Contents
What is precocious puberty
Precocious puberty is when a person’s sexual and physical traits develop and mature earlier than normal. Precocious (meaning prematurely developed) puberty (secondary sex characteristics) begins in girls younger than 7½ or 8 and in boys younger than age 9. In the United States, precocious puberty affects about 1 – 2% of children (roughly 3 million children) 1. Yet, in most of these children, early puberty is a variation of normal and no medical problem is present. The actual age that defines sexual precocity is therefore dependent on the epidemiological data that one uses to define the average age of pubertal onset. Different populations and different time periods will therefore have differing definitions of precocious puberty. Recently, most likely because of increasing weight in the population, puberty appears to be having an earlier age of onset 1.
Many more girls are affected than boys. One study suggests that African American girls have some early breast development or some early pubic hair more often than white girls or Hispanic girls.
The cause of precocious puberty is not always known. Some cases of precocious puberty are due to conditions that cause changes in the body’s release of hormones. Treatment involves medications that can stop the release of sexual hormones 2.
Signs of Precocious Puberty
In girls, the telltale signs of precocious puberty include any of the following before 7 or 8 years of age:
- breast development
- pubic or underarm hair development
- rapid height growth — a growth “spurt”
- start of menstruation (her period)
- acne
- “mature” body odor
In boys, the signs of precocious puberty before 9 years of age include:
- enlargement of the testicles or penis
- pubic, underarm, or facial hair development
- rapid height growth — a growth “spurt”
- voice deepening
- acne
- “mature” body odor.
How Precocious Puberty Affects Kids
When puberty ends, growth in height stops. Because their skeletons mature and bone growth stops at an earlier age than normal, kids with precocious puberty usually don’t reach their full adult height potential. Their early growth spurt may make them initially tall when compared with their peers, but they may stop growing too soon and end up at a shorter height than they would have otherwise.
Going through puberty early also can be difficult for kids emotionally and socially. For example, girls with precocious puberty may be confused or embarrassed about physical changes such as getting their periods or having enlarged breasts well before any of their peers. But the hardest part may be the teasing that kids with the condition — especially girls — may experience.
Even emotions and behavior may change in kids with precocious puberty. Girls can become moody and irritable. Boys can become more aggressive and also develop a sex drive inappropriate for their age.
Children affected by precocious puberty may experience problems such as:
- Failure to reach their full height because their growth halts too soon
- Psychological and social problems, such as anxiety over being “different” from their peers. However, many children do not experience major psychological or social problems, particularly when the onset of puberty is only slightly early.
Who is at risk of early puberty?
There is a greater chance of being affected by precocious puberty if a child is 3:
- Female
- African American
- Obese
Normal puberty
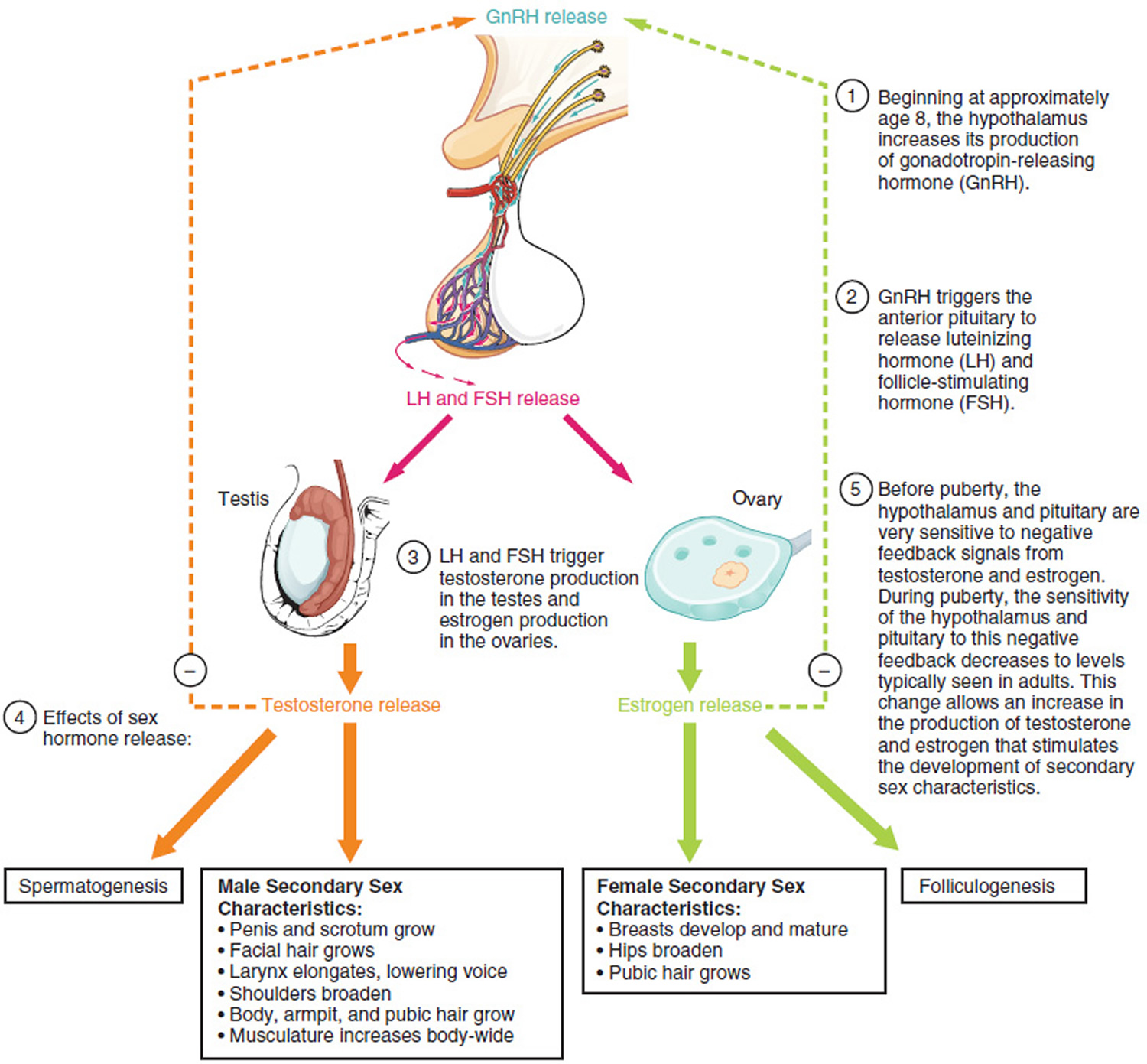
Normal puberty typically begins between ages 8 and 13 for girls (the average age is about 10) and ages 9 and 14 for boys (the average age is about 11) 4. The start of puberty depends on various factors such as family history, nutrition and gender. Normally, the hypothalamus initiates puberty by releasing a hormone called gonadotropin-releasing hormone (GnRH) that stimulates the anterior pituitary gland to release gonadotropins – follicle-stimulating hormone (FSH) and luteinizing hormone (LH), the hormones which control growth and function of the sex organs (see Figure 1). When gonadotropins follicle-stimulating hormone (FSH) and luteinizing hormone (LH) are released, synthesis and secretion of sex steroids (such as estrogen, progesterone or testosterone) occur in the testicles (testosterone) or ovaries (estrogen & progesterone), leading to development of secondary sexual characteristics. If this occurs prematurely, a child starts to develop secondary sexual characteristics and proceeds to sexual maturity at an unexpectedly early age. Since the maturing of one’s bones is usually accelerated by this condition, early fusion of the growth plates occurs, resulting in shortening of adult stature. However, during childhood, children with precocious puberty are often taller than their peers.
Many kids who show some of the early signs of puberty have what’s known as “partial” precocious puberty. Some girls, usually beginning between the ages of 6 months and 3 years, may show breast development that later disappears or may last without other physical changes of puberty.
Similarly, some girls and boys may have early growth of pubic and/or underarm hair that isn’t related to other changes in sexual development.
Kids with “partial” precocious puberty may need to see their doctor to rule out “true” precocious puberty or other health problems. But most need no treatment and usually will show the other expected signs of puberty at the usual age.
Many children who go through puberty early or late have other family members who went through puberty early or late. Just as there are differences in the age at which puberty starts, there are also differences in the rate at which a child goes through puberty.
Near the end of puberty, growth in height stops. Because the bones of children with precocious puberty mature and stop growing earlier than normal, these children can be shorter than expected as adults. Precocious puberty can also cause emotional and social problems for children who are ahead of their peers in terms of sexual maturity.
See your doctor if your child shows any signs of early sexual maturation (before age 7 or 8 in girls or age 9 in boys), including breast development, rapid height growth, menstruation, acne, enlarged testicles or penis, or pubic or underarm hair.
Figure 1. Normal puberty
Precocious puberty complications
Possible complications of precocious puberty include:
- Short height. Children with precocious puberty may grow quickly at first and be tall, compared with their peers. But, because their bones mature more quickly than normal, they often stop growing earlier than usual. This can cause them to be shorter than average as adults. Early treatment of precocious puberty, especially when it occurs in very young children, can help them grow taller than they would without treatment.
- Social and emotional problems. Girls and boys who begin puberty long before their peers may be extremely self-conscious about the changes occurring in their bodies. This may affect self-esteem and increase the risk of depression or substance abuse.
Early onset puberty causes
In approximately 90% of girls who experience precocious puberty, no underlying cause can be identified—although heredity and being overweight may contribute in some cases. When a cause cannot be identified, the condition is called idiopathic precocious puberty. In boys with precocious puberty, approximately 50% of cases are idiopathic. In the remaining 10% of girls and 50% of boys with precocious puberty, an underlying cause can be identified.
Sometimes the cause is an abnormality involving the brain. In other children, the signs of puberty occur because of a problem such as a tumor or genetic abnormality in the ovaries, testes, or adrenal glands, causing overproduction of sex hormones.
Precocious puberty can be divided into two categories, depending on where in the body the abnormality occurs—central precocious puberty and peripheral precocious puberty.
The onset of puberty is normally triggered by the hypothalamus (the area of the brain that helps control pituitary gland function). It signals the pituitary gland (a pea-sized gland near the base of the brain) to release hormones that stimulate the ovaries (in girls) or testicles (in boys) to make sex hormones.
Sometimes, precocious puberty stems from a structural problem in the brain (such as a tumor), brain injury due to head trauma, an infection (such as meningitis), or a problem in the ovaries or thyroid gland that triggers the onset of puberty ahead of schedule — but this usually isn’t the case.
For the majority of girls, there’s no medical problem at fault — they simply start puberty too early for no known reason.
In boys, the condition is less common and more likely to be related to another medical problem. And for about 5% of boys, precocious puberty is inherited. (Less than 1% of girls with precocious puberty have inherited the condition.) Early puberty can be passed to a son by his father or to the son from his maternal grandfather through his mother (who will not be affected by the disorder).
Central Precocious Puberty
Central precocious puberty occurs when the hypothalamus releases GnRH (gonadotropin-releasing hormone) which stimulates the pituitary gland to begin puberty at an early age. In most girls with central precocious puberty, there is no underlying medical problem. In boys, the condition is less common and is more likely to have a link to a medical problem. Such problems include a tumor, brain trauma (such as a blow to the head, brain surgery, or radiation treatment to the head), or inflammation (such as meningitis).
Central precocious puberty is the most common form of precocious puberty and affects many more girls than boys.
There’s usually no identifiable cause for this type of precocious puberty.
In central precocious puberty, the puberty process starts too soon. The pattern and timing of the steps in the process are otherwise normal. For the majority of children with this condition, there’s no underlying medical problem and no identifiable reason for the early puberty.
In rare cases, the following may cause central precocious puberty:
- A tumor in the brain or spinal cord (central nervous system)
- Prior radiation to the brain or spinal cord (central nervous system)
- A defect in the brain present at birth, such as excess fluid buildup (hydrocephalus) or a noncancerous tumor (hamartoma)
- Prior infection of the brain
- Other brain abnormalities
- Injury to the brain or spinal cord
Often, however, there is no identifiable abnormality in the brain; this is called idiopathic central precocious puberty.
Peripheral Precocious Puberty
The less common peripheral precocious puberty occurs without the involvement of the gonadotropin hormone in your brain (GnRH) that normally triggers the start of puberty. In peripheral precocious puberty, the abnormality is not in the brain but in the testicles, ovaries, or adrenal glands, causing overproduction of sex hormones, like testosterone and estrogens.
Peripheral precocious puberty may be caused by 5:
- Tumors of the ovary, testis, or adrenal gland
- In boys, tumors that secrete a hormone called hCG, or human chorionic gonadotropin
- Certain rare genetic syndromes, such as McCune-Albright syndrome (a rare genetic disease that affects bones and skin color and causes hormonal problems) or familial male precocious puberty
- Severe hypothyroidism, in which the thyroid gland secretes abnormally low levels of hormones
- Disorders of the adrenal gland, such as congenital adrenal hyperplasia — a group of genetic disorders involving abnormal hormone production by the adrenal glands
- Exposure of the child to medicines or creams that contain estrogens or androgens
In girls, peripheral precocious puberty may also be associated with:
- Ovarian cysts
- Ovarian tumors
In boys, peripheral precocious puberty may also be caused by:
- A tumor in the cells that make sperm (germ cells) or in the cells that make testosterone (Leydig cells)
- Gene mutation — a rare disorder called gonadotropin-independent familial sexual precocity, which is caused by a defect in a gene, can result in the early production of testosterone in boys, usually between ages 1 and 4.
Risk factors for precocious puberty
Factors that increase a child’s risk of precocious puberty include:
- Being a girl. Girls are much more likely to develop precocious puberty.
- Being African-American. Precocious puberty appears to affect African-Americans more often than children of other races.
- Being obese. Children who are significantly overweight have a higher risk of developing precocious puberty.
- Being exposed to sex hormones. Coming in contact with an estrogen or testosterone cream or ointment, or other substances that contain these hormones (such as an adult’s medication or dietary supplements), can increase your child’s risk of developing precocious puberty.
- Having other medical conditions. Precocious puberty may be a complication of McCune-Albright syndrome or congenital adrenal hyperplasia — conditions that involve abnormal production of the male hormones (androgens). In rare cases, precocious puberty may also be associated with hypothyroidism.
- Having received radiation therapy of the central nervous system. Radiation treatment for tumors, leukemia or other conditions can increase the risk of precocious puberty.
Precocious puberty signs and symptoms
The symptoms of precocious puberty are similar to the signs of normal puberty but they manifest earlier—before the age of 8 in girls and before age 9 in boys.
Normal Puberty
In Girls
The signs of puberty include:
- Growth of pubic and other body hair
- Growth spurt
- Breast development
- Onset of menstruation (after puberty is well advanced)
- Acne
In Boys
The signs of puberty include 6:
- Growth of pubic hair, other body hair, and facial hair
- Enlargement of penis and testicular enlargement (>3 ml)
- Muscle growth
- Growth spurt
- Acne
- Deepening of the voice
Precocious puberty diagnosis
To identify whether a child is entering puberty, a pediatrician (a physician specializing in the treatment of children) will carefully examine the following:
- In girls, the growth of pubic hair and breasts
- In boys, the increase in size of the testicles and penis and the growth of pubic hair
The pediatrician will compare what he or she finds against the Tanner scale, a 5-point scale that gauges the extent of puberty development in children 7.
After giving a child a complete physical examination and analyzing his or her medical history, a health care provider may perform tests to diagnose precocious puberty, including 8:
- A blood test to check the level of hormones, such as the gonadotropins (luteinizing hormone [LH] and follicle-stimulating hormone [FSH]), estradiol, testosterone, dehydroepiandrosterone sulfate (DHEAS), and thyroid hormones
- A gonadotropin-releasing hormone agonist (GnRHa) stimulation test, which can tell whether a child’s precocious puberty is gonadotropin-dependent or gonadotropin-independent
- Measuring blood 17-hydroxyprogesterone to test for congenital adrenal hyperplasia
- Thyroid testing. The doctor may also test your child’s thyroid if he or she shows any signs of slow thyroid function (hypothyroidism), such as fatigue, sluggishness, increased sensitivity to cold, constipation, a drop in school performance or pale, dry skin.
- A “bone age” X-ray to determine if bones are growing at a normal rate
The health care provider may also use imaging techniques to rule out a tumor or other organ abnormality as a cause.
These imaging methods may include 8:
- Ultrasound (sonography) to examine the gonads. An ultrasound painlessly creates an image on a computer screen of blood vessels and tissues, allowing a health care provider to monitor organs and blood flow in real time
- An MRI (magnetic resonance imaging) scan of the brain and pituitary gland using an instrument that produces detailed images of organs and bodily structures.
Precocious puberty treatment
If your doctor thinks that your child has precocious puberty, he or she may refer you to a pediatric endocrinologist (a doctor who specializes in growth and hormonal disorders in children) for further evaluation and treatment.
Once precocious puberty is diagnosed, the goal of treating it is to stop or even reverse sexual development and stop the rapid growth and bone maturation that can eventually result in adult short stature.
There are a number of reasons to treat precocious puberty 9.
Treatment for precocious puberty can help stop puberty until the child is closer to the normal time for sexual development. One reason to consider treating precocious puberty is that rapid growth and bone maturation, caused by precocious puberty, can prevent a child from reaching his or her full height potential. Children grow rapidly in height during puberty and reach their final adult height after puberty. Children who go through puberty too early may not reach their full adult height potential because their growth stops too soon.
Another reason to consider treating precocious puberty is that a young child may not be psychologically ready for the physical and hormonal changes that occur in puberty.
However, not all children with precocious puberty require treatment, particularly if the onset of puberty is only slightly early. The goal of treatment is to prevent the production of sex hormones to prevent the early halt of growth, short stature in adulthood, emotional effects, social problems, and problems with libido (especially in boys).
If precocious puberty is caused by a specific medical problem, treating the underlying problem can often stop the progression of precocious puberty. In addition, precocious puberty can often be stopped by medical treatment to block the hormones that cause puberty.
Depending upon the cause, there are two possible approaches to treatment:
- treating the underlying cause or disease, such as a tumor
- lowering the high levels of sex hormones with medicine to stop sexual development from progressing
Sometimes, treatment of a related health problem can stop the precocious puberty. But in most cases, no other disease is triggering the condition, so treatment usually involves hormone therapy to stop sexual development.
The currently approved hormone treatment is with drugs called gonadotropin releasing hormone (GnRH) analogues — synthetic hormones that block the body’s production of the sex hormones that cause the early puberty — usually includes a monthly injection of a medication, such as leuprolide (Lupron Depot), which delays further development. Some newer formulations can be given at longer intervals. In 2017, Triptodur was approved by the US Food and Drug Administration (FDA) for pediatric patients ages 2 years and older with central precocious puberty. Triptodur is a gonadotropin releasing hormone (GnRH) analog that is given via intramuscular injection of 22.5 mg once every 24 weeks or twice yearly 10.
Dramatic results are usually seen within a year of starting treatment with an Gn-RH analogue, which is generally safe and usually causes no side effects in kids.
In girls, breast size may decrease — or at least there will be no further development. In boys, the penis and testicles may shrink back to the size expected for their age. Growth in height will also slow down to a rate expected for kids before puberty. A child’s behavior usually becomes more age-appropriate, too.
The child continues to receive this medication until he or she reaches the normal age of puberty. On average, 16 months after he or she stops receiving the medication, the process of puberty begins again.
Treating an underlying medical condition
If another medical condition is causing your child’s precocious puberty, treatment of that condition is necessary to stop the progress of puberty. For example, if a child has a tumor that’s producing hormones and causing precocious puberty, puberty usually will stop when the tumor is surgically removed.
Caring for Your Child
Give your child a simple, truthful explanation about what’s happening. Explain that these changes are normal for older kids and teens, but that his or her body has started developing a little too early. Keep your child informed about treatment and what can be expected along the way.
Also be sure to watch for signs that teasing or other difficulties associated with precocious puberty may be affecting your child’s emotional development.
Common warning signs to discuss with your doctor include:
- poor grades
- problems at school
- loss of interest in daily activities
- depression
How you cope with the issue can also determine how well your child will cope. The goal is to prevent kids from dwelling on sexual development or developing a poor self-image or low self-esteem. To create a supportive environment, try not to focus your comments on appearance. Instead, offer praise for achievements in school or sports and support your child’s participation in other activities.
The important thing to remember is that kids with precocious puberty can be treated. Doctors can help them preserve their adult height potential as well as limit the emotional and social difficulties they may face from maturing early.
- Precocious Puberty. https://rarediseases.org/rare-diseases/precocious-puberty/[↩][↩]
- Precocious puberty. https://medlineplus.gov/ency/article/001168.htm[↩]
- Precocious puberty. https://www.mayoclinic.org/diseases-conditions/precocious-puberty/symptoms-causes/syc-20351811[↩]
- Puberty and Precocious Puberty: Condition Information. https://www.nichd.nih.gov/health/topics/puberty/conditioninfo/default[↩]
- Lavin, N. (2009). Manual of Endocrinology and Metabolism. Lippincott Williams & Williams.[↩]
- Styne, D. M., & Grumbach, M. M. (2008). Puberty: Ontogeny, neuroendocrinology, physiology, and disorders. In Kronenberg, H. M., Melmed, S., Polonsky, K. S., & Larsen, P. R. (Eds.), Williams textbook of endocrinology (11th ed., chap. 24). Philadelphia, PA: Saunders Elsevier.[↩]
- Marshall, W. A., & Tanner, J. M. (1969). Variations in pattern of pubertal changes in girls. Archives of Disease in Childhood, 44, 291–303. [↩]
- Styne D. M., & Grumbach, M. M. (2008) Puberty: Ontogeny, Neuroendocrinology, Physiology, and Disorders. In Kronenberg, H. M., Melmed, S., Polonsky, K. S., & Larsen, P. R. (Eds.), Williams Textbook of Endocrinology (11th ed., chap. 24). Philadelphia, PA: Saunders Elsevier.[↩][↩]
- Long, D. (2015). Precocious Puberty. Pediatrics in Review, 36(7), 319.[↩]
- Triptodur. http://www.triptodur.com/[↩]





{kind=link}