Contents
What is pseudomembranous colitis
Pseudomembranous colitis, also known as antibiotic-associated diarrhea, is an inflammatory condition of the colon characterized by elevated yellow-white plaques that coalesce to form pseudomembranes on the mucosa 1. Pseudomembranous colitis is commonly a manifestation of severe colonic disease that is usually associated with Clostridium difficile infection as a result of the use of broad-spectrum antibiotics, but can be caused by a number of different etiologies. The use of broad spectrum antibiotics – especially ampiciliin and clindamycin, although any broad-specturm antibiotic has the potential to cause it. These broad-spectrum antibiotics affect the normal bowel flora of the bowel, leading to overgrowth of the bacterium Clostridium difficile, which causes the colitis. Around 3-10% of adults receiving antibiotics will get diarrhoea as a result of pseudomembranous colitis. Prior to the use of broad-spectrum antibiotics, pseudomembranous colitis was more frequently related with ischemic disease, obstruction, sepsis, uremia, and heavy metal poisoning 2. Clostridium difficile is more common in people who need to take antibiotics for a long period of time.The elderly also have a higher risk of getting it. The infection can spread in hospitals and nursing homes.
The list of associated causes is vast, although Clostridium difficile infection is still the most common cause. Symptoms usually occur 5-10 days after ingesting antibiotics.
Symptoms of pseudomembranous colitis include:
- Watery or bloody diarrhea;
- Pus or mucus in your stool;
- Abdominal cramps;
- Loss of appetite;
- Abdominal pain or tenderness;
- Nausea;
- Fever;
- Dehydration.
Most pseudomembranous colitis cases are mild complaints and resolve on stopping the antibiotics. More severe cases result in protracted diarrhoea, and if untreated, can be severe.
On endoscopic examination, pseudomembranous colitis is characterized by elevated yellow-white nodules or plaques that form pseudomembranes on the mucosal surfaces of the colon (see Figure 1) 3. Endothelial damage from the initial event or disease process causes small areas of necrosis in the surface epithelium. The eruption of neutrophils, nuclear debris, and other inflammatory elements from the lamina propria onto the epithelium then leads to pseudomembrane formation 4. Pseudomembranes can be up to two centimeters in diameter, scattered among areas of normal or erythematous mucosa; however, confluent pseudomembranes that cover the entirety of the mucosa can be seen in severe disease 4.
Pseudomembranous colitis is easily treated with the discontinuation of the offending antibiotic and use of a specific antibiotic against Clostridium difficile. The disease can be severe if untreated, however, and in some it can relapse after treatment. Rarely, they are severe enough to need surgery.
Figure 1. Pseudomembranous colitis – flexible sigmoidoscopy showing diffuse pseudomembranes covering severely edematous and friable mucosa in the rectosigmoid colon in a patient with Clostridium difficile infection.
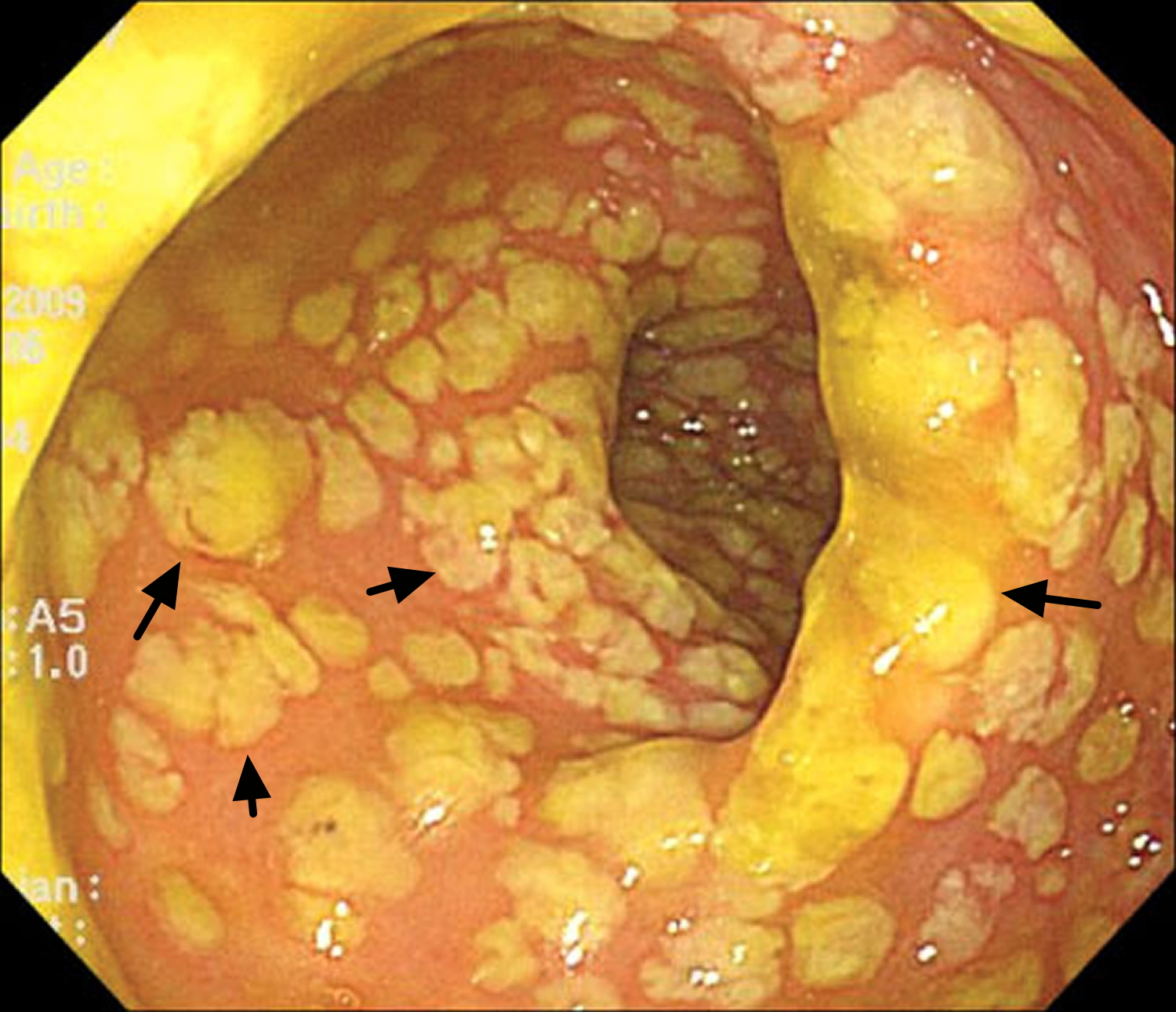
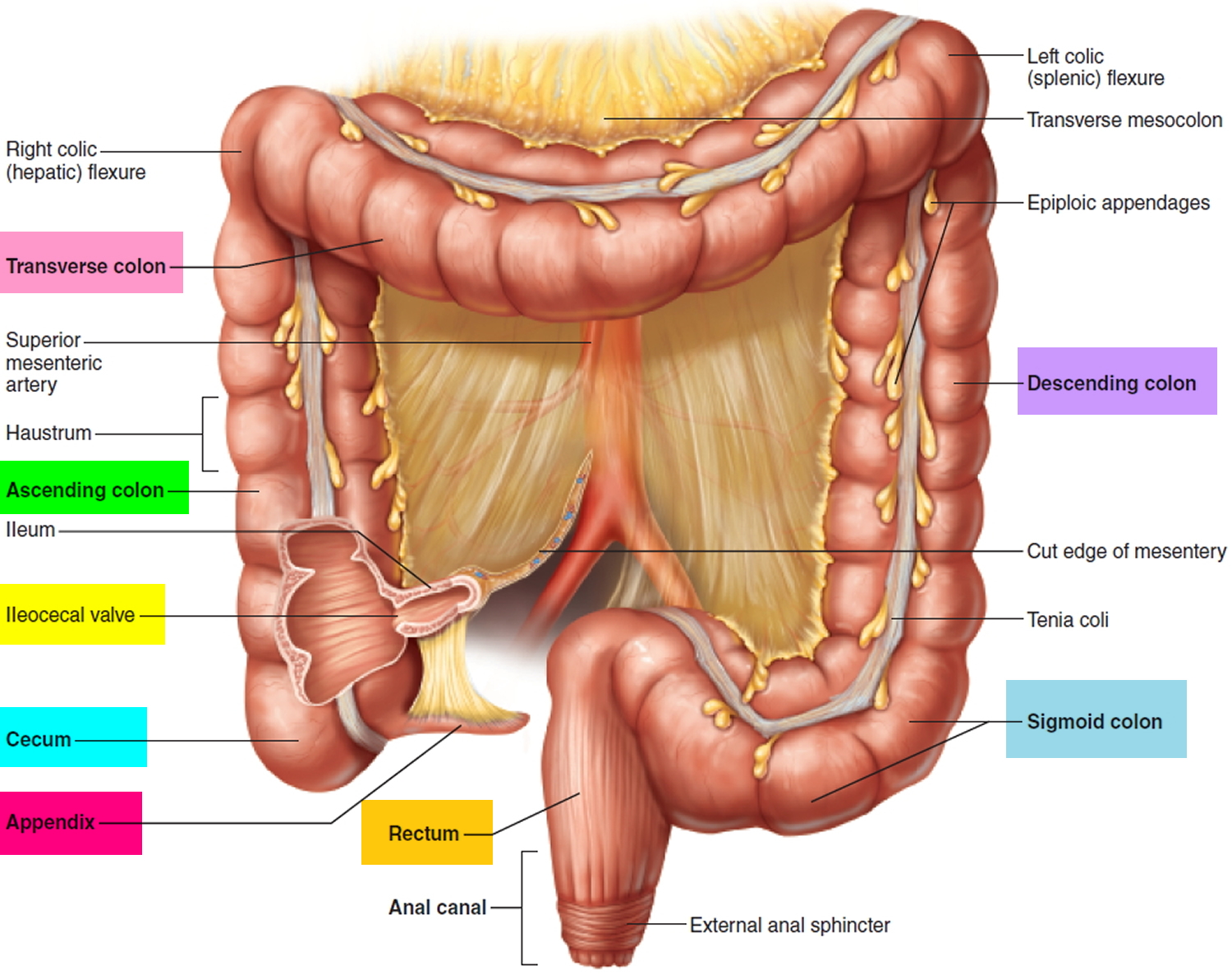
Figure 2. Large intestine (colon)
 Classification of pseudomembranous lesions can be made based on the degree and depth of inflammatory changes, with grading of lesions from type 1 (“summit lesions”, focal surface epithelial inflammation or necrosis) to type 3 (complete mucosal necrosis and significant inflammatory debris). Histologic examination of biopsy samples vary based on the underlying cause, disease severity, and time course of the disease, which can make identification of the inciting trigger challenging.
Classification of pseudomembranous lesions can be made based on the degree and depth of inflammatory changes, with grading of lesions from type 1 (“summit lesions”, focal surface epithelial inflammation or necrosis) to type 3 (complete mucosal necrosis and significant inflammatory debris). Histologic examination of biopsy samples vary based on the underlying cause, disease severity, and time course of the disease, which can make identification of the inciting trigger challenging.
What is Clostridium difficile?
Clostridium difficile is a Gram-positive, spore-forming bacterium usually spread by the fecal-oral route. Clostridium difficile is non-invasive and produces toxins A and B that cause disease, ranging from asymptomatic carriage, to mild diarrhea, to colitis, or pseudomembranous colitis. Clostridium difficile infection is defined as the acute onset of diarrhea with documented toxigenic Clostridium difficile or its toxin and no other documented cause for diarrhea 5. Patients with Clostridium difficile infection typically have extended lengths-of-stay in hospitals, and Clostridium difficile infection is a frequent cause of large hospital outbreaks of disease with costs of $3.2 billion dollars annually. This guideline provides recommendations for the diagnosis and management of patients with Clostridium difficile infection as well as for the prevention and control of outbreaks while supplementing previously published guidelines. New molecular diagnostic stool tests will likely replace current enzyme immunoassay tests.
Rates of Clostridium difficile infection have been increasing since 2000, especially in the elderly with a recent hospitalization or residing in long-term care facility 6. Carriage of Clostridium difficile occurs in 5–15% of healthy adults, but may be as high as 84.4% in newborns and healthy infants, and up to 57% in residents in long-term care facility. Transmission in health-care facilities results mostly from environmental surface contamination and hand carriage by staff members and infected patients.
The two biggest risk factors are exposure to antibiotics and exposure to the organism; others are comorbid conditions, gastrointestinal tract surgery, and medications that reduce gastric acid, including proton-pump inhibitors 7.
Pseudomembranous colitis complications
Treatment of pseudomembranous colitis is usually successful. However, even with prompt diagnosis and treatment, pseudomembranous colitis can be life-threatening. Possible complications include:
- Abnormally low levels of potassium in your blood (hypokalemia), due to the loss of potassium during excessive diarrhea
- Dehydration leading to abnormally low blood pressure (hypotension), related to significant loss of fluids and electrolytes due to diarrhea
- Kidney failure, due to severe dehydration resulting from diarrhea
- A hole in your bowel (perforated colon), which can lead to an infection of your abdominal cavity
- Toxic megacolon, a rare but serious swelling of the colon, leaving it incapable of expelling gas and stool, which could cause your colon to rupture
In addition, pseudomembranous colitis may sometimes return, days or even weeks after apparently successful treatment.
Pseudomembranous colitis causes
Usually, your body keeps the many bacteria in your colon in a naturally healthy balance. However, antibiotics and other medications can upset this balance. Pseudomembranous colitis occurs when certain bacteria — usually Clostridium difficile — rapidly outgrow other bacteria that normally keep them in check. Certain toxins produced by Clostridium difficile, which are usually present in only tiny amounts, rise to levels high enough to damage the colon.
While almost any antibiotic can cause pseudomembranous colitis, some antibiotics are more likely to cause pseudomembranous colitis than others:
- Fluoroquinolones, such as ciprofloxacin (Cipro) and levofloxacin (Levaquin)
- Penicillins, such as amoxicillin and ampicillin
- Clindamycin (Cleocin)
- Cephalosporins, such as cefixime (Suprax)
Other medications
Other medications besides antibiotics can sometimes cause pseudomembranous colitis. Chemotherapy drugs that are used to treat cancer may disrupt the normal balance of bacteria in the colon.
Medications/chemicals
- Alosetron
- Cisplatin
- Cocaine
- Cyclosporine A
- Dextroamphetamine
- Docetaxel
- 5-Fluorouracil
- Gold
- Glutaraldehyde
- NSAIDs
- Paraquat
Certain diseases that affect the colon, such as ulcerative colitis or Crohn’s disease, may also predispose people to pseudomembranous colitis.
Clostridium difficile spores are resistant to many common disinfectants and can be transmitted from the hands of health care professionals to patients. Increasingly, Clostridium difficile has been reported in people with no known risk factors, including people with no recent health care contact or use of antibiotics. This is called community-acquired Clostridium difficile.
Infectious causes
Bacterial
- Clostridium difficile
- Clostridium ramosum
- Escherichia coli O157:H7
- Klebsiella oxytoca
- Plesiomonas shigelloides
- Salmonella enterica
- Shigella species
- Staphylococcus aureus
- Yersinia enterocolitica
Parasites
- Entamoeba histolytica
- Schistosoma mansoni
- Strongyloides stercoralis
Virus
- Cytomegalovirus
Other colitis
- Behcet’s disease
- Collagenous colitis
- Inflammatory bowel disease
- Ischemic colitis
Risk factors for pseudomembranous colitis
Factors that may increase your risk of pseudomembranous colitis include:
- Taking antibiotics
- Staying in the hospital or a nursing home
- Increasing age, especially over 65 years
- Having a weakened immune system
- Having a colon disease, such as inflammatory bowel disease or colorectal cancer
- Undergoing intestinal surgery
- Receiving chemotherapy treatment for cancer
Pseudomembranous colitis symptoms
Signs and symptoms of pseudomembranous colitis may include:
- Watery or bloody diarrhea;
- Pus or mucus in your stool;
- Abdominal cramps;
- Loss of appetite;
- Abdominal pain or tenderness;
- Nausea;
- Fever;
- Dehydration
Symptoms of pseudomembranous colitis can begin as soon as one to two days after you start taking an antibiotic, or as long as several weeks after you finish taking the antibiotic.
Pseudomembranous colitis diagnosis
The best standard laboratory test for Clostridium difficile infection diagnosis has not been clearly established. For the past 30 years, the two primary reference tests are the Clostridium difficile cytotoxin neutralization assay and toxigenic culture 8. Clostridium difficile culture alone is not sufficient because not all Clostridium difficile strains produce toxin 9.
Tests and procedures used to diagnose pseudomembranous colitis and to search for complications include:
- Stool sample. Only stools from patients with diarrhea should be tested for Clostridium difficile. There are a number of different stool sample tests used to detect Clostridium difficile infection of the colon.
- Nucleic acid amplification tests for Clostridium difficile toxin genes such as PCR (polymerase chain reaction) are superior to toxins A+B enzyme immunoassay testing as a standard diagnostic test for Clostridium difficile infection.
- Glutamate dehydrogenase screening tests for C difficile can be used in two- or three-step screening algorithms with subsequent toxin A and B enzyme immunoassay testing, but the sensitivity of such strategies is lower than nucleic acid amplification tests.
- Because Clostridium difficile carriage is increased in patients on antimicrobial therapy, only diarrheal stools warrant testing 5. Very occasionally, a patient with ileus and complicated disease will have a formed stool 5, in which case the laboratory should be made aware of this special clinical situation. Rectal swabs can be used for PCR and thus may be useful in timely diagnosis of patients with ileus 10.
- Routine stool cultures.
- Full blood count. These may reveal an abnormally high white blood cell count (leukocytosis), which may indicate pseudomembranous colitis.
- Urea and electrolytes – dehydration. Low potassium and acidosis may develop.
- Albumin – low blood albumin levels due to stool protein losses.
- Colonoscopy or sigmoidoscopy. In both of these tests, your doctor uses a tube with a miniature camera at its tip to examine the inside of your colon for signs of pseudomembranous colitis — raised, yellow plaques (lesions), as well as swelling.
- Imaging tests. If you have severe symptoms, your doctor may obtain an abdominal X-ray or an abdominal CT scan to look for complications such as toxic megacolon or colon rupture.
Table 1. Diagnostic testing for Clostridium difficile
| Test | Sensitivity | Specificity | Availability | Expensea | Utilization |
|---|---|---|---|---|---|
| C. difficile culture | Low | Moderate | Limited | $5–10 | No diagnostic use; only toxigenic organisms cause disease |
| Toxigenic culture | High | High | Limited | $10–30 | Reference method Epidemiologic tool Limited diagnostic use |
| CCNA | High | High | Limited | $15–25 | Reference method Limited diagnostic use |
| GDH | High | Low | Widely | $5–15 | Diagnostically as a screening test; must be confirmed |
| Toxin EIA tests | Low | High | Widely | $5–15 | Must detect toxins A+B; inferior sensitivity |
| NAATs | High | High | Widely | $20–50 | Use only in acute disease; false positives of concern |
| CCNA, Clostridium difficile cytotoxin neutralization assay; GDH, glutamate dehydrogenase; EIA, enzyme immunoassay; NAAT, nucleic acid amplification tests. a Cost of goods; does not reflect laboratory changes. | |||||
Glutamate dehydrogenase (GDH) is an enzyme produced by Clostridium difficile in relatively large amounts compared with toxins A and B 11. Although glutamate dehydrogenase (GDH) is sensitive, it is not as specific for Clostridium difficile infection, because this enzyme is produced by both toxigenic and non-toxigenic organisms. Additionally, antibodies against Clostridium difficile glutamate dehydrogenase (GDH) may cross react with the same enzyme in other clostridial species 12. Reports and meta-analyses detail sensitivity ranging from 75% to >90% with a negative predictive value of between 95% and 100%, although its positive predictive values have been found to be as low as 50% 13. The sensitivity of glutamate dehydrogenase antigen detection has led to its use as a screening test as part of Clostridium difficile infection testing algorithms, although it should be noted that as many as 10% of patients with toxigenic organisms can be missed by this method. In this approach, glutamate dehydrogenase (GDH) is the initial test, and glutamate dehydrogenase (GDH)-negative specimens are reported as negative with no further testing done. Glutamate dehydrogenase (GDH)-positive specimens must undergo additional testing for C. difficile either by nucleic acid amplification test or by enzyme immunoassay testing followed by nucleic acid amplification test if the enzyme immunoassay results are discordant 14.
Evidence suggests that nucleic acid amplification tests for toxigenic Clostridium difficile are good stand-alone tests for toxigenic Clostridium difficile. There are several Food and Drug Administration (FDA)-approved nucleic acid amplification test’s, including PCR assays and isothermal amplification tests. PCR is an excellent confirmatory test, but data for isothermal amplification testing are not yet sufficient to recommend it.
Clinical practice guidelines have evolved over the past 3 years to suggest the following diagnostic approaches 15.
- (1) Glutamate dehydrogenase (GDH) screen followed by a confirmatory test in two- or three-step algorithms.
- (2) Nucleic acid amplification test for toxigenic Clostridium difficile, but only in patients with documented diarrhea. Their use in any other clinical setting may yield false positive test results.
- (3) Enzyme immunoassay for toxin A+B lacks sensitivity compared with Clostridium difficile cytotoxin neutralization assay and toxigenic culture and should not be used as a stand-alone test. More information on microbiological testing is in the appendix.
Several studies have shown that repeat testing after a negative test is positive in <5% of specimens and repeat testing increases the likelihood of false positives 16. If repeat testing is requested, the physician should confer with the laboratory to explain the clinical rationale. There is no evidence that repeated testing can enhance the sensitivity or negative predictive values of nucleic acid amplification tests for Clostridium difficile diagnosis compared with toxigenic cultures. Empiric therapy for Clostridium difficile infection should not be discontinued or withheld in patients with a high pre-test suspicion for Clostridium difficile infection. Studies have shown that both toxin A+B enzyme immunoassay and toxigenic culture may remain positive for a long as 30 days in patients who have resolution of symptoms 17. False positive “test of cure” specimens may complicate clinical care and result in additional courses of inappropriate anti-Clostridium difficile therapy.
Pseudomembranous colitis treatment
Treatment strategies include:
- Stopping the antibiotic or other medication that’s thought to be causing your signs and symptoms, if possible. Sometimes, this may be enough to resolve your condition or at least ease signs, such as diarrhea.
- If a patient has a strong pre-test suspicion for Clostridium difficile infection, empiric therapy for Clostridium difficile infection should be considered regardless of the laboratory testing result, as the negative predictive values for Clostridium difficile infection are insufficiently high to exclude disease in these patients.
- Starting an antibiotic likely to be effective against Clostridium difficile. If you still experience signs and symptoms, your doctor may use a different antibiotic to treat Clostridium difficile. This allows the normal bacteria to grow back, restoring the healthy balance of bacteria in your colon. You may be given antibiotics by mouth, through a vein or through a tube inserted through the nose into the stomach (nasogastric tube). Depending on your condition, doctors will use most often use metronidazole (Flagyl), vancomycin, fidaxomicin (Dificid) or a combination to eradicate the organisms.
- Patients with mild-to-moderate Clostridium difficile infection should be treated with metronidazole 500 mg orally three times per day for 10 days 6. Failure to respond to metronidazole therapy within 5–7 days should prompt consideration of a change in therapy to vancomycin at standard dosing.
- Metronidazole treatment should be avoided in pregnancy and breast feeding. First trimester exposure to metronidazole is not recommended in FDA guidelines because of concern regarding ready placental transmission and case reports describing facial anomalies following exposure. Metronidazole and its active metabolites are readily detected in breast milk and in the plasma of infants.
- Patients with severe Clostridium difficile infection should be treated with vancomycin 125 mg orally four times per day for 10 days 6.
- Oral vancomycin cannot reach segments of colon that are not in continuity with the gastrointestinal tract, such as the patient with an upstream ileostomy, Hartman’s pouch, or colostomy. In patients in whom oral antibiotics cannot reach a segment of the colon, such as with Hartman’s pouch, ileostomy, or colon diversion, vancomycin therapy delivered via enema should be added to treatments above until the patient improves. When Clostridium difficile infection is documented in an excluded segment of diverted colon, administration of vancomycin by enema is recommended to guarantee that treatment will reach the affected area, using vancomycin enemas of 500 mg in 100–500 ml of normal saline every 6 hour for Clostridium difficile infection 18, volume depending on length of segment to be treated. The duration of enema therapy should continue until the patient has significant improvement.
- Oral cholestyramine to help bind the toxin of Clostridium difficile.
- The use of anti-peristaltic agents to control diarrhea from confirmed or suspected Clostridium difficile infection should be limited or avoided, as they may obscure symptoms and precipitate complicated disease. Use of anti-peristaltic agents in the setting of Clostridium difficile infection must always be accompanied by medical therapy for Clostridium difficile infection.
- Having fecal microbial transplantation. If your condition is extremely severe, you may be given a transplant of stool (fecal transplant) from a healthy donor to restore the balance of bacteria in your colon. The donor stool may be delivered through a nasogastric tube, inserted into the colon or placed in a capsule you swallow. Often, doctors will use a combination of antibiotic treatment followed by fecal microbial transplantation.
Once you begin treatment for pseudomembranous colitis, signs and symptoms may begin to improve within a few days.
Researchers are exploring new treatments for pseudomembranous colitis, including alternative antibiotics and a vaccine.
Summary of the first-line antibiotics evidence
The two first-line antibiotics used most often to treat Clostridium difficile infection in North America are metronidazole and vancomycin; a third, fidaxomicin, was approved for treatment of Clostridium difficile infection in 2011. Treatment for Clostridium difficile infection can be initiated before laboratory confirmation for patients with a high pre-test suspicion of disease. Two older randomized control trials that compared vancomycin and metronidazole for treatment of Clostridium difficile infection did not demonstrate superiority of metronidazole compared with vancomycin 19. However, two more recent randomized control trials concluded vancomycin is superior to metronidazole for patient with severe Clostridium difficile infection 20. In one, 150 patients were stratified by an ad-hoc definition of Clostridium difficile infection severity and then randomized to oral metronidazole or vancomycin 20. Clinical cure was defined as a negative follow-up toxin assay and absence of diarrhea on day 6 of therapy. Using this definition, 90% of patients treated with metronidazole and 98% treated with vancomycin were cured of mild Clostridium difficile infection, but cure rates were lower in the severe disease group treated with metronidazole (76%) compared with vancomycin (97%). Although widely cited as evidence that vancomycin is superior to metronidazole for the treatment of severe Clostridium difficile infection, this study has potential limitations, including nonstandard dose of metronidazole and using an invalidated definition of cure (a negative follow-up toxin assay) when metronidazole is known to be inferior to vancomycin for microbiological end points during Clostridium difficile infection therapy 21. Most importantly, the definition of mild Clostridium difficile infection in the trial included many patients who would be considered as having severe Clostridium difficile infection by the proposed definition based on cohort studies in this treatment guideline.
Although the continued preference for metronidazole as the treatment of choice in mild-to-moderate Clostridium difficile infection is based on equal efficacy for most patients, an additional and important reason remains cost. Oral vancomycin costs $71 to 143 per day (depending on the dosing regimen chosen) compared with metronidazole, which costs $2 per day. Although the intravenous formulation of vancomycin can be compounded by inpatient hospital pharmacies and some outpatient pharmacies at approximately half this cost, the cost difference remains substantial and can impair compliance. Another reason that vancomycin is not used in the inpatient setting is the theoretical risk of promoting acquisition of vancomycin-resistant enterococcus. However, vancomycin-resistant enterococcus has not been shown to be a valid reason to avoid use of vancomycin for treatment of Clostridium difficile infection, as both vancomycin and metronidazole treatment for Clostridium difficile infection have been shown to promote vancomycin-resistant enterococcus acquisition in prospective observational studies 21.
Although it is common practice to prescribe 10–14 days of treatment for Clostridium difficile infection, treatment duration is 10 days in all the previous randomized control trials of both metronidazole and vancomycin. Because there is no evidence that supports longer treatment durations as more efficacious, the use of 14-day treatment courses is not recommended for the initial treatment of mild-to-moderate Clostridium difficile infection when a treatment response has been observed by day 10. There is also no evidence to support the practice of extending anti-Clostridium difficile infection therapy for the duration of therapy if the patient is also on a non-Clostridium difficile infection antibiotic.
An alternate antibiotic is fidaxomicin (200 mg orally 2 times per day for 10 days) for the treatment of mild-to-moderate Clostridium difficile infection. On the basis of two randomized control trials with oral vancomycin, the FDA granted approval for fidaxomicin in May 2011 22. In both published phase III trials, fidaxomicin demonstrated non-inferiority to vancomycin in the modified intention-to-treat and the per-protocol analyses for clinical response at the end of therapy and at 25 days post therapy. Further post-hoc analyses suggested that fidaxomicin is superior to vancomycin as there were fewer recurrences at 25 days after therapy. However, this superiority was seen only with initial infections not caused by NAP1/BI/027 where fidaxomicin was associated with a 16.9 and 19.6% risk reduction for recurrence in the two trials, which translates to a number needed to treat of 5–6 patients with non-/NAP1/BI/027 Clostridium difficile infection treated with fidaxomicin to prevent one recurrence.
There are several important limitations to these findings. First, neither trial extended to 90 days, the full extent needed to document recurrences by identical strains. Second, there is no biological plausibility to explain a strain-specific superiority of fidaxomicin; there are no differences in minimal inhibitory concentrations between NAP1/BI/027 and non-NAP1/BI/027 strains, and both vancomycin and fidaxomicin have similar spectra of activity against Gram-positive stool bacteria. Third, surveillance testing in a patient on the fidaxomicin study arm has already revealed the evolution of a Clostridium difficile strain with an elevated minimal inhibitory concentration to fidaxomicin due to a mutation in RNA polymerase B. Resistance to vancomycin in vitro has not been observed in vancomycin trials to date. Finally, the cost of fidaxomicin is significantly higher than that of vancomycin. Given the limited data available, researchers urge caution in committing patients to a course of this drug before more definitive evidence of superiority in post-marketing clinical trials.
Table 2. Clostridium difficile infection severity scoring system and summary of recommended treatments
| Severity | Criteria | Treatment | Comment |
|---|---|---|---|
| Mild-to-moderate disease | Diarrhea plus any additional signs or symptoms not meeting severe or complicated criteria | Metronidazole 500mg orally three times a day for 10 days. If unable to take metronidazole, vancomycin 125 mg orally four times a day for 10 days | If no improvement in 5–7 days, consider change to vancomycin at standard dose (vancomycin 125mg four times a day for 10 days) |
| Severe disease | Serum albumin <3g/dl plus ONE of the following: WBC ≥15,000 cells/mm3, Abdominal tenderness | Vancomycin 125 mg orally four times a day for 10 days | |
| Severe and complicated disease | Any of the following attributable to CDI: Admission to intensive care unit for CDI Hypotension with or without required use of vasopressors Fever ≥38.5 °C Ileus or significant abdominal distention Mental status changes WBC ≥35,000 cells/mm3 or <2,000 cells/mm3 Serum lactate levels >2.2 mmol/l End organ failure (mechanical ventilation, renal failure, etc.) | Vancomycin 500 mg orally four times a day and metronidazole 500 mg IV every 8 h, and vancomycin per rectum (vancomycin 500 mg in 500 ml saline as enema) four times a day | Surgical consultation suggested |
| Recurrent CDI | Recurrent CDI within 8 weeks of completion of therapy | Repeat metronidazole or vancomycin pulse regimen | Consider FMT after 3 recurrences |
| CDI, Clostridium difficile infection; FMT, fecal microbiota transplant; IV, intravenous; WBC, white blood cell. | |||
Treating recurring pseudomembranous colitis
The natural occurrence of new, more-aggressive strains of Clostridium difficile, which are more resistant to antibiotics, has made treating pseudomembranous colitis increasingly difficult and recurrences more common. With each recurrence, your chance of having an additional recurrence increases. Treatment options may include:
- Repeat antibiotics. You may need a second or third round of antibiotics to resolve your condition.
- Surgery. Surgery may be an option in people who have progressive organ failure, rupture of the colon and inflammation of the lining of the abdominal wall (peritonitis). Surgery has typically involved removing all or part of the colon (total or subtotal colectomy). A newer surgery that involves laparoscopically creating a loop of colon and cleaning it (diverting loop ileostomy and colonic lavage) is less invasive and has had positive results.
- Fecal microbial transplantation. Fecal microbial transplantation is used to treat recurrent pseudomembranous colitis. You’ll receive healthy, cleaned stool in a capsule, nasogastrically or inserted into your colon.
The first recurrence of Clostridium difficile infection can be treated with the same regimen that was used for the initial episode. If severe, however, vancomycin should be used. The second recurrence should be treated with a pulsed vancomycin regimen.
Repeat courses of antibiotics, usually metronidazole or vancomycin are necessary to treat recurring pseudomembranous colitis; both have similar recurrence rates. Re-treatment with a 10–14-day regimen is common. Use of vancomycin is recommended for repeated recurrences because of the risk of neuropathy with repeated administration of metronidazole 5. The use of vancomycin, 125 mg four times daily for 10 days, is preferred for any recurrence if it is severe, even if the initial episode had been treated with metronidazole. If the initial episode was treated with vancomycin, a tapered and pulsed regimen or just a pulsed regimen of vancomycin may be considered; none of these recommendations for extended vancomycin regimens have been studied in randomized control trials. Evidence that longer, tapered, pulsed-dosing is more effective than conventional regimens comes from evaluation of placebo-treated patients in a trial of a probiotic adjunct to antibiotic therapy in patients who already had one or more recurrences. Patients who had a standard 10–14-day course had recurrence rates of up to 54%, compared with 31% in those who had tapering regimens (gradually lowered doses) and 14% in those who had pulsed (every 2–3 day) regimens 23. There are no controlled data to support specific tapering or pulse regimens 24. We here propose a simple cost-effective regimen: a standard 10-day course of vancomycin at a dose of 125 mg given four times daily, followed by 125 mg daily pulsed every 3 days for ten doses. There is no convincing evidence of efficacy of other antibiotics, such as rifampin or rifaximin. In one study, six of seven patients responded to treatment with vancomycin and rifampin 25. In three small series, a total of 16 of 20 patients had no further recurrences when treated with 2 weeks of rifaximin after a 2-week course of vancomycin 26; a recently published randomized control trial of this regimen did not find a decrease in documented Clostridium difficile infection recurrences with rifaximin 27. Moreover, high-level resistance to rifampin is a concern and should limit its use 28.
If there is a third recurrence after a pulsed vancomycin regimen, fecal microbiota transplant (FMT) should be considered.
Fecal microbiota transplant is the term used when stool is taken from a healthy individual and instilled into a sick person to cure a certain disease 29. Studies show that patients with recurrent Clostridium difficile infection have abnormally proportioned colon microbiota, and that reintroduction of normal bacteria via donor feces corrects this imbalance, restoring phylogenetic richness and colonization resistance.
The first documented use of fecal microbiota transplant in the English language was a case series of four patients with pseudomembranous enterocolitis, three of whom were critically ill; fecal enemas (donated by the residents caring for the patients) were administered as an adjunct to antibiotic treatment; all four patients had resolution of symptoms within hours of fecal microbiota transplant 30. The first documented case of confirmed recurrent Clostridium difficile infection treated with fecal microbiota transplant was reported in 1983 in a 65-year-old woman who had “prompt and complete normalization of bowel function” 31. Up until 1989, retention enemas had been the most common technique for fecal microbiota transplant; however, alternative methods subsequently were used, including fecal infusion via nasogastric duodenal tube in 1991 32, colonoscopy in 2000 33, and self-administered enemas in 2010 34. By 2011, approximately 325 cases of fecal microbiota transplant had been reported worldwide, including approximately 75% by colonoscopy or retention enema, and 25% by nasogastric or nasoduodenal tube, or by esophagogastroduodenoscopy 35. Overall, mean cure rates to date are approximately 91% 36. In a recent series of 70 patients with recurrent Clostridium difficile infection, fecal microbiota transplant was effective even in patients with the C. difficile NAP1/BI/027 strain 37. A retrospective multicenter follow-up study of recurrent Clostridium difficile infection patients treated with fecal microbiota transplant demonstrated a 91% primary cure rate and a 98% secondary cure rate 38.
Fecal microbiota transplant appears to be safe, with no adverse effects or complications directly attributed to the procedure yet described in the existing literature 29, 39. The potential for transmission of infectious agents is a concern, however, and a recent publication outlines rigorous screening of stool donors’ blood and stool for common bacterial and viral enteropathogens 29. In one series, a standardized filtered, frozen, and then thawed preparation of stool from pre-screened universal donors showed cure rates equal to or better than those from patient-identified donors 40.
Long-term follow-up of fecal microbiota transplant is limited. In the only such follow-up study to date, 77 patients had fecal microbiota transplant and were followed for >3 months (3 months to >10 years). Of these 77 subjects, four developed an autoimmune disease (rheumatoid arthritis, Sjögren’s syndrome, idiopathic thrombocytopenic purpura, and peripheral neuropathy) at some time after the fecal microbiota transplant, although a clear relationship between the new disease and the fecal microbiota transplant was not evident 38. Randomized control trials are necessary to prove the efficacy of fecal microbiota transplant and to determine the optimal route of administration among other variables and safety in immunosuppressed patients needs to be established. An randomized control trial of donor feces administered by duodenal infusion with gut lavage showed significant efficacy compared to vancomycin or vancomycin with gut lavage without donor feces 41. The study was terminated early because it was deemed unethical to continue as the cure rate was 81% compared to 23% with vancomycin alone and 31% with vancomycin and gut lavage. An National Institute of Health funded blinded randomized control trial is underway, using fecal microbiota transplant via colonoscopy with donor or recipient stool for transplant.
Home remedies
Some research suggests that concentrated supplements of good bacteria and yeasts (probiotics) can help prevent Clostridium difficile infection, but more studies are needed for their use in treating recurrences. They are safe to use and available in capsule or liquid form without a prescription.
To cope with the diarrhea and dehydration that can occur with pseudomembranous colitis, try to:
- Drink plenty of fluids. Water is best, but fluids with added sodium and potassium (electrolytes) also may be beneficial. Avoid beverages that are high in sugar or contain alcohol or caffeine, such as coffee, tea and colas, which can aggravate your symptoms.
- Choose soft, easy-to-digest foods. These include applesauce, bananas and rice. Avoid high-fiber foods, such as beans, nuts and vegetables. If you feel your symptoms are improving, slowly add high-fiber foods back to your diet.
- Eat several small meals, rather than a few large meals. Space the smaller meals throughout the day.
- Avoid irritating foods. Stay away from spicy, fatty or fried foods, and any other foods that make your symptoms worse.
There is limited evidence for the use of adjunct probiotics to decrease recurrences in patients with recurrent Clostridium difficile infection.
A probiotic is a living organism that, when ingested, is beneficial to the host. Several probiotics have been tested in patients with recurrent Clostridium difficile infection, always as an adjunct to antibiotics. In one study, the yeast Saccharomyces boulardii resulted in fewer recurrences in a group of patients with recurrent Clostridium difficile infection (35% vs. 65%) 42; however, the study had inadequate randomization by the type of adjunct Clostridium difficile infection antibiotic. In a later study, its efficacy was limited to the subgroup of patients treated with high doses (2 gm/day) of vancomycin (17% vs. 50%) but not in those given metronidazole or lower doses of vancomycin in whom recurrence rates were 56–60% 17. A small trial of Lactobacillus plantarum 299v combined with metronidazole had recurrence rates of 35% compared with 66% in the control groups, a difference that was not statistically significant 43. Two small randomized control trials of Lactobacillus rhamnosus GG failed to show efficacy in treating recurrent Clostridium difficile infection 44. One uncontrolled study using Kefir (an over-the-counter probiotic drink) as an adjunct to antibiotics did result in decreased recurrence of C. difficile 45.
A meta-analysis of probiotics for the prevention of antibiotic-associated diarrhea and for the treatment of Clostridium difficile infection concluded that S. boulardii was only effective for C. difficile disease 46; however, a Cochrane analysis concluded that there was insufficient evidence to recommend probiotics, in general, as an adjunct to antibiotics in the treatment of C. difficile diarrhea 47. The most recent systematic review and meta-analysis of S. boulardii concluded that although there is strong evidence from numerous large randomized control trials for efficacy in prevention of antibiotic-associated diarrhea, the evidence for efficacy in the treatment of C. difficile as an adjunct to antibiotics is weak and more randomized control trials are needed 48.
Thus, there are no strong data to support the use of probiotics for recurrent Clostridium difficile infection treatment, and only weak evidence of therapeutic efficacy for S. boulardii. There is no evidence for the use of probiotics in the treatment of initial or severe disease. Moreover, these are live organisms and they should be used cautiously, if at all, in individuals with significant immune suppression because of the possible risk of bacteremia or fungemia. There are cases of S. boulardii fungemia reported in patients with central venous catheters, and thus its use in an ICU or in immunocompromised patients is not recommended 49. There are also numerous case reports of invasive lactobacillus infections in non-immunosuppressed (mostly elderly) patients 50. Finally, the use of probiotics is not regulated by the Food and Drug Administration, there is no good quality control for most probiotics, and studies have shown that some probiotics contain no live organisms, or alternatively, contain organisms not on the product label 51. In view of the lack of efficacy data, abundant data on potential harm, high costs, and lack of biological plausibility for these non-human micro-organisms to confer colonization resistance, their use cannot be recommended.
Non-toxigenic strains of C. difficile have been used to treat Clostridium difficile infection. Two patients with recurrent Clostridium difficile infection were given a non-toxigenic strain of C. difficile with resolution of symptom, but no randomized control trials have been done 52.
Surgery for complicated Clostridium difficile infection
Surgical consultation should be obtained on all patients with complicated Clostridium difficile infection. Surgical therapy should be considered in patients with any one of the following attributed to Clostridium difficile infection:
- hypotension requiring vasopressor therapy;
- clinical signs of sepsis and organ dysfunction;
- mental status changes;
- White Blood Cell count ≥ 50,000 cells/μl, lactate ≥ 5 mmol/l; or
- complicated Clostridium difficile infection with failure to improve on medical therapy after 5 days.
A major challenge in the management of severe, complicated Clostridium difficile infection is the inability to predict in which patient medical therapy will fail, and lack of consensus on the indications or timing of surgery except the very rare complication of colonic perforation. The vague term “clinical deterioration” is frequently mentioned in already critically ill patients in whom medical therapy has failed. These strategies rely on surgery as a salvage therapy, which may account for the poor outcomes associated with subtotal colectomy in complicated Clostridium difficile infection, and mortality rates that range from 35% to 80% 53, 54.
It has become evident that surgery is of benefit to patients at the advanced extreme of Clostridium difficile infection, and early surgical consultation has been associated with improved survival. Data reviewed in several series suggest that earlier colectomy (time from presentation to surgery) was associated with a significantly decreased mortality 55. In an analysis of the literature from January 1989 to May 2009, earlier diagnosis and treatment with subtotal colectomy and end-ileostomy reduced mortality associated with fulminant Clostridium difficile infection 56. One study demonstrated a trend toward decreased mortality rates in patients with fulminant disease who underwent colectomy compared with those who did not 57. These investigators further showed that admission of patients with complicated Clostridium difficile infection to a surgical service was associated with a decreased mortality and a shorter mean interval from admission to operation compared with admission to a non-surgical service.
Independent risk factors for mortality in patients who underwent colectomy that have been found consistently among multiple studies include the development of shock, as determined by the need for vasopressors, and increased lactate (≥5 mmol/l), mental status changes, end organ failure, renal failure, and the need for preoperative intubation and ventilation 56.
The above findings suggest that early operative management before the development of shock and organ failure leads to improved survival. Currently, there is no scoring system that creates a threshold for operative management. However, the more negative prognostic signs a patient has, the earlier surgical consultation and operative management should be considered.
The established operative management of severe, complicated Clostridium difficile infection has been subtotal colectomy with end-ileostomy. Survival of patients treated with segmental colectomy were worse than those treated with subtotal colectomy 58, likely because Clostridium difficile infection usually involves the entire colon. Intraoperative assessment of the extent of disease is difficult based upon the external appearance of the colon from the serosal surface. Although some series have reported perforation or infarction of the colon to be common findings at the time of surgery, colonic necrosis and perforation are not inherent to the disease process 59; they likely result from the development of shock with secondary non-occlusive ischemia and the use of vasopressors or when abdominal compartment syndrome develops and compromises colonic perfusion.
Interest has developed in early operative management other than colon resection given that the colon is most often viable at this stage without perforation 60. A recent case-controlled series demonstrated that loop ileostomy with intraoperative colon lavage with polyethylene glycol 3350/balanced electrolyte solution and post-operative antegrade colonic vancomycin flushes via the ileostomy led to colon preservation in over 90% of patients and had significantly improved survival compared with historical controls who had undergone colectomy (19% vs. 50% mortality) 60. Over 80% of cases were performed using a minimally invasive surgical approach, and a majority of patients who were followed long term had restoration of gastrointestinal continuity. Advantages of this approach are the potential willingness to utilize this treatment earlier in the course of disease based upon potential preservation of the colon and fewer long-term adverse consequences. Further validation of this approach is required.
- Farooq PD, Urrunaga NH, Tang DM, von Rosenvinge EC. Pseudomembranous Colitis. Disease-a-month : DM. 2015;61(5):181-206. doi:10.1016/j.disamonth.2015.01.006. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4402243/[↩]
- Surawicz CM, McFarland LV. Pseudomembranous Colitis: Causes and Cures. Digestion. 1999;60(2):91–100. https://www.karger.com/Article/FullText/7633[↩]
- Kawamoto S, Horton KM, Fishman EK. Pseudomembranous Colitis: Spectrum of Imaging Findings with Clinical and Pathologic Correlation. Radiographics. 1999;19(4):887–897. https://www.ncbi.nlm.nih.gov/pubmed/10464797[↩]
- Carpenter HA, Talley NJ. The Importance of Clinicopathological Correlation in the Diagnosis of Inflammatory Conditions of the Colon: Histological Patterns With Clinical Implications. Am J Gastroenterol. 2000;95(4):878–896. https://www.ncbi.nlm.nih.gov/pubmed/10763932[↩][↩]
- Cohen SH, Gerding DN, Johnson S et al. Clinical practice guidelines for Clostridium difficile infection in adults: 2010 update by the Society for Healthcare Epidemiology of America (SHEA) and the Infectious Diseases Society of America (IDSA). Infect Control and Hosp Epidemiol 2010;31:431–455.[↩][↩][↩][↩]
- Guidelines for Diagnosis, Treatment, and Prevention of Clostridium difficile Infections. Am J Gastroenterol 2013; 108:478–498; doi:10.1038/ajg.2013.4; published online 26 February 2013. https://gi.org/guideline/diagnosis-and-management-of-c-difficile-associated-diarrhea-and-colitis/[↩][↩][↩][↩][↩]
- Janarthanan S, Ditah I, Phil M et al. Clostridium difficile-associated diarrhea and proton pump inhibitor therapy: a meta-analysis. Am J Gastroentrol 2012;107:1001–1010.[↩]
- Planche T, Wilcox M. Reference assays for Clostridium difficile infection: one or two gold standards? J Clin Pathol 2011;64:1–5.[↩]
- Rea MC, O’Sullivan O, Shanahan F et al. Clostridium difficile carriage in elderly subjects and associated changes in the intestinal microbiota. J Clin Microbiol 2012;50:867–875.[↩]
- Kundrapu S, Sunkesula VCK, Jury LA et al. Utility of perirectal swab specimens for diagnosis of Clostridium difficile infection. Clin Infect Dis. 2012;55:1527–1530.[↩]
- Lyerly DM, Barroso LA, Wilkins TD. Identification of the latex test-reactive protein of Clostridium difficile as glutamate dehydrogenase. J Clin Microbiol 1991;29:2639–2642.[↩]
- Lyerly DM, Ball DW, Toth J et al. Characterization of cross-reactive proteins detected by Culturette brand rapid latex test for Clostridium difficile. J Clin Microbiol 1988;26:397–400.[↩]
- Shetty N, Wren MW, Coen PG. The role of glutamate dehydrogenase for the detection of Clostridium difficile in faecal samples: a meta-analysis. J Hosp Infect 2011;77:1–6.[↩]
- Quinn CD, Sefers SE, Babiker W et al. C. Diff Quik Chek complete enzyme immunoassay provides a reliable first-line method for detection of Clostridium difficile in stool specimens. J Clin Microbiol 2010;48:603–605.[↩]
- Cheng AC, Ferguson JK, Richards MJ et al. Australasian Society for Infectious Diseases guidelines for the diagnosis and treatment of Clostridium difficile infection. Med J Aust 2011;194:353–358.[↩]
- Luo RF, Banaei N. Is repeat PCR needed for diagnosis of Clostridium difficile infection? J Clin Microbiol 2010;48:3738–3741.[↩]
- Surawicz CM, McFarland LV, Greenberg RN et al. The search for a better treatment for recurrent Clostridium difficile disease: the use of high dose vancomycin combined with Saccharomyces boulardii. Clin Infect Dis 2000;31:1012–1017.[↩][↩]
- Apisarnthanarak A, Razavi B, Mundy LM. Adjunctive intracolonic vancomycin for severe Clostridium difficile colitis: case series and review of the literature. Clin Infect Dis 2002;35:690.[↩]
- Wenisch C, Parschalk B, Hasenhundl M et al. Comparison of vancomycin, teicoplanin, metronidazole, and fusidic acid for the treatment of Clostridium difficile-associated diarrhea. Clin Infect Dis 1996;22:813–818.[↩]
- Zar FA, Bakkanagari SR, Moorthi KM et al. A comparison of vancomycin and metronidazole for the treatment of Clostridium difficile-associated diarrhea, stratified by disease severity. Clin Infect Dis 2007;45:302–307.[↩][↩]
- Al-Nassir WN, Sethi AK, Li Y et al. Both oral metronidazole and oral vancomycin promote persistent overgrowth of vancomycin-resistant enterococci during treatment of Clostridium difficile-associated disease. Antimicrob Agents Chemother 2008;52:2403–2406.[↩][↩]
- Cornely OA, Crook DW, Esposito R et al. Fidaxomicin versus vancomycin for infection with Clostridium difficile in Europe, Canada, and the USA: a double-blind, non-inferiority, randomised controlled trial. Lancet Infect Dis 2012;12:281–289.[↩]
- McFarland LV, Elmer GW, Surawicz CM. Breaking the cycle: treatment strategies for 163 cases of recurrent Clostridium difficile disease. Am J Gastroenterol 2002;97:1769–1775.[↩]
- Tedesco FJ, Gordon D, Fortson WC. Approach to patients with multiple relapses of antibiotic-associated pseudomembranous colitis. Am J Gastroenterology 1985;80:867–868.[↩]
- Buggy BP, Fekety R, Silva J Jr. Therapy of relapsing Clostridium difficile-associated diarrhea and colitis with the combination of vancomycin and rifampin. J Clin Gastroenterol 1987;9:155–159.[↩]
- Johnson S, Schriever C, Galang M et al. Interruption of recurrent Clostridium difficile-associated diarrhea episodes by serial therapy with vancomycin and rifaximin. Clin Infect Dis 2007;44:846–848.[↩]
- Garey KW, Ghantoji SS, Shah DN et al. A randomized, double-blind, placebo-controlled pilot study to assess the ability of rifaximin to prevent recurrent diarrhea in patients with Clostridium difficile infection. J Antimicrob Chemother 2011;66:2850–2855.[↩]
- Curry SR, Marsh JW, Shutt KA et al. High frequency of rifampin resistance identified in an epidemic Clostridium difficile clone from a large teaching hospital. CID 2009;43:91–93.[↩]
- Bakken JS, Borody T, Brandt LJ et al. Fecal Microbiota Transplantation (FMT) Workgroup. Treating Clostridium difficile infection with fecal microbiota transplantation. Clin Gastroenterol Hepatol 2011;9:1044–1049.[↩][↩][↩]
- Eiseman B, Silen W, Bascom GS et al. Fecal enema as an adjunct in the treatment of pseudomembranous enterocolitis. Surgery 1958;44:854–859.[↩]
- Schwan A, Sjolin S, Trottestam U et al. Relapsing Clostridium difficile enterocolitis cured by rectal infusion of homologous faeces. Lancet 1983;2:845.[↩]
- Aas J, Gessert CE, Bakken JS. Recurrent Clostridium difficile colitis: case series involving 18 patients treated with donor stool administered via a nasogastric tube. Clin Infect Dis 2003;36:580–585.[↩]
- Lund-Tønnesen S, Berstad A, Schreiner A et al. Clostridium difficile-assosiert diare behandlet med homolog feces. Tidsskr Nor Laegeforen 1998;118:1027–1030.[↩]
- Silverman MS, Davis I, Pillai DR. Success of self-administered home fecal transplantation for chronic Clostridium difficile infection. Clin Gastroenterol Hepatol 2010;8:471–473.[↩]
- Brandt LJ, Reddy S. Fecal microbiota transplantation for recurrent Clostridium difficile infection. J Clin Gastroenterol 2011;45:S159–S167.[↩]
- Gough E, Shaikh H, Manges AR. Systematic review of intestinal microbiota transplantation (fecal bacteriotherapy) for recurrent Clostridium difficile infection. Clin Infect Dis 2011;53:994–1002.[↩]
- Mattila E, Uusitalo-Seppälä R, Wuorela M et al. Fecal transplantation, through colonoscopy, is effective therapy for recurrent Clostridium difficile infection. Gastroenterology 2010;142:490–496.[↩]
- Brandt LJ, Aroniadis OC, Mellow M et al. Long-term follow-up of colonoscopic fecal microbiota transplant for recurrent Clostridium difficile infection. Am J Gastroenterol 2012;107:1079–1087.[↩][↩]
- Borody TJ, Warren EF, Leis SM et al. Bacteriotherapy using fecal flora: toying with human motions. J Clin Gastroenterol 2004;38:475–483.[↩]
- Hamilton MJ, Weingarden AR, Sadowsky MJ et al. Standardized frozen preparation for transplantation of fecal microbiota for recurrent Clostridium difficile infection. Am J Gastroenterol 2012;107:761–767.[↩]
- van Nood E, Vrieze A, Nieuwdorp M et al. Duodenal infusion of donor feces for recurrent Clostridium difficile. N Engl J Med 2013;368:407–415.[↩]
- McFarland LV, Surawicz CM, Greenberg RN et al. A randomized placebo-controlled trial of Saccharomyces boulardii in combination with standard antibiotics for Clostridium difficile disease. JAMA 1994;271:1913–1918.[↩]
- Wullt M, Hagslatt M-L J, Odenholt I. Lactobacillus plantarum 299v for the treatment of recurrent Clostridium difficile-associated diarrhea: a double-blind, placebo-controlled trial. Scan J Infect Dis 2003;35:365–367.[↩]
- Lawrence SJ, Korzenik JR, Mundy LM. Probiotics for recurrent Clostridium difficile disease. J Med Microbiol 2005;54:905–906.[↩]
- Bakken JS. Resolution of recurrent Clostridium difficile-associated diarrhea using staggered antibiotic withdrawal and kefir. Minn Med 2009;92:38–40.[↩]
- McFarland LV. Meta-analysis of probiotics for prevention of antibiotic associated diarrhea and treatment of Clostridium difficile disease. Am J Gastroenterol 2006;1010:812–822.[↩]
- Pillai A, Nelson RL. Probiotics for treatment of Clostridium difficile-associated colitis in adults. Cochrane Database Syst Rev 2008;1:CD004611.[↩]
- McFarland LV. Systematic review and meta-analysis of Saccharomyces boulardii in adult patients. World J Gastroenterol 2010;16:2202–2222.[↩]
- Munoz P, Bouza E, Cuenca-Estrella M et al. Saccharomyces cerevisiaefungemia: an emerging infectious disease. Clin Infect Dis 2005;40:1625–1634.[↩]
- Segarra-Newnham M. Probiotics for Clostridium difficile-associated diarrhea: focus on Lactobacillus rhamnosus GG and Saccharomyces boulardii. Ann Pharmacother 2007;41:1212–1221.[↩]
- Drago L, Rodighiero V, Celeste T et al. Microbiological evaluation of commercial probiotic products available in the USA in 2009. J Chemother 2010;22:373–377.[↩]
- Seal D, Borriello SP, Barclay F et al. Treatment of relapsing Clostridium difficile diarrhoea by administration of a non-toxigenic strain. Eur J Clin Microbiol 1987;6:51–53.[↩]
- Lamontagne F, Labbe AC, Haeck O et al. Impact of emergency colectomy on survival of patients with fulminant Clostridium difficile colitis during an epidemic caused by a hypervirulent strain. Ann Surg 2007;245:267–272.[↩]
- Longo WE, Mazuski JE, Virgo KS et al. Outcome after colectomy for Clostridium difficile colitis. Dis Colon Rectum 2004;47:1620–1626.[↩]
- Arkelov A, Livert D, Kohli H. Predictors of fatal outcome after colectomy for fulminant Clostridium difficile colitis: a 10-year experience. Am Surg2011;77:977–980.[↩]
- Ali SO, Welch JP, Dring RJ. Early surgical intervention for fulminant pseudomembranous colitis. Am Surg 2008;74:20–26.[↩][↩]
- Sailhamer EA, Carson K, Chang Y et al. Fulminant Clostridium difficile colitis: patterns of care and predictors of mortality. Arch Surg 2009;144:433–439; discussion 439–40.[↩]
- Koss K, Clark MA, Sanders DS et al. The outcome of surgery in fulminant Clostridium difficile colitis. Colorectal Dis 2006;8:149–154.[↩]
- Bolton RP, Culshaw MA. Faecal metronidazole concentrations during oral and intravenous therapy for antibiotic associated colitis due to Clostridium difficile. Gut 1986;27:1169–1172.[↩]
- Neal MD, Alverdy JC, Hall DE et al. Diverting loop ileostomy and colonic lavage: an alternative to total abdominal colectomy for the treatment of severe, complicated Clostridium difficile associated disease. Ann Surg2011;254:423–427;discussion 427–9.[↩][↩]





{kind=link}