Contents
- What is osteochondroma
- Is osteochondroma serious?
- Osteochondroma causes
- Osteochondroma symptoms
- Osteochondroma complications
- Osteochondroma diagnosis
- Osteochondroma treatment
- Hereditary multiple osteochondromas
What is osteochondroma
An osteochondroma is a benign (non-cancerous) bone tumor that develops during childhood or adolescence. Osteochondroma is an abnormal growth that forms on the surface of a bone near the growth plate surrounded by a cartilage layer 1. Osteochondromas can develop as a single tumor (osteocartilaginous exostosis) or as many tumors (multiple osteochondromatosis). Because symptoms and treatment options may vary depending on which form a patient has.
Growth plates are areas of developing cartilage tissue near the ends of long bones in children. Bone growth occurs from the growth plate, and when a child is fully grown, the growth plates harden into solid bone. An osteochondroma is an outgrowth of the growth plate and is made up of both bone and cartilage. As a child grows, an osteochondroma may grow larger, as well. Once a child has reached skeletal maturity, the osteochondroma typically stops growing, too.
Osteochondromas generally affect the extremities of the long bones in an immature skeleton and deform them. Osteochondromas usually occur singly, but a multiple form of presentation may be found. Osteochondromas have a very characteristic appearance and are easily diagnosed. However, an atypical site (in the axial skeleton) and/or malignant transformation of the lesion may sometimes make it difficult to identify osteochondromas immediately by means of radiographic examination 1. In these cases, imaging examinations that are more refined are necessary. Although osteochondromas do not directly affect these patients’ life expectancy, certain complications may occur, with varying degrees of severity.
In most cases of osteochondroma, no treatment is required other than regular monitoring of the tumor to identify any changes or complications.
Figure 1. Osteochondroma
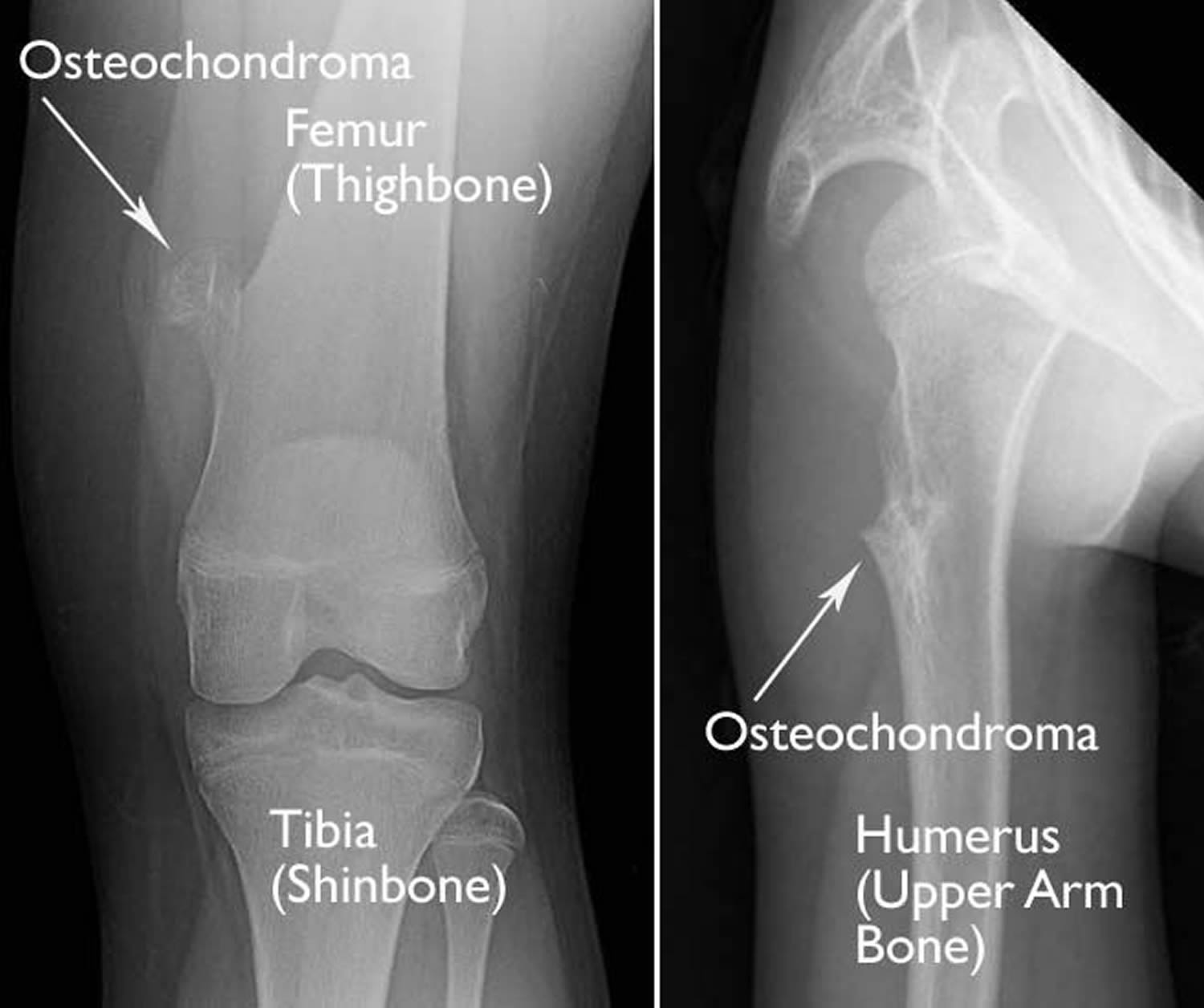
Footnote: (Left) This x-ray taken of the front of the knee shows a typical pedunculated osteochondroma on the femur. (Right) This x-ray of the shoulder taken from the side shows a sessile osteochondroma on the humerus.
[Source 2 ]Figure 2. Osteochondroma knee (sessile osteochondroma)
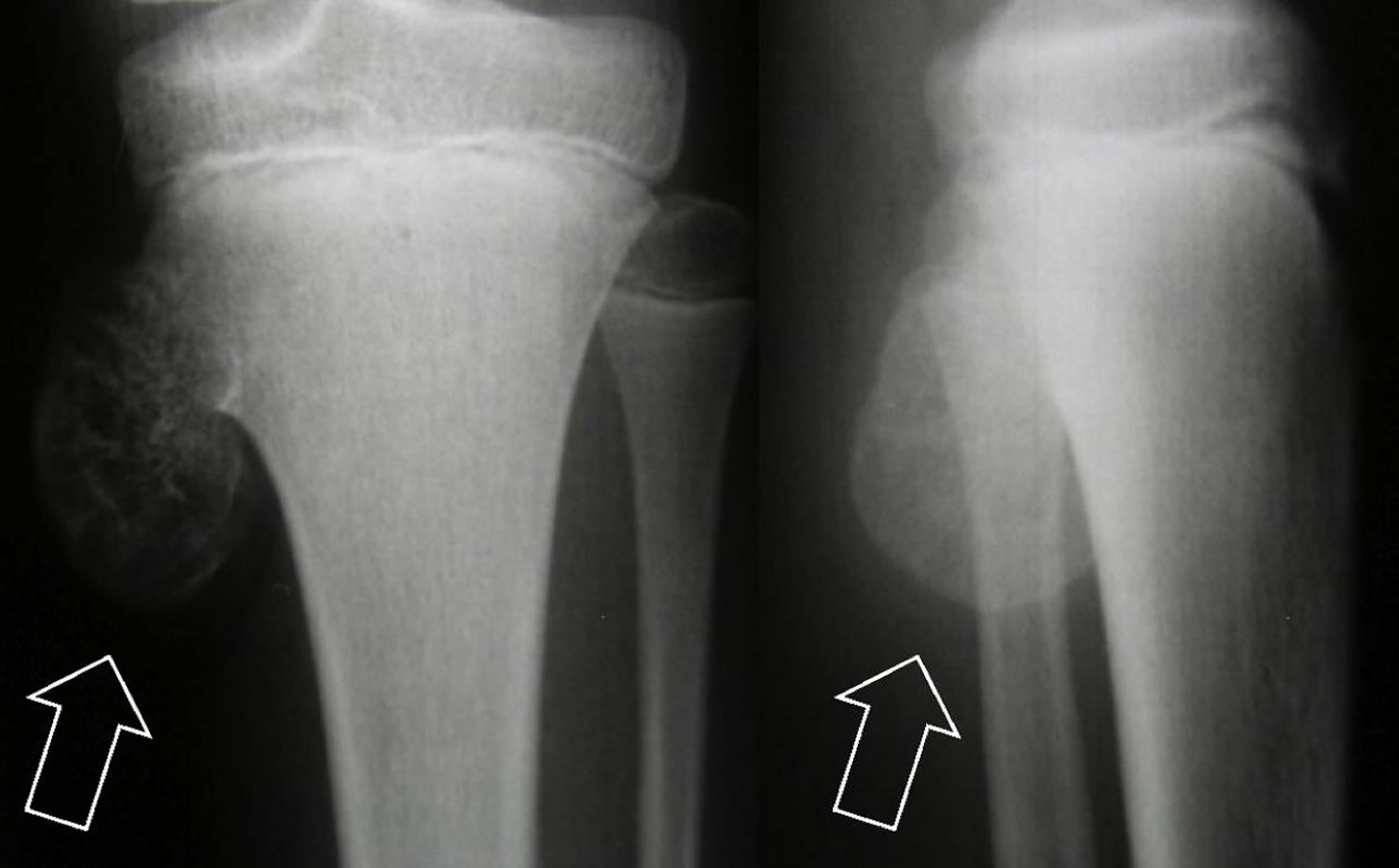
Footnote: Anteroposterior (AP) radiograph (A) and lateral radiograph (B) of the left knee. Note exostosis (osteochondroma – arrows) in the proximal region of the tibia in a skeletally immature patient.
[Source 1 ]Solitary osteochondroma
Solitary osteochondromas are thought to be the most common benign bone tumor, accounting for 35% to 40% of all benign bone tumors. A benign bone tumor is not cancer and does not spread (metastasize) to other parts of the body.
As a child grows, a solitary osteochondroma may develop if bone grows out from the growth plate instead of in line with it. Solitary osteochondromas are commonly found at the end of long bones where they meet to form joints, such as the knee, hip, and shoulder.
Solitary osteochondroma bone outgrowth may have a stalk or stem that sticks out from the normal bone. If the tumor has a stalk, the structure is called pedunculated osteochondroma. If the tumor outgrowth is attached to the bone with a broader base, it is called sessile osteochondroma.
Is osteochondroma serious?
Osteochondromas are typically benign; however, in some instances these tumors become malignant (cancerous). The estimated risk of malignant transformation in hereditary multiple osteochondromas (see description below) has varied within studies, the majority of researchers agree the lifetime risk is between 1-2% 3. The average age for a malignant transformation to occur is between 28-35 years old. Malignant transformation is very rare in children, but the risk increases with age, especially after the age of 30 4.
In 2011, a group of researchers tried to find risk factors which might indicate individuals with hereditary multiple osteochondromas at a greater risk for developing chondrosarcomas (the cancerous form of osteochondromas). The study looked at gender, number of exostoses, genetic disposition and type of mutation. None of the factors were found to correlate with an increased or decreased risk of malignant transformation 5.
In people with the hereditary multiple osteochondromas, where people develop multiple benign (noncancerous) osteochondromas, the multiple osteochondromas can disrupt bone growth and can cause growth disturbances of the arms, hands, and legs, leading to short stature, knock-knees and ankles, and deformities of the forearms. Often these problems with bone growth do not affect the right and left limb equally, resulting in uneven limb lengths (limb length discrepancy). Bowing of the forearm or ankle and abnormal development of the hip joints (hip dysplasia) caused by osteochondromas can lead to difficulty walking and general discomfort. Multiple osteochondromas may also result in pain, limited range of joint movement, and pressure on nerves, blood vessels, the spinal cord, and tissues surrounding the osteochondromas.
Is screening recommended for malignant transformation in hereditary multiple osteochondromas?
At present, medical researchers agree that more studies need to be performed to determine the best screening protocols for those with hereditary multiple osteochondromas, including the study of benefit/cost/risk 6.
However a compelling study was published in 2014 by Czajka and DiCaprio 3 which compares the screening of malignant transformation in people with hereditary multiple osteochondromas to the screening of breast and cervical cancer in women. The authors conclude that screening should be offered to individuals with hereditary multiple osteochondromas over the age of 16 (or when bone growth has been completed). They propose screening should include a thorough clinical examination and a full body MRI every two years. If an MRI is not possible than a bone scan be performed, followed by an ultrasound of the cartilage cap of any suspicious findings 3.
The Czajka and DiCaprio 3 further recommend that individuals with hereditary multiple osteochondromas should be made aware of warning signs of malignant transformation and taught self examination techniques.
Osteochondroma causes
The exact cause of osteochondroma is unknown. It does not result from injury. Both males and females are equally likely to develop it.
Osteochondromas are thought to be associated with a gene called EXT 1. How a defect in this gene may cause the tumors is currently poorly understood. Researchers are investigating it.
Because the cause of a solitary osteochondroma is unknown, doctors have not been able to find a way to prevent it.
Osteochondroma symptoms
In many cases, solitary osteochondromas do not cause any symptoms, or symptoms may arise long after tumors develop. Osteochondromas are most often diagnosed in patients aged 10 to 30 years.
Symptoms of an osteochondroma include:
- A painless bump near the joints. The knee and shoulder are most often involved.
- Pain with activity. An osteochondroma can be located under a tendon (the tough, fibrous tissue that connects muscle to bone). When it is, the tendon may move and “snap” over the bony tumor, causing pain.
- Numbness or tingling. An osteochondroma can be located near a nerve, such as behind the knee. If the tumor puts pressure on a nerve, there may be numbness and tingling in the associated limb.
- Changes in blood flow. A tumor that presses on a blood vessel may cause periodic changes in blood flow. This can cause loss of pulse or changes in color of the limb. Changes in blood flow resulting from an osteochondroma are rare.
In some cases, an injury can cause the stalk of a pedunculated osteochondroma to break. This will cause immediate pain and swelling in the area of the tumor.
Osteochondroma complications
Among the possible complications of these lesions are fractures (generally of pedunculated exostoses, at their base), vascular lesions (formation of pseudoaneurysm) and neurological complications (compression of peripheral nerves, which involves the spine or the periarticular regions), formation of a bursa (which affects the cartilaginous surface of the lesion, resulting from local friction) and malignant transformation 7. This last complication, which is the most feared of all the complications, is very variable in frequency: in solitary osteochondroma cases, it occurs in less than 1% 8; while in patients with multiple osteochondromas it may range from 1% to 30% 9 in different series. However, studies conducted more recently have suggested that the prevalence is lower: 3% to 5% in individuals with multiple osteochondromatosis 10.
Osteochondroma diagnosis
Because many osteochondromas do not cause any discomfort or other symptoms, they are often discovered by accident when an x-ray is done for an unrelated reason.
If you do have symptoms that cause you to seek a doctor’s care, your appointment will begin with a medical history and a physical examination.
Medical History and Physical Examination
Before a physical examination, your doctor will talk with you about your general health, as well as your symptoms in order to get a good history of the problem. During the physical examination, your doctor will look for tenderness over the bone and check your range of motion in the area of your pain.
Tests
In order to diagnose osteochondroma, your doctor will order imaging tests.
- X-rays. These tests provide clear pictures of dense structures like bone, and will show the bony growth of an osteochondroma.
- Other imaging scans. Your doctor may also request computerized tomography (CT) scans or magnetic resonance imaging (MRI) scans to help further define the tumor. These scans can provide more detail, especially of soft tissues. They can also provide cross-sectional images. An MRI scan may be used to look for cartilage on the surface of the tumor. Although it is rare for an osteochondroma to change into a cancerous tumor, it is possible. In adults, a thick covering of cartilage over the tumor is one sign of such a change. A tumor in an adult patient should be checked for cancer if it is enlarging or has become painful.
- Bone biopsy. In some cases, a bone biopsy may be ordered to determine if a tumor is cancerous. In a bone biopsy, a tissue sample of the tumor is taken and examined under a microscope. Your doctor may give you a local anesthetic to numb the area and take a sample using a needle. Biopsies can also be performed as a small operation.
Osteochondroma treatment
In most cases of solitary osteochondroma, treatment consists of careful observation over time. Your doctor may want to take regular x-rays to keep track of any changes in the tumor.
Osteochondroma surgery
Your doctor may consider surgery if the osteochondroma:
- Causes pain
- Puts pressure on a nerve or blood vessel
- Has a large cap of cartilage
To completely remove an osteochondroma, your doctor will perform a surgical procedure called excision. In this procedure, the tumor will be removed at the level of the normal bone.
How long it takes to return to daily activities will vary depending on the tumor’s size and location. If you have any pain or discomfort, you may want to limit some activity. Your doctor will provide you with specific instructions to guide your recovery.
Hereditary multiple osteochondromas
Hereditary multiple osteochondromas is also referred to as multiple osteocartilaginous exostosis, multiple hereditary exostosis, familial osteochondromatosis, multiple osteochondromatosis or diaphyseal aclasia. Hereditary multiple osteochondromas is a condition in which people develop multiple benign (noncancerous) bone tumors called osteochondromas. The number of osteochondromas and the bones on which they are located vary greatly among affected individuals. The osteochondromas are not present at birth, but approximately 96 percent of affected people develop multiple osteochondromas by the time they are 12 years old. Osteochondromas typically form at the end of long bones and on flat bones such as the hip and shoulder blade.
The incidence of hereditary multiple osteochondromas is estimated to be 1 in 50,000 individuals. This condition occurs more frequently in some isolated populations: the incidence is approximately 1 in 1,000 in the Chamorro population of Guam and 1 in 77 in the Ojibway Indian population of Manitoba, Canada.
About 96% of females with a mutation responsible for hereditary multiple osteochondromas will develop osteochondromas (a phenomenon known as reduced penetrance), and 100% of males will develop osteochondromas 11. It is not known why some females with a mutation responsible for hereditary multiple osteochondromas do not develop signs and symptoms.
Both pedunculated and sessile osteochondromas may develop. Multiple osteochondromas can disrupt bone growth and can cause growth disturbances of the arms, hands, and legs, leading to short stature, knock-knees and ankles, and deformities of the forearms. Often these problems with bone growth do not affect the right and left limb equally, resulting in uneven limb lengths (limb length discrepancy). Bowing of the forearm or ankle and abnormal development of the hip joints (hip dysplasia) caused by osteochondromas can lead to difficulty walking and general discomfort. Multiple osteochondromas may also result in pain, limited range of joint movement, and pressure on nerves, blood vessels, the spinal cord, and tissues surrounding the osteochondromas.
Due to these more obvious signs, children with severe multiple osteochondromatosis are often identified early. However, like solitary osteochondroma, mild osteochondromatosis may not be diagnosed until early adulthood. Hereditary multiple osteochondromas is more common in males than females.
Osteochondromas are typically benign; however, in some instances these tumors become malignant (cancerous). The risk of hereditary multiple osteochondromas changing to cancer (malignant transformation) is greater than solitary osteochondroma. Researchers estimate that people with hereditary multiple osteochondromas have a 1 in 20 to 1 in 200 lifetime risk of developing cancerous osteochondromas (called sarcomas).
Hereditary multiple osteochondromas cause
Over 70% of the time, multiple osteochondromatosis is inherited. The other 30% of cases occur randomly.
Like solitary osteochondroma, mutations in the EXT1 and EXT2 genes cause hereditary multiple osteochondromas. The EXT1 gene and the EXT2 gene provide instructions for producing the proteins exostosin-1 and exostosin-2, respectively. The two exostosin proteins bind together and form a complex found in a cell structure called the Golgi apparatus, which modifies newly produced enzymes and other proteins. In the Golgi apparatus, the exostosin-1 and exostosin-2 complex modifies a protein called heparan sulfate so it can be used by the cell.
When there is a mutation in exostosin-1 or exostosin-2, heparan sulfate cannot be processed correctly and is nonfunctional. Although heparan sulfate is involved in many bodily processes, it is unclear how the lack of this protein contributes to the development of osteochondromas.
If the condition is caused by a mutation in the EXT1 gene it is called hereditary multiple osteochondromas type 1. A mutation in the EXT2 gene causes hereditary multiple osteochondromas type 2. While both type 1 and type 2 involve multiple osteochondromas, mutations in the EXT1 gene likely account for 55 to 75 percent of all cases of hereditary multiple osteochondromas, and the severity of symptoms associated with osteochondromas seems to be greater in type 1.
Researchers estimate that about 15 percent of people with hereditary multiple osteochondromas have no mutation in either the EXT1 or the EXT2 gene. It is not known why multiple osteochondromas form in these individuals.
Multiple osteochondromas inheritance pattern
Hereditary multiple osteochondromas is inherited in an autosomal dominant pattern, which means one copy of the altered gene in each cell is sufficient to cause the disorder.
About 96% of females with a mutation responsible for hereditary multiple osteochondroma will develop osteochondromas (a phenomenon known as reduced penetrance), and 100% of males will develop osteochondromas 11.
Hereditary multiple osteochondromas symptoms
The symptoms of multiple osteochondromatosis are similar to those of solitary osteochondroma, only often more severe. It can cause painless bumps at the sites of tumors. Pain and other discomforts are possible should tumors put pressure on soft tissues, nerves, or blood vessels.
Signs and symptoms of malignant transformation in hereditary multiple osteochondromas
A doctor may become suspicious of a malignant transformation if there is an increase in the size of the tumor in adults when bone growth is already complete. In addition, cancer should be suspected if the thickness of the cartilaginous cap of the osteochondroma is over 1-2 centimeters (normally, after bone growth is complete, the cap is only a few millimeters thick) 3.
Other signs of a malignant transformation may include bone pain, temporary loss of sensory or motor function due to compression of a nerve (neurapraxia) or pressure related symptoms in nearby organs 3.
Hereditary multiple osteochondromas diagnosis
Diagnosing multiple osteochondromatosis includes a medical history and physical examination, as well as imaging tests. The median age of diagnosis is three years; nearly all affected individuals are diagnosed by age 12 years 11.
Multiple osteochondromatosis can be seen on a plain x-ray. The findings are generally more severe than those of solitary osteochondroma.
Orthopaedic oncology evaluation. If you have any symptoms of a tumor becoming cancerous, you should be evaluated by a doctor who specializes in the treatment of bone tumors (an orthopedic oncologist).
Symptoms and signs of a tumor becoming cancerous are:
- Growth of an osteochondroma after puberty
- Pain at the site of an osteochondroma
- A cartilage cap thicker than 2 cm
- Surface irregularities and unorganized chalk deposits with light areas in the middle of the tumor and cartilage cap may be seen on a bone scan, ultrasound or preferably an MRI. However the diagnosis of chondrosarcoma can only be confirmed by a bone biopsy 3.
If cancer is suspected, you will need a thorough evaluation that includes MRI and CT scans of the tumors. Your doctor may also order a CT scan of your chest to look for any disease that may have traveled through the bloodstream to your lungs. A biopsy of the tumor tissue will confirm whether there is any cancer.
When an osteochondroma becomes cancerous, it most commonly changes into a cancer called chondrosarcoma.
Hereditary multiple osteochondromas treatment
In most cases, treatment consists of careful observation over time. Your doctor may want to take regular x-rays to keep track of any changes in the tumors.
Indications for surgical removal of tumors are the same as for solitary osteochondromas: pain, pressure on nerves or blood vessels, and a large cap of cartilage.
Surgical treatment
If surgical removal of an osteochondroma is indicated, the procedure is the same as with a solitary tumor. Deformities such as knock-knees or ankles may require surgery to straighten the bone.
Should multiple osteochondromatosis become cancerous, treatment will depend on the stage of the cancer’s progress. In general, malignant tumors are removed using surgery and no further treatment is recommended. Rarely, radiation therapy and chemotherapy are used in combination with surgery.
Chondrosarcomas in a person with hereditary multiple osteochondromas tend to be well differentiated and low grade tumors. The tumors usually grow slowly and do not readily metastasize. Surgical removal is the recommended treatment as the condrosarcomas do not respond to radiation or chemotherapy 3.
The prognosis or long term outlook after surgical removal of the chondrosarcoma for a person with hereditary multiple osteochondromas is good as long as the tumor has not metastasized 3.
- de Souza AM, Bispo Júnior RZ. Osteochondroma: ignore or investigate?. Rev Bras Ortop. 2014;49(6):555-64. Published 2014 Oct 27. doi:10.1016/j.rboe.2013.10.002 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4487501/[↩][↩][↩]
- Osteochondroma. https://orthoinfo.aaos.org/en/diseases–conditions/osteochondroma/[↩]
- Czajka CM & DiCaprio MR. What is the Proportion of Patients With Multiple Hereditary Exostoses Who Undergo Malignant Degeneration. Clin Orthop Relat Res. July 2015; 473(7):2344-61. http://www.ncbi.nlm.nih.gov/pubmed/25582066[↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Sonne-Holm E, Wong C, & Sonne-Holm S. Multiple cartilaginous exostoses and development of chondrosarcomas–a systematic review. Dan Med J. September 2014; 61(9):A4895. http://www.ncbi.nlm.nih.gov/pubmed/25186537[↩]
- Pedrini E, Tremosini M, Milanesi A et al. Genotype-phenotype correlation study in 529 patients with multiple hereditary exostoses: Identification of protective and risk factors. J Bone Joint Surg. 2011; 93-A:2292-302. http://www.ncbi.nlm.nih.gov/pubmed/22258776[↩]
- Wuyts W, Schmale GA, Chansky HA & Raskind WH. Hereditary Multiple Osteochondromas. GeneReveiws. November 2013; http://www.ncbi.nlm.nih.gov/pubmed/22258776[↩]
- Shah Z.K., Peh W.C., Wong Y., Shek T.W., Davies A.M. Sarcomatous transformation in diaphyseal aclasis. Australas Radiol. 2007;51(2):110–119.[↩]
- Khurana J., Abdul-Karim F., Bovée J.V.M. Osteochondroma. In: Fletcher C.D., Unni K.K., Mertens F., editors. Pathology and genetics of tumours of the soft tissues and bones. IARC Press; Lyon: 2002. pp. 234–237.[↩]
- Meissner S.A., Vieth V., August C., Winkelmann W. Radiology–pathology conference: osteosarcoma in a cartilaginous exostosis of the femur. Clin Imaging. 2006;30(3):206–209.[↩]
- Bell R.S. Musculoskeletal images. Malignant transformation in familial osteochondromatosis? Can J Surg. 1999;42(1):8[↩]
- Wuyts W, Schmale GA, Chansky HA, et al. Hereditary Multiple Osteochondromas. 2000 Aug 3 [Updated 2013 Nov 21]. In: Adam MP, Ardinger HH, Pagon RA, et al., editors. GeneReviews® [Internet]. Seattle (WA): University of Washington, Seattle; 1993-2019. Available from: https://www.ncbi.nlm.nih.gov/books/NBK1235[↩][↩][↩]





{kind=link}