
Contents
- What is placental abruption
What is placental abruption
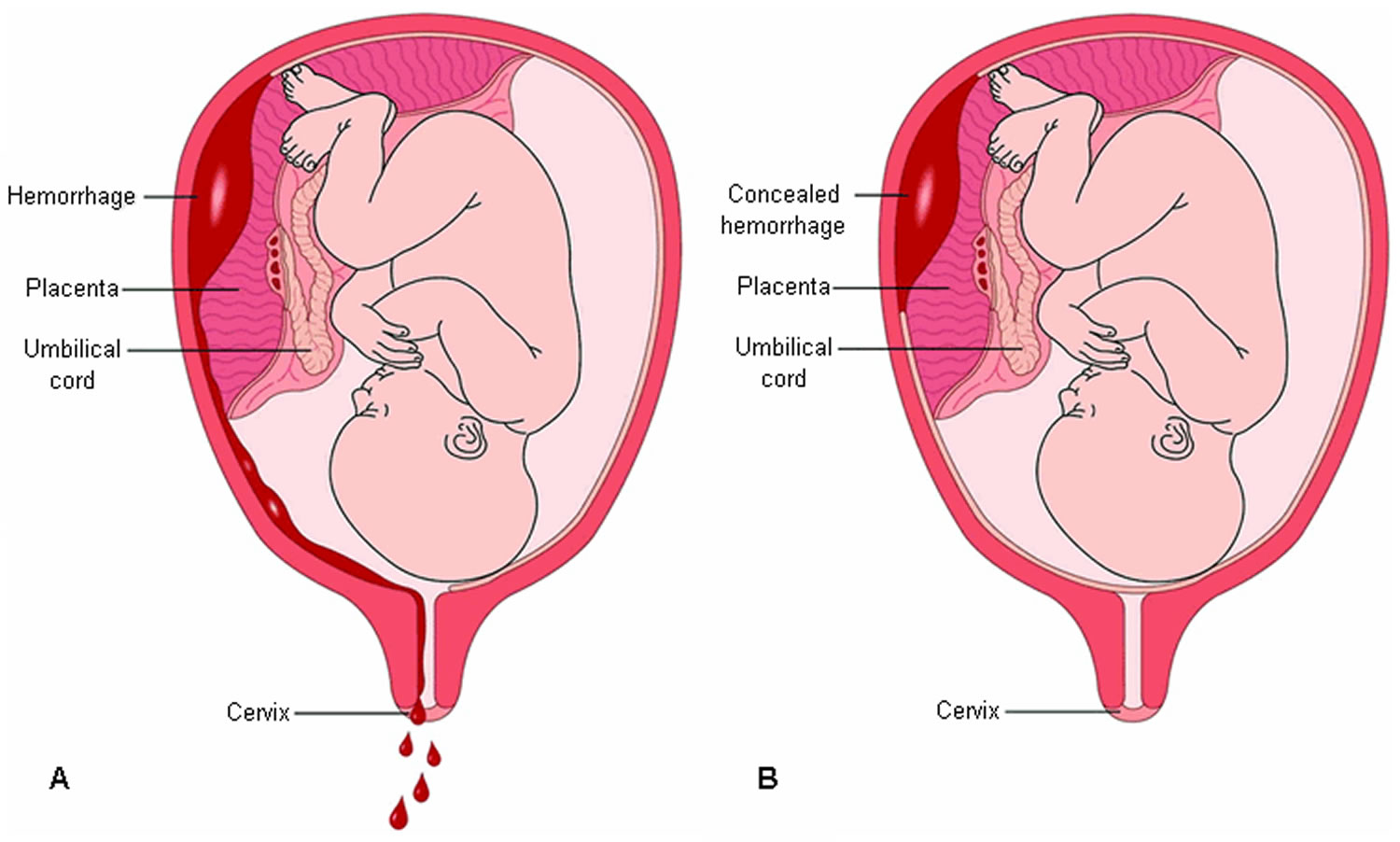
Placental abruption is a serious condition in which the normally-implanted placenta separates from the wall of the uterus before birth (after the 20th week of gestation and before the 3rd stage of labor). The placenta can separate partially or completely. If this happens, your baby may not get enough oxygen and nutrients in the womb. Placental abruption can cause stomach pain, bleeding from the vagina and frequent contractions. You also may have serious bleeding. In approximately two thirds of placental abruption cases, the bleeding which may be revealed (blood typically passes through the cervix and out the vagina) and in approximately one third of cases the bleeding is concealed (no visible blood loss) the blood remains trapped behind the placenta. Left untreated, placental abruption puts both mother and baby in jeopardy. Placental abruption can affect the baby by increasing the risk of premature birth, growth problems and stillbirth.
- Placental abruption is most common in the third trimester, but it can begin any time after 20 weeks of pregnancy.
It’s not clear what causes placental abruption, but factors that increase the risk include injury to the abdominal area, smoking, cocaine use and high blood pressure.
If you’re near your due date, the baby will need to be born straight away, and a caesarean section may be recommended. However, if the baby is very premature and the abruption is minor, you may be kept in hospital for close observation.
Normally, the placenta grows onto the upper part of the uterus and stays there until your baby is born. During the last stage of labor, the placenta separates from the uterus, and your contractions help push it into the vagina (birth canal). This is also called the afterbirth.
About 1 in 100 pregnant women (1 percent) have placental abruption. Placental abruption usually happens in the third trimester, but it can happen any time after 20 weeks of pregnancy. Mild cases may cause few problems. An placental abruption is mild if only a very small part of the placenta separates from the uterus wall. A mild abruption usually isn’t dangerous.
If you have severe placental abruption (greater separation between the placenta and the uterus), your baby is at higher risk for:
- Growth problems
- Premature birth – birth that happens too early, before 37 weeks of pregnancy
- Stillbirth – when a baby dies in the womb after 20 weeks of pregnancy
Placental abruption is related to about 1 in 10 premature births (10 percent). Premature babies (born before 37 weeks of pregnancy) are more likely than babies born later to have health problems during the first weeks of life, lasting disabilities, and even death.
Placental abruption is an emergency so it is important to seek medical attention as soon as possible if you experience any vaginal blood loss or other symptoms. It is particularly important for you to seek medical attention for signs of vaginal bleeding within 24 hours if you have a Rhesus negative blood group as you will need to be administered anti-D to avoid Rhesus disease.
Figure 1. Normal placenta and pregnancy – the placenta attaches to the wall of the uterus (womb) and supplies the baby with food and oxygen through the umbilical cord.
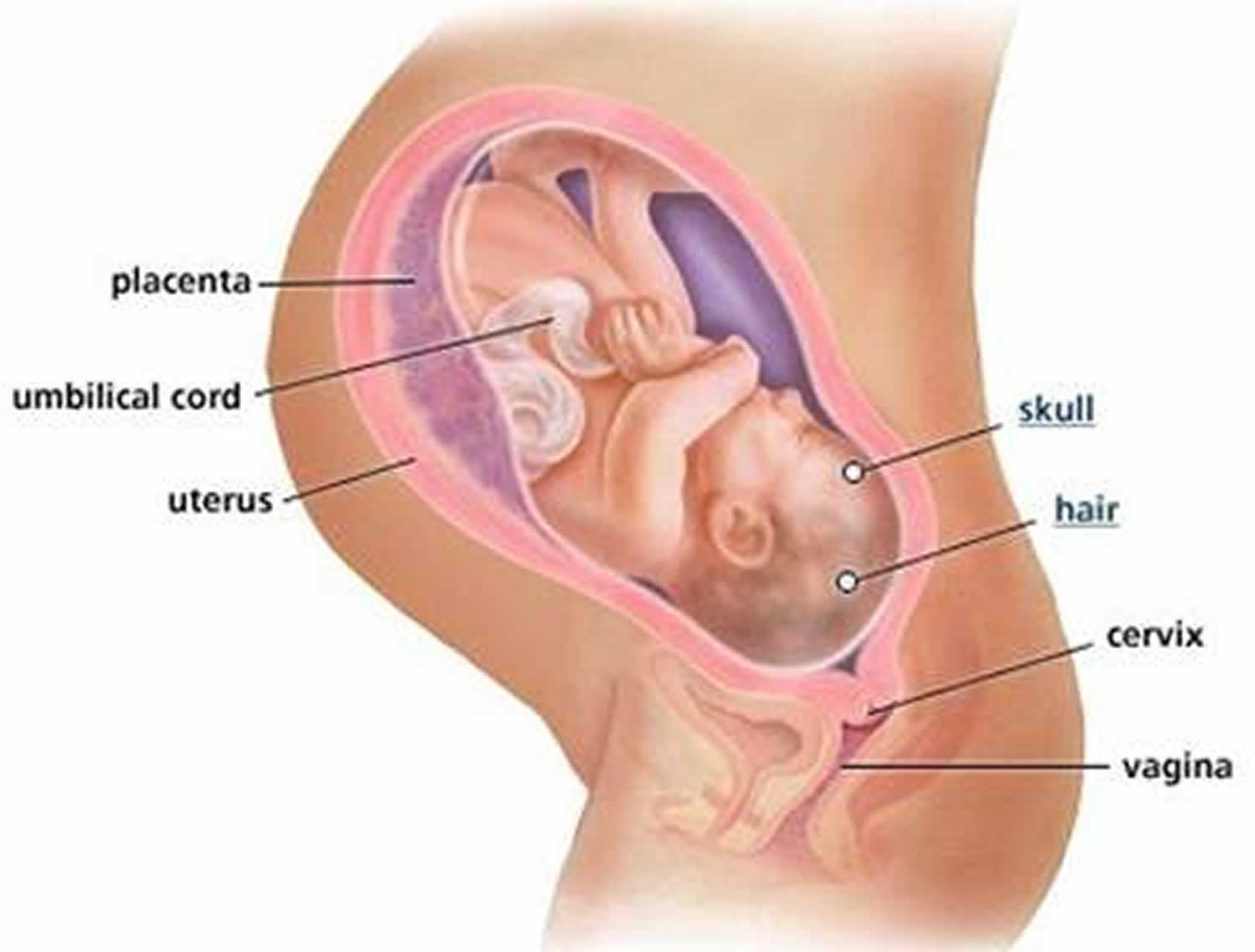
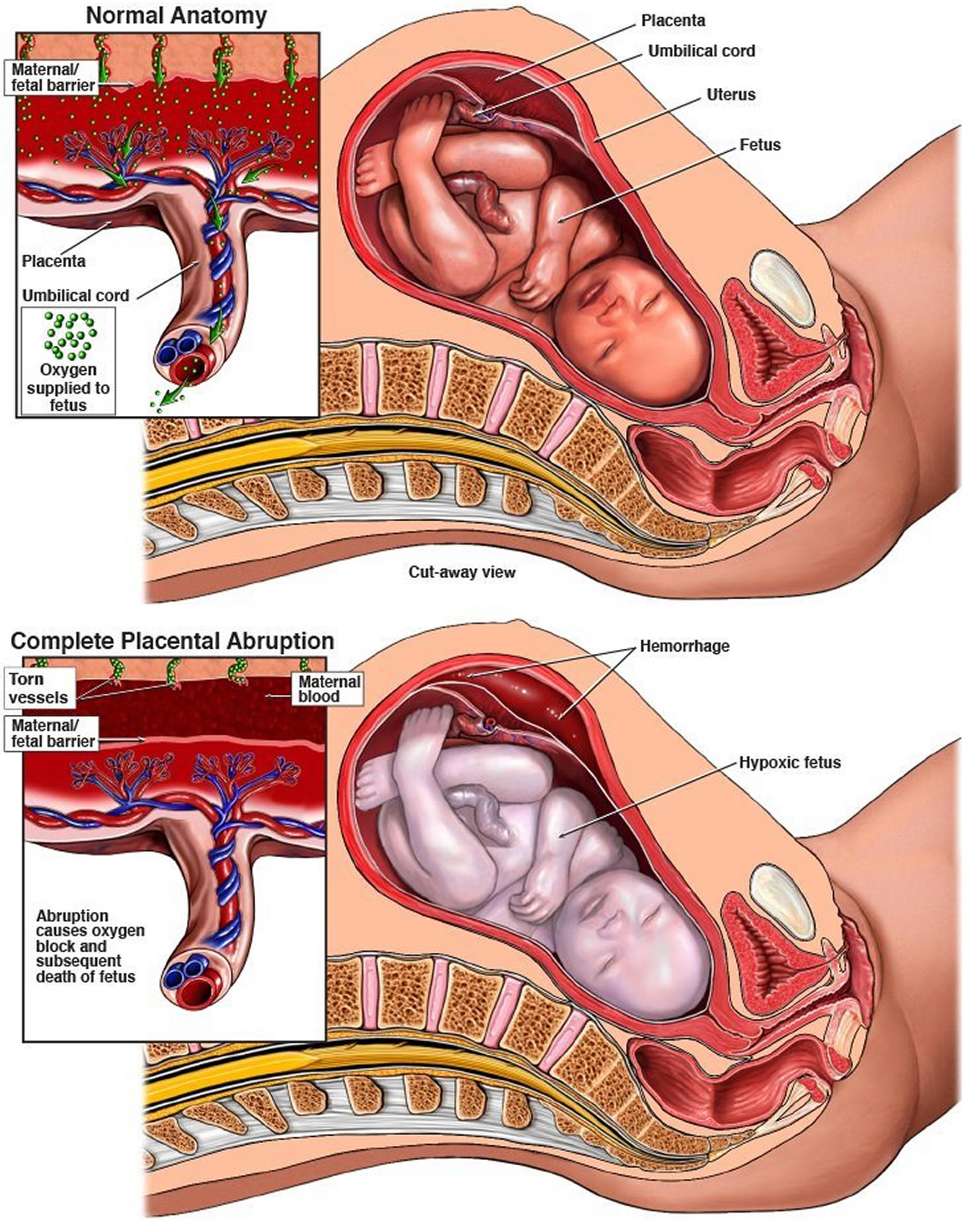
Figure 2. Placental abruption
What is the placenta
The placenta is an organ attached to the lining of your womb during pregnancy.
It keeps your unborn baby’s blood supply separate from your own blood supply, as well as providing a link between the two. The link allows the placenta to carry out functions that your unborn baby can’t perform for itself.
The placenta is connected to your baby by the umbilical cord. Your baby is inside a bag of fluid called the amniotic sac, which is made of membranes.
What does the placenta do?
Oxygen and nutrients pass from your blood supply into the placenta. From there, the umbilical cord carries the oxygen and nutrients to your unborn baby. Waste products from the baby, such as carbon dioxide, pass back along the umbilical cord to the placenta and then into your bloodstream, for your body to dispose of them.
The placenta produces hormones that help your baby grow and develop. The placenta also gives some protection against infection for your baby while it’s in the womb, protecting it against most bacteria. However, it doesn’t protect your baby against viruses.
Alcohol, nicotine and other drugs can also cross the placenta and can cause damage to your unborn baby.
Towards the end of your pregnancy, the placenta passes antibodies from you to your baby, giving them immunity for about three months after birth. However, it only passes on antibodies that you already have.
What happens after my baby is born?
After your baby is born, more contractions will push the placenta out through the vagina.
Your midwife will offer you a medicine to stimulate your contractions and help push the placenta out. They’ll inject the medicine into your thigh just as the baby is born. It makes your womb contract so the placenta comes away from the wall of your womb. This also helps prevent the heavy bleeding some women experience.
Breastfeeding your baby as soon as possible after the birth helps your womb to contract and push the placenta out.
You may choose to let your body push the placenta out in its own time, which may involve some loss of blood.
After the birth, your midwife will check the placenta and membranes, to make sure that they’re complete and nothing has been left behind.
If you have a caesarean section, after your baby is born, the placenta will also be delivered.
What does placental abruption feel like
The main symptom of placental abruption is vaginal bleeding. You also may have discomfort and tenderness or sudden, ongoing belly or back pain. Sometimes, these symptoms may happen without vaginal bleeding because the blood is trapped behind the placenta (see Figure 2 above). If you have any of these symptoms, call your healthcare provider.
Some mothers have no symptoms while others present with one or more of the classic triad of symptoms including:
- Abdominal pain,
- Vaginal bleeding and
- Uterine contractions, often coming one right after another.
Abdominal pain and back pain often begin suddenly. The amount of vaginal bleeding can vary greatly, and doesn’t necessarily correspond to how much of the placenta has separated from the uterus.
Signs and symptoms of placental abruption may also include:
- Back pain
- Uterine tenderness
- Uterine contractions
- Firmness in the uterus or abdomen
However, note that severe placental abruption can occur in the absence of any of these signs and is only found out following delivery of the placenta.
Other reported symptoms include backache, nausea, restlessness and faintness. Symptom severity depends on several factors including the location of the placenta, whether the bleeding is revealed (blood loss from the genital tract) or concealed (no evidence of bleeding from the genital tract), and the degree of placental abruption.
- Note that the volume of vaginal blood loss is a poor indicator of the degree of placental abruption. It’s possible for the blood to become trapped inside the uterus, so even with a severe placental abruption, there might be no visible bleeding.
Placental abruption also has the potential to affect your unborn child. Depending on the severity, your baby may be unaffected, distressed and be requiring urgent delivery or may be deceased. This will be determined by monitoring the baby’s heart rate.
- In some cases, placental abruption develops slowly (chronic abruption), which can cause light, intermittent vaginal bleeding. Your baby might not grow as quickly as expected, and you might have low amniotic fluid (oligohydramnios) or other complications.
If your provider thinks you are having an abruption, you may need to get checked at the hospital. Your provider can look for abruption by doing a physical exam and an ultrasound. An ultrasound can find many, but not all, placental abruptions.
Placental abruption complications
Placental abruption can cause life-threatening problems for both mother and baby.
For the mother, placental abruption can lead to:
- Shock due to blood loss
- Blood clotting problems (disseminated intravascular coagulation)
- The need for a blood transfusion
- Failure of the kidneys or other organs resulting from significant blood loss
- Rarely, when uterine bleeding cannot be controlled, hysterectomy may be necessary
For the baby, placental abruption can lead to:
- Restricted growth from not getting enough nutrients
- Not getting enough oxygen
- Premature birth
- Stillbirth
Placental abruption prognosis
Cases of placental abruption vary widely in severity and implications. Cases with minor bleeding may have little or no consequences, however more severe placental abruption can lead to fetal death and severe maternal morbidity and mortality. The risks to the mother primarily depend on the severity of the placental abruption. However, the risk to the fetus depends not only on the severity of the placental abruption but also the gestational age at which the placental abruption occurs.
As with most obstetric emergencies, doctors need to consider both the effects on the mother and the effects on the fetus.
Effects on the mother
The acute blood loss seen with placental abruption, depending on the severity, may result in:
- Hypovolaemic shock
- Disseminated intravascular coagulation (DIC)
- Acute renal failure
- Feto-maternal hemorrhage
In extreme cases, placental abruption may also result in maternal death, usually as a consequence of the above listed complications.
In subsequent pregnancies, the risk of placental abruption reoccurring is ~10% and increases to 25% following a second episode.
Effects on the fetus
Placental abruption represents a significant cause of fetal and neonatal death. Outcomes depend on the size of the placental abruption, time to delivery, gestational age at placental abruption and delivery and other factors.
In cases of chronic or recurrent placental abruption, the area of placenta available for nutrient and waste exchange is reduced, which may lead to intrauterine growth restriction.
Placental abruption causes
What causes placental abruption
Scientists don’t really know what causes placental abruption. You may be at higher risk for placental abruption if:
- You smoke cigarettes.
- You use cocaine.
- You’re 35 or older.
- You have high blood pressure.
- You have an infection in your uterus.
- Your water breaks before 37 weeks.
- You had placental abruption in a previous pregnancy.
- You have problems with the uterus or umbilical cord.
- You have more fluid around the baby than is normal.
- You’re pregnant with twins, triplets or more.
- Your belly is harmed from a car accident or physical abuse.
If you’ve had a placental abruption in a past pregnancy, you have about a 1 in 10 (10 percent) chance of it happening again in a later pregnancy.
Risk factors for placental abruption
The exact cause of placental abruption is unknown, but there are a number of risk factors including:
- Disorders of blood pressure
- High parity
- Increased maternal age
- Low socioeconomic groups
- Prolonged preterm rupture of the membranes
- Polyhydramnios
- Following delivery of a first twin
- Trauma (e.g. fall; motor vehicle accident)
- Cigarette smoking (the more that is smoked, the more the risk is increased)
- Cocaine and drug use
- Preeclampsia
- Oligohydramnios
- Chorioamnionitis
Placental abruption prevention
In most cases, you can’t prevent placental abruption. But you may be able to reduce your risk by getting treatment for high blood pressure, not smoking or using street drugs, and always wearing a seatbelt when riding in a car. If you’ve had abdominal trauma — from an auto accident, fall or other injury — seek immediate medical help.
If you’ve had a placental abruption, and you’re planning another pregnancy, talk to your health care provider before you conceive to see if there are ways to reduce the risk of another abruption.
Placental abruption signs and symptoms
The clinical presentation of placental abruption varies widely. Some mothers have no symptoms while others present with one or more of the classic triad of symptoms including:
- Abdominal pain,
- Vaginal bleeding and
- Uterine contractions, often coming one right after another.
Abdominal pain and back pain often begin suddenly. The amount of vaginal bleeding can vary greatly, and doesn’t necessarily correspond to how much of the placenta has separated from the uterus.
Signs and symptoms of placental abruption may also include:
- Back pain
- Uterine tenderness
- Uterine contractions
- Firmness in the uterus or abdomen
However, note that severe placental abruption can occur in the absence of any of these signs and is only found out following delivery of the placenta.
Other reported symptoms include backache, nausea, restlessness and faintness. Symptom severity depends on several factors including the location of the placenta, whether the bleeding is revealed (blood loss from the genital tract) or concealed (no evidence of bleeding from the genital tract), and the degree of placental abruption.
- Note that the volume of vaginal blood loss is a poor indicator of the degree of placental abruption. It’s possible for the blood to become trapped inside the uterus, so even with a severe placental abruption, there might be no visible bleeding.
Placental abruption also has the potential to affect your unborn child. Depending on the severity, your baby may be unaffected, distressed and be requiring urgent delivery or may be deceased. This will be determined by monitoring the baby’s heart rate.
- In some cases, placental abruption develops slowly (chronic abruption), which can cause light, intermittent vaginal bleeding. Your baby might not grow as quickly as expected, and you might have low amniotic fluid (oligohydramnios) or other complications.
Placental abruption diagnosis
If your health care provider suspects placental abruption, he or she will do a physical exam to check for uterine tenderness or rigidity. To help identify possible sources of vaginal bleeding, your provider will likely recommend blood and urine tests and ultrasound.
On examination, your doctor will be examining you for signs and symptoms of placental abruption as well as other differential diagnoses depending on your presenting symptoms. They will be especially concerned with your vital signs, including heart rate and blood pressure to assess whether you are showing any signs of shock. They will also feel your abdomen to determine the tone of your uterus, if there is any pain or tenderness and whether or not it is contracting. A speculum examination may be performed to assess any vaginal loss and whether or not your cervix is open or closed.
Other than your health, they will also be concerned with the health of your unborn child. They will be interested in foetal movements, the foetal heart rate and how far along you are in the pregnancy. If there are any signs of fetal compromise, active bleeding, uterine activity or tenderness a cardiotocograph (CTG) will be applied for continuous monitoring.
Several blood tests will be ordered and an ultrasound may be necessary.
Placental abruption ultrasound
During an ultrasound, high-frequency sound waves create an image of your uterus on a monitor. However, it’s not always possible to see a placental abruption on an ultrasound.
Figure 3. Placental abruption ultrasound

Note: Crescent of avascular, low echogenicity between placenta and uterine wall consistent with placental abruption. Scan showed an otherwise live fetus, with normal growth parameters, liquor volume and Doppler parameters.
Placental abruption treatment
It isn’t possible to reattach a placenta that’s separated from the wall of the uterus. Treatment depends on how serious the placental abruption is and how far along you are in your pregnancy.
As the presentation of placental abruption is highly variable, treatment is individualized on a case-by-case basis. Your healthcare provider may simply monitor you and your baby. But sometimes you may need to give birth right away.
All women with placental abruption require intravenous fluids as even with large blood losses, pulse and blood pressure can remain within normal limits.
Women in shock require immediate, rapid intravenous fluid therapy and possibly a blood transfusion. Their urinary output is also carefully monitored.
The stability of the mother is the priority. This means that in cases where the fetus is alive and delivery is urgent, accelerated delivery should not compromise the mother’s resuscitation. In many cases, a caesarean section will be required. In severe cases where the fetus has died, delivery is delayed until the mother is stable. Once stable, and in the absence of other contraindications, vaginal delivery can be allowed.
If you need to give birth right away, your provider may give you medicines called corticosteroids. These medicines help speed up development of your baby’s lungs and other organs.
Mild placental abruption
If you have a mild abruption at 24 to 34 weeks of pregnancy, you need careful monitoring in the hospital. If tests show that you and your baby are doing well, your provider may give you treatment to try to keep you pregnant for as long as possible. Your provider may want you to stay in the hospital until you give birth. If the bleeding stops, you may be able to go home.
If you have a mild abruption at or near full term, your provider may recommend inducing labor or cesarean birth (c-section). You may need to give birth right away, if:
- The abruption gets worse.
- You are bleeding heavily.
- Your baby is having problems.
Moderate or severe placental abruption
If you have a moderate to severe abruption, you usually need to give birth right away. Needing to give birth quickly may increase your chances of having a cesarean section (c-section).
If you lose a lot of blood due to placental abruption, you may need a blood transfusion. It’s very rare, but if you have heavy bleeding that can’t be controlled, you may need a hysterectomy. A hysterectomy is when your uterus is removed by surgery. A hysterectomy can prevent deadly bleeding and other problems in your body. But it also means that you can’t get pregnant again in the future.
Management in subsequent pregnancy
The risk of placental abruption occurring again in a subsequent pregnancy is increased approximately ten fold. These women are also at increased risk of other adverse pregnancy outcomes including preeclampsia and preterm birth.
Women in this situation are encouraged to minimize exposure to those predisposing factors that are within your control, particularly cocaine and tobacco use. Prior to the next pregnancy it is also important to have good blood pressure control in those with hypertension.
It would be reasonable in subsequent pregnancies to increase the frequency of ultrasounds in the second half of the pregnancy to monitor fetal growth. If a mother has a history of two or more prior placental abruptions, amniocentesis for lung maturity and delivery at 37 weeks gestation may be carried out.





{kind=link}