
Contents
Radial artery
The radial artery originates from the brachial artery at approximately the neck of the radius and passes along the lateral aspect of the forearm (Figure 1 and 2).
The radial artery is just deep to the brachioradialis muscle in the proximal half of the forearm, related on its lateral side to the superficial branch of the radial nerve in the middle third of the forearm, and medial to the tendon of the brachioradialis muscle and covered only by deep fascia, superficial fascia, and skin in the distal forearm.
Branches of the radial artery originating in the forearm include a radial recurrent artery, which contributes to an anastomotic network around the elbow joint and to numerous vessels that supply muscles on the lateral side of the forearm; a small palmar carpal branch, which contributes to an anastomotic network of vessels that supply the carpal bones and joints. A somewhat larger branch, the superficial palmar branch, which enters the hand by passing through, or superficial to, the thenar muscles at the base of the thumb and anastomoses with the superficial palmar arch formed by the ulnar artery.
In the distal forearm, the radial artery lies immediately lateral to the large tendon of the flexor carpi radialis muscle and directly anterior to the pronator quadratus muscle and the distal end of the radius (Figure 1). In the distal forearm, the radial artery can be located using the flexor carpi radialis muscle as a landmark. The radial pulse can be felt by gently palpating the radial artery against the underlying muscle and bone.
The radial artery leaves the forearm, passes around the lateral side of the wrist, and penetrates the posterolateral aspect of the hand between the bases of metacarpals I and II (Figure 2). Branches of the radial artery in the hand often provide the major blood supply to the thumb and lateral side of the index finger.
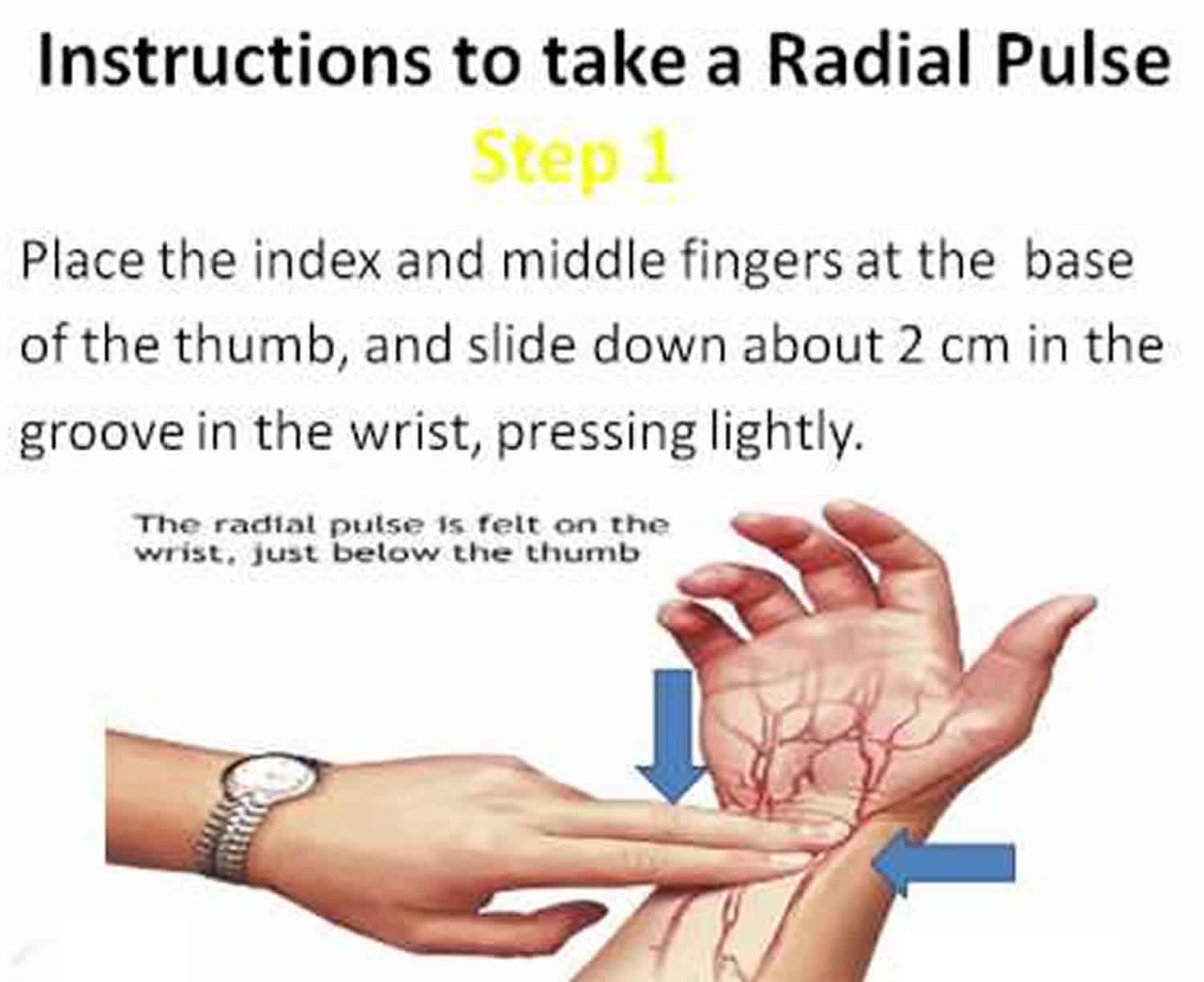
Radial pulse in the distal end of radius at the wrist, where the radial artery is covered only by fascia and skin, this is the most common site for taking a radial pulse (Figure 3 and 4).
Figure 1. Radial artery
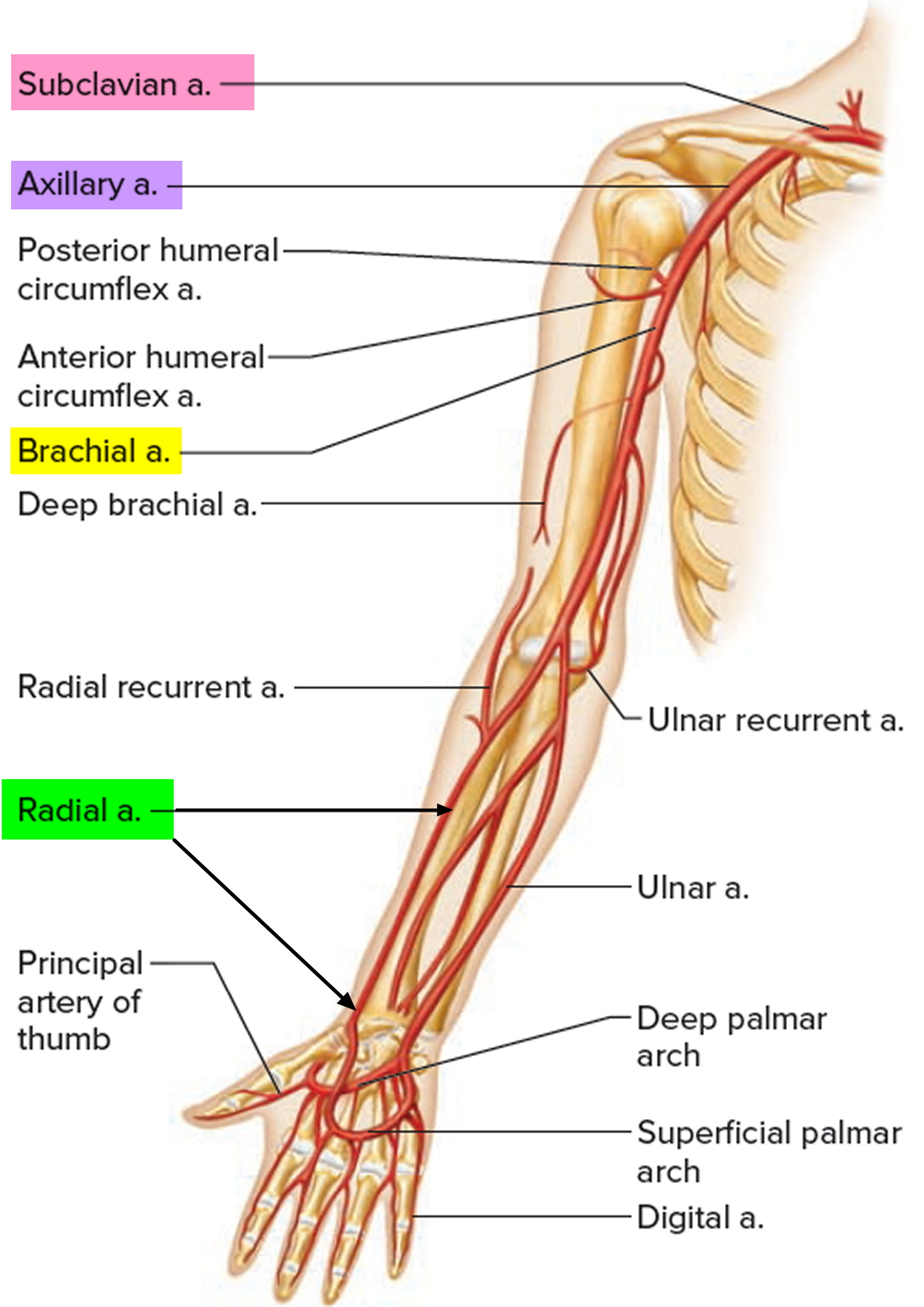
Figure 2. Radial artery at the elbow

Figure 3. Radial artery at the wrist
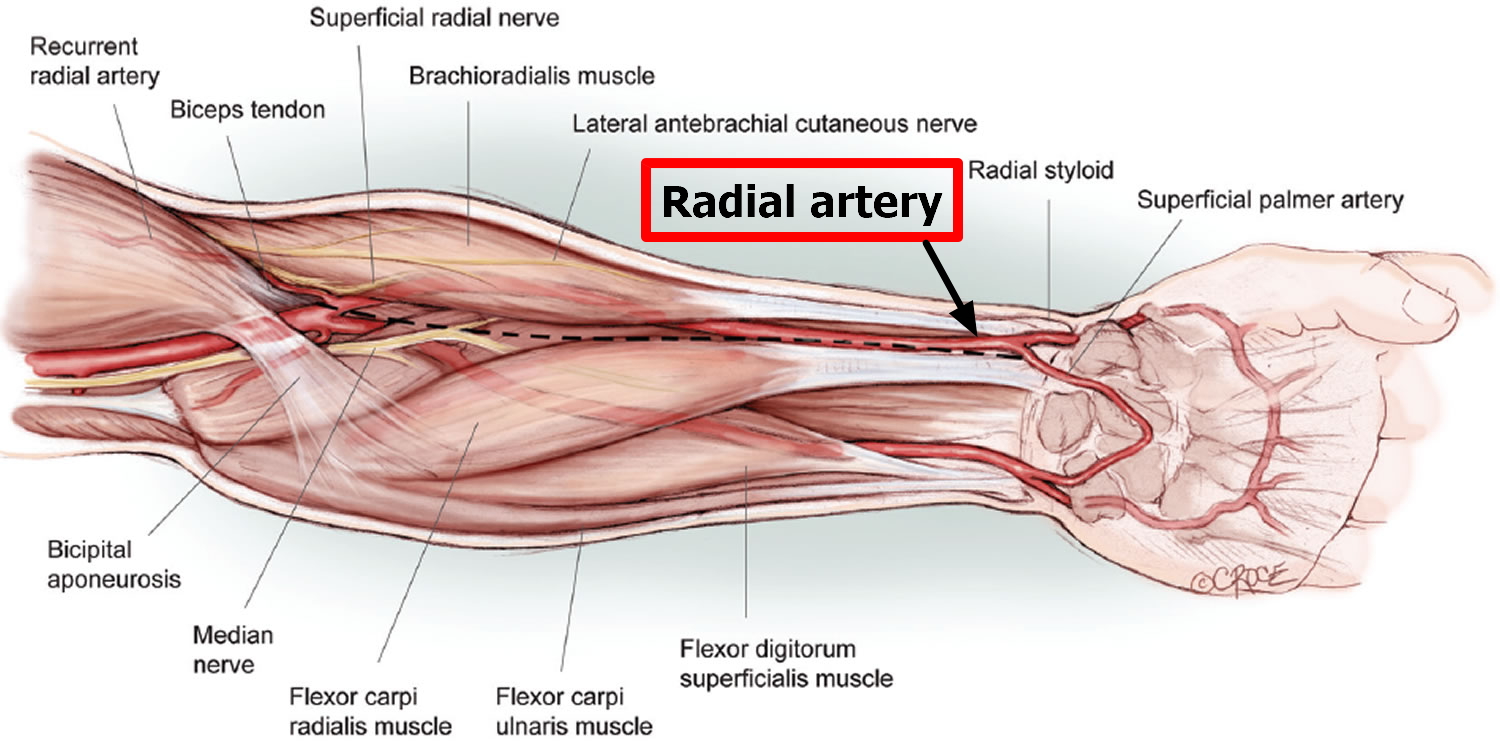
Figure 4. How to take a radial pulse
Finding your pulse
The easiest places to find your pulse are:
Your wrist
- Put one of your hands out so you’re looking at your palm.
- Use the first finger (your index finger) and middle finger of your other hand and place the pads of these fingers on the inside of your wrist, at the base of your thumb.
- Press lightly and feel the pulse. If you can’t feel anything press slightly harder or move your fingers around until you feel your pulse.
How to check your pulse
Once you’ve found your pulse, continue to feel it for about 20-30 seconds. Feel your pulse and check if it’s regular or irregular. You can work out your heart rate in beats per minute (bpm) by:
- counting the number of beats in your pulse after 60 seconds, or
- counting the beats for 30 seconds and multiplying by two.
If your pulse feels irregular, you should check for a full 60 seconds.
What should you check?
Your heart rate:
- Most adults have a resting heart rate between 60 and 100 bpm
- Your heart rate may be lower if you do lots of exercise and are very fit. Some athletes have heart rates ranging from 40 to 60 bpm.
Your heart rhythm:
- Occasional irregularities such as missed beats are very common and usually nothing to worry about, but it is still best to check this with your doctor.
- An irregular pulse could also be a sign of an arrhythmia (an abnormal heart rhythm), such as Atrial Fibrillation (AF). This is more likely if you are 65 or older.
Listen to the example heart rhythms below to help you spot an irregular heart beat:
Regular pulse
Irregular pulse
Radial artery catheterization
Cardiac catheterization is a minimally invasive procedure commonly used to diagnose and treat heart conditions. During catheterization, small tubes (catheters) are inserted into the circulatory system under x-ray guidance in order to obtain information about blood flow and pressures within the heart and to determine if there are obstructions within the blood vessels feeding the heart muscle (coronary arteries).
The catheters necessary for cardiac catheterization can be inserted either into the femoral artery (in the groin), or into the radial artery (in the wrist). The femoral artery is a larger vessel and provides a more direct route to the heart. Because of these advantages, the femoral artery has become the standard entry site for catheterization procedures. However, there has been a recent increase in the use of the radial artery for cardiac catheterization procedures.
Deciding Between the Radial and Femoral Approach
The biggest factor driving the decision to use the radial artery is the physician performing the procedure. The procedure can be more challenging technically, and the physician must have enough experience to feel comfortable with radial procedures. Many physicians are more comfortable with the femoral approach, and will therefore recommend it alone. There are a growing number of physicians in the United States, however, who prefer to use the radial artery as their default approach.
There are also many physicians who use the radial approach in selective situations where the femoral approach may be more complicated, such as in obese patients or patients with obstructions in the blood vessels supplying the lower extremity. The femoral approach may be selected for patients in whom preservation of the radial artery is essential, such as patients requiring dialysis fistulas or patients who require the radial artery to be used for bypass surgery.
The Radial Artery Catheterization Procedure
Before beginning the procedure, the physician performing the procedure may test the blood supply to the hand. There are 2 arteries that supply blood to the hand (the radial artery and ulnar artery), and if both are working it is safe to proceed. The procedure can be performed from either wrist, and the physician may have specific reasons to use one side over the other. Both the groin (femoral) and the wrist (radial) may be prepped for the procedure in the rare event that the arteries in the arm do not allow catheters to get to the heart easily and the femoral artery needs to be used. A nurse administers medication through a vein for sedation. The cardiologist then delivers a local anesthetic to the wrist and inserts a short tube (sheath or introducer) into the radial artery. Medications are given through the sheath to relax the radial artery, which may cause a temporary burning sensation in the hand and arm. A blood thinner is also given to help prevent clots from forming in the artery.
Catheters are then advanced through the sheath and guided to the heart, and the coronary angiogram (and stent placement if necessary) is performed. Once the procedure is complete, the catheters and sheath are removed from the radial artery, and a compression device is placed on the wrist (Figure 4), which is typically worn for 2 hours. The patient is allowed to sit up and eat after the procedure. It is recommended that no undue stress be put on the radial artery as it heals.
Patients are asked to avoid lifting anything heavy (like suitcases or grocery bags) with that hand, but should otherwise be able to use the hand for activities such as eating and writing. By the third day after the procedure, normal activity with the hand can be resumed.
Figure 4. Radial artery catheterization

Note: Left wrist post radial artery catheterization with placement of a compression band, which is typically worn for 2 hours.
Advantages of Radial Artery Catheterization
Any catheter placement into a blood vessel is associated with a risk of bleeding. After removal of the catheter from the femoral artery, the patient will need to lie flat without bending the leg for 2 to 6 hours to allow the artery to heal. In some cases, even with prolonged immobility, internal bleeding can occur and can be severe enough to require blood transfusions or surgery to repair the femoral artery. These complications are rare, but they may be less common if the catheter is inserted in the wrist 1. Because the radial artery is much smaller and located closer to the skin surface, internal bleeding is eliminated and any external bleeding can be easily compressed.
After the catheter is removed from the radial artery, a compression device is placed around the wrist to apply pressure on the artery, and there is no requirement for the patient to remain immobile. In general, patients find radial catheterization more comfortable than femoral catheterization because they are able to sit up, walk, and eat immediately. This is a particular advantage for patients with back problems because there is no need for heavy pressure on the leg and prolonged immobility.
Risks of Radial Artery Catheterization
Any invasive procedure carries some risk of significant bleeding. Using the radial artery rather than the femoral artery may reduce the risk of bleeding from the puncture site, particularly in patients who are obese or require blood thinning agents to treat their heart condition. There are, however, risks unique to radial artery catheterization. Though rare, spasm of the muscles lining the wall of the radial artery may be experienced by some patients. This can make it difficult for the cardiologist to maneuver the catheters and may cause the patient discomfort. This is temporary, and can be prevented and treated with medications in the majority of cases. Occasionally, it can be severe enough to necessitate switching to the femoral artery. Another potential risk is that the radial artery may close after the procedure. This may result because of a blood clot forming in the artery. Blood thinners given during the procedure help to prevent this, and with modern techniques it has become very rare, occurring in less than 2% of cases. When radial artery occlusion does occur, it generally causes no issue for the hand because there are redundant blood supplies to the hand.
- Radial Artery Catheterization. Circulation. 2011;124:e407-e408. https://doi.org/10.1161/CIRCULATIONAHA.111.019802[↩]
{kind=link}