
Contents
- What is patellofemoral pain syndrome
What is patellofemoral pain syndrome
Patellofemoral pain syndrome (often called anterior knee pain or runner’s knee) is the medical term for pain felt under and around your kneecap, where your patella (kneecap) articulates with your thigh bone (femur). This joint is known as your patellofemoral joint (see Figures 1 and 2). Patellofemoral pain syndrome is one of the most common knee complaints of both the young active sportsperson and the elderly. The pain can get worse when you’re active or when you sit for a long time. You can have the pain in one or both knees.
Aching kneecaps (patellofemoral pain) affect 25% of the population at some time in their lives but it is more common in athletes. The sports where patellofemoral pain syndrome is typically seen are those when running, jumping and landing or the squatting position is required.
Sports include running, tennis, netball, football, volleyball, basketball, skiing and other jumping sports.
Patellofemoral pain syndrome occurs when nerves sense pain in the soft tissues and bone around the kneecap. These soft tissues include the tendons, the fat pad beneath the patella, and the synovial tissue that lines the knee joint.
In some cases of patellofemoral pain, a condition called chondromalacia patella is present. Chondromalacia patella is the softening and breakdown of the articular cartilage on the underside of the kneecap. There are no nerves in articular cartilage—so damage to the cartilage itself cannot directly cause pain. It can, however, lead to inflammation of the synovium and pain in the underlying bone.
Patellofemoral pain syndrome can be defined as anterior knee pain involving the patella and retinaculum that excludes other intraarticular and peri-patellar pathology 1. Palpation of the bony and soft tissue structures should be performed in an attempt to identify the anatomic site of the pain. Chondromalacia patellae, a condition in which there is softening of the patellar articular cartilage, occurs in only a subset of patients who present with anterior knee pain 2.
Patellofemoral pain syndrome is mainly due to excessive patellofemoral joint pressure from poor kneecap alignment, which in time, affects the joint surface behind the kneecap (retropatellar joint). Studies have shown patellofemoral pain syndrome to be the most common single diagnosis among runners and in sports medicine centers 3. Eleven percent of musculoskeletal complaints in the office setting are caused by anterior knee pain (which most commonly results from patellofemoral pain syndrome), and patellofemoral pain syndrome constitutes 16 to 25 percent of all injuries in runners 3.
The diagnosis of patellofemoral pain syndrome is made clinically, and although management can be challenging, a well-designed, nonoperative treatment program usually allows patients to return to recreational and competitive activities.
Untreated patellofemoral pain syndrome can also predispose you to patellar tendonitis.
Patellofemoral joint anatomy and biomechanics
Your knee is the largest joint in your body and one of the most complex. It is made up of the lower end of the femur (thighbone), the upper end of the tibia (shinbone), and the patella (kneecap).
The patellofemoral joint comprises the patella and the femoral trochlea. The patella acts as a lever and also increases the moment arm of the patellofemoral joint, the quadriceps and patellar tendons 4. Contact of the patella with the femur is initiated at 20 degrees of flexion and increases with further knee flexion, reaching a maximum at 90 degrees 5.
Ligaments and tendons connect the femur to the bones of the lower leg. The four main ligaments in the knee attach to the bones and act like strong ropes to hold the bones together.
Muscles are connected to bones by tendons. The quadriceps tendon connects the muscles in the front of the thigh to the patella. Segments of the quadriceps tendon—called the patellar retinacula—attach to the tibia and help to stabilize the patella. Stretching from your patella to your tibia is the patellar tendon.
Several structures in the knee joint make movement easier. For example, the patella rests in a groove on the top of the femur called the trochlea. When you bend or straighten your knee, the patella moves back and forth inside this trochlear groove.
A slippery substance called articular cartilage covers the ends of the femur, trochlear groove, and the underside of the patella. Articular cartilage helps your bones glide smoothly against each other as you move your leg.
Also aiding in movement is the synovium—a thin lining of tissue that covers the surface of the joint. The synovium produces a small amount of fluid that lubricates the cartilage. In addition, just below the kneecap is a small pad of fat that cushions the kneecap and acts as a shock absorber.
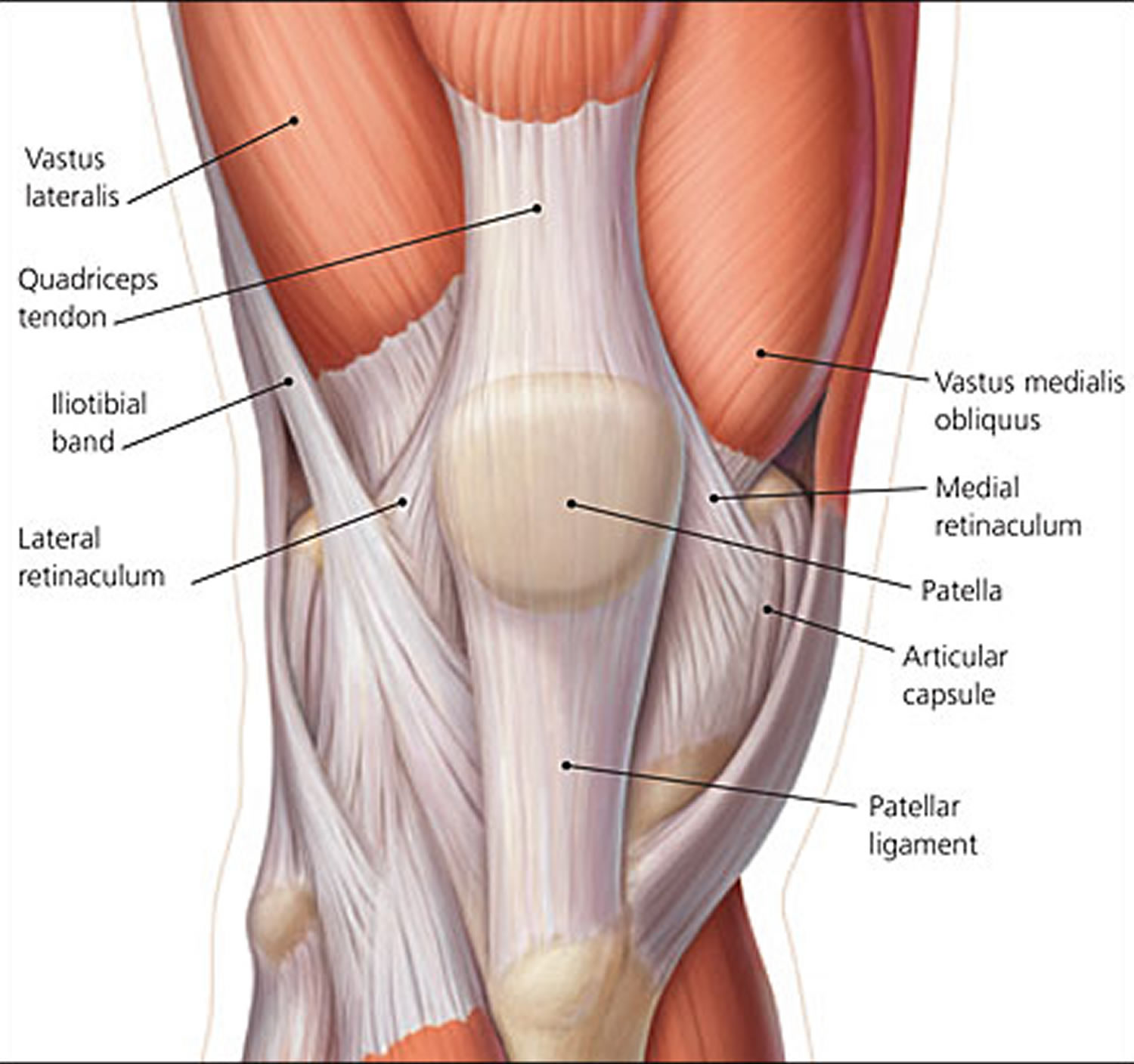
Stability of the patellofemoral joint involves dynamic and static stabilizers (Figure 3), which control movement of the patella within the trochlea, referred to as “patellar tracking.” Dynamic stability of the patellofemoral joint is provided by the quadriceps tendon, patellar tendon, vastus medialis oblique, vastus lateralis, and iliotibial band. The vastus medialis oblique is the only muscle that provides a medial force and is therefore of particular importance in stabilizing the patella. Static stability is provided via the articular capsule, the femoral trochlea, the medial and lateral retinacula, and the patellofemoral ligaments.
Patellar tracking can be altered by imbalances in these stabilizing forces affecting the distribution of forces along the patellofemoral articular surface, the patellar and quadriceps tendons, and the adjacent soft tissues. Forces on the patella range from between one third and one half of a person’s body weight during walking to three times body weight during stair climbing and up to seven times body weight during squatting 6. Abnormalities of patellar tracking must be understood to appreciate the possible causes of patellofemoral pain syndrome and to determine the focus of treatment.
What biomechanical issues cause patellofemoral pain syndrome?
Poor foot posture (e.g., flat feet) and weak hip control muscles can both allow your knee to abnormally twist and result in a lateral deviation of your patella.
When poor biomechanics are repeated with each step of your walking or running pattern that poor habit repeatedly traumatizes your patellofemoral joint.
Figure 1. Knee anatomy
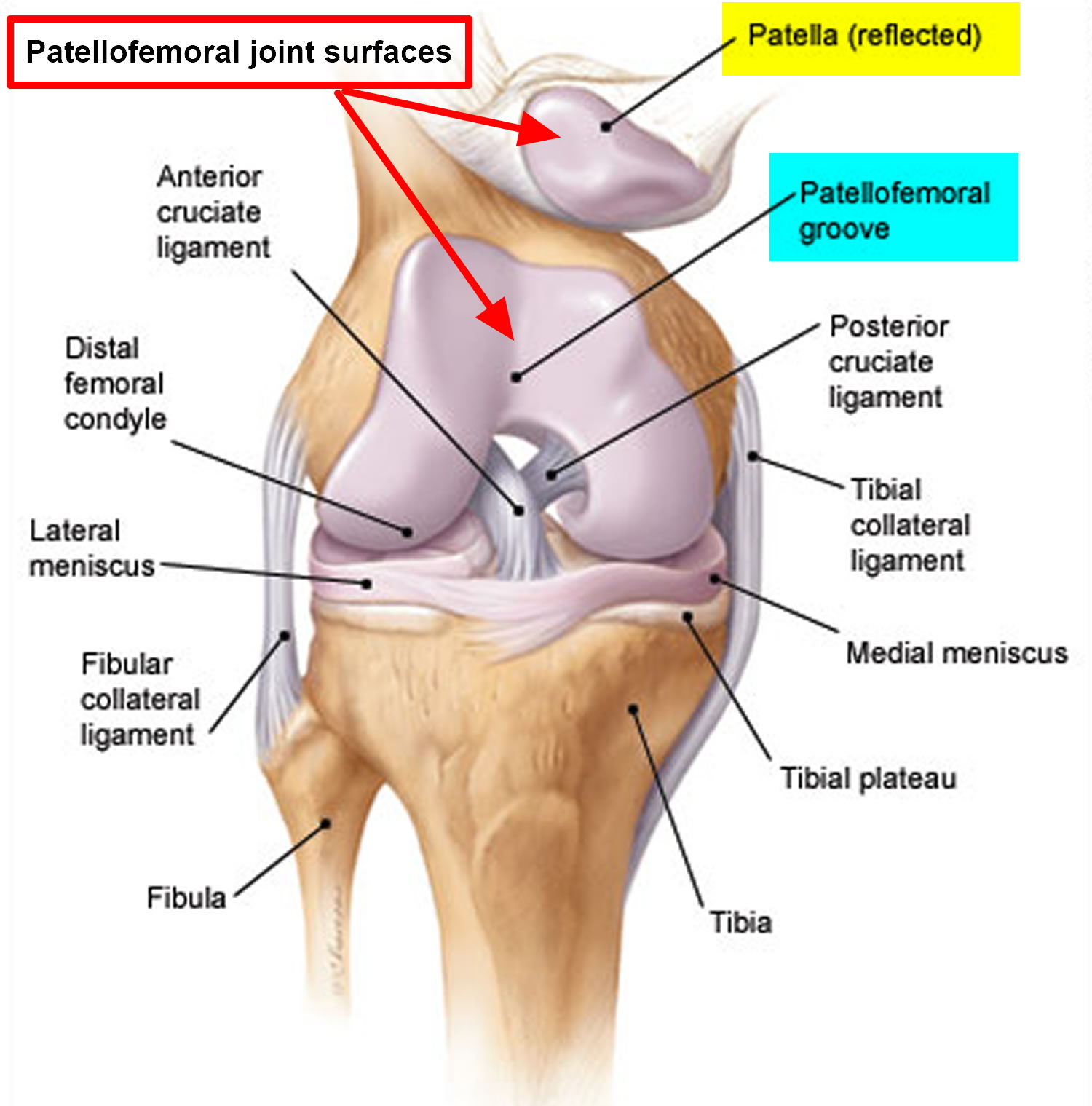
Figure 2. Patellofemoral joint
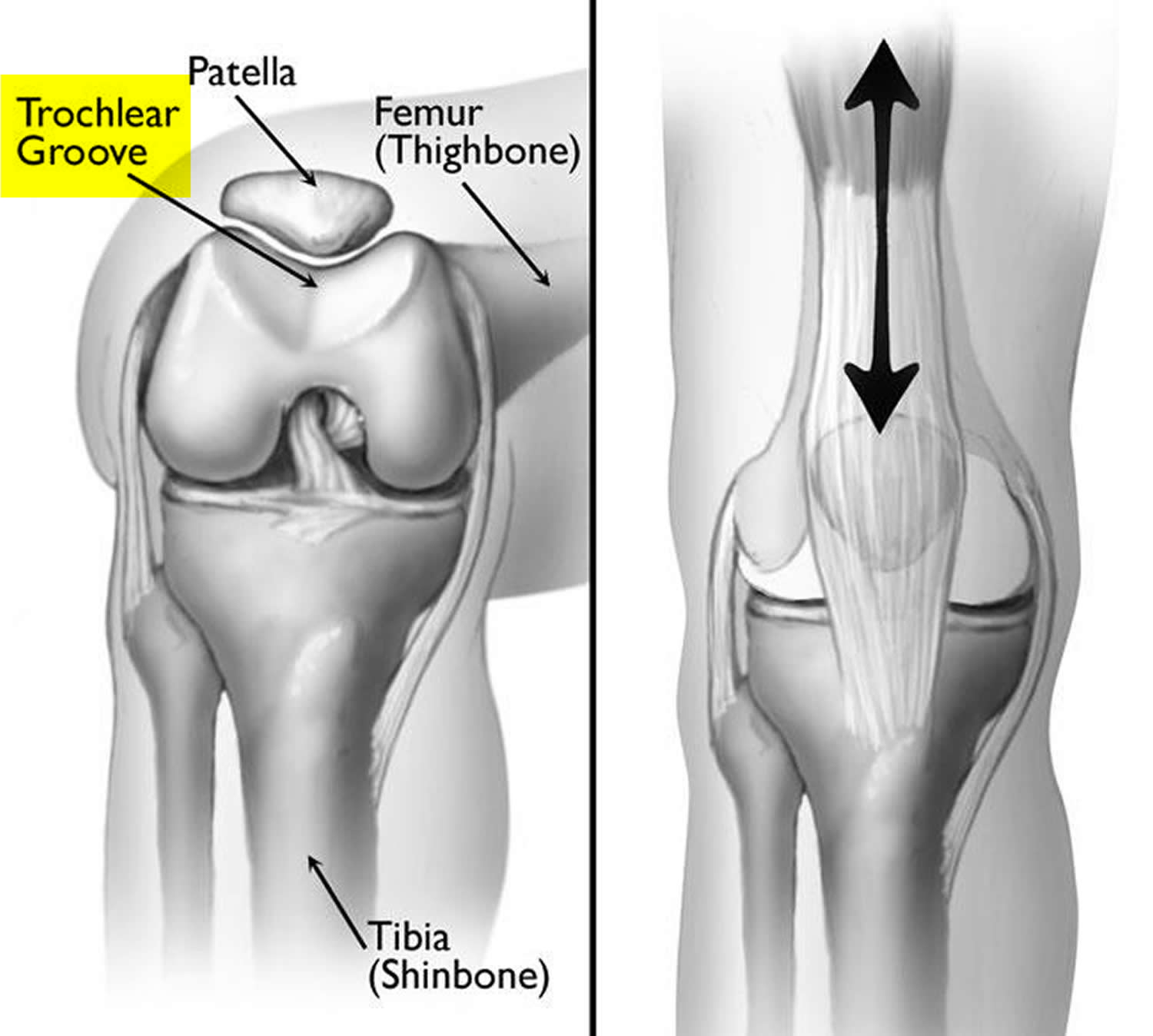
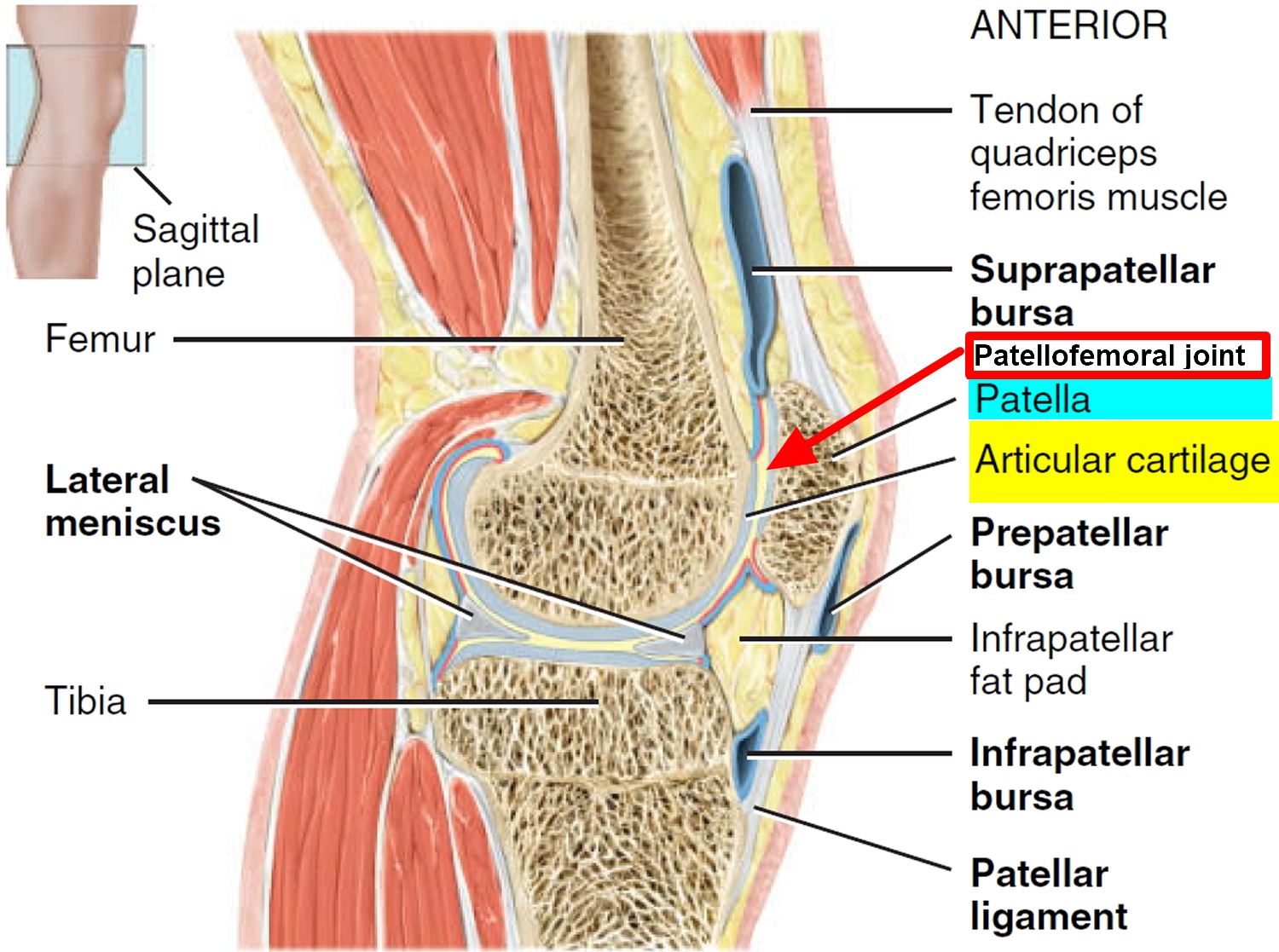
Figure 3. Patellofemoral joint stabilizers
Patellofemoral pain syndrome recovery time
Patellofemoral pain syndrome is usually fully relieved with simple measures or physical therapy. Approximately 90% of patellofemoral syndrome sufferers will be pain-free within six weeks of starting a physiotherapist guided rehabilitation program for patellofemoral pain syndrome. It may recur, however, if you do not make adjustments to your training routine or activity level. It is essential to maintain appropriate conditioning of the muscles around the knee, particularly the quadriceps and the hamstrings.
There are additional steps that you can take to prevent recurrence of patellofemoral knee pain. They include:
- Wearing shoes appropriate to your activities
- Warming up thoroughly before physical activity
- Incorporating stretching and flexibility exercises for the quadriceps and hamstrings into your warm-up routine, and stretching after physical activity
- Increasing training gradually
- Reducing any activity that has hurt your knees in the past
- Maintaining a healthy body weight to avoid over-stressing your knees
For those who fail to respond, surgery may be required to repair associated injuries such as severely damaged or arthritic joint surfaces.
Patellofemoral pain syndrome prognosis
There are few long-term studies on the treatment of patellofemoral pain syndrome. Two studies in which patients were instructed on a program of home exercises reported successful outcomes in approximately 75 to 85 percent of patients with patellofemoral pain syndrome 7, 8. A study of athletes who visited a sports medicine clinic and were instructed on vastus medialis oblique training found that 54 percent were pain free or had mild symptoms after nearly six years 9. Interestingly, arthroscopy findings of the patellar articular surface have not been shown to be predictive of outcome 7. Findings associated with a poorer result include a hypermobile patella, older age, bilateral symptoms, and patellar pain and crepitation on examination 8.
Patellofemoral pain syndrome causes
Doctors aren’t certain what causes patellofemoral pain syndrome, but it’s been associated with:
- Overuse. Running or jumping sports puts repetitive stress on your knee joint, which can cause irritation under the kneecap.
- Muscle imbalances or weaknesses. Patellofemoral pain can occur when the muscles around your hip and knee don’t keep your kneecap properly aligned.
- Inward movement of the knee during a squat has been found to be associated with patellofemoral pain.
- Injury. Trauma to the kneecap, such as a dislocation or fracture, has been linked to patellofemoral pain syndrome.
- Knee surgery, particularly repair to the anterior cruciate ligament using your own patellar tendon as a graft, increases the risk of patellofemoral pain.
Overuse
In many cases, patellofemoral pain syndrome is caused by vigorous physical activities that put repeated stress on the knee —such as jogging, squatting, and climbing stairs. It can also be caused by a sudden change in physical activity. This change can be in the frequency of activity—such as increasing the number of days you exercise each week. It can also be in the duration or intensity of activity—such as running longer distances.
Other factors that may contribute to patellofemoral pain include:
- Use of improper sports training techniques or equipment
- Changes in footwear or playing surface
Patellar Malalignment
Patellofemoral pain syndrome can also be caused by abnormal tracking of the kneecap in the trochlear groove. In this condition, the patella is pushed out to one side of the groove when the knee is bent. This abnormality may cause increased pressure between the back of the patella and the trochlea, irritating soft tissues.
Your patella normally glides up and down through the femoral groove. As your knee is bent, pressure between your kneecap and the groove increases.
This retropatellar pressure is further increased if the patella does not ride normally through the groove, but “mistracks”, meaning it travels more to one side, making it rub against the femur.
Repeated trauma causes an increase in your retro patellar joint forces, which can lead to kneecap pain, joint irritation and eventually degeneration of your patella joint surface.
The most common causes of patellar malalignment are an abnormal muscle imbalance and poor biomechanical control.
Factors that contribute to poor tracking of the kneecap include:
- Problems with the alignment of the legs between the hips and the ankles. Problems in alignment may result in a kneecap that shifts too far toward the outside or inside of the leg, or one that rides too high in the trochlear groove—a condition called patella alta.
- Muscular imbalances or weaknesses, especially in the quadriceps muscles at the front of the thigh. When the knee bends and straightens, the quadriceps muscles and quadriceps tendon help to keep the kneecap within the trochlear groove. Weak or imbalanced quadriceps can cause poor tracking of the kneecap within the groove.
What Causes a Muscle Imbalance?
Your quadriceps (thigh) muscles attach to the patella and through it to the patella tendon, which attaches to the top of your shin.
If there is a muscle imbalance between the quadriceps muscles: vastus lateralis, which pulls your patella up and outwards, and the vastus medialis oblique, which is the only quadriceps muscle that pulls your kneecap up and slightly in, then your patella will track laterally in the groove.
Common reasons for a weak vastus medialis oblique include knee injury, post-surgery, swelling or disuse.
The longstanding tightness of your lateral knee structures (lateral retinaculum, vastus lateralis, and iliotibial band) will encourage your kneecap to drift sideways over time. Especially, if your vastus medialis oblique is also weak.
Your hip muscles have been shown in the research to be very important in the control of your thigh. Poor buttock muscle control allows your knee to roll in and apply a relative lateral displacement of the patella. Most successful rehabilitation programs require assessment and correction of your hip and buttock muscle control.
Patellofemoral pain syndrome is more common during adolescence because the long bones are growing faster than the muscles, tendons and ligaments, putting abnormal stresses on the joints. Active children who do not stretch the appropriate muscles are predisposed to patellar malalignment.
Risk factors for patellofemoral pain syndrome
Several factors may create a predisposition for the development of patellofemoral pain syndrome via alterations in patellar tracking, increased patellofemoral joint forces, or combinations of these biomechanical features. Overuse, trauma, and anatomic factors appear to be the main contributors.
Lower extremity malalignment (caused by abnormalities such as an increased standing Q angle, pes planus (flat foot), or subtalar pronation often has been implicated as a cause of patellofemoral pain syndrome. However, evidence to support a causal relationship between static measures of lower extremity malalignment and lower extremity injury is limited 10. In one prospective study, a small subgroup of runners with patellofemoral pain syndrome was found to have differences in ankle dorsiflexion, genu varum, and forefoot varus compared with noninjured participants 10. Analyses that include a dynamic component may eventually yield more useful information on the role of lower extremity morphology in the development of patellofemoral pain syndrome 10.
Risk Factors for Patellofemoral Pain Syndrome
- Anatomic anomalies (e.g., hypoplasia of the medial patellar facet, patella alta)
- Malalignment and altered biomechanics of the lower extremity (static or dynamic)
- Muscle dysfunction (e.g., quadriceps weakness, improper firing pattern)
- Patellar hypermobility
- Poor quadriceps, hamstring, or iliotibial band flexibility
- Previous surgery
- Tight lateral structures (i.e., lateral retinaculum and iliotibial band)
- Training errors or overuse
- Trauma
- Age. Patellofemoral pain syndrome typically affects adolescents and young adults. Knee problems in older populations are more commonly caused by arthritis.
- Sex. Women are twice as likely as men are to develop patellofemoral pain. This may be because a woman’s wider pelvis increases the angle at which the bones in the knee joint meet.
- Certain sports. Participation in running and jumping sports can put extra stress on your knees, especially when you increase your training level.
Changes in activity patterns, such as an increase in running mileage, running stadium steps for conditioning, or the addition of resistance training exercises that affect the patellofemoral joint, often are associated with symptom onset. Excessively worn or inappropriate footwear also may contribute.
Patellofemoral pain syndrome prevention
Sometimes knee pain just happens. But certain steps may help prevent the pain.
- Maintain strength. Strong quadriceps and hip abductor muscles help keep the knee balanced during activity, but avoid deep squatting during your weight training.
- Think alignment and technique. Ask your doctor or physical therapist about flexibility and strength exercises to optimize your technique for jumping, running and pivoting — and to help the patella track properly in its groove. Especially important is exercise for your outer hip muscles to prevent your knee from caving inward when you squat, land from a jump or step down from a step.
- Lose excess pounds. If you’re overweight, losing weight relieves stress on your knees.
- Warm up. Before running or other exercise, warm up with five minutes or so of light activity.
- Stretch. Promote flexibility with gentle stretching exercises.
- Increase intensity gradually. Avoid sudden changes in the intensity of your workouts.
- Practice shoe smarts. Make sure your shoes fit well and provide good shock absorption. If you have flat feet, consider shoe inserts.
Patellofemoral pain syndrome symptoms
The onset of your kneecap pain is normally gradual rather than traumatic.
Patellofemoral pain symptoms are normally noticed during weight bearing or jarring activities that involve knee bending.
Patellofemoral pain syndrome usually causes a dull, aching pain in the front of your knee. This pain can be aggravated when you:
- Walk up or down stairs
- Kneel or squat
- Sit with a bent knee for long periods of time, such as one does in a movie theater or when riding on an airplane.
- Hopping
- Running
- Popping or crackling sounds in your knee when climbing stairs or when standing up after prolonged sitting.
As your patellofemoral pain syndrome progresses your knee will become painful while walking and then ultimately even at rest.
You can also experience kneecap pain when you are in sustained knee bend e.g. sitting in a chair. A nickname for this condition is “theater knee”.
Patellofemoral pain syndrome diagnosis
Your doctor will ask about your history of knee problems and will press on areas of your knee and move your leg into a variety of positions to help rule out other conditions that have similar signs and symptoms.
A complete examination of the knee, including a careful assessment of the patellofemoral joint, should be performed. The examination should aim to identify features that may alter patellofemoral mechanics.
Quadriceps muscle bulk, especially the vastus medialis oblique, should be assessed by visual inspection and comparison with the opposite side. Measurement of quadriceps muscle girth can be used as a baseline in assessing progress with rehabilitation. Any surgical scars should be noted.
The knee should be assessed for an effusion. A joint effusion is uncommon in patellofemoral pain syndrome and should prompt evaluation for other causes of knee pain. Quadriceps muscle tone can be assessed by direct palpation at rest and with isometric contraction. Careful palpation should be performed in an attempt to isolate the location of the pain. The ligaments also should be examined as part of the comprehensive examination.
Dynamic patellar tracking can be assessed by having the patient perform a single leg squat and stand. Imbalance between the medial and lateral patellar forces (caused by vastus medialis oblique dysfunction or lateral structure tightness) can be manifested by an abrupt medial deviation of the patella as the patella engages the trochlea early in flexion, known as the “J” sign 11. Alternatively, the “J” sign may be observed with the patient supine or seated and the knee extended from a flexed position. Lateral deviation of the patella can be observed during the terminal phase of extension (Figure 4) 12.
Clinical tests for patellar mobility and position, and provocative tests for pain should be performed. The patellar glide (Figure 5), patellar tilt (Figure 6), and patellar grind (Figure 7) tests should be performed as part of the routine assessment of patients with anterior knee pain. Positive results on these tests are consistent with the diagnosis of patellofemoral pain syndrome. The patellar apprehension test is used to assess for lateral instability and is positive when pain or discomfort occurs with lateral translation of the patella.
Medial patellar instability can be assessed by displacing the patella medially with the knee extended, then flexing the knee and releasing the patella. Pain indicates medial subluxation 13. Finally, flexibility of the iliotibial band (ITB), quadriceps, hamstrings, hip flexors, and the gastrocnemius should be evaluated. Tightness of the iliotibial band (ITB) and tightness of the quadriceps have been shown to be risk factors for patellofemoral pain syndrome 14. Poor flexibility in these areas may contribute to stress across the patellofemoral joint, and attention should be directed to this in therapy.
Figure 4. Lateral patellar tracking (“J” sign). As the knee is extended from 90 degrees flexion (A) to full extension (B), the patella demonstrates an abnormal path, deviating laterally at full extension.
Figure 5. Patellofemoral pain syndrome – patellar glide test
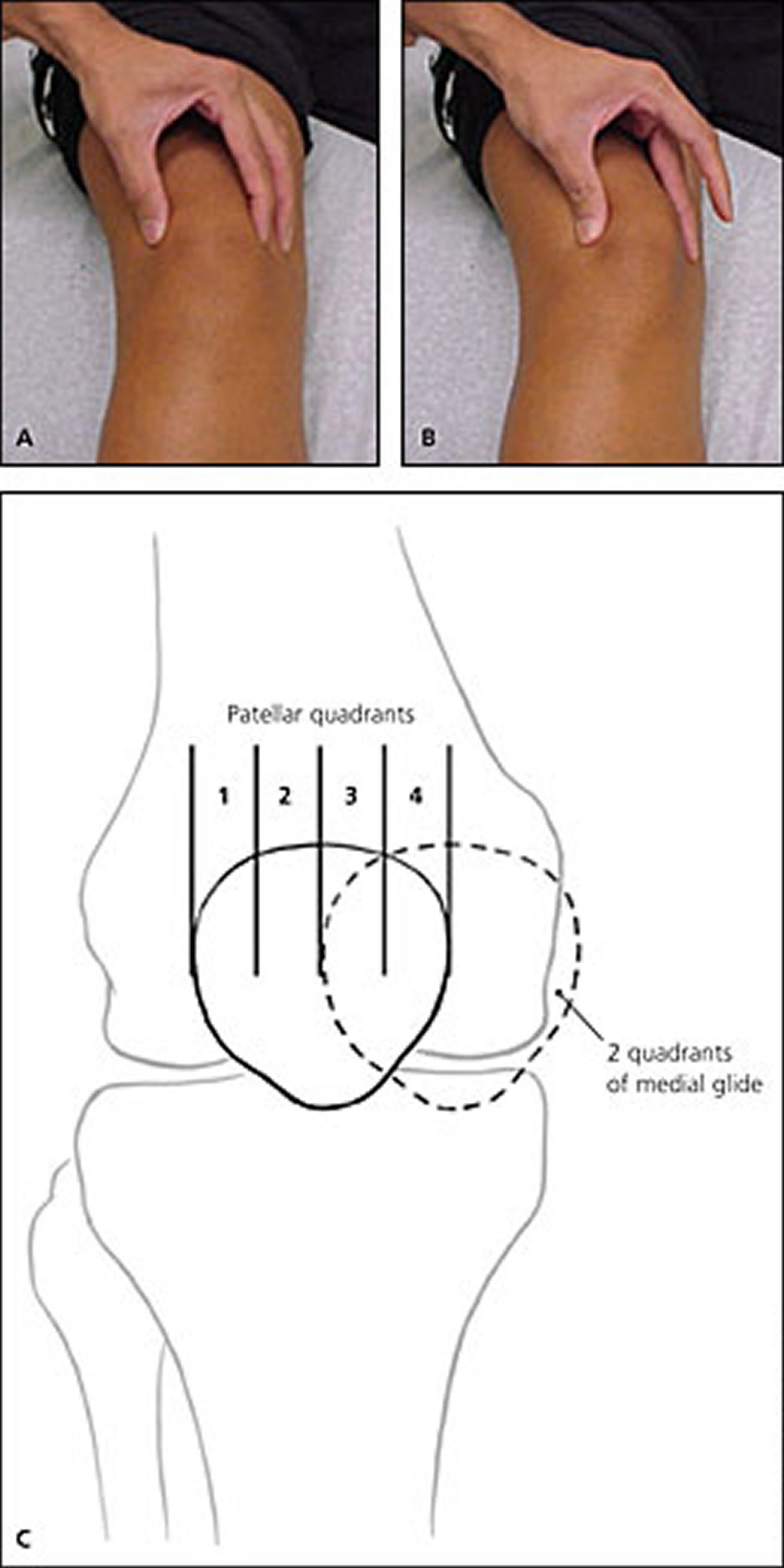
Note: Patellar mobility testing. Depicted is medial glide testing performed on the right knee. The patella is grasped in the resting position (A), then translated medially (B). The extent of displacement is described in relation to the width of the patella and measured in quadrants (C). Displacement of less than one quadrant medially indicates tightness of the lateral structures. Displacement of more than three quadrants is considered hypermobile 13.
Figure 6. Patellofemoral pain syndrome – patellar tilt test
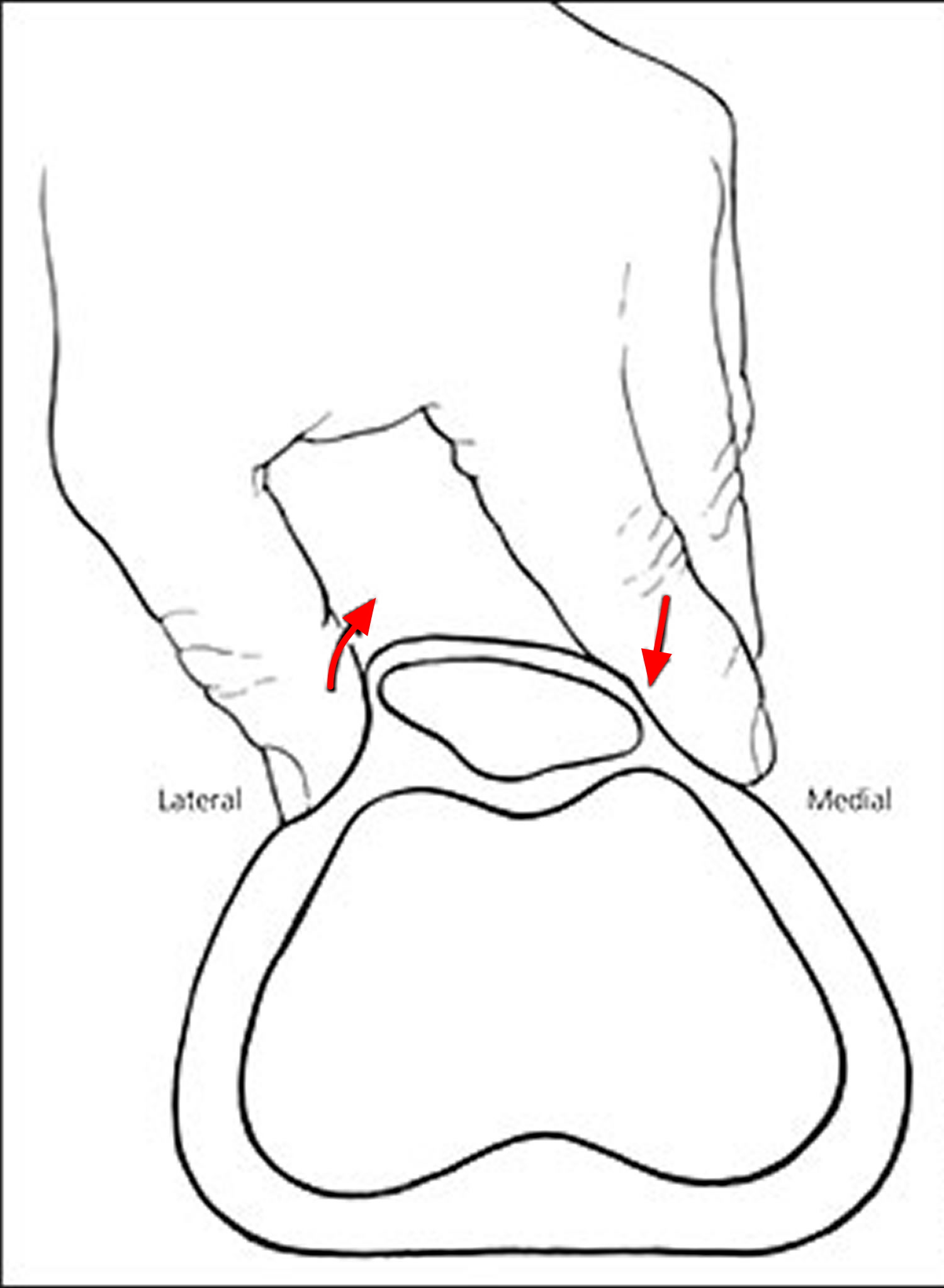
Figure 7. Patellofemoral pain syndrome – patellar grind test

Note: Patellar grind (or inhibition) test. While the patient is in the supine position with the knee extended, the examiner displaces the patella inferiorly into the trochlear groove (pictured). The patient is then asked to contract the quadriceps while the examiner continues to palpate the patella and provides gentle resistance to superior movement of the patella. The test is positive if pain is produced, although comparison to the contralateral knee is needed to interpret the result.
To help determine the cause of your knee pain, your doctor might recommend imaging tests such as:
- X-rays. A small amount of radiation passes through your body in the process of creating X-ray images. This technique visualizes bone well, but it is less effective at viewing soft tissues.
- CT scans. These combine X-ray images from various angles to create cross-sectional images of internal structures. CT scans can visualize both bone and soft tissues, but the procedure delivers a much higher dose of radiation than do plain X-rays.
- MRI. Using radio waves and a strong magnetic field, MRIs produce detailed images of bones and soft tissues, such as the knee ligaments and cartilage. But MRIs are much more expensive than X-rays or CT scans.
Patellofemoral pain syndrome is primarily a clinical diagnosis and, for many patients, treatment can be initiated without imaging. Radiography is an adjunct to the history and physical examination and should be performed in patients with a history of trauma or surgery, those with an effusion, and those whose pain does not improve with treatment. Radiography also may be helpful if a symptomatic bipartite patella is suspected.
In persons older than 50 years, radiography should be considered to assess for patellofemoral osteoarthritis. In patients who are skeletally immature, radiography may be helpful to evaluate for other causes of anterior knee pain, such as osteochondritis dissecans, physeal injury, or bone tumors. Other radiographic findings that may mimic patellofemoral pain syndrome include loose bodies and occult fractures.
When indicated, radiography should include the following views: weight-bearing anterior-posterior, weight-bearing true lateral, and axial. The axial view is taken with 20 to 45 degrees of knee flexion. Abnormalities of lateral patellar displacement, lateral patellar tilt, and dysplasia of the trochlea can be assessed on the axial view. Although these findings may indicate malalignment, they also may be seen in asymptomatic patients and are not predictive of outcome 15. In symptomatic patients, such findings, in combination with the physical examination, may assist in tailoring treatment.
Computed tomography and magnetic resonance imaging (MRI) are not necessary for most patients with patellofemoral pain syndrome. MRI can be helpful in detecting articular cartilage injuries, chondromalacia patellae, patellar stress fractures, and loose bodies. In addition, a pattern of marrow edema involving the medial aspect of the patella and the lateral aspect of the femoral condyle, and tears of the patellofemoral ligament can be seen with MRI and are suggestive of patellar subluxation or dislocation.
Patellofemoral pain syndrome treatment
The aim of treatment is to reduce your pain and inflammation in the short-term and then, more importantly, correct the cause to prevent it returning in the long-term. Usually, putting ice on your knee, changing your activities, and following a physical therapy program works best. This type of program may include exercises to make your muscles stronger and more flexible. Taping the knee or using shoe insoles can be helpful for some people. It may take weeks or months of treatment for the pain to go away.
The RICE Method
RICE stands for rest, ice, compression, and elevation.
- Rest. Avoid putting weight on the painful knee.
- Ice. Use cold packs for 20 minutes at a time, several times a day. Do not apply ice directly on skin.
- Compression. To prevent additional swelling, lightly wrap the knee in an elastic bandage, leaving a hole in the area of the kneecap. Make sure that the bandage fits snugly and does not cause additional pain.
- Elevation. As often as possible, rest with your knee raised up higher than your heart.
Tips to help relieve your pain:
- Take a break from physical activity that causes a lot of pounding on your legs, such as running, volleyball or basketball. If you want to keep exercising, try swimming or another low-impact activity. You may want to try working out on nonimpact elliptical trainers, which are popular at gyms. Because these machines support your body weight, they put less stress on your knees. As your knees feel better, you can go back to your normal sports. But do this slowly, increasing the amount of time you do the sports activity a little at a time.
- Talk to your doctor about footwear. It may help to bring your shoes in for the doctor to see. Proper walking or running shoes can help knee pain. Even a simple arch support insert from a shoe store can be helpful. This insert is less expensive than a custom-made support or brace.
- Ice your knees for 10 to 20 minutes after activity. This can ease the pain and speed up healing. To keep your hands free, use an elastic wrap to hold the ice pack in place. A medicine such as ibuprofen (one brand name: Motrin) may also help relieve your pain, but talk to your doctor before you take this medicine.
- Analgesics. Although nonsteroidal anti-inflammatory drugs (NSAIDs) are commonly prescribed for patients with patellofemoral pain syndrome, there is little evidence supporting their effectiveness 16. NSAIDs or acetaminophen may be considered at the initiation of treatment for patients with symptoms during daily activities and for those whose symptoms are not controlled with ice applications.
Active rest
Reduction of loading to the patellofemoral joint and surrounding soft tissues is the first step to reduce pain. If resistance training exercises have been identified as playing a role in causing the injury, cessation of specific exercises such as full squats and lunges is indicated. Runners should reduce mileage to a level that does not provoke pain (while running or the day after running). Alternative activities such as bicycling, swimming, or the use of an elliptical trainer can be used to maintain fitness while treatment is ongoing. Ice or other methods of cold application may further reduce symptoms. Heat is generally not recommended. Patients may find ice application after activity particularly helpful. Although symptoms usually abate with these methods, further treatment is necessary to avoid recurrence.
Physical therapy
A well-structured rehabilitation program is the mainstay of treatment. Several studies have shown physical therapy to be effective in treating patellofemoral pain syndrome 17. However, there is no one program that will be effective for all patients. The rehabilitation program should focus on correcting maltracking of the patella by addressing the findings identified on the physical examination. Some patients may require significant strengthening of the quadriceps. Others may have excellent quadriceps strength but excessively tight lateral structures or poor quadriceps flexibility. Soft tissue techniques and flexibility exercises can be helpful for these patients. A detailed assessment of the imbalances of patellar tracking is therefore essential to tailoring treatment. Specific exercises can then be prescribed as part of a home rehabilitation program. Patients who require further assessment or ongoing instruction can be referred to a physical therapist.
Your physiotherapist will normally apply kinesiology supportive taping or similar to help relieve your pain and commence your patellofemoral joint realignment phase.
Patellofemoral pain syndrome taping
Patellar taping has been suggested as a method to treat patellofemoral pain syndrome by improving alignment and quadriceps function. Although the results from uncontrolled studies were encouraging, the results of three randomized clinical trials have not been consistent: two found no benefit when patellar taping was added to a program of physical therapy 18, 19, 20. More studies are needed to determine the role of patellar taping in treating patellofemoral pain syndrome.
Patellofemoral pain syndrome foot orthoses
Prospective studies have yet to demonstrate strong relationships between static measures of lower extremity malalignment and lower extremity injuries. Moreover, alignment was not found to be predictive of outcome in patients with patellofemoral pain syndrome in two long-term studies 21, 7. Other studies, however, have shown that orthoses can be effective in some patients with patellofemoral pain syndrome 22. Over-the-counter soft orthoses are a reasonable choice for patients who have patellofemoral pain syndrome with malalignment. For those with persistent symptoms, a custom orthotic can be considered.
Patellofemoral pain syndrome bracing
A variety of braces, sleeves, and straps have been used in the treatment of patellofemoral pain syndrome. Although bracing alone may provide some symptomatic relief, three prospective randomized studies found no significant benefit when bracing was used in addition to physical therapy 23, 24, 25.
Figure 8. Patellofemoral pain syndrome brace

Patellofemoral pain syndrome exercises
These exercises can help strengthen your muscles and relieve your pain. Each exercise should take a few minutes. Doing them twice a day is a good start. Your doctor will tell you which exercises are right for you. After you do the exercises, reverse your position, and do the exercises with your other leg, so both knees get the benefit of stretching.
Be patient! Keep exercising to get better. Patellofemoral pain can be hard to treat, and your knees won’t get better overnight. Some people are lucky and get better quickly. But it might take 6 weeks or longer for your knee to get better. You’ll be less likely to get patellofemoral pain again if you stay in good shape, but don’t make sudden changes in your workouts.
Quadriceps strengthening: Isometrics
Lie flat on a firm surface, such as a floor. Bend your left leg to a 90 degree angle, with your foot flat on the floor. Hold your right leg straight for 10 to 20 seconds and then relax. Do the exercise 5 to 10 times.
Figure 9. Quadriceps strengthening – Isometrics

Quadriceps strengthening: Straight leg lift
Lie flat on a firm surface, such as a floor. Bend your left leg to a 90 degree angle, with your foot flat on the floor. Raise your right leg several inches, and hold it up for 5 to 10 seconds. Then lower your leg to the floor slowly over a few seconds. Do the exercise 5 to 10 times and then switch legs.
Figure 10. Quadriceps strengthening – Straight leg lift

Hip adductor strengthening
While sitting, squeeze a rubber ball between your knees. Hold the squeeze for 5 to 10 seconds. Do the exercise 5 to 10 times. (If you don’t have a ball, put your hands or fists between your knees and then squeeze.)
Figure 11. Patellofemoral pain syndrome – Hip adductor strengthening

Hip abductor strengthening
For this exercise, use a wall or sturdy chair for balance. Stand on your left leg with the knee slightly bent. You can use you’re left hand to hold onto the wall or chair. Slowly raise your right foot about 30 degrees, hold for a few seconds, and then slowly lower the foot and straighten both legs. Do the exercise 10 times. Don’t let your pelvis tilt (be crooked), and don’t let your knees turn inward during bending. Remember to switch legs.
You can also tie a rubber band around a stable object. The foot of a bed or a table are good places. Place one foot inside the loop, then slowly lift your foot and leg out to the side, making sure to keep your toes pointed forward. Hold 2 seconds, then slowly return to the starting position. Repeat this exercise 10 times, then switch legs. To make this exercise more challenging, try it without holding onto anything to challenge your balance.
Figure 12. Patellofemoral pain syndrome – Hip abductor strengthening

Patellofemoral pain syndrome stretching
Iliotibial band and buttock stretch
Sit on the floor with your legs out straight. Cross your right foot over your left knee. Twist your trunk to the right and use your left arm to “push” your right leg. You should feel the stretch in your right buttock and the outer part of your right thigh. Hold the stretch for 10 to 20 seconds. Do the exercise 5 to 10 times then switch legs.
Iliotibial band stretch
Stand up straight, with your right leg crossed in front of your left leg. Hold your hands together and move them toward the floor. You should feel a stretch in the outer part of your left thigh. Hold the stretch for 10 to 20 seconds. Do the exercise 5 to 10 times and then switch legs.
Figure 13. Patellofemoral pain syndrome – Iliotibial band stretch
Hamstring stretch
Lie flat on the floor with your legs out straight. Bend your left knee toward your chest. Grip your thigh with your hands to keep the thigh steady. Straighten your left leg in the air until you feel a stretch. Hold the stretch for 5 to 10 seconds. Do the exercise 5 to 10 times then switch legs.
Figure 14. Patellofemoral pain syndrome – Hamstring stretch

Calf stretch
Stand facing a wall. Put both hands against the wall and move your right foot back until you can feel a stretch in your calf muscle. Keep your left leg bent, with your knee lined up over your toes. Keep your right heel on the ground to feel the back of the leg stretch. Hold for 10 to 20 seconds. Do the exercise 6 to 10 times and then switch legs.
Figure 15. Patellofemoral pain syndrome – Calf stretch

Patellofemoral pain syndrome surgery
Surgical consultation for patellofemoral pain syndrome may be considered for those patients whose symptoms persist despite their completing at least six to 12 months of a thorough program of rehabilitation, and in whom other causes of anterior knee pain have been excluded.
Surgical options include release of the lateral retinaculum, articular cartilage procedures, proximal realignment, and distal realignment—often with antero-medialization of the tibial tubercle 13. Patients with tight lateral structures may benefit from lateral release, with proximal realignment in some cases. Distal realignment with anteromedialization of the tibial tubercle may benefit those with lateral compression and associated articular cartilage injury.
Surgical treatments may include:
Arthroscopy
During arthroscopy, your surgeon inserts a small camera, called an arthroscope, into your knee joint. The camera displays pictures on a television screen, and your surgeon uses these images to guide miniature surgical instruments.
- Debridement. In some cases, removing damaged articular cartilage from the surface of the patella can provide pain relief.
- Lateral release. If the lateral retinaculum tendon is tight enough to pull the patella out of the trochlear groove, a lateral release procedure can loosen the tissue and correct the patellar malalignment.
Tibial Tubercle Transfer
In some cases, it may be necessary to realign the kneecap by moving the patellar tendon along with a portion of the tibial tubercle—the bony prominence on the tibia (shinbone).
A traditional open surgical incision is required for this procedure. The doctor partially or totally detaches the tibial tubercle so that the bone and the tendon can be moved toward the inner side of the knee. The piece of bone is then reattached to the tibia using screws. In most cases, this transfer allows for better tracking of the kneecap in the trochlear groove.
Most studies of surgical treatment for patellofemoral disorders are uncontrolled case series. Controlled studies of surgical outcomes are limited and are highly dependent on proper patient selection. Because it is essential that the surgical procedure specifically address the individual characteristics of patellar maltracking in each patient, consultation should be obtained from a surgeon with significant experience in treating patellofemoral joint disorders.
- Reid DC. The myth, mystic and frustration of anterior knee pain [Editorial]. Clin J Sport Med. 1993;3:139–43.[↩]
- Cutbill JW, Ladly KO, Bray RC, Thorne P, Verhoef M. Anterior knee pain: a review. Clin J Sport Med. 1997;7:40–5.[↩]
- Taunton JE, Ryan MB, Clement DB, McKenzie DC, Lloyd-Smith DR, Zumbo BD. A retrospective case-control analysis of 2002 running injuries. Br J Sports Med. 2002;36:95–101.[↩][↩]
- Beynnon BD, Johnson RJ, Coughlin KM. Relevant biomechanics of the knee. In: DeLee JC, Drez D, Miller MD, eds. Orthopaedic Sports Medicine: Principles and Practice. 2nd ed. Philadelphia, Pa.: Saunders, 2003:1590.[↩]
- Fu FH, Seel MJ, Berger RA. Patellofemoral biomechanics. In: Fox JM, Del Pizzo W, eds. The Patellofemoral Joint. New York, N.Y.: McGraw-Hill, 1993:49.[↩]
- Reilly DT, Martens M. Experimental analysis of the quadriceps muscle force and patellofemoral joint reaction force for various activities. Acta Orthop Scand. 1972;43:126–37.[↩]
- Karlsson J, Thomee R, Sward L. Eleven year follow-up of patellofemoral pain syndrome. Clin J Sport Med. 1996;6:22–6.[↩][↩][↩]
- Kannus P, Natri A, Paakkala T, Jarvinen M. An outcome study of chronic patellofemoral pain syndrome. Seven-year follow-up of patients in a randomized, controlled trial. J Bone Joint Surg Am. 1999;81:355–63.[↩][↩]
- Blond L, Hansen L. Patellofemoral pain syndrome in athletes: a 5.7-year retrospective follow-up study of 250 athletes. Acta Orthop Belg. 1998;64:393–400.[↩]
- Lun V, Meeuwisse WH, Stergiou P, Stefanyshyn D. Relation between running injury and static lower limb alignment in recreational runners. Br J Sports Med. 2004;38:576–80.[↩][↩][↩]
- Post WR. Clinical evaluation of patients with patellofemoral disorders. Arthroscopy. 1999;15:841–51.[↩]
- Walsh WM. Recurrent dislocation of the knee in the adult. In: DeLee JC, Drez D, Miller MD, eds. Orthopaedic Sports Medicine: Principles and Practice. 2nd ed. Philadelphia, Pa.: Saunders, 2003:1718–21.[↩]
- Fulkerson JP. Diagnosis and treatment of patients with patellofemoral pain. Am J Sports Med. 2002;30:447–56.[↩][↩][↩]
- Witvrouw E, Lysens R, Bellemans J, Cambier D, Vanderstraeten G. Intrinsic risk factors for the development of anterior knee pain in an athletic population. A two-year prospective study. Am J Sports Med. 2000;28:480–9.[↩]
- Elias DA, White LM. Imaging of patellofemoral disorders. Clin Radiol. 2004;59:543–57.[↩]
- Heintjes E, Berger MY, Bierma-Zeinstra SM, Bernsen RM, Verhaar JA, Koes BW. Pharmacotherapy for patellofemoral pain syndrome Cochrane Database Syst Rev. 2004;(3):CD003470.[↩]
- Witvrouw E, Danneels L, Van Tiggelen D, Willems TM, Cambier D. Open versus closed kinetic chain exercises in patellofemoral pain: a 5-year prospective randomized study. Am J Sports Med. 2004;32:1122–30.[↩]
- Clark DI, Downing N, Mitchell J, Coulson L, Syzpryt EP, Doherty M. Physiotherapy for anterior knee pain: a randomised controlled trial. Ann Rheum Dis. 2000;59:700–4.[↩]
- Kowall MG, Kolk G, Nuber GW, Cassisi JE, Stern SH. Patellar taping in the treatment of patellofemoral pain. A prospective randomized study. Am J Sports Med. 1996;24:61–6.[↩]
- Whittingham M, Palmer S, Macmillan F. Effects of taping on pain and function in patellofemoral pain syndrome: a randomized controlled trial. J Orthop Sports Phys Ther. 2004;34:504–10.[↩]
- Kannus P, Niittymaki S. Which factors predict outcome in the non-operative treatment of patellofemoral pain syndrome? A prospective follow-up study. Med Sci Sports Exerc. 1994;26:289–96.[↩]
- Crossley K, Bennell K, Green S, McConnell J. A systematic review of physical interventions for patellofemoral pain syndrome. Clin J Sport Med. 2001;11:103–10.[↩]
- Finestone A, Radin EL, Lev B, Shlamkovitch N, Wiener M, Milgrom C. Treatment of overuse patellofemoral pain. Prospective randomized controlled clinical trial in a military setting. Clin Orthop Relat Res. 1993;293:208–10.[↩]
- Miller MD, Hinkin DT, Wisnowski JW. The efficacy of orthotics for anterior knee pain in military trainees. A preliminary report. Am J Knee Surg. 1997;10:10–3.[↩]
- Lun VM, Wiley JP, Meeuwisse WH, Yanagawa TL. Effectiveness of patellar bracing for treatment of patellofemoral pain syndrome. Clin J Sport Med. 2005;15:235–40.[↩]





{kind=link}