
Contents
What is prolactinoma
Prolactinoma is a benign (noncancerous) pituitary tumor which produces the hormone called prolactin. Prolactinomas are adenomas arising from lactotroph cells in the pituitary gland that secrete prolactin and prolactinomas are the most common type of pituitary tumor and most frequently diagnosed functioning pituitary tumor type, accounting for about 40% of all pituitary adenomas 1. Almost all pituitary tumors are noncancerous (benign). Prolactinoma may occur as part of an inherited condition called multiple endocrine neoplasia type 1 (MEN 1). Symptoms of prolactinoma are caused by hyperprolactinemia too much prolactin in the blood or by pressure of the tumor on surrounding tissues. Prolactinoma tumors come in various sizes, but the vast majority are less than 10mm (<1 cm or 3/8 of an inch) in diameter. These small tumors occur more often in women. Larger tumors are more common in men. They tend to occur at an older age. The tumor can grow to a large size before symptoms appear.
Prolactinoma tumor is often detected at an earlier stage in women than in men because of irregular menstrual periods.
Prolactinomas occur most commonly in people under age 40. Prolactinomas can occur in both men and women, but more often in women than men and rarely occur in children. Most prolactinomas occur in women between 20 and 34 years old. Clinically significant pituitary tumors affect the health of approximately 14 out of 100,000 people.
Prolactin stimulates the breast to produce milk during pregnancy. After giving birth, a mother’s prolactin levels fall unless she breastfeeds her infant, but prolactin receptors have been found in several tissues, including the liver, ovary, testis, and prostate 2. The primary action of prolactin is the initiation and maintenance of lactation, each time the baby nurses, prolactin levels rise to maintain milk production. Moreover, prolactin can act as a growth factor, neurotransmitter, or immunoregulator via autocrine or paracrine mechanisms 3.
Although small benign pituitary tumors are fairly common in the general population, symptomatic prolactinomas are uncommon.
The outlook for prolactinomas depends heavily on the success of medical and surgical therapies. Tests to scan for recurrence following treatment are important.
Very few patients with prolactinomas require surgery, as most prolactinomas (particularly microprolactinomas) shrink in size following treatment with medication. Treat prolactinoma with bromocriptine or cabergoline.
Hormone replace therapy may be required after treatment.
Is osteoporosis a risk in women with high prolactin levels?
Women whose ovaries produce inadequate estrogen are at increased risk for osteoporosis. Hyperprolactinemia can reduce estrogen production. Although estrogen production may be restored after treatment for hyperprolactinemia, even a year or 2 without estrogen can compromise bone strength. Women should protect themselves from osteoporosis by increasing exercise and calcium intake through diet or supplements and by not smoking. Women treated for hyperprolactinemia may want to have periodic bone density measurements and discuss estrogen replacement therapy or other bone-strengthening medications with their doctor.
The pituitary gland
The pituitary gland (hypophysis) is located at the base of the brain where it sits in the middle of the head in a bony box called the sella turcica, where a pituitary stalk (infundibulum) attaches it to the hypothalamus. The gland is about 1 centimeter in diameter and consists of an anterior pituitary or anterior lobe, and a posterior pituitary, or posterior lobe. The pituitary stalk (infundibulum) contains both blood vessels and nerves. The pituitary gland controls a system of hormones in the body that regulate growth, metabolism, the stress response, and functions of the sex organs via the thyroid gland, adrenal gland, ovaries, and testes. The optic nerves sit directly above the pituitary gland. Enlargement of the gland can cause symptoms such as headaches or visual disturbances. Pituitary tumors may also impair production of one or more pituitary hormones, causing reduced pituitary function, also called hypopituitarism.
The pituitary gland, sometimes also called the master gland, because it plays a critical role in regulating growth and development, metabolism, and reproduction. The pituitary gland (hypophysis) produces prolactin and other key hormones including:
- Growth hormone (GH), which regulates growth
- Adrenocorticotropin (ACTH), which stimulates the adrenal glands to produce cortisol, a hormone important in metabolism and the body’s response to stress
- Thyrotropin (TSH or thyroid stimulating hormone), which signals the thyroid gland to produce thyroid hormone, also involved in metabolism and growth
- Luteinizing hormone (LH) and follicle-stimulating hormone (FSH), which regulate ovulation and estrogen and progesterone production in women and sperm formation and testosterone production in men.
Prolactin production and release is mediated via tonic inhibition by dopamine secreted by the hypothalamus.
Figure 1. The pituitary gland location

Figure 2. Pituitary gland
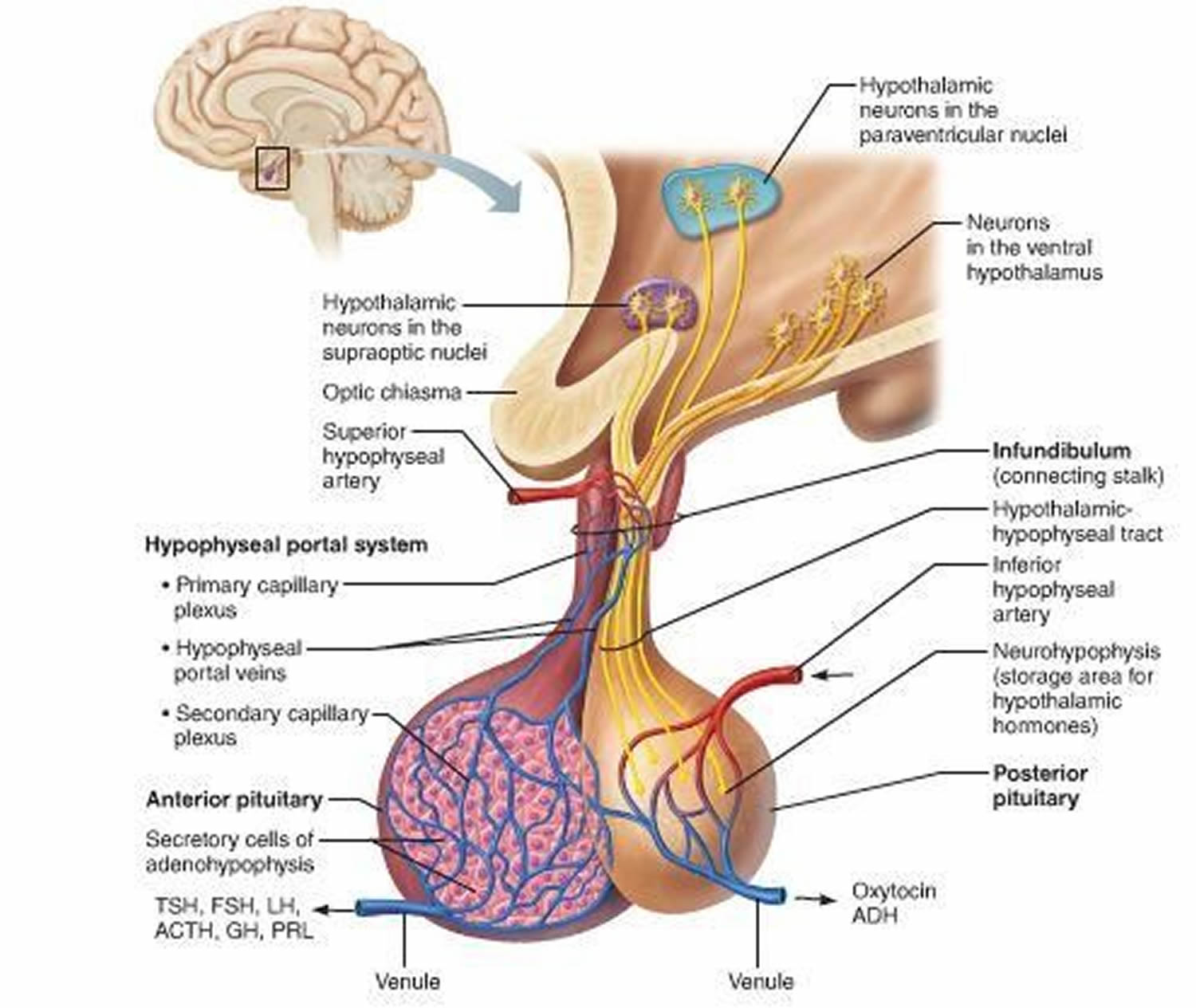
Figure 3. The hypothalamus and pituitary gland (anterior and posterior) endocrine pathways and target organs

Prolactinoma and pregnancy
If a woman has a small prolactinoma, she can usually conceive and have a normal pregnancy after effective medical therapy. If she had a successful pregnancy before, the chance of her having more successful pregnancies is high.
A woman with prolactinoma should discuss her plans to conceive with her physician so she can be carefully evaluated prior to becoming pregnant. This evaluation will include an MRI scan to assess the size of the tumor and an eye examination with measurement of visual fields. As soon as a woman is pregnant, her doctor will usually advise her to stop taking bromocriptine or cabergoline. Although these drugs are safe for the fetus in early pregnancy, their safety throughout an entire pregnancy has not been established. Many doctors prefer to use bromocriptine in patients who plan to become pregnant because it has a longer record of safety in early pregnancy than cabergoline.
Bromocriptine (Parlodel) is an ergoline derivative, a dopamine D2 receptor agonist with agonist and antagonistic properties on D1 receptors. It is generally required to multiple dosing throughout the day because of its short half life 4. In women taking bromocriptine during early pregnancy, the incidence of abortions, ectopic pregnancies, or congenital malformations is no higher than that in the general population 5. In a study of 2,587 pregnant women, out of which 2,437 were to increase the risk of spontaneous abortion, congenital abnormalities, or multiple pregnancies, and did not affect post-natal development 6. In other studies, among 6,329 patients treated with bromocriptine during early pregnancy, the risk of spontaneous abortions was 9.9%, which was not higher than that in the general population (10.9%) 7. Moreover, long-term follow-up to 9 years of children born from mothers taking bromocriptine did not cause detrimental effects on fetal outcomes in term of physical development as well as no psychomotor developmental abnormality reported to 5.5 years (1–20 years) follow-up 8.
Furthermore, optimal outcome was found with continuous use of bromocriptine throughout pregnancy in around 100 cases 9.
Cabergoline (Dostinex) is an ergoline derivative dopamine agonist with higher affinity and selectivity for D2 dopamine receptors. It has long duration of action allowing administration once or twice weekly with better tolerability and patient compliance 10. Moreover, pregnancy rate is higher with cabergoline in infertile women with prolactinoma than with bromocriptine 11.
The same results have been reported in women who were on cabergoline before and during pregnancy 12. In one report, over 800 such pregnancies have been described 13 (of which approximately 350 were exposed during the first weeks of pregnancy), with no significant difference in the frequency of spontaneous abortion, premature delivery, multiple pregnancy, or neonatal malformations 14.
In retrospective study on 103 pregnancies in 90 women with hyperprolactinemia and the follow-up of the 61 children, no significant abnormalities related neither to cabergoline doses nor to the time of exposure 15. Data of 12 years follow-up in the children born from mother treated with cabergoline showed no influence on their post-natal development such as physical problems or of psychomotor retardation 16. In consistent with previous studies, finding from meta-analysis showed no significant increase in the risk of miscarriages or fetal malformation with dopamine agonist used 17.
The pituitary enlarges and prolactin production increases during pregnancy in women without pituitary disorders. Women with prolactin-secreting tumors may experience further pituitary enlargement and must be closely monitored during pregnancy. Less than 3 percent of pregnant women with small prolactinomas have symptoms of tumor growth such as headaches or vision problems. In women with large prolactinomas, the risk of symptomatic tumor growth is greater, and may be as high as 32 percent 18.
The determination of the appropriate treatment option is an individual choice depending mainly on tumor size. The proposed therapeutic approach is shown in Figure 1 19. The outcomes of prolactinomas after pregnancy have been extensively discussed, with variable results. A recent study showed a prolactin normalization rate of more than 40% without medical treatment, for a median follow-up of 22 months after delivery and cessation of lactation 20.
Most endocrinologists see patients every 2 months throughout the pregnancy. A woman should consult her endocrinologist promptly if she develops symptoms of tumor growth-particularly headaches, vision changes, nausea, vomiting, excessive thirst or urination, or extreme lethargy. Bromocriptine or, less often, cabergoline treatment may be reinitiated and additional treatment may be required if the woman develops symptoms during pregnancy.
Figure 1. Approach to managing prolactinomas during pregnancy
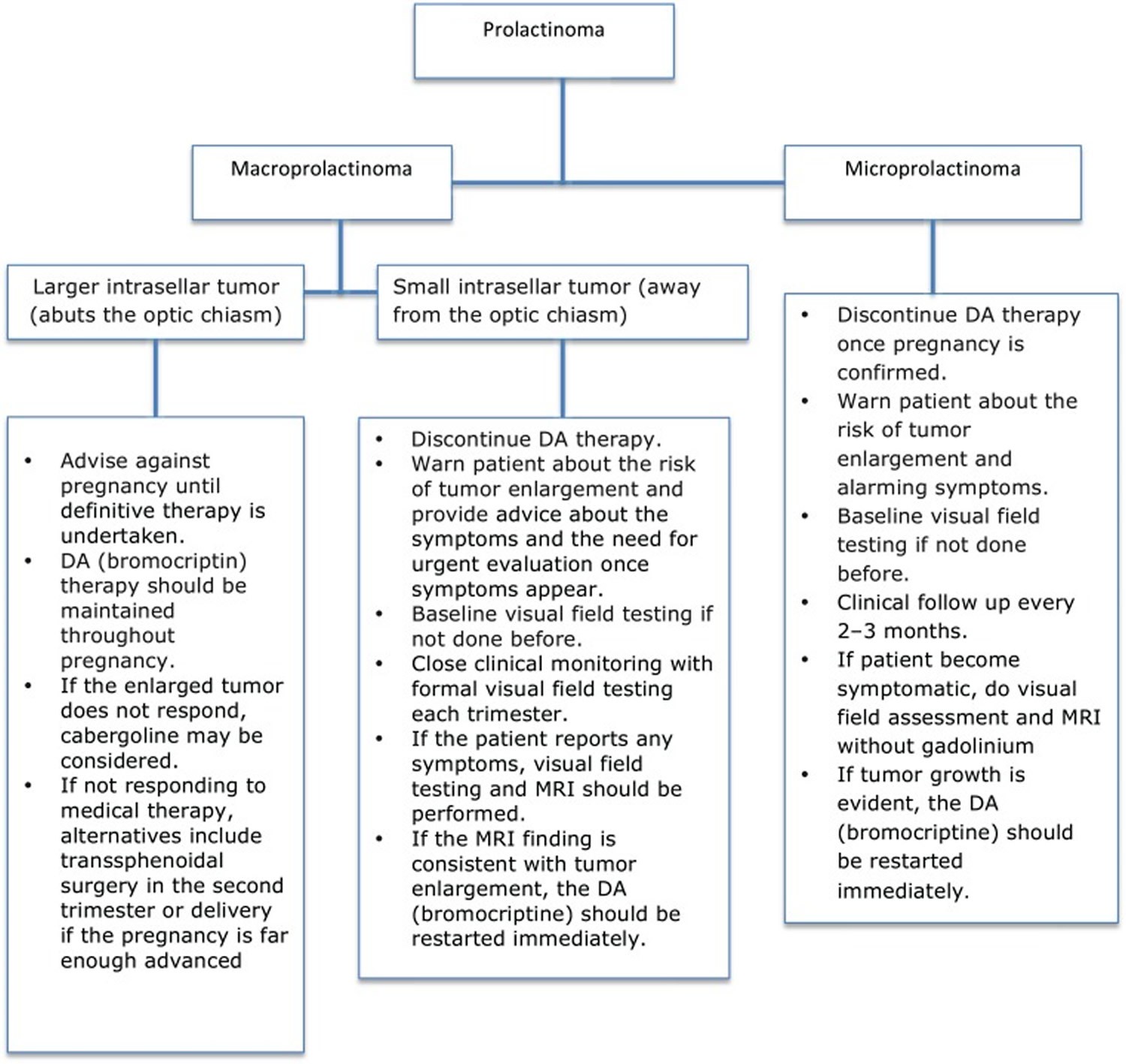
Note: DA = dopamine agonist
[Source 21]Impact of Pregnancy and Breastfeeding on Prolactin Levels, Tumor Volume, and Remission Rate
The current literature demonstrates that pregnancy induces remission of hyperprolactinemia in two-thirds of women after discontinuation of dopamine agonist. In one study, pregnancy has been found to induce remission in 76% of non-tumoral hyperprolactinemia, 70% in microprolactinomas, and 64% in macroprolactinomas with higher recurrence rate among patients with macroprolactinomas and those with microprolactinomas with visible tumor on MRI at the time of treatment withdrawal 22.
In recent study, complete remission was found in 100% with non-tumoral hyperprolactinemia, 66% of patients with microprolactinomas, and 70% with macroprolactinomas 23. Underlying mechanisms are uncertain but have generally been attributed to the autoinfarction of the tumor 23.
On the other hand, there is no data to suggest breastfeeding is associated with an increased prolactin production or risk of tumor enlargement 16. Thus, women could breastfeed normally and restart dopamine agonist after cessation of lactation.
Prolactinoma complications
Complications of prolactinoma may include:
- Vision loss. Left untreated, a prolactinoma may grow large enough to compress your optic nerve.
- Hypopituitarism. With larger prolactinomas, pressure on the normal pituitary gland can cause dysfunction of other hormones controlled by the pituitary, resulting in hypothyroidism, adrenal insufficiency and growth hormone deficiency.
- Bone loss (osteoporosis). Too much prolactin can reduce production of the hormones estrogen and testosterone, resulting in decreased bone density and an increased risk of osteoporosis.
- Pregnancy complications. During a normal pregnancy, a woman’s production of estrogen increases. In a woman with a large prolactinoma, these high levels of estrogen may cause tumor growth and associated signs and symptoms, such as headaches and changes in vision.
If you have prolactinoma and you want to become or are already pregnant, talk to your doctor. Adjustments in your treatment and monitoring may be necessary.
Prolactinoma causes
The cause of pituitary tumors remains largely unknown. Most pituitary tumors are sporadic, meaning they are not genetically passed from parents to their children.
In some people, high blood levels of prolactin can be traced to causes other than pituitary prolactinoma.
Prescription drugs. Prolactin secretion in the pituitary is normally suppressed by the brain chemical dopamine. Drugs that block the effects of dopamine at the pituitary or deplete dopamine stores in the brain may cause the pituitary to secrete prolactin. These drugs include older antipsychotic medications such as trifluoperazine (Stelazine) and haloperidol (Haldol); the newer antipsychotic drugs risperidone (Risperdal) and molindone (Moban); metoclopramide (Reglan), used to treat gastroesophageal reflux and the nausea caused by certain cancer drugs; and less often, verapamil, alpha-methyldopa (Aldochlor, Aldoril), and reserpine (Serpalan, Serpasil), used to control high blood pressure. Some antidepressants may cause hyperprolactinemia, but further research is needed.
Other pituitary tumors. Other tumors arising in or near the pituitary may block the flow of dopamine from the brain to the prolactin-secreting cells. Such tumors include those that cause acromegaly, a condition caused by too much growth hormone, and Cushing’s syndrome, caused by too much cortisol. Other pituitary tumors that do not result in excess hormone production may also block the flow of dopamine.
Hypothyroidism. Increased prolactin levels are often seen in people with hypothyroidism, a condition in which the thyroid does not produce enough thyroid hormone. Doctors routinely test people with hyperprolactinemia for hypothyroidism.
Chest involvement. Nipple stimulation also can cause a modest increase in the amount of prolactin in the blood. Similarly, chest wall injury or shingles involving the chest wall may also cause hyperprolactinemia.
How do oral contraceptives and hormone replacement therapy affect prolactinoma?
Oral contraceptives are not thought to contribute to the development of prolactinomas, although some studies have found increased prolactin levels in women taking these medications. Because oral contraceptives may produce regular menstrual bleeding in women who would otherwise have irregular menses due to hyperprolactinemia, prolactinoma may not be diagnosed until women stop oral contraceptives and find their menses are absent or irregular. Women with prolactinoma treated with bromocriptine or cabergoline may safely take oral contraceptives. Similarly, postmenopausal women treated with medical therapy or surgery for prolactinoma may be candidates for estrogen replacement therapy.
Prolactinoma symptoms
In women, high levels of prolactin in the blood often cause infertility and changes in menstruation. In some women, periods may stop. In others, periods may become irregular or menstrual flow may change. Women who are not pregnant or nursing may begin producing breast milk. Some women may experience a loss of libido-interest in sex. Intercourse may become painful because of vaginal dryness.
In men, the most common symptom of prolactinoma is erectile dysfunction. Because men have no reliable indicator such as changes in menstruation to signal a problem, many men delay going to the doctor until they have headaches or eye problems caused by the enlarged pituitary pressing against nearby optic nerves. They may not recognize a gradual loss of sexual function or libido. Only after treatment do some men realize they had a problem with sexual function.
Prolactinoma symptoms in women:
- Milky discharge from the breasts (galactorrhea) when not pregnant or breast-feeding
- Breast tenderness
- Decreased sexual interest
- Painful intercourse due to vaginal dryness
- Acne and excessive body and facial hair growth (hirsutism)
- Decreased peripheral vision
- Headache
- Infertility
- Irregular menstrual periods (oligomenorrhea) or no menstrual periods (amenorrhea)
- Vision changes
Prolactinoma symptoms in men:
- Decreased sexual interest
- Decreased peripheral vision
- Enlargement of breast tissue (gynecomastia)
- Headache
- Erectile dysfunction (impotence)
- Infertility
- Vision changes
- Decreased body and facial hair
Symptoms caused by pressure from a larger tumor may include:
- Headaches
- Lethargy
- Nasal drainage
- Nausea and vomiting
- Problems with the sense of smell
- Vision changes, such as double vision, drooping eyelids or visual field loss
- Reduction of other hormone production by the pituitary gland (hypopituitarism) as a result of tumor pressure
- Low bone density
- Loss of interest in sexual activity
- Infertility
There may be no symptoms, especially in men. Women tend to notice signs and symptoms earlier than men do, when tumors are smaller in size, probably because they’re alerted by missed or irregular menstrual periods. Men tend to notice signs and symptoms later, when tumors are larger and more likely to cause headache or vision problems.
Prolactinoma diagnosis
A doctor will test for prolactin blood levels in women with unexplained milk secretion, called galactorrhea, or with irregular menses or infertility and in men with impaired sexual function and, in rare cases, milk secretion.
Tests that may be ordered include:
- Pituitary MRI or brain CT scan
- Testosterone level in men
- Prolactin level
- Thyroid function tests
If prolactin levels are high, a doctor will test thyroid function and ask first about other conditions and medications known to raise prolactin secretion. The doctor may also request magnetic resonance imaging (MRI), which is the most sensitive test for detecting pituitary tumors and determining their size. MRI scans may be repeated periodically to assess tumor progression and the effects of therapy. Computerized tomography (CT) scan also gives an image of the pituitary but is less precise than the MRI.
The doctor will also look for damage to surrounding tissues and perform tests to assess whether production of other pituitary hormones is normal. Depending on the size of the tumor, the doctor may request an eye exam with measurement of visual fields.
Prolactinoma treatment
The goals of treatment are to return prolactin secretion to normal, reduce tumor size, correct any visual abnormalities, and restore normal pituitary function. In the case of large tumors, only partial achievement of these goals may be possible.
Prolactinoma medication
Because dopamine is the chemical that normally inhibits prolactin secretion, doctors may treat prolactinoma with the dopamine agonists bromocriptine (Parlodel) or cabergoline (Dostinex). Agonists are drugs that act like a naturally occurring substance. These drugs shrink the tumor and return prolactin levels to normal in approximately 80 percent of patients. Both drugs have been approved by the U.S. Food and Drug Administration for the treatment of hyperprolactinemia. Bromocriptine is the only dopamine agonist approved for the treatment of infertility. This drug has been in use longer than cabergoline and has a well-established safety record.
Nausea and dizziness are possible side effects of bromocriptine. To avoid these side effects, bromocriptine treatment must be started slowly. A typical starting dose is one-quarter to one-half of a 2.5 milligram (mg) tablet taken at bedtime with a snack. The dose is gradually increased every 3 to 7 days as needed and taken in divided doses with meals or at bedtime with a snack. Most people are successfully treated with 7.5 mg a day or less, although some people need 15 mg or more each day. Because bromocriptine is short acting, it should be taken either twice or three times daily.
Bromocriptine treatment should not be stopped without consulting a qualified endocrinologist-a doctor specializing in disorders of the hormone-producing glands. Prolactin levels rise again in most people when the drug is discontinued. In some, however, prolactin levels remain normal, so the doctor may suggest reducing or discontinuing treatment every 2 years on a trial basis.
Cabergoline is a newer drug that may be more effective than bromocriptine in normalizing prolactin levels and shrinking tumor size. Cabergoline also has less frequent and less severe side effects. Cabergoline is more expensive than bromocriptine and, being newer on the market, its long-term safety record is less well defined. As with bromocriptine therapy, nausea and dizziness are possible side effects but may be avoided if treatment is started slowly. The usual starting dose is .25 mg twice a week. The dose may be increased every 4 weeks as needed, up to 1 mg two times a week. Cabergoline should not be stopped without consulting a qualified endocrinologist.
Recent studies suggest prolactin levels are more likely to remain normal after discontinuing long-term cabergoline therapy than after discontinuing bromocriptine. More research is needed to confirm these findings.
In people taking cabergoline or bromocriptine to treat Parkinson’s disease at doses more than 10 times higher than those used for prolactinomas, heart valve damage has been reported. Rare cases of valve damage have been reported in people taking low doses of cabergoline to treat hyperprolactinemia. Before starting these medications, the doctor will order an echocardiogram. An echocardiogram is a sonogram of the heart that checks the heart valves and heart function.
Because limited information exists about the risks of long-term, low-dose cabergoline use, doctors generally prescribe the lowest effective dose and periodically reassess the need for continuing therapy. People taking cabergoline who develop symptoms of shortness of breath or swelling of the feet should promptly notify their physician because these may be signs of heart valve damage.
Common side effects
Nausea and vomiting, nasal stuffiness, headache, and drowsiness are common side effects of these medications. However, these side effects often can be minimized if your doctor starts you with a very low dose of medication and gradually increases the dose.
Cabergoline is the preferred treatment because it appears to be more effective than bromocriptine. It also has less frequent and less severe side effects. However, it’s more expensive than bromocriptine and it’s newer, so its long-term safety record isn’t as well-established.
There have been rare cases of heart valve damage with cabergoline, but usually in people taking much higher doses for Parkinson’s disease. Some people may also develop compulsive behaviors, such as gambling, while taking these medications.
If medication shrinks the tumor significantly and your prolactin level remains normal for two years, you may be able to taper off the medication with your doctor’s guidance. However, recurrence is common. Don’t stop taking your medication without your doctor’s approval.
Prolactinoma surgery
Surgery to remove all or part of the tumor should only be considered if medical therapy cannot be tolerated or if it fails to reduce prolactin levels, restore normal reproduction and pituitary function, and reduce tumor size. If medical therapy is only partially successful, it should be continued, possibly combined with surgery or radiation.
The type of surgery you have will depend largely on the size and extent of your tumor:
- Transsphenoidal surgery. Most people who need surgery have this procedure, in which the tumor is removed through the nasal cavity. Complication rates are low because no other areas of the brain are touched during surgery, and this surgery leaves no visible scars.
- Transcranial surgery. If your tumor is large or has spread to nearby brain tissue, you may need this procedure, also known as a craniotomy. The surgeon reaches the tumor through the upper part of the skull.
Most often, the tumor is removed through the nasal cavity. Rarely, if the tumor is large or has spread to nearby brain tissue, the surgeon will access the tumor through an opening in the skull.
The results of surgery depend a great deal on tumor size and prolactin levels as well as the skill and experience of the neurosurgeon. The higher the prolactin level before surgery, the lower the chance of normalizing serum prolactin. Serum is the portion of the blood used in measuring prolactin levels. In the best medical centers, surgery corrects prolactin levels in about 80 percent of patients with small tumors and a serum prolactin less than 200 nanograms per milliliter (ng/ml). A surgical cure for large tumors is lower, at 30 to 40 percent. Even in patients with large tumors that cannot be completely removed, drug therapy may be able to return serum prolactin to the normal range-20 ng/ml or less-after surgery. Depending on the size of the tumor and how much of it is removed, studies show that 20 to 50 percent will recur, usually within 5 years.
Because the results of surgery are so dependent on the skill and knowledge of the neurosurgeon, a patient should ask the surgeon about the number of operations he or she has performed to remove pituitary tumors and for success and complication rates in comparison to major medical centers. The best results come from surgeons who have performed hundreds or even thousands of such operations. To find a surgeon, contact The Pituitary Society (see For More Information).
Radiation
Rarely, radiation therapy is used if medical therapy and surgery fail to reduce prolactin levels. Depending on the size and location of the tumor, radiation is delivered in low doses over the course of 5 to 6 weeks or in a single high dose. Radiation therapy is effective about 30 percent of the time.
- Ciccarelli A, Daly AF, Beckers A. The epidemiology of prolactinomas. Pituitary (2005) 8(1):3–6.10.1007/s11102-005-5079-0 https://www.ncbi.nlm.nih.gov/pubmed/16411062[↩]
- Inder WJ. Hyperprolactinaemia – differential diagnosis, investigation and management. Eur Endocr Rev (2006):76–1002.[↩]
- Kars M, Dekkers OM, Pereira AM, Romijn JA. Update in prolactinomas. Neth J Med (2010) 68(3):104–12. http://www.njmonline.nl/getpdf.php?id=897[↩]
- Mah PM, Webster J. Hyperprolactinemia: etiology, diagnosis, and management. Semin Reprod Med (2002) 20(4):365–74.10.1055/s-2002-36709 https://www.ncbi.nlm.nih.gov/pubmed/12536359[↩]
- Krupp P, Monka C. Bromocriptine in pregnancy: safety aspects. Klin Wochenschr (1987) 65(17):823–7.10.1007/BF01727477 https://www.ncbi.nlm.nih.gov/pubmed/3657044[↩]
- Webster J. A comparative review of the tolerability profiles of dopamine agonists in the treatment of hyperprolactinaemia and inhibition of lactation. Drug Safety (1996) 14(4):228–38.10.2165/00002018-199614040-00003 https://www.ncbi.nlm.nih.gov/pubmed/8713691[↩]
- Gillam MP, Molitch ME, Lombardi G, Colao A. Advances in the treatment of prolactinomas. Endocr Rev (2006) 27(5):485–534.10.1210/er.2005-9998 https://academic.oup.com/edrv/article/27/5/485/2355195[↩]
- Shibli-Rahhal A, Schlechte J. Hyperprolactinemia and infertility. Endocrinol Metab Clin North Am (2011) 40(4):837–46.10.1016/j.ecl.2011.08.008 https://www.ncbi.nlm.nih.gov/pubmed/22108283[↩]
- Chrisoulidou A, Boudina M, Karavitaki N, Bili E, Wass J. Pituitary disorders in pregnancy. Hormones (2015) 14(1):70–80.10.14310/horm.2002.1575 https://www.ncbi.nlm.nih.gov/pubmed/25885105[↩]
- Colao A, Di Sarno A, Sarnacchiaro F, Ferone D, Di Renzo G, Merola B, et al. Prolactinomas resistant to standard dopamine agonists respond to chronic cabergoline treatment. J Clin Endocrinol Metab (1997) 82(3):876–83.10.1210/jcem.82.8.4178-3 https://www.ncbi.nlm.nih.gov/pubmed/9062500[↩]
- Ono M, Miki N, Amano K, Kawamata T, Seki T, Makino R, et al. Individualized high-dose cabergoline therapy for hyperprolactinemic infertility in women with micro- and macroprolactinomas. J Clin Endocrinol Metab (2010) 95(6):2672–9.10.1210/jc.2009-2605 https://www.ncbi.nlm.nih.gov/pubmed/20357175[↩]
- Ciccarelli E, Grottoli S, Razzore P, Gaia D, Bertagna A, Cirillo S, et al. Long-term treatment with cabergoline, a new long-lasting ergoline derivate, in idiopathic or tumorous hyperprolactinaemia and outcome of drug-induced pregnancy. J Endocrinol Invest (1997) 20(9):547–51.10.1007/BF03348017 https://www.ncbi.nlm.nih.gov/pubmed/9413809[↩]
- Molitch ME. Prolactinoma in pregnancy. Best Pract Res Clin Endocrinol Metab (2011) 25(6):885–96.10.1016/j.beem.2011.05.011 https://www.ncbi.nlm.nih.gov/pubmed/22115164[↩]
- Ricci E, Parazzini F, Motta T, Ferrari CI, Colao A, Clavenna A, et al. Pregnancy outcome after cabergoline treatment in early weeks of gestation. Reprod Toxicol (2002) 16(6):791–3.10.1016/S0890-6238(02)00055-2 https://www.ncbi.nlm.nih.gov/pubmed/12401507[↩]
- Stalldecker G, Mallea-Gil MS, Guitelman M, Alfieri A, Ballarino MC, Boero L, et al. Effects of cabergoline on pregnancy and embryo-fetal development: retrospective study on 103 pregnancies and a review of the literature. Pituitary (2010) 13(4):345–50.10.1007/s11102-010-0243-6 https://www.ncbi.nlm.nih.gov/pubmed/20676778[↩]
- Lebbe M, Hubinont C, Bernard P, Maiter D. Outcome of 100 pregnancies initiated under treatment with cabergoline in hyperprolactinaemic women. Clin Endocrinol (2010) 73(2):236–42.10.1111/j.1365-2265.2010.03808.x https://www.ncbi.nlm.nih.gov/pubmed/20455894[↩][↩]
- Wang AT, Mullan RJ, Lane MA, Hazem A, Prasad C, Gathaiya NW, et al. Treatment of hyperprolactinemia: a systematic review and meta-analysis. Syst Rev (2012) 1:33.10.1186/2046-4053-1-33 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3483691/[↩]
- Gillam MP, Molitch ME, Lombardi G, Colao A. Advances in the treatment of prolactinomas. Endocr Rev (2006) 27(5):485–534.10.1210/er.2005-9998 https://www.ncbi.nlm.nih.gov/pubmed/16705142[↩]
- Imran SA, Ur E, Clarke DB. Managing prolactin-secreting adenomas during pregnancy. Can Fam Physician (2007) 53(4):653–8. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1952594/[↩]
- Domingue ME, Devuyst F, Alexopoulou O, Corvilain B, Maiter D. Outcome of prolactinoma after pregnancy and lactation: a study on 73 patients. Clin Endocrinol (2014) 80(5):642–8.10.1111/cen.12370 https://www.ncbi.nlm.nih.gov/pubmed/24256562[↩]
- Almalki MH, Alzahrani S, Alshahrani F, et al. Managing Prolactinomas during Pregnancy. Frontiers in Endocrinology. 2015;6:85. doi:10.3389/fendo.2015.00085. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4443771/[↩]
- Colao A, Di Sarno A, Cappabianca P, Di Somma C, Pivonello R, Lombardi G. Withdrawal of long-term cabergoline therapy for tumoral and nontumoral hyperprolactinemia. N Engl J Med (2003) 349(21):2023–33.10.1056/NEJMoa022657 https://www.ncbi.nlm.nih.gov/pubmed/14627787[↩]
- Auriemma RS, Perone Y, Di Sarno A, Grasso LF, Guerra E, Gasperi M, et al. Results of a single-center observational 10-year survey study on recurrence of hyperprolactinemia after pregnancy and lactation. J Clin Endocrinol Metab (2013) 98(1):372–9.10.1210/jc.2012-3039 https://www.ncbi.nlm.nih.gov/pubmed/23162092[↩][↩]





{kind=link}