Contents
- What is osteoarthritis
- Subsets of Primary Osteoarthritis
- Osteoarthritis vs rheumatoid arthritis
- Osteoarthritis causes
- Complications of Osteoarthritis
- Osteoarthritis symptoms
- Diagnosis of Osteoarthritis
- Osteoarthritis treatment
- DO NOT USE Glucosamine and Chondroitin
- Medications
- American College of Rheumatology guidelines
- For hand osteoarthritis, the American College of Rheumatology conditionally recommends using one or more of the following:
- For knee osteoarthritis, the American College of Rheumatology conditionally recommends using one of the following:
- For hip osteoarthritis, the American College of Rheumatology conditionally recommends using one or more of the following for initial management:
- American Academy of Orthopaedic Surgeons guidelines
- Agency for Healthcare Research and Quality findings
- Intra-articular injections
- Physical Therapy
- Surgical procedures
- Mesenchymal stem cell therapy
What is osteoarthritis
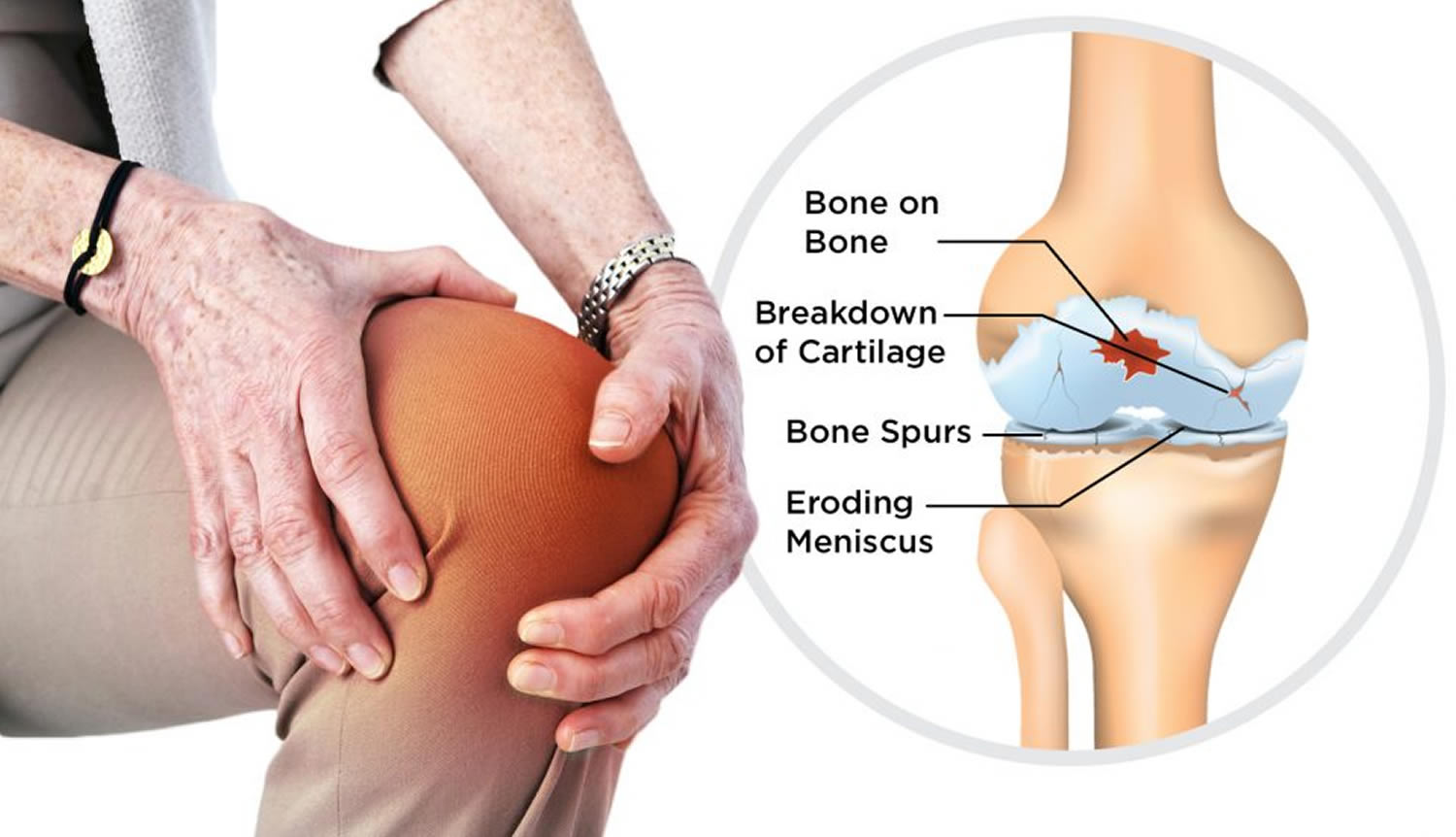
Osteoarthritis is a disease that breaks down the (hyaline) cartilage in your joints. Cartilage is the slippery tissue that covers the ends of bones in a joint 1. Osteoarthritis can be thought of as a degenerative disorder arising from the biochemical breakdown of articular cartilage in the synovial joints. However, the current view holds that osteoarthritis involves not only the articular cartilage but the entire joint organ, including the subchondral bone and synovium. Healthy cartilage absorbs the shock of movement. When you lose cartilage, your bones rub together. The rubbing causes pain, swelling, and loss of motion of the joint. Over time, this rubbing can permanently damage the joint.
Osteoarthritis (see the images below) is the most common type of joint disease, affecting more than 30 million individuals in the United States alone 2. Osteoarthritis is the leading cause of chronic disability in older adults, costing the US greater than $185 billion annually 3.
Osteoarthritis is commonly referred to as “wear and tear” of the joints, but doctors now know that osteoarthritis is a disease of the entire joint, involving the cartilage, joint lining, ligaments, and bone.
Osteoarthritis can cause bone spurs to grow on the edges of the joint. This causes the affected bones to slowly get bigger. Bits of bone or cartilage can break off and float inside the joint space, which causes more pain and damage.
- Unlike some other forms of arthritis, osteoarthritis affects only joints and not internal organs. It is the most common type of arthritis. However, osteoarthritis can occur together with other types of arthritis, such as gout or rheumatoid arthritis.
This arthritis tends to occur in the hand joints, spine, hips, knees, and great toes. The lifetime risk of developing osteoarthritis of the knee is about 46%, and the lifetime risk of developing osteoarthritis of the hip is 25%, according to the Johnston County Osteoarthritis Project, a long-term study from the University of North Carolina and sponsored by the Centers for Disease Control and Prevention (CDC) and the National Institutes of Health.
Risk factors for osteoarthritis include:
- Being overweight
- Getting older
- Injuring a joint
Although it is more common in older people, it is not really accurate to say that the joints are just “wearing out.” It is characterized by breakdown of the cartilage (the tissue that cushions the ends of the bones between joints), bony changes of the joints, deterioration of tendons and ligaments, and various degrees of inflammation of the joint lining (called the synovium) 4.
No single test can diagnose osteoarthritis. Most doctors use several methods, including medical history, a physical exam, x-rays, or lab tests.
Osteoarthritis is a top cause of disability in older people. The goal of osteoarthritis treatment is to reduce pain and improve function. There is no cure for the disease, but some treatments attempt to slow disease progression. Treatments include exercise, medicines, and sometimes surgery.
Stages of Osteoarthritis
The progression of osteoarthritis is characteristically slow, occurring over several years or decades. Over this period, the patient can become less and less active and thus more susceptible to diseases related to decreasing physical activity (including potential weight gain).
Early in the disease process, the joints may appear normal. However, the patient’s gait may be antalgic (is a gait that develops as a way to avoid pain while walking) if weight-bearing joints are involved.
Pain is usually the initial source of morbidity in osteoarthritis, with the disease’s primary symptom being deep, achy joint pain exacerbated by extensive use. Also, reduced range of motion and crepitus are frequently present. Stiffness during rest (gelling) may develop, with morning joint stiffness usually lasting for less than 30 minutes.
Initially, pain can be relieved by rest and may respond to simple analgesics. However, joints may become unstable as the osteoarthritis progresses; therefore, the pain may become more prominent (even during rest) and may not respond to medications.
The disease characteristic of osteoarthritis has been divided into 3 stages.
Several systems have been advocated for use in the grading of focal cartilage change; however, a simple description of the extent of disease (ie, surface, partial-thickness, or full-thickness irregularity with or without underlying subchondral bone change) is generally sufficient and prevents the confusion that may occur with numeric grading systems. Such systems are in any case intended more for research purposes than for clinical use.
Stage 1 Osteoarthritis
In stage 1, proteolytic breakdown of the cartilage matrix occurs. Chondrocyte metabolism is affected, leading to an increased production of enzymes, which includes metalloproteinases (eg, collagenase, stromelysin) that destroy the cartilage matrix. Chondrocytes also produce protease inhibitors, including tissue inhibitors of metalloproteinases (TIMP) 1 and 2, but in amounts insufficient to counteract the proteolytic effect.
Stage 2 Osteoarthritis
Stage 2 involves the fibrillation and erosion of the cartilage surface, with a subsequent release of proteoglycan and collagen fragments into the synovial fluid.
Stage 3 Osteoarthritis
In stage 3, the breakdown products of cartilage induce a chronic inflammatory response in the synovium. Synovial macrophage production of metalloproteinases, as well as cytokines such as interleukin (IL) 1, tumor necrosis factor (TNF)-alpha, occurs. These can diffuse back into the cartilage and directly destroy tissue or stimulate chondrocytes to produce more metalloproteinases. Other proinflammatory molecules (eg, nitric oxide [NO], an inorganic free radical) may also be a factor in stage 3.
Further progression
Eventually, the above events alter the joint architecture, and compensatory bone overgrowth occurs in an attempt to stabilize the joint. As the joint architecture is changed and further mechanical and inflammatory stress occurs on the articular surfaces, the disease progresses unchecked.
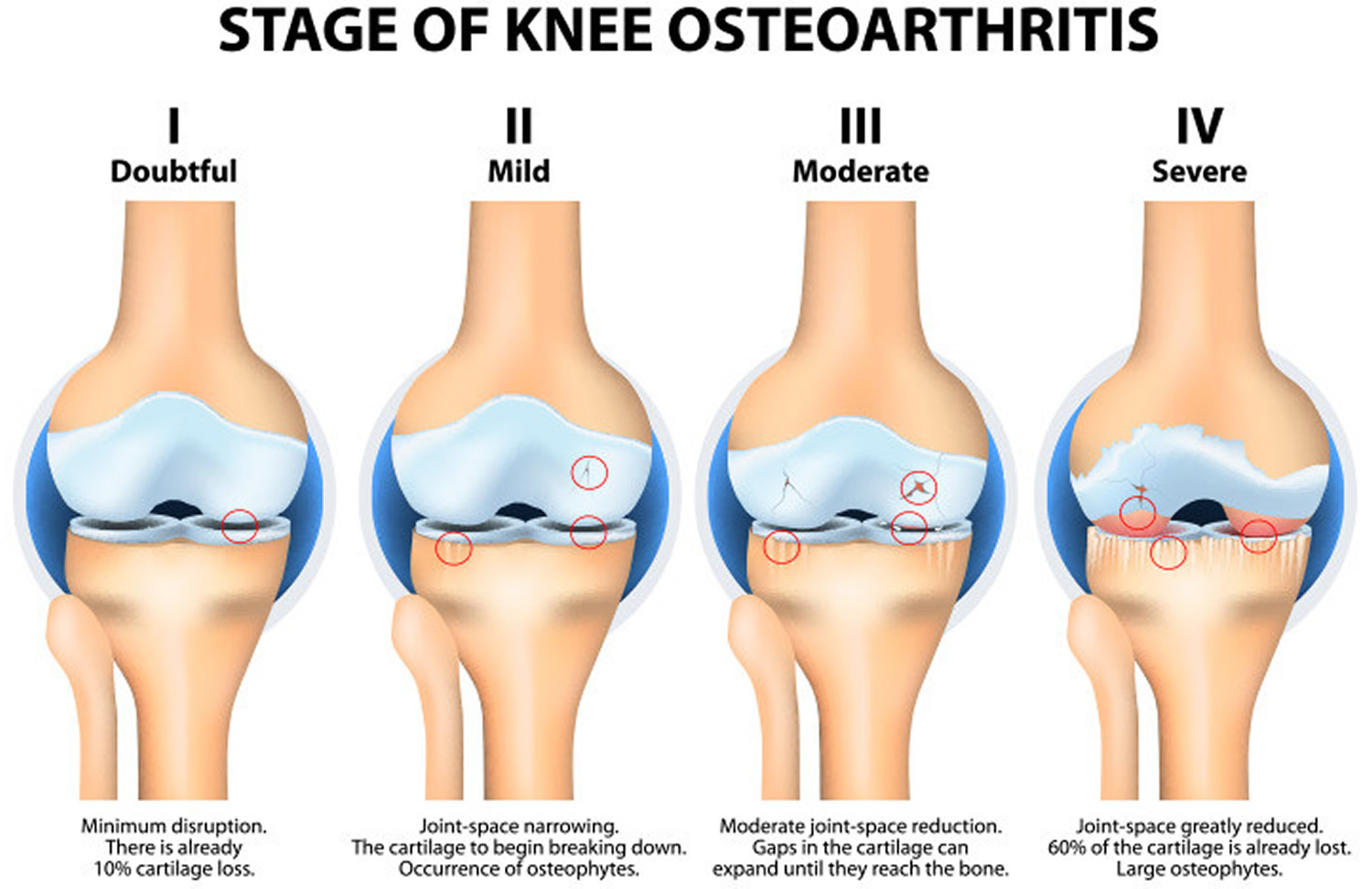
Figure 1. Osteoarthritis knee
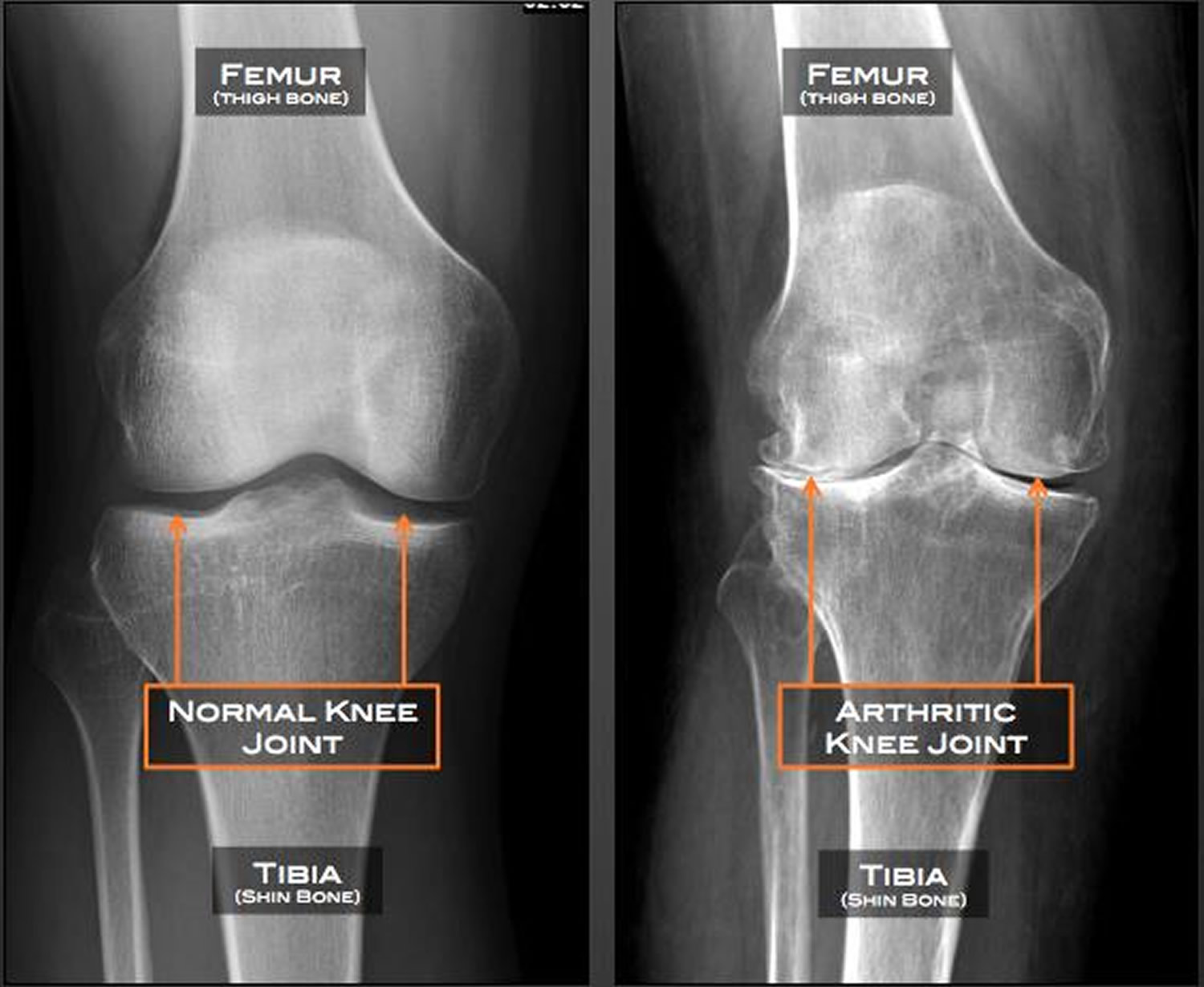
Figure 2. Osteoarthritis of the spine – in osteoarthritis of the spine, disks narrow and bone spurs form.
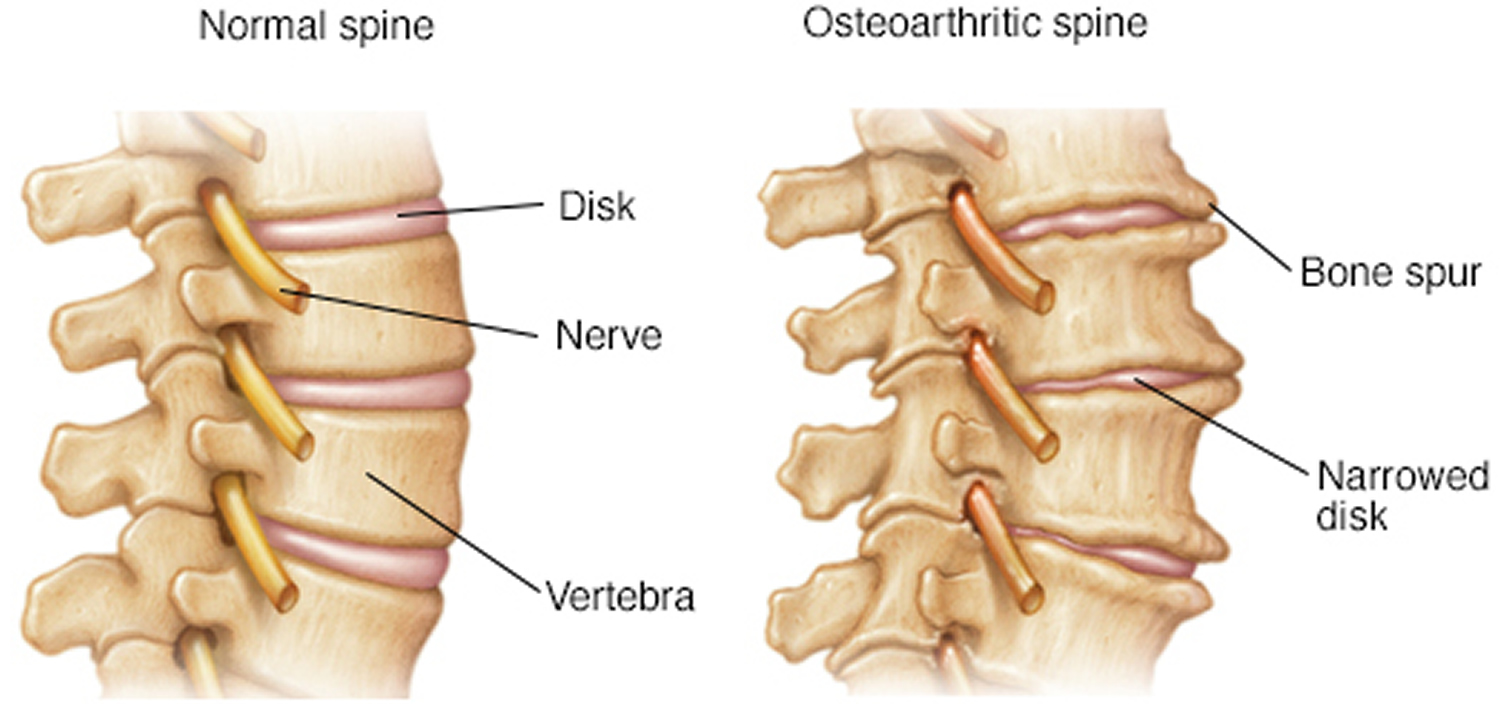
Figure 3. Osteoarthritis hip (X-ray)
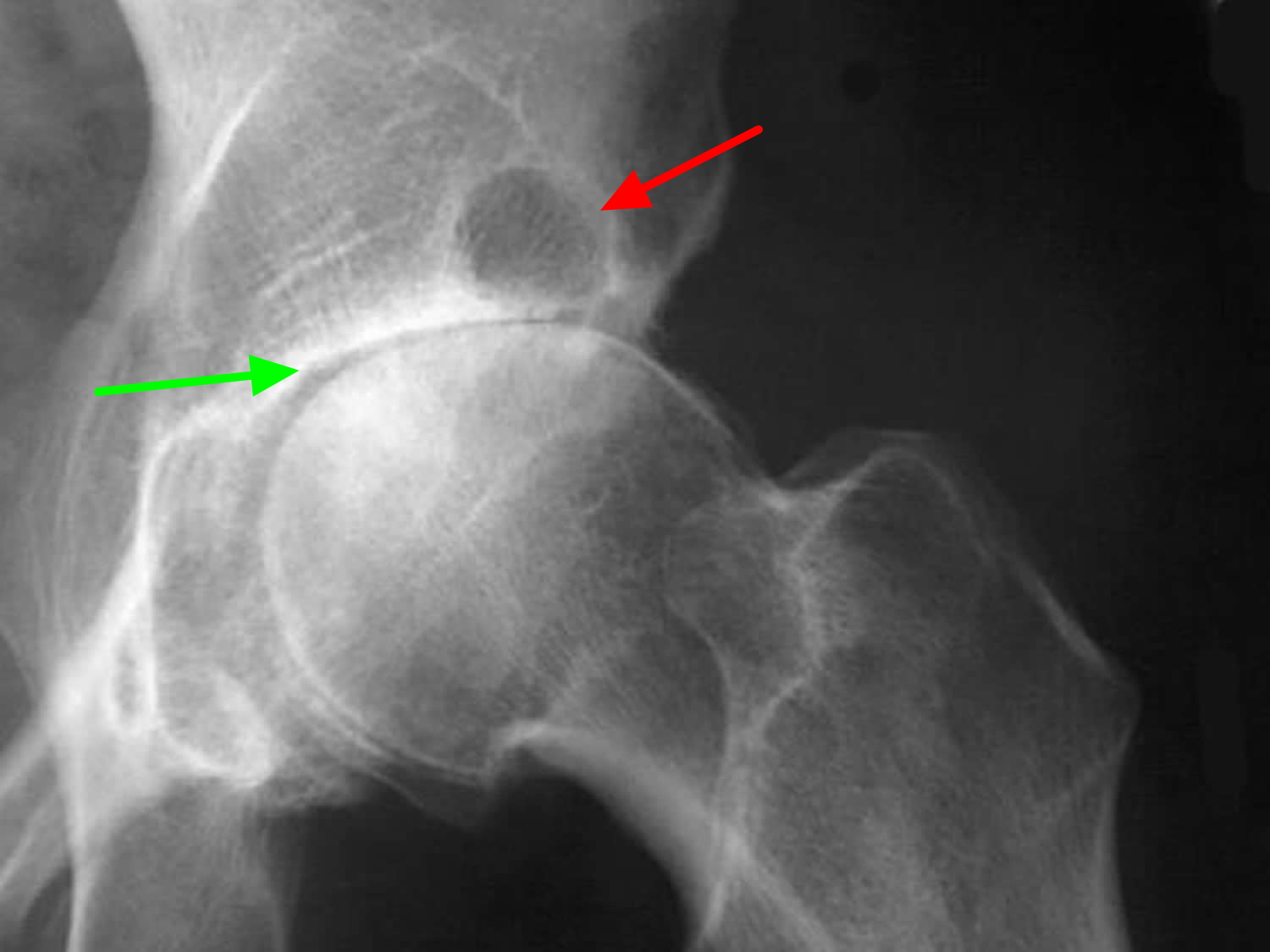 Note: Anteroposterior (AP) radiograph of the hip reveals severe superior migration of the femoral head (which reflects loss of articular cartilage), subchondral sclerosis, prominent osteophytes, and a large Egger cyst in the superior acetabulum. Mild flattening of the superior aspect of the femoral head is present.
Note: Anteroposterior (AP) radiograph of the hip reveals severe superior migration of the femoral head (which reflects loss of articular cartilage), subchondral sclerosis, prominent osteophytes, and a large Egger cyst in the superior acetabulum. Mild flattening of the superior aspect of the femoral head is present.Figure 4. Osteoarthritis hands
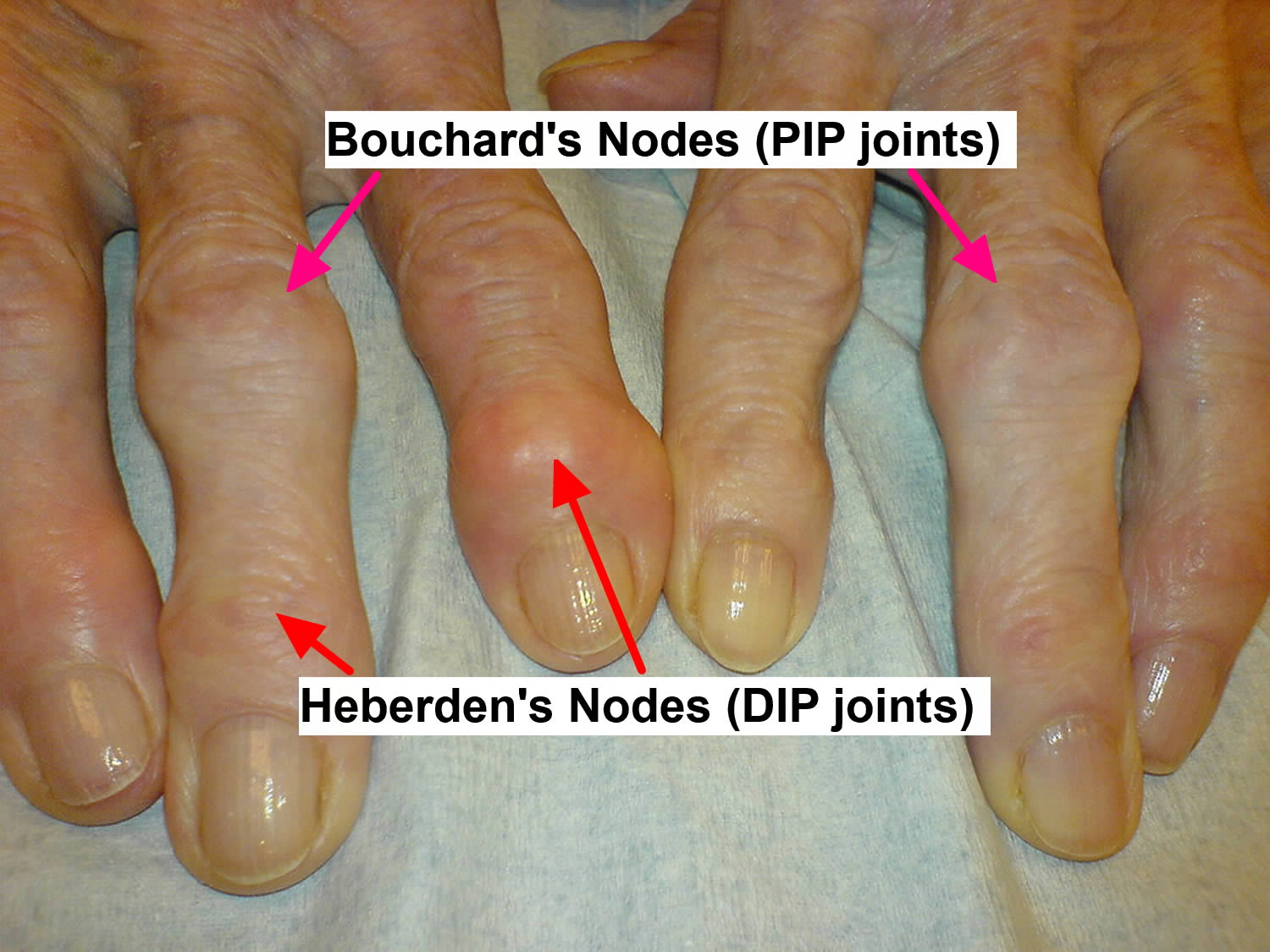
Osteoarthritis of the hand
- Distal interphalangeal (DIP) joints are most often affected
- Proximal interphalangeal (PIP) joints and the carpometacarpal (cmc) joints at the base of the thumb are also typically involved
- Heberden nodes, which represent palpable osteophytes in the DIP joints, are more characteristic in women than in men
- Inflammatory changes are typically absent, less pronounced, or go unnoticed.
Hand osteoarthritis has been classified as follows:
- Erosive
- Thumb base
- Interphalangeal (with or without nodes)
- Widespread hand
Marshall et al 5 report that thumb base osteoarthritis tends to be most prevalent symptomatic form of hand osteoarthritis, followed by interphalangeal joint osteoarthritis. Erosive and generalized hand osteoarthritis were found in older populations and predominantly in women. Over time, erosive osteoarthritis tends to have the poorest characteristics and leads to the most disability.
Subsets of Primary Osteoarthritis
Certain diseases are often categorized as subsets of primary osteoarthritis. These include primary generalized osteoarthritis (PGOA), erosive osteoarthritis, and chondromalacia patellae.
Primary generalized osteoarthritis
Kellgren and Moore 6 described primary generalized osteoarthritis (PGOA) in 1952. The disease is characterized by familial and often premature development of Heberden and Bouchard nodes, as well as the precocious degeneration of the articular cartilage at multiple joints, including the first carpometacarpal joints, knee joints, hip joints, and spine articulations. The radiographic appearance of primary generalized osteoarthritis (PGOA) is indistinguishable from that of nonfamilial primary osteoarthritis, although the disease typically progresses relatively rapidly and has a severe appearance on images 7.
Erosive osteoarthritis
Erosive (i.e, inflammatory) osteoarthritis is a form of primary osteoarthritis marked by a greater degree of inflammation, with erosive abnormalities and in some cases, osseous ankylosis. The disease most commonly occurs in postmenopausal women, and it may be hereditary. Laboratory findings are generally uninformative.
Erosive osteoarthritis is typically bilateral and symmetrical, and it occurs in the interphalangeal joints (particularly the distal interphalangeal [DIP] joints) of the hands. In rare cases, patients have erosive osteoarthritis at the base of the first metacarpal or even in the feet 8.
Radiographically, the erosions are centrally located, in contrast to the marginal erosions in rheumatoid arthritis. In addition, osteophytes are present in erosive osteoarthritis; consequently, interphalangeal joints may assume a gull-wing configuration, with central erosions flanked by raised lips of bone. Periarticular soft-tissue swelling is evident. Osseous fusion, which severely limits joint motion, may occur 9.
Chondromalacia patellae
Chondromalacia patellae is a syndrome of crepitus and pain at the anterior knee that most commonly occurs in young adults. Conventional radiographs provide little information, and although arthrography enables a more direct assessment of cartilaginous integrity, many consider magnetic resonance imaging (MRI) to be the initial imaging study of choice. Chondromalacia patellae is associated with cartilaginous changes along the undersurface of the patella.
Osteoarthritis vs rheumatoid arthritis
Rheumatoid arthritis is a chronic inflammatory disease where your immune system mistakenly attacks the linings of your joints. This results in joint pain, stiffness, swelling, and destruction. Joints are where two or more bones join together, such as at your knees, hips, or shoulders. In some people, rheumatoid arthritis can also damage a wide variety of body systems, including the skin, eyes, lungs, heart and blood vessels.
Rheumatoid arthritis causes pain, swelling, and stiffness. If joints on one side of your body have rheumatoid arthritis, usually those joints on the other side do too. This disease often occurs in more than one joint. Rheumatoid arthritis can affect any joint in the body. In some people, rheumatoid arthritis can also cause the lining of the joints to become damaged and deformed. If you have this disease, you also may feel sick and tired, and sometimes get fevers.
Rheumatoid arthritis predominantly affects the wrists, as well as the metacarpophalangeal (MCP) and proximal interphalangeal (PIP) joints. It rarely, if ever, involves the distal interphalangeal (DIP) joints or the lumbosacral spine.
Rheumatoid arthritis is associated with prominent, prolonged (>1 hour) morning stiffness and overtly swollen, warm joints. Radiographic findings include bone erosion (eg, periarticular osteopenia or marginal erosions of bone) rather than formation. Laboratory findings that further differentiate rheumatoid arthritis from osteoarthritis include the following:
- Systemic inflammation (elevated erythrocyte sedimentation rate [ESR] or C-reactive protein [CRP] level)
- Positive serologies (rheumatoid factor [RF] or anti–cyclic citrullinated peptide [anti-CCP] antibodies)
- Inflammatory joint fluid with a predominance of polymorphonuclear leukocytes (PMNs)
- Elevated white blood cell (WBC) count
Osteoarthritis causes
Osteoarthritis occurs when the cartilage that cushions the ends of bones in your joints gradually deteriorates. Cartilage is a firm, slippery tissue that permits nearly frictionless joint motion.
In osteoarthritis, the slick surface of the cartilage becomes rough. Eventually, if the cartilage wears down completely, you may be left with bone rubbing on bone.
Risk factors for Osteoarthritis
Factors that may increase your risk of osteoarthritis include:
- Older age. The risk of osteoarthritis increases with age.
- Sex. Women are more likely to develop osteoarthritis, though it isn’t clear why.
- Obesity. Carrying extra body weight contributes to osteoarthritis in several ways, and the more you weigh, the greater your risk. Increased weight puts added stress on weight-bearing joints, such as your hips and knees. In addition, fat tissue produces proteins that may cause harmful inflammation in and around your joints.
- Joint injuries. Injuries, such as those that occur when playing sports or from an accident, may increase the risk of osteoarthritis. Even injuries that occurred many years ago and seemingly healed can increase your risk of osteoarthritis.
- Certain occupations. If your job includes tasks that place repetitive stress on a particular joint, that joint may eventually develop osteoarthritis.
- Genetics. Some people inherit a tendency to develop osteoarthritis.
- Bone deformities. Some people are born with malformed joints or defective cartilage, which can increase the risk of osteoarthritis.
Complications of Osteoarthritis
Osteoarthritis is a degenerative disease that worsens over time. Joint pain and stiffness may become severe enough to make daily tasks difficult.
Some people are no longer able to work. When joint pain is this severe, doctors may suggest joint replacement surgery.
Osteoarthritis symptoms
Osteoarthritis symptoms often develop slowly and worsen over time. Signs and symptoms of osteoarthritis include:
- Deep, achy joint pain exacerbated by extensive use – The disease’s primary symptom
- Pain. Your joint may hurt during or after movement.
- Tenderness. Your joint may feel tender when you apply light pressure to it.
- Stiffness. Joint stiffness may be most noticeable when you wake up in the morning or after a period of inactivity usually lasting for less than 30 minutes.
- Reduced range of motion. You may not be able to move your joint through its full range of motion and crepitus (grating sound or sensation produced by friction between bone and cartilage) – frequently present
- Grating sensation. You may hear or feel a grating sensation when you use the joint.
- Bone spurs. These extra bits of bone, which feel like hard lumps, may form around the affected joint.
Diagnosis of Osteoarthritis
Physical examination findings in patients with osteoarthritis are mostly limited to the affected joints. Reduced range of motion and crepitus (grating sound or sensation produced by friction between bone and cartilage) are frequently present.
Malalignment with a bony enlargement may occur. Most cases of osteoarthritis do not involve erythema or warmth over the affected joint(s); however, a bland effusion may be present. Limitation of joint motion or muscle atrophy around a more severely affected joint may occur.
Osteoarthritis of the hand most often affects the distal interphalangeal (DIP) joints but also typically involves the proximal interphalangeal (PIP) joints and the joints at the base of the thumb. Heberden nodes, which represent palpable osteophytes in the DIP joints, are more characteristic in women than in men. Inflammatory changes are typically absent or at least not pronounced.
During the physical exam, your doctor will closely examine your affected joint, checking for tenderness, swelling or redness, and for range of motion in the joint. Your doctor may also recommend imaging and lab tests.
Imaging tests
Pictures of the affected joint can be obtained during imaging tests. Examples include:
- X-rays. Cartilage doesn’t show up on X-ray images, but cartilage loss is revealed by a narrowing of the space between the bones in your joint. An X-ray may also show bone spurs around a joint. Some people may have X-ray evidence of osteoarthritis before they experience any symptoms.
- Magnetic resonance imaging (MRI). An MRI uses radio waves and a strong magnetic field to produce detailed images of bone and soft tissues, including cartilage. An MRI isn’t commonly needed to diagnose osteoarthritis but may help provide more information in complex cases.
Plain radiography is the imaging method of choice because it is more cost-effective than other modalities and because radiographs can be obtained more readily and quickly 10. One important characteristic of primary osteoarthritis is that the abnormalities found in the load-bearing (i.e, highly stressed) areas of the affected joint differ from those found in the non–load-bearing areas. In the load-bearing areas, radiographs can depict joint-space loss, as well as subchondral bony sclerosis and cyst formation
Lab tests
Analyzing your blood or joint fluid can help confirm the diagnosis.
- Blood tests. Although there is no blood test for osteoarthritis, certain tests may help rule out other causes of joint pain, such as rheumatoid arthritis. Levels of acute-phase reactants are typically within the reference range in patients with osteoarthritis. The erythrocyte sedimentation rate (ESR) is not usually elevated, though it may be slightly so in cases of erosive inflammatory arthritis. The synovial fluid analysis usually shows a white blood cell (WBC) count below 2000/µL, with a mononuclear predominance.
- Joint fluid analysis. Your doctor may use a needle to draw fluid out of the affected joint. Examining and testing the fluid from your joint can determine if there’s inflammation and if your pain is caused by gout or an infection. A diagnostic joint aspiration for synovial fluid analysis can help exclude inflammatory arthritis, infection, or crystal arthropathy. The presence of noninflammatory joint fluid helps distinguish osteoarthritis from other causes of joint pain. Other synovial fluid findings that aid in the differentiation of osteoarthritis from other conditions are negative Gram stains and cultures, as well as the absence of crystals when fluid is viewed under a polarized microscope.
Osteoarthritis treatment
Currently, the process underlying osteoarthritis cannot be reversed, but symptoms can usually be effectively managed with lifestyle changes, physical and other therapies, medications, and surgery. The goals of osteoarthritis treatment include alleviation of pain and improvement of functional status 11.
Exercising and achieving a healthy weight are generally the most important ways to treat osteoarthritis.
Table 1. Treatments for Knee Osteoarthritis
| Treatment | Evidence |
|---|---|
Physical therapy and weight loss | Combination of aerobic and strength training is recommended, and weight loss if body mass index is greater than 25 kg/m2; home programs are as effective as supervised programs 12 |
Ice improves range of motion and strength, but not pain 13 | |
There is some evidence for patellar taping or therapeutic ultrasonography to improve physical function and decrease pain 14 | |
Pharmacotherapy | Extended-release acetaminophen, 1,300 mg three times daily, is effective and well tolerated; however, other studies show inconclusive evidence of effectiveness 15 |
Glucosamine/chondroitin supplements show mixed benefit and are not recommended by the American Academy of Orthopaedic Surgeons 12 | |
Opioid analgesics should be used only if conservative pharmacotherapy is ineffective in patients who are not candidates for surgery 16 | |
Selective and nonselective nonsteroidal anti-inflammatory drugs are effective 16 | |
Injections | Corticosteroid injections provide short-term improvements in pain and function 17 |
Hyaluronic injections have questionable benefit for pain and function, and are best reserved for patients in whom first-line conservative treatments have been ineffective and who are not candidates for surgery 12 | |
Braces, orthoses, and other therapies | Limited evidence for medial unloader valgus brace 18 |
DO NOT USE Glucosamine and Chondroitin
- Do NOT use glucosamine and chondroitin to treat patients with symptomatic osteoarthritis of the knee 20. Both glucosamine and chondroitin sulfate do not provide relief for patients with symptomatic osteoarthritis of the knee.
- Do NOT use lateral wedge insoles to treat patients with symptomatic medial compartment osteoarthritis of the knee 20. In patients with symptomatic osteoarthritis of the knee, the use of lateral wedge or neutral insoles does not improve pain or functional outcomes. Comparisons between lateral and neutral heel wedges were investigated, as were comparisons between lateral wedged insoles and lateral wedged insoles with subtalar strapping. The systematic review concludes that there is only limited evidence for the effectiveness of lateral heel wedges and related orthoses. In addition, the possibility exists that those who do not use them may experience fewer symptoms from osteoarthritis of the knee.
Your doctor may also suggest:
Medications
Osteoarthritis symptoms, primarily pain, may be helped by certain medications, including:
Acetaminophen. Acetaminophen (Tylenol, others) has been shown to be effective for people with osteoarthritis who have mild to moderate pain. Taking more than the recommended dosage of acetaminophen can cause liver damage.
Nonsteroidal anti-inflammatory drugs (NSAIDs). Over-the-counter NSAIDs, including ibuprofen (Advil, Motrin IB, others) and naproxen sodium (Aleve, others), taken at the recommended doses, typically relieve osteoarthritis pain. Stronger NSAIDs, available by prescription, may also slightly reduce inflammation along with relieving pain.
NSAIDs can cause stomach upset, cardiovascular problems, bleeding problems, and liver and kidney damage. Topical NSAIDs have fewer side effects and may relieve pain just as well.
Duloxetine (Cymbalta). Normally used as an antidepressant, this medication is also approved to treat chronic pain, including osteoarthritis pain.
American College of Rheumatology guidelines
The American College of Rheumatology has issued guidelines for pharmacologic treatment of osteoarthritis of the hand, hip, and knee 21.
For hand osteoarthritis, the American College of Rheumatology conditionally recommends using one or more of the following:
- Topical capsaicin
- Topical nonsteroidal anti-inflammatory drugs (NSAIDs)
- Oral NSAIDs
- Tramadol
The American College of Rheumatology conditionally recommends against using intra-articular therapies or opioid analgesics for hand osteoarthritis. For patients 75 years and older, the American College of Rheumatology conditionally recommends the use of topical rather than oral NSAIDs.
For knee osteoarthritis, the American College of Rheumatology conditionally recommends using one of the following:
- Acetaminophen
- Oral NSAIDs
- Topical NSAIDs
- Tramadol
- Intra-articular corticosteroid injections
The American College of Rheumatology conditionally recommends against using chondroitin sulfate, glucosamine, or topical capsaicin for knee osteoarthritis. The American College of Rheumatology has no recommendations regarding the use of intra-articular hyaluronates, duloxetine, and opioid analgesics.
For hip osteoarthritis, the American College of Rheumatology conditionally recommends using one or more of the following for initial management:
- Acetaminophen
- Oral NSAIDs
- Tramadol
- Intra-articular corticosteroid injections
The American College of Rheumatology conditionally recommends against using chondroitin sulfate or glucosamine for hip osteoarthritis. The ACR has no recommendation regarding the use of topical NSAIDs, intra-articular hyaluronate injections, duloxetine, or opioid analgesics.
American Academy of Orthopaedic Surgeons guidelines
A 2013 clinical practice guideline from the American Academy of Orthopaedic Surgeons recommends the following pharmacologic treatments for symptomatic osteoarthritis of the knee 22:
- Oral NSAIDs
- Topical NSAIDs
- Tramadol
The American Academy of Orthopaedic Surgeons was unable to recommend for or against the use of the following for symptomatic knee osteoarthritis:
- Acetaminophen
- Opioids
- Pain patches
- Intra-articular corticosteroid injections
- Growth factor injections and/or platelet rich plasma
The recommendation on acetaminophen is a downgrade from the previous American Academy of Orthopaedic Surgeons guideline, and reflects the use of new criteria that resulted in the selection of only one study, which found no statistical significance or minimum clinically important improvement with acetaminophen compared with placebo.
The American Academy of Orthopaedic Surgeons does not recommend treatment with any of the following:
- Intra-articular hyaluronic acid
- Glucosamine and/or chondroitin sulfate or hydrochloride
Agency for Healthcare Research and Quality findings
A comparison of analgesics for osteoarthritis carried out by the Agency for Healthcare Research and Quality (AHRQ) found 23:
- A total of 273 studies were included.
- Overall, we found no clear differences in efficacy for pain relief associated with different NSAIDs.
- Celecoxib was associated with a lower risk of ulcer complications compared to nonselective NSAIDs.
- Coprescribing of proton pump inhibitors, misoprostol and H2-antagonists reduce the risk of endoscopically detected gastroduodenal ulcers compared to placebo in persons prescribed NSAIDs.
- Celecoxib and most nonselective, nonaspirin NSAIDs appeared to be associated with an increased risk of serious cardiovascular harms. There was no clear association between longer duration of NSAID use or higher doses and increased risk of serious cardiovascular harms.
- There were no clear differences between glucosamine or chondroitin and oral NSAIDs for pain or function, though evidence from a systematic review of higher-quality trials suggests that glucosamine had some very small benefits over placebo for pain. Head-to-head trials showed no difference between topical and oral NSAIDs for efficacy in patients with localized osteoarthritis, lower risk of gastrointestinal (GI) adverse events, and higher risk of dermatological adverse events, but serious gastrointestinal (GI) and cardiovascular harms were not evaluated. No head-to-head trials compared topical salicylates or capsaicin to oral NSAIDs.
Treatment of Osteoarthritis of the Knee 24:
- Home-based exercise programs and tai chi show short- to medium-term benefits for symptoms (primarily pain, function, and quality of life) but lack data on long-term benefits.
- Strength and resistance training, pulsed electromagnetic field therapy, and transcutaneous electrical nerve stimulation show mostly short-term benefits, whereas agility training shows short- and long-term benefits.
- Weight loss and general exercise programs show medium- and longterm benefits.
- Intra-articular platelet-rich plasma, balneotherapy, and whole body vibration show medium-term benefits.
- Glucosamine-chondroitin and glucosamine or chondroitin sulfate alone show medium-term benefits with no long-term benefits for pain or function.
Analgesics, NSAIDs, and COX-2 inhibitors
Begin treatment with acetaminophen for mild or moderate osteoarthritic pain without apparent inflammation. If the clinical response to acetaminophen is not satisfactory or if the clinical presentation of osteoarthritis is inflammatory, consider using an NSAID.
Use the lowest effective dose or intermittent dosing if symptoms are intermittent, then try full doses if the patient’s response is insufficient.
Topical NSAID preparations, particularly diclofenac, are available. These preparations can be particularly useful in patients with symptomatic disease that is limited to a few sites or in patients who are at increased risk for adverse events with systemic NSAIDs.
In patients with highly resistant pain, consider the analgesic tramadol. Options in patients at an elevated risk for GI toxicity from NSAIDs include the addition of a proton-pump inhibitor or misoprostol to the treatment regimen and the use of the selective cyclooxygenase (COX)-2 inhibitor celecoxib instead of a nonselective NSAID.
Duloxetine
The selective serotonin-norepinephrine reuptake inhibitor duloxetine has been found to be effective in treating osteoarthritis pain 25. For example, in patients with knee osteoarthritis who had persistent moderate pain despite optimized NSAID therapy, a randomized, double-blind trial found significant additional pain reduction and functional improvement with duloxetine as compared with placebo 26.
However, duloxetine was also associated with significantly more nausea, dry mouth, constipation, fatigue, and decreased appetite than placebo was 26. To date, trials of duloxetine in osteoarthritis have been short in duration (10-13 weeks), and studies comparing duloxetine directly with other therapies have not been performed.
Intra-articular injections
Intra-articular pharmacologic therapy includes injection of a corticosteroid or sodium hyaluronate (ie, hyaluronic acid [HA] or hyaluronan), which may provide pain relief and have an anti-inflammatory effect on the affected joint 27. Ultrasound guidance can facilitate arthrocentesis and injection and is increasingly being adopted by physicians such as rheumatologists and physiatrists for this purpose.
Corticosteroid
After the introduction of the needle into the joint and before steroid administration, aspiration of as much synovial fluid as possible should be attempted. Aspiration often provides symptomatic relief for the patient and allows laboratory evaluation of the fluid, if necessary. Infected joint fluid and bacteremia are contraindications to steroid injection.
In patients with osteoarthritic knee pain, steroid injections generally result in clinically and statistically significant pain reduction as soon as 1 week after injection. The effect may last, on average, anywhere from 4 to 6 weeks per injection, but the benefit is unlikely to continue beyond that time frame 28.
However, in a randomized trial by McAlindon et al 29 comprising 140 patients with symptomatic knee osteoarthritis with synovitis, intra-articular injections of steroid (40 mg triamcinolone, every 12 weeks for 2 years) resulted in significantly greater cartilage volume loss and no significant difference in knee pain, compared with placebo injections of saline. The authors concluded that their findings do not support the use of intra-articular steroid injections for symptomatic knee osteoarthritis 29.
In October 2017, FDA approved triamcinolone acetonide extended-release injectable suspension (Zilretta) for intra-articular treatment of osteoarthritic knee pain. Approval was based on data from a randomized, double-blind international phase III trial in which 484 patients were treated and followed for up to 24 weeks. Patients receiving Zilretta reported a statistically significant reduction in the weekly mean of the average daily pain intensity scores (ADP) from baseline to week 12 30.
For hip osteoarthritis, a randomized, placebo-controlled study confirmed the effectiveness of corticosteroid injection, with benefits often lasting as long as 3 months 31.
Some controversial evidence exists regarding frequent steroid injections and subsequent damage to cartilage (chondrodegeneration). Accordingly, it is usually recommended that no more than three injections per year be delivered to any individual osteoarthritic joint. Systemic glucocorticoids have no role in the management of osteoarthritis.
Sodium hyaluronate
Intra-articular injection of sodium hyaluronate, also referred to as viscosupplementation, has been shown to be safe and possibly effective for symptomatic relief of knee osteoarthritis 32. In the United States, intra-articular sodium hyaluronates are classified as medical devices rather than as drugs 33.
Intra-articular sodium hyaluronates approved by the FDA for the treatment of osteoarthritic knee pain include the naturally extracted, non–cross-linked sodium hyaluronate products Hyalgan 34, Supartz, Orthovisc, and Euflexxa, as well as the cross-linked sodium hyaluronate product known as hylan G-F 20 (Synvisc).
Euflexxa is derived from a fermentation process (Streptococcus), whereas the source material for the other products listed is chicken combs. At present, no distinct advantage or disadvantage has been associated with any particular source of sodium hyaluronates.
Some differences between the viscosupplements do exist in the FDA-approved prescribing information. For example, whereas Hyalgan and Synvisc have been established as safe for repeat treatment, the safety and efficacy of other products for repeat treatment have not been established.
The exact mechanisms of action through which HAs provide symptomatic relief are unknown. Possible mechanisms include direct binding to receptors (CD44 in particular) in the synovium and cartilage that can lead to several biologic activation pathways 35.
The HA class in general has demonstrated a very favorable safety profile for chronic pain management in knee osteoarthritis, with the most common adverse event being injection-site pain. Although any intra-articular injection (whether of HAs or of steroids) may elicit an inflammatory response and possible effusion, only the cross-linked hylan G-F 20 product has been associated with a clinically distinct acute inflammatory side effect (ie, severe acute inflammatory reaction [SAIR] or HA-associated intra-articular pseudosepsis).
Prolotherapy
In a randomized, controlled trial of 90 adults with painful knee osteoarthritis who were randomized to either dextrose prolotherapy, saline injections, or at-home exercise, the patients on prolotherapy experienced significantly greater improvement in pain, function, and stiffness over the other 2 groups. Injections were administered at 1, 5, and 9 weeks, with additional injections provided as needed at weeks 13 and 17 36.
Additional pharmacologic agents
Muscle relaxants may benefit patients with evidence of muscle spasm. Judicious use of narcotics (eg, oxycodone and acetaminophen with codeine) is reserved for patients with severe osteoarthritis.
Glucosamine and chondroitin sulfate have been used in Europe for many years and continue to be popular with patients worldwide. In the United States, however, the glucosamine/chondroitin arthritis intervention trial (GAIT) reported, at best, limited benefit from glucosamine (500 mg 3 times daily), chondroitin sulfate (400 mg 3 times daily), or the combination of the 2 in patients with knee osteoarthritis 37.
In GAIT patients overall, glucosamine and chondroitin sulfate alone or in combination did not reduce pain effectively at 24 weeks, but in patients with moderate-to-severe pain at baseline, the rate of response was significantly higher with combined therapy than with placebo (79.2% vs. 54.3%) 38. At 2 years, no treatment achieved a clinically important difference in loss of joint-space width, though treatment effects on Kellgren-Lawrence grade 2 knees showed a trend toward improvement relative to the placebo group 37.
The AHRQ comparison found no clear difference between glucosamine or chondroitin and oral NSAIDs for relieving pain or improving function. However, the AHRQ observed that most trials showing therapeutic benefits from glucosamine used pharmaceutical-grade glucosamine that is not available in the United States, noting that the trial findings may therefore be inapplicable to currently available over-the-counter preparations.
Another agent, S-adenosylmethionine (SAM-e), is a European supplement receiving significant attention in the United States. A systematic review of SAM-e found that the evidence was inconclusive, with a number of small trials of questionable quality; the authors concluded that the effects of SAM-e on pain and function may be potentially clinically relevant but are expected to be small 39.
Chondroprotective drugs (ie, matrix metalloproteinase [MMP] inhibitors and growth factors) are being tested as disease-modifying drugs in the management of osteoarthritis. For example, MMP-13 is specifically expressed in the cartilage of individuals with osteoarthritis but not in the cartilage of normal adults 40. German researchers reported on the synthesis and biologic evaluation of an MMP-13 selective inhibitor that has demonstrated efficacy as a disease-modifying intra-articular injection for osteoarthritis 41.
Other investigational agents include monoclonal antibodies that inhibit nerve growth factor (NGF), such as tanezumab. Anti-NGF agents have been shown to reduce chronic pain in patients with osteoarthritis 42.
Physical Therapy
- Physical therapy. A physical therapist can work with you to create an individualized exercise program that will strengthen the muscles around your joint, increase your range of motion and reduce pain. Regular gentle exercise that you do on your own, such as swimming or walking, can be equally effective.
- Occupational therapy. An occupational therapist can help you discover ways to do everyday tasks or do your job without putting extra stress on your already painful joint. For instance, a toothbrush with a large grip could make brushing your teeth easier if you have finger osteoarthritis. A bench in your shower could help relieve the pain of standing if you have knee osteoarthritis.
- Tai chi and yoga. These movement therapies involve gentle exercises and stretches combined with deep breathing. Many people use these therapies to reduce stress in their lives, and research suggests that tai chi and yoga may reduce osteoarthritis pain and improve movement. When led by a knowledgeable instructor, these therapies are safe. Avoid moves that cause pain in your joints.
Surgical procedures
If conservative treatments don’t help, you may want to consider procedures such as:
- Realigning bones. If osteoarthritis has damaged one side of your knee more than the other, an osteotomy might be helpful. In a knee osteotomy, a surgeon cuts across the bone either above or below the knee, and then removes or adds a wedge of bone. This shifts your body weight away from the worn-out part of your knee.
- Joint replacement. In joint replacement surgery (arthroplasty), your surgeon removes your damaged joint surfaces and replaces them with plastic and metal parts. Surgical risks include infections and blood clots. Artificial joints can wear out or come loose and may need to eventually be replaced.
Mesenchymal stem cell therapy
Mesenchymal stem cell therapy continues to be a promising investigational approach to knee osteoarthritis 43. To date there are several studies evaluating the effacy of mesenchymal stem cells in knee osteoarthritis with favorable results. However, the variability in cointerventions surrounding mesenchymal stem cell injection, including timing, frequency, culturing mode, and long-term risk warrant further research. Mesenchymal stem cells have also shown modest benefit in knee osteoarthritis after partial or complete meniscectomy in animal studies, over the short term.
Table 1. Summary of osteoarthritis treatment guidelines
| Intervention | Current Guidelines | FDA Approval for Indicated Use | CMS Coverage | Brand Names |
|---|---|---|---|---|
| Glucosamine Chondroitin |
| Evidence insufficient to demonstrate reduction in risk or disease modification (2004); Unclear regarding treatment of symptoms | Not relevant (over-the-counter) | |
| Platelet Rich Plasma |
| Off-label use for an FDA-approved product | CMS National Coverage Determination: covered only for certain chronic non-healing wounds | |
| Mesenchymal Stem Cells |
| Not approved by the FDA | Not covered for OA National Coverage Determination for Stem Cell Transplantation | |
| Duloxetine | ACR: has no recommendation on using Duloxetine. AAOS: not mentioned | Indicated for treatment of chronic musculoskeletal pain including discomfort from osteoarthritis and chronic lower back pain | Not found (Medicare Part D coverage is plan dependent) |
|
| Herbal blends |
| Not relevant | Not relevant (over-the-counter) | |
| Topical or transdermal analgesics |
| FDA approval for OA in 1988. Black box warning regarding cardiovascular effects. Capsaicin patch is FDA-approved. | Not relevant for over-the-counter products; Coverage for prescription products is plan dependent. |
|
| Intraarticular corticosteroids |
| Approved by the FDA for intra-lesional administration | Coverage is based on reasonable and necessary in addition to any other applicable regulation and guidance. |
|
| Intraarticular prolotherapy | Not addressed for knee OA | Injected dextrose is FDA-approved for treatment of hypoglycemia only | National noncoverage. | Abbot Labs manufactures dextrose for IV use |
| Acupuncture |
| FDA approves acupuncture needles as medical devices | CMS National Coverage Determination (2004): not covered | |
| Weight loss | ACR: strongly recommends weight loss (for persons who are overweight) AAOS: suggests weight loss for patients with symptomatic osteoarthritis of the knee OAK and a BMI ≥ 25. (moderate) | Not searched | Bariatric Surgery for the Treatment of Morbid Obesity Certain procedures for the treatment of obesity are covered for Medicare beneficiaries who have a BMI ≥35, have at least one co-morbidity related to obesity and have been previously unsuccessful with the medical treatment of obesity. Other Treatments for Obesity Nationally Noncovered Indications
Where weight loss is necessary before surgery in order to ameliorate the complications posed by obesity when it coexists with pathological conditions such as cardiac and respiratory diseases, diabetes, or hypertension (and other more conservative techniques to achieve this end are not regarded as appropriate), supplemented fasting with adequate monitoring of the patient is eligible for coverage on a case-by-case basis or pursuant to a local coverage determination. The risks associated with the achievement of rapid weight loss must be carefully balanced against the risk posed by the condition requiring surgical treatment | Not relevant |
| Physical therapy |
| Not relevant | Covered under Part B subject to certain conditions and limitations | |
| Braces and/or orthotics (orthoses or wedges) |
| Unloader braces are approved by the FDA as medical equipment [need to check orthotics] | Medicare Part B covers medically necessary arm, leg, back, and neck braces under the durable medical equipment prefabricated orthotics benefit, subject to certain conditions and limitations. Shoes and foot orthotics are covered under certain circumstances only when criteria are met. | Ortho VQ and others |
Note: ACR = American College of Rheumatology; AAOS = American Academy of Orthopaedic Surgeons; OA = Osteoarthritis; OAK = Osteoarthritis Knee
[Source 44]- Osteoarthritis. https://medlineplus.gov/osteoarthritis.html[↩]
- Osteoarthritis Fact Sheet. Centers for Disease Control and Prevention. https://www.cdc.gov/arthritis/basics/osteoarthritis.htm[↩]
- Kotlarz H, Gunnarsson CL, Fang H, Rizzo JA. Insurer and out-of-pocket costs of osteoarthritis in the US: evidence from national survey data. Arthritis Rheum. 2009 Dec. 60 (12):3546-53.[↩]
- Osteoarthritis. https://www.rheumatology.org/I-Am-A/Patient-Caregiver/Diseases-Conditions/Osteoarthritis[↩]
- Marshall M, Peat G, Nicholls E, van der Windt D, Myers H, Dziedzic K. Subsets of symptomatic hand osteoarthritis in community-dwelling older adults in the United Kingdom: prevalence, inter-relationships, risk factor profiles and clinical characteristics at baseline and 3-years. Osteoarthritis Cartilage. 2013 Nov. 21(11):1674-84.[↩]
- KELLGREN JH, MOORE R. Generalized osteoarthritis and Heberden’s nodes. Br Med J. 1952 Jan 26. 1(4751):181-7.[↩]
- McGonagle D, Hermann KG, Tan AL. Differentiation between osteoarthritis and psoriatic arthritis: implications for pathogenesis and treatment in the biologic therapy era. Rheumatology (Oxford). 2015 Jan. 54 (1):29-38. [↩]
- Belhorn LR, Hess EV. Erosive osteoarthritis. Semin Arthritis Rheum. 1993 Apr. 22(5):298-306.[↩]
- Keen HI, Wakefield RJ, Conaghan PG. A systematic review of ultrasonography in osteoarthritis. Ann Rheum Dis. 2009 May. 68(5):611-9.[↩]
- Recht MP, Goodwin DW, Winalski CS, White LM. MRI of articular cartilage: revisiting current status and future directions. AJR Am J Roentgenol. 2005 Oct. 185(4):899-914.[↩]
- [Guideline] Zhang W, Moskowitz RW, Nuki G, Abramson S, Altman RD, Arden N, et al. OARSI recommendations for the management of hip and knee osteoarthritis, Part II: OARSI evidence-based, expert consensus guidelines. Osteoarthritis Cartilage. 2008 Feb. 16(2):137-62.[↩]
- Brown GA. AAOS clinical practice guideline: treatment of osteoarthritis of the knee: evidence-based guideline, 2nd edition. J Am Acad Orthop Surg. 2013;21(9):577–579.[↩][↩][↩]
- Brosseau L, Wells GA, Tugwell P, et al. Ottawa Panel evidence-based clinical practice guidelines for the management of osteoarthritis in adults who are obese or overweight. Phys Ther. 2011;91(6):843–861.[↩]
- Rutjes AW, Nüesch E, Sterchi R, Jüni P. Therapeutic ultrasound for osteoarthritis of the knee or hip. Cochrane Database Syst Rev. 2010;(1):CD003132.[↩]
- Prior MJ, Harrison DD, Frustaci ME. A randomized, double-blind, placebo-controlled 12 week trial of acetaminophen extended release for the treatment of signs and symptoms of osteoarthritis. Curr Med Res Opin. 2014;30(11):2377–2387.[↩]
- Hochberg MC, Altman RD, April KT, et al. American College of Rheumatology 2012 recommendations for the use of nonpharmacologic and pharmacologic therapies in osteoarthritis of the hand, hip, and knee. Arthritis Care Res (Hoboken). 2012;64(4):465–474.[↩][↩]
- Jones T, Kelsberg G, Safranek S. FPIN’s clinical inquiries: Intra-articular corticosteroid injections for osteoarthritis of the knee. Am Fam Physician. 2014;90(2):115–116.[↩]
- Brouwer RW, Jakma TS, Verhagen AP, Verhaar JA, Bierma-Zeinstra SM. Braces and orthoses for treating osteoarthritis of the knee. Cochrane Database Syst Rev. 2005;(1):CD004020.[↩]
- Nonsurgical Management of Knee Pain in Adults. Am Fam Physician. 2015 Nov 15;92(10):875-883. https://www.aafp.org/afp/2015/1115/p875.html[↩]
- American Academy of Orthopaedic Surgeons. https://www.aaos.org/uploadedFiles/PreProduction/Quality/Guidelines_and_Reviews/Osteoarthritis%20of%20the%20Knee%20-%20non-arthroplasty.pdf[↩][↩]
- Jordan JM, Helmick CG, Renner JB, Luta G, Dragomir AD, Woodard J, et al. Prevalence of knee symptoms and radiographic and symptomatic knee osteoarthritis in African Americans and Caucasians: the Johnston County Osteoarthritis Project. J Rheumatol. 2007 Jan. 34(1):172-80.[↩]
- American Academy of Orthopaedic Surgeons. Treatment of Osteoarthritis (OA) of the Knee. AAOS: American Academy of Orthopaedic Surgeons.[↩]
- Analgesics for Osteoarthritis: An Update of the 2006 Comparative Effectiveness Review. https://effectivehealthcare.ahrq.gov/topics/osteoarthritis-pain/research/[↩]
- Treatment of Osteoarthritis of the Knee: An Update Review. https://effectivehealthcare.ahrq.gov/topics/osteoarthritis-knee-update/research-2017[↩]
- Citrome L, Weiss-Citrome A. A systematic review of duloxetine for osteoarthritic pain: what is the number needed to treat, number needed to harm, and likelihood to be helped or harmed?. Postgrad Med. 2012 Jan. 124(1):83-93.[↩]
- Frakes EP, Risser RC, Ball TD, Hochberg MC, Wohlreich MM. Duloxetine added to oral nonsteroidal anti-inflammatory drugs for treatment of knee pain due to osteoarthritis: results of a randomized, double-blind, placebo-controlled trial. Curr Med Res Opin. 2011 Dec. 27(12):2361-72.[↩][↩]
- Lineker SC, Bell MJ, Boyle J, Badley EM, Flakstad L, Fleming J, et al. Implementing arthritis clinical practice guidelines in primary care. Med Teach. 2009 Mar. 31(3):230-7.[↩]
- Godwin M, Dawes M. Intra-articular steroid injections for painful knees. Systematic review with meta-analysis. Can Fam Physician. 2004 Feb. 50:241-8.[↩]
- McAlindon TE, LaValley MP, Harvey WF, Price LL, Driban JB, Zhang M, et al. Effect of Intra-articular Triamcinolone vs Saline on Knee Cartilage Volume and Pain in Patients With Knee Osteoarthritis: A Randomized Clinical Trial. JAMA. 2017 May 16. 317 (19):1967-1975.[↩][↩]
- Baraf HSB, et al. Effectiveness of FX006 Intra-Articular Injection in Patients with Knee Osteoarthritis Who Present with and without Clinical Inflammation at Baseline: A Pooled Analysis of Data from 3 Double-Blind, Randomized, Parallel-Group Clinical Trials. ACR/ARHP Annual meeting. September 18, 2017.[↩]
- Lambert RG, Hutchings EJ, Grace MG, Jhangri GS, Conner-Spady B, Maksymowych WP. Steroid injection for osteoarthritis of the hip: a randomized, double-blind, placebo-controlled trial. Arthritis Rheum. 2007 Jul. 56(7):2278-87.[↩]
- Bellamy N, Campbell J, Robinson V, Gee T, Bourne R, Wells G. Viscosupplementation for the treatment of osteoarthritis of the knee. Cochrane Database Syst Rev. 2006 Apr 19. CD005321.[↩]
- Goldberg VM, Buckwalter JA. Hyaluronans in the treatment of osteoarthritis of the knee: evidence for disease-modifying activity. Osteoarthritis Cartilage. 2005 Mar. 13(3):216-24.[↩]
- Altman RD, Moskowitz R. Intraarticular sodium hyaluronate (Hyalgan) in the treatment of patients with osteoarthritis of the knee: a randomized clinical trial. Hyalgan Study Group. J Rheumatol. 1998 Nov. 25(11):2203-12.[↩]
- Waddell DD, Kolomytkin OV, Dunn S, Marino AA. Hyaluronan suppresses IL-1beta-induced metalloproteinase activity from synovial tissue. Clin Orthop Relat Res. 2007 Dec. 465:241-8.[↩]
- Rabago D, Patterson JJ, Mundt M, Kijowski R, Grettie J, Segal NA, et al. Dextrose prolotherapy for knee osteoarthritis: a randomized controlled trial. Ann Fam Med. 2013 May-Jun. 11(3):229-37. [↩]
- Sawitzke AD, Shi H, Finco MF, Dunlop DD, Bingham CO 3rd, Harris CL, et al. The effect of glucosamine and/or chondroitin sulfate on the progression of knee osteoarthritis: a report from the glucosamine/chondroitin arthritis intervention trial. Arthritis Rheum. 2008 Oct. 58(10):3183-91.[↩][↩]
- Clegg DO, Reda DJ, Harris CL, et al. Glucosamine, chondroitin sulfate, and the two in combination for painful knee osteoarthritis. N Engl J Med. 2006 Feb 23. 354(8):795-808.[↩]
- Rutjes AW, Nüesch E, Reichenbach S, Jüni P. S-Adenosylmethionine for osteoarthritis of the knee or hip. Cochrane Database Syst Rev. 2009 Oct 7. CD007321.[↩]
- Hathcock JN, Shao A. Risk assessment for glucosamine and chondroitin sulfate. Regul Toxicol Pharmacol. 2007 Feb. 47(1):78-83.[↩]
- Gege C, Bao B, Bluhm H, Boer J, Gallagher BM, Korniski B, et al. Discovery and evaluation of a non-Zn chelating, selective matrix metalloproteinase 13 (MMP-13) inhibitor for potential intra-articular treatment of osteoarthritis. J Med Chem. 2012 Jan 26. 55(2):709-16.[↩]
- Brown MT, Murphy FT, Radin DM, Davignon I, Smith MD, West CR. Tanezumab reduces osteoarthritic knee pain: results of a randomized, double-blind, placebo-controlled phase III trial. J Pain. 2012 Aug. 13(8):790-8.[↩]
- Cui GH, Wang YY, Li CJ, Shi CH, Wang WS. Efficacy of mesenchymal stem cells in treating patients with osteoarthritis of the knee: A meta-analysis. Exp Ther Med. 2016 Nov. 12 (5):3390-3400.[↩]
- Treatment of Osteoarthritis of the Knee: An Update. https://effectivehealthcare.ahrq.gov/topics/osteoarthritis-knee-update/research-protocol[↩]





{kind=link}