
Contents
- What causes pimple like bumps on penis
- How are penis skin disorders diagnosed ?
- How are penis skin disorders treated ?
- Benign pimples on penis
- Non-sexually transmitted skin infections
- Sexually transmitted infections
- Non-infectious skin lesions and miscellaneous conditions that are commonly found in the genital area include:
What causes pimple like bumps on penis
Penis skin problems are very common and can be very itchy or painful, distressing and embarrassing. They can interfere with sexual functioning, self-image and interpersonal relationships. Some genital disorders are contagious, including sexually transmitted diseases, whilst others may be just a normal pimple, it can be an ingrown hair or probably skin cyst.
It is quite difficult to decide whether pimples on their penis is a normal one or demands immediate medical assistance because studies have reported that spots on penis can also be an indication of cancer. Despite these challenges, primary care physicians are capable of diagnosing and managing many penile lesions, and determining which patients require subspecialist referral. Because many penile cutaneous lesions are diagnosed on physical examination, the key to narrowing a differential diagnosis is defining the predominant characteristic of the lesions (see Table 1).
Most papules (bumps) are benign, whereas ulcers or irregularly shaped masses may suggest malignancy. However, there are exceptions to both rules. Lesions localized to the penis usually involve different diagnostic and treatment considerations than lesions with extended or systemic findings. Biopsy is usually reserved for an unclear diagnosis, or if neoplasm is a consideration. Management options for noninfectious lesions are summarized in Table 2.
How are penis skin disorders diagnosed ?
Careful history and full skin examination, including of genital skin, are recommended. Tests often include:
- Swabs from the affected skin, urethral or vagina for bacteria, yeast and virus culture
- Blood tests
- Skin biopsy
How are penis skin disorders treated ?
Treatment depends on the individual condition.
Genital skin is delicate, so treatment must be undertaken gently. Wash once or twice daily with warm water. Avoid soap; a pH balanced non-soap cleanser can be used but should be rinsed off.
Table 1. Causes of pimple like bumps on penis skin
| Lesion | Characteristic symptoms | Typical clinical appearance | Differential diagnosis |
|---|---|---|---|
| Inflammatory and papulosquamous lesions | |||
| Angiokeratomas | Asymptomatic | Red or blue papules; may appear only on the glans penis or also on the scrotum, groin, thighs, and abdominal wall | Pearly papules |
| Lichen nitidus | Asymptomatic | Pinhead-sized, hypopigmented papules; often extragenital | Herpes simplex virus, pearly papules |
| Lichen planus | Pruritus, soreness | Flat-topped, polygonal, violaceous papules; often extragenital | Secondary syphilis |
| Lichen sclerosus | Phimosis, painful erections, obstructive voiding, itching, pain, bleeding | Hypopigmented, thinned, phimotic prepuce; texture similar to cellophane; isolated to prepuce and glans penis | Carcinoma in situ, leukoplakia, scleroderma |
| Psoriasis | Pruritus | Red or salmon-colored, papulosquamous, circinate plaques that are often associated with white or silvery scales; usually systemic | Carcinoma in situ |
| Infectious lesions | |||
| Genital herpes | Primary disease: constitutional symptoms followed by genital vesicles Recurrent disease: prodromal local paresthesias, pruritus, burning sensation, hypersensitivity | Vesicles on an erythematous base that become a pustule before crusting over; heals without scarring; isolated to dermatome | Lichen nitidus |
| Human papillomavirus lesions (HPV) | Asymptomatic | Exophytic, flesh-colored, warts; lobulated or irregular surface; may appear on perineum and perianal area; diagnosis confirmed by culture, DNA detection with polymerase chain reaction, or biopsy | Squamous cell carcinoma |
| Primary syphilis lesions | Painless | Ulcer (chancre); isolated; darkfield microscopy is needed for diagnosis | Zoon balanitis |
| Scabies | Pruritus that is worse at night; family members or other close contacts are affected | Genital burrows; may become superinfected and crusted; may appear on fingers Detection of mite, egg, or pellet confirms diagnosis | Psoriasis |
| Cancer lesions | |||
| Carcinoma in situ (erythroplasia of Queyrat, Bowen disease) | Pruritus, pain | Variable appearance; plaque or ulcer isolated to glans penis, prepuce, and other areas of the penis; biopsy needed for diagnosis | Psoriasis, lichen sclerosus, Zoon balanitis, invasive penile cancer, lichen planus, herpes simplex virus, syphilis, group B streptococcal balanitis, candidiasis, Reiter syndrome |
| Invasive squamous cell carcinoma | Delayed presentation, usually painless | Exophytic or endophytic appearance; presentation varies; local or metastatic; biopsy is needed for diagnosis | Giant condyloma (human papillomavirus) |
Table 2. Management Options for Noninfectious Penile Lesions
| Diagnosis | Primary management option | Alternate option |
|---|---|---|
| Inflammatory and papulosquamous lesions | ||
| Angiokeratoma | Observation | Surgery, cryoablation, electrocautery, laser ablation |
| Lichen nitidus | Observation | Topical corticosteroids, vitamin A analogues, cyclosporine (Sandimmune), itraconazole (Sporanox), phototherapy |
| Lichen planus | Topical corticosteroids | Circumcision for isolated prepuce lichen planus |
| Lichen sclerosus | Topical corticosteroids | Circumcision for isolated prepuce lichen sclerosus |
| Psoriasis | Topical corticosteroids | Vitamin D3 analogues, tacrolimus (Protopic), or pimecrolimus (Elidel) |
| Cancer lesions | ||
| Carcinoma in situ | Circumcision for isolated prepuce lesions | Mohs micrographic surgery Topical imiquimod (Aldara) |
| Invasive squamous | Circumcision for isolated prepuce lesions Mohs micrographic surgery for nonisolated lesions | Partial or radical penectomy Laser therapy, radiation, and brachytherapy have been attempted as alternatives |
Genital itch in males
- Pruritus ani (itchy anus)
- Balanitis (inflammation of the glans penis in males)
- Dermatitis (eczema), including:
- Lichen simplex (dermatitis due to localised itch-scratch-itch response and resulting in thickened skin on scrotum)
- Atopic dermatitis (eczema)
- Seborrhoeic dermatitis (usually affects scalp as well)
- Irritant contact dermatitis (from wetness, incontinence, vigorous cleansing) the most common cause of nonspecific balanitis (in males)
- Intertrigo (in skin folds)
- Allergic contact dermatitis (most often due to fragrances, preservatives or rubber)
Genital pain in males
- Balanitis (inflammation of the tip of the penis)
- Behcet disease
- Erosive lichen planus (which often also affects the mouth)
- Plasma cell balanitis
- Fixed drug eruption
- Crohn disease, which may cause swelling, ulcers and granulomas
- Pudendal nerve entrapment syndrome
- Dysaesthesia and/or burning discomfort (and less often, itching) of the penis (penodynia) and/or scrotum (scrotodynia) in the absence of a primary skin problem. The affected area is often redder than normal.
Benign pimples on penis
Pearly penile papules
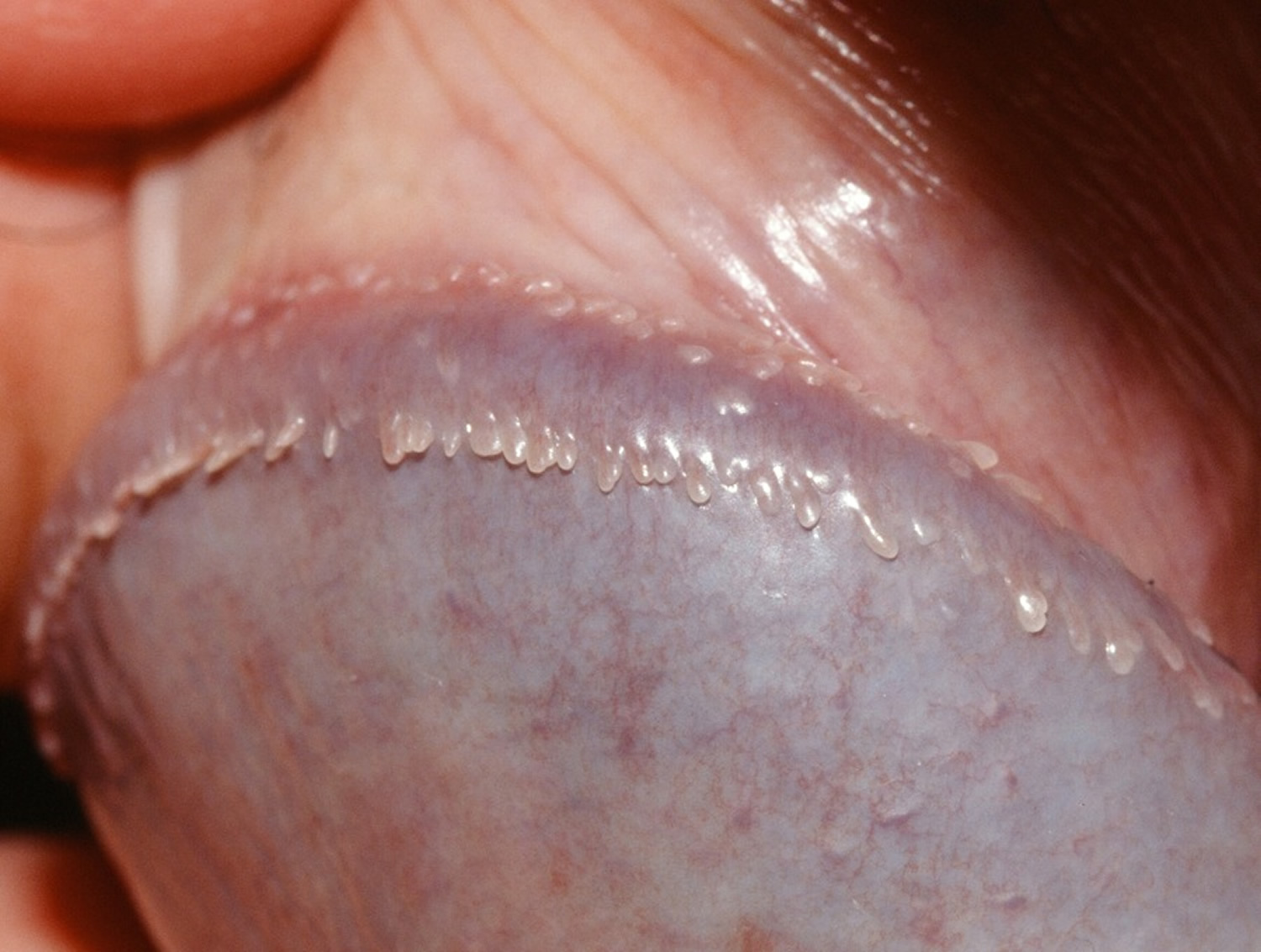
Pearly penile papules are small dome-shaped to thread-like skin-coloured bumps that are typically located on the sulcus or corona of the glans penis. The papules are commonly arranged all the way around the head of the penis in one or several rows.
Penile papules have been reported to be present in between 8% and 43% of men. They are more common in men that have not been circumcised. They become less apparent with increased age.
Figure 1. Pearly penile papules

What are the symptoms of pearly penile papules ?
The pearly penile papules do not cause any symptoms but patients are often anxious as to their nature.
What is the cause of pearly penile papules ?
Penile papules are a normal anatomic variant. They are not due to sexual activity or lack of hygiene. They are not infectious or contagious, unlike genital warts. They are not malignant or pre-malignant.
- Pearly penile papules are most commonly found in men between 20 and 40 years of age.
- Pearly penile papules seem to regress with age.
- Some consider these lesions as vestigial remnants of penile spines, which are found in the same location in other primates and contributes to sexual pleasure and quicker orgasms.
- Vestibular papillomatosis is considered to be female equivalent of pearly penile papules.
Investigations pearly penile papules
The lesions are usually diagnosed by their clinical appearance so no specific tests are required. They can usually be readily distinguished from other lesions found on the penis, including viral warts, molluscum contagiosum and ectopic sebaceous glands (Fordyce spots).
Pearly penile papule show a typical appearance under the dermatoscope.
Skin biopsy or pearly penile papules has characteristic microsopic features. There is a variable number of thin-walled dilated blood vessels in the dermis with a proliferation of fibroblast cells which may be star-shaped or have multiple nuclei. Concentric fibrosis may also be found around skin appendage structures.
Management of pearly penile papules
Patients should be reassured as to the nature of the lesions. Treatment is not necessary. If treatment is desired, carbon dioxide laser vaporisation or electrosurgery may destroy the lesions but they may be replaced by scarring 2. Cryotherapy and excision have been used as well.
Fordyce Spots
Fordyce spots are are normal small (1–5mm) superficial sebaceous (oil-producing) glands, slightly elevated yellowish or white papules or spots that can appear on the glans or shaft of the penis, or the vulva of the female, the inside of the cheeks and on the vermilion border of the lips. They are also called Fordyce granules.
Fordyce spots are normally seen on the moist tissue that lines some organs and body cavities (mucosal surfaces). The “spots” are asymptomatic and can be found on the head of the penis, the inner foreskin, and, most commonly, at the border of the lips. These sebaceous glands are not associated with hair follicles. These lesions are asymptomatic, but itching or irritation may occur if people treat the bumps inappropriately.
Fordyce spots are a variant of sebaceous glands (the glands that normally produce sebum and are usually found within hair follicles). Fordyce spots are visible sebaceous glands without hair follicles. They are present in 80–95% of adults. They are probably present at birth but become bigger and more visible from about puberty onwards. They may occur as a solitary lesion or more frequently in crops of about 50–100. They are easier to see when the skin is stretched.
The most common location for Fordyce spots is at the border of the lips, especially near the corners of the mouth. Other locations include the back portions of the inner cheeks and inside the mouth, including the tonsils. The head of the penis and inner portion of the foreskin may be affected as well.
Fordyce spots can appear at any point in life, but the incidence of appearance increases with age, with the largest prevalence in elderly patients.
Sometimes Fordyce spots cause anxiety but they are completely harmless whether on the lips or on the genitals. They are not a sexually transmitted disease and they are not infectious.
Figure 2. Fordyce spots penis


What work-up is required for Fordyce spots ?
Fordyce spots are normal and non-cancerous (benign), but seek medical evaluation if Fordyce spots become itchy or irritated.
The importance of recognising these papules as Fordyce spots is in the differential diagnosis of other conditions that may appear similar. Some sexually transmitted diseases (STDs) may start off looking like Fordyce spots on the genitals so it is essential to get a proper diagnosis from your doctor. STDs need to be treated appropriately with medication.
What is the treatment for Fordyce spots ?
Fordyce spots are generally harmless and do not require any treatment. Avoid picking or squeezing the spots.
The patient should be reassured that the lesions are neither dangerous, nor contagious. They are totally benign.
Fordyce spots can be a cause of cosmetic concern for some patients. Electrosurgery and vaporising laser treatment (CO2 laser) have been used successfully to remove the spots. Other reported treatments for Fordyce spots include bichloracetic acid, photodynamic therapy, micro-punch excision surgery and oral isotretinoin. The lesions disappear during isotretinoin therapy, but then recur after stopping. Topical 100% dichloroacetic acid has been used 3.
Non-sexually transmitted skin infections
Non-venereal skin infections may present in the genital area, presumably because the organisms thrive in warmth and humidity.
Bacterial infection
Bacterial skin infections include:
- Boils (deep infection of hair follicle)
- Folliculitis (surface infection of hair follicle)
- Impetigo (school sores)
- Erythrasma (dry brown patches)
- Cutaneous tuberculosis (rare)
- Bacterial vaginosis (cause of frothy discharge)
What is folliculitis ?
Folliculitis is inflammation of the hair follicle due to infection, chemical irritation or physical injury. Bacterial folliculitis is the most common form of folliculitis.
What causes bacterial folliculitis ?
Bacterial folliculitis is usually due to Staphylocoocus aureus. Less often, coagulase-negative staphylococci and gram-negative organisms are responsible including anaerobes. Spa pool folliculitis is caused by pseudomonas.
Figure 3. Folliculitis

Who gets bacterial folliculitis ?
Bacterial folliculitis affects children and adults, with adolescents and young adult males most often infected. It is prevalent worldwide.
The following factors predispose to bacterial folliculitis:
- Maceration and occlusion (clothing, dressings, ointments)
- Frequent shaving, waxing or other forms of d/epilation
- Friction from tight clothing
- Atopic dermatitis
- Acne or other follicular skin disorder
- Use of topical corticosteroids
- Previous long-term use of antibiotics
- Anaemia, obesity, diabetes, HIV/AIDS, hepatitis, cancer and other chronic illness
- Bathing in an inadequately cleansed hot tub or pool
What are the clinical features of bacterial folliculitis ?
Bacterial folliculitis may be superficial or involve the whole hair follicle (a boil). It may arise on any body site, but is most often diagnosed in scalp, beard area, axilla, buttocks and extremities. Systemic symptoms are uncommon. Different types of bacterial folliculitis are described below.
Superficial folliculitis
Superficial staphylococcal folliculitis presents with one or more follicular pustules. They may be itchy or mildly sore. Superficial folliculitis heals without scarring.
A hordeolum or stye is bacterial folliculitis affecting an eyelash.
Furunculosis / boils
Furunculosis or boils presents as one or more painful, hot, firm or fluctuant, red nodules or walled-off abscesses (collections of pus). A carbuncle is the name used when a focus of infection involves several follicles and has multiple draining sinuses. Recovery leaves a scar.
Gram-negative folliculitis
Gram negative folliculitis develops in individuals using long term antibiotics for acne. The infection with gram negative organisms causes pustules in acne sites of the face, neck and upper trunk.
Hot tub folliculitis
Hot tub or spa pool folliculitis presents with painful papules and pustules on the trunk some hours after soaking in hot water, mainly in sites that were covered by bathing costume. It may be accompanied by mild systemic symptoms including fever. Untreated, it settles within about 10 days without scarring.
Complications of bacterial folliculitis
Soft tissue infection
Bacterial folliculitis can lead to cellulitis and lymphangiitis; subsequent bacteraemia might result in osteomyelitis, septic arthritis or pneumonia.
How is bacterial folliculitis diagnosed ?
Bacterial folliculitis is usually diagnosed clinically but can be confirmed by bacterial swabs sent for microscopy, culture and sensitivity.
Blood count may reveal neutrophil leucocytosis when folliculitis is widespread.
Skin biopsy is rarely necessary. Histology shows dense neutrophilic infiltrate in subcutaneous tissue and foreign body reaction around a hair shaft.
How can folliculitis be prevented ?
- Keep skin clean and if dry, well moisturised.
- Minimise shaving and waxing. When shaving, use new blade each time and moisturise the skin afterwards.
- Do not wear tight fitting clothes.
- Ensure adequate sterilisation of hot tubs.
- In case of repeated episodes of staphylococcal folliculitis, apply mupirocin ointment to the nostrils to eliminate S aureus carrier state.
What is the treatment for bacterial folliculitis ?
- Warm compresses to relieve itch and pain
- Analgesics and anti-inflammatories to relieve pain.
- Antiseptic cleansers (eg hydrogen peroxide, chlorhexidine, triclosan)
- Incision and drainage of fluctuant lesions and abscesses
- Topical antibiotics such as erythromycin, clindamycin, mupirocin and fusidic acid. To reduce bacterial resistance, these should be applied for courses of no more than one week
- Oral or intravenous antibiotics for more extensive or severe infections
- Photodynamic therapy
- Repeated laser hair removal
Fungal infections
Fungal skin infections include:
- Tinea cruris (Jock itch)
- Vulvovaginal candidiasis (thrush)
Viral infections
Viral skin infections include:
- Genital herpes, the commonest cause of recurrent blisters or sores
- Genital warts, the commonest cause of papules in this region
- Herpes zoster (shingles)
- Molluscum contagiosum
Infestations
The groin is also a favored site for some parasitic infestations:
- Pubic lice
- Scabies
- Schistosomiasis
- Amoebiasis
- Filariasis
- Leishmaniasis
Sexually transmitted infections
Important sexually transmitted infections (STIs) include:
- Syphilis
- Gonorrhoea
- Lymphogranuloma venereum
- Chancroid
- Granuloma inguinale (donovanosis)
- Trichomoniasis
- Genital herpes.
Sexually transmitted diseases (STDs) or sexually transmitted infections (STIs) are infections that are passed from person to person by sexual activity. Although sexually transmitted infections (STIs) are most often spread through vaginal, anal, or oral intercourse, skin-to-skin contact is enough to transmit many STDs.
Sexually transmitted infections (STIs) affect an enormous number of people throughout the world, regardless of age, sex, socioeconomic status, or ethnicity. Approximately 19 million new infections occur each year in the United States, and about half of these infections are in people aged 15-24. Roughly 50% of people in the United States will have at least one STD during their life.
People at higher risk for STDs are those who do not use condoms, have more than one partner, or have sex with people who have multiple partners, use intravenous drugs, and/or share needles. You can decrease your risk for getting an STD by using condoms every time you have sex (even during oral sex), limiting your number of sexual partners, or abstaining from sexual activity. If you think that you or your partner may have an STD, see your doctor as soon as possible. Early treatment can decrease your chance of spreading the infection and can prevent possible complications.
There are many types of STDs, and all have slightly different symptoms. STDs that cause prominent skin changes are discussed here. For example:
- Genital warts, caused by the human papillomavirus (HPV), and molluscum contagiosum appear as small, painless bumps or growths.
- Genital herpes (herpes simplex virus), primary syphilis, chancroid, and lymphogranuloma venereum (LGV) cause open sores, blisters, or ulcerations in the genital region.
- Pubic lice and scabies mites can cause itchy, red bumps in the genital region.
- Gonorrhea can cause a discharge from the vagina, penis, or rectum.
Important infections that are not discussed here include chlamydia, HIV, hepatitis, syphilis, and certain forms of gonorrhea.
Anogenital wart
Genital warts (condyloma acuminata) are caused by the human papillomavirus (HPV), which has over 200 different strains. Subtypes number 6 and 11 cause 90% of genital warts and are considered low risk because they very rarely will cause genital or anal cancer. On the other hand, subtypes 16 and 18, for example, are considered high risk because, although they rarely cause genital warts, they can lead to cervical or anal precancer and cancer.
HPV is spread by skin-to-skin contact during sexual activity; there does not need to be vaginal or anal intercourse to spread the infection. Most people who become infected with HPV will not have symptoms and will clear the infection on their own. For people who do develop genital warts, there are many options for treatment, all of which are meant to remove the visible warts. There is no cure for genital warts.
In 2006, the FDA approved the first HPV vaccine (Gardasil®) that protects against the 4 strains of HPV that cause 70% of cervical cancers and 90% of genital warts. It protects against the high-risk strains, 16 and 18, that can cause cervical cancer and the low-risk strains, 6 and 11, that cause most genital warts. The HPV vaccine is a series of 3 shots over a 6-month period. In the US, Gardasil is approved for girls/women and boys/men ages 9–26.
Who’s at risk of genital wart?
Genital warts are the most common sexually transmitted disease and affect millions of people throughout the world. It is estimated that 75–80% of sexually active men and women will be infected with HPV at some point in their lives. Approximately 15% of the United States population is infected with HPV. HPV infection occurs in people of all ages and both sexes. Your risk of acquiring the virus is higher if you have had many sexual partners and if you first had sexual intercourse at a young age. Over 50% of girls will get HPV within 2 years of becoming sexually active.
HPV is spread through skin-to-skin contact and does not require actual intercourse to be passed from one person to another. A person can be infected without any visible signs of infection and, therefore, can pass the infection on without knowing it. Condoms can decrease the risk of spreading the virus, but they do not completely prevent transmission.
You can decrease your risk of getting genital warts by using condoms, having few sexual partners, or by abstaining from sexual activity. Unfortunately, condoms do not completely protect against HPV, and an infected person can spread the virus even if he/she does not have any visible warts.
Genital wart treatment
If you have visible warts, see your doctor for treatment to remove the warts and to reduce the chance of passing the virus to other partners. Also, if your partner has been diagnosed with genital warts, you should be checked for infection.
For women, it is important to have a Pap smear and general gynecologic examination, usually every year, to look for any signs of abnormal cervical cells, which can be the first sign of cervical cancer.
There is no cure for genital warts. The goal of treatment is to remove visible warts and decrease the risk of spreading the virus. There are many different treatments that your doctor may recommend, none of which are 100% effective. Most treatment types will get rid of the warts in 60–90% of cases, however.
Some treatments are applied by the patient. These include the following:
- Imiquimod 3.75% cream (Zyclara®) – Imiquimod works by boosting your immune system to kill the virus. Apply once daily for up to 8 weeks. This medication may weaken condoms, and you should avoid sexual activity while the cream is on your skin. Do not use imiquimod during pregnancy.
- Imiquimod 5% cream (Aldara®) – Apply once daily (at bedtime) 3 times a week for up to 16 weeks.
- Podofilox 0.5% gel or solution (Condylox®) – This should not be used during pregnancy.
Treatments applied by a physician:
- Podophyllin resin, 15–25% solution – This should not be used during pregnancy.
- Trichloroacetic acid
- Cryotherapy – Liquid nitrogen is used to freeze the warts.
- Surgical removal – This may need to be performed by a specialist with local anesthesia; usually for large amounts of warts.
- Laser treatment – Carbon dioxide laser treatment is useful for a large amount of urethral or vaginal warts.
Most of these treatments require multiple applications. If there is no improvement after 3 treatment cycles or if the warts are not gone after 6 treatment cycles, your doctor will usually switch you to a different medication. Common side effects of all treatments include skin irritation and redness. Some people may also develop scars at the site of the warts.
Cryotherapy
Cryotherapy every 1-3 weeks is perhaps the most common treatment. Waiting longer between treatments allows the lesions to grow back. In one study, freezing every 7-8 days cleared the lesions in fewer sessions than freezing every 14-21 days 4. Cryotherapy for warts may be done as follows: Freeze until white with 1 mm margin. Let thaw, repeat.
Cautery/Curettage
Local anesthesia followed by light cautery, curettage, or both is often more effective than freezing. There is a higher risk of scarring however. Patients are often seen monthly until the area stays clear.
Candida Injection
Several condyloma may be injected every 3-4 weeks for 3-5 treatments.
Podofilox
Podofilox is applied to each wart twice daily for three consecutive days a week. Significant inflammation should be expected.
Imiquimod
For external genital/perianal warts, imiquimod 5% cream (Aldara) is to be applied three days a week (e.g., Monday, Wednesday, and Friday) for up to 16 weeks. Patients should be warned about the potential for significant inflammation and rarely the development of permanent white spots.
Trichloroacetic acid (TCA) or bichloroacetic acid (BCA)
Trichloroacetic acid (TCA) or bichloroacetic acid (BCA) may be applied in the office with repeat treatments every 2-3 weeks until clearing is achieved.
5% KOH
The application of 5% KOH (Potassium hydroxide) daily for 12 weeks resulted in 70% of patients clear or almost clear 5.
Ingenol Mebutate
Ingenol mebutate appears highly effective in the treatment of anogenital warts with just one application. In one report of 10 patients using either 0.015% or 0.05% ingenol mebutate or placebo, all warts cleared within 3-7 days. No sites treated with vehicle cleared. There were no recurrences in three months at sites which cleared. There was mild to moderate burning x 1-2 days. 6. In a similar study [JEADV 2016;30;1041], a single application of either 0.015% or 0.05% gel cleared 13/17 patients with anogenital warts. Up to three applications cleared 16/17.
Smoking and Condyloma
Every smokers have significant increased risk of external genital warts compared to non-smokers even when corrected for sexual behavior (age at onset of sex, number of partners, use of condoms). The study found 0.6% increased risk per each extra cigarette/day 7.
Condyloma of the Urethral Meatus
Condyloma of the urethral meatus may be treated with any of the destructive methods above. In addition, 5% fluorouracil (5-FU) may be applied after voiding twice to three times daily for 2-3 weeks. The urethra may be dried with one end of a cotton-tipped applicator and then the 5-FU applied with the other end. The opening is then pressed closed and the excess wiped off. Painful urination and discharge may occur with this therapy.
Figure 4. Penis genital wart – Condyloma acuminata


Genital herpes
Herpes simplex is one of the commonest infections of mankind throughout the world. There are two main types of herpes simplex virus (HSV): herpes simplex virus type 1 (HSV-1), which is mainly associated with facial infections and herpes simplex virus type 2 (HSV-2), which is mainly genital, although there is considerable overlap. Herpes lesions on the face, sometimes referred to as cold sores, are primarily due to HSV-1. HSV infections are contagious and are spread to other people by skin-to-skin contact with the infected area.
Both types of HSV produce 2 kinds of infections: primary and recurrent. Both type 1 and type 2 herpes simplex viruses reside in a latent state in the nerves that supply sensation to the skin. With each episode of herpes simplex, the virus grows down the nerves and out into the skin or mucous membranes where it multiplies, causing the clinical lesion. After each episode it “dies back” up the nerve fiber and enters the resting state again.
Herpes simplex virus (HSV) causes lifelong infection with potential for reactivation or recurrence. Often people refer only to HSV-2 when discussing genital herpes but both types can cause infection in the genital area. Clinically, about 60–70% of primary genital infections are due to HSV-2 with the rest due to HSV-1.
Because herpes simplex virus (HSV) is so contagious, HSV causes a primary infection in most people who are exposed to the virus. However, only about 20% of people who are infected with HSV actually develop visible blisters or sores. Appearing 5–6 days after a person’s first exposure to HSV, the sores of a primary infection last about 2–6 weeks. These sores heal completely, rarely leaving a scar. Nevertheless, the virus remains in the body, hibernating in nerve cells.
Certain triggers can cause the hibernating virus to wake up, become active, and travel back to the skin, causing a recurrent infection. These outbreaks tend to be milder than primary infections and generally occur in the same location as the primary infection. The frequency of recurrence is unpredictable and tends to become less over time.
Figure 5. Penis herpes


How common is genital herpes ?
Studies have found that up to 1 in 5 adults have evidence of HSV-2 infection. Most of these people have either no or only very mild symptoms, such that they are unaware of having been infected.
Who’s at risk of genital herpes?
Genital herpes can affect anyone who is sexually active. In fact, approximately 10–60% of the general population is infected with genital herpes.
Herpes is spread from person to person by direct skin-to-skin contact. The virus is most contagious when there are visible sores in the genital region. HSV can also be spread when there are no sores present, however, which is called asymptomatic shedding. Remember that only 20% of people who are infected with HSV actually develop visible blisters or sores, which means that approximately 80% of people with HSV have not been diagnosed and are unaware of their condition. Therefore, they can unknowingly transmit the infection to their sexual partners.
Transmission of genital herpes
Direct skin-to-skin contact spreads HSV infection most easily. Thus, sexual contact, including oro-genital contact, is the most common way to transmit genital HSV infection. The virus can be shed in saliva and genital secretions from individuals, even if they have no symptoms, especially in the days and weeks following a clinical episode. The amount shed during active lesions is 100 to 1000 times greater. Minor injury helps spread the virus, especially into the skin. Vertical (mother to baby) transmission or auto (self) inoculation may also occur. Because HSV dies quickly with drying at room temperature, spread from objects like bath towels (fomites) is unusual.
Primary genital herpes infection
A few days after exposure to HSV, a newly infected person typically develops a group of painful blisters or pus-filled bumps in the genital region. Because these fluid-filled lesions easily burst, many people never even notice them but instead see small, painful red sores or ulcers. These lesions usually last for 2–6 weeks for a primary infection and 5–10 days for recurrent infections. Eventually, a scab develops over each sore, which then falls off, leaving a red area that fades with time.
Primary or first genital HVS infections may be mild and unnoticed, but should lesions develop, the severity is generally greater than in recurrences.
Penile ulceration from herpetic infection is the most frequent cause of genital ulceration seen in sexual health clinics. The ulcers are most frequent on the glans, foreskin and shaft of the penis. They are sore or painful and last for 2 to 3 weeks, if untreated. The local lymph glands are enlarged and tender.
In women, similar lesions occur on the external genitalia and the mucosae of the vulva, vagina and cervix. Pain and difficulty passing urine are common.
Some people also have flu-like symptoms with fever, headache, fatigue and muscular aches and pains. Symptoms tend to be more severe in women than in men.
Following the initial infection immunity develops but does not fully protect against further episodes (recurrence). Where immunity is deficient, e.g in those living with HIV/AIDS, both initial and recurrent infections tend to occur more frequently and to be more pronounced.
Recurrent genital herpes infection
After the initial infection, obvious or inapparent, there may be no further clinical manifestations throughout life. Recurrences are more frequent with type 2 genital herpes than with type 1.
Recurrent HSV infections are usually milder than the primary infection, though the lesions look similar. Many people with recurrent HSV infections have burning, tingling, or pain in the area of the outbreak up to 24 hours before any visible signs. This is called the prodromal phase of the infection. Because many people never develop the symptoms of a primary HSV infection, they may mistake a recurrent infection for a primary infection.
Most people will have a recurrence of genital herpes during the first year after a primary infection. On average, most people will get about 4 outbreaks per year, although the frequency of recurrence is extremely variable and tends to decrease over the years.
Recurrences can be triggered by:
- Minor trauma, such as those caused by dental work or cuts from shaving
- Other infections.
- Fever or illness.
- Ultraviolet radiation (sun exposure).
- Menstrual cycle (flare-ups may occur before the monthly period).
- Emotional stress.
- Surgery.
- Friction to the area – for example, with sexual intercourse or tight-fitting clothes.
- Immunosuppression.
In most cases, however, no reason for the recurrence is evident.
Recurrent infections differ from first infections in that the blisters are usually smaller in size and more closely grouped. They also tend to be of shorter duration than the initial infection, usually 5–10 days. Generally the affected person feels quite well.
Itching or burning can precede by an hour or two the development of small, closely grouped blisters on a red base. These then produce shallow ulcers, on the glans or shaft of the penis in men and on the labia, vagina or cervix in women. Recurrences can cause distressingly painful symptoms or the lesions can be unnoticed. Lesions normally heal in 7–10 days without scarring. Recurrences tend to be in the same region, but not always at the identical site.
Complications of genital herpes
Complications may include:
- Urethritis (inflammation of the urethra, the urinary outflow tract). This results in ulceration. There may be no tell-tale blisters so that the presentation is identical to gonorrhoea or chlamydia urethritis.
- Proctitis (rectal infection). This can occur without external lesions. Symptoms include fever, rectal pain, watery discharge, and autonomic nerve dysfunction that may result in difficulty passing urine.
- Neurogenic (nerve) pain -leg and thigh pain. This often leads up to a recurrence.
- Meningitis. This is rare.
- Widespread infection. This is seen in debilitated or immune suppressed patients.
Asymptomatic shedding of herpes virus
Intermittent shedding of HSV from genital skin may occur without symptoms or with unrecognised minor symptoms. The frequency of asymptomatic shedding is more common in those with type 2 genital herpes and in those who have been infected recently. Shedding is most likely to occur in the week before or after a recurrence.
The amount shed from active lesions (ie, when a person has symptoms) is much greater than between episodes. This is when the infection is most likely to be passed on and sexual contact should therefore be avoided. One study of couples who avoided sexual contact during recurrences found that, over 12 months, only 1 out of 10 passed the virus on to their partner. In that study, condoms were not used. Using condoms may reduce the risk of infection even further.
Genital herpes treatments
Untreated HSV infections will go away on their own, but antiviral medications can reduce symptoms, shorten the duration of outbreaks, and decrease the chance of spreading the virus. These medicines are most effective if taken during the first 24 hours of symptoms. If you experience burning and tingling before the appearance of blisters, you can start the medicine as soon as you feel these symptoms. Unfortunately, these medicines do not cure HSV infections.
If you have herpes simplex, ask your doctor’s advice. Antiviral drugs are indicated for primary herpes simplex infection, as symptoms may last for 3 weeks if no treatment is given. Patients with significant recurrences may require repeated courses or continuous prophylactic therapy for 2 months or more. Mild uncomplicated recurrences of herpes simplex usually require no treatment.
Available antiviral drugs include:
- Aciclovir (Zovirax®)
- Valaciclovir (Valtrex®)
- Famciclovir (Famvir®)
Each of these medications is equally effective and usually taken for 7–10 days for primary infections and 1–5 days (depending on dose) for recurrent infections. Talk to your doctor about getting a prescription for these medicines for possible future outbreaks, as they are most effective if taken early on.
Initial Infection
- Acyclovir 200 mg 5/day x 5 days–longer if severe infection.
- Valaciclovir 1 gram twice daily for 10 days.
These antiviral drugs will stop the herpes simplex virus multiplying once it reaches the skin or mucous membranes but cannot eradicate the virus from its resting stage within the nerve cells. They can therefore shorten and prevent episodes while the drug is being taken, but a single course cannot prevent future episodes.
Different formulations of topical antiviral creams are available.
More severe HSV infections may require additional medications such as:
- Oral antibiotics if the area is also infected with bacteria
- Oral antifungals if the area is also infected with yeast
- Topical anesthetic cream, such as lidocaine ointment, to reduce pain
If you have frequent or severe herpes outbreaks, your doctor may recommend taking an antiviral medication every day to decrease the frequency and severity of attacks. This type of therapy may also be effective in decreasing the chance that an uninfected partner will acquire the virus. If you are taking a daily antiviral medicine to suppress your outbreaks, talk to your doctor about stopping these medicines yearly to see if you still need daily treatment.
Recurrent Infection
- Acyclovir 200 mg 5/day x 5 days.
- Famciclovir 1000 mg twice daily x 1 day.
- Valaciclovir 500 mg twice daily for 3 days.
Topical Zinc
- Applying zinc topically to genital area decreases recurrences of genital herpes
Topical ZnSO4 has been found to be an effective therapeutic modality not only for treatment but also for prolonging remissions in herpes genitalis. Topical 4% ZnSO4 dissolved in distilled water has been found to be most efficacious out of the three concentrations, without any side effects. The protocol was to apply topical ZnSO4 on the first visit, then after every 5 days for 1 month, followed by every 10 days for 2 months and then after every 15 days for 3 months for the total period of 6 months 8.
Suppressive Therapy
- Acyclovir 200 mg twice, three times or four times daily or 400 mg twice daily
- Famciclovir 250 twice daily
- Valaciclovir 1 gram once daily if recurrences > 9/year.
- Valaciclovir 500 mg once daily if recurrences < 10/year.
- Valaciclovir 500 mg twice daily if HIV positive.
Other treatments being studied include:
- Imiquimod cream, an immune enhancer
- Human leukocyte interferon alpha cream.
Both appear less beneficial than conventional antiviral drugs.
Herpes vaccine development
Vaccine development is an area of active research, and several different approaches are being tested in animal models, including “therapeutic” vaccines that might help those already infected. In May 2015, a promising vaccine design was announced 9.
Non-infectious skin lesions and miscellaneous conditions that are commonly found in the genital area include:
- Psoriasis
- Angiokeratomas (red/purple spots)
- Hidradenitis suppurativa (boil-like lumps in skin folds)
- Hailey Hailey (blisters in skin folds)
- Sebaceous adenitis (inflamed papules)
- Milia, pilar and epidermal cysts
- Penile intraepithelial neoplasia or PIN (also called penile squamous cell carcinoma in situ, Bowen disease of penis, erythroplasia of Quyerat)
- Anal intraepithelial neoplasia or AIN (also called anal squamous cell carcinoma in situ)
- Invasive squamous cell carcinoma including penile cancer and anal cancer (arising from genital warts). Penis cancer can also arise from lichen sclerosus or lichen planus)
- Extramammary Paget disease
- Genital melanotic macules or melanosis (harmless brown marks in which there is more pigment in the skin cells)
- Mucosal melanoma (a rare form of skin cancer in which there is uncontrolled proliferation of pigment cells)
- Pearly penile papules
- Peyronie disease, in which a fibrous band appears on the penis.
Penile intraepithelial neoplasia
Penile intraepithelial neoplasia is a rare pre-cancerous disease of the outer skin layer (epidermis) of the penis.
The risk of progression to squamous cell carcinoma (SCC) in untreated cases is estimated to be between 10 and 30%.
Other names for penile intraepithelial neoplasia include:
- Squamous intraepithelial lesion
- Erythroplasia of Queyrat
- Bowen disease of the penis
- In-situ squamous cell carcinoma of the penis
- P.I.N. (Penile intraepithelial neoplasia)
Bowen disease typically presents as a well-demarcated, scaly plaque on keratinized penile skin. Erythroplasia of Queyrat is characterized by moist, red plaques located on the mucosal surfaces of the glans and prepuce. Finally bowenoid papulosis typically presents with multiple, flesh-colored papillomatous papules on the penile shaft, glans, or foreskin.
Figure 6. Penile intraepithelial neoplasia

How is penile intraepithelial neoplasia recognized ?
The diagnosis is often delayed, because penile intraepithelial neoplasia may resemble other conditions such as balanitis, candidiasis, dermatitis and psoriasis.
Lesions are single or multiple, red plaques on the glans or inner aspect of the foreskin. They may have a smooth, velvety, moist, scaly, eroded or warty surface.
The following signs and symptoms may occur:
- Redness and inflammation
- Itching
- Crusting or scaling
- Pain
- Ulcers
- Bleeding
- In the late stages, discharge from penis, difficulty pulling back foreskin or difficulty passing urine
Who is at risk of penile intraepithelial neoplasia and what causes it ?
Uncircumcised males over 50 years of age are most at risk of getting penile intraepithelial neoplasia, although it may rarely occur in younger men.
Penile intraepithelial neoplasia is associated with:
- Chronic infection with human papilloma virus (HPV), the cause of genital warts. HPV-16 is the most common type identified.
- Chronic skin disease, especially lichen sclerosus and lichen planus
- Smoking
- Immune suppression by medications or disease
- Chronic irritation by urine, friction or injury to the penile area.
If left untreated, 10–30% of cases develop into invasive squamous cell carcinoma (cancer) of the penis.
What is the treatment for penile intraepithelial neoplasia ?
Skin biopsy should be performed to confirm the diagnosis, as it may resemble other forms of chronic balanitis. Biopsy is also essential to rule out invasive squamous cell carcinoma, which requires more aggressive treatment.
It is important to maintain good genital hygiene. Penile intraepithelial neoplasia can be treated in several different ways. Multidisciplinary care may be necessary.
- 5-fluorouracil cream
- Imiquimod cream
- Cryotherapy
- Curettage and cautery
- Laser vaporisation
- Photodynamic therapy
- Radiotherapy
- Excision
- Interferon alpha
Surgery, if possible, is the gold standard. However, significant morbidity can occur and medical interventions are often employed initially. These include cryotherapy, topical 5-fluorouracil (5-FU), and imiqimod, either as monotherapy or in combination.
In one report 10, good results were obtained with cryotherapy (2 freeze/thaw cycles consisting of 10 seconds of funneled spray application of liquid nitrogen per lesion per cycle) followed by at-home treatment with topical imiquimod 3 to 5 times a week for at least 8 weeks. The average number of cryotherapy sessions was 5.1. The average number of months using topical imiquimod was 7.8 months. Patients were instructed to wait at least 3 to 4 days after cryotherapy before applying the imiquimod, and to use hydrocortisone and skin moisturizer during the treatment period to ameliorate any skin irritation. All 8 patients exhibited a complete response to therapy. During the follow-up period (range 5-59 months), none of the patients exhibited signs of recurrence.
Mohs micrographic surgery appears to be highly effective and the surgical treatment of choice in severe or recurrent cases of penile intraepithelial neoplasia. Mohs micrographic surgery, or Mohs surgery, is a precise surgical technique in which the complete excision of skin cancer is checked by microscopic margin control. The skin cancer is progressively removed in stages. After each stage, the excision margins are microscopically examined for remaining cancer cells and this process is repeated until all cancer has been removed. The histological processing takes place on the day of surgery and the wound is only closed after it has been confirmed that the entire cancer has been removed. It offers the highest cure rates while maximizing preservation of healthy tissue.
The disease recurs in 3-10% of patients, so close follow-up is necessary to ensure a complete cure.
Partners of patients with penile intraepithelial neoplasia should be screened for other forms of intraepithelial neoplasia caused by human papilloma virus in the genital area (cervical, vulvar and anal cancer).
Many national immunisation programmes now include a vaccine against the causative human papillomaviruses HPV-16 and 18. Vaccination of boys and young men should be included, to reduce the risk of developing penile intraepithelial cancer in the future.
Inflammatory and Papulosquamous Lesions
Psoriasis
Psoriasis may occur at any age, with bimodal peaks at 16 to 22 years of age and at 57 to 60 years of age 11. The prevalence of psoriasis in the United States is 1 to 2 percent 12, with genital involvement occurring in up to 40 percent of patients 13. Psoriasis presents as red or salmon-colored, papulosquamous, circinate plaques (Figure 1), often associated with white or silvery scales 11. Pruritus and psychosocial distress are common. Exacerbating factors include stress, excessive alcohol and tobacco use, acute infections (particularly streptococcal), and some medication use (e.g., beta blockers, lithium) 14. Extragenital psoriasis occurs on the extensor surfaces of elbows and knees, scalp, lumbosacral region, umbilicus, and nails. Psoriatic arthritis occurs in up to 25 percent of patients.
Psoriasis is usually clinically apparent in the presence of nail pitting or confirmatory lesions elsewhere on the body 15. Punch or shave biopsy is indicated if lesions are atypical. Treatment depends on whether the disease is localized or disseminated 16. First-line localized treatment includes mild to midstrength topical corticosteroids 17. Once-daily application of corticosteroids is sufficient because genital skin is permeable, and corticosteroid receptors remain saturated for almost 24 hours. As a general rule, no more than 50 g of ultrapotent or 100 mg of potent topical corticosteroids should be applied over a long-term period9 because continuous use may cause skin atrophy. Lesions may reappear when corticosteroid use is discontinued 18. To avoid overdose, daily ultrapotent topical corticosteroid use should be limited to two weeks, followed by weekend dosing.10 If long-term therapy is required, tacrolimus (Protopic) or pimecrolimus (Elidel) may be appropriate, without the risk of atrophy 19. Vitamin D3 analogues are a first-line option for localized disease, and are usually applied once or twice daily. Patients with refractory disease should be referred to a dermatologist.
Figure 7. Penis psoriasis



- Noninfectious Penile Lesions. Am Fam Physician. 2010 Jan 15;81(2):167-174. http://www.aafp.org/afp/2010/0115/p167.html[↩][↩]
- JAMA Dermatol. 2013 Jun; 149(6):748-50[↩]
- Dermatologic Surgery 34.3 (2008): 397-399.[↩]
- Dermatologica Sinica September 2014; 32, Issue 3, Pages 154–156[↩]
- Int J Dermatol 2014;53:1145-50[↩]
- J Invest Dermatol 2014;134:S90-107[↩]
- Sex Transm Infect 2010;86:258[↩]
- Indian J Sex Transm Dis. 2013 Jan;34(1):32[↩]
- https://www.hhmi.org/news/radical-vaccine-design-effective-against-herpes-viruses[↩]
- JAAD Case Reports 2017;3;546[↩]
- Griffiths CE, Barker JN. Pathogenesis and clinical features of psoriasis. Lancet. 2007;370(9583):263–271.[↩][↩]
- Gudjonsson JE, Elder JT. Psoriasis: epidemiology. Clin Dermatol. 2007;25(6):535–546.[↩]
- MacDonald A, Burden AD. Psoriasis: advances in pathophysiology and management. Postgrad Med J. 2007;83(985):690–697.[↩]
- Menter A, Griffiths CE. Current and future management of psoriasis. Lancet. 2007;370(9583):272–284.[↩]
- Farber EM, Nall L. Genital psoriasis. Cutis. 1992;50(4):263–266.[↩]
- Quan MB, Ruben BS. Pustular psoriasis limited to the penis. Int J Dermatol. 1996;35(3):202–204.[↩]
- van de Kerkhof PC, Vissers WH. Established treatments of psoriasis. Curr Drug Targets Inflamm Allergy. 2004;3(2):145–156.[↩]
- Lebwohl M. A clinician’s paradigm in the treatment of psoriasis. J Am Acad Dermatol. 2005;53(1 suppl 1):S59–S69.[↩]
- Kalb RE, et al. Treatment of intertriginous psoriasis: from the Medical Board of the National Psoriasis Foundation. J Am Acad Dermatol. 2009;60(1):120–124.[↩]





{kind=link}