having regular exams will ensure that your prescription is correct.
- Reduce eyestrain. Look away from your computer or near-task work, including reading, every few minutes.
- Recognize symptoms. You may have a serious medical problem if you have a sudden loss of vision in one eye, experience sudden hazy or blurred vision, or see flashes of light, black spots, or halos around lights. These may indicate certain conditions, such as glaucoma, stroke, or a retinal tear or detachment. See your doctor immediately if you experience any of these symptoms.
- Vitale, S et al. 2009. Increased prevalence of myopia in the United States between 1971-1972 and 1999-2004. Arch Ophthalmol 127(12): 1632-1639.[↩]
- Rudnicka AJ, et al. 2016. Global variations and time trends in the prevalence of childhood myopia, a systematic review and quantitative meta-analysis: implications for aetiology and early prevention. British Journal of Ophthalmology 100(7):10.1136/bjophthalmol-2015-307724.[↩]
- Verhoeven VJ, et al., 2013. Genome-wide meta-analyses of multi-ancestry cohorts identify multiple new susceptibility loci for refractive error and myopia. Nature Genetics 45:314-318. doi:10.1038/ng.2554.[↩]
- The Collaborative Longitudinal Evaluation of Ethnicity and Refractive Error (CLEERE) Study: https://clinicaltrials.gov/ct2/show/NCT00000169[↩]
- Jones-Jordan, LA, et al. 2012. Time outdoors, visual activity, and myopia progression in juvenile-onset myopes. Clinical and Epidemiologic Research 53: 7169-7175.[↩]
- Food and Drug Administration [Internet]. Silver Spring (MD); LASIK Quality of Life Collaboration Project. https://www.fda.gov/MedicalDevices/ProductsandMedicalProcedures/SurgeryandLifeSupport/LASIK/ucm190291.htm[↩][↩]





{kind=link}