
Contents
What is Prader Willi syndrome
Prader-Willi syndrome is a rare and complex genetic condition that affects many parts of the body that results in a number of physical, mental and behavioral problems. In infancy, Prader-Willi syndrome is characterized by weak muscle tone (hypotonia), feeding difficulties, poor growth, and delayed development. Beginning in childhood, affected individuals develop an insatiable appetite, which leads to chronic overeating (hyperphagia) and obesity. Some people with Prader-Willi syndrome, particularly those with obesity, also develop type 2 diabetes (the most common form of diabetes).
Prader-Willi syndrome was first described in 1956 by Drs. Prader, Labhart, and Willi.
Prader-Willi syndrome affects males and females in equal numbers and occurs in all ethnic groups and geographic regions in the world. Most estimates place the incidence between 1 in 10,000-30,000 individuals in the general population worldwide.
Signs and symptoms of Prader-Willi syndrome can vary among individuals. Symptoms may slowly change over time from childhood to adulthood. People with Prader-Willi syndrome typically have mild to moderate intellectual impairment and learning disabilities. Behavioral problems are common, including temper outbursts, stubbornness, and compulsive behavior such as picking at the skin. Sleep abnormalities can also occur. Additional features of this condition include distinctive facial features such as a narrow forehead, almond-shaped eyes, and a triangular mouth; short stature; and small hands and feet. Some people with Prader-Willi syndrome have unusually fair skin and light-colored hair. Both affected males and affected females have underdeveloped genitals. Puberty is delayed or incomplete, and most affected individuals are unable to have children (infertile).
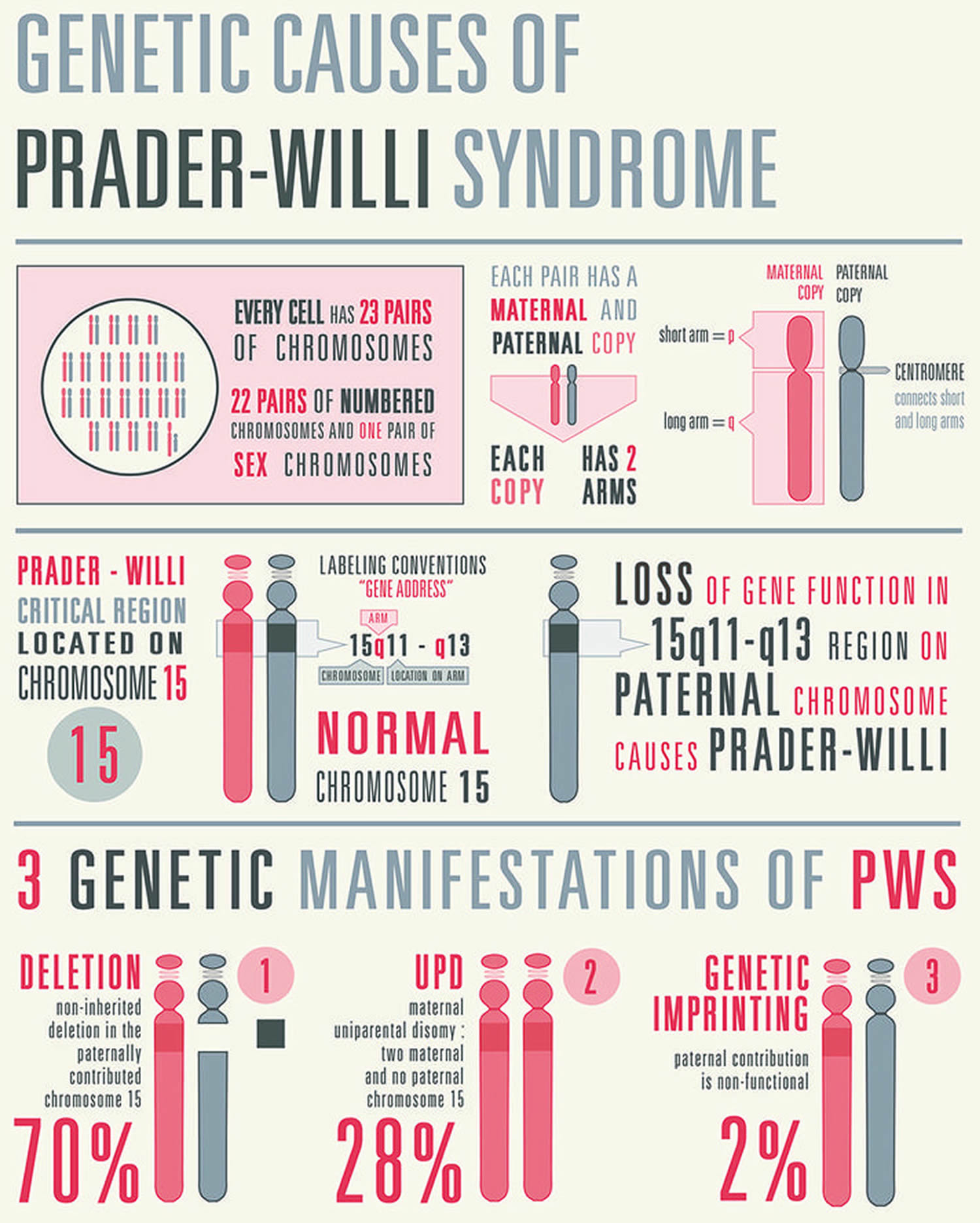
Prader-Willi syndrome is caused by the loss of function of genes in a particular region of chromosome 15. People normally inherit one copy of this chromosome from each parent. Some genes are turned on (active) only on the copy that is inherited from a person’s father (the paternal copy). This parent-specific gene activation is caused by a phenomenon called genomic imprinting.
Most cases of Prader-Willi syndrome are not inherited, particularly those caused by a deletion in the paternal chromosome 15 (about 70 % of cases) or by maternal uniparental disomy (about 25% of cases). These genetic changes occur as random events during the formation of reproductive cells (eggs and sperm) or in early embryonic development. Affected people typically have no history of the disorder in their family.
Rarely, a genetic change responsible for Prader-Willi syndrome can be inherited. For example, it is possible for a genetic change that abnormally inactivates genes on the paternal chromosome 15 to be passed from one generation to the next.
Is Prader-Willi syndrome curable?
Currently, there is no cure for Prader-Willi syndrome. The lives individuals with Prader-Willi syndrome can be improved with an early diagnosis and careful management of symptoms and support from healthcare professionals who will help you manage the problems. The treatment plan will be continually reassessed as your child gets older and their needs change.
Prader Willi syndrome cause
Prader-Willi syndrome occurs when the genes in a specific region of chromosome 15 are not present or do not function. This region of chromosome 15 is located at 15q11.2-q13 and has been designated the Prader-Will syndrome/Angelman syndrome region (Prader-Willi syndrome/Angelman syndrome). Chromosome 15q11.2-q13 refers to bands 11.2-13 on the long arm of chromosome 15. The numbered bands specify the location of the thousands of genes that are present on each chromosome. In individuals with Prader-Willi syndrome, the nonfunctioning Prader-Willi syndrome/Angelman syndrome region is always located on the number 15 chromosome inherited from the father (the paternal copy). This parent-specific gene activation is caused by a phenomenon called genomic imprinting.
Three specific abnormalities are primarily associated with Prader-Willi syndrome:
- Chromosomal deletion,
- Uniparental disomy and
- Genetic imprinting errors in the region controlling gene activity.
These genetic changes occur as random events during the formation of reproductive cells (eggs and sperm) or in early embryonic development. Affected people typically have no history of the disorder in their family.
Prader-Willi syndrome is associated with a specific process known as genetic imprinting. Normally, everyone has two copies of every gene – one received from the father and one received from the mother. In most cases, both genes are “turned on” or active. However, some genes are preferentially silenced or “turned off” based upon which parent gave the gene to the child (genetic imprinting). Genetic imprinting is controlled by chemical switches through a process called methylation and other chemical changes at the DNA level. Proper genetic imprinting is necessary for normal development. Defective imprinting has been associated with several disorders including Prader-Willi syndrome.
Imprinted genes tend to cluster or group together on chromosomes. Several imprinted genes are found in a cluster on the long arm (q) of chromosome 15. The cluster contains a functional region known as an imprinting center that regulates the imprinted genes in this region.
In most cases (about 70%), the Prader-Willi syndrome/Angelman syndrome region of the father’s chromosome 15 is missing or deleted. This chromosomal deletion results from a random error in development and is not inherited (or de novo deletion). Thus, most cases of Prader-Willi syndrome occur sporadically and the risk of recurrence in another pregnancy is less than 1%.
In about 25% of cases of Prader-Willi syndrome, the affected person inherits two copies of chromosome 15 from the mother and no copy of the father’s chromosome 15 (referred to as maternal uniparental disomy). This type of genetic change also occurs as a result of a random error in development. In most cases, the risk of recurrence of uniparental disomy is estimated to be less than 1%.
In less than 5% of cases of Prader-Willi syndrome, the Prader-Willi syndrome/Angelman syndrome region of the father’s chromosome 15 is present, but the genes do not work properly. This form of Prader-Willi syndrome is due to a defect in genes called the imprinting center and is sometimes due to a genetic change (e.g., microdeletion) that can be passed from one generation to the next.
In a very small proportion of cases, Prader-Willi syndrome has occurred due to a balanced translocation of chromosome 15. Translocations occur when portions of certain chromosomes break off and are rearranged, resulting in shifting of genetic (e.g., genes of the imprinting center) material and an altered set of chromosomes. If a chromosomal translocation is balanced (meaning that it consists of rearranged chromosomes without anything missing or extra), then it is usually harmless to the carrier. However, such a chromosomal rearrangement may be associated with an increased risk of abnormal chromosomal development in the carrier’s offspring depending on events that occur in the egg or sperm production.
Rarely, a genetic change responsible for Prader-Willi syndrome can be inherited. For example, it is possible for a genetic change that abnormally inactivates genes on the paternal chromosome 15 to be passed from one generation to the next.
A number of imprinted genes have been mapped to the Prader-Willi syndrome/Angelman syndrome region of chromosome 15. However, the specific genes involved and their role in the development of the various symptoms of Prader-Willi syndrome are being characterized but not yet known. Many symptoms associated with Prader-Willi syndrome are believed to be due to malfunction of the hypothalamus, a gland in the brain that regulates hormone secretions and under genetic control. Hormones produced by the hypothalamus affect body temperature, hunger, moods, sex drive, sleep, and thirst. The hypothalamus also influences the release of hormones from other glands, especially the pituitary gland, which regulates the release of certain hormones including growth and sex hormones.
Prader-Willi syndrome chromosome
Most cases of Prader-Willi syndrome (about 70 percent) occur when a segment of the paternal chromosome 15 is deleted in each cell. People with this chromosomal change are missing certain critical genes in this region because the genes on the paternal copy have been deleted, and the genes on the maternal copy are turned off (inactive). In another 25 percent of cases, a person with Prader-Willi syndrome has two copies of chromosome 15 inherited from his or her mother (maternal copies) instead of one copy from each parent. This phenomenon is called maternal uniparental disomy. Rarely, Prader-Willi syndrome can also be caused by a chromosomal rearrangement called a translocation, or by a mutation or other defect that abnormally turns off (inactivates) genes on the paternal chromosome 15.
It appears likely that the characteristic features of Prader-Willi syndrome result from the loss of function of several genes on chromosome 15. Among these are genes that provide instructions for making molecules called small nucleolar RNAs (snoRNAs). These molecules have a variety of functions, including helping to regulate other types of RNA molecules. (RNA molecules play essential roles in producing proteins and in other cell activities.) Studies suggest that the loss of a particular group of snoRNA genes, known as the SNORD116 cluster, may play a major role in causing the signs and symptoms of Prader-Willi syndrome. However, it is unknown how a missing SNORD116 cluster could contribute to intellectual disability, behavioral problems, and the physical features of the disorder.
In some people with Prader-Willi syndrome, the loss of a gene called OCA2 is associated with unusually fair skin and light-colored hair. The OCA2 gene is located on the segment of chromosome 15 that is often deleted in people with this disorder. However, loss of the OCA2 gene does not cause the other signs and symptoms of Prader-Willi syndrome. The protein produced from this gene helps determine the coloring (pigmentation) of the skin, hair, and eyes.
Researchers are studying other genes on chromosome 15 that may also be related to the major signs and symptoms of Prader-Willi syndrome.
Prader-Willi syndrome prevention
If you have a child with Prader-Willi syndrome and would like to have another baby, consider seeking genetic counseling. A genetic counselor may help determine your risk of having another child with Prader-Willi syndrome.
Prader-Willi syndrome complications
In addition to having constant hunger, people with Prader-Willi syndrome have low muscle mass, so they need fewer than average calories, and they may not be physically active. This combination of factors makes them prone to obesity and the medical problems related to obesity, such as:
- Type 2 diabetes
- High blood pressure, high cholesterol and heart disease
- Sleep apnea
- Other complications, such as an increased risk of liver disease and gallbladder stones
Complications of inadequate hormone production
Complications arising from inadequate hormone production may include:
- Sterility. Although there have been a few reports of women with Prader-Willi syndrome becoming pregnant, most people with this disorder are unable to have children.
- Osteoporosis. Osteoporosis causes bones to become weak and brittle, so they may break easily. People with Prader-Willi syndrome are at an increased risk of developing osteoporosis because they have low levels of sex hormones and may also have low levels of growth hormone — both hormones help maintain strong bones.
Other complications
Other complications that can result from Prader-Willi syndrome include:
- Effects of binge eating. Eating large amounts of food quickly, called binge eating, can cause the stomach to become abnormally enlarged. People with Prader-Willi syndrome may not report pain and they rarely vomit. Binge eating can also cause choking. Rarely, a person may eat so much that it causes stomach rupture.
- Reduced quality of life. Behavioral problems can interfere with family functioning, successful education and social participation. They can also reduce the quality of life for children, teenagers and adults with Prader-Willi syndrome.
Prader Willi syndrome life expectancy
Early diagnosis and treatment can improve the quality of life for people with Prader-Willi syndrome. A team of health professionals will likely work with you to manage the condition.
If obesity is not prevented by controlling food intake, people with Prader-Willi syndrome are likely to die a lot younger than would normally be expected. If their diet is well controlled and they don’t become overweight, adults can have a good quality of life and probably a normal life expectancy.
Many adults with Prader-Willi syndrome take part in activities such as voluntary or part-time work but, because of their behavioural problems and learning difficulties, it’s unlikely they’ll be able to live fully independent lives.
Prader Willi syndrome symptoms
The symptoms and severity of Prader-Willi syndrome can vary from one person to another. Many features of Prader-Willi syndrome are nonspecific and others may develop slowly over time or can be subtle. It is important to note that affected individuals may not have all of the symptoms discussed below. Affected individuals should talk to their physician and medical team about their specific case, associated symptoms and overall prognosis. Often this requires input from a clinical geneticist or genetic counselor with experience in this genetic disorder to supply the most recent and accurate information about the disorder and discuss genetic testing options or treatment plans.
Infants
Signs and symptoms that may be present from birth include:
- Poor muscle tone (floppiness). A primary sign during infancy is poor muscle tone (hypotonia). Babies may rest with their elbows and knees loosely extended instead of fixed, and they may feel floppy or like rag dolls when they’re held.
- Distinct facial features. Children may be born with almond-shaped eyes, a narrowing of the head at the temples, a turned-down mouth and a thin upper lip.
- Poor sucking reflex. Infants may have a poor sucking reflex due to decreased muscle tone. Poor sucking makes feeding difficult and can result in failure to thrive.
- Generally poor responsiveness. A baby may seem unusually tired, respond poorly to stimulation, have a hard time waking up or have a weak cry.
- Underdeveloped genitals. Males may have a small penis and scrotum. The testicles may be small or not descended from the abdomen into the scrotum (cryptorchidism). In females, the clitoris and labia may be small.
Initially, infants will exhibit diminished muscle tone (hypotonia), which can cause a baby to feel “floppy” when held. Infantile hypotonia, which is often severe, is a near universal feature of Prader-Willi syndrome. Hypotonia can be present before birth (prenatally) potentially causing decreased fetal movements and abnormal positioning of the fetus (e.g., breech position). Prenatal hypotonia is associated with an increased risk of requiring an assisted delivery. After birth, hypotonia is associated with lethargy, a weak cry, poor responsiveness to stimuli, and poor reflexes including poor sucking ability, which result in feeding difficulties and failure to thrive. Infants are usually unable to breastfeed and may require tube feeding. Hypotonia slowly improves over time, but some adults with Prader-Willi syndrome may continue to have some degree of hypotonia.
Affected infants may also have distinctive facial features including almond-shaped eyes, a thin upper lip, a downturned mouth, a narrow bridge of the nose, a narrow forehead, and a disproportionately long, narrow head (dolichocephaly). Distinctive facial features can be noticeable shortly after birth or may develop slowly over time.
Early childhood to adulthood
Other features of Prader-Willi syndrome appear during early childhood and remain throughout life, requiring careful management. These features may include:
- Food craving and weight gain. A classic sign of Prader-Willi syndrome is a constant craving for food, resulting in rapid weight gain, starting around age 2 years. Constant hunger leads to eating often and consuming large portions. Unusual food-seeking behaviors, such as hoarding food, or eating frozen food or even garbage, may develop.
- Underdeveloped sex organs. A condition called hypogonadism occurs when sex organs (testes in men and ovaries in women) produce little or no sex hormones. This results in underdeveloped sex organs, incomplete or delayed puberty, and in nearly all cases, infertility. Without treatment, women may not start menstruating until their 30s or may never menstruate, and men may not have much facial hair and their voices may never fully deepen.
- Poor growth and physical development. Underproduction of growth hormone can result in short adult height, low muscle mass and high body fat. Other endocrine problems may include underproduction of thyroid hormone (hypothyroidism) or central adrenal insufficiency, which prevents the body from responding appropriately during stress or infections.
- Cognitive impairment. Mild to moderate intellectual disability, such as issues with thinking, reasoning and problem-solving, is a common feature of the disorder. Most children with Prader-Willi syndrome have mild to moderate learning difficulties with a low IQ. Even those without significant intellectual disability have some learning disabilities. Most children with Prader-Willi syndrome can attend a mainstream school with extra support, although some will move to a special school at secondary level. Their short-term memory is usually poor, although they often have a good long-term memory. Despite these problems, children with Prader-Willi syndrome tend to be good at solving puzzles, such as word searches and jigsaws.
- Delayed motor development. Toddlers with Prader-Willi syndrome often reach milestones in physical movement — for example, sitting up or walking — later than other children do. For example, a child with the syndrome will typically begin sitting up at around 12 months and start walking at around 24 months. Many are late to talk and have difficulty pronouncing some sounds.
- Speech problems. Speech is often delayed. Poor articulation of words may be an ongoing problem into adulthood.
- High pain and vomiting tolerance. Children with Prader-Willi syndrome have a high tolerance for pain, which can be potentially dangerous. For example, a serious condition such as appendicitis would cause severe pain in most people but may pass unnoticed or be a minor upset for a child with Prader-Willi syndrome. Therefore, if a child with Prader-Willi syndrome does complain of pain, it should be taken seriously.
- Behavioral problems. Children and adults may at times be stubborn, angry, controlling or manipulative. They may throw temper tantrums, especially when denied food, and may not tolerate changes in routine. They may also develop obsessive-compulsive or repetitive behaviors, or both. For example, repeating the same activity (such as playing the same game or watching the same video repeatedly) or asking the same question over and over again, or frequently returning to the same topic in a conversation. Keeping a very strict daily routine – any unexpected disruption to the routine can upset them. Other mental health disorders, such as anxiety and skin picking, may develop. As many as 4 out of 5 children with Prader-Willi syndrome persistently pick their skin, usually their face, hands or arms. They may scratch, pierce or pull at their skin, sometimes using paper clips or tweezers. It can result in open sores, scarring and infection. Some children may pick out pieces of poo from their bottom. As well as causing embarrassment for children and parents, this can result in bleeding and infection. While these behavioral problems can be challenging for parents to deal with, children with Prader-Willi syndrome also have many positive aspects to their personality, such as being affectionate, kind, caring and funny.
- Sleep disorders. Children and adults with Prader-Willi syndrome may have sleep disorders, including disruptions of the normal sleep cycle and a condition in which breathing pauses during sleep (sleep apnea). These disorders can result in excessive daytime sleepiness and worsen behavior problems.
- Other signs and symptoms. These may include small hands and feet, curvature of the spine (scoliosis), hip problems, reduced saliva flow, nearsightedness and other vision problems, problems regulating body temperature, poor muscle tone in the gut, which can cause constipation or a swollen tummy, tooth decay because they don’t produce much saliva, weakening of the bones (osteoporosis) when they become adults because they don’t have the sex hormones needed to keep bones healthy or a lack of pigment (hypopigmentation) causing hair, eyes and skin to be pale.
As affected infants grow older, their feeding and appetite will improve and they will grow appropriately. Typically, between 2-4.5 years of age, their weight increases although there may not be a noticeable change in appetite or caloric intake. Between 4.5-8 years old, appetite and caloric intake usually increases, often thereafter developing a need to eat an extraordinarily large amount of food (hyperphagia) usually because they do not feel satisfied after completing a meal (satiety). In addition, there is a decreased calorie requirement in people with Prader-Willi syndrome. Consequently, overeating, rapid weight gain, and morbid obesity occurs if not controlled by others. Not all affected children will go through these stages.
If left uncontrolled and untreated, morbid obesity can develop, potentially leading to life-threatening heart and lung complications, diabetes, high blood pressure (hypertension), and to other serious complications. The compulsion to eat is so overwhelming that people with this disorder, if left unsupervised, may endanger themselves by eating harmful food such as spoiled food or garbage and excessive quantities, harmful to the stomach. Affected children may also exhibit unusual behaviors regarding food including hoarding and/or foraging for food, stealing food, and stealing money to buy food.
Some affected individuals have developed serious, life-threatening gastrointestinal complications due to episodes of binge eating. Such complications can include severe bloating (gastric dilatation) with the development of a hole or tear in the intestinal wall (perforation) and tissue loss (necrosis).
Children with Prader-Willi syndrome also have varying levels of cognitive impairment, ranging from borderline or low normal intelligence with learning disabilities to mild to moderate intellectual disability. The attainment of motor milestones (e.g. walking or sitting up) and language development are often delayed.
Affected children generally have sweet and loving personalities, but often develop distinct behavioral issues. Such issues can include temper tantrums, stubbornness, obsessive/compulsive behavior, manipulative behavior, and skin picking, which can cause chronic open wounds, scarring and infection. In some cases, the behavior profile may be suggestive of autism. Psychosis occurs in approximately 10-20% of late adolescents and young adults. Evidence shows that the type of chromosome 15 defect may relate to certain behavioral problems which will require additional studies for determination.
Hypogonadism is a common finding in Prader-Willi syndrome. Hypogonadism refers to inadequate function of the sex organs, the testes in males and the ovaries in females. The sex organs in affected individuals fail to produce sufficient sex hormones, which can result in underdeveloped sex organs, incomplete development at puberty, delayed onset of puberty, and infertility. Genital underdevelopment is evident at birth. Affected males may exhibit a small penis, underdeveloped scrotum, and small testes. Failure of one or both testes to descend (cryptorchidism) is a common finding, as well. Affected females may exhibit an abnormally small clitoris or labia minor. Absence of a menstrual cycle (primary amenorrhea) is common and in some cases the initial menstrual period (menarche) may not occur until 30 years of age or older.
Individuals with Prader-Willi syndrome have growth hormone (GH) insufficiency, a condition characterized by the inadequate secretion of growth hormone from the anterior pituitary gland, a small gland located at the base of the brain that is responsible for the production of several hormones. Children may be significantly below average height based upon sex and age (short stature). Growth hormone (GH) deficiency affects both children and adults and the final adult height of affected individuals is shorter than unaffected family members. Growth hormone insufficiency also results in an increase in the amount of fat and a relative decrease in muscle mass (altered body composition). If growth hormone (GH) isn’t replaced, the average adult height for people with Prader-Willi syndrome is 159cm (5ft 2in) for a man and 149cm (4ft 10in) for a woman.
Affected individuals may also have abnormally small hands and feet, side-to-side curvature of the spine (scoliosis), and, in approximately 10% of individuals, a malformed hip (hip dysplasia). Scoliosis can occur at any age including infancy and varies in severity. Sleep problems are common, including excessive daytime sleepiness, reduced rapid eye movement (REM) latency, disruption of the normal sleep cycle, and central and/or obstructive sleep apnea.
Some individuals may have lack of color (pigment) known as hypopigmentation affecting the hair, eyes and skin. They may appear fair-skinned compared to other family members. Nearsightedness (myopia) and misaligned eyes (strabismus) may also occur.
Affected individuals may also experience recurrent respiratory infections. Up to 25% of affected individuals may have an underactive thyroid gland (hypothyroidism). In addition, the rates of certain conditions are increased in individuals with Prader-Willi syndrome including fractures due to decreased bone density (osteopenia), altered temperature sensation, a high vomiting threshold, and swelling (edema) and ulcerations of the legs, especially in obese adults. Some individuals may have reduced flow of saliva with abnormally thick, sticky saliva. Additional symptoms that can occur in affected individuals include a high pain threshold, a tendency to bruise easily without known cause, and seizures.
Some individuals with Prader-Willi syndrome may develop central adrenal insufficiency, a condition characterized by deficiency of adrenocorticotropic hormone (ACTH). This hormone is produced by the pituitary gland. One of the main functions of adrenocorticotropic hormone (ACTH) is to stimulate the adrenal glands to produce cortisol, which helps to regulate blood sugar and the body to deal with stress. In some cases, central adrenal insufficiency may only be detectable during periods of stress (e.g., during illness or injury). The exact percentage of affected individuals with central adrenal insufficiency and its overall implications to individuals with Prader-Willi syndrome are not yet fully understood.
Prader Willi syndrome diagnosis
A diagnosis of Prader-Willi syndrome is based upon a detailed patient history, a thorough clinical evaluation and identification of characteristic symptoms. Consensus diagnostic criteria for Prader-Willi syndrome have been established and are effective for identifying potential cases of Prader-Willi syndrome. All infants and newborns with unexplained hypotonia and poor suck should be tested for Prader-Willi syndrome. To confirm a diagnosis of Prader-Willi syndrome, certain specialized tests are required including DNA methylation tests and fluorescent in situ hybridization (FISH). More recently, high resolution chromosomal microarray studies with several hundred thousand DNA probes from throughout the genome representing all chromosomes can be utilized to identify small deletion or duplications of the chromosomes that cannot be seen with routine chromosome studies. Microarrays can help identify the typical chromosome 15q11q13 deletion as well as smaller rearrangements of this region, imprinting defects and possibly maternal disomy 15 seen in Prader-Willi syndrome.
Checklist for diagnosing Prader-Willi syndrome
A checklist of symptoms known to be typical of Prader-Willi syndrome is also used to identify which children should be tested.
The checklist can also be helpful for parents concerned about their child’s development, behavior and eating habits, and who want to know whether their child may have Prader-Willi syndrome.
Major criteria
One point is given for each of the following symptoms a child has:
- floppiness and weak muscles, becoming apparent during or shortly after birth
- feeding problems and failure to grow during the first year of life
- rapid weight gain in children aged 1 to 6 years
- characteristic facial features, such as almond-shaped eyes and thin upper lips
- underactive testicles or ovaries (hypogonadism), resulting in delayed sexual development
- delayed physical development or learning difficulties
Minor criteria
Half a point is given for each of the following symptoms a child has:
- lack of movement during pregnancy, such as kicking in the womb, or an unusual lack of energy after birth
- sleep disturbances, such as sleep apnoea
- delayed or absent puberty
- unusually fair hair, skin and eyes
- narrow hands
- thick and sticky saliva
- crossed eyes or long-sightedness (hyperopia)
- problems pronouncing words and sounds properly
- frequent skin picking
Overall score
If your child is under the age of 3 and scores 5 points, with at least 3 points from the major criteria, Prader-Willi syndrome would be strongly suspected and genetic testing would be recommended.
If your child is over the age of 3 and scores 8 points, with at least 4 points from the major criteria, Prader-Willi syndrome would be strongly suspected and testing would be recommended.
Genetic testing
Approximately 99% or more of cases of Prader-Willi syndrome can be diagnosed by DNA methylation study. This test allows for the examination of the Prader-Willi syndrome/Angelman syndrome critical region of chromosome 15. If the methylation pattern is consistent with maternal inheritance, then this indicates that the paternal chromosome 15 is not present or not active. This finding is diagnostic of Prader-Willi syndrome, but methylation tests cannot distinguish among the different underlying causes of Prader-Willi syndrome (i.e., deletions, imprinting defects or maternal disomy 15).
If DNA methylation tests indicate Prader-Willi syndrome, then additional tests are necessary to determine the underlying cause of the disorder. This is important for determining whether there is an increased risk for the parents or other family members to have an affected child. A FISH test or microarray, which analyses chromosomes, can detect a deletion, the most common cause of Prader-Willi syndrome. If no deletion is present, then additional testing is performed to distinguish between uniparental maternal disomy and or a defect of the imprint center.
Prenatal diagnosis is possible in families with a previous history of Prader-Willi syndrome. Prior identification of a disease causing abnormality can facilitate prenatal testing, but it is available by methylation analysis following amniocentesis regardless of cause.
Prader Willi syndrome treatment
The treatment of Prader-Willi syndrome is directed toward the specific symptoms that are apparent in each individual. Early intervention and strict maintenance to treatment can greatly improve the overall health and quality of life for affected individuals and their families. Treatment may require the coordinated efforts of a team of specialists. Clinical geneticists, pediatricians, orthopedists, endocrinologists, speech therapists, psychologists, dieticians, nutritionists, and other healthcare professionals may need to systematically and comprehensively plan an effective program for the child’s treatment. Genetic counseling may be of benefit for affected individuals and their families to further discuss the condition, provide information and to quote recurrence risks. Parents are strongly recommended to undergo appropriate parenting techniques for the behavioral and eating issues associated with Prader-Willi syndrome; such education correlates with better prognosis.
Specific therapeutic procedures and interventions may vary, depending upon numerous factors, such as disease severity; the presence or absence of certain symptoms; an individual’s age and general health; and/or other elements. Decisions concerning the use of particular drug regimens and/or other treatments should be made by physicians and other members of the health care team in careful consultation with the patient based upon the specifics of his or her case; a thorough discussion of the potential benefits and risks, including possible side effects and long-term effects; patient preference; and other appropriate factors.
Infants and young children care
Although specific treatments vary depending on symptoms, most children with Prader-Willi syndrome will need the following:
- Good nutrition for infants. Many infants with Prader-Willi syndrome have difficulty feeding due to decreased muscle tone. Your child’s pediatrician may recommend a high-calorie formula or special feeding methods to help your baby gain weight and will monitor your child’s growth.
- Human growth hormone (GH) treatment. Human growth hormone (GH) treatment in children with Prader-Willi syndrome helps increase growth, improves muscle tone and decreases body fat. A doctor who treats hormonal disorders (endocrinologist) can help determine whether your child would benefit from growth hormone and discuss any risks. A sleep study is usually recommended before starting growth hormone treatment.
- Sex hormone treatment. Your endocrinologist may suggest that your child take hormone replacement therapy (testosterone for males or estrogen and progesterone for females) to replenish low levels of sex hormones. Hormone replacement therapy usually starts when your child reaches the normal age for puberty and can help reduce the risk of developing thinning of the bones (osteoporosis). Surgery may be needed to correct undescended testicles.
- Weight management. A dietitian can help you develop a healthy, reduced-calorie diet to help manage your child’s weight while ensuring proper nutrition. A restricted-calorie diet may require supplemental vitamins or minerals to ensure balanced nutrition. Increasing physical activity and exercise can help manage weight and improve physical functioning.
- Treatment of sleep disturbances. Treating sleep apnea and other sleep problems can improve daytime sleepiness and behavioral issues.
- Various therapies. Your child will likely benefit from a range of therapies, including physical therapy to improve movement skills and strength, speech therapy to improve verbal skills, and occupational therapy to learn everyday skills. Developmental therapy to learn age-appropriate behaviors, social skills and interpersonal skills also may help. In the U.S., early intervention programs with these types of therapy are usually available for infants and toddlers through a state’s health department. During school years, educational planning and support can maximize learning.
- Behavior management. Setting strict limits on behavior, schedules and access to food and strict supervision of food intake may be required. Some people may need medication to manage behavior problems.
- Mental health care. A mental health professional, such as a psychologist or a psychiatrist, may help address psychological problems — for example, obsessive-compulsive behaviors, skin picking or a mood disorder.
- Other treatments. These may include addressing specific symptoms or complications identified by eye exams for vision problems, tests for hypothyroidism or diabetes, and examinations for scoliosis.
In infants, special nipples or gavage feeding may be used to ensure adequate nutrition. Gavage feeding is a procedure in which a small, thin tube is passed through the nose and mouth to the stomach to directly feed a newborn who has feeding difficulties.
In males, the treatment of hypogonadism with either testosterone or human chorionic gonadotropin (hCG) may be beneficial during infancy, potentially increasing the size of the genitalia or prompting testicular descent into the scrotum when cryptorchidism is present. Although cryptorchidism may occasionally resolve spontaneously or with hormone therapy, most males may require surgical treatment.
Individuals with Prader-Willi syndrome also benefit from growth hormone (GH) therapy, which can help to increase height, improve lean body mass, mobility and respiratory function, decrease body fat and ultimately improve the quality of life. Some studies have shown that growth hormone (GH) therapy may improve development and behavior. In June of 2000, the Food and Drug Administration (FDA) approved the use of human growth hormone for the treatment of children with genetically-confirmed Prader-Willi syndrome and evidence of growth failure. Studies have shown that the earlier growth hormone therapy is started the more beneficial it is and that therapy can begin as early as two to three months of age. Growth hormone therapy has been shown to improve facial appearance and overall body build (body habitus). It is recommended that affected individuals undergo a sleep study to detect and treat obstructive sleep apnea before initiating growth hormone therapy because some reports suggest a link between premature death and growth hormone therapy in certain individuals with Prader-Willi syndrome (e.g., those with profound hypotonia or obesity and pre-existing respiratory or cardiac problems). However, other researchers have expressed doubt as to whether growth hormone therapy had a direct role in these cases but decisions regarding growth hormone therapy in individuals with Prader-Willi syndrome are best made after consultation with a pediatric endocrinologist after a sleep study and assessments for adrenal gland insufficiency.
Hormone treatments
Treatment with an artificial version of the human growth hormone (GH) is usually recommended for children with Prader-Willi syndrome.
Human growth hormone (GH) also has a number of other important health benefits. For example, it:
- increases muscle size while lowering the amount of body fat
- increases muscle strength, which helps with developmental progress such as walking and running
- should increase energy levels, which will help your child become more physically active
- helps normalize facial appearance, making the distinctive facial features associated with Prader-Willi syndrome less noticeable
It’s usually recommended that treatment with human growth hormone (GH) begins during early childhood, from 6 months to 2 years of age, and would normally carry on until the end of growth. A test looking for breathing problems (a sleep study) is normally done before starting growth hormone.
A type of human growth hormone (GH) called somatropin is used to treat children with Prader-Willi syndrome. Somatropin is given by daily injection. Most children tolerate somatropin well and side effects are uncommon.
It’s usual to replace female sex hormones (often with the combined oral contraceptive pill) to:
- encourage development of secondary sex characteristics (breast development) and periods
- improve bone strength and prevent osteoporosis
Replacing male sex hormone (testosterone) is more contentious. Although this will encourage development of puberty and build muscle strength, it’s possible that some behavioral problems will be exaggerated.
Children with Prader-Willi syndrome require early intervention to assess and treat issues with motor skills, intellectual disability, and speech and language development. Early intervention may include physical and occupational therapy, special education, and speech therapy. An individualized education plan should be created at the start of school. Behavioral therapy and, in some cases, psychoactive medications such as specific serotonin reuptake inhibitors may be beneficial to manage difficult behavior or psychosis.
Children should receive an ophthalmological exam to evaluate for eye abnormalities potentially associated with Prader-Willi syndrome such as strabismus and to assess visual acuity. Children should also be assessed for hip dysplasia and scoliosis which can occur in this patient population. Evaluation and treatment of sleep disturbance is recommended as well. Some researchers recommend that all individuals with Prader-Willi syndrome be screened for hypothyroidism (which occurs with increased incidence in Prader-Willi syndrome) and central adrenal insufficiency.
During childhood, a program consisting of a low calorie diet, regular exercise and a strict supervision of food intake and access should be formulated. Strict supervision of food intake should be based upon height, weight and body mass index (BMI). Such a program should begin before signs of obesity to help to prevent its development. Limiting the access to food may require locking cabinets and refrigerators. Some individuals may require vitamin supplementation, especially for calcium and vitamin D.
Transition to adult care
Most people with Prader-Willi syndrome will need specialized care and supervision throughout their lives. Many adults with the disorder live in residential care facilities that enable them to eat healthy diets, live safely, work and enjoy leisure activities.
As your child approaches adulthood, consider these strategies:
- Find local resources and services for adults through your child’s school and organizations such as the Prader-Willi Syndrome Association.
- Investigate guardianship issues, wills and special needs trusts that address future care and supervision for your child.
- Talk to your child’s doctor for suggestions about making the transition to adult medical care.
Sex hormones can be replaced at puberty as they can stimulate the development of secondary sexual characteristics and improve self-image and bone density. In males, the use of such therapy has been controversial because testosterone replacement by monthly injection may contribute to behavioral issues in males; use of a testosterone patch or gel will avert this problem. Sex hormone replacement therapy may increase the risk of stroke in females, as in the general population, and hygiene issues should also be considered. Sex education and consideration of contraception are important, particularly in females, as rarely pregnancy has occurred. Decreased flow of saliva may be improved with special toothpastes, gels, mouthwash and gum.
Managing weight and diet
The most important aspect of caring for a child with Prader-Willi syndrome is trying to manage their diet and prevent them gaining too much weight. It’s also probably one of the biggest challenges.
The inability to control food intake is often the biggest obstacle keeping those with Prader-Willi syndrome from living independently. To date, no medications have proven effective in regulating appetite in Prader-Willi syndrome, and therefore, strict environmental control and constant supervision are the only ways to prevent life-threatening overeating and extreme obesity at present.
Your child will never learn to control their food intake themselves, so you need to do this for them. Children with Prader-Willi syndrome burn up less energy, and need fewer calories and less food than other children. A children’s dietitian can give you information about what food to give your child.
Advice about diet:
- start to get into good habits with a healthy diet and regular mealtimes as soon as your child starts on solid food – don’t wait for them to show signs of an increased appetite
- avoid sugary items, sweets and high-calorie snacks
- give smaller portions of carbohydrates such as potatoes, rice or pasta
- increase the amount of lower-calorie items such as vegetables, salads and fruit
- give a vitamin supplement
Your child will not learn to control their food intake themselves and you need to take control of things:
- keep to regular mealtimes and do not allow any extra portions
- stop them accessing food outside of mealtimes – you may need to lock cupboards and the fridge, or lock the kitchen – and make sure they can’t get food from the bins or freezer
- keep food out of their view
- make sure there are no times they can access food unsupervised
- make sure everyone who is in contact with the child (school staff, relatives and friends) knows about the issues with food
It’s also important to let relatives, friends, other parents and teachers know about the need to restrict your child’s diet.
Some medications have been used to try to suppress children’s appetites but have all been unsuccessful.
Weight loss surgery isn’t recommended for children with Prader-Willi syndrome because they don’t have the willpower to stick to the strict diet required after surgery.
Taking food
Many children with Prader-Willi syndrome will try to take food if they get the opportunity. This isn’t because they’re being naughty but because they aren’t able to control their impulses when it comes to food. Nevertheless, taking food is a behavioral problem that needs to be addressed, otherwise your child could become severely obese.
Tips to prevent stealing food include trying to establish a contract to reward good behavior. In younger children, a verbal agreement, such as: “If you stick to your diet then you can play an extra hour with your puzzles”, should be sufficient. In older children and teenagers, a written contract may be more appropriate, particularly as children with Prader-Willi syndrome respond well to clear instructions.
Most children with the syndrome will automatically lie about taking food, even when the evidence is overwhelming. So rather than asking: “Did you steal that food?”, say something along the lines of: “I know you stole that food and we need to talk about why that’s wrong.”
It’s important your child understands the consequences of their actions and what’s considered acceptable behaviour. If they steal food or money to buy food, always insist they apologise and pay any money back.
Controlling the urge to take food should always be highly praised and persistent good behaviour rewarded.
Exercise
Exercise plays an important part in helping your child maintain a healthy weight. Children should do at least 60 minutes of exercise a day.
Many children with Prader-Willi syndrome have reduced energy levels. It may be a good idea to break down their exercise into 5 to 10-minute sessions throughout the day to stop them getting tired and discouraged. Your child’s care team should be able to recommend a suitable exercise plan.
Children with Prader-Willi syndrome usually prefer individual activities to team sports, such as:
- swimming
- walking
- exercising in a gym
It’s important not to promise food as a reward to encourage your child to participate in exercise because it can encourage unhealthy behavior.
Dealing with tantrums
Parents often learn to recognise the warning signs of a temper tantrum. It’s sometimes possible to stop the tantrum before it starts using a number of approaches. For example:
- try to take their mind off the situation by doing or saying something unexpected, or talking about a subject they’re interested in
- encourage them to go to a quiet place for a few minutes and try some deep breathing or listen to soothing music
- avoid saying things like, “You’d better not have a tantrum about this”
- remain as cool and calm as possible – if you feel your child’s frustration is directed at you, then your partner or another carer can take over the situation
After a tantrum, try to remain as calm as possible. If your child hurts themselves or others, you may need to be taught special restraint techniques. Your child’s care team will be able to advise you about this.
It’s important not to give in to the demands that provoked the tantrums. While this may be tempting, it will signal to your child that tantrums are an effective way of getting what they want.
Treatment for skin picking
Frequent skin picking can lead to scarring and skin infections such as cellulitis, an infection of the underlying tissue. It’s very important for cellulitis to be identified early and treated with large doses of antibiotics.
It’s recommended you keep your child’s nails as short as possible. This should help minimise damage to the skin. Try to keep any affected part of the body covered up and use clothes to limit access if possible.
Keep any areas of damaged skin as clean as possible. If your child has a history of frequent skin infections, their care team may prescribe an antibiotic cream you can use on damaged areas to prevent infection.
Two types of treatment that are moderately effective in helping prevent people with Prader-Willi syndrome from picking their skin are cognitive behavioual therapy (CBT) and medication.
Cognitive behavioural therapy
Cognitive behavioural therapy (CBT) is a type of talking therapy. It aims to modify unhelpful and unhealthy patterns of behaviour by changing the way people think.
It’s thought people with Prader-Willi syndrome pick their skin as a way of coping with situations such as feeling unhappy or bored. CBT can help people understand the thought patterns that drive skin picking and encourage them to find new ways of thinking about and coping with these situations.
Medication
A type of antidepressant – selective serotonin reuptake inhibitors (SSRIs) – or antipsychotics (medication usually used to treat psychosis) are sometimes recommended to treat Prader-Willi syndrome.
However, these medications can cause side effects and are not usually recommended for children under the age of 18.
Medication is usually only considered if the symptoms of skin picking are severe enough to justify the associated risks of treatment.
Treatment for psychosis
A small number of people with Prader-Willi syndrome develop psychosis, usually during the teenage years or adulthood.
Psychosis is a mental health problem that causes people to perceive or interpret things differently from those around them. The symptoms of psychosis usually begin abruptly and will cause the person affected to suddenly become very upset and agitated, and act in ways that are uncharacteristic.
Contact your child’s care team if you notice a sudden and unusual change in their behaviour.
Psychosis can be treated with cognitive behavioual therapy (CBT) or medication such as antipsychotics.
Adults with Prader-Willi syndrome
Most adults with Prader-Willi syndrome are unable to live fully independent lives, such as living in their own home and having a full-time job because their behavioral issues and problems with food mean these environments and situations are too demanding.
However, adults with Prader-Willi syndrome can have active social lives and become involved in clubs or volunteering. Adults with the syndrome who don’t live with their parents will probably require residential care.
Lifestyle and home remedies
Tips to help you take care of your loved one with Prader-Willi syndrome include the following:
- Learn about Prader-Willi syndrome. Managing hormone levels and weight can improve development and behavior and prevent complications. Work with your health care team to develop a plan of care for managing symptoms and addressing issues.
- Stick to a strict meal plan. Eating a low-calorie diet is essential to keep your child from becoming overweight. Structure mealtime and the type of food to help develop routines and to help your child understand expectations. Use small dishes for serving meals. To help prevent binging, avoid buying high-calorie snacks. Store food out of your child’s reach. Lock pantries, refrigerators and cupboards.
- Encourage regular daily activity. Increasing physical activity and exercise can help manage weight and improve physical functioning.
- Set limits. Create a firm schedule and set expectations for managing behavior. If needed, talk to your health care team about ways to address problems.
- Schedule regular medical care. Talk with your doctor about a regular schedule of health appointments and tests to check for problems or complications related to Prader-Willi syndrome.
Most children with Prader-Willi syndrome cope best if they have a very structured environment and daily routine. For example, you should:
- establish a regular daily routine and give plenty of notice if any changes are planned
- not put pressure on a child to speed up to complete a task – give them plenty of warning if they need to complete an activity, such as getting dressed to go out
- ensure other people, such as relatives and teachers, are briefed about how to interact with your child
- avoid eating in front of your child so they don’t start to think about food
Coping and support
Having a child with Prader-Willi syndrome is challenging and can take a lot of patience. Managing eating problems, behavior and medical issues can impact the whole family.
Some options for coping and support can include:
- Talking to a mental health professional. If you’re having trouble coping or feel overwhelmed, talk to a mental health counselor or therapist.
- Joining a support group. Some people find it helpful to talk with others who share similar experiences. Ask your health care provider about family support groups in your area. Organizations such as the Prader-Willi Syndrome Association (https://www.pwsausa.org/), The Foundation for Prader-Willi Research (https://www.fpwr.org/) or Prader-Willi Syndrome Association UK (http://www.pwsa.co.uk/) provide resources, support groups and educational materials.
- Seeking other sources of support. Options for additional support can include asking about sources of respite care, asking for support from family and friends, and taking time for your own interests and activities.





{kind=link}