Contents
What is nephrotic syndrome
Nephrotic syndrome is not a specific disease but the name given to the set of problems that causes the kidneys to leak large amounts of protein into the urine. Nephrotic syndrome can lead to a range of problems, including swelling of body tissues and a greater chance of catching infections.
Nephrotic syndrome includes the following:
- Albuminuria—large amounts of protein in the urine. In nephrotic syndrome, damaged glomeruli allow 3 grams or more of protein to leak into the urine when measured over a 24-hour period, which is more than 20 times the amount that healthy glomeruli allow.
- Hyperlipidemia—higher than normal fat and cholesterol levels in the blood
- Edema, or swelling, usually in the legs, feet, or ankles and less often in the hands or face
- Hypoalbuminia—low levels of albumin in the blood
Albumin is a protein that acts like a sponge, drawing extra fluid from the body into the bloodstream where it remains until removed by the kidneys. When albumin leaks into the urine, the blood loses its capacity to absorb extra fluid from the body, causing edema.
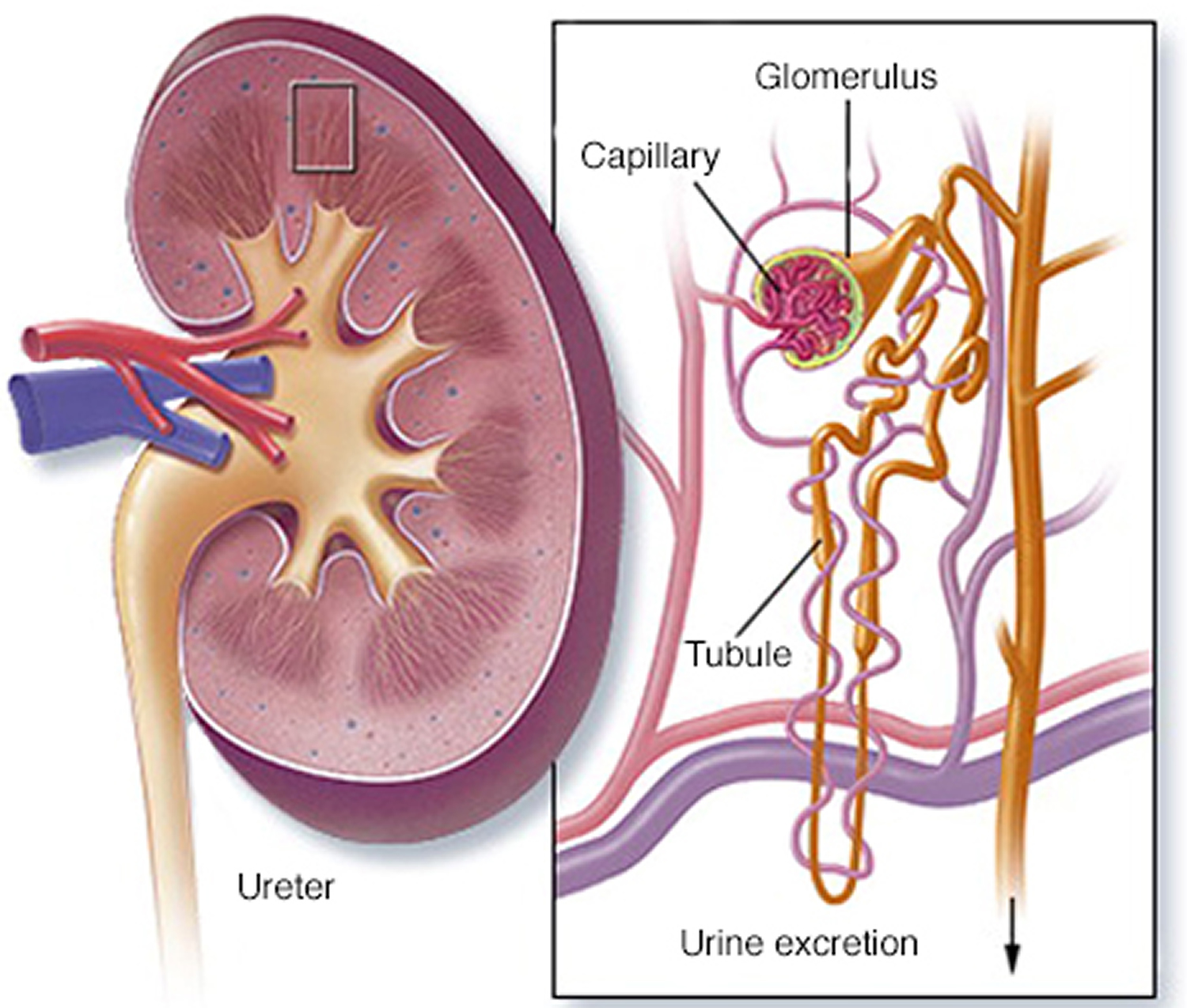
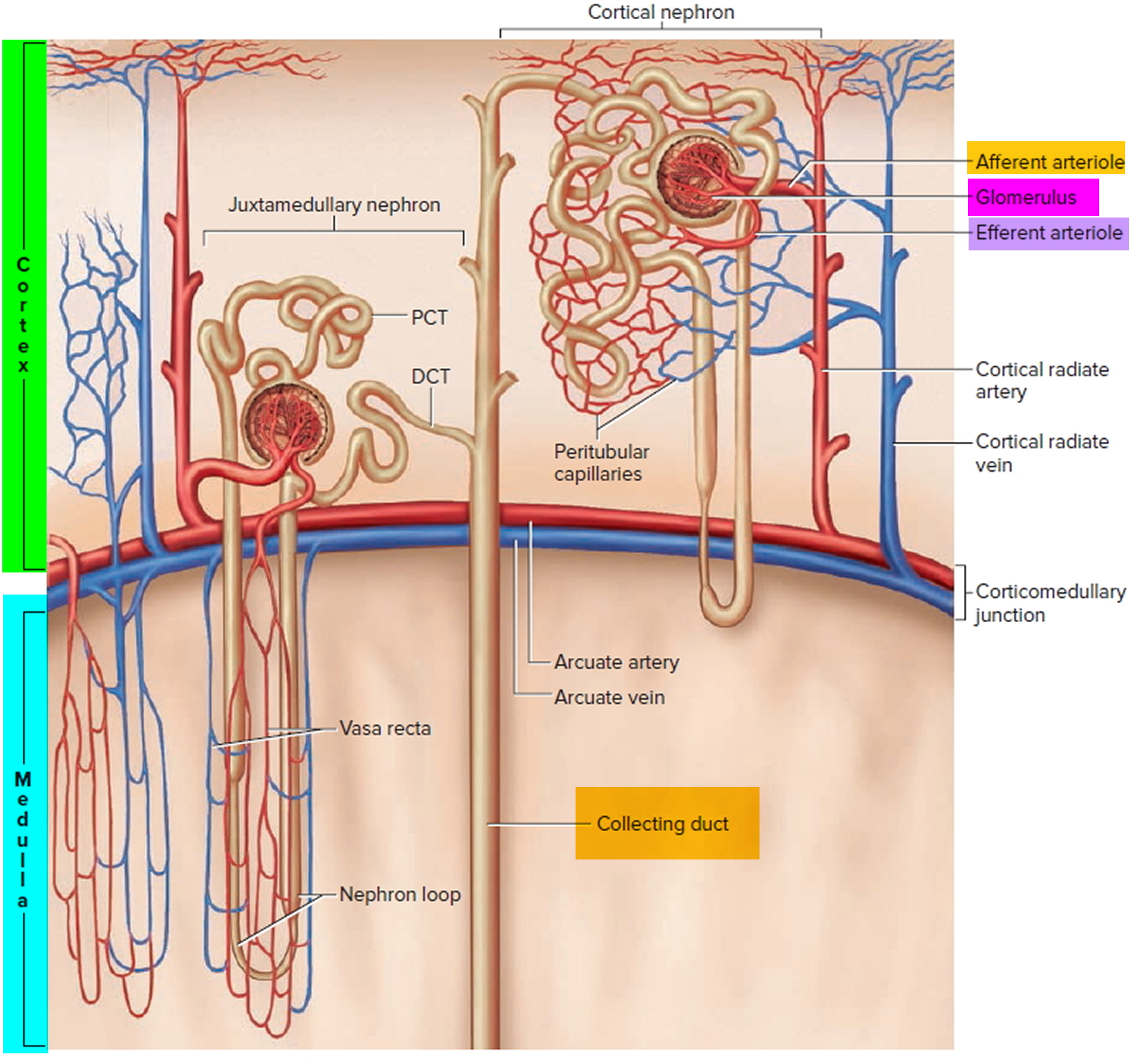
Nephrotic syndrome results from a problem with the kidneys’ filters, called glomeruli (see Figures 3 and 4). Glomeruli are tiny blood vessels in the kidneys that remove wastes and excess fluids from the blood and send them to the bladder as urine.
One of the main jobs of your kidneys is to filter your blood. This allows you to pass your body’s waste products, extra fluid and salts through your urine. The glomeruli are the parts of the kidney where this happens
With healthy kidneys, proteins in your blood don’t usually leak into the urine during the filtering process. But if the glomeruli become damaged, proteins such as albumin can leak into your urine along with the waste products. If too many proteins leak out, that is known as nephrotic syndrome.
Although nephrotic syndrome can affect people of any age, it’s usually first diagnosed in children aged between 2 and 5 years old. It affects more boys than girls.
Kidneys and kidney function
The kidneys are two bean-shaped organs, each about the size of a fist. They are located just below the rib cage, one on each side of the spine (Figures 1 to 4). Every day, your kidneys filter about 120 to 150 quarts of blood to produce about 1 to 2 quarts of urine, composed of wastes and extra fluid. Children produce less urine than adults and the amount produced depends on their age. The urine flows from the kidneys to the bladder through tubes called ureters. The bladder stores urine. When the bladder empties, urine flows out of the body through a tube called the urethra, located at the bottom of the bladder.
Kidneys work at the microscopic level. The kidney is not one large filter. Each kidney is made up of about a million filtering units called nephrons. Each nephron filters a small amount of blood. The nephron includes a filter, called the glomerulus, and a tubule. The nephrons work through a two-step process. The glomerulus lets fluid and waste products pass through it; however, it prevents blood cells and large molecules, mostly proteins, from passing. The filtered fluid then passes through the tubule, which sends needed minerals back to the bloodstream and removes wastes.
Figure 1. Kidney location
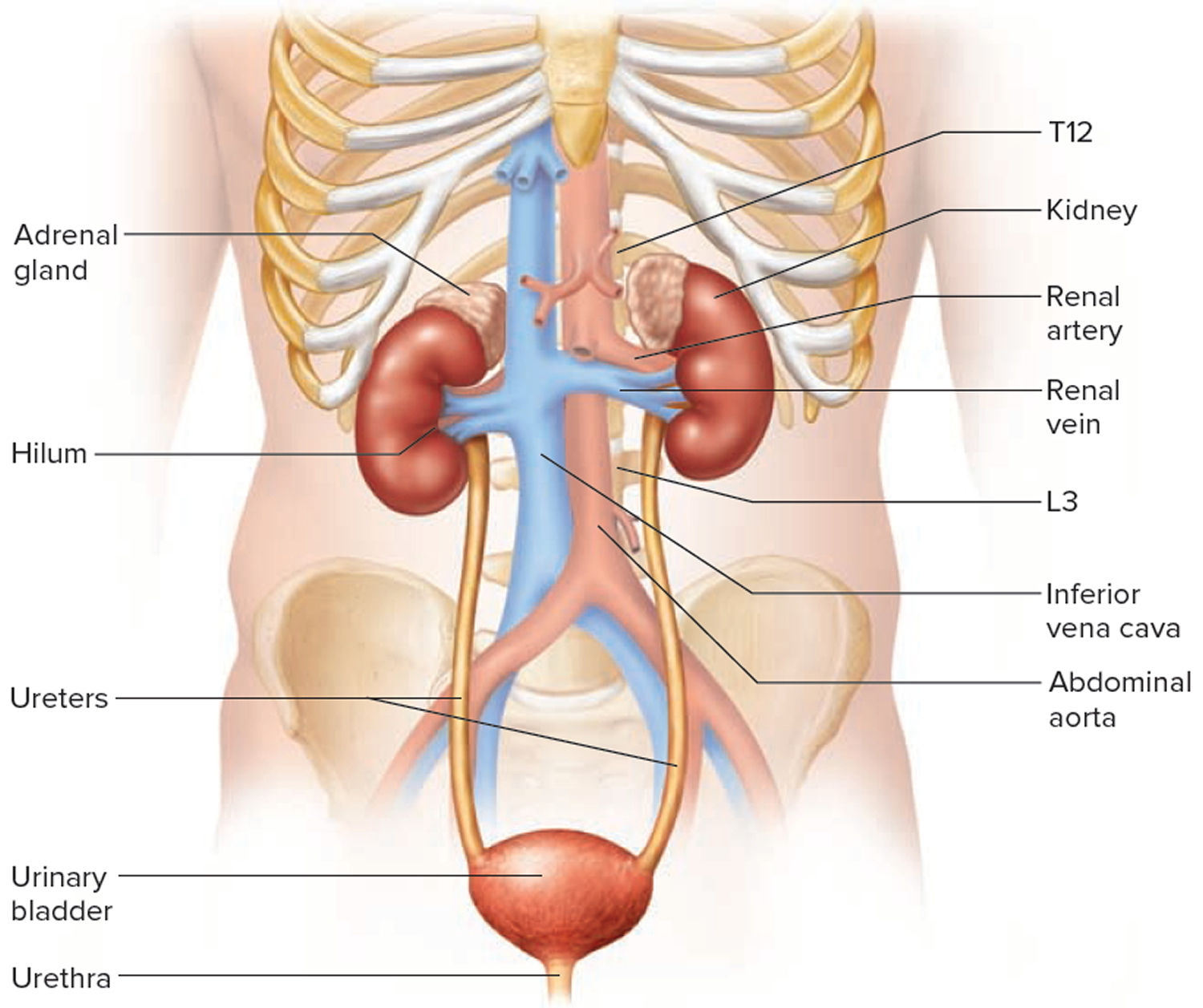
Figure 2. Kidney anatomy
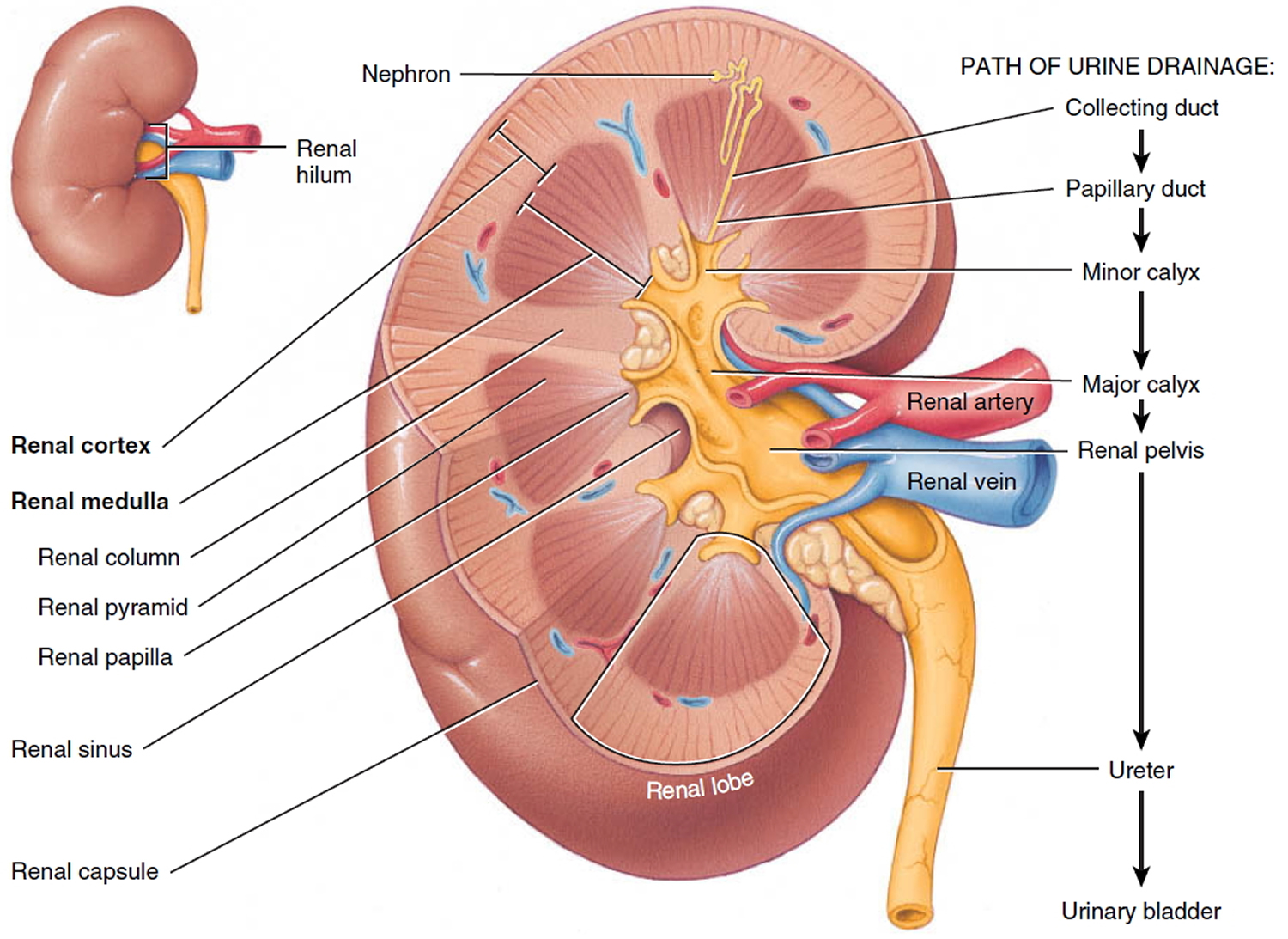 Figure 3. Kidney structure
Figure 3. Kidney structure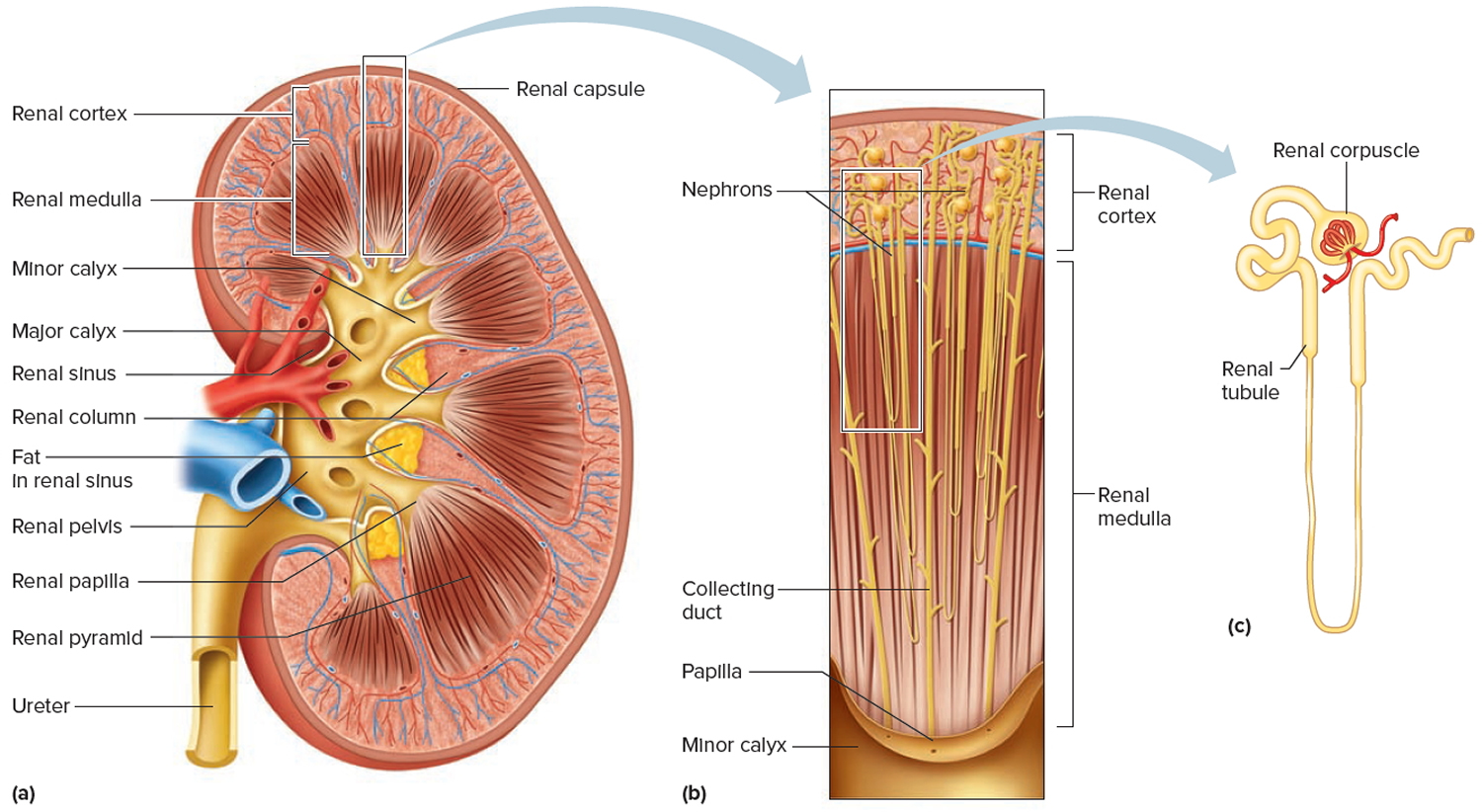
Figure 4. Microcirculation of the kidney
Nephrotic syndrome in children
Childhood nephrotic syndrome is not a disease in itself; rather, it is a group of symptoms that:
- indicate kidney damage—particularly damage to the glomeruli, the tiny units within the kidney where blood is filtered
- result in the release of too much protein from the body into the urine
When the kidneys are damaged, the protein albumin, normally found in the blood, will leak into the urine. Proteins are large, complex molecules that perform a number of important functions in the body.
The two types of childhood nephrotic syndrome are:
- Primary—the most common type of childhood nephrotic syndrome, which begins in the kidneys and affects only the kidneys
- Secondary—the syndrome is caused by other diseases
Around 1 in every 50,000 children are diagnosed with nephrotic syndrome each year. Childhood nephrotic syndrome tends to be more common in families with a history of allergies or those of an Asian background, although it’s unclear why.
A health care provider may refer a child with nephrotic syndrome to a nephrologist—a doctor who specializes in treating kidney disease. A child should see a pediatric nephrologist, who has special training to take care of kidney problems in children, if possible. However, in many parts of the country, pediatric nephrologists are in short supply, so the child may need to travel. If traveling is not possible, some nephrologists who treat adults can also treat children.
The symptoms of childhood nephrotic syndrome can usually be controlled with steroid medication. Most children with nephrotic syndrome respond well to steroids and aren’t at risk of kidney failure.
However, a small number of children have congenital (inherited) nephrotic syndrome and usually do less well. They may eventually have kidney failure and need a kidney transplant.
Most children with nephrotic syndrome have times when their symptoms are under control (remission), followed by times when symptoms return (relapses).
In most cases, relapses become less frequent as they get older and often stop by their late teens.
Some of the main symptoms associated with nephrotic syndrome in children include:
- swelling – the low level of protein in the blood reduces the flow of water from body tissues back into the blood vessels, leading to swelling (oedema). Swelling is usually first noticed around the eyes, then around the lower legs and rest of the body.
- infections – antibodies are a specialised group of proteins in the blood that help to fight infection. When these are lost, children are much more likely to get infections.
- urine changes – occasionally, the high levels of protein being passed into the urine can cause it to become frothy. Some children with nephrotic syndrome may also pass less urine than usual during relapses.
- blood clots – important proteins that help to prevent the blood clotting can be passed out in the urine of children with nephrotic syndrome. This can increase their risk of potentially serious blood clots. During a relapse, the blood also becomes more concentrated, which can lead to clotting.
Nephrotic syndrome in children causes
While idiopathic, or unknown, diseases are the most common cause of primary childhood nephrotic syndrome, researchers have linked certain diseases and some specific genetic changes that damage the kidneys with primary childhood nephrotic syndrome.
The cause of secondary childhood nephrotic syndrome is an underlying disease or infection. Called a primary illness, it’s this underlying disease or infection that causes changes in the kidney function that can result in secondary childhood nephrotic syndrome.
Congenital diseases—diseases that are present at birth—can also cause childhood nephrotic syndrome.
Primary Childhood Nephrotic Syndrome
The following diseases are different types of idiopathic childhood nephrotic syndrome:
- Minimal change disease means that their kidneys appear normal or nearly normal if a tissue sample is studied under a standard microscope. Most children with nephrotic syndrome have “minimal change disease”. Minimal change disease is the most common cause of idiopathic childhood nephrotic syndrome 1. Minimal change disease involves damage to the glomeruli that can be seen only with an electron microscope. This type of microscope shows tiny details better than any other microscope. The cause of minimal change disease is unknown.
- Focal segmental glomerulosclerosis is scarring in scattered regions of the kidney:
- “Focal” means that only some of the glomeruli become scarred.
- “Segmental” means damage affects only part of an individual glomerulus.
- Membranoproliferative glomerulonephritis is a group of disorders involving deposits of antibodies that build up in the glomeruli, causing thickening and damage. Antibodies are proteins made by the immune system to protect the body from foreign substances such as bacteria or viruses.
Secondary Childhood Nephrotic Syndrome
Some common diseases that can cause secondary childhood nephrotic syndrome include
- Diabetes, a condition that occurs when the body cannot use glucose—a type of sugar—normally
- Henoch-Schönlein purpura, a disease that causes small blood vessels in the body to become inflamed and leak
- Hepatitis, inflammation of the liver caused by a virus
- Human immunodeficiency virus (HIV), a virus that alters the immune system
- Lupus, an autoimmune disease that occurs when the body attacks its own immune system
- Malaria, a disease of the blood that is spread by mosquitos
- Streptococcal infection, an infection that results when the bacteria that causes strep throat or a skin infection is left untreated
- Sickle cell anaemia
- In very rare cases, certain types of cancer – such as leukemia, multiple myeloma or lymphoma.
Other causes of secondary childhood nephrotic syndrome can include certain medications, such as aspirin, ibuprofen, or other nonsteroidal anti-inflammatory drugs (NSAIDs), and exposure to chemicals, such as mercury and lithium.
Congenital nephrotic syndrome
Congenital nephrotic syndrome is a kidney condition that begins in infancy and typically leads to irreversible kidney failure (end-stage renal disease) by early childhood. Children with congenital nephrotic syndrome begin to have symptoms of the condition between birth and 3 months of life 2. Children with congenital nephrotic syndrome typically develop end-stage renal disease between ages 2 and 8, although with treatment, some may not have kidney failure until adolescence or early adulthood.
Congenital nephrotic syndrome affects 1 to 3 per 100,000 children worldwide. In Finland, where this condition is particularly common, congenital nephrotic syndrome is estimated to affect 1 in 10,000 children.
The features of congenital nephrotic syndrome are caused by failure of the kidneys to filter waste products from the blood and remove them in urine. Signs and symptoms of this condition are excessive protein in the urine (proteinuria), increased cholesterol in the blood (hypercholesterolemia), an abnormal buildup of fluid in the abdominal cavity (ascites), and swelling (edema). Affected individuals may also have blood in the urine (hematuria), which can lead to a reduced number of red blood cells (anemia) in the body, abnormal blood clotting, or reduced amounts of certain white blood cells. Low white blood cell counts can lead to a weakened immune system and frequent infections in people with congenital nephrotic syndrome.
Researchers have found that medications are not effective in treating congenital nephrotic syndrome, and that most children will need a kidney transplant by the time they are 2 or 3 years old. A kidney transplant is surgery to place a healthy kidney from someone who has just died or a living donor, most often a family member, into a person’s body to take over the job of the failing kidney.
To keep the child healthy until the transplant, the health care provider may recommend the following:
- albumin injections to make up for the albumin lost in urine
- diuretics to help remove extra fluid that causes swelling
- antibiotics to treat the first signs of infection
- growth hormones to promote growth and help bones mature
- removal of one or both kidneys to decrease the loss of albumin in the urine
- dialysis to artificially filter wastes from the blood if the kidneys fail
If your child has congenital nephrotic syndrome, they’ll need frequent albumin infusions to help them grow and develop normally. This often requires a stay in hospital.
Sometimes parents can be trained to administer the treatment at home. Your child will be regularly reviewed at a clinic, where their blood pressure, growth, weight, kidney function and bone health will be monitored.
It can be difficult for parents to decide which option is best, so you should talk to your doctor about the pros and cons of hospital-based and home-based treatment.
Congenital nephrotic syndrome Genetic Changes
Mutations in the NPHS1 or NPHS2 gene cause most cases of congenital nephrotic syndrome. These genes provide instructions for making proteins that are found in the kidneys. Specifically, the proteins produced from the NPHS1 and NPHS2 genes are found in cells called podocytes, which are located in specialized kidney structures, called glomeruli, that filter the blood. The proteins are found at the podocyte cell surface in the area between two podocytes called the slit diaphragm. The slit diaphragm is known as a filtration barrier because it captures proteins from blood so that they remain in the body while allowing other molecules like sugars and salts to be excreted in urine. The proteins produced from the NPHS1 and NPHS2 genes also help relay cell signals.
Mutations in the NPHS1 or NPHS2 gene result in a decrease or absence of functional protein, which impairs the formation of normal slit diaphragms. Without a functional slit diaphragm, more molecules pass through the kidneys abnormally and get excreted in urine, including proteins and blood cells. The filtering ability of the kidneys worsens from birth, eventually leading to end-stage renal disease.
NPHS1 gene mutations cause all cases of congenital nephrotic syndrome of the Finnish type. This form of the condition is found in people of Finnish ancestry. NPHS1 gene mutations can cause congenital nephrotic syndrome in non-Finnish individuals, but they are a less common cause than NPHS2 gene mutations, which appear to be the most frequent cause of all cases.
Mutations in other genes cause a small number of cases of congenital nephrotic syndrome. Fifteen to 20 percent of individuals with congenital nephrotic syndrome do not have an identified mutation in one of the genes associated with this condition. In these cases, the cause of the condition may be environmental, including infections such as congenital syphilis or toxoplasmosis, or it may be caused by mutations in unidentified genes.
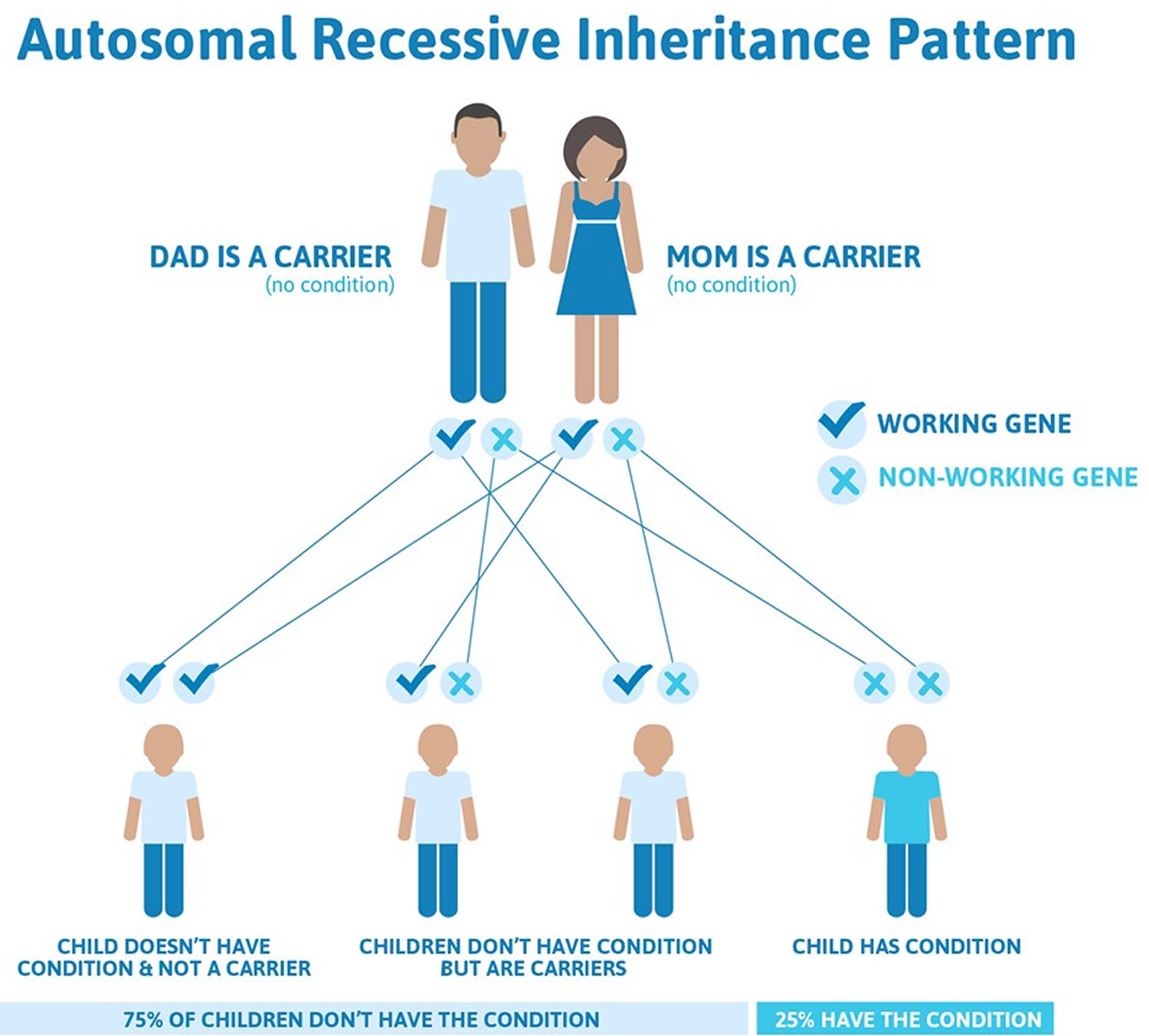
Congenital nephrotic syndrome is inherited in an autosomal recessive pattern, which means both copies of the gene in each cell have mutations. The parents of an individual with an autosomal recessive condition each carry one copy of the mutated gene, but they typically do not show signs and symptoms of the condition.
Figure 5. Congenital nephrotic syndrome autosomal recessive inheritance pattern
Diagnosing nephrotic syndrome in children
Nephrotic syndrome can usually be diagnosed after dipping a dipstick into a urine sample. If there are large amounts of protein in a person’s urine, there will be a color change on the stick.
A blood test showing a low level of a protein called albumin will confirm the diagnosis.
In some cases, when the initial treatment doesn’t work, your child may need a kidney biopsy. This is when a very small sample of kidney tissue is removed using a needle so it can be studied under a microscope.
Pediatric nephrotic syndrome treatment
The main treatment for nephrotic syndrome is steroids, but additional treatments may also be used if a child develops significant side effects.
Most children have relapses until their late teens and need to take steroids when these occur.
Your child may be referred to a childhood kidney specialist (pediatric nephrologist) for tests and specialist treatment.
Steroids
Children diagnosed with nephrotic syndrome for the first time are normally prescribed at least a 4-week course of the steroid medicine prednisolone, followed by a smaller dose every other day for 4 more weeks.
This stops protein leaking from your child’s kidneys into their urine.
When prednisolone is prescribed for short periods, there’s usually no serious or long-lasting side effects, although some children may experience:
- increased appetite
- weight gain
- red cheeks
- mood changes
Most children respond well to treatment with prednisolone, with the protein often disappearing from their urine and the swelling going down within a few weeks. This period is known as remission.
Other medications may be used alongside or in place of steroids if your child’s remission can’t be maintained with steroids or they experience significant side effects.
Additional medications that may be used include:
- levamisole
- cyclophosphamide
- ciclosporin
- tacrolimus
- mycophenolate
- rituximab
Diuretics
Diuretics, or “water tablets”, may also be given to help reduce the fluid build-up. They work by increasing the amount of urine produced.
Penicillin
Penicillin is an antibiotic, and may be prescribed during relapses to reduce the chances of an infection.
Nephrotic syndrome diet
You may be advised to reduce the amount of salt in your child’s diet to prevent further water retention and edema. This means avoiding processed foods and not adding salt to what you eat.
Vaccinations
Children with nephrotic syndrome are advised to have the pneumococcal vaccine. Some children may also be recommended the varicella (chickenpox) vaccination between relapses.
Live vaccines, such as MMR (measles, mumps and rubella vaccine), chickenpox and BCG (Bacillus Calmette-Guérin vaccine or tuberculosis vaccine), shouldn’t be given while your child is taking medication to control their symptoms.
Albumin infusions
Most of the protein lost in nephrotic syndrome is a type called albumin. If your child’s symptoms are severe, they may be admitted to hospital to receive albumin infusions.
Albumin is slowly added to the blood over a few hours through a thin plastic tube called a cannula, which is inserted into one of the veins in their arm.
Caring for your child at home
If your child has been diagnosed with nephrotic syndrome, you’ll need to monitor their condition on a daily basis to check for signs of relapses.
You’ll need to use a dipstick to test your child’s urine for protein the first time they urinate each day.
The results of a dipstick test are recorded as either:
- negative – 0mg of proteinuria per decilitre of urine (mg/dL)
- trace – 15-30mg/dL
- 1+ – 30-100mg/dL
- 2+ – 100-300mg/dL
- 3+ – 300/1,000mg/dL
- 4+ – over 1,000mg/dL
The result for each day needs to be written down in a diary for your doctor or specialist nurse to review during your outpatient appointments.
You should also note down the dose of any medication they’re taking and any other comments, such as whether your child is feeling unwell.
If the dipstick shows 3+ or more of protein in the urine for 3 days in a row, this means your child is having a relapse.
If this happens, you either need to follow the advice given about starting steroids or contact your doctor.
You should seek immediate medical advice if:
- your child has come into contact with someone who has chickenpox or measles and your doctor has told you that your child is not immune to these illnesses
- your child is unwell or has a fever
- your child has diarrhea and is vomiting.
Childhood nephrotic syndrome diet
Children who have nephrotic syndrome may need to make changes to their diet, such as:
- limiting the amount of sodium, often from salt, they take in each day
- reducing the amount of liquids they drink each day
- eating a diet low in saturated fat and cholesterol to help control elevated cholesterol levels
Parents or caretakers should talk with the child’s health care provider before making any changes to the child’s diet.
Dialysis and kidney transplants
In some cases, your doctor may recommend surgery to remove one or both of your child’s kidneys.
This will stop proteins being lost in your child’s urine and reduce their risk of potentially serious problems, such as blood clots.
This means they’ll be dependent on dialysis, where a machine replicates kidney function, from an early age until they can receive a kidney transplant.
A person only needs one kidney to survive, so a living person can donate a kidney. Ideally, this should be a close relative.
Nephrotic vs Nephritic syndrome
Acute nephritic syndrome is a group of disorders that cause inflammation of the internal kidney structures (specifically, the glomeruli) or glomerulonephritis.
Acute nephritic syndrome is often caused by an immune response triggered by an infection or other disease.
Common causes of acute nephritic syndrome in children and adolescents include:
- Hemolytic uremic syndrome
- Henoch-Schönlein purpura
- IgA nephropathy
- Post-streptococcal glomerulonephritis
Common causes of acute nephritic syndrome in adults include:
- Abdominal abscesses
- Goodpasture syndrome
- Hepatitis B or C
- Infective endocarditis
- Membranoproliferative GN I
- Membranoproliferative GN II
- Rapidly progressive (crescentic) glomerulonephritis
- SLE or lupus nephritis
- Vasculitis
- Viral diseases such as mononucleosis, measles, mumps
The inflammation affects the function of the glomerulus. This is the part of the kidney that filters blood to make urine and remove waste. As a result, blood and protein appear in the urine, and excess fluid builds up in the body.
Swelling of the body occurs when the blood loses a protein called albumin. Albumin keeps fluid in the blood vessels. When it is lost, fluid collects in the body tissues.
Blood loss from the damaged kidney structures leads to blood in the urine.
Risk Factors for Acute Nephritic Syndrome (Acute Glomerulonephritis, Acute Nephritis Syndrome)
Infections with Group A Streptococcal bacteria
In warm climates, the disease most commonly follows infected skin lesions and occurs more often in the summer. In cold climates the disease occurs more frequently because of streptococcal throat infection during winter months. The risk of developing acute nephritic syndrome depends on the type of streptococcal bacteria.
Other causes
There are a variety of other causes of acute nephritic syndrome. The following is a list of such conditions:
Primary renal diseases:
- Immunoglobulin A nephropathy;
- Membranoproliferative glomerulonephritis;
- Idiopathic rapidly progressive crescenteric glomerulonephritis.
Secondary renal diseases:
- Subacute bacterial endocarditis;
- Infected ventriculoperitoneal shunt;
- Glomerulonephritis with visceral abscess;
- Glomerulonephritis with bacterial, viral or parasitic infections.
Multi-system disease:
- Systemic lupus erythematosus (SLE);
- Wegener’s granulomatosis;
- Goodpasture’s syndrome;
- Microscopic polyarteritis;
- Mixed cryoglobulinaemia;
- Henoch-Schonlein purpura;
- Haemolytic uraemic syndrome.
Allergy:
Acute allergic tubulointerstitial nephritis.
Acute Nephritic Syndrome (Acute Glomerulonephritis, Acute Nephritis Syndrome) prognosis/outlook
The outlook depends on the disease that is causing the nephritis. When the condition improves, symptoms of fluid retention (such as swelling and cough) and high blood pressure may go away in 1 or 2 weeks. Urine tests may take months to return to normal.
Children tend to do better than adults and usually recover completely. Only rarely do they develop complications or progress to chronic glomerulonephritis and chronic kidney disease.
Adults do not recover as well or as quickly as children. Although it is unusual for the disease to return, in some adults, the disease does return and they will develop end-stage kidney disease and may need dialysis or a kidney transplant. Some forms of glomerulonephritis such as, rapidly progressive crescentic glomerulonephritis move to end stage renal failure if early treatment is not administered (especially when due to anti-glomerular basement membrane antibody disease and systemic vasculitis.)
The microscopic appearance of the kidney defines the prognosis of the condition. Clinical findings of no urine production, heavy amounts of protein in the urine and persistent elevated blood pressure are associated with poor prognosis. Recovery from other post-infectious cases is expected except when associated with the complication of abscess formation where only 50% recover renal function. Recovery from causes other than streptococcal infection is less predictable.
Acute nephritic syndrome symptoms
Common symptoms of nephritic syndrome are:
- Blood in the urine (urine appears dark, tea-colored, or cloudy)
- Decreased urine output (little or no urine may be produced)
- Swelling of the face, eye socket, legs, arms, hands, feet, abdomen, or other areas
- High blood pressure
Other symptoms that may occur include:
- Blurred vision, usually from burst blood vessels in the retina of the eye
- Cough containing mucus or pink, frothy material from fluid buildup in the lungs
- Shortness of breath, from fluid buildup in the lungs
- General ill feeling (malaise), drowsiness, confusion, aches and pains, headache
Symptoms of acute kidney failure or chronic kidney disease may develop.
Acute Nephritic Syndrome (Acute Glomerulonephritis, Acute Nephritis Syndrome) diagnosis
Blood tests and urine analysis will be required to obtain a diagnosis of acute nephritic syndrome. This may require the collection of urine over a 24 hour period to assess the amount of protein lost over this time period. The function of the kidneys will also be tested using a simple blood test to detect signs of renal failure and treat these accordingly.
During an examination, your health care provider may find the following signs:
- High blood pressure
- Abnormal heart and lung sounds
- Signs of excess fluid (edema) such as swelling in the legs, arms, face, and belly
- Enlarged liver
- Enlarged veins in the neck
Tests that may be done include:
- Blood electrolytes
- Blood urea nitrogen (BUN)
- Creatinine – blood
- Creatinine clearance
- Potassium test
- Protein in the urine
- Urinalysis
- Urine appearance and color
A kidney biopsy will show inflammation of the glomeruli, which may indicate the cause of the condition.
Tests to find the cause of acute nephritic syndrome may include:
- ANA titer (lupus)
- Antiglomerular basement membrane antibody
- Antineutrophil cytoplasmic antibody for vasculitis (ANCA)
- Blood culture
- Culture of the throat or skin
- Serum complement (C3 and C4)
Acute nephritic syndrome treatment
The goal of treatment is to reduce inflammation in the kidney and control high blood pressure. You may need to stay in a hospital to be diagnosed and treated.
Your provider may recommend:
- Bed rest until you feel better with treatment
- A diet that limits salt, fluids, and potassium
- Medicines to control high blood pressure, reduce inflammation, or to remove fluid from your body
- Kidney dialysis, if needed
The principles of managing acute nephritic syndrome include:
- Control and prevention of elevated blood pressure: The presence of hypertension can increase the rate of deterioration of renal function in this condition. This may involve the use of anti-hypertension medications, and restriction of fluid and salt from the diet.
- Anti-inflammatory and immunosupressant therapy: To control the inflammatory process of some causes of nephritic syndrome including vasculitis causes.
- Supportive therapy for renal failure: Blood tests will be required regularly to ensure that renal failure is diagnosed and controlled early. Dialysis may be required if the renal failure cannot be controlled by conservative means.
- Antibiotic therapy: For those with proven post-streptococcal nephritic syndrome.
Nephrotic syndrome causes
Nephrotic syndrome can be caused by diseases that affect the kidneys directly, such as focal segmental glomerulosclerosis (FSGS) or membranous nephropathy, as well as underlying diseases that affect the whole body.
Diseases that affect only the kidneys are called primary causes of nephrotic syndrome. The glomeruli are usually the targets of these diseases for reasons that are not fully understood. In focal segmental glomerulosclerosis—the most common primary cause of nephrotic syndrome—scar tissue forms in parts of the glomeruli. In membranous nephropathy, immune molecules form harmful deposits on the glomeruli.
Nephrotic syndrome can also be caused by systemic diseases, which are diseases that affect many parts of the body, such as diabetes or lupus. Systemic diseases that affect the kidneys are called secondary causes of nephrotic syndrome. More than 50 percent of nephrotic syndrome cases in adults have secondary causes, with diabetes being the most common 3.
Kidney diseases that commonly cause nephrotic syndrome include:
- Minimal change disease – this causes a small change in the filters of the kidneys. This is the most common cause of nephrotic syndrome in children. Minimal change disease results in abnormal kidney function, but when the kidney tissue is examined under a microscope, it appears normal or nearly normal. The cause of the abnormal function typically can’t be determined.
- Focal segmental glomerulosclerosis – this causes scar tissue to build up in the kidneys’ filters. Characterized by scattered scarring of some of the glomeruli, this condition may result from another disease or a genetic defect or occur for no known reason.
- Membranous glomerulopathy, also called glomerulous nephropathy – this causes thickening of the lining of the filters. This kidney disorder is the result of thickening membranes within the glomeruli. The exact cause of the thickening isn’t known, but it’s sometimes associated with other medical conditions, such as hepatitis B, malaria, lupus and cancer.
- Nephritis, which is inflammation of the kidneys.
- Diabetic kidney disease. Diabetes can lead to kidney damage (diabetic nephropathy) that affects the glomeruli.
- Systemic lupus erythematosus. This chronic inflammatory disease can lead to serious kidney damage.
- Amyloidosis. This disorder occurs when substances called amyloid proteins accumulate in your organs. Amyloid buildup often affects the kidneys, damaging their filtering system.
- Blood clot in a kidney vein. Renal vein thrombosis, which occurs when a blood clot blocks a vein connected to the kidney, can cause nephrotic syndrome.
Risk factors for nephrotic syndrome
Factors that can increase your risk of nephrotic syndrome include:
- Medical conditions that can damage your kidneys. Certain diseases and conditions increase your risk of developing nephrotic syndrome, such as diabetes, lupus, amyloidosis and other kidney diseases.
- Certain medications. Examples of medications that can cause nephrotic syndrome include nonsteroidal anti-inflammatory drugs and drugs used to fight infections.
- Certain infections. Examples of infections that increase the risk of nephrotic syndrome include HIV, hepatitis B, hepatitis C and malaria.
Nephrotic syndrome signs and symptoms
One of the most common symptoms of nephrotic syndrome is fluid retention, which causes puffy eyes, a swollen abdomen and swollen ankles and feet.
Other symptoms can include:
- frothy urine
- extreme tiredness
- infections
- anemia (lack of red blood cells)
- hyperlipidemia
- hypoalbumina.
Nephrotic syndrome can lead to serious illness such as blood clots and kidney failure.
People with nephrotic syndrome may also experience:
- weight gain due to excess fluid retention
- fatigue
- loss of appetite
Nephrotic syndrome complications
The loss of different proteins from the body can lead to a variety of complications in people with nephrotic syndrome. Blood clots can form when proteins that normally prevent them are lost through the urine. Blood clots can block the flow of blood and oxygen through a blood vessel. Loss of immunoglobulins—immune system proteins that help fight disease and infection—leads to an increased risk of infections. These infections include pneumonia, a lung infection; cellulitis, a skin infection; peritonitis, an abdominal infection; and meningitis, a brain and spine infection. Medications given to treat nephrotic syndrome can also increase the risk of these infections.
Other complications of nephrotic syndrome include:
- Hypothyroidism—a condition in which the thyroid gland does not produce enough thyroid hormone to meet the body’s needs
- Anemia—a condition in which red blood cells are fewer or smaller than normal, which means less oxygen is carried to the body’s cells
- Coronary artery disease, also called coronary heart disease—heart disease caused by narrowing of the arteries that supply blood to the heart
- High blood cholesterol and elevated blood triglycerides. When the level of the protein albumin in your blood falls, your liver makes more albumin. At the same time, your liver releases more cholesterol and triglycerides.
- High blood pressure, also called hypertension—a condition in which blood flows through the blood vessels with a force greater than normal
- Acute kidney failure. If your kidneys lose their ability to filter blood due to damage to the glomeruli, waste products may build up quickly in your blood. If this happens, you may need emergency dialysis — an artificial means of removing extra fluids and waste from your blood — typically with an artificial kidney machine (dialyzer).
- Chronic kidney disease. Nephrotic syndrome may cause your kidneys to gradually lose their function over time. If kidney function falls low enough, you may require dialysis or a kidney transplant.
- Infections. People with nephrotic syndrome have an increased risk of infections.
Nephrotic syndrome diagnosis
Nephrotic syndrome can usually be diagnosed after dipping a dipstick into a urine sample. If there are large amounts of protein in a person’s urine, there will be a color change on the stick.
To confirm whether you have nephrotic syndrome, your doctor is likely to:
- assess your symptoms
- take your medical history
- examine you
- ask you to do a series of urine tests, usually over a 24-hour period
- take a blood sample for testing.
A more precise measurement is usually needed to confirm the diagnosis. Either a single urine sample or a 24-hour collection of urine can be sent to a lab for analysis. With the single urine sample, the lab measures both albumin and creatinine, a waste product of normal muscle breakdown. The comparison of the measurements is called a urine albumin-to-creatinine ratio. A urine sample containing more than 30 milligrams of albumin for each gram of creatinine may signal a problem. With a 24-hour collection of urine, the lab measures only the amount of albumin present. The single urine sample is easier to collect than the 24-hour sample and is usually sufficient to confirm diagnosis, though the 24-hour collection may be used in some cases.
Once nephrotic syndrome is diagnosed, blood tests are usually needed to check for systemic diseases that may be causing the nephrotic syndrome and to find out how well the kidneys are working overall. A blood test involves drawing blood at a health care provider’s office or commercial facility and sending the sample to a lab for analysis.
Though blood tests can point toward systemic diseases, a kidney biopsy is usually needed to diagnose the specific underlying disease causing the nephrotic syndrome and to determine the best treatment. A kidney biopsy is a procedure that involves taking a piece of kidney tissue for examination with a microscope. Kidney biopsies are performed by a health care provider in a hospital with light sedation and local anesthetic. A biopsy is often not needed for a person with diabetes because the person’s medical history and lab tests may be enough to diagnose the problem as being a result of diabetes.
Nephrotic syndrome treatment
Treating nephrotic syndrome includes addressing the underlying cause as well as taking steps to reduce high blood pressure, edema, high cholesterol, and the risks of infection. Treatment usually includes medications and changes in diet.
Nephrotic syndrome diet
It will be important to follow the right diet. You might see a dietitian who is likely to recommend a diet with:
- a reasonable amount of protein, but not too much
- not much fat
- very little salt.
You might also be advised to restrict how much fluid you drink.
Eating, diet, and nutrition have not been shown to play a role in causing or preventing nephrotic syndrome in adults. For people who have developed nephrotic syndrome, limiting intake of dietary sodium, often from salt, and fluid may be recommended to help reduce edema. A diet low in saturated fat and cholesterol may also be recommended to help control hyperlipidemia.
Medications
Medications that lower blood pressure can also significantly slow the progression of kidney disease causing nephrotic syndrome. Two types of blood pressure lowering medications, angiotensin-converting enzyme (ACE) inhibitors and angiotensin receptor blockers, have proven effective in slowing the progression of kidney disease by reducing the pressure inside the glomeruli and thereby reducing albuminuria. Many people require two or more medications to control their blood pressure. In addition to an angiotensin-converting enzyme (ACE) inhibitor or an angiotensin receptor blocker, a diuretic—a medication that aids the kidneys in removing fluid from the blood—can also be useful in helping to reduce blood pressure as well as edema. Beta blockers, calcium channel blockers, and other blood pressure medications may also be needed.
Statin medications may be given to lower cholesterol.
People with nephrotic syndrome should receive the pneumococcal vaccine, which helps protect against a bacterium that commonly causes infection, and yearly flu shots.
Blood thinning medications are usually only given to people with nephrotic syndrome who develop a blood clot; these medications are not used as a preventive measure.
Medicines to manage the symptoms, such as:
- fluid tablets (diuretics) – to reduce fluid retention
- blood pressure medicine – to reduce pressure in your kidneys’ filters, so that less protein is filtered out
- pneumococcal vaccine – if you are at high risk of infection
- anti-clotting medicine – to help thin your blood if there is a risk of blood clots forming
- steroid tablets – which seems to be helpful for minimal change disease
- cholesterol-reducing medications. Medications called statins can help lower cholesterol levels. However, it’s currently unclear whether or not cholesterol-lowering medications can specifically improve the outcomes of people with nephrotic syndrome, such as avoiding heart attacks or decreasing the risk of early death. Statins include atorvastatin (Lipitor), fluvastatin (Lescol), lovastatin (Altoprev), pravastatin (Pravachol), rosuvastatin (Crestor) and simvastatin (Zocor).
Nephrotic syndrome may go away once the underlying cause has been treated.
If you suspect you have nephrotic syndrome symptoms, contact your doctor.
Lifestyle and home remedies
Changes to your diet may help you cope with nephrotic syndrome. Your doctor may refer you to a dietitian to discuss how what you eat can help you cope with the complications of nephrotic syndrome. A dietitian may recommend that you:
- Choose lean sources of protein
- Reduce the amount of fat and cholesterol in your diet to help control your blood cholesterol levels
- Eat a low-salt diet to help control the swelling (edema) you experience
- Limit foods that increase blood sugar levels when taking medications that can lead to weight gain, such as steroids
Some people with nephrotic syndrome may also be deficient in the mineral zinc. A recent study showed treatment with zinc supplements in children under 18 improved nephrotic syndrome. But always check with your doctor before giving your child a supplement or taking one yourself to avoid any potential adverse interactions.
- Nephrotic syndrome. The Merck Manuals Online Medical Library. www.merckmanuals.com[↩]
- Bakkaloglu SA, Schaefer F. Diseases of the kidney and urinary tract in children. In: Taal MW, Chertow GM, Marsden PA, et al., eds. Brenner and Rector’s The Kidney. 9th ed. Philadelphia: Saunders; 2011: 2622–2643.[↩]
- Nephrotic Syndrome. The Merck Manuals Online Medical Library. www.merckmanuals.com[↩]





{kind=link}