Contents
What is pinched nerve
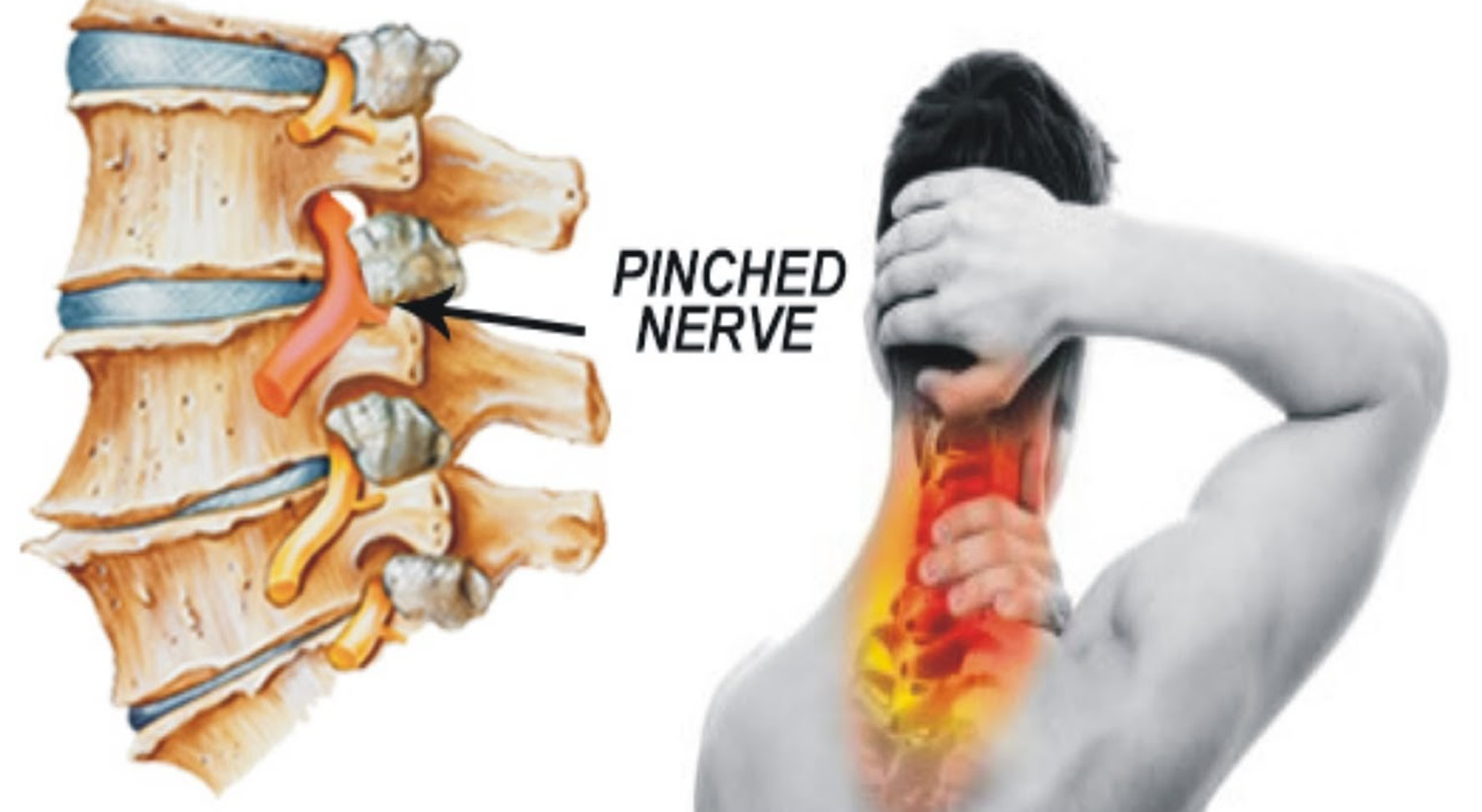
A pinched nerve occurs when too much pressure is applied to a nerve by surrounding tissues, such as bones, cartilage, muscles or tendons. This pressure disrupts the nerve’s function, causing pain, tingling, numbness or weakness.
A pinched nerve can occur at a number of sites in your body. A herniated disk in your lower spine, for example, may put pressure on a nerve root, causing pain that radiates down the back of your leg. Likewise, a pinched nerve in your wrist can lead to pain and numbness in your hand and fingers (carpal tunnel syndrome).
With rest and other conservative treatments, most people recover from a pinched nerve within a few days or weeks. Sometimes, surgery is needed to relieve pain from a pinched nerve.
Pinched nerve causes
A pinched nerve occurs when too much pressure (compression) is applied to a nerve by surrounding tissues.
In some cases, this tissue might be bone or cartilage, such as in the case of a herniated spinal disk that compresses a nerve root. In other cases, muscle or tendons may cause the condition.
In the case of carpal tunnel syndrome, a variety of tissues may be responsible for compression of the carpal tunnel’s median nerve, including swollen tendon sheaths within the tunnel, enlarged bone that narrows the tunnel, or a thickened and degenerated ligament.
A number of conditions may cause tissue to compress a nerve or nerves, including:
- Injury
- Rheumatoid or wrist arthritis
- Stress from repetitive work
- Hobbies or sports activities
- Obesity
If a nerve is pinched for only a short time, there’s usually no permanent damage. Once the pressure is relieved, nerve function returns to normal. However, if the pressure continues, chronic pain and permanent nerve damage can occur.
Risk factors for pinched nerve
The following factors may increase your risk of experiencing a pinched nerve:
- Sex. Women are more likely to develop carpal tunnel syndrome, possibly due to having smaller carpal tunnels.
- Bone spurs. Trauma or a condition that causes bone thickening, such as osteoarthritis, can cause bone spurs. Bone spurs can stiffen the spine as well as narrow the space where your nerves travel, pinching nerves.
- Rheumatoid arthritis. Inflammation caused by rheumatoid arthritis can compress nerves, especially in your joints.
- Thyroid disease. People with thyroid disease are at higher risk of carpal tunnel syndrome.
Other risk factors include:
- Diabetes. People with diabetes are at higher risk of nerve compression.
- Overuse. Jobs or hobbies that require repetitive hand, wrist or shoulder movements, such as assembly line work, increase your likelihood of a pinched nerve.
- Obesity. Excess weight can add pressure to nerves.
- Pregnancy. Water and weight gain associated with pregnancy can swell nerve pathways, compressing your nerves.
- Prolonged bed rest. Long periods of lying down can increase the risk of nerve compression.
Pinched nerve prevention
The following measures may help you prevent a pinched nerve:
- Maintain good positioning — don’t cross your legs or lie in any one position for a long time.
- Incorporate strength and flexibility exercises into your regular exercise program.
- Limit repetitive activities and take frequent breaks when engaging in these activities.
- Maintain a healthy weight.
Pinched nerve symptoms
Pinched nerve signs and symptoms include:
- Numbness or decreased sensation in the area supplied by the nerve
- Sharp, aching or burning pain, which may radiate outward
- Tingling, pins and needles sensations (paresthesia)
- Muscle weakness in the affected area
- Frequent feeling that a foot or hand has “fallen asleep”
The problems related to a pinched nerve may be worse when you’re sleeping.
See your doctor if the signs and symptoms of a pinched nerve last for several days and don’t respond to self-care measures, such as rest and over-the-counter pain relievers.
Pinched nerve diagnosis
Your doctor will ask about your symptoms and conduct a physical examination.
If your doctor suspects a pinched nerve, you may undergo some tests. These tests may include:
- Nerve conduction study. This test measures electrical nerve impulses and functioning in your muscles and nerves through electrodes placed on your skin. The study measures the electrical impulses in your nerve signals when a small current passes through the nerve. Test results tell your doctor whether you have a damaged nerve.
- Electromyography (EMG). During an EMG, your doctor inserts a needle electrode through your skin into various muscles. The test evaluates the electrical activity of your muscles when they contract and when they’re at rest. Test results tell your doctor if there is damage to the nerves leading to the muscle.
- Magnetic resonance imaging (MRI). This test uses a powerful magnetic field and radio waves to produce detailed views of your body in multiple planes. This test may be used if your doctor suspects you have nerve root compression.
- High-resolution ultrasound. Ultrasound uses high-frequency sound waves to produce images of structures within your body. It’s helpful for diagnosing nerve compression syndromes, such as carpal tunnel syndrome.
Pinched nerve treatment
The most frequently recommended treatment for pinched nerve is rest for the affected area. Your doctor will ask you to stop any activities that cause or aggravate the compression.
Depending on the location of the pinched nerve, you may need a splint or brace to immobilize the area. If you have carpal tunnel syndrome, your doctor may recommend wearing a splint during the day as well as at night because wrists flex and extend frequently during sleep.
Physical therapy
A physical therapist can teach you exercises that strengthen and stretch the muscles in the affected area to relieve pressure on the nerve. He or she may also recommend modifications to activities that aggravate the nerve.
Medications
Nonsteroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen (Advil, Motrin IB, others) or naproxen sodium (Aleve), can help relieve pain.
Corticosteroid injections, given by mouth or by injection, may help minimize pain and inflammation.
Surgery
If the pinched nerve doesn’t improve after several weeks to a few months with conservative treatments, your doctor may recommend surgery to take pressure off the nerve. The type of surgery varies depending on the location of the pinched nerve.
Surgery may entail removing bone spurs or a part of a herniated disk in the spine, for example, or severing the carpal ligament to allow more room for the nerve to pass through the wrist.
Pinched nerve in neck
Pinched nerve in neck commonly called cervical radiculopathy, occurs when a nerve in the neck is compressed or irritated where it branches away from the spinal cord. This may cause pain that radiates into the shoulder, as well as muscle weakness and numbness that travels down the arm and into the hand.
Pinched nerve in neck (cervical radiculopathy) is often caused by “wear and tear” or degenerative changes that causes a herniated, or bulging, intervertebral disk that occur in the spine as you age, such as arthritis. In younger people, it is most often caused by a sudden injury that results in a herniated disk.
Pinched nerve in neck causes
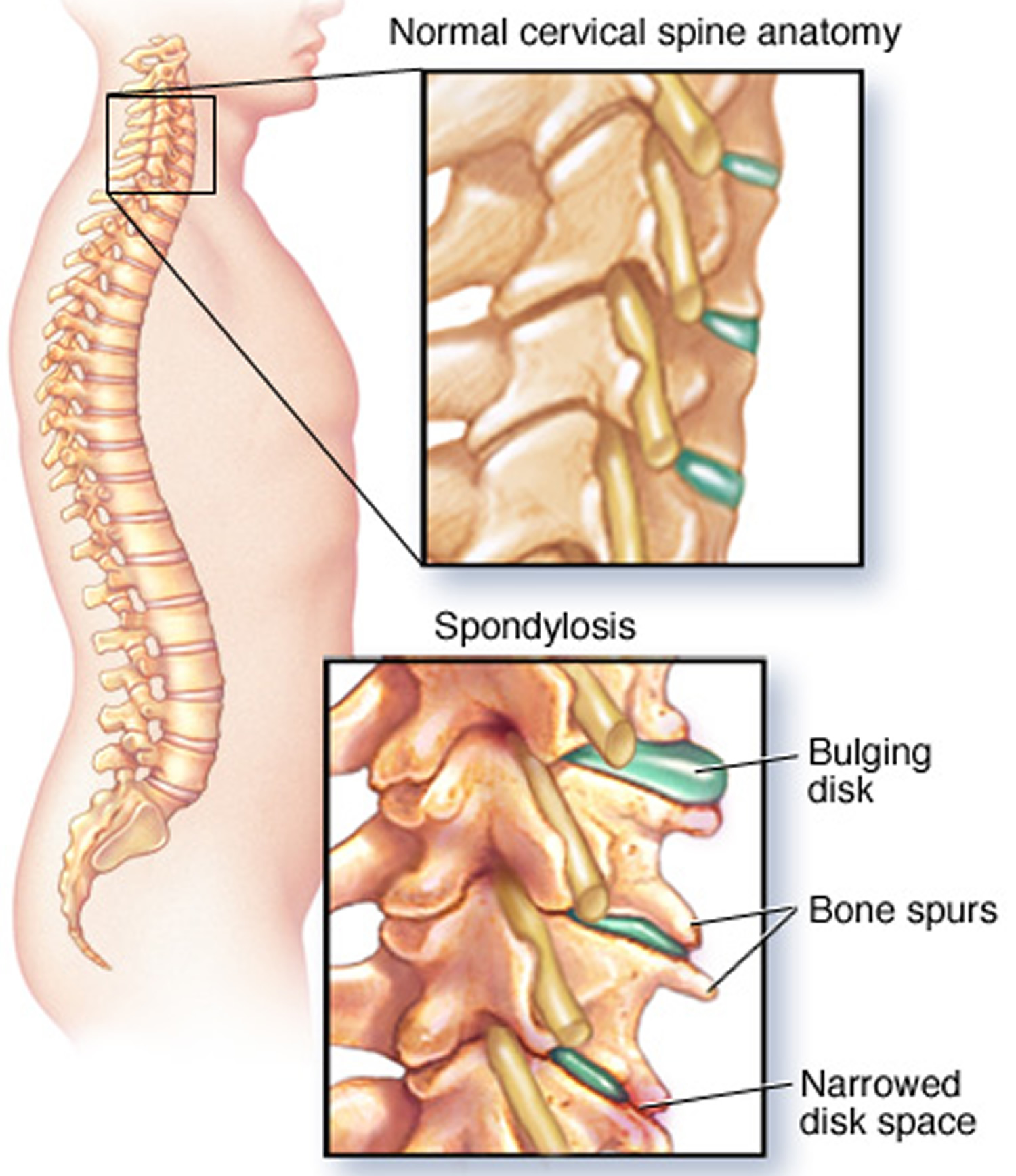
Degenerative changes. As the intervertebral disks in the spine age, they lose height and begin to bulge. They also lose water content, begin to dry out, and become stiffer. This problem causes settling or collapse of the intervertebral disk spaces and loss of disk space height.
As the intervertebral disks lose height, the vertebrae move closer together. The body responds to the collapsed disk by forming more bone —called bone spurs—around the disk to strengthen it. These bone spurs contribute to the stiffening of the spine. They may also narrow the foramen—the small openings on each side of the spinal column where the nerve roots exit—and pinch the nerve root.
Degenerative changes in the disks are often called arthritis or spondylosis. These changes are normal and they occur in everyone. In fact, nearly half of all people middle-aged and older have worn disks and pinched nerves that do not cause painful symptoms. It is not known why some patients develop symptoms and others do not.
Figure 1. Pinched nerve in neck
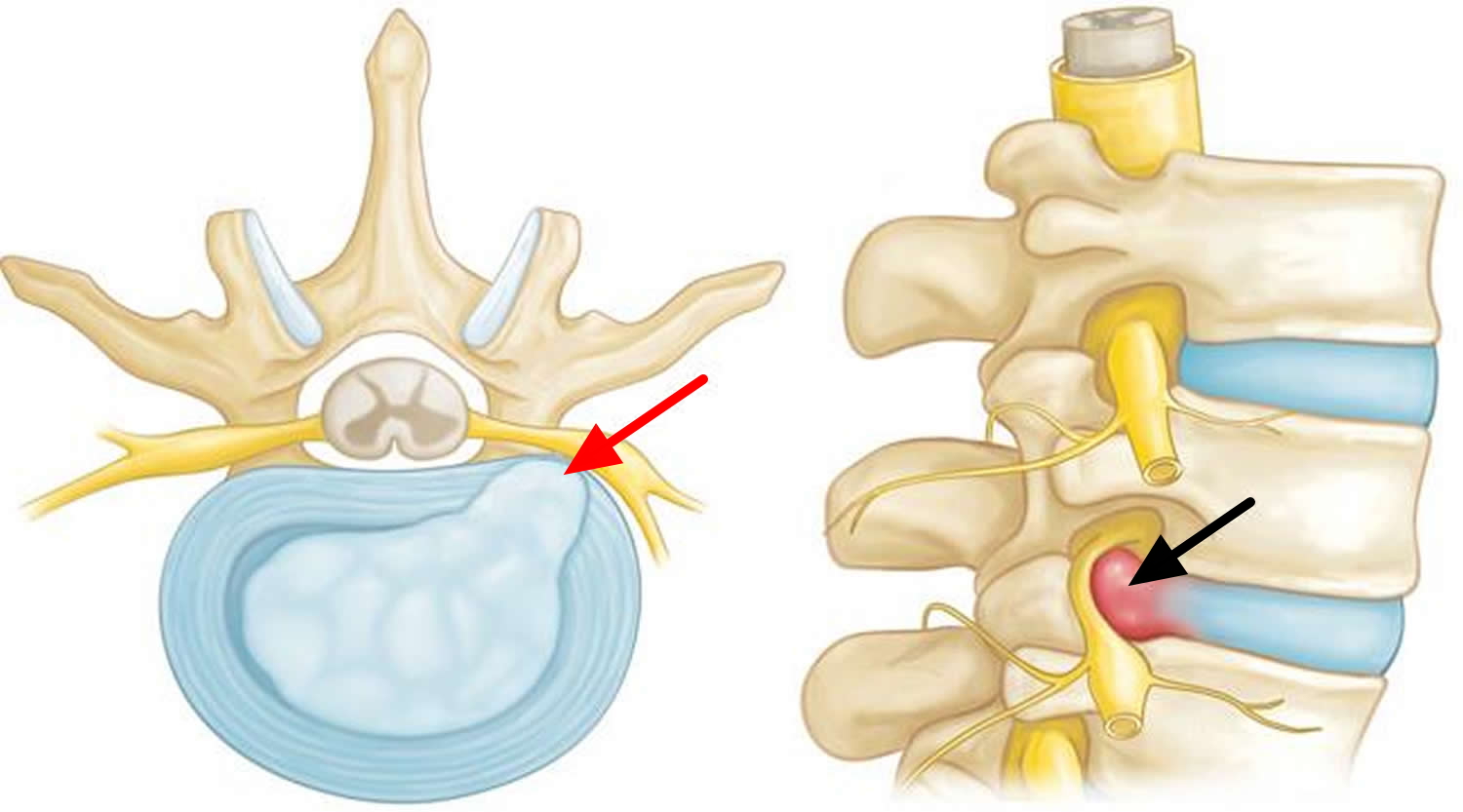
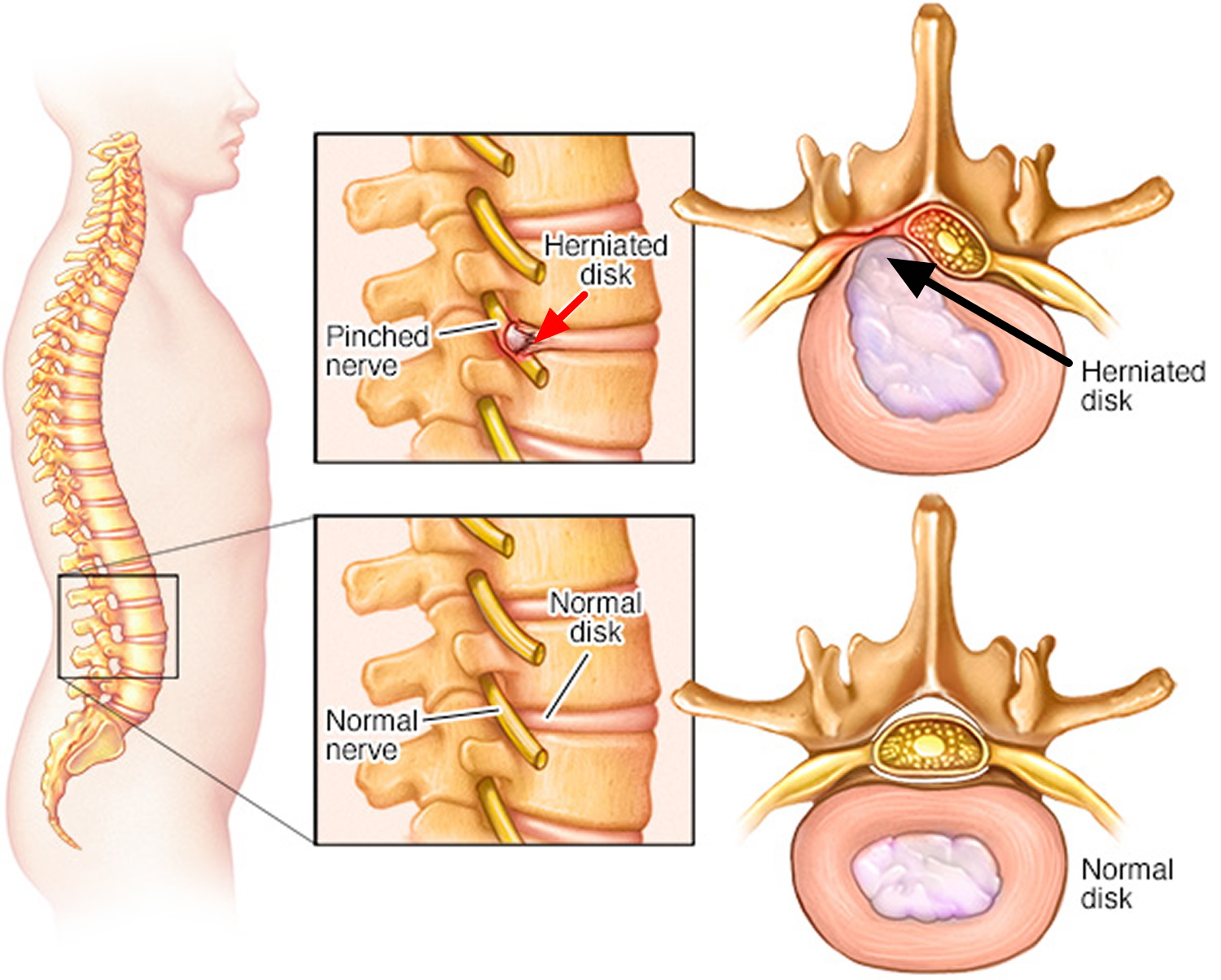
Herniated disk. A disk herniates when its jelly-like center (nucleus) pushes against its outer ring (annulus). If the disk is very worn or injured, the nucleus may squeeze all the way through. When the herniated disk bulges out toward the spinal canal, it puts pressure on the sensitive nerve root, causing pain and weakness in the area the nerve supplies.
A herniated disk often occurs with lifting, pulling, bending, or twisting movements.
Figure 2. In a herniated disk, the soft, jelly-like center of the disk can push all the way through the outer ring.
Pinched nerve in neck symptoms
In most cases, the pain of cervical radiculopathy starts at the neck and travels down the arm in the area served by the damaged nerve. This pain is usually described as burning or sharp. Certain neck movements—like extending or straining the neck or turning the head—may increase the pain. Other symptoms include:
- Tingling or the feeling of “pins and needles” in the fingers or hand
- Weakness in the muscles of the arm, shoulder, or hand
- Loss of sensation
Some patients report that pain decreases when they place their hands on top of their head. This movement may temporarily relieve pressure on the nerve root.
Pinched nerve in neck diagnosis
Physical Examination
After discussing your medical history and general health, your doctor will ask you about your symptoms. He or she will then examine your neck, shoulder, arms and hands—looking for muscle weakness, loss of sensation, or any change in your reflexes.
Your doctor may also ask you to perform certain neck and arm movements to try to recreate and/or relieve your symptoms.
Tests
- X-rays. These provide images of dense structures, such as bone. An x-ray will show the alignment of bones along your neck. It can also reveal whether there is any narrowing of the foramen and damage to the disks.
- Computed tomography (CT) scans. More detailed than a plain x-ray, a CT scan can help your doctor determine whether you have developed bone spurs near the foramen in your cervical spine.
- Magnetic resonance imaging (MRI) scans. These studies create better images of the body’s soft tissues. An MRI of the neck can show if your nerve compression is caused by damage to soft tissues—such as a bulging or herniated disk. It can also help your doctor determine whether there is any damage to your spinal cord or nerve roots.
- Electromyography (EMG). Electromyography measures the electrical impulses of the muscles at rest and during contractions. Nerve conduction studies are often done along with EMG to determine if a nerve is functioning normally. Together, these tests can help your doctor determine whether your symptoms are caused by pressure on spinal nerve roots and nerve damage or by another condition that causes damage to nerves, such as diabetes.
Pinched nerve in neck treatment
In most cases, cervical radiculopathy responds well to conservative treatment that includes medication and physical therapy. It is important to note that the majority of patients with pinched nerve in neck get better over time and do not need treatment. For some patients, the pain goes away relatively quickly—in days or weeks. For others, it may take longer.
It is also common for cervical radiculopathy that has improved to return at some point in the future. Even when this occurs, it usually gets better without any specific treatment.
In some cases, cervical radiculopathy does not improve, however. These patients require evaluation and treatment.
Nonsurgical Treatment
Initial treatment for cervical radiculopathy is nonsurgical. Nonsurgical treatment options include:
- Soft cervical collar. This is a padded ring that wraps around the neck and is held in place with Velcro. Your doctor may advise you to wear a soft cervical collar to allow the muscles in your neck to rest and to limit neck motion. This can help decrease the pinching of the nerve roots that accompany movement of the neck. A soft collar should only be worn for a short period of time since long-term wear may decrease the strength of the muscles in your neck.
- Physical therapy. Specific exercises can help relieve pain, strengthen neck muscles, and improve range of motion. In some cases, traction can be used to gently stretch the joints and muscles of the neck.
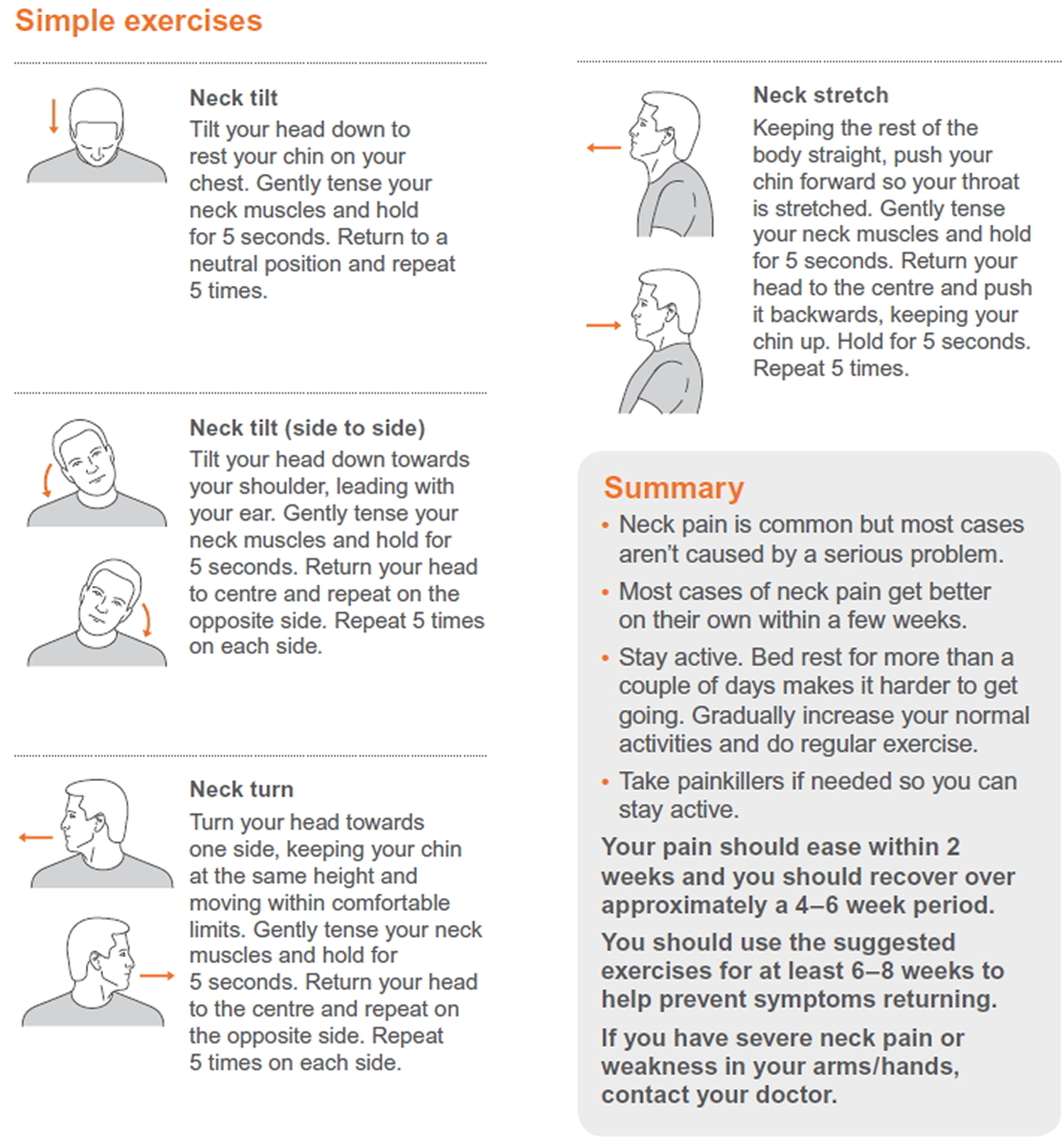
Cervical flexion
Increasing neck movement by moving the head forwards in sitting.
Cervical side-flexion
Active neck movement bending side to side (side-flexion) in sitting position
Cervical rotation
Active neck movement by turning side to side (rotation) in sitting position.
Chin tucks (cervical retraction)
Strengthening of the stabilising neck muscles by drawing the chin in gently in sitting position.
Figure 3. Neck exercises for neck pain including pinched nerve in the neck
Medications. In some cases, medications can help improve your symptoms.
- Nonsteroidal anti-inflammatory drugs (NSAIDs). NSAIDs, including aspirin, ibuprofen, and naproxen, may provide relief if your pain is caused by nerve irritation or inflammation.
- Oral corticosteroids. A short course of oral corticosteroids may help relieve pain by reducing swelling and inflammation around the nerve.
Steroid injection. In this procedure, steroids are injected near the affected nerve to reduce local inflammation. The injection may be placed between the laminae (epidural injection), in the foramen (selective nerve injection), or into the facet joint. Although steroid injections do not relieve the pressure on the nerve caused by a narrow foramen or by a bulging or herniated disk, they may lessen the swelling and relieve the pain long enough to allow the nerve to recover.
Narcotics. These medications are reserved for patients with severe pain that is not relieved by other options. Narcotics are usually prescribed for a limited time only.
Surgical Treatment
If after a period of time nonsurgical treatment does not relieve your symptoms, your doctor may recommend surgery. There are three surgical procedures to treat cervical radiculopathy. The procedure your doctor recommends will depend on many factors, including what symptoms you are experiencing and the location of the involved nerve root.
They are:
- Anterior Cervical Diskectomy and Fusion
- Artificial Disk Replacement
- Posterior Cervical Laminoforaminotomy
The procedure your doctor recommends will depend on a number of factors–most importantly, the type and location of your problem. Other factors include:
- Your preference for a procedure
- Your doctor’s preference and experience
- Your overall health and medical history (including whether you have had prior neck surgery)
Anterior Cervical Diskectomy and Fusion
Anterior Cervical Diskectomy and Fusion is the most commonly performed procedure to treat cervical radiculopathy. The procedure involves removing the problematic disk or bone spurs and then stabilizing the spine through spinal fusion.
The goals of anterior cervical diskectomy and fusion are to:
- Restore alignment of the spine
- Maintain the space available for the nerve roots to leave the spine
- Limit motion across the degenerated segment of the spine
Procedure. An “anterior” approach means that the doctor will approach your neck from the front. He or she will operate through a 1- to 2-inch incision along the neck crease. The exact location and length of your incision may vary depending on your specific condition.
During the procedure, your doctor will remove the problematic disk and any additional bone spurs, if necessary. The disk space is restored to the height it was prior to the disk wearing out. This makes more room for the nerves to leave the spine and aids in decompression.
Spinal fusion. After the disk space has been cleared out, your doctor will use spinal fusion to stabilize your spine. Spinal fusion is essentially a “welding” process. The basic idea is to fuse together the vertebrae so that they heal into a single, solid bone. Fusion eliminates motion between the degenerated vertebrae and takes away some spinal flexibility. The theory is that if the painful spine segments do not move, they should not hurt.
All spinal fusions use some type of bone material, called a bone graft, to help promote the fusion. The small pieces of bone are placed into the space left where the disk has been removed. Sometimes larger, solid pieces are used to provide immediate structural support to the vertebrae.
In some cases, the doctor may implant a metal, plastic, or bone spacer between the two adjoining vertebrae. This spacer, or “cage,” usually contains bone graft material to allow a spinal fusion to occur between the two vertebrae.
After the bone graft is placed or the cage is inserted, your doctor will use metal screws, plates and rods to increase the rate of fusion and further stabilize the spine.
Bone graft sources. The bone graft will come from either your own bone (autograft) or from a donor (allograft). If an autograft is used, the bone is usually taken from your hip area. Harvesting the bone graft requires an additional incision during your surgery. It lengthens surgical time and may cause increased pain after the operation. Your doctor will talk to you about the advantages and disadvantages of using an autograft versus an allograft, as well as a traditional bone graft versus a cage.
Artificial Disk Replacement
This procedure involves removing the degenerated disk and replacing it with artificial parts, as is done in hip or knee replacement. The goal of disk replacement is to allow the spinal segment to keep some flexibility and maintain more normal motion.
Similar to anterior cervical diskectomy and fusion, your doctor will use an “anterior” approach for the surgery—making a 1- to 2-inch incision along the neck crease. The exact location and length of your incision may vary depending on your specific condition.
During the surgery, your doctor will remove your problematic disk and then insert an artificial disk implant into the disk space. The implant is made of all metal or metal and plastic. It is designed to maintain the motion between the vertebrae after the degenerated disk has been removed. The implant may help restore the height between the vertebrae and widen the passageway for the nerve roots to exit the spinal canal.
Although no longer considered a new technology, the development of artificial disk replacement is more recent than that of anterior cervical diskectomy and fusion. To date, the outcomes of artificial disk replacement surgery are promising and are comparable to that of anterior cervical diskectomy and fusion surgery. The long-term outcomes are still being researched.
Artificial disk replacement may be an option for you—depending on the type and location of your problem. Your doctor will talk with you about your options.
Posterior Cervical Laminoforaminotomy
“Posterior” refers to the back part of your body. In this procedure, the doctor will make a 1- to 2-inch incision along the midline of the back of the neck. The exact location and size of your scar may vary depending on your condition.
During a posterior cervical laminoforaminotomy, the doctor uses a burr and other specialized tools to thin down the lamina—the bony arch that forms the backside of the spinal canal. Removing this allows the doctor better access to the damaged nerve.
He or she then removes the bone, bone spurs, and tissues that are compressing the nerve root. If your compression is due to a herniated disk, your doctor will remove the portion of the disk that is compressing the nerve, as well.
Unlike anterior cervical diskectomy and fusion, posterior cervical laminoforaminotomy does not require spinal fusion to stabilize the spine. Because of this, you will maintain better range of motion in your neck and your recovery will be quicker.
The procedure can be performed as open surgery, in which your doctor uses a single, larger incision to access your spine. It can also be done using a minimally invasive method, where several smaller incisions are made. Your doctor will discuss with you whether posterior cervical laminoforaminotomy is an option for you and, if so, how the surgery will be performed.
Complications
As with any surgical procedure, there are risks associated with cervical spine surgery. Possible complications can be related to the approach used, the bone graft, healing, and long-term changes. Before your surgery, your doctor will discuss each of the risks with you and will take specific measures to help avoid potential complications.
General Risks
The possible risks and complications for any cervical spine surgery include:
- Infection
- Bleeding
- Nerve injury
- Spinal cord injury
- Reaction to anesthesia
- The need for additional surgery in the future
- Failure to relieve symptoms
- Tear of the sac covering the nerves (dural tear)
- Life-threatening medical problems, such as heart attack, lung complications, or stroke
Anterior Cervical Diskectomy and Fusion and Artificial Disk Replacement Risks
There are additional potential risks and complications when an anterior approach is used in spine surgery. They include:
- Misplaced, broken, or loosened plates, screws, or implants
- Soreness or difficulty with swallowing
- Voice changes
- Breathing difficulty
- Injury to the esophagus
- Pain at the site the bone was taken from—if an autograft is used
- Nonunion of the spinal fusion (in Anterior Cervical Diskectomy and Fusion)
Recovery
After surgery, you will typically stay in the hospital for 1 or 2 days. This will vary, however, depending on the type of surgery you have had and how many disk levels were involved.
Most patients are able to walk and eat on the first day after surgery. It is normal to have difficulty swallowing solid foods for a few weeks or have some hoarseness following anterior cervical spine surgery.
You may need to wear a soft or a rigid cervical collar at first. How long you should wear it will depend on the type of surgery you have had.
After spinal fusion, it may take from 6 to 12 months for the bone to become solid. Because of this, your doctor will give you specific restrictions for some time period after your surgery. Right after your operation, your doctor may recommend only light activity, like walking. As you regain strength, you will be able to slowly increase your activity level.
Physical Therapy
Usually by 4 to 6 weeks, you can gradually begin to do range-of-motion and strengthening exercises. Your doctor may prescribe physical therapy during the recovery period to help you regain full function.
Return to Work
Most people are able to return to a desk job within a few days to a few weeks after surgery. They may be able to return to full activities by 3 to 4 months, depending on the procedure. For some people, healing may take longer.
Outcomes
Most patients experience favorable outcomes after surgery for cervical radiculopathy. In most cases, they experience relief from their pain and other symptoms and are able to successfully return to the activities of daily life after a period of recovery.
Pinched nerve in arm
Ulnar nerve entrapment occurs when the ulnar nerve in the arm becomes compressed or irritated.
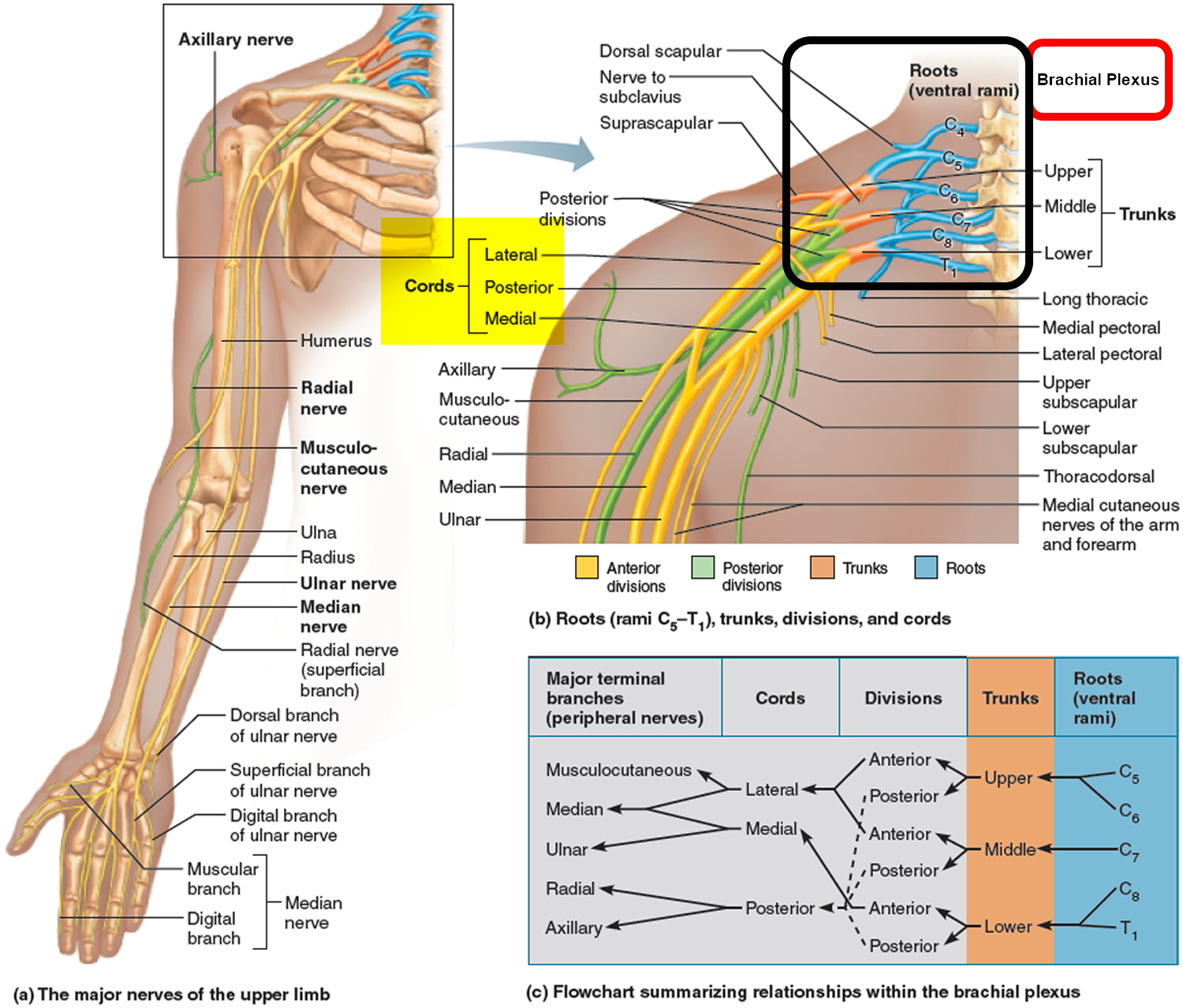
The ulnar nerve is one of the three main nerves in your arm. It travels from your neck down into your hand, and can be constricted in several places along the way, such as beneath the collarbone or at the wrist. The most common place for compression of the nerve is behind the inside part of the elbow. Ulnar nerve compression at the elbow is called “cubital tunnel syndrome.”
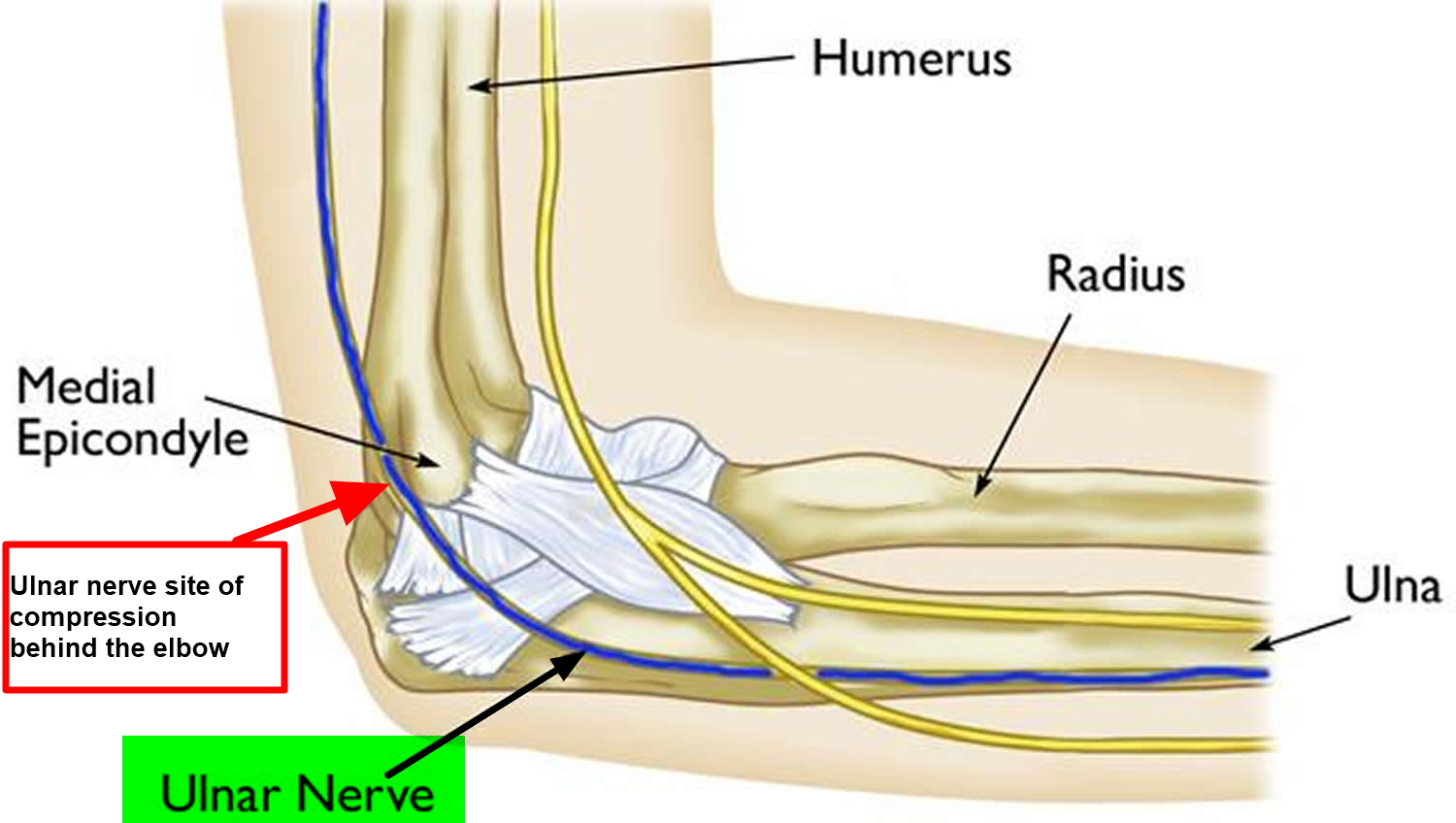
At the elbow, the ulnar nerve travels through a tunnel of tissue (the cubital tunnel) that runs under a bump of bone at the inside of your elbow. This bony bump is called the medial epicondyle. The spot where the nerve runs under the medial epicondyle is commonly referred to as the “funny bone.” At the funny bone the nerve is close to your skin, and bumping it causes a shock-like feeling.
Numbness and tingling in the hand and fingers are common symptoms of cubital tunnel syndrome. In most cases, symptoms can be managed with conservative treatments like changes in activities and bracing. If conservative methods do not improve your symptoms, or if the nerve compression is causing muscle weakness or damage in your hand, your doctor may recommend surgery.
Figure 4. Ulnar nerve
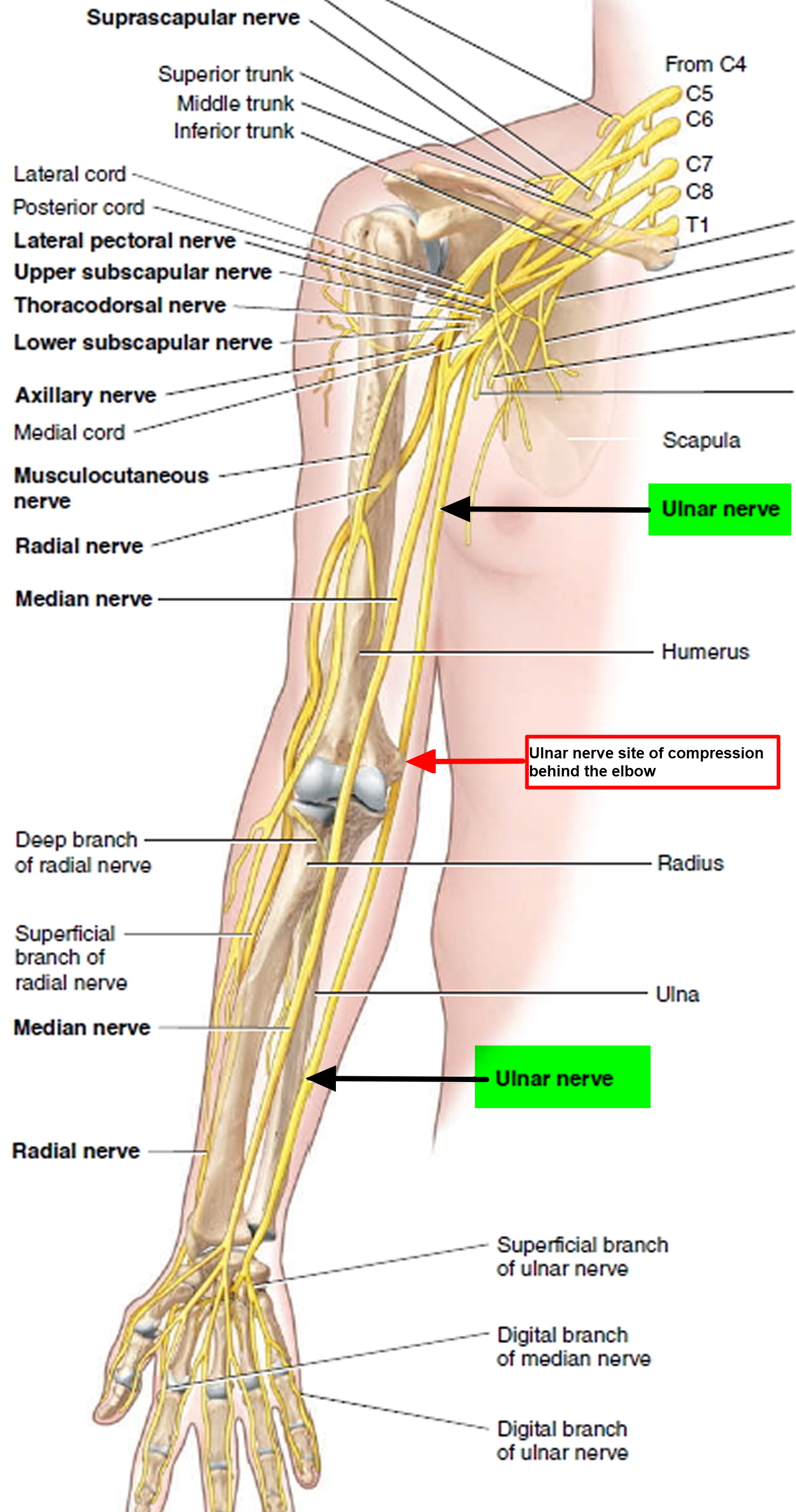
Figure 5. The ulnar nerve runs behind the medial epicondyle of the humerus on the inside of the elbow.
Beyond the elbow, the ulnar nerve travels under muscles on the inside of your forearm and into your hand on the side of the palm with the little finger. As the nerve enters the hand, it travels through another tunnel (Guyon’s canal).
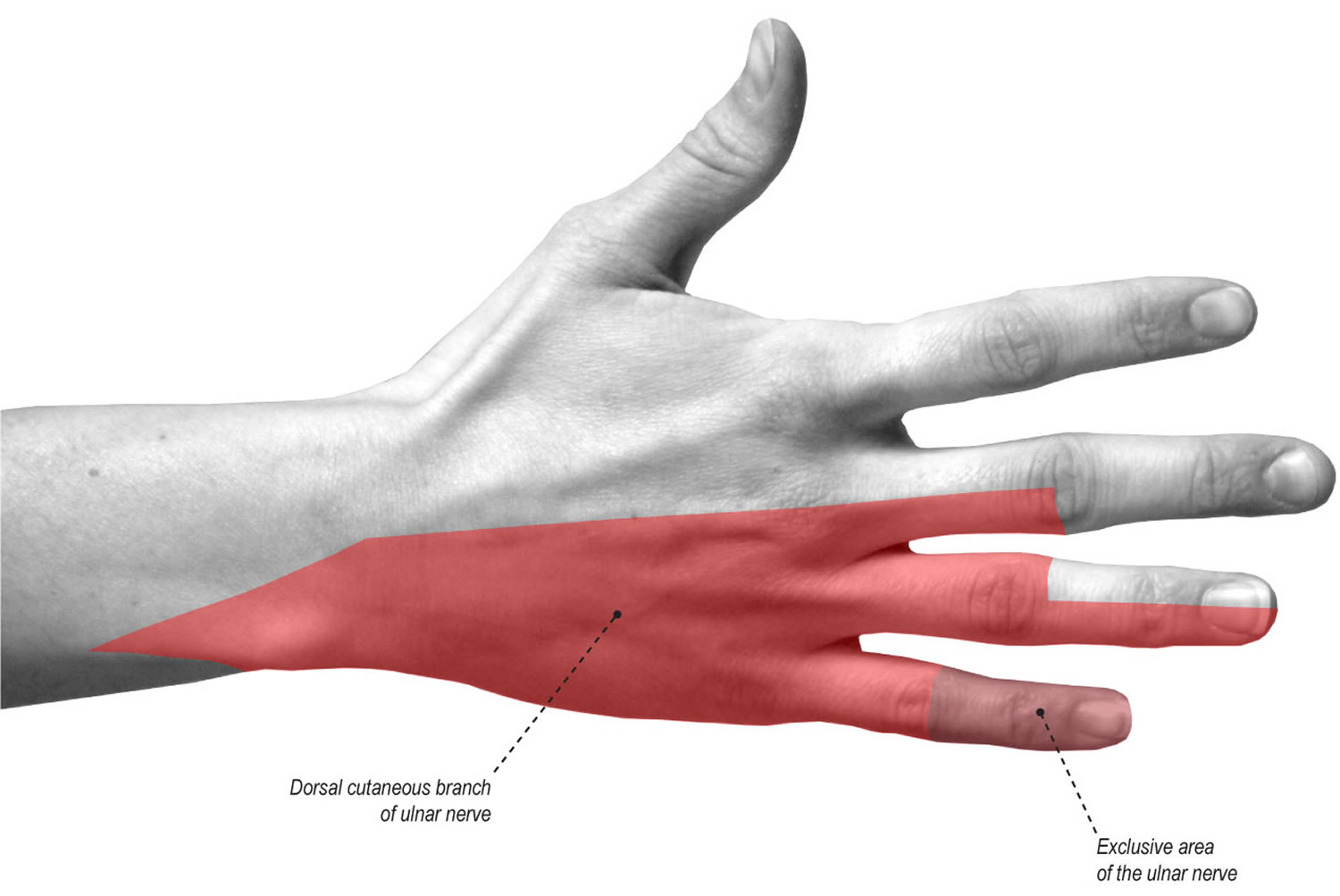
The ulnar nerve gives feeling to the little finger and half of the ring finger. It also controls most of the little muscles in the hand that help with fine movements, and some of the bigger muscles in the forearm that help you make a strong grip.
Figure 6. The ulnar nerve gives sensation (feeling) to the little finger and to half of the ring finger on both the palm and back side of the hand.
Pinched nerve in arm causes
In many cases of cubital tunnel syndrome, the exact cause is not known. The ulnar nerve is especially vulnerable to compression at the elbow because it must travel through a narrow space with very little soft tissue to protect it.
Common causes of pinched nerve in arm
There are several things that can cause pressure on the nerve at the elbow:
- When your bend your elbow, the ulnar nerve must stretch around the boney ridge of the medial epicondyle. Because this stretching can irritate the nerve, keeping your elbow bent for long periods or repeatedly bending your elbow can cause painful symptoms. For example, many people sleep with their elbows bent. This can aggravate symptoms of ulnar nerve compression and cause you to wake up at night with your fingers asleep.
- In some people, the nerve slides out from behind the medial epicondyle when the elbow is bent. Over time, this sliding back and forth may irritate the nerve.
- Leaning on your elbow for long periods of time can put pressure on the nerve.
- Fluid buildup in the elbow can cause swelling that may compress the nerve.
- A direct blow to the inside of the elbow can cause pain, electric shock sensation, and numbness in the little and ring fingers. This is commonly called “hitting your funny bone.”
Risk Factors for pinched nerve in arm
Some factors put you more at risk for developing cubital tunnel syndrome. These include:
- Prior fracture or dislocations of the elbow
- Bone spurs/ arthritis of the elbow
- Swelling of the elbow joint
- Cysts near the elbow joint
- Repetitive or prolonged activities that require the elbow to be bent or flexed
Pinched nerve in arm symptoms
Cubital tunnel syndrome can cause an aching pain on the inside of the elbow. Most of the symptoms, however, occur in your hand.
- Numbness and tingling in the ring finger and little finger are common symptoms of ulnar nerve entrapment. Often, these symptoms come and go. They happen more often when the elbow is bent, such as when driving or holding the phone. Some people wake up at night because their fingers are numb.
- The feeling of “falling asleep” in the ring finger and little finger, especially when your elbow is bent. In some cases, it may be harder to move your fingers in and out, or to manipulate objects.
- Weakening of the grip and difficulty with finger coordination (such as typing or playing an instrument) may occur. These symptoms are usually seen in more severe cases of nerve compression.
- If the nerve is very compressed or has been compressed for a long time, muscle wasting in the hand can occur. Once this happens, muscle wasting cannot be reversed. For this reason, it is important to see your doctor if symptoms are severe or if they are less severe but have been present for more than 6 weeks.
Home Remedies for pinched nerve in arm
There are many things you can do at home to help relieve symptoms. If your symptoms interfere with normal activities or last more than a few weeks, be sure to schedule an appointment with your doctor.
- Avoid activities that require you to keep your arm bent for long periods of time.
- If you use a computer frequently, make sure that your chair is not too low. Do not rest your elbow on the armrest.
- Avoid leaning on your elbow or putting pressure on the inside of your arm. For example, do not drive with your arm resting on the open window.
- Keep your elbow straight at night when you are sleeping. This can be done by wrapping a towel around your straight elbow or wearing an elbow pad backwards.
Pinched nerve in arm diagnosis
Medical History and Physical Examination
Your doctor will discuss your medical history and general health. He or she may also ask about your work, your activities, and what medications you are taking.
After discussing your symptoms and medical history, your doctor will examine your arm and hand to determine which nerve is compressed and where it is compressed. Some of the physical examination tests your doctor may do include:
- Tap over the nerve at the funny bone. If the nerve is irritated, this can cause a shock into the little finger and ring finger — although this can happen when the nerve is normal as well.
- Check whether the ulnar nerve slides out of normal position when you bend your elbow.
- Move your neck, shoulder, elbow, and wrist to see if different positions cause symptoms.
- Check for feeling and strength in your hand and fingers.
Tests
- X-rays. These imaging tests provide detailed pictures of dense structures, like bone. Most causes of compression of the ulnar nerve cannot be seen on an x-ray. However, your doctor may take x-rays of your elbow or wrist to look for bone spurs, arthritis, or other places that the bone may be compressing the nerve.
- Nerve conduction studies. These tests can determine how well the nerve is working and help identify where it is being compressed. Nerves are like “electrical cables” that travel through your body carrying messages between your brain and muscles. When a nerve is not working well, it takes too long for it to conduct. During a nerve conduction test, the nerve is stimulated in one place and the time it takes for there to be a response is measured. Several places along the nerve will be tested and the area where the response takes too long is likely to be the place where the nerve is compressed. Nerve conduction studies can also determine whether the compression is also causing muscle damage. During the test, small needles are put into some of the muscles that the ulnar nerve controls. Muscle damage is a sign of more severe nerve compression.
Pinched nerve in arm treatment
Unless your nerve compression has caused a lot of muscle wasting, your doctor will most likely first recommend nonsurgical treatment.
Nonsurgical Treatment
- Non-steroidal anti-inflammatory (NSAIDs) medicines. If your symptoms have just started, your doctor may recommend an anti-inflammatory medicine, such as ibuprofen, to help reduce swelling around the nerve.
Although steroids, such as cortisone, are very effective anti-inflammatory medicines, steroid injections are generally not used because there is a risk of damage to the nerve.
- Bracing or splinting. Your doctor may prescribe a padded brace or split to wear at night to keep your elbow in a straight position.
- Nerve gliding exercises. Some doctors think that exercises to help the ulnar nerve slide through the cubital tunnel at the elbow and the Guyon’s canal at the wrist can improve symptoms. These exercises may also help prevent stiffness in the arm and wrist.
Surgical Treatment
Your doctor may recommend surgery to take pressure off of the nerve if:
- Nonsurgical methods have not improved your condition
- The ulnar nerve is very compressed
- Nerve compression has caused muscle weakness or damage
There are a few surgical procedures that will relieve pressure on the ulnar nerve at the elbow. Your orthopaedic surgeon will talk with you about the option that would be best for you.
These procedures are most often done on an outpatient basis, but some patients do best with an overnight stay at the hospital.
Cubital tunnel release. In this operation, the ligament “roof” of the cubital tunnel is cut and divided. This increases the size of the tunnel and decreases pressure on the nerve.
After the procedure, the ligament begins to heal and new tissue grows across the division. The new growth heals the ligament, and allows more space for the ulnar nerve to slide through.
Cubital tunnel release tends to work best when the nerve compression is mild or moderate and the nerve does not slide out from behind the bony ridge of the medial epicondyle when the elbow is bent.
Ulnar nerve anterior transposition. In many cases, the nerve is moved from its place behind the medial epicondyle to a new place in front of it. Moving the nerve to the front of the medial epicondyle prevents it from getting caught on the bony ridge and stretching when you bend your elbow. This procedure is called an anterior transposition of the ulnar nerve.
The nerve can be moved to lie under the skin and fat but on top of the muscle (subcutaneous transposition), or within the muscle (intermuscular transposition), or under the muscle (submuscular transposition).
Medial epicondylectomy. Another option to release the nerve is to remove part of the medial epicondyle. Like ulnar nerve transposition, this technique also prevents the nerve from getting caught on the boney ridge and stretching when your elbow is bent.
Surgical Recovery
Depending on the type of surgery you have, you may need to wear a splint for a few weeks after the operation. A submuscular transposition usually requires a longer time (3 to 6 weeks) in a splint.
Your surgeon may recommend physical therapy exercises to help you regain strength and motion in your arm. He or she will also talk with you about when it will be safe to return to all your normal activities.
Surgical Outcome
The results of surgery are generally good. Each method of surgery has a similar success rate for routine cases of nerve compression. If the nerve is very badly compressed or if there is muscle wasting, the nerve may not be able to return to normal and some symptoms may remain even after the surgery. Nerves recover slowly, and it may take a long time to know how well the nerve will do after surgery.
Nerve gliding exercises. Some doctors think that exercises to help the ulnar nerve slide through the cubital tunnel at the elbow and the Guyon’s canal at the wrist can improve symptoms. These exercises may also help prevent stiffness in the arm and wrist.
Pinched nerve in lower back
Pinched sciatic nerve, also called sciatica, is the most common form of lower back pain caused by compression or irritation of the sciatic nerve, the longest nerve in the human body. The sciatic nerve is a large nerve the size of a little finger. The sciatic nerve originates from the L4-S3 spinal column in the lower back and travels behind the hip joint, down the buttock and down the back of the leg to the lateral aspect of the foot. The sciatic nerve is actually two nerves—tibial nerve and common fibular nerve — bound together by common sheath of connective tissue; splits into its two divisions, usually at the knee. As sciatic nerve descends through thigh, it sends branches to hamstring muscles and adductor magnus.
Pinched sciatic nerve has been reported to occur in 1 to 10% of the population and you are most likely to get sciatica between the ages of 30 and 50 years. It may happen as a result of the general wear and tear of aging, plus any sudden pressure on the disks that cushion the bones (vertebrae) of your lower spine.
A pinched sciatic nerve can cause pain anywhere along the distribution of the sciatic nerve from the lower back to the sole of the foot. It can also cause changes in sensation and muscle power of the leg. Pinched sciatic nerve is variously described as a tingling or “pins and needles”, burning, stabbing, cramping or throbbing pain that radiates from the back or buttock area down the leg to the knee, calf or foot. It can be as intense as a toothache or bad cramp and as debilitating as a headache that just won’t go away. You may have pain, especially when you move, sneeze, or cough. You may also have weakness, numbness, or a burning sensation down your leg. Pinched sciatic nerve for nine out of 10 cases will resolve on their own within 4 to 6 weeks but can last longer.
The sciatic nerve may be injured because of a herniated (slipped) disc in your spinal column that is pressing on the nerve roots in the lumbar spine, dislocated hip, osteoarthritis of the lumbosacral spine, pathological shortening of the lateral rotator muscles of the thigh (especially piriformis), pressure from the uterus during pregnancy, inflammation, irritation, or an improperly administered gluteal intramuscular injection. In addition, sitting on a wallet or other object for a long period of time can compress the nerve and induce pain.
Pinched sciatic nerve can also be caused by pelvic fractures, gunshot wounds and other trauma to the buttocks or thighs. Spinal stenosis, which occurs as people get older, can but pressure on the sciatic nerve on both sides and this can result in sciatica on both sides of the body. Masses in the pelvis such as a tumor, abscess or bleeding can also put pressure on the sciatic nerve.
Pinched nerve in lower back symptoms
Pain that radiates from your lower (lumbar) spine to your buttock and down the back of your leg is the hallmark of sciatica. You might feel the discomfort almost anywhere along the nerve pathway, but it’s especially likely to follow a path from your low back to your buttock and the back of your thigh and calf.
The pain can vary widely, from a mild ache to a sharp, burning sensation or excruciating pain. Sometimes it can feel like a jolt or electric shock. It can be worse when you cough or sneeze, and prolonged sitting can aggravate symptoms. Usually only one side of your body is affected.
Some people also have numbness, tingling or muscle weakness in the affected leg or foot. You might have pain in one part of your leg and numbness in another part.
Pinched nerve in lower back causes
Sciatica occurs when the sciatic nerve becomes pinched, usually by a herniated disk in your spine or by an overgrowth of bone (bone spur) on your vertebrae. More rarely, the nerve can be compressed by a tumor or damaged by a disease such as diabetes.
Risk factors for pinched sciatic nerve
Risk factors for sciatica include:
- Age. Age-related changes in the spine, such as herniated disks and bone spurs, are the most common causes of sciatica.
- Obesity. By increasing the stress on your spine, excess body weight can contribute to the spinal changes that trigger sciatica.
- Occupation. A job that requires you to twist your back, carry heavy loads or drive a motor vehicle for long periods might play a role in sciatica, but there’s no conclusive evidence of this link.
- Prolonged sitting. People who sit for prolonged periods or have a sedentary lifestyle are more likely to develop sciatica than active people are.
- Diabetes. This condition, which affects the way your body uses blood sugar, increases your risk of nerve damage.
Pinched nerve in lower back prevention
The following measures may help prevent sciatica:
- Weight loss
- Improved general physical condition
- Good back care
- Exercise regularly. To keep your back strong, pay special attention to your core muscles — the muscles in your abdomen and lower back that are essential for proper posture and alignment. Ask your doctor to recommend specific activities.
- Maintain proper posture when you sit. Choose a seat with good lower back support, armrests and a swivel base. Consider placing a pillow or rolled towel in the small of your back to maintain its normal curve. Keep your knees and hips level.
- Use good body mechanics. If you stand for long periods, rest one foot on a stool or small box from time to time. When you lift something heavy, let your lower extremities do the work. Move straight up and down. Keep your back straight and bend only at the knees. Hold the load close to your body. Avoid lifting and twisting simultaneously. Find a lifting partner if the object is heavy or awkward.
Figure 7. Sciatic nerve
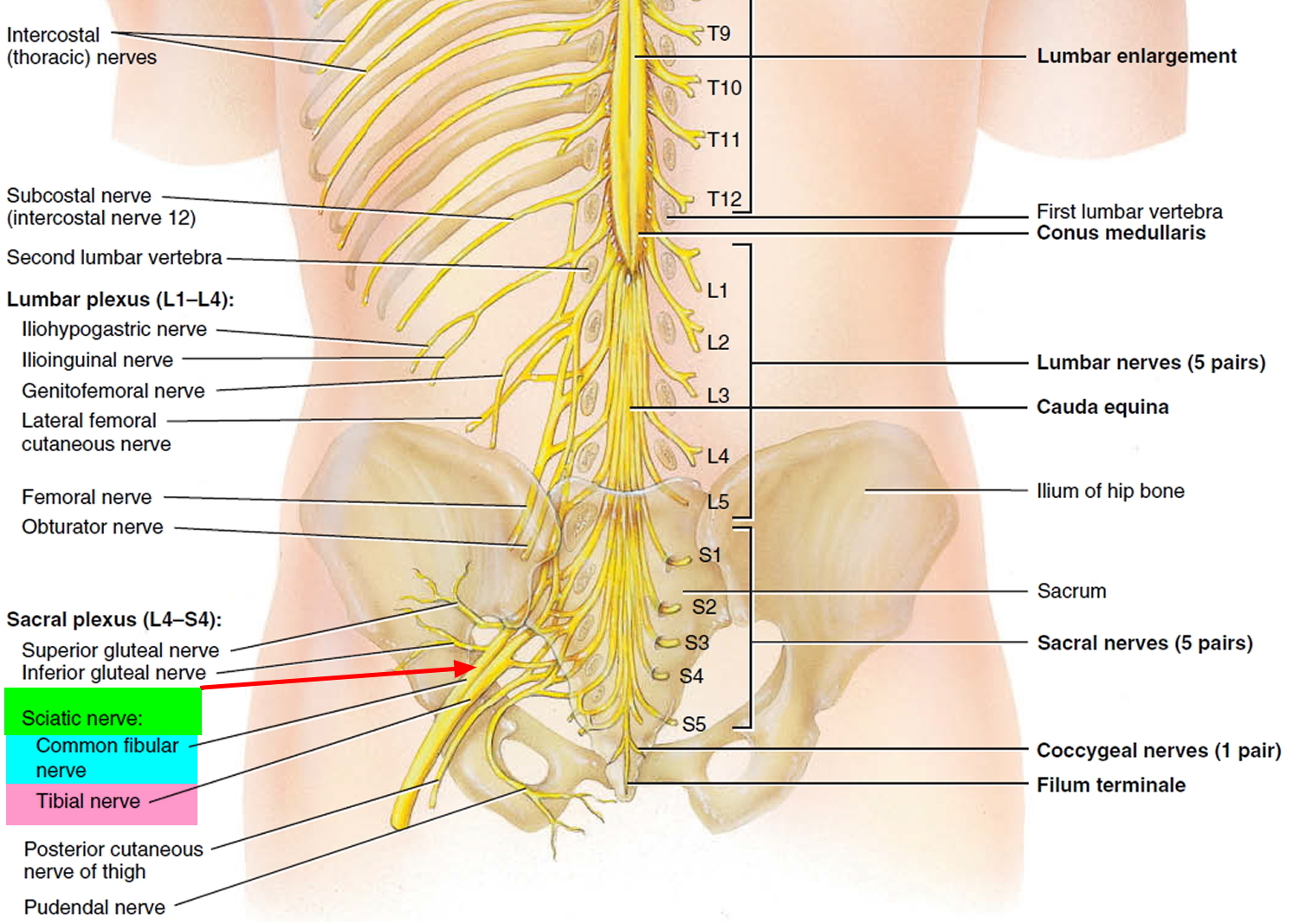
Figure 8. Sciatic nerve branches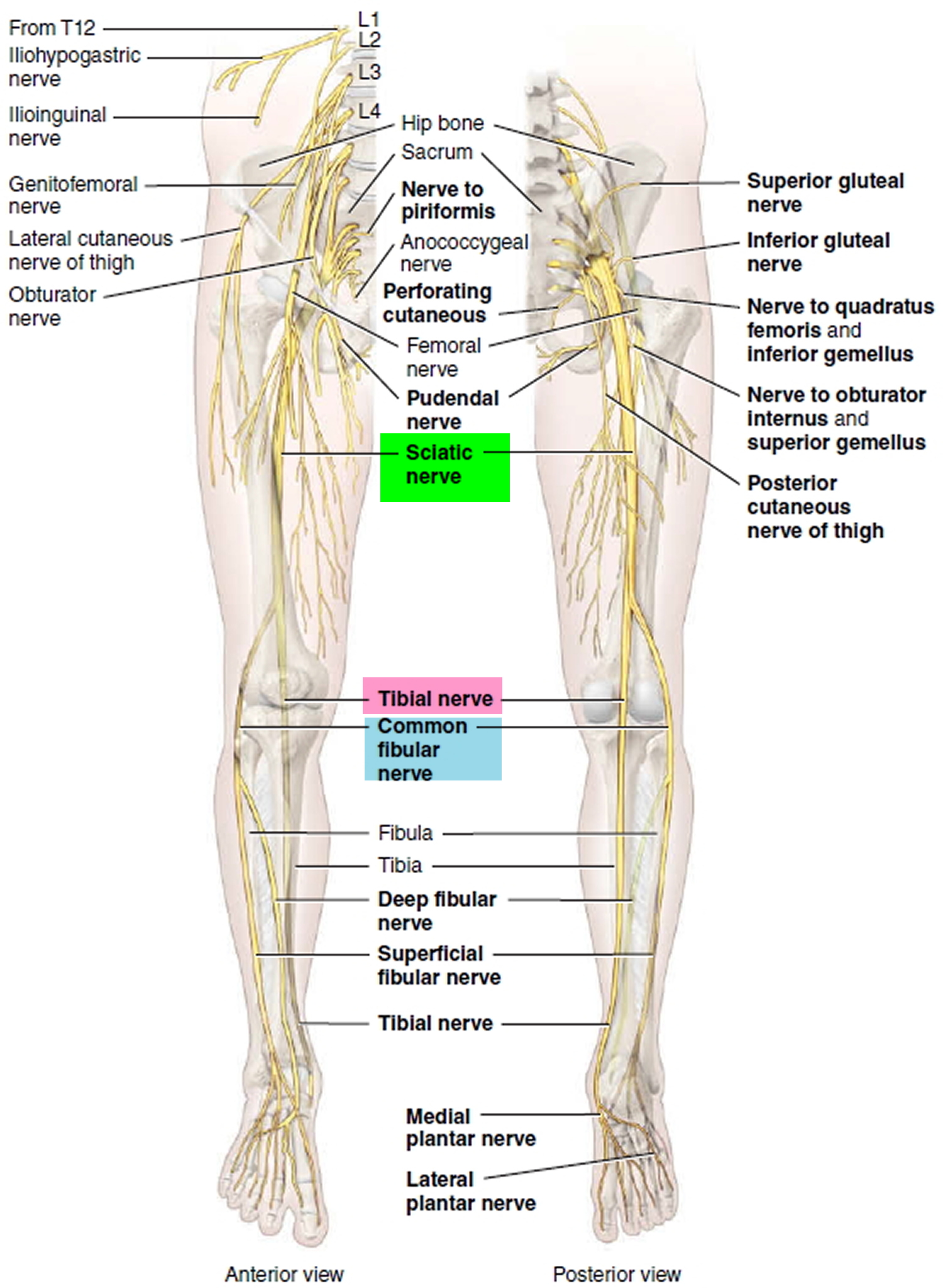
Figure 9. Herniated disk lower back
Pinched nerve in back diagnosis
Sciatica is a clinical diagnosis and does not usually require any investigations. In some cases, when the diagnosis is uncertain or if the pain is not spontaneously resolving, imaging and other investigations may be required.
Tests
Many people have herniated disks or bone spurs that will show up on X-rays and other imaging tests but have no symptoms. So doctors don’t typically order these tests unless your pain is severe, or it doesn’t improve within a few weeks.
- X-ray. An X-ray of your spine may reveal an overgrowth of bone (bone spur) that may be pressing on a nerve.
- MRI. This procedure uses a powerful magnet and radio waves to produce cross-sectional images of your back. An MRI produces detailed images of bone and soft tissues such as herniated disks. During the test, you lie on a table that moves into the MRI machine.
- CT scan. When a CT is used to image the spine, you may have a contrast dye injected into your spinal canal before the X-rays are taken — a procedure called a CT myelogram. The dye then circulates around your spinal cord and spinal nerves, which appear white on the scan.
- Electromyography (EMG). This test measures the electrical impulses produced by the nerves and the responses of your muscles. This test can confirm nerve compression caused by herniated disks or narrowing of your spinal canal (spinal stenosis).
Pinched nerve in back prognosis (outlook)
Approximately 90% cases of sciatica will resolve with conservative treatment, of which most gradually settle within 12 weeks (3 months).
Pinched nerve in back complications
Complications of sciatica can include:
- Incorrect diagnosis
- Chronic low back pain
- Loss of bowel or bladder function
- Persistent numbness or weakness of the leg
- Addiction to pain killers if they are not prescribed appropriately
- Persistent psychosocial problems related to chronic pain
Pinched nerve in back treatment
Acute sciatica:
Nonsurgical Treatment
The condition usually heals itself, given sufficient time and rest. Approximately 80% to 90% of patients with sciatica get better over time without surgery, typically within several weeks.
Nonsurgical treatment is aimed at helping you manage your pain without long-term use of medications. Nonsteroidal anti-inflammatory drugs such as ibuprofen, aspirin, or muscle relaxants may also help. In addition, you may find it soothing to put gentle heat or cold on your painful muscles. It is important that you continue to move. Do not remain in bed, as too much rest may cause other parts of the body to feel discomfort.
Find positions that are comfortable, but be as active as possible. Motion helps to reduce inflammation. Most of the time, your condition will get better within a few weeks.
Sometimes, your doctor may inject your spinal area with a cortisone-like drug.
As soon as possible, start stretching exercises so you can resume your physical activities without sciatica pain. Your doctor may want you to take short walks and may prescribe physical therapy.
Spontaneous recovery can be expected, however supportive treatment can include:
- Relative bed rest for no more than 2 days
- Return to normal activities as soon as possible
- Simple analgesics such as paracetamol (acetaminophen)
- 2 weeks of NSAIDs such as ibuprofen or naproxen
- Basic exercise such as swimming and walking should be continued
- Physiotherapy may be useful after the initial injury
Pinched sciatic nerve exercise
Some simple exercises and stretches you can do at home can help ease pain from sciatica (pain in your buttocks, legs and feet) and improve your strength and flexibility.
Aim to do these exercises every day, along with other activities like walking, swimming or yoga.
Your pain should start to ease within 2 weeks and will usually pass in about 4 to 6 weeks.
See a doctor if:
- your pain doesn’t improve within a few weeks
- you experience severe pain while trying any of these exercises
Sciatic mobilizing stretch
Start position: Lie on your back. Place a small, flat cushion or book under your head. Bend your knees and keep your feet straight and hip-width apart. Keep your upper body relaxed and your chin gently tucked in.
Action: Bend one knee up towards your chest. Hold the back of your upper leg with both hands. Then slowly straighten the knee. Hold for 20 to 30 seconds, taking deep breaths. Bend the knee and return to the starting position.
Repeat 2 or 3 times, alternating legs.
Tips:
- Don’t press your lower back down into the floor as you stretch.
- Only stretch as far as is comfortable.
Figure 10. Sciatic mobilizing stretch

Knee to chest stretch
Start position: Lie on your back on a mat or the carpet. Place a small, flat cushion or book under your head. Bend your knees and keep your feet straight and hip-width apart. Keep your upper body relaxed and your chin gently tucked in.
Action: Bend one knee up towards your chest and hold it with both hands. Hold for 20 to 30 seconds with controlled deep breaths.
Repeat 3 times, alternating legs.
Tips:
- Don’t tense your neck, chest or shoulders.
- Only stretch as far as is comfortable.
Variation: Grasp both knees and press into your chest.
Figure 11. Knee to chest stretch

Back extensions
Start position: Lie on your front and rest on your forearms with your elbows bent at your sides. Look towards the floor and keep your neck straight.
Action: Keeping your neck straight, arch your back up by pushing down on your hands. You should feel a gentle stretch in the stomach muscles. Breathe and hold for 5 to 10 seconds. Return to the starting position.
Repeat 8 to 10 times.
Tips:
- Don’t bend your neck backwards.
- Keep your hips on the floor.
Figure 12. Back extensions

Standing hamstring stretch
Start position: Stand upright and raise one leg on to a stable object, such as a step. Keep that leg straight and your toes pointing up.
Action: Lean forward while keeping your back straight. Hold for 20 to 30 seconds while taking deep breaths.
Repeat 2 or 3 times with each leg.
Tips:
- Only stretch as far as is comfortable.
- Your lower back shouldn’t arch at any time.
Figure 13. Standing hamstring stretch

Lying deep gluteal stretch
Start position: Lie on your back. Place a small, flat cushion or book under your head. Bend your left leg and rest your right foot on your left thigh.
Action: Grasp your left thigh and pull it towards you. Keep the base of your spine on the floor throughout and your hips straight. You should feel the stretch in your right buttock. Hold for 20 to 30 seconds while taking deep breaths.
Repeat 2 or 3 times with each leg.
Tips:
- Use a towel around your thigh if you can’t hold it.
Figure 14. Lying deep gluteal stretch

Chronic sciatica:
If a trial of NSAIDs, rest and physiotherapy has not brought relief, an injection of local anesthetic into the spinal (epidural space) may bring relief.
Surgical intervention:
You might need surgery if you still have disabling leg pain after 3 months or more of nonsurgical treatment. A part of your surgery, your herniated disk may be removed to stop it from pressing on your nerve.
There are some cases when surgery may be necessary in patients with sciatica, including:
- Loss of control of bladder or bowel function.
- Changes in sensation over the perineal area (around the genitals and anus).
- Progressive muscle weakness, such as foot drop or quadriceps weakness.
- Consider surgery in cases with severe prolonged pain or disabling pain, or failure of conservative treatment with persistent pain.
The surgery (laminotomy with discectomy) may be done under local, spinal, or general anesthesia. This surgery is usually very successful at relieving pain, particularly if most of the pain is in your leg.
Rehabilitation
Your doctor may give you exercises to strengthen your back. It is important to walk and move while limiting too much bending or twisting. It is acceptable to perform routine activities around the house, such as cooking and cleaning.
Following treatment for sciatica, you will probably be able to resume your normal lifestyle and keep your pain under control. However, it is always possible for your disk to rupture again.
- Neck pain exercises. http://www.csp.org.uk/publications/neck-pain-exercises[↩]





{kind=link}