
Contents
What is OHSS
Ovarian hyperstimulation syndrome (OHSS) is a serious complication that is sometimes seen in women who take fertility medicines that stimulate egg production (oocytes) and therefore embryos available during assisted reproductive technology (ART). Ovarian hyperstimulation syndrome (OHSS) is an excessive response to taking the medicines (especially injectable gonadotropins) used to make eggs grow. Rarely, OHSS can result from taking other medications you take by mouth, such as clomiphene citrate (Clomid, Serophene) or gonadotropin-releasing hormone. Occasionally OHSS occurs spontaneously, not related to fertility treatments.
Despite the growing number of cycles of assisted reproduction, the true incidence of OHSS remains unknown because there is no mandatory reporting for mild and moderate cases. Furthermore, the lack of an internationally agreed classification system makes it difficult to compare data from different units 1. It is known that the incidence of OHSS varies between different types of fertility treatment, with treatments involving greater degrees of ovarian stimulation being associated with a higher incidence. In cycles of conventional in vitro fertilisation (IVF), mild OHSS has been estimated o affect around one-third of cycles, while the combined incidence of moderate or severe OHSSvaries from 3.1% to 8% 2. The 14th European IVF-Monitoring report 3, analyzing data from 25 European countries, found an incidence of hospitalization due to OHSS of 0.3% in 2010. Data from the USA showed OHSS to be the commonest complication of IVF treatment 4, with an incidence of moderate or severe OHSS in 2011 of 1.1%. OHSS is rare following ovulation induction with clomifene, or monofollicular ovulation induction with gonadotropins, but it has been reported. Very rarely, OHSS may occur spontaneously, in association with pregnancy 5.
Women with OHSS have a large number of growing follicles along with high estradiol levels. This leads to fluid leaking into the abdomen (belly), which can cause bloating, nausea, and swelling of the abdomen. When OHSS is severe, blood clots, shortness of breath, abdominal pain, dehydration, and vomiting are possible. Rare maternal deaths are reported. However, in most cases OHSS is self-limiting and requires supportive management and monitoring while awaiting resolution.
OHSS can be classified as mild, moderate, or severe.
- Mild OHSS – One out of three women has symptoms of mild OHSS during controlled ovarian stimulation for in vitro fertilization (IVF). These symptoms may include mild abdominal bloating, nausea, and weight gain due to fluid. Mild OHSS is common in women having IVF treatment; affecting as many as 33 in 100 women (33%). However, just over 1 in 100 women (1%) will develop moderate or severe OHSS.
- Moderate OHSS – Women with moderate OHSS typically have more of mild OHSS symptoms, but the swelling is worse because of fluid build-up in the abdomen. This can cause abdominal pain and vomiting.
- Severe OHSS – Women with severe OHSS usually have vomiting and cannot keep down liquids. You’ll have symptoms of moderate OHSS with extreme thirst and dehydration. You may only pass small amounts of urine which is dark in color and/or you may experience difficulty breathing or shortness of breath because of a build-up of fluid in your chest. A serious, but rare, complication is formation of a blood clot (thrombosis) in your legs or lungs. The symptoms of this are a swollen, tender leg or pain in your chest and breathlessness. You should report any unusual symptoms to your doctor. You may also experience significant discomfort from swelling of the abdomen. Women with more severe OHSS may require inpatient treatment to manage the symptoms and reduce the risk of further complications.
Figure 1. Proposed classification of OHSS severity
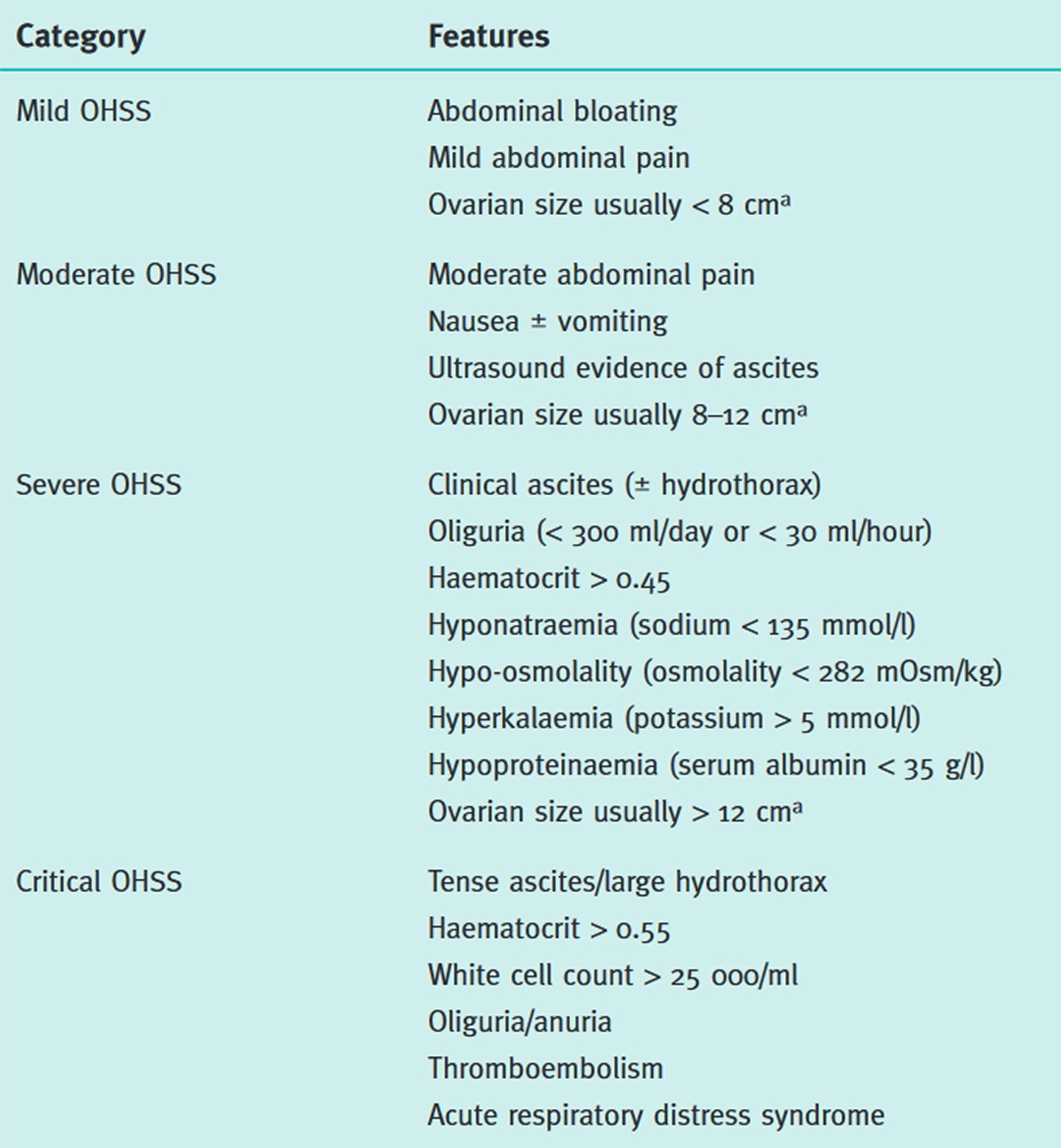
Note: a Ovarian size may not correlate with severity of OHSS in cases of assisted reproduction because of the effect of follicular aspiration. Women demonstrating any feature of severe or critical OHSS should be classified in that category.
[Source 6]In all cases of OHSS, the ovaries are enlarged. The size of the ovary is a marker of the degree of OHSS. If symptoms are present, a transvaginal or abdominal ultrasound can be done to measure ovary size and the amount of fluid collected. OHSS can be serious, so careful monitoring and managing the symptoms are important whenever it occurs.
Complications from OHSS can be severe. You may become dehydrated and pressure in your abdomen may increase from too much fluid. These problems can lead to blood clots forming within the blood vessels. Blood clots can travel to your lungs or to other important organs. This can be potentially life-threatening.
These complications can usually be avoided by recognizing the signs, symptoms, and laboratory evidence that OHSS is getting worse and getting appropriate treatment.
Office visits for ultrasound exams to measure the ovaries and fluid in the abdomen, and blood tests, are routinely done. Decreased activity and drinking lots of electrolyte-rich fluids (over 120 ounces per day) are recommended. Medicines for nausea are available. If there is fluid in the abdomen, drainage of fluid using a syringe (paracentesis) can provide significant relief in most cases. On occasion, more than one drainage is helpful. A medicine called cabergoline also can reduce the fluid accumulation. There is rarely a need for hospitalization.
If OHSS does not improve with outpatient care, the woman may be treated in the hospital with close monitoring. The doctor may order intravenous (IV) fluids and medicines for nausea and may remove fluid from the abdomen. Other supportive therapy may be given as needed.
- OHSS is relatively common after ovulation induction or ovarian stimulation for IVF. It is important you make contact with your fertility clinic if you develop symptoms of OHSS.
- A few women develop OHSS as an after-effect of other fertility treatment or even in a normal conception but this is very rare.
- Women with symptoms of OHSS should see a doctor familiar with assisted reproduction as soon as they have symptoms.
- A standard pelvic exam is NOT generally recommended because the ovaries are enlarged and the cysts that are present may burst under pressure.
- If you develop OHSS, your ovaries will be enlarged and painful. You should avoid having sex or doing strenuous exercise to avoid injury to the ovaries.
- Women should notify their doctor when they have:
- Difficulty breathing
- Continued vomiting or nausea
- Difficulty tolerating fluids
- Abdominal swelling
- Decreased urination
- Weight gain of over 3 pounds in 2 days
- Sudden onset of abdominal pain
- Other symptoms such as facial numbness, weakness, lower extremity swelling, or redness
- OHSS often can be managed with decreased activity, drinking electrolyte-rich fluids, draining fluid that accumulates in the abdomen, medication for nausea and pain, careful monitoring, and frequent doctor visits.
- Severe OHSS (continued vomiting, severe swelling of the abdomen, shortness of breath, inability to drink fluids or abnormal laboratory results) may require hospitalization for intensive monitoring and treatment. The risk of OHSS can be reduced by use of lower doses of gonadotropins, leuprolide (vs. hCG) to trigger ovulation, and cabergoline.
Figure 2. Uterus anatomy
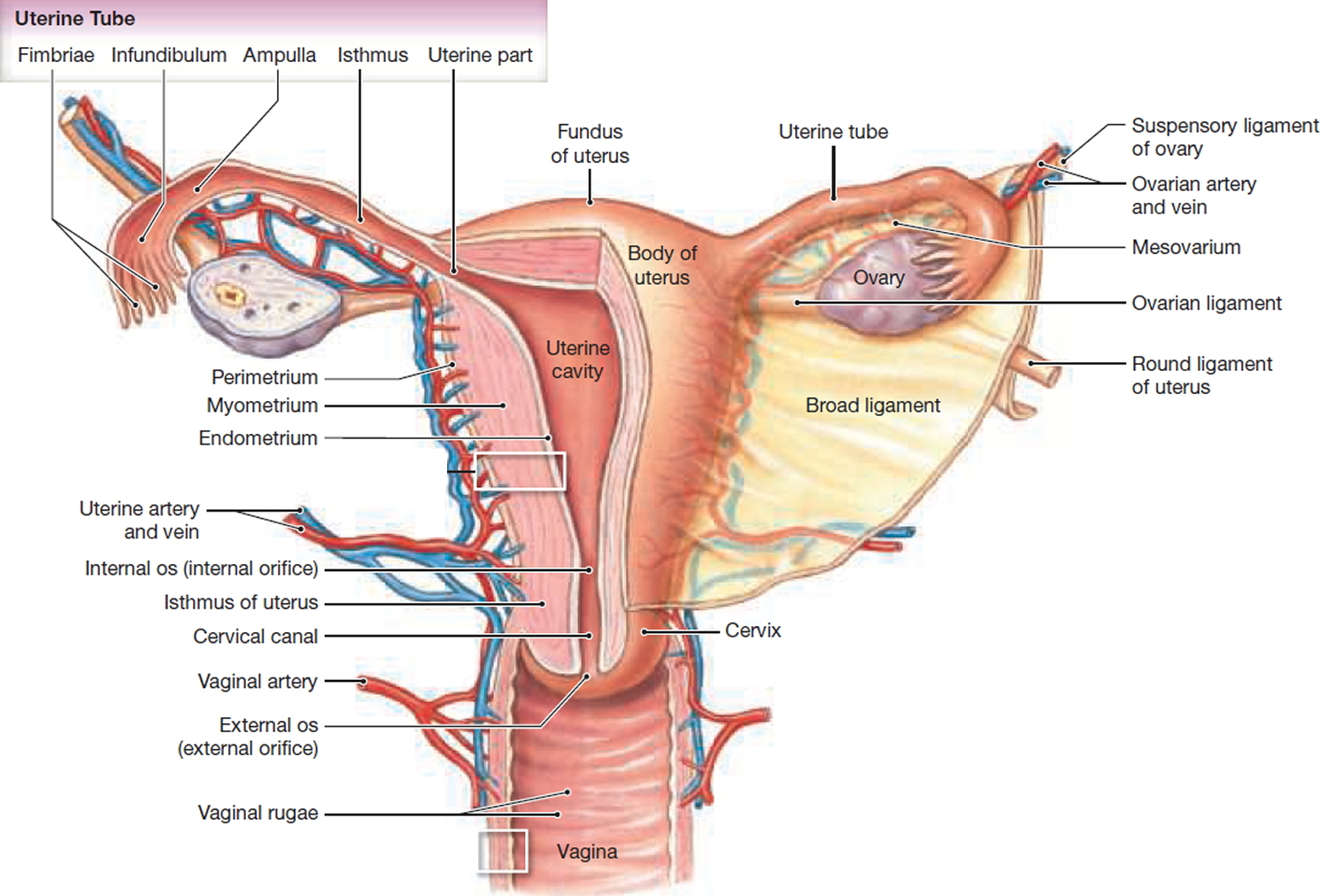
Figure 3. Blood supply to the uterus
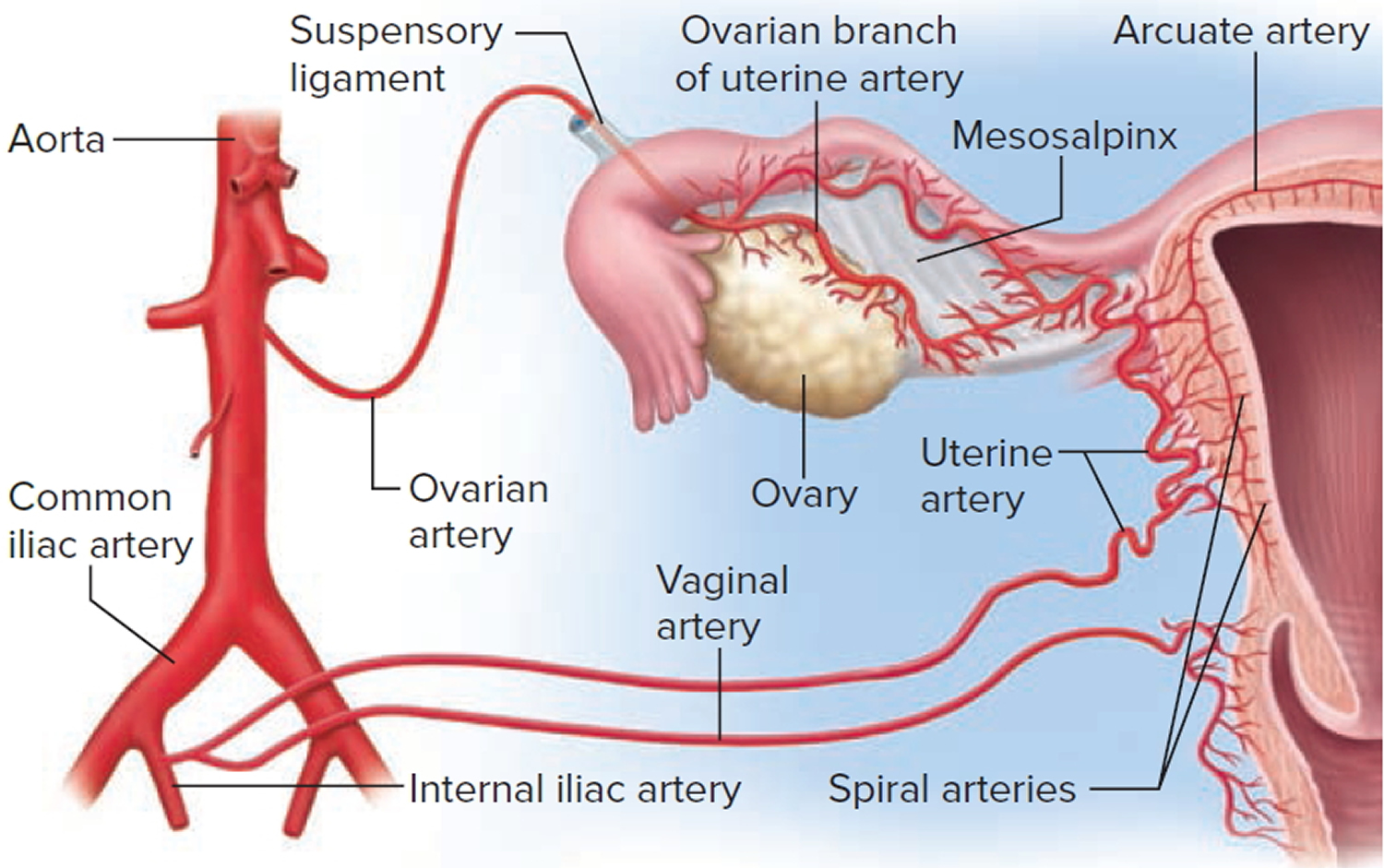
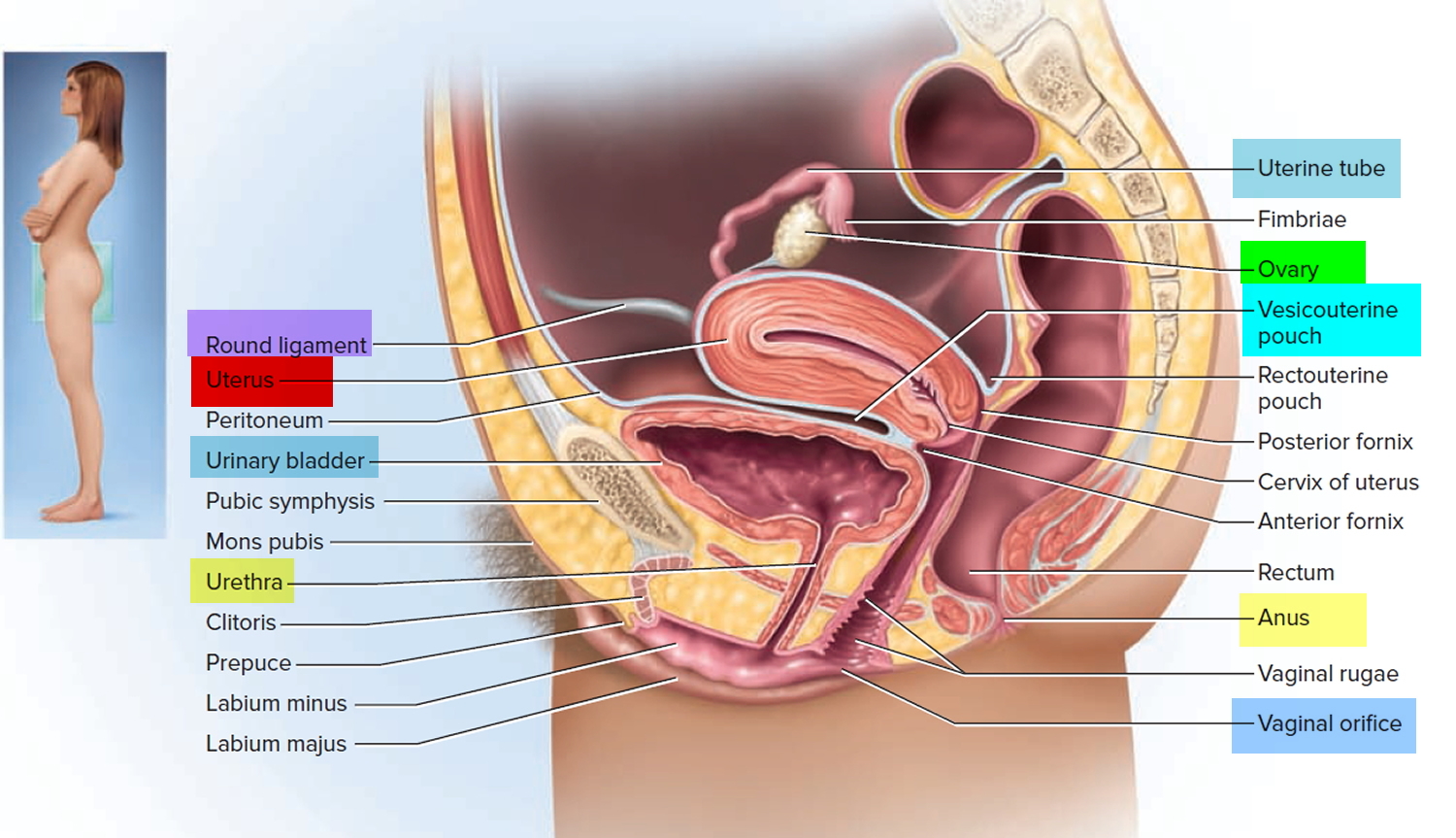
Figure 4. Uterus location
How long does OHSS last?
OHSS symptoms usually appear a few days after ovulation. Symptoms usually resolve within 7-14 days, unless pregnancy occurs. Pregnant women often continue to have symptoms for 2-3 weeks or more after a positive pregnancy test. The symptoms gradually go away, and the rest of the pregnancy is not affected. If your fertility treatment does not result in a pregnancy, OHSS usually gets better by the time your next period starts.
Are there any ongoing concerns if I have had OHSS and become pregnant?
- To lower the risk of developing a blood clot in your legs or lungs, you will be advised to continue wearing support stockings and taking heparin (blood-thinning) injections until 12 weeks of your pregnancy.
- You may be at increased risk of developing pre-eclampsia or giving birth to your baby prematurely. However, there are no known risks to your baby’s development as a result of OHSS.
OHSS complications
About 1 to 2 percent of women undergoing ovarian stimulation develop a severe form of ovarian hyperstimulation syndrome. Severe OHSS can be life-threatening.
OHSS complications may include:
- Fluid collection in the abdomen and sometimes the chest
- Electrolyte disturbances (sodium, potassium, others)
- Blood clots in large vessels, usually in the legs
- Kidney failure
- Twisting of an ovary (ovarian torsion)
- Rupture of a cyst in an ovary, which can lead to serious bleeding
- Breathing problems
- Pregnancy loss from miscarriage or termination because of complications
- Rarely, death
Rarely, OHSS may be associated with life-threatening complications, including renal failure, acute respiratory distress syndrome (ARDS), haemorrhage from ovarian rupture, and thrombo embolism 7. The precise risk of mortality from OHSS is unknown, because there is no obligation to report such cases internationally. There were three deaths from OHSS between 1984 and 2008 in the Netherlands; it is estimated that 100 000 IVF cycles were performed during this period 7. No deaths were reported in 209 cases of severe or critical OHSS arising from 73,492 cycles of IVF performed between 1987 and 1996 in 16 out of 19 tertiary centres in Israe 8. The 2011 triennial report of the Confidential Enquiries into Maternal Deaths in the UK 9 did not identify any maternal deaths due to OHSS in the period 2006–08, during which time approximately 119,000 IVF and intracytoplasmic sperm injection (ICSI) cycles were carried out in 92,813 women.
OHSS causes
The cause of ovarian hyperstimulation syndrome isn’t fully understood, although having a high level of human chorionic gonadotropin (hCG) — a hormone usually produced during pregnancy — introduced into your system to stimulate the ovaries during IVF treatment to make eggs grow plays a role. Sometimes there is an excessive response to these drugs, leading to OHSS. During fertility treatments, HCG may be given as a “trigger” so that a mature follicle will release its egg. OHSS usually happens within a week after you receive an HCG injection. If you become pregnant during a treatment cycle, OHSS may worsen as your body begins producing its own HCG in response to the pregnancy. Injectable fertility medications are more likely to cause OHSS than is treatment with clomiphene, a medication given as a pill you take by mouth.
Exposure of ovaries to human chorionic gonadotrophin (hCG) or luteinising hormone (LH) following controlled ovarian stimulation by follicle-stimulating hormone (FSH) underlies most cases of OHSS. Exposure of hyperstimulated ovaries to hCG leads to the production of proinflammatory mediators. Chief among these is vascular endothelial growth factor (VEGF), but a variety of cytokines are likely to be involved in the pathogenesis and clinical features of OHSS 7. The occurrence of ovarian enlargement with the local and systemic effects of proinflammatory mediators, including increased vascular permeability and a prothrombotic effect, is responsible for the clinical features of OHSS.
Overstimulated ovaries enlarge and release chemicals into the bloodstream. Fluid from the blood vessels leaks into your abdomen and in severe cases into the space around the heart and lungs. OHSS can affect the kidneys, liver and lungs. A very small number of deaths due to OHSS have been reported.
Certain patient and cycle characteristics increase the risk of OHSS; women with a previous history of OHSS, polycystic ovary syndrome, increased antral follicle count (AFC) or high levels of anti-Müllerian hormone (AMH) are at an increased risk of OHSS. Evidence from meta-analysis 10 also shows a reduced risk of OHSS in IVF cycles employing gonadotrophin-releasing hormone (GnRH) antagonists compared with cycles where GnRH agonists are used as part of the regimen for controlled ovarian hyperstimulation. However, OHSS still occurs despite these preventive measures and can occur in patients and treatment cycles that do not meet any criteria that might be considered ‘high risk’ for the development of OHSS. The outcome of treatment also influences the incidence, which is higher in cycles where conception occurs, compared with cycles without conception, and higher still in cycles resulting in multiple pregnancy, highlighting the important role of endogenous hCG.
The risk is higher in women who:
- have polycystic ovaries or polycystic ovary syndrome (PCOS)
- are under 30 years old
- have had OHSS previously
- get pregnant in the same IVF cycle as they get their symptoms, particularly if this is a multiple pregnancy (more than one baby).
Risk factors for OHSS
Factors that increase your risk of OHSS include:
- Polycystic ovary syndrome — a common reproductive disorder that causes irregular menstrual periods, excess hair growth and unusual appearance of the ovaries on ultrasound examination
- Large number of follicles
- Age under 30
- Low body weight
- High or steeply increasing level of estradiol (estrogen) before an hCG trigger shot
- Previous episodes of OHSS
In some cases, OHSS affects women who have no risk factors at all.
How to prevent OHSS
To decrease your chances of developing ovarian hyperstimulation syndrome, you’ll need an individualized plan for your fertility medications. Expect your doctor to carefully monitor each treatment cycle, including frequent ultrasounds to check the development of follicles and blood tests to check your hormone levels.
There are several strategies used to lower the risk of OHSS. Reducing the dose of ovarian stimulation medications may reduce the risk of OHSS. Use of a medicine called leuprolide instead of human chorionic gonadotripin (hCG) to prepare the eggs for release can prevent OHSS. Another medicine called cabergoline also can help reduce the fluid accumulation.
Pregnancy can make OHSS worse or last longer. If a woman develops OHSS, avoiding immediate pregnancy by freezing her eggs/embryos for transfer at a later time can help the OHSS resolve more quickly and keep it from progressing.
Some patients who are at high risk for OHSS may be given extra IV fluids at the time of egg retrieval. Giving IV fluids early can help prevent worsening of symptoms later on.
Strategies to help prevent OHSS include:
- Adjusting or changing medication. Your doctor uses the lowest possible dose of gonadotropins to achieve the goals of stimulating your ovaries and triggering ovulation. Giving women who have polycystic ovary syndrome the drug metformin (Glucophage, Glumetza, others) during ovarian stimulation may help prevent hyperstimulation.
- Coasting. If your estrogen level is high or you have a large number of developed follicles, your doctor may have you stop injectable medications and wait a few days before giving HCG, which triggers ovulation. This is known as coasting.
- Avoiding use of an HCG trigger shot. Because OHSS often develops after an HCG trigger shot is given, alternatives to HCG for triggering have been developed using Gn-RH agonists, such as leuprolide (Lupron), as a way to prevent or limit OHSS.
- Freezing embryos. If you’re undergoing IVF, all the follicles (mature and immature) may be removed from your ovaries to reduce the chance of OHSS. Mature follicles are fertilized and frozen, and your ovaries are allowed to rest. You can resume the IVF process at a later date, when your body is ready.
OHSS symptoms
Symptoms of ovarian hyperstimulation syndrome often begin within 10 days after using injectable medications to stimulate ovulation. Symptoms can range from mild to severe and may worsen or improve over time.
Mild to moderate OHSS
With mild to moderate ovarian hyperstimulation syndrome, symptoms can include:
- Mild to moderate abdominal pain
- Abdominal bloating or increased waist size
- Nausea
- Vomiting
- Diarrhea
- Tenderness in the area of your ovaries
- Sudden weight increase of more than 6.6 pounds (3 kilograms)
Some women who use injectable fertility drugs get a mild form of OHSS, which goes away after about a week. If pregnancy occurs, however, symptoms of OHSS may worsen and last several days to weeks.
Severe OHSS
With severe ovarian hyperstimulation syndrome, you might have:
- Rapid weight gain — such as 33 to 44 pounds (15 to 20 kilograms) in five to 10 days
- Severe abdominal pain
- Severe, persistent nausea and vomiting
- Blood clots in legs
- Decreased urination
- Shortness of breath
- Tight or enlarged abdomen
OHSS diagnosis
Your doctor will ask you to describe your symptoms and will examine you. In addition, your doctor may:
- ask about how much urine you are passing and whether it is darker than normal (concentrated)
- measure your blood pressure, pulse rate and breathing rate
- take an initial measurement of your waistline and check your weight to see whether the fluid is building up or reducing
- arrange an ultrasound scan to measure the size of your ovaries and to check whether there is any fluid build-up in your abdomen
- take blood tests to measure how concentrated your blood is and how well your kidneys are working.
A diagnosis is made on the basis of your symptoms, the examination findings and the results of your tests. If you are well enough to go home, you may be advised to attend for regular check-ups.
OHSS treatment
Although there is no treatment that can reverse OHSS, it will usually get better within a week or two or somewhat longer if you’re pregnant. Treatment is to help symptoms and prevent complications.
OHSS treatment includes:
- pain relief such as paracetamol or codeine
- anti-sickness drugs to help reduce nausea and vomiting
- an intravenous drip to replace fluids. If you are vomiting, you may need a drip to replace the fluids you have lost. The fluid will help to keep you hydrated and may contain sugar and carbohydrates (for energy), and minerals and chemical elements (for regulating and maintaining the organs in your body).
- support stockings and heparin injections to prevent thrombosis (a blood clot in the leg or lungs). Heparin injections for blood thinning should be continued for 7 days from cure of your symptoms if you are not pregnant or until the end of the 12th week of your pregnancy.
If your abdomen is tense and swollen because of fluid build-up, you may be offered a procedure known as a paracentesis. This is when a thin needle or tube is inserted under ultrasound guidance into your abdomen to remove fluid. You may be offered a local anesthetic for this procedure. This treatment helps relieve discomfort and improve kidney function and your breathing. Rarely, advice may be sought from a more specialist team which may involve anesthetists and/or intensive care doctors.
Surgery is only indicated in patients with OHSS if there is a coincident problem such as adnexal torsion, ovarian rupture or ectopic pregnancy and should be performed by an experienced surgeon.
Many women can be managed as outpatients but you may need admission if:
- your pain is not helped by pain-relieving medications
- you have severe nausea and vomiting
- your condition is not getting better
- you will be unable to attend hospital easily for monitoring and follow-up.
It is important that, if you are admitted to a hospital which is not the one where you had your fertility treatment, your care is discussed and coordinated with a specialist in this condition.
Mild to moderate OHSS
Mild OHSS typically resolves on its own. Treatment for moderate OHSS may involve:
- Anti-nausea medication, prescription painkillers or both
- Frequent physical exams and ultrasounds
- Daily weigh-ins and waist measurements to check for drastic changes
- Measurements of how much urine you produce each day
- Blood tests to monitor for dehydration, electrolyte imbalance and other problems
- Adequate fluid intake
- Drainage of excess abdominal fluid using a needle inserted in your abdominal cavity
- Support stockings, to help prevent blood clots
Severe OHSS
With severe OHSS, you may need to be admitted to the hospital for monitoring and aggressive treatment, including IV fluids. Your doctor may give you a medication called cabergoline to lessen your symptoms. In some cases, your doctor may also give you another medication — known as a gonadotropin-releasing hormone (Gn-RH) antagonist — to help suppress ovarian activity.
Serious complications may require additional treatments, such as surgery for a ruptured ovarian cyst or intensive care for liver or lung complications. You may also need anticoagulant medications to decrease the risk of blood clots in your legs.
OHSS treatment home
If you have mild OHSS, you can be looked after at home. Ensure that you drink fluids at regular intervals depending on how thirsty you feel, is the most physiological approach to correcting intravascular dehydration.
If you have pain, take paracetamol or codeine (no more than the maximum dose). You should avoid anti-inflammatory drugs (aspirin or aspirin-like drugs such as ibuprofen or naproxen), which can affect your kidneys and these drugs can interfere with implantation of the newly fertilized egg. It is advisable to remain active to reduce the risk of thrombosis (blood clots).
- Avoid sexual intercourse, as it may be painful and can cause a cyst in your ovary to rupture.
- Maintain a light physical activity level, avoiding strenuous or high-impact activities.
- Weigh yourself on the same scale and measure around your abdomen each day, reporting unusual increases to your doctor.
- Call your doctor if your signs and symptoms get worse.
- gers-Hochschild F, Mansour R, Ishihara O, Adamson GD, de Mouzon J, Nygren KG, et al. International Committee for Monitoring Assisted Reproductive Technology: world report on assisted reproductive technology, 2005. Fertil Steril 2014;101:366–78.e14.[↩]
- Delvigne A, Rozenberg S. Epidemiology and prevention of ovarian hyperstimulation syndrome (OHSS): a review. Hum Reprod Update 2002;8:559–77.[↩]
- Kupka MS, Ferraretti AP, de Mouzon J, Erb K, D’Hooghe T, Castilla JA, et al.; European IVF-Monitoring Consortium, for the European Society of Human Reproduction and Embryology (ESHRE). Assisted reproductive technology in Europe, 2010: results generated from European registers by ESHRE. Hum Reprod 2014;29:2099–113[↩]
- Kawwass JF, Kissin DM, Kulkarni AD, Creanga AA, Session DR, Callaghan WM, et al.; National ART Surveillance System (NASS) Group. Safety of assisted reproductive technology in the United States, 2000-2011. JAMA 2015;313:88–90[↩]
- Sridev S, Barathan S. Case report on spontaneous ovarian hyperstimulation syndrome following natural conception associated with primary hypothyroidism. J Hum Reprod Sci 2013;6:158–61[↩]
- https://www.rcog.org.uk/globalassets/documents/guidelines/green-top-guidelines/gtg_5_ohss.pdf[↩]
- Braat DD, Schutte JM, Bernardus RE, Mooij TM, van Leeuwen FE. Maternal death related to IVF in the Netherlands 1984–2008. Hum Reprod 2010;25:1782–6.[↩][↩][↩]
- Abramov Y, Elchalal U, Schenker JG. Severe OHSS: An ‘epidemic’ of severe OHSS: a price we have to pay? Hum Reprod 1999;14:2181–3.[↩]
- https://www.hfea.gov.uk[↩]
- Al-Inany HG, Youssef MA, Aboulghar M, Broekmans F, Sterrenburg M, Smit J, et al. GnRH antagonists are safer than agonists: an update of a Cochrane review. Hum Reprod Update 2011;17:435[↩]





{kind=link}