Contents
- Polycystic ovarian syndrome
- What age does polycystic ovarian syndrome start?
- Can polycystic ovarian syndrome be prevented or avoided?
- Can I still get pregnant if I have PCOS?
- What are my treatment options for PCOS if I want to get pregnant?
- How does PCOS affect pregnancy?
- How can I prevent problems from PCOS during pregnancy?
- Will PCOS symptoms go away at menopause?
- Does being Overweight cause polycystic ovarian syndrome?
- How does obesity interact with polycystic ovarian syndrome?
- Should obese women with polycystic ovarian syndrome lose weight before treatment or should they receive treatment irrespective of the possible outcome?
- Does polycystic ovarian syndrome cause obesity?
- Polycystic ovarian syndrome causes
- Polycystic ovarian syndrome pathophysiology
- Polycystic ovarian syndrome symptoms
- Polycystic ovarian syndrome complications
- Polycystic ovarian syndrome diagnosis
- Polycystic ovarian syndrome treatment
- Polycystic ovarian syndrome prognosis
Polycystic ovarian syndrome
polycystic ovarian syndrome also known as “PCOS”, “polycystic ovary syndrome“, “polycystic ovarian disease” or “PCOD” is the most common hormone disorder that affects 6 to 20% of girls and women of childbearing age 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16. Polycystic ovarian syndrome was named Stein—Leventhal Syndrome in 1935 after the authors who described polycystic ovarian morphology in patients suffering from hirsutism, amenorrhoea and infertility 17, 18. Polycystic ovarian syndrome affects 4% to 18% (as many as 5 million) of US women and girls of reproductive age 19, 20.
Many doctors struggle to recognize polycystic ovarian syndrome (PCOS) since there are no clear diagnostic criteria that unequivocally identify PCOS 15. Polycystic ovarian syndrome (PCOS) is characterized by two or more of the following: irregular menstrual periods due lack of ovulation (anovulation), androgen excess (hyperandrogenism) and polycystic ovaries (the organ that produces and releases eggs), accompanied by metabolic abnormalities, such as insulin resistance and obesity 2, 21. If you have PCOS, your ovaries produce unusually high levels of hormones called androgens (testosterone, androstenedione or dehydroepiandrosterone sulfate [DHEAS]). This causes your reproductive hormones to become imbalanced. As a result, people with PCOS often have irregular menstrual cycles, missed periods or you may have periods that last many days and unpredictable ovulation. With PCOS, many small sacs of fluid develop along the outer edge of the ovary. These are called cysts. Small follicle cysts (fluid-filled sacs with immature eggs) may be visible on your ovaries on ultrasound. These follicles (small fluid-filled cysts containing immature eggs) fail to regularly release eggs or ovulation (anovulation). However, despite the name “polycystic”, you don’t need to have cysts on your ovaries to have PCOS. The ovarian cysts aren’t dangerous or painful.
Polycystic ovarian syndrome (PCOS) is also a common cause of infertility, insulin resistance, increases the risk of type 2 diabetes 22. Obesity is frequently observed in women with PCOS, predominantly in the form of abdominal obesity, aggravating metabolic and reproductive complication as well as PCOS-associated complications 23. Early diagnosis and treatment of polycystic ovarian syndrome (PCOS) along with weight loss may lower your risk of long-term complications such as type 2 diabetes and heart disease.
Girls and women with PCOS can develop serious health problems, especially if they are overweight or obese, including 24:
- Type 2 diabetes
- Gestational diabetes (diabetes when pregnant)
- Heart disease—women with PCOS have a higher risk of heart disease that increases with age
- High blood pressure (hypertension)
- High LDL (low density lipoprotein or “bad”) cholesterol and low HDL (high density lipoprotein or “good”) cholesterol (dyslipidemia) can increase your risk for heart and blood vessels disease (cardiovascular disease)
- Sleep apnea—a disorder that causes your breathing to stop during sleep
- Stroke
Studies show women with PCOS have higher rates of depression, anxiety, eating disorders, infertility and postpartum depression compared with women without polycystic ovarian syndrome, though the connection is not fully understood 1, 25.
The exact causes of PCOS aren’t yet known but it’s a multifactorial disorder that may involve the complex interaction of a number of genetic and environmental factors 26, 27, 28. For example, environmental factors implicated in PCOS such as being overweight or obese can be exacerbated by poor dietary choices and physical inactivity; infectious agents and toxins may also play a role 28. Imbalances in androgen levels (male reproductive hormones) may play an important part in PCOS. Family history of PCOS and overweight may also contribute 28. Polycystic ovarian syndrome is also burdened with insulin resistance that is worsened by hyperandrogenism-related fatty tissue accumulation and dysfunction with lipotoxicity and oxidative stress 29. These complex endocrine-metabolic interactions determine the risks of women with PCOS developing infertility, diabetes and/or cardiovascular disease 29.
There is no single test to diagnose PCOS. To help diagnose PCOS and rule out other causes of your symptoms, your doctor may talk to you about your medical history and do a physical exam and order tests such as blood test and pelvic ultrasound. Blood tests will check your androgen hormone or male hormone levels. Your doctor will also check for other hormones related to other common health problems that can be mistaken for PCOS, such as thyroid disease. Your doctor may also test your cholesterol levels and test you for diabetes. Pelvic ultrasound uses sound waves to examine your ovaries for cysts and check the endometrium (lining of the uterus or womb).
You may be diagnosed with PCOS if you have at least two of the following symptoms 30:
- Irregular periods, including periods that come too often, not often enough, or not at all
- Signs that you have high levels of androgens:
- Extra hair growth on your face, chin, and body (hirsutism)
- Acne
- Thinning of scalp hair
- Higher than normal blood levels of androgens
- Multiple cysts on one or both ovaries
PCOS treatment focuses on managing the things that are concerning you. This could include infertility, hirsutism, acne or obesity. Specific treatment might involve lifestyle changes or medication. You might need to lose weight. Eating healthy and getting plenty of exercise can help manage PCOS. The reproductive and metabolic features of PCOS are sometimes reversible with lifestyle modifications such as weight loss and exercise 31. Losing weight may help to lower your blood glucose levels, improve the way your body uses insulin, and help your hormones reach normal levels. Even a 10% loss in body weight (for example, a 150-pound woman losing 15 pounds) can help make your menstrual cycle more regular and improve your chances of getting pregnant 32. In overweight and obese PCOS women and girls, exercise and calorie-restrictive diets are the best first-line interventions for weight loss and impaired glucose tolerance 12.
Medicine can help regulate your menstrual cycle and reduce abnormal hair growth and acne. Birth control pills (for women not trying to have a baby) and metformin are 2 prescription medicines that are often helpful. If you have diabetes or high blood pressure, those conditions also need treatment. If you want to have a baby, there are medicines that may help you get pregnant.
The types of medicines that treat PCOS and its symptoms include:
- Hormonal birth control, including the pill, patch, shot, vaginal ring, and hormone intrauterine device (IUD). For women who don’t want to get pregnant, hormonal birth control can:
- Make your menstrual cycle more regular
- Lower your risk of endometrial cancer
- Help improve acne and reduce extra hair on the face and body. Ask your doctor about birth control with both estrogen and progesterone.
- Anti-androgen medicines. These medicines block the effect of androgens and can help reduce scalp hair loss, facial and body hair growth, and acne. They are not approved by the Food and Drug Administration (FDA) to treat PCOS symptoms. These medicines can also cause problems during pregnancy.
- Metformin. Metformin is often used to treat type 2 diabetes and may help some women with PCOS symptoms. It is not approved by the FDA to treat PCOS symptoms. Metformin improves insulin’s ability to lower your blood sugar and can lower both insulin and androgen levels. After a few months of use, metformin may help restart ovulation, but it usually has little effect on acne and extra hair on the face or body. Recent research shows that metformin may have other positive effects, including lowering body mass and improving cholesterol levels.
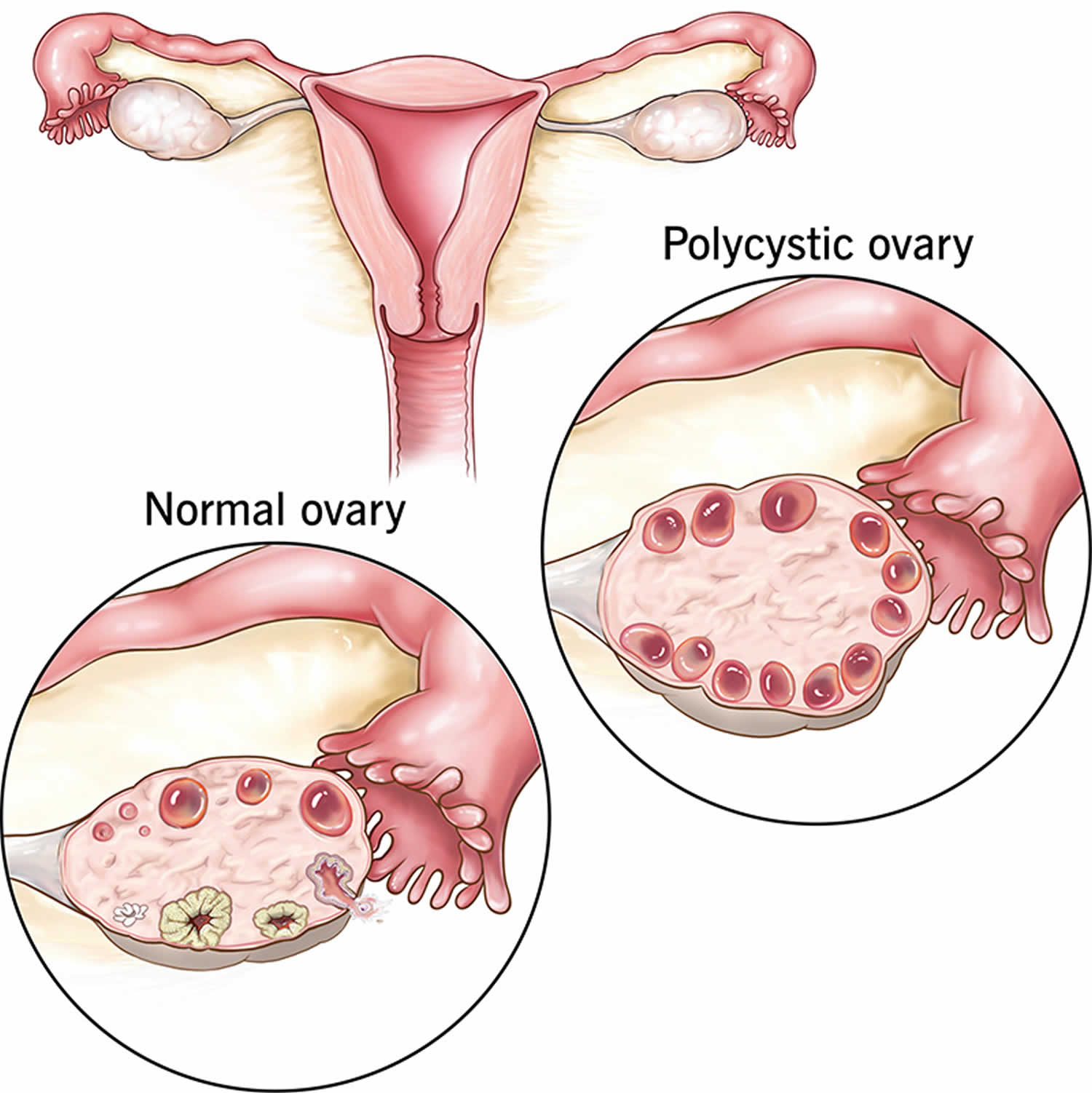
Figure 1. Polycystic ovarian syndrome
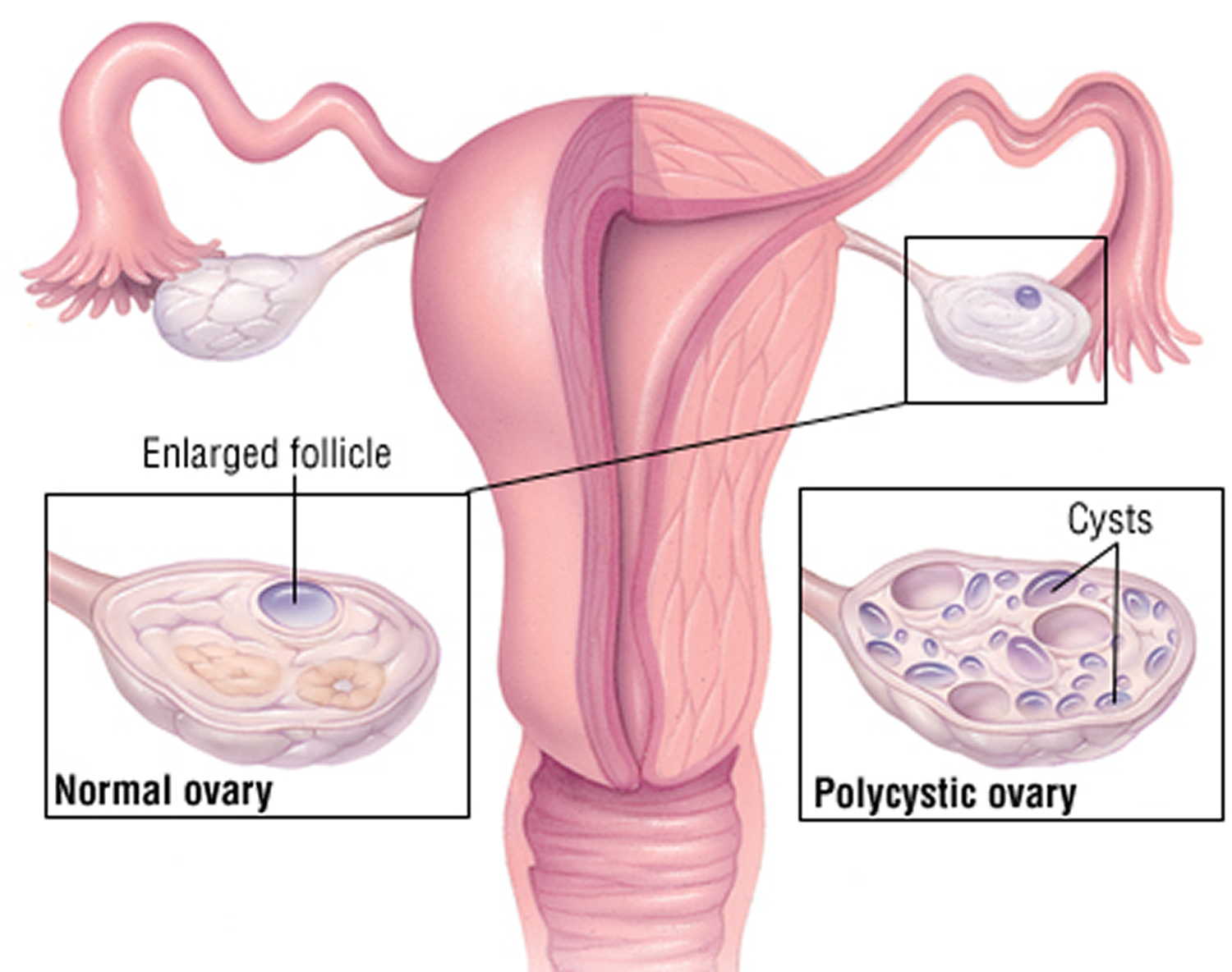
Footnote: The ovaries develop numerous small collections of fluid containing immature eggs called follicles and may fail to regularly release eggs.
Figure 2. Polycystic ovaries ultrasound – ultrasound scan of a polycystic ovary showing multiple cysts (black) that form when follicles fail to ovulate
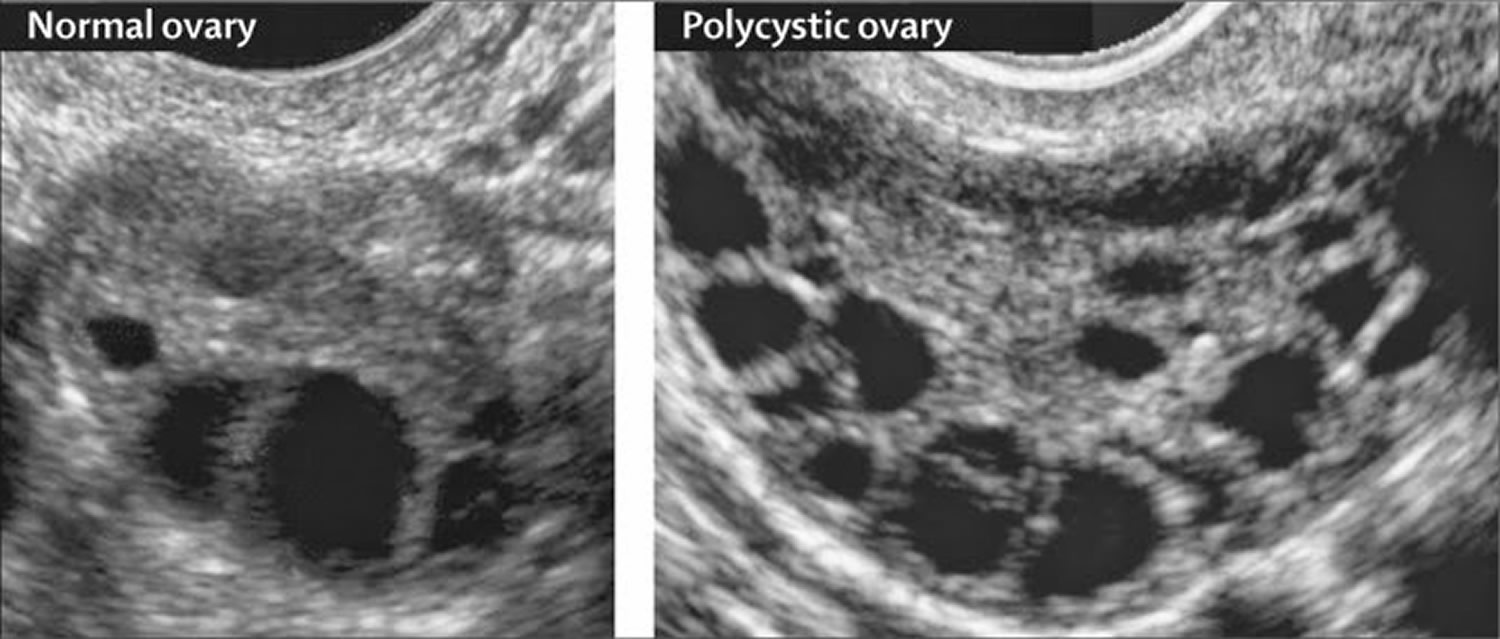
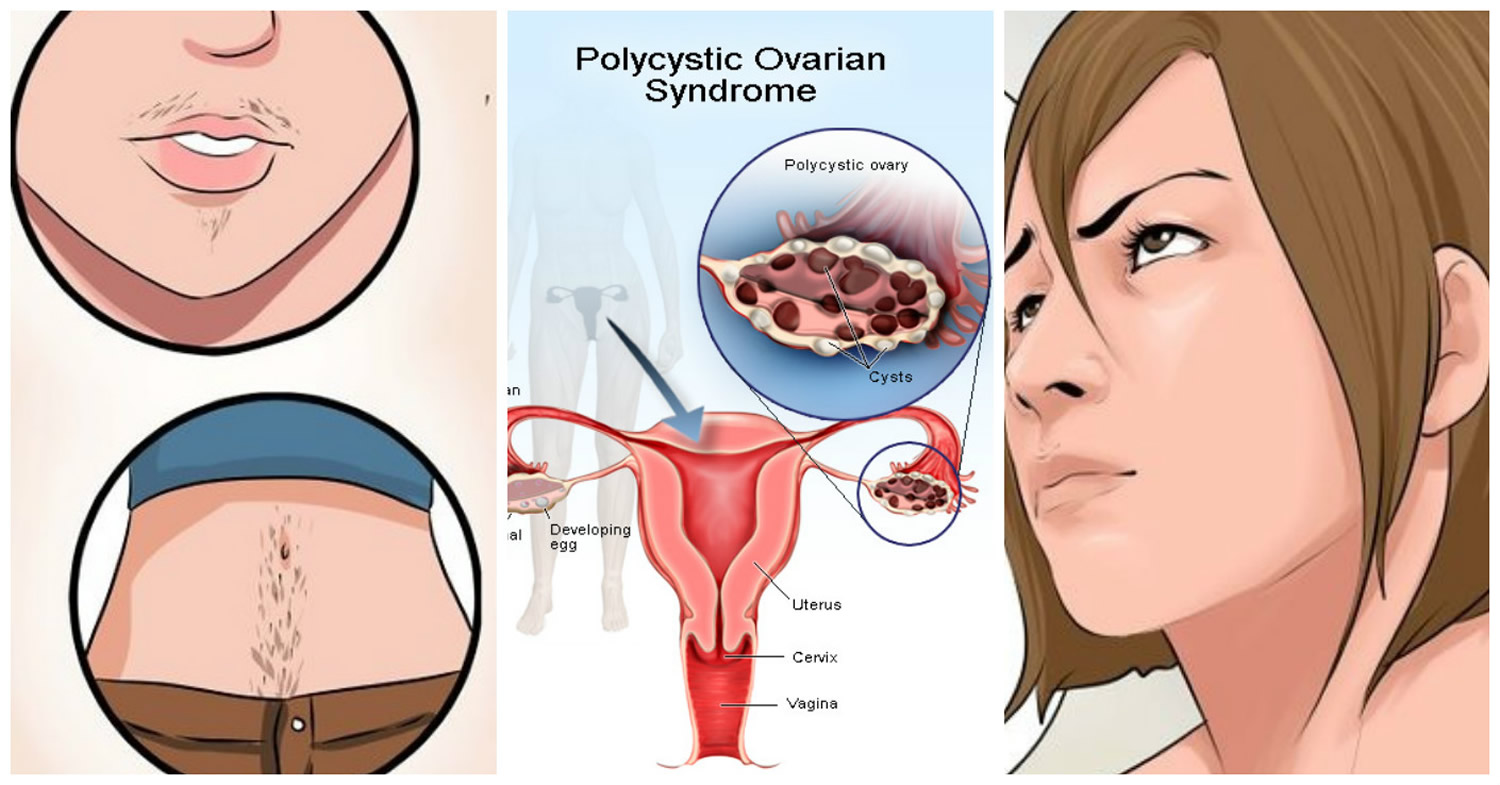
Figure 3. Polycystic Ovary Syndrome
What age does polycystic ovarian syndrome start?
Girls and women can get PCOS any time after puberty. Most women are diagnosed in their 20s or 30s when they’re trying to get pregnant. You may have a higher chance of getting PCOS if you have obesity or if other people in your family have PCOS.
Can polycystic ovarian syndrome be prevented or avoided?
There is no way to prevent polycystic ovarian syndrome. There is also no cure. However, you can manage symptoms of PCOS through lifestyle changes and medication. Talk to your doctor about how to best manage your symptoms.
Can I still get pregnant if I have PCOS?
Yes. Having PCOS does not mean you can’t get pregnant. PCOS is one of the most common, but treatable, causes of infertility in women. In women with PCOS, the hormonal imbalance interferes with the growth and release of eggs from the ovaries (ovulation). If you don’t ovulate, you can’t get pregnant. Your doctor can talk with you about ways to help you ovulate and to raise your chance of getting pregnant.
What are my treatment options for PCOS if I want to get pregnant?
You have several options to help your chances of getting pregnant if you have PCOS:
- Losing weight. If you have overweight or obesity, losing weight through healthy eating and regular physical activity can help make your menstrual cycle more regular and improve your fertility. Find a personalized healthy eating plan using the MyPlate Plan tool.
- Medicine. After ruling out other causes of infertility in you and your partner, your doctor might prescribe medicine to help you ovulate, such as clomiphene (Clomid).
- In vitro fertilization (IVF). IVF may be an option if medicine does not work. In IVF, your egg is fertilized with your partner’s sperm in a laboratory and then placed in your uterus to implant and develop. Compared to medicine alone, IVF has higher pregnancy rates and better control over your risk of having twins and triplets by allowing your doctor to transfer a single fertilized egg into your uterus.
- Surgery. Surgery is another option, usually only if the other options do not work. The outer shell called the cortex of ovaries is thickened in women with PCOS and thought to play a role in preventing spontaneous ovulation. Ovarian drilling is a surgery in which the doctor makes a few holes in the surface of your ovary using lasers or a fine needle heated with electricity. Surgery usually restores ovulation, but only for 6 to 8 months. With newer medications available, surgeons rarely perform this procedure.
How does PCOS affect pregnancy?
PCOS can cause problems during pregnancy for you and for your baby. Women with PCOS have higher rates of 33:
- Miscarriage (spontaneous abortion)
- Diabetes during pregnancy (gestational diabetes)
- High blood pressure during pregnancy (preeclampsia)
- Cesarean section (C-section)
Your baby also has a higher risk of being heavy (macrosomia) and of spending more time in a neonatal intensive care unit (NICU).
How can I prevent problems from PCOS during pregnancy?
You can lower your risk of problems during pregnancy by:
- Reaching a healthy weight before you get pregnant. Use this interactive tool to see your healthy weight before pregnancy and what to gain during pregnancy.
- Reaching healthy blood sugar levels before you get pregnant. You can do this through a combination of healthy eating habits, regular physical activity, weight loss, and medicines such as metformin.
- Taking folic acid. Talk to your doctor about how much folic acid you need.
Will PCOS symptoms go away at menopause?
Yes and no. PCOS affects many systems in your body. Many women with PCOS find that their menstrual cycles become more regular as they get closer to menopause. However, their PCOS hormonal imbalance does not change with age, so they may continue to have symptoms of PCOS. Also, the risks of PCOS-related health problems, such as type 2 diabetes, stroke, and heart attack, increase with age. These risks may be higher in women with PCOS than those without.
Does being Overweight cause polycystic ovarian syndrome?
Since its original description in 1935 by Stein and Leventhal 17, 18, obesity has been recognized as a common feature of the polycystic ovary syndrome. In the United States, some studies report that the prevalence of overweight and obesity in women with polycystic ovary syndrome is as high as 80% 34.
Reproductive disturbances are more common in obese women regardless of the diagnosis of PCOS. Obese women are more likely to have menstrual irregularity and anvolatory infertility than normal-weight women 34. In reproductive-age women, the relative risk of anovulatory infertility increases at a BMI of 24 kg/m2 and continues to rise with increasing BMI 35. Consistent with a pathophysiologic role for obesity, weight reduction can restore regular menstrual cycles in these women 34.
Despite the higher frequency of reproductive abnormalities in obese women, the majority of obese women do not develop hyperandrogenemia and do not have PCOS. In obesity increased androgen production has been reported especially in women with upper-body obesity. However, androgen clearance rates are also increased, and circulating bioavailable androgens remain in the normal range 34. In contrast, in PCOS bioavailable androgen levels are increased 36. This abnormality is further worsened by obesity, especially central obesity, since sex hormone binding globulin (SHBG), levels are reduced in this state due to hyperinsulinemia. Furthermore, PCOS is characterized by abnormalities in the gonadotropin hormone releasing hormone, or GnRH, pulse generator leading to preferential increase in luteinising hormone (LH) release over follicle stimulating hormone (FSH) 36. These abnormalities are independent of obesity. Moreover, obese reproductively normal women do not have abnormalities in 24-hour LH and FSH plasma concentrations.
Nonetheless, the prevalence of PCOS among obese reproductive-age women has not been well studied. In a recent study from Spain, PCOS was 5-fold more common among unselected premenopausal overweight or obese women seeking advice for weight loss compared to that of the general population (28.3% vs 5.5%, respectively) 37. In this study, the increased prevalence of PCOS in overweight and obese women was irrespective of the degree of obesity and was independent of the presence or absence of the metabolic syndrome or its features 37. The study demonstrates the prevalence of PCOS may be markedly increased in overweight and obese women. Routine screening by obtaining at least a menstrual history and a careful evaluation for hyperandrogenism may be indicated in these women as well.
How does obesity interact with polycystic ovarian syndrome?
Obesity has a profound effect on both natural and assisted conception, obesity influences the chance of becoming pregnant and the likelihood of a healthy pregnancy 38. Obesity is associated with increased rates of congenital anomalies (neural tube defects and cardiac defects), miscarriage, gestational diabetes, hypertension, problems during delivery, stillbirth, and maternal mortality 39. Of the 261 deaths reported between 2000 and 2002 to the UK Confidential Enquiry into Maternal Health, 78 women (35%) were obese, compared with 23% of women in the general population, and of these more than a quarter had a body mass index (BMI) >35 kg/m2 39.
Should obese women with polycystic ovarian syndrome lose weight before treatment or should they receive treatment irrespective of the possible outcome?
Several studies show that weight loss improves the endocrine profile and reproductive outcome in women with polycystic ovary syndrome 40. Even losing 5-10% of total body weight can reduce central fat by up to 30%, improve insulin sensitivity, and restore ovulation 41. Lifestyle modification is a key component of improving reproductive function in overweight anovulatory women with the syndrome 41. Treatment is harder to monitor in obese women as it is difficult to see the number of developing follicles in the ovaries; this increases the risk of multiple ovulation and multiple pregnancy 42. UK guidelines for the management of overweight women with polycystic ovary syndrome advise weight loss, preferably to a BMI of <30 kg/m2 before starting drugs for ovarian stimulation 43.
Does polycystic ovarian syndrome cause obesity?
Androgens play an important role in determination of body composition. Men have less body fat with greater distribution of fat in the upper portion of the body (android) compared to women, who tend to accumulate fat in the lower portion of the body (gynoid). Vague 44 first reported that the prevalence of diabetes, hypertension, and atherosclerosis was higher in women with android obesity compared to gynoid obesity. Moreover, he observed that the prevalence of android body habitus increases in women after the age of menopause and women with android obesity tend to have features of hyperandrogenism such as hirsutism 44. Women with upper-body obesity have also been noted to have decreased insulin sensitivity and are at higher risk for cardiovascular disease and diabetes. Independent of BMI, women with PCOS have been reported to have a high prevalence of upper-body obesity as demonstrated by increased waist circumference and waist-hip ratio compared to BMI-matched control women. Consistent with these findings, studies using dual-energy X-ray absorptiometry have revealed increased accumulation of central fat in women with PCOS 45.
Chronic exposure to higher testosterone levels in women with PCOS may modify body fat distribution in these women. Support for this hypothesis is provided by studies of androgen administration in nonobese female to male transsexuals that lead to increases in visceral fat and adversely impact insulin sensitivity 46. In post-menopausal women exposure to androgens increases visceral fat in both obese and normal-weight women 47. In rats, testosterone administration of a single high dose early in life leads to development of insulin resistance and centralization of adipose tissue mass as an adult 48. It may be that early androgen exposure adversely impacts future body fat distribution with greater accumulation of central fat.
However, few studies have examined visceral fat content in women with PCOS. Studies of isolated abdominal fat cells from women with PCOS have revealed larger-sized cells in both obese and nonobese women with PCOS compared to control women, suggesting a preferential abdominal accumulation of adipose tissue 49. Femoral adipocytes are smaller in obese women with PCOS than reproductively normal women consistent with a shift to android body fat distribution in PCOS women. These observations raise the hypothesis that hyperandrogenemia may contribute to the development of visceral adiposity in PCOS women necessitating further investigation in this area.
Lower fasting levels of the peptide hormone, ghrelin, have been reported in women with PCOS compared to weight-matched control women. Ghrelin is produced by the gastric endocrine cells and has been implicated in regulation of appetite and body weight. Ghrelin levels increase sharply before meals leading to hunger and initiation of food intake and drop after feeding leading to suppression of appetite and satiety. Fasting ghrelin levels are reported to be lower in obese individuals due to chronic positive energy balance. However, there is evidence that ghrelin homeostasis in PCOS may be dysregulated. In addition to lower fasting ghrelin levels, women with PCOS have less marked post-parandial reduction in the level of this hormone, as well as less satiety following a test meal. Lack of suppression of ghrelin following food intake may interfere with meal termination and lead to weight gain in these women 50.
Polycystic ovarian syndrome causes
The exact cause of polycystic ovarian syndrome (PCOS) is currently unknown, but may involve multitude of factors. Factors that might play a role in polycystic ovarian syndrome include 29:
- Insulin resistance. Insulin is a hormone that the pancreas makes. Insulin allows cells to use sugar (glucose), your body’s primary energy supply. If cells become resistant to the action of insulin, then blood sugar (glucose) levels can go up. This can cause your body to make more insulin to try to bring down the blood sugar level. Too much insulin (hyperinsulinemia) might cause your body to make too much of the male hormone androgen. You could have trouble with ovulation, the process where eggs are released from the ovary. One sign of insulin resistance is dark, velvety patches of skin on the lower part of the neck, armpits, groin or under the breasts called acanthosis nigricans. A bigger appetite and weight gain may be other signs. Many women with PCOS have insulin resistance, especially those who have overweight or obesity, have unhealthy eating habits, do not get enough physical activity, and have a family history of diabetes (usually type 2 diabetes). Over time, insulin resistance can lead to type 2 diabetes.
- Low-grade inflammation. White blood cells make substances in response to infection or injury. This response is called low-grade inflammation. Research shows that people with PCOS have a type of long-term, low-grade inflammation that leads polycystic ovaries to produce androgens. This can lead to heart and blood vessel problems.
- Genetics. Research suggests that certain genes might be linked to PCOS. Having a family history of PCOS may play a role in developing the condition. Several susceptible genes have been identified as contributors to the pathophysiology of polycystic ovarian syndrome. These genes are involved in various levels of steroidogenesis and androgenic pathways. Twin studies have estimated about 70% heritability. Also, the environment is a fundamental component in the expression of these genes and the development and progression of polycystic ovarian syndrome 51, 52, 53.
- Excess androgen (hyperandrogenism). With PCOS, the ovaries may produce high levels of androgen (male hormones). Having too much androgen interferes with ovulation. This means that eggs don’t develop on a regular basis and aren’t released from the follicles where they develop. Excess androgen also can result in hirsutism, male-pattern baldness and acne.
Two popular hypotheses assumed that individuals with a genetic predisposition exposed to certain environmental factors lead to the expression of PCOS features. The most common environmental factors include obesity with abdominal fat accumulation and insulin resistance. The link between obesity and the prevalence of PCOS is highly correlated; among women with body mass index (BMI) <25 kg/m², the prevalence is 4.3%, and in women with BMI > 30kg/m² it is 14%, although selection bias may play a role in assessment 54. Some hypotheses also include fetal androgen exposure 55.
Figure 4. Polycystic ovarian syndrome causes
Polycystic ovarian syndrome pathophysiology
The pathogenesis of PCOS is complex and multifactorial, including genetic, environmental, and transgenerational components 3. These sources drive the underpinnings of unbalanced hypothalamus-pituitary-ovarian axis signaling, promoting ovarian and adrenal hyperandrogenism. Nearly all causes of polycystic ovarian syndrome are due to functional ovarian hyperandrogenism 12. Two-thirds of PCOS presentations have typical functional ovarian hyperandrogenism, characterized by dysregulation of androgen secretion with an over-response of 17-hydroxyprogesterone (17-OHP) to gonadotropin stimulation 12. The remaining PCOS present with atypical functional ovarian hyperandrogenism with lack of overresponse of 17-OHP, but testosterone elevation can detect it after suppressing adrenal androgen production 12. About 3% of PCOS patients have a related isolated functional adrenal hyperandrogenism 12. The remainder of PCOS cases is mild. These lack evidence of steroid secretory abnormalities; most of these patients are obese, which scientists theorize accounts for their atypical PCOS. Specific testing for the functional ovarian hyperandrogenism subpopulation has low clinical utility in the present day 57.
Neuroendocrine disorder
Women with PCOS present with gonadotropin-releasing hormone (GnRH) neuronal network dysfunction and increased pulse amplitude for pituitary activity, shown as high serum luteinizing hormone levels and high ovarian androgen response, most likely relating to decreased responsiveness to steroid hormone negative feedback 58. Different animal models have successfully been able to recapitulate the hyperandrogenism driven neuroendocrine pathology of PCOS and other central mechanisms involved 59. Recently, aberrant neuroendocrine signaling was linked with adipose tissue dysfunction in a murine model 60, whereas other studies have proposed high anti-Müllerian hormone (AMH) promoting GnRH neuron activation and PCOS onset 61. Given the central role of hyperandrogenism and obesity in the impairments in neuronal circuitry and the high prevalence of psychological distress among women with PCOS, the central dysfunction most likely involves larger and more complex neuronal networks than previously recognized 62, 63.
Genetic factors
The genetic factors and familial clustering are described in the early PCOS literature 64; however, as more genetic data has started to accumulate, it has become obvious that polycystic ovary syndrome harbors multigenetic background. The genome-wide association studies have identified a total of 19 risk gene loci for PCOS located in the neuroendocrine, metabolic, and reproductive pathways 65, with the reproductive and metabolic populations segregating in a recent unsupervised clustering analysis 66. In line with this, Mendelian randomization analyses suggest a causal link between PCOS and variants associated with BMI, fasting insulin, menopause timing, depression, and male-pattern balding 67. From all genes of interest, the gene loci with the most potential, namely THADA, FSHR, INS-VNTR, and DENND1A, would require validation in the future. Interestingly, the clinically validated PCOS cases have similar genetic profile to the self-reported ones 67. Known genetic risk variations (alleles) account for less than 10% of PCOS heritability; therefore, other causal factors also have to be considered.
Transgenerational transmission of PCOS
Animal studies and human data show PCOS having transgenerational origins, with a 5-fold higher risk for daughters born to mothers with PCOS for inheriting the syndrome 59, 68. In a mice model, prenatal androgen excess alone can predispose to transgenerational transmission of PCOS. Early androgen exposure may increase susceptibility to polycystic ovary syndrome. Longer anogenital distance has been shown in infant girls born to PCOS mothers, and daughters of PCOS mothers have higher metabolic and androgenic risk 68, 69. Maternal testosterone in women with PCOS was found to be a predictor of infant anogenital distance 70. The mechanism through which the daughters are exposed to hyperandrogenism remains elusive, although anti-Müllerian hormone (AMH) could be one of the players. A recent study showed that mice subjected to high levels of anti-Müllerian hormone (AMH) at late pregnancy produced PCOS offspring with high luteinizing hormone pulsatility and increased androgen levels 71. The mechanism was thought to transit via anti-Müllerian hormone (AMH) effect on aromatase activity in the placenta, promoting hyperandrogenism. Even though anti-Müllerian hormone (AMH) levels have been reported to be high in the second and third trimesters in women with PCOS 71, 72, the role of anti-Müllerian hormone (AMH) on transgenerational transmission in humans warrants further studies.
Insulin Resistance
Insulin Resistance is not considered a diagnostic criterion in polycystic ovarian syndrome 73. However, it is recognized by many as a common feature in PCOS independent of obesity 74, 75. An estimated prevalence of insulin resistance among polycystic ovary syndrome patients of 60–70% has been reported 76. However, being overweight or obese is common among polycystic ovary syndrome women, affecting up to 88% of these women 77, 78, 79, therefore casting doubt on the role insulin resistance plays in the pathogenesis of polycystic ovary syndrome. Further, clinical quantification of insulin resistance is not accurate enough 80 to enable a better understanding of the role of insulin resistance in polycystic ovary syndrome pathogenesis or to incorporate it into the work up programme of polycystic ovary syndrome patients. However, it is generally acceptable that insulin resistance plays a significant role in polycystic ovary syndrome either directly or through obesity and represents a clinical concern to physicians and patients.
Polycystic ovarian syndrome symptoms
Girls and women with PCOS may have few symptoms, while others may have them all. It’s common for women to not find out they have PCOS until they are trying to get pregnant. PCOS often develops as young as age 11 or 12, around first menstrual period (menarche). Sometimes symptoms develop later after you have had periods for a while.
The symptoms of PCOS vary. The most common signs and symptoms of PCOS include:
- Irregular periods. Abnormal menstruation involves missing periods or not having a period at all. It may also involve heavy bleeding during periods.
- Abnormal hair growth. You may grow excess facial hair or experience heavy hair growth on your arms, chest and abdomen (hirsutism). This affects up to 70% of people with PCOS.
- Acne. PCOS can cause acne, especially on your back, chest and face. This acne may continue past your teenage years and may be difficult to treat.
- Obesity. Between 40% and 80% of people with PCOS have obesity and have trouble maintaining a weight that’s healthy for them.
- Darkening of the skin. You may get patches of dark skin, especially in the folds of your neck, armpits, groin (between the legs) and under your breasts. This is known as acanthosis nigricans.
- Cysts. Many people with PCOS have ovaries that appear larger or with many follicles (egg sac cysts) on ultrasound.
- Skin tags. Skin tags are little flaps of extra skin. They’re often found in your armpits or on your neck.
- Thinning hair. People with PCOS may lose patches of hair on their head or start to bald.
- Infertility. PCOS is the most common cause of infertility in women. Not ovulating regularly or frequently can result in not being able to conceive.
PCOS signs and symptoms are typically more severe in people with obesity.
Can I have PCOS but not have any symptoms?
Yes, it’s possible to have PCOS and not have any symptoms. Many women don’t even realize they have polycystic ovarian syndrome until they have trouble getting pregnant or are gaining weight for unknown reasons. It’s also possible to have mild PCOS, where the symptoms aren’t severe enough for you to notice.
Polycystic ovarian syndrome complications
Polycystic ovarian syndrome complications can include:
- Infertility
- Gestational diabetes or pregnancy-induced high blood pressure (preeclampsia)
- Miscarriage or premature birth (babies born alive before 37 weeks of pregnancy are completed)
- Nonalcoholic steatohepatitis (NASH) — a severe liver inflammation caused by fat buildup in the liver
- Metabolic syndrome — a cluster of conditions including high blood pressure, high blood sugar, and unhealthy cholesterol or triglyceride levels that significantly increase your risk of heart and blood vessel (cardiovascular) disease
- Type 2 diabetes or prediabetes
- Sleep apnea
- Venous thromboembolism 81
- Depression, anxiety and eating disorders
- Abnormal uterine bleeding
- Cancer of the uterine lining (endometrial cancer)
Obesity commonly occurs with PCOS and can worsen complications of the disorder.
High insulin levels from polycystic ovarian syndrome can lead to serious health problems, especially for women who are obese 20:
- Diabetes —more than half of women with polycystic ovarian syndrome develop type 2 diabetes by age 40
- Gestational diabetes (diabetes when pregnant)—which puts the pregnancy and baby at risk and can lead to type 2 diabetes later in life
- Heart disease —the risk of heart attack is 4 to 7 times higher compared to women the same age who don’t have PCOS
- High blood pressure —which can damage the heart, brain, and kidneys
- High LDL (“bad”) cholesterol and low HDL (“good”) cholesterol—increasing the risk for heart disease
- Stroke —plaque (cholesterol and white blood cells) clogging blood vessels can lead to blood clots that in turn can cause a stroke.
Polycystic ovarian syndrome diagnosis
If your doctor thinks you might have PCOS, they might want you to see a gynecologist or an endocrinologist for a diagnosis.
A diagnosis of PCOS is made when you have at least two of these:
- Irregular periods or missed periods. Having few menstrual periods or having periods that aren’t regular are common signs of PCOS. So is having periods that last for many days or longer than is typical for a period. For example, you might have fewer than nine periods a year. And those periods may occur more than 35 days apart. You may have trouble getting pregnant.
- Too much androgen (hyperandrogenism). High levels of the hormone androgen may result in excess facial and body hair. This is called hirsutism. Sometimes, severe acne and male-pattern baldness can happen, too.
- Polycystic ovaries. Your ovaries might be bigger. Many follicles containing immature eggs may develop around the edge of the ovary. The ovaries might not work the way they should. Many people don’t develop cysts.
There’s no single test to specifically diagnose polycystic ovary syndrome (PCOS). Your doctor is likely to start with a discussion of your symptoms, medications and any other medical conditions. Your doctor also may ask about your menstrual periods and any weight changes. A physical exam includes checking for signs of excess facial hair, hair loss, insulin resistance (discolored skin and skin tags) and acne.
Base on your symptoms, medical history and physical exam, your doctor might then recommend:
- Pelvic exam. During a pelvic exam, your doctor can check your reproductive organs for masses, growths or other changes.
- Blood tests. Blood tests can measure hormone levels. This testing can exclude possible causes of menstrual problems or androgen excess that mimic PCOS. You might have other blood testing, such as fasting cholesterol and triglyceride levels. A glucose tolerance test can measure your body’s response to sugar (glucose).
- Pelvic ultrasound. An ultrasound can check the appearance of your ovaries and the thickness of the lining of your uterus. A wandlike device (transducer) is placed in your vagina. The transducer emits sound waves that are translated into images on a computer screen.
If you have a diagnosis of PCOS, your doctor might recommend more tests for complications. These tests can include:
- Regular checks of blood pressure, glucose tolerance, and cholesterol and triglyceride levels
- Screening for depression and anxiety
- Screening for obstructive sleep apnea
Table 1. PCOS Diagnostic Features
| Feature | Definition |
|---|---|
| Irregular menstrual periods | • > 1 year and < 3 years post menarche: < 21 or > 45 days • > 3 years post menarche: < 21 or > 35 days • > 1 year post menarche: any cycle > 90 days • Primary amenorrhea at age 15 or > 3 years post thelarche |
| Biochemical hyperandrogenism | • Calculated free testosterone or free androgen index • Calculated bioavailable testosterone • Liquid chromatography/mass spectrometer with extraction is the preferred method of assay measure; reference range upper limits of normal free testosterone 1.06 ng/dL, total testosterone 60 ng/dL • Can consider androstenedione or dehydroepiandrosterone sulfate (DHEAS) if testosterone is normal and high index of suspicion for hyperandrogenism |
| Clinical hyperandrogenism | • Examination specifically for acne, alopecia, and hirsutism • For adolescents use severe acne and hirsutism • Use standardized visual scale of modified Ferriman-Gallwey ≥ 4-6 recognizing there are ethnic variations that are not well defined |
| Ultrasound criteria | • Ultrasound should be transvaginal and using high resolution • In this setting follicle count per ovary should be ≥ 20 or ovarian volume ≥ 10 mL • Ultrasound should not be used in those < 8 years post menarche |
Polycystic ovarian syndrome treatment
Polycystic ovarian syndrome treatments can include medications, lifestyle changes or a combination of both. PCOS treatment focuses on managing the things that are concerning you. This could include infertility, hirsutism, acne or obesity.
Lifestyle changes such as healthy eating habits, losing weight, regular physical activity and maintaining a body weight that’s healthy for you can help relieve PCOS-related symptoms. Losing weight may help to lower your blood glucose levels, improve the way your body uses insulin, and help your hormones reach normal levels. Even a 10% loss in body weight (for example, a 150-pound woman losing 15 pounds) can help make your menstrual cycle more regular and improve your chances of getting pregnant 32. In overweight and obese PCOS women and girls, exercise and calorie-restrictive diets are the best first-line interventions for weight loss and impaired glucose tolerance 12. Different studies have shown that hirsutism can improve as well as regulation of the menstrual cycle and ovulation. Low-carbohydrate diets have been used, hoping that these will have a better effect on hyperinsulinism, but studies have shown no difference in outcomes with low-carbohydrate diets 82, 83, 84.
If you don’t plan to become pregnant, your treatments may include:
- Hormonal birth control. Options include birth control pills, patches, shots, a vaginal ring or an intrauterine device (IUD). Hormonal birth control helps to regulate your menstrual cycle, some forms will also improve acne and help with excess hair growth.
- Insulin-sensitizing medicine. Metformin is a drug used to treat diabetes. It works by helping your body process insulin. Once insulin is under control, some people with PCOS see improvements in their menstrual cycles.
- Medications to block androgens. Some medications can block the effect of androgens. This helps control acne or hair growth. Talk to your doctor about whether such treatment is right for you.
If you want to become pregnant now or in the future, treatment for PCOS includes:
- Drugs to induce ovulation (releasing an egg). A successful pregnancy begins with ovulation. Certain drugs have been proven to induce ovulation in people with PCOS. The medications clomiphene and letrozole are taken orally, while gonadotropins are given by injection.
- In vitro fertilization (IVF). This is an option for people with PCOS when medication doesn’t help with ovulation. Your provider fertilizes your egg with your partner’s sperm in a lab before transferring it to your uterus.
- Surgery. Surgery is another option, usually only if the other options do not work. The outer shell called the cortex of ovaries is thickened in women with PCOS and thought to play a role in preventing spontaneous ovulation. Ovarian drilling is a surgery in which the doctor makes a few holes in the surface of your ovary using lasers or a fine needle heated with electricity. Surgery usually restores ovulation, but only for 6 to 8 months. With newer medications available, surgeons rarely perform this procedure.
Lifestyle changes
Obesity is frequently observed in women with PCOS, predominantly in the form of abdominal obesity, aggravating metabolic and reproductive complication as well as PCOS-associated complications 23.
Obesity can:
- increase the risk of diabetes
- cause or worsen hypertension
- raise bad cholesterol (LDL) and triglycerides, and reduce good cholesterol (HDL)
- produce substances that cause inflammation in the blood vessels, which can lead to heart disease
Your doctor may recommend weight loss through a low-calorie diet combined with moderate exercise activities. Even a modest reduction in your weight — for example, losing 5% of your body weight — might improve your condition. Losing weight may increase the effectiveness of medications your doctor recommends for PCOS, and it can help with infertility. Your doctor and a registered dietitian can work with you to determine the best weight-loss plan.
Healthy eating includes:
- A regular schedule for meals and healthy snacks.
- Smaller portion sizes.
- More high-fiber foods, such as fruits, nonstarchy vegetables and whole grains.
- Fewer refined grains, starchy vegetables and sweets.
- Modest servings of low-fat dairy, low-fat meats and fish.
- Healthy cooking oils, such as olive oil or canola oil.
- Fewer calories.
Your doctor may recommend seeing a registered dietitian, who can help you:
- Identify healthy food choices.
- Plan well-balanced, nutritional meals.
- Develop new habits and address barriers to changing habits.
- Monitor carbohydrate intake to keep your blood sugar levels more stable.
Physical activity
Exercise is important for losing weight or maintaining a healthy weight. It also helps with managing blood sugar.
- Aerobic exercise. Choose an aerobic exercise that you enjoy, such as walking, swimming, biking or running. Adults should aim for 30 minutes or more of moderate aerobic exercise on most days of the week, or at least 150 minutes a week.
- Resistance exercise. Resistance exercise increases your strength, balance and ability to perform activities of daily living more easily. Resistance training includes weightlifting, yoga and calisthenics. Adults living with type 2 diabetes should aim for 2 to 3 sessions of resistance exercise each week.
- Limit inactivity. Breaking up long periods of inactivity, such as sitting at the computer, can help control blood sugar levels. Take a few minutes to stand, walk around or do some light activity every 30 minutes.
Dietary supplements
Alpha-lipoic acid 85 and omega-3 fatty acids are two supplements that improve lipid and insulin sensitivity in women through their anti-inflammatory and antioxidant properties, although omega-3 fatty acids are high in calories 86. Studies suggest that coenzyme Q10 has beneficial effects on glucose and lipid metabolism, insulin, HOMA-IR, and total testosterone levels in women with PCOS and can also improve ovarian function 87, 88, 89. Vitamin E combined with coenzyme Q10 can improve insulin resistance and serum sex hormone binding globulin (SHBG) levels in PCOS 90, 91. Supplementation with probiotics, prebiotics, and synbiotics in women with PCOS can improve insulin resistance, protect the intestinal barrier, and regulate the immune system, lipid profile, and other metabolic disorders 92, 93.
Periods Medications
To regulate your periods, your doctor might recommend:
- Combination birth control pills. Pills that contain both estrogen and progestin decrease androgen production and regulate estrogen. Regulating your hormones can lower your risk of endometrial cancer and correct irregular bleeding, excess hair growth and acne.
- Progestin therapy. Taking progestin for 10 to 14 days every 1 to 2 months can regulate your periods and protect against endometrial cancer. This progestin therapy doesn’t improve androgen levels and won’t prevent pregnancy. The progestin-only minipill or progestin-containing intrauterine device is a better choice if you also wish to avoid pregnancy.
Hormonal birth control, either oral birth control pills, patch, or vaginal rings, is the first-line treatment for menstrual abnormalities, hirsutism, and acne 12. The Endocrine Society does not favor any choice over another. The progestin component decreases luteinizing hormone (LH) levels, indirectly decreasing ovarian androgen production and increasing sex hormone-binding globulin (SHBG). Additionally, some progestins have been shown to have direct antiandrogenic properties as a direct inhibitor 5 alpha-reductase activity to prevent the conversion of free testosterone to its more potent form, 5 alpha-dihydrotestosterone (DHT). For this reason, they are highly effective for symptoms of hyperandrogenism and controlling the menstrual cycle 12.
Screening for contraindication for hormonal contraceptives should be done in all patients. Women 35 or older who smoke more than 15 cigarettes daily, uncontrolled high blood pressure greater than 160/100, uncontrolled diabetes with severe peripheral vascular disease are considered absolute contraindications 12. The 2024 U.S. Medical Eligibility Criteria for Contraceptive Use (U.S. MEC) comprises recommendations for the use of specific contraceptive methods by persons who have certain characteristics or medical conditions. Patients with diabetes and without vascular complications do not have any contraindication to use hormonal contraceptives.
Regarding the metabolic effect of hormonal contraceptives, higher estrogen activity increases HDL (high density lipoprotein or “good”) cholesterol and decreases LDL (low density lipoprotein or “good”) cholesterol. No impact on body weight and fat distribution between PCOS and healthy women.
Oral contraceptive initial dosing of 20 mcg of ethinyl estradiol combined with a progestin with antiandrogenic properties such as desogestrel and drospirenone or with neutral effects like norethindrone acetate. Progestin with antiandrogenic properties has been shown to have a higher risk of venous thromboembolism (VTE). If hyperandrogenic symptoms are not controlled completely with this initial dose, ethinyl estradiol can be increased to 30 to 35 mcg 12.
PCOS fertility treatment
To help you ovulate so that you can become pregnant, your doctor might recommend:
- Clomiphene. This oral selective estrogen receptor modulator (SERM), competitive inhibitor of estrogen receptors (ERs) or anti-estrogen medication is taken during the first part of your menstrual cycle.
- Letrozole (Femara). This breast cancer treatment can work to stimulate the ovaries. Letrozole lowers the levels of the female sex hormone estrogen in the body.
- Metformin. Metformin is a medicine for type 2 diabetes that you take by mouth improves insulin resistance and lowers insulin levels. If you don’t become pregnant using clomiphene, your doctor might recommend adding metformin to help you ovulate. If you have prediabetes, metformin can slow the progression to type 2 diabetes and help with weight loss. The Endocrine Society recommends starting metformin in PCOS patients with type 2 diabetes or impaired glucose tolerance who fail lifestyle modifications. Metformin decreases progression from impaired glucose tolerance to type 2 diabetes. Metformin also improves menstrual cycles, abnormal waist to hip ratio, and vascular markers in non-obese women with PCOS 94.
- Metformin is also second-line therapy for menstrual irregularities in patients with a contraindication for hormonal contraceptives. It is commonly used in the adolescent girls as monotherapy, and it helps restore normal menses, weight loss, and reduce insulin resistance. Even though it should not be used primarily to treat clinical hyperandrogenism, it can mildly improve androgen excess symptoms.
- Gonadotropins. These hormone medications are given by injection.
First-line therapy for infertility in PCOS patients is clomiphene citrate 12. This is a selective estrogen receptor modulator (SERM), competitive inhibitor of estrogen receptors (ERs), and has mixed agonist and antagonist activity. Clomiphene enhances fertility and ovulation, especially by its effect on the hypothalamus, where it binds for a prolonged period to estrogen receptors (ERs) and depletes them, blocking the negative feedback inhibition effect of circulating endogenous estrogen. This results in the pulsatile release of a hypothalamic gonadotropin-releasing hormone (GnRH), promoting the secretion of follicle-stimulating hormone (FSH) and luteinizing hormone (LH) and indirectly stimulating ovulation 12.
New evidence for estrogen modulators such as letrozole (Femara) has shown that it can be used in ovulatory infertility. Letrozole (Femara) is an aromatase inhibitor that blocks estrogen synthesis, reducing negative estrogenic feedback at the pituitary. A double-blind multicenter trial reported that letrozole, compared to clomiphene, was associated with higher live-birth and ovulation rates among infertile women with polycystic ovary syndrome. For women with PCOS who are seeking pregnancy, the ovulation induction agent letrozole is associated with higher live birth rates compared with clomiphene citrate 95. However, for safety reasons additional studies regarding the ability to cause birth defects in a developing fetus (teratogenicity) need to be done, but future guidelines can change after this new evidence.
Metformin is suggested as an add-on treatment for infertility, helping prevent ovarian hyperstimulation syndrome in a patient undergoing in vitro fertilization (IVF). Metformin was shown higher benefits in obese patients. After pregnancy is confirmed, it is now allowed for patients with diabetes or glucose intolerance to continue metformin as a treatment for sugar control, but attention should be given to avoid maternal gastrointestinal disturbances (diarrhea, nausea, stomach discomfort, gas, indigestion and constipation).
If needed, talk with your doctor about procedures that may help you become pregnant. For example, in vitro fertilization (IVF) may be an option.
Acne and excessive hair growth treatment
To reduce excessive hair growth or improve acne, your doctor might recommend:
- Birth control pills. These pills decrease androgen production that can cause excessive hair growth and acne.
- Spironolactone (Aldactone). This medication blocks the effects of androgen on the skin, including excessive hair growth and acne. Spironolactone can cause birth defects, so effective birth control is needed while taking this medication. This medication isn’t recommended if you’re pregnant or planning to become pregnant.
- Eflornithine (Vaniqa). This cream can slow facial hair growth.
- Hair removal. Electrolysis and laser hair removal are two options for removing hair. Electrolysis uses a tiny needle inserted into each hair follicle. The needle sends out a pulse of electric current. The current damages and then destroys the follicle. Laser hair removal is a medical procedure that uses a concentrated beam of light to remove unwanted hair. You might need multiple treatments of electrolysis or laser hair removal. Shaving, plucking or using creams that dissolve unwanted hair may be other options. But these are temporary, and hair may thicken when it grows back.
- Acne treatments. Medications, including pills and topical creams or gels, may help improve acne. Talk to your doctor about options.
Clinical hyperandrogenism requires long-term treatment and takes several months before effects are evident.
Cosmetic interventions should be initiated while medications start working. These can be bleaching and temporary hair removal methods. You can try facial hair removal creams, laser hair removal, or electrolysis to remove excess hair. You can find hair removal creams and products at drugstores. Procedures like laser hair removal or electrolysis must be done by a doctor and may not be covered by health insurance.
Slowing hair growth. A prescription skin treatment (eflornithine HCl cream) can help slow down the growth rate of new hair in unwanted places.
First-line treatment of excessive facial hair growth (hirsutism) is low-dose or antiandrogenic oral birth control pills which effectively lowers androgens level and effect. Additionally, contraceptive properties are beneficial when combined with antiandrogenic drugs because the latter requires reliable contraception as they are highly teratogenic. Mild hirsutism can be treated oral birth control pills alone.
Medication interventions include topical eflornithine (Vaniqa) for face hirsutism, which can be an expensive treatment with potentially serious side effects if the body absorbs it.
Add-on antiandrogen administration can be done for moderate, severe hirsutism and mild hirsutism without adequate hair growth control after 6 months to 1 year of oral birth control pills. As those drugs have similar effectiveness, the PCOS Society suggest prescribing finasteride, cyproterone acetate, which is not available in the United States, or spironolactone, instead of flutamide when an antiandrogen is needed, due to potential side effects like liver damage. They act by blocking androgens effects over the hair follicle; finasteride also has inhibition of 5 alpha-reductase the enzyme that converts testosterone to dihydrotestosterone (DHT) 96.
Spironolactone is the most common add-on anti-androgen medication prescribed after oral birth control pills; it is a nonselective mineralocorticoid receptor antagonist and suppresses testosterone levels. Spironolactone also has additional benefits regarding the risk of cardiovascular disease compared to oral birth control pills. Combinations of spironolactone with metformin were superior to monotherapy with either drug regarding improved menstrual cycles, glucose during oral glucose tolerance tests (OGTT) and testosterone levels 97, 98.
Metformin alone or other insulin sensitizers are not considered target treatment for hirsutism due to no consistent evidence showing superior effect than placebo 99, 100.
Diabetes medications
Medicines for type 2 diabetes include the following.
Metformin is generally the first medicine prescribed for type 2 diabetes. It works mainly by lowering glucose production in the liver and improving the body’s sensitivity to insulin so it uses insulin more effectively. Some people experience vitamin B-12 deficiency while taking metformin and may need to take supplements. Other possible side effects, which may improve over time, include:
- Nausea.
- Abdominal pain.
- Bloating.
- Diarrhea.
Dipeptidyl peptidase-4 (DPP-4) inhibitors decrease the degradation of incretins, therefore, increasing glucose-dependent insulin release to help reduce blood sugar levels but tend to have a very modest effect. Examples include sitagliptin (Januvia), saxagliptin (Onglyza) and linagliptin (Tradjenta). In patients with type 2 diabetes, DPP4 inhibitors are considered weight neutral. New data suggest that in obese women with PCOS, DPP4 inhibitors have beneficial effects in weight loss and lower blood glucose levels. It prevented weight gain in women who were transitioning from GLP-1 agonists. Evidence suggests that the effect of DPP4 inhibitors on the weight of women with PCOS is based on increasing growth hormone, which is reduced in patients with PCOS. These, in turn, decrease visceral fat mass. Data is still limited, and it is considered experimental 101.
Possible side effects DPP4 inhibitors are:
- Risk of pancreatitis.
- Joint pain.
Sodium-glucose co-transporter-2 (SGLT2) inhibitors affect the blood-filtering functions in your kidneys by blocking the return of glucose to the bloodstream. As a result, glucose is removed in the urine. SGLT2 inhibitors increase urinary glucose secretion, improves weight loss and cardiovascular risk in patients with type 2 diabetes. These medicines may reduce the risk of heart attack and stroke in people with a high risk of those conditions. Examples include canagliflozin (Invokana), dapagliflozin (Farxiga) and empagliflozin (Jardiance). Limited data in obese patients shows promising data for weight loss and fat mass reduction with treatment with SGLT2 inhibitors compared to metformin, but its effect on hormonal and metabolic parameters was similar. More data is needed to implement this medication in clinical practice 102. Possible side effects of SGLT2 inhibitors include:
- Vaginal yeast infections.
- Urinary tract infections.
- Low blood pressure.
- High cholesterol.
- Risk of gangrene.
- Risk of bone fractures (canagliflozin).
- Risk of amputation (canagliflozin).
Thiazolidinediones also called “glitazones” are insulin sensitizers that act on intracellular metabolic pathways to enhance insulin action and increase insulin sensitivity in critical tissues 103. Thiazolidinediones also increase adiponectin levels, decrease hepatic gluconeogenesis, and increase insulin-dependent glucose uptake in muscle and fat 104. Adiponectin, a cytokine secreted by fat tissue, increases insulin sensitivity, and fatty acid oxidation increases with thiazolidinedione therapy 105, 106, 107. There are two thiazolidinediones, rosiglitazone, and pioglitazone, currently approved by the FDA as monotherapy or combined with metformin or sulfonylureas to manage type 2 diabetes mellitus. Thiazolidinediones workn by regulating gene expression through binding to peroxisome proliferator-activated receptor-gamma (PPARγ), a nuclear transcription regulator 106. Peroxisome proliferator-activated receptors (PPARs) are a family of ligand-activated transcription factors of nuclear hormone receptors that regulate energy homeostasis. The genes activated by the PPAR-gamma (PPARγ) subtype are present in muscle, fat, and liver, regulating glucose metabolism, fatty acid storage, and adipocyte differentiation 108. The binding of thiazolidinedione will induce a conformational change to alter gene expression of numerous pathways involved in metabolism regulation, including lipoprotein lipase, glucokinase, fatty acyl-CoA synthase, and others 109. PPAR-gamma agonists improve insulin resistance by increasing adiponectin, GLUT4 expression, and opposing the effect of TNF-alpha in adipocytes. Increased GLUT 4 expression will increase glucose uptake in adipocytes and skeletal muscle cells in response to insulin 108. In PCOS, PPAR-gamma (PPARγ) agonist treatment improved hormonal and metabolic outcomes but had an adverse effect on weight. It can be superior in patients with nonalcoholic fatty liver disease (NAFLD) compared to metformin 110.
Myoinositol. Myoinositol is an over-the-counter food supplement that increases insulin sensitivity. Compared with placebo improved insulin sensitivity in women with PCOS without significant effect on BMI (body mass index). Data is limited, and its use has been mostly applied as fertility treatment of PCOS or when metformin is not tolerated, given it has fewer gastrointestinal side effects 111.
Other medicines your doctor might prescribe in addition to diabetes medications include blood pressure and cholesterol-lowering medicines, to help prevent heart and blood vessel disease.
Surgical interventions
Surgical interventions can sometimes relieve PCOS-related symptoms. Weight loss surgery (bariatric surgery) is an effective treatment for obesity and PCOS symptoms after all other treatment options have failed and it should be offered to severely obese patients 112. Weight loss surgery (bariatric surgery) risks include surgical and dietary complications and pregnancy should not be pursued during the 12 months following the surgery.
Laparoscopic ovarian drilling is a procedure in which ovarian tissue is destroyed with a laser beam or with a surgical needle using minimally invasive laparoscopic techniques, aiming to rebalance and improve ovarian function in PCOS 3. The procedure is not commonly used, but it has remained as an option in cases of clomiphene citrate–resistant ovaries and when letrozole is not an option due to off-label use. However, the recent Cochrane Review summarized that although reducing the number of multiple pregnancies and the risk for ovarian hyperstimulation syndrome, laparoscopic ovarian drilling may actually decrease the live birth rate in women with anovulatory PCOS and clomiphene citrate resistance compared with medical ovulation induction alone 113. Furthemore, laparoscopic ovarian drilling also subjects women to the risks associated with surgery, such as complications from anesthesia, infection, and adhesions.
Living with polycystic ovarian syndrome
If you have PCOS, you are more likely to develop high blood pressure, high cholesterol, or type 2 diabetes. This means you have a greater risk for stroke and heart attacks. It is important to work with your doctor on a health plan to minimize these risks.
Problems with menstrual periods may also cause women who have PCOS to be infertile (unable to get pregnant). PCOS also causes you to have a higher risk for cancer of the uterus (endometrial cancer) or breast (breast cancer) 114, 115. You should see your doctor regularly for health screenings.
Women who have PCOS are also more likely to have anxiety or depression. If you are feeling anxious or depressed, talk to your doctor. Treatment is available.
Polycystic ovarian syndrome prognosis
Women with PCOS report poorer health status than non-PCOS counterparts 116. PCOS is associated with an increased risk of metabolic complications starting from a young age. These medical conditions in addition to PCOS include cardiovascular disease (CVD) risk factors such as obesity, impaired glucose tolerance, type 2 diabetes, dyslipidemia, and hypertension 3.
Studies have found links between PCOS and other health problems:
- Type 2 diabetes. More than half of women with PCOS will have type 2 diabetes or prediabetes (glucose intolerance) before the age of 40 117.
- High blood pressure. Women with PCOS are at greater risk of having high blood pressure compared with women of the same age without PCOS. High blood pressure is a leading cause of heart disease and stroke.
- High cholesterol. Women with PCOS often have higher levels of LDL (bad) cholesterol and low levels of HDL (good) cholesterol. High cholesterol raises your risk of heart disease and stroke.
- Sleep apnea. This is when momentary and repeated stops in breathing interrupt sleep. Many women with PCOS have overweight or obesity, which can cause sleep apnea. Sleep apnea raises your risk of heart disease and diabetes.
- Depression and anxiety. Depression and anxiety are common among women with PCOS.
- Endometrial cancer. Problems with ovulation, obesity, insulin resistance, and diabetes (all common in women with PCOS) increase the risk of developing cancer of the endometrium (lining of the uterus or womb).
Researchers do not know if PCOS causes some of these problems, if these problems cause PCOS, or if there are other conditions that cause PCOS and other health problems.
Obesity is one of the most common concerns expressed in surveys of patients with PCOS 118. The obesity rate varies from 50% to 80%. According to an examination of high-quality studies in a large meta-analysis, the risk of obesity in women with PCOS was reported to be 4-fold higher compared with controls and also higher in white women compared with Asian women 119. The increased preference for abdominal fat deposition, seen primarily in the hyperandrogenic polycystic ovary syndrome, further predisposes this population to other cardiometabolic complications 120.
The risk of impaired glucose tolerance is 3-fold higher with PCOS, independent of body mass index (BMI), and highest in women living in Asia and in North and South America 121. Although the risk of type 2 diabetes is also increased in this reproductive-age population, there are mixed data regarding these findings independent of weight. In women over age 40, a few longitudinal studies and other cross-sectional studies indicate an increased risk of type 2 diabetes independent of body mass index (BMI) 122. In adolescent girls with PCOS, there are only a few small studies examining the risk of type 2 diabetes, and these show an overall low prevalence 123.
Hyperlipidemia or dyslipidemia reflected by high triglycerides and low high-density lipoprotein (HDL) cholesterol, is the commonest metabolic abnormality detected in PCOS 124. High low-density lipoprotein (LDL or “bad”) cholesterol levels and a decrease in high-density lipoprotein (HDL or “good”) cholesterol increases cardiovascular disease risk 125.
The association between hypertension and PCOS is mixed. Most studies do not demonstrate a higher risk of hypertension independent of body mass index (BMI), although longitudinal data demonstrate elevated blood pressure even in lean women with PCOS 126. The few studies in adolescent girls and older women do not show significant differences compared with control groups 127.
Reproductive-age women with PCOS have a 2-fold increased risk of metabolic syndrome 128. More importantly, in adolescent girls with PCOS, the risk of metabolic syndrome is at least 2-fold higher than in girls without PCOS 129.
Women with PCOS are at an increased risk of endometrial hyperplasia and infertility related to anovulation 3. Premenopausal women with PCOS may have a 4-fold increased risk of endometrial cancer 130. For women with PCOS who are seeking pregnancy, the ovulation induction agent letrozole is associated with higher live birth rates compared with clomiphene citrate 95. Use of metformin in conjunction with these medications may improve the ovulation rate in a subpopulation of obese women. Depending on the ethnicity and study population assessed the obesity rate varies from 50% to 80% 131. Metformin, on the other hand, has not been shown to reduce the risk of gestational diabetes; thus, its use should be limited to prior to pregnancy for metabolic management and to facilitate weight loss. Once pregnant, women with PCOS are at an increased risk of miscarriage, gestational diabetes, pregnancy-induced hypertension, and preeclampsia 132.
Endometrial cancer
Recent interest in the long term risks of PCOS has also focused on its possible associations with endometrial cancer. Prolonged anovulation which characterizes the syndrome is considered to be the main mechanism responsible for continual unopposed secretion of oestrogens and consequent increased risk of endometrial carcinoma 133. The known factors which increase the risk of developing endometrial cancer are obesity, longterm use of unopposed oestrogens, nulliparity, infertility, hypertention and diabetes 134, 135. Most of these factors are known also to be associated with PCOS. Endometrial hyperplasia may be a precursor to adenocarcinoma. A precise estimate rate of pregression is practically impossible to be determined, but it estimated that 18% of cases of adenomatous hyperplasia will progress to cancer in the following 2 to 10 years. In women with PCOS intervals between menstruation of more than three months may be associated with endometrial hyperplasia and later carcinoma 133. Evidence from a big study in which 1270 women with chronic anovulation participated, the excess risk of endometrial cancer was identified to be 3.1 136. However a more recent appraisal of the evidence for association between PCOS and endometrial cancer was inconclusive 137. The true risk of endometrial carcinoma in women diagnosed with PCOS has not been clearly defined yet.
Ovarian cancer
There has been much debate and concerns about the risk of ovarian cancer in women with anovulation, particularly because of the extend use of drugs for induction of ovulation to these patients. Several lines of evidence might suggest that there is a connection between PCOS and increased risk of ovarian cancer. The risk appears to be increased in nulliparous women (multiple ovulations), with early menarche and late menopause. Without any evidence based data to support this theory, it may be that inducing multiple ovulations in women with infertility will increase their risk. So, although women with PCOS are expected to be in low risk groups for developing ovarian cancer due to their life time reduced ovulation rate, by using ovulation induction treatments and inducing multifollicular ovulations theoretically an imbalance to their risk for ovarian cancer will be technically created
There are only a few studies addressing the possibility of association of polycystic ovaries and ovarian cancer with conflicting evidence. Large Danish studies suggest that infertility on its own increases the risk of borderline and invasive ovarian tumors 138, 139. Another study linking clomiphene and ovarian cancer suggests that the relative risk for ovarian cancer for women with PCOS is 4.1 compared to controls 140. The large UK study though concludes that the standardized mortality rate for ovarian cancer is only 0.39 141. Even more recent evidence about association between polycystic ovarian syndrome and ovarian malignancy are still conflicting but generally reassuring 142.
Breast cancer
Obesity, hyperandrogenism and infertility are features known to be associated with the development of breast cancer. However studies failed to show any significant increase in the risk of developing breast cancer in women with PCOS 141. On the other hand though, it seems that there is a positive association between PCOS and the presence of family history of breast cancer. In a study of 217 women the proportion of women with positive family history of breast cancer was significantly higher in women with PCOS compared with controls 143.
- Yadav S, Delau O, Bonner AJ, Markovic D, Patterson W, Ottey S, Buyalos RP, Azziz R. Direct economic burden of mental health disorders associated with polycystic ovary syndrome: Systematic review and meta-analysis. Elife. 2023 Aug 3;12:e85338. doi: 10.7554/eLife.85338[↩][↩]
- Zhao H, Zhang J, Cheng X, Nie X, He B. Insulin resistance in polycystic ovary syndrome across various tissues: an updated review of pathogenesis, evaluation, and treatment. J Ovarian Res. 2023 Jan 11;16(1):9. doi: 10.1186/s13048-022-01091-0[↩][↩]
- Kathleen M Hoeger, Anuja Dokras, Terhi Piltonen, Update on PCOS: Consequences, Challenges, and Guiding Treatment, The Journal of Clinical Endocrinology & Metabolism, Volume 106, Issue 3, March 2021, Pages e1071–e1083, https://doi.org/10.1210/clinem/dgaa839[↩][↩][↩][↩][↩]
- Zawadzki J, Dunaif A. Diagnostic criteria for polycystic ovary syndrome: towards a rational approach. In: Dunaif A, Givens HR, Haseltine FP, Merriam GR, ed. Polycystic Ovary Syndrome. Boston, MA: Blackwell Scientific; 1992:377–384.[↩]
- Diamanti-Kandarakis E, Kouli CR, Bergiele AT, Filandra FA, Tsianateli TC, Spina GG, Zapanti ED, Bartzis MI. A survey of the polycystic ovary syndrome in the Greek island of Lesbos: hormonal and metabolic profile. J Clin Endocrinol Metab. 1999 Nov;84(11):4006-11. doi: 10.1210/jcem.84.11.6148[↩]
- Diamanti-Kandarakis E, Dunaif A. New perspectives in polycystic ovary syndrome. Trends Endocrinol Metab. 1996 Oct;7(8):267-71. doi: 10.1016/s1043-2760(96)00125-7[↩]
- Dapas M, Lin F, Nadkarni G, Sisk R, Legro R, Urbanek M, et al. Distinct subtypes of polycystic ovary syndrome with novel genetic associations: an unsupervised, phenotypic clustering analysis. PLoS Med. 2020;17(6):e1003132. doi: 10.1371/journal.pmed.1003132[↩]
- Bozdag G, Mumusoglu S, Zengin D, Karabulut E, Yildiz B. The prevalence and phenotypic features of polycystic ovary syndrome: a systematic review and meta-analysis. Hum Reprod (Oxford, England) 2016;31(12):2841–2855. doi: 10.1093/humrep/dew218[↩]
- Azziz R, Carmina E, Dewailly D, Diamanti-Kandarakis E, Escobar-Morreale H, Futterweit W, et al. Positions statement: criteria for defining polycystic ovary syndrome as a predominantly hyperandrogenic syndrome: an Androgen Excess Society guideline. J Clin Endocrinol Metab. 2006;91(11):4237–4245. doi: 10.1210/jc.2006-0178[↩]
- The Rotterdam ESHRE/ASRM-sponsored PCOS consensus workshop groxup Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome (PCOS) Hum Reprod (Oxford, England) 2004;19(1):41–47. doi: 10.1093/humrep/deh098[↩]
- Zawadzki JK, Dunaif A. Diagnostic criteria for polycystic ovary syndrome: towards a rational approach. Boston. 1992;77–84.[↩]
- Rasquin LI, Anastasopoulou C, Mayrin JV. Polycystic Ovarian Disease. [Updated 2022 Nov 15]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK459251[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Anagnostis P, Tarlatzis BC, Kauffman RP. Polycystic ovarian syndrome (PCOS): Long-term metabolic consequences. Metabolism. 2018;86:33–43. 10.1016/j.metabol.2017.09.016[↩]
- Raperport C, Homburg R. The Source of Polycystic Ovarian Syndrome. Clin Med Insights Reprod Health. 2019;13:1179558119871467. 10.1177/1179558119871467[↩]
- Knochenhauer E. S., Key T. J., Kahsar-Miller M., Waggoner W., Boots L. R., Azziz R. Prevalence of the polycystic ovary syndrome in unselected black and white women of the southeastern United States: a prospective study. Journal of Clinical Endocrinology and Metabolism . 1998;83:3078–3082. doi: 10.1210/jc.83.9.3078[↩][↩]
- Riestenberg C, Jagasia A, Markovic D, Buyalos RP, Azziz R. Health care-related economic burden of polycystic ovary syndrome in the United States: pregnancy-related and long-term health consequences. The Journal of Clinical Endocrinology and Metabolism. 2022;107:575–585. doi: 10.1210/clinem/dgab613[↩]
- The Stein-Leventhal syndrome. LEVENTHAL ML. Am J Obstet Gynecol. 1958 Oct; 76(4):825-38. https://www.ncbi.nlm.nih.gov/pubmed/13583027/[↩][↩]
- Stein I.F., Leventhal M. (1935) Amenorrhoea associated with bilateral polycystic ovaries. Am J Obstet Gynecol 29: 181–191.[↩][↩]
- National Center for Biotechnology Information. The effect of a healthy lifestyle for women with polycystic ovary syndrome. https://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0014488/[↩]
- Centers for Disease Control and Prevention. PCOS and Diabetes, Heart Disease, Stroke. https://www.cdc.gov/diabetes/library/spotlights/pcos.html[↩][↩]
- International evidence-based guideline for the assessment and management of polycystic ovary syndrome. Copyright Monash University, Melbourne Australia 2018. https://www.monash.edu/__data/assets/pdf_file/0004/1412644/PCOS_Evidence-Based-Guidelines_20181009.pdf[↩][↩]
- Moore AM, Prescott M, Marshall CJ, Yip SH, Campbell RE. Enhancement of a robust arcuate GABAergic input to gonadotropin-releasing hormone neurons in a model of polycystic ovarian syndrome. Proc Natl Acad Sci U S A. 2015;112(2):596–601. 10.1073/pnas.1415038112[↩]
- Dadachanji R, Patil A, Joshi B, Mukherjee S. Elucidating the impact of obesity on hormonal and metabolic perturbations in polycystic ovary syndrome phenotypes in Indian women. PLoS One. 2021;16(2):e0246862. 10.1371/journal.pone.0246862[↩][↩]
- Diabetes and Polycystic Ovary Syndrome (PCOS). https://www.cdc.gov/diabetes/risk-factors/pcos-polycystic-ovary-syndrome.html[↩]
- Chaudhari AP, Mazumdar K, Mehta PD. Anxiety, Depression, and Quality of Life in Women with Polycystic Ovarian Syndrome. Indian J Psychol Med. 2018 May-Jun;40(3):239-246. doi: 10.4103/IJPSYM.IJPSYM_561_17[↩]
- Azziz R, Carmina E, Chen Z, Dunaif A, Laven JSE, Legro RS, Lizneva D, Natterson-Horowtiz B, Teede HJ, Yildiz BO. Polycystic ovary syndrome. Nature Reviews. Disease Primers. 2016;2:16057. doi: 10.1038/nrdp.2016.57[↩]
- Xita N, Georgiou I, Tsatsoulis A. The genetic basis of polycystic ovary syndrome. Eur J Endocrinol. 2002 Dec;147(6):717-25. doi: 10.1530/eje.0.1470717[↩]
- Diamanti-Kandarakis E, Kandarakis H, Legro RS. The role of genes and environment in the etiology of PCOS. Endocrine. 2006 Aug;30(1):19-26. doi: 10.1385/ENDO:30:1:19[↩][↩][↩]
- Dumesic DA, Abbott DH, Sanchita S, Chazenbalk GD. Endocrine-Metabolic Dysfunction in Polycystic Ovary Syndrome: an Evolutionary Perspective. Curr Opin Endocr Metab Res. 2020 Jun;12:41-48. doi: 10.1016/j.coemr.2020.02.013[↩][↩][↩]
- Goodman, N. F., Cobin, R. H., Futterweit, W., Glueck, J. S., Legro, R. S., & Carmina, E. (2015). American Association of Clinical Endocrinologists, American College of Endocrinology, and Androgen Excess and PCOS Society disease state clinical review: guide to the best practices in the evaluation and treatment of polycystic ovary syndrome – part 1. Endocrine Practice, 11, 1291–300. doi: 10.4158/EP15748.DSC[↩]
- Shannon M, Wang Y. Polycystic ovary syndrome: a common but often unrecognized condition. J Midwifery Womens Health. 2012 May-Jun;57(3):221-30. doi: 10.1111/j.1542-2011.2012.00161.x[↩]
- Polycystic Ovary Syndrome (PCOS). https://www.acog.org/womens-health/faqs/Polycystic-Ovary-Syndrome-PCOS[↩][↩]
- Boomsma CM, Fauser BC, Macklon NS. Pregnancy complications in women with polycystic ovary syndrome. Semin Reprod Med. 2008 Jan;26(1):72-84. doi: 10.1055/s-2007-992927[↩]
- Sam S. Obesity and Polycystic Ovary Syndrome. Obesity management. 2007;3(2):69-73. doi:10.1089/obe.2007.0019. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2861983/[↩][↩][↩][↩]
- Physical activity, body mass index, and ovulatory disorder infertility. Rich-Edwards JW, Spiegelman D, Garland M, Hertzmark E, Hunter DJ, Colditz GA, Willett WC, Wand H, Manson JE. Epidemiology. 2002 Mar; 13(2):184-90. https://www.ncbi.nlm.nih.gov/pubmed/11880759/[↩]
- Polycystic ovary syndrome: syndrome XX ? Sam S, Dunaif A. Trends Endocrinol Metab. 2003 Oct; 14(8):365-70. https://www.ncbi.nlm.nih.gov/pubmed/14516934/[↩][↩]
- Prevalence and characteristics of the polycystic ovary syndrome in overweight and obese women. Alvarez-Blasco F, Botella-Carretero JI, San Millán JL, Escobar-Morreale HF. Arch Intern Med. 2006 Oct 23; 166(19):2081-6. https://www.ncbi.nlm.nih.gov/pubmed/17060537/[↩][↩]
- Should obese women with polycystic ovary syndrome receive treatment for infertility ? Balen AH, Dresner M, Scott EM, Drife JO. BMJ. 2006 Feb 25; 332(7539):434-5. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1382524/[↩]
- Lewis G, ed. Why mothers die 2000-2002 London: Confidential Enquiry into Maternal and Child Health, 2004.[↩][↩]
- Improving reproductive performance in overweight/obese women with effective weight management. Norman RJ, Noakes M, Wu R, Davies MJ, Moran L, Wang JX. Hum Reprod Update. 2004 May-Jun; 10(3):267-80. https://www.ncbi.nlm.nih.gov/pubmed/15140873/[↩]
- National Institute for Clinical Excellence. Fertility assessment and treatment for people with fertility problems. A clinical guideline. London: RCOG Press, 2004.[↩][↩]
- Balen AH, Dresner M, Scott EM, Drife JO. Should obese women with polycystic ovary syndrome receive treatment for infertility?: Given the risks such women will face in pregnancy, they should lose weight first. BMJ : British Medical Journal. 2006;332(7539):434-435. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1382524/[↩]
- Balen AH. PCOS, obesity and reproductive function: RCOG Special Study Group on Obesity. 2007. London: RCOG Press.[↩]
- The degree of masculine differentiation of obesities: a factor determining predisposition to diabetes, atherosclerosis, gout, and uric calculous disease. VAGUE J. Am J Clin Nutr. 1956 Jan-Feb; 4(1):20-34. https://www.ncbi.nlm.nih.gov/pubmed/13282851/[↩][↩]
- Body fat distribution in women with polycystic ovary syndrome. Douchi T, Ijuin H, Nakamura S, Oki T, Yamamoto S, Nagata Y. Obstet Gynecol. 1995 Oct; 86(4 Pt 1):516-9. https://www.ncbi.nlm.nih.gov/pubmed/7675372/[↩]
- Long-term testosterone administration increases visceral fat in female to male transsexuals. Elbers JM, Asscheman H, Seidell JC, Megens JA, Gooren LJ. J Clin Endocrinol Metab. 1997 Jul; 82(7):2044-7. https://www.ncbi.nlm.nih.gov/pubmed/9215270/[↩]
- Ovarian and adrenal function in polycystic ovary syndrome. Rosenfield RL. Endocrinol Metab Clin North Am. 1999 Jun; 28(2):265-93. https://www.ncbi.nlm.nih.gov/pubmed/10352919/[↩]
- Imprinting of female offspring with testosterone results in insulin resistance and changes in body fat distribution at adult age in rats. Nilsson C, Niklasson M, Eriksson E, Björntorp P, Holmäng A. J Clin Invest. 1998 Jan 1; 101(1):74-8. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC508542/[↩]
- Evidence for distinctive and intrinsic defects in insulin action in polycystic ovary syndrome. Dunaif A, Segal KR, Shelley DR, Green G, Dobrjansky A, Licholai T. Diabetes. 1992 Oct; 41(10):1257-66. https://www.ncbi.nlm.nih.gov/pubmed/1397698/[↩]
- Ghrelin and measures of satiety are altered in polycystic ovary syndrome but not differentially affected by diet composition. Moran LJ, Noakes M, Clifton PM, Wittert GA, Tomlinson L, Galletly C, Luscombe ND, Norman RJ. J Clin Endocrinol Metab. 2004 Jul; 89(7):3337-44. https://www.ncbi.nlm.nih.gov/pubmed/15240612/[↩]
- Goyal A, Ganie MA. Idiopathic Hyperprolactinemia Presenting as Polycystic Ovary Syndrome in Identical Twin Sisters: A Case Report and Literature Review. Cureus. 2018 Jul 19;10(7):e3004. doi: 10.7759/cureus.3004[↩]
- Albu D, Albu A. The relationship between anti-Müllerian hormone serum level and body mass index in a large cohort of infertile patients. Endocrine. 2019 Jan;63(1):157-163. doi: 10.1007/s12020-018-1756-4[↩]
- Spinedi E, Cardinali DP. The Polycystic Ovary Syndrome and the Metabolic Syndrome: A Possible Chronobiotic-Cytoprotective Adjuvant Therapy. Int J Endocrinol. 2018 Jul 25;2018:1349868. doi: 10.1155/2018/1349868[↩]
- Teede HJ, Joham AE, Paul E, Moran LJ, Loxton D, Jolley D, Lombard C. Longitudinal weight gain in women identified with polycystic ovary syndrome: results of an observational study in young women. Obesity (Silver Spring). 2013 Aug;21(8):1526-32. doi: 10.1002/oby.20213[↩]
- Puttabyatappa M, Padmanabhan V. Ovarian and Extra-Ovarian Mediators in the Development of Polycystic Ovary Syndrome. J Mol Endocrinol. 2018 Oct 16;61(4):R161-R184. doi: 10.1530/JME-18-0079[↩]
- Balkrishna A, Rana M, Mishra S, Srivastava D, Bhardwaj R, Singh S, Rajput SK, Arya V. Incredible Combination of Lifestyle Modification and Herbal Remedies for Polycystic Ovarian Syndrome Management. Evid Based Complement Alternat Med. 2023 Jun 20;2023:3705508. doi: 10.1155/2023/3705508[↩]
- Carvalho LML, Dos Reis FM, Candido AL, Nunes FFC, Ferreira CN, Gomes KB. Polycystic Ovary Syndrome as a systemic disease with multiple molecular pathways: a narrative review. Endocr Regul. 2018 Oct 1;52(4):208-221. doi: 10.2478/enr-2018-0026[↩]
- Eagleson CA, Gingrich MB, Pastor CL, Arora TK, Burt CM, Evans WS, Marshall JC. Polycystic ovarian syndrome: evidence that flutamide restores sensitivity of the gonadotropin-releasing hormone pulse generator to inhibition by estradiol and progesterone. J Clin Endocrinol Metab. 2000 Nov;85(11):4047-52. doi: 10.1210/jcem.85.11.6992[↩]
- Stener-Victorin E, Padmanabhan V, Walters KA, Campbell RE, Benrick A, Giacobini P, Dumesic DA, Abbott DH. Animal Models to Understand the Etiology and Pathophysiology of Polycystic Ovary Syndrome. Endocr Rev. 2020 Jul 1;41(4):bnaa010. doi: 10.1210/endrev/bnaa010[↩][↩]
- Cox MJ, Edwards MC, Rodriguez Paris V, Aflatounian A, Ledger WL, Gilchrist RB, Padmanabhan V, Handelsman DJ, Walters KA. Androgen Action in Adipose Tissue and the Brain are Key Mediators in the Development of PCOS Traits in a Mouse Model. Endocrinology. 2020 Jul 1;161(7):bqaa061. doi: 10.1210/endocr/bqaa061[↩]
- Cimino I, Casoni F, Liu X, Messina A, Parkash J, Jamin SP, Catteau-Jonard S, Collier F, Baroncini M, Dewailly D, Pigny P, Prescott M, Campbell R, Herbison AE, Prevot V, Giacobini P. Novel role for anti-Müllerian hormone in the regulation of GnRH neuron excitability and hormone secretion. Nat Commun. 2016 Jan 12;7:10055. doi: 10.1038/ncomms10055[↩]
- Hatanaka Y, Kabuta T, Wada K. Disturbance in Maternal Environment Leads to Abnormal Synaptic Instability during Neuronal Circuitry Development. Front Neurosci. 2017 Feb 6;11:35. doi: 10.3389/fnins.2017.00035[↩]
- Coyle C, Campbell RE. Pathological pulses in PCOS. Mol Cell Endocrinol. 2019 Dec 1;498:110561. doi: 10.1016/j.mce.2019.110561[↩]
- Legro RS. The genetics of polycystic ovary syndrome. Am J Med. 1995 Jan 16;98(1A):9S-16S. doi: 10.1016/s0002-9343(99)80053-9[↩]
- Hiam D, Moreno-Asso A, Teede HJ, Laven JSE, Stepto NK, Moran LJ, Gibson-Helm M. The Genetics of Polycystic Ovary Syndrome: An Overview of Candidate Gene Systematic Reviews and Genome-Wide Association Studies. J Clin Med. 2019 Oct 3;8(10):1606. doi: 10.3390/jcm8101606[↩]
- Dapas M, Lin FTJ, Nadkarni GN, Sisk R, Legro RS, Urbanek M, Hayes MG, Dunaif A. Distinct subtypes of polycystic ovary syndrome with novel genetic associations: An unsupervised, phenotypic clustering analysis. PLoS Med. 2020 Jun 23;17(6):e1003132. doi: 10.1371/journal.pmed.1003132[↩]
- Day F, Karaderi T, Jones MR, et al. Large-scale genome-wide meta-analysis of polycystic ovary syndrome suggests shared genetic architecture for different diagnosis criteria. PLoS Genet. 2018 Dec 19;14(12):e1007813. doi: 10.1371/journal.pgen.1007813. Erratum in: PLoS Genet. 2019 Dec 5;15(12):e1008517. doi: 10.1371/journal.pgen.1008517[↩][↩]
- Risal S, Pei Y, Lu H, Manti M, Fornes R, Pui HP, Zhao Z, Massart J, Ohlsson C, Lindgren E, Crisosto N, Maliqueo M, Echiburú B, Ladrón de Guevara A, Sir-Petermann T, Larsson H, Rosenqvist MA, Cesta CE, Benrick A, Deng Q, Stener-Victorin E. Prenatal androgen exposure and transgenerational susceptibility to polycystic ovary syndrome. Nat Med. 2019 Dec;25(12):1894-1904. doi: 10.1038/s41591-019-0666-1[↩][↩]
- Barrett ES, Hoeger KM, Sathyanarayana S, Abbott DH, Redmon JB, Nguyen RHN, Swan SH. Anogenital distance in newborn daughters of women with polycystic ovary syndrome indicates fetal testosterone exposure. J Dev Orig Health Dis. 2018 Jun;9(3):307-314. doi: 10.1017/S2040174417001118[↩]
- Glintborg D, Jensen RC, Schmedes AV, Brandslund I, Kyhl HB, Jensen TK, Andersen MS. Anogenital distance in children born of mothers with polycystic ovary syndrome: the Odense Child Cohort. Hum Reprod. 2019 Oct 2;34(10):2061-2070. doi: 10.1093/humrep/dez122. Erratum in: Hum Reprod. 2020 Jan 1;35(1):254. doi: 10.1093/humrep/dez237[↩]
- Tata B, Mimouni NEH, Barbotin AL, Malone SA, Loyens A, Pigny P, Dewailly D, Catteau-Jonard S, Sundström-Poromaa I, Piltonen TT, Dal Bello F, Medana C, Prevot V, Clasadonte J, Giacobini P. Elevated prenatal anti-Müllerian hormone reprograms the fetus and induces polycystic ovary syndrome in adulthood. Nat Med. 2018 Jun;24(6):834-846. doi: 10.1038/s41591-018-0035-5[↩][↩]
- Piltonen TT, Giacobini P, Edvinsson Å, Hustad S, Lager S, Morin-Papunen L, Tapanainen JS, Sundström-Poromaa I, Arffman RK. Circulating antimüllerian hormone and steroid hormone levels remain high in pregnant women with polycystic ovary syndrome at term. Fertil Steril. 2019 Mar;111(3):588-596.e1. doi: 10.1016/j.fertnstert.2018.11.028[↩]
- Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome (PCOS). Rotterdam ESHRE/ASRM-Sponsored PCOS consensus workshop group. Hum Reprod. 2004 Jan; 19(1):41-7. https://www.ncbi.nlm.nih.gov/pubmed/14688154/[↩]
- Steroid secretion in polycystic ovarian disease after ovarian suppression by a long-acting gonadotropin-releasing hormone agonist. Chang RJ, Laufer LR, Meldrum DR, DeFazio J, Lu JK, Vale WW, Rivier JE, Judd HL. J Clin Endocrinol Metab. 1983 May; 56(5):897-903. https://www.ncbi.nlm.nih.gov/pubmed/6403570/[↩]
- Characterization of groups of hyperandrogenic women with acanthosis nigricans, impaired glucose tolerance, and/or hyperinsulinemia. Dunaif A, Graf M, Mandeli J, Laumas V, Dobrjansky A. J Clin Endocrinol Metab. 1987 Sep; 65(3):499-507. https://www.ncbi.nlm.nih.gov/pubmed/3305551/[↩]
- Prevalence of insulin resistance in the polycystic ovary syndrome using the homeostasis model assessment. DeUgarte CM, Bartolucci AA, Azziz R. Fertil Steril. 2005 May; 83(5):1454-60. https://www.ncbi.nlm.nih.gov/pubmed/15866584/[↩]
- Restored insulin sensitivity but persistently increased early insulin secretion after weight loss in obese women with polycystic ovary syndrome. Holte J, Bergh T, Berne C, Wide L, Lithell H. J Clin Endocrinol Metab. 1995 Sep; 80(9):2586-93. https://www.ncbi.nlm.nih.gov/pubmed/7673399/[↩]
- The impact of obesity on hyperandrogenism and polycystic ovary syndrome in premenopausal women. Pasquali R, Casimirri F. Clin Endocrinol (Oxf). 1993 Jul; 39(1):1-16. https://www.ncbi.nlm.nih.gov/pubmed/8348699/[↩]
- Improvement in endocrine and ovarian function during dietary treatment of obese women with polycystic ovary syndrome. Kiddy DS, Hamilton-Fairley D, Bush A, Short F, Anyaoku V, Reed MJ, Franks S. Clin Endocrinol (Oxf). 1992 Jan; 36(1):105-11. https://www.ncbi.nlm.nih.gov/pubmed/1559293/[↩]
- Detecting insulin resistance in polycystic ovary syndrome: purposes and pitfalls. Legro RS, Castracane VD, Kauffman RP. Obstet Gynecol Surv. 2004 Feb; 59(2):141-54. https://www.ncbi.nlm.nih.gov/pubmed/14752302/[↩]
- Is polycystic ovary syndrome another risk factor for venous thromboembolism ? United States, 2003–2008. Am J Obstet Gynecol. 2012; 207(5):377.e1-377.e8. http://dx.doi.org/10.1016/j.ajog.2012.08.007[↩]
- Norman RJ, Teede HJ. A new evidence-based guideline for assessment and management of polycystic ovary syndrome. Med J Aust. 2018 Sep 1;209(7):299-300. doi: 10.5694/mja18.00635[↩]
- Tay CT, Moran LJ, Wijeyaratne CN, Redman LM, Norman RJ, Teede HJ, Joham AE. Integrated Model of Care for Polycystic Ovary Syndrome. Semin Reprod Med. 2018 Jan;36(1):86-94. doi: 10.1055/s-0038-1667310[↩]
- Htet T, Cassar S, Boyle JA, Kuczynska-Burggraf M, Gibson-Helm M, Chiu WL, Stepto NK, Moran LJ. Informing Translation: The Accuracy of Information on Websites for Lifestyle Management of Polycystic Ovary Syndrome. Semin Reprod Med. 2018 Jan;36(1):80-85. doi: 10.1055/s-0038-1667309[↩]
- Laganà AS, Monti N, Fedeli V, Gullo G, Bizzarri M. Does Alpha-lipoic acid improve effects on polycystic ovary syndrome? Eur Rev Med Pharmacol Sci. 2022 Feb;26(4):1241-1247. doi: 10.26355/eurrev_202202_28116[↩]
- Iervolino M, Lepore E, Forte G, Laganà A, Buzzaccarini G, Unfer V. Natural molecules in the management of Polycystic Ovary Syndrome (PCOS): an analytical review. Nutrients. 2021;13(5):1677. doi: 10.3390/nu13051677[↩]
- Özcan P, Fıçıcıoğlu C, Kizilkale O, Yesiladali M, Tok O, Ozkan F, et al. Can Coenzyme Q10 supplementation protect the ovarian reserve against oxidative damage? J Assist Reprod Genet. 2016;33(9):1223–1230. doi: 10.1007/s10815-016-0751-z[↩]
- Rahmani E, Jamilian M, Samimi M, Zarezade Mehrizi M, Aghadavod E, Akbari E, et al. The effects of coenzyme Q10 supplementation on gene expression related to insulin, lipid and inflammation in patients with polycystic ovary syndrome. Gynecol Endocrinol. 2018;34(3):217–222. doi: 10.1080/09513590.2017.1381680[↩]
- Samimi M, Zarezade Mehrizi M, Foroozanfard F, Akbari H, Jamilian M, Ahmadi S, et al. The effects of coenzyme Q10 supplementation on glucose metabolism and lipid profiles in women with polycystic ovary syndrome: a randomized, double-blind, placebo-controlled trial. Clin Endocrinol. 2017;86(4):560–566. doi: 10.1111/cen.13288[↩]
- Tefagh G, Payab M, Qorbani M, Sharifi F, Sharifi Y, Ebrahimnegad Shirvani M, et al. Effect of vitamin E supplementation on cardiometabolic risk factors, inflammatory and oxidative markers and hormonal functions in PCOS (polycystic ovary syndrome): a systematic review and meta-analysis. Sci Rep. 2022;12(1):5770. doi: 10.1038/s41598-022-09082-3[↩]
- Izadi A, Ebrahimi S, Shirazi S, Taghizadeh S, Parizad M, Farzadi L, Gargari BP. Hormonal and Metabolic Effects of Coenzyme Q10 and/or Vitamin E in Patients With Polycystic Ovary Syndrome. J Clin Endocrinol Metab. 2019 Feb 1;104(2):319-327. doi: 10.1210/jc.2018-01221[↩]
- Ahmadi S, Jamilian M, Karamali M, Tajabadi-Ebrahimi M, Jafari P, Taghizadeh M, et al. Probiotic supplementation and the effects on weight loss, glycaemia and lipid profiles in women with polycystic ovary syndrome: a randomized, double-blind, placebo-controlled trial. Hum Fertil (Camb) 2017;20(4):254–261. doi: 10.1080/14647273.2017.1283446[↩]
- Li Y, Tan Y, Xia G, Shuai J. Effects of probiotics, prebiotics, and synbiotics on polycystic ovary syndrome: a systematic review and meta-analysis. Crit Rev Food Sci Nutr. 2023;63(4):522-538. doi: 10.1080/10408398.2021.1951155[↩]
- Glintborg D, Altinok ML, Mumm H, Hermann AP, Ravn P, Andersen M. Body composition is improved during 12 months’ treatment with metformin alone or combined with oral contraceptives compared with treatment with oral contraceptives in polycystic ovary syndrome. J Clin Endocrinol Metab. 2014 Jul;99(7):2584-91. doi: 10.1210/jc.2014-1135[↩]
- Franik S, Eltrop SM, Kremer JA, Kiesel L, Farquhar C. Aromatase inhibitors (letrozole) for subfertile women with polycystic ovary syndrome. Cochrane Database Syst Rev. 2018 May 24;5(5):CD010287. doi: 10.1002/14651858.CD010287.pub3. Update in: Cochrane Database Syst Rev. 2022 Sep 27;9:CD010287. doi: 10.1002/14651858.CD010287.pub4[↩][↩]
- Zito PM, Bistas KG, Patel P, et al. Finasteride. [Updated 2024 Feb 28]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK513329[↩]
- Glintborg D, Andersen M. Medical comorbidity in polycystic ovary syndrome with special focus on cardiometabolic, autoimmune, hepatic and cancer diseases: an updated review. Curr Opin Obstet Gynecol. 2017 Dec;29(6):390-396. doi: 10.1097/GCO.0000000000000410[↩]
- Ganie MA, Khurana ML, Nisar S, Shah PA, Shah ZA, Kulshrestha B, Gupta N, Zargar MA, Wani TA, Mudasir S, Mir FA, Taing S. Improved efficacy of low-dose spironolactone and metformin combination than either drug alone in the management of women with polycystic ovary syndrome (PCOS): a six-month, open-label randomized study. J Clin Endocrinol Metab. 2013 Sep;98(9):3599-607. doi: 10.1210/jc.2013-1040[↩]
- Teede HJ, Misso ML, Costello MF, Dokras A, Laven J, Moran L, Piltonen T, Norman RJ; International PCOS Network. Recommendations from the international evidence-based guideline for the assessment and management of polycystic ovary syndrome. Clin Endocrinol (Oxf). 2018 Sep;89(3):251-268. doi: 10.1111/cen.13795[↩]
- Teede HJ, Misso ML, Costello MF, Dokras A, Laven J, Moran L, Piltonen T, Norman RJ; International PCOS Network. Recommendations from the international evidence-based guideline for the assessment and management of polycystic ovary syndrome. Fertil Steril. 2018 Aug;110(3):364-379. doi: 10.1016/j.fertnstert.2018.05.004[↩]
- Devin JK, Nian H, Celedonio JE, Wright P, Brown NJ. Sitagliptin Decreases Visceral Fat and Blood Glucose in Women With Polycystic Ovarian Syndrome. J Clin Endocrinol Metab. 2020 Jan 1;105(1):136–51. doi: 10.1210/clinem/dgz028[↩]
- Javed Z, Papageorgiou M, Deshmukh H, Rigby AS, Qamar U, Abbas J, Khan AY, Kilpatrick ES, Atkin SL, Sathyapalan T. Effects of empagliflozin on metabolic parameters in polycystic ovary syndrome: A randomized controlled study. Clin Endocrinol (Oxf). 2019 Jun;90(6):805-813. doi: 10.1111/cen.13968[↩]
- Yamanouchi T. Concomitant therapy with pioglitazone and insulin for the treatment of type 2 diabetes. Vasc Health Risk Manag. 2010 Apr 15;6:189-97. doi: 10.2147/vhrm.s5838[↩]
- Eggleton JS, Jialal I. Thiazolidinediones. [Updated 2023 Feb 20]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK551656[↩]
- Yau H, Rivera K, Lomonaco R, Cusi K. The future of thiazolidinedione therapy in the management of type 2 diabetes mellitus. Curr Diab Rep. 2013 Jun;13(3):329-41. doi: 10.1007/s11892-013-0378-8[↩]
- Vieira R, Souto SB, Sánchez-López E, Machado AL, Severino P, Jose S, Santini A, Fortuna A, García ML, Silva AM, Souto EB. Sugar-Lowering Drugs for Type 2 Diabetes Mellitus and Metabolic Syndrome-Review of Classical and New Compounds: Part-I. Pharmaceuticals (Basel). 2019 Oct 10;12(4):152. doi: 10.3390/ph12040152[↩][↩]
- Gor D, Gerber BS, Walton SM, Lee TA, Nutescu EA, Touchette DR. Antidiabetic drug use trends in patients with type 2 diabetes mellitus and chronic kidney disease: A cross-sectional analysis of the National Health and Nutrition Examination Survey. J Diabetes. 2020 May;12(5):385-395. doi: 10.1111/1753-0407.13003[↩]
- Tyagi S, Gupta P, Saini AS, Kaushal C, Sharma S. The peroxisome proliferator-activated receptor: A family of nuclear receptors role in various diseases. J Adv Pharm Technol Res. 2011 Oct;2(4):236-40. doi: 10.4103/2231-4040.90879[↩][↩]
- Choi SS, Park J, Choi JH. Revisiting PPARγ as a target for the treatment of metabolic disorders. BMB Rep. 2014 Nov;47(11):599-608. doi: 10.5483/bmbrep.2014.47.11.174[↩]
- Tay CT, Joham AE, Hiam DS, Gadalla MA, Pundir J, Thangaratinam S, Teede HJ, Moran LJ. Pharmacological and surgical treatment of nonreproductive outcomes in polycystic ovary syndrome: An overview of systematic reviews. Clin Endocrinol (Oxf). 2018 Nov;89(5):535-553. doi: 10.1111/cen.13753[↩]
- Zeng L, Yang K. Effectiveness of myoinositol for polycystic ovary syndrome: a systematic review and meta-analysis. Endocrine. 2018 Jan;59(1):30-38. doi: 10.1007/s12020-017-1442-y[↩]
- Ortiz-Flores AE, Luque-Ramírez M, Escobar-Morreale HF. Pharmacotherapeutic management of comorbid polycystic ovary syndrome and diabetes. Expert Opin Pharmacother. 2018 Dec;19(17):1915-1926. doi: 10.1080/14656566.2018.1528231[↩]
- Bordewijk EM, Ng KYB, Rakic L, Mol BWJ, Brown J, Crawford TJ, van Wely M. Laparoscopic ovarian drilling for ovulation induction in women with anovulatory polycystic ovary syndrome. Cochrane Database Syst Rev. 2020 Feb 11;2(2):CD001122. doi: 10.1002/14651858.CD001122.pub5[↩]
- Armeni E, Lambrinoudaki I. Cardiovascular Risk in Postmenopausal Women with Polycystic Ovary Syndrome. Curr Vasc Pharmacol. 2019;17(6):579-590. doi: 10.2174/1570161116666180828154006[↩]
- Neven ACH, Laven J, Teede HJ, Boyle JA. A Summary on Polycystic Ovary Syndrome: Diagnostic Criteria, Prevalence, Clinical Manifestations, and Management According to the Latest International Guidelines. Semin Reprod Med. 2018 Jan;36(1):5-12. doi: 10.1055/s-0038-1668085[↩]
- Karjula S, Morin-Papunen L, Franks S, Auvinen J, Järvelin MR, Tapanainen JS, Jokelainen J, Miettunen J, Piltonen TT. Population-based Data at Ages 31 and 46 Show Decreased HRQoL and Life Satisfaction in Women with PCOS Symptoms. J Clin Endocrinol Metab. 2020 Jun 1;105(6):1814–26. doi: 10.1210/clinem/dgz256[↩]
- Lorenz LB, Wild RA. Polycystic ovarian syndrome: an evidence-based approach to evaluation and management of diabetes and cardiovascular risks for today’s clinician. Clin Obstet Gynecol. 2007 Mar;50(1):226-43. doi: 10.1097/GRF.0b013e31802f5197[↩]
- Gibson-Helm M, Teede H, Dunaif A, Dokras A. Delayed Diagnosis and a Lack of Information Associated With Dissatisfaction in Women With Polycystic Ovary Syndrome. J Clin Endocrinol Metab. 2017 Feb 1;102(2):604-612. doi: 10.1210/jc.2016-2963[↩]
- Lim SS, Davies MJ, Norman RJ, Moran LJ. Overweight, obesity and central obesity in women with polycystic ovary syndrome: a systematic review and meta-analysis. Hum Reprod Update. 2012 Nov-Dec;18(6):618-37. doi: 10.1093/humupd/dms030[↩]
- Daan NM, Louwers YV, Koster MP, Eijkemans MJ, de Rijke YB, Lentjes EW, Fauser BC, Laven JS. Cardiovascular and metabolic profiles amongst different polycystic ovary syndrome phenotypes: who is really at risk? Fertil Steril. 2014 Nov;102(5):1444-1451.e3. doi: 10.1016/j.fertnstert.2014.08.001[↩]
- Kakoly NS, Khomami MB, Joham AE, Cooray SD, Misso ML, Norman RJ, Harrison CL, Ranasinha S, Teede HJ, Moran LJ. Ethnicity, obesity and the prevalence of impaired glucose tolerance and type 2 diabetes in PCOS: a systematic review and meta-regression. Hum Reprod Update. 2018 Jul 1;24(4):455-467. doi: 10.1093/humupd/dmy007[↩]
- Cooney LG, Dokras A. Beyond fertility: polycystic ovary syndrome and long-term health. Fertil Steril. 2018 Oct;110(5):794-809. doi: 10.1016/j.fertnstert.2018.08.021[↩]
- Li H, Li L, Gu J, Li Y, Chen X, Yang D. Should All Women with Polycystic Ovary Syndrome Be Screened for Metabolic Parameters?: A Hospital-Based Observational Study. PLoS One. 2016 Nov 30;11(11):e0167036. doi: 10.1371/journal.pone.0167036. Erratum in: PLoS One. 2017 Apr 26;12(4):e0176806. doi: 10.1371/journal.pone.0176806[↩]
- Wild RA, Rizzo M, Clifton S, Carmina E. Lipid levels in polycystic ovary syndrome: systematic review and meta-analysis. Fertil Steril. 2011 Mar 1;95(3):1073-9.e1-11. doi: 10.1016/j.fertnstert.2010.12.027[↩]
- Roe A, Hillman J, Butts S, Smith M, Rader D, Playford M, Mehta NN, Dokras A. Decreased cholesterol efflux capacity and atherogenic lipid profile in young women with PCOS. J Clin Endocrinol Metab. 2014 May;99(5):E841-7. doi: 10.1210/jc.2013-3918[↩]
- Ollila ME, Kaikkonen K, Järvelin MR, Huikuri HV, Tapanainen JS, Franks S, Piltonen TT, Morin-Papunen L. Self-Reported Polycystic Ovary Syndrome Is Associated With Hypertension: A Northern Finland Birth Cohort 1966 Study. J Clin Endocrinol Metab. 2019 Apr 1;104(4):1221-1231. doi: 10.1210/jc.2018-00570[↩]
- Amiri M, Ramezani Tehrani F, Behboudi-Gandevani S, Bidhendi-Yarandi R, Carmina E. Risk of hypertension in women with polycystic ovary syndrome: a systematic review, meta-analysis and meta-regression. Reprod Biol Endocrinol. 2020 Mar 17;18(1):23. doi: 10.1186/s12958-020-00576-1[↩]
- Behboudi-Gandevani S, Amiri M, Bidhendi Yarandi R, Noroozzadeh M, Farahmand M, Rostami Dovom M, Ramezani Tehrani F. The risk of metabolic syndrome in polycystic ovary syndrome: A systematic review and meta-analysis. Clin Endocrinol (Oxf). 2018 Feb;88(2):169-184. doi: 10.1111/cen.13477[↩]
- Fazleen NE, Whittaker M, Mamun A. Risk of metabolic syndrome in adolescents with polycystic ovarian syndrome: A systematic review and meta-analysis. Diabetes Metab Syndr. 2018 Nov;12(6):1083-1090. doi: 10.1016/j.dsx.2018.03.014[↩]
- Barry JA, Azizia MM, Hardiman PJ. Risk of endometrial, ovarian and breast cancer in women with polycystic ovary syndrome: a systematic review and meta-analysis. Hum Reprod Update. 2014 Sep-Oct;20(5):748-58. doi: 10.1093/humupd/dmu012[↩]
- Wang R, Li W, Bordewijk EM, Legro RS, et al. Reproductive Medicine Network+; International Ovulation Induction IPDMA Collaboration. First-line ovulation induction for polycystic ovary syndrome: an individual participant data meta-analysis. Hum Reprod Update. 2019 Nov 5;25(6):717-732. doi: 10.1093/humupd/dmz029[↩]
- Bahri Khomami M, Joham AE, Boyle JA, Piltonen T, Silagy M, Arora C, Misso ML, Teede HJ, Moran LJ. Increased maternal pregnancy complications in polycystic ovary syndrome appear to be independent of obesity-A systematic review, meta-analysis, and meta-regression. Obes Rev. 2019 May;20(5):659-674. doi: 10.1111/obr.12829[↩]
- Ultrasound and menstrual history in predicting endometrial hyperplasia in polycystic ovary syndrome. Cheung AP. Obstet Gynecol. 2001 Aug; 98(2):325-31. https://www.ncbi.nlm.nih.gov/pubmed/11506853/[↩][↩]
- The role of obesity in the increased prevalence of obstructive sleep apnea syndrome in patients with polycystic ovarian syndrome. Gopal M, Duntley S, Uhles M, Attarian H. Sleep Med. 2002 Sep; 3(5):401-4. https://www.ncbi.nlm.nih.gov/pubmed/14592171/[↩]
- Long-term health consequences of PCOS. Wild RA. Hum Reprod Update. 2002 May-Jun; 8(3):231-41. https://www.ncbi.nlm.nih.gov/pubmed/12078834/[↩]
- Balen A, Rajkhowa R. Health consequences of polycystic ovary syndrome. In: Balen A, editor. Reproductive endocrinology for the MRCOG and beyond. 1st ed. London: RCOG press; 2003. pp. 99–107.[↩]
- Polycystic ovary syndrome and endometrial carcinoma. Hardiman P, Pillay OC, Atiomo W. Lancet. 2003 May 24; 361(9371):1810-2. https://www.ncbi.nlm.nih.gov/pubmed/12781553/[↩]
- Infertility, fertility drugs, and invasive ovarian cancer: a case-control study. Mosgaard BJ, Lidegaard O, Kjaer SK, Schou G, Andersen AN. Fertil Steril. 1997 Jun; 67(6):1005-12. https://www.ncbi.nlm.nih.gov/pubmed/9176436/[↩]
- Ovarian stimulation and borderline ovarian tumors: a case-control study. Mosgaard BJ, Lidegaard O, Kjaer SK, Schou G, Andersen AN. Fertil Steril. 1998 Dec; 70(6):1049-55. https://www.ncbi.nlm.nih.gov/pubmed/9848294/[↩]
- Ovarian tumors in a cohort of infertile women. Rossing MA, Daling JR, Weiss NS, Moore DE, Self SG. N Engl J Med. 1994 Sep 22; 331(12):771-6. http://www.nejm.org/doi/full/10.1056/NEJM199409223311204[↩]
- Mortality of women with polycystic ovary syndrome at long-term follow-up. Pierpoint T, McKeigue PM, Isaacs AJ, Wild SH, Jacobs HS. J Clin Epidemiol. 1998 Jul; 51(7):581-6. https://www.ncbi.nlm.nih.gov/pubmed/9674665/[↩][↩]
- Polycystic ovary syndrome and gynecological cancers: is there a link ? Gadducci A, Gargini A, Palla E, Fanucchi A, Genazzani AR. Gynecol Endocrinol. 2005 Apr; 20(4):200-8. https://www.ncbi.nlm.nih.gov/pubmed/16019362/[↩]
- Familial associations in women with polycystic ovary syndrome. Atiomo WU, El-Mahdi E, Hardiman P. Fertil Steril. 2003 Jul; 80(1):143-5. https://www.ncbi.nlm.nih.gov/pubmed/12849816/[↩]





{kind=link}