
Contents
What is ear pain ?
Ear pain or otalgia in or about the external ear and temporal bone may occur from multiple causes, many of which are remote from the ear itself 1. When the cause arises from the ear (primary otalgia), the ear examination is usually abnormal and the diagnosis is typically apparent 2. In secondary or referred otalgia, the ear examination is usually normal, and the pain may be referred from a variety of sites 2. To ascertain the etiology of otalgia accurately, a detailed history relating to ear, dental, sinus, jaw, neck, tongue, mouth, and neurologic disorders in the head and neck region must be taken. Symptoms referable to one of these sites will usually point to the most likely cause.
Acute, chronic, or recurrent pain may be present. The sensation may vary from a deep aching to a sharp, quick lancing discomfort. Only a vague fullness may be present, or there may be a blocked feeling to the ear. Acute, sudden pain may be accompanied by fever, nasal congestion, nasal or ear drainage, or headache. Chronic pain usually exists by itself, and fewer associated complaints are noted. Tinnitus, dizziness, or hearing impairment are commonly seen with recurrent ear pain. The pain may seem deep and penetrating within the canal, or it may be more diffuse and extend either anterior or posterior to the pinna. The patient may volunteer that neck motion, chewing, swallowing, coughing, nose blowing, Valsalva maneuver, or flying aggravate or precipitate the discomfort.
Ear pain without obvious physical findings must be followed at periodic intervals until the source is located. Since 50% of patients have pain from dental sources, dental referral is often needed. Insidious dental infection or decay may be very difficult to identify, and this, as well as more remote causes, must often be pursued on more than one visit.
The Ear
The ear, has outer, middle, and inner parts. The ear also functions in the sense of equilibrium.
Outer (External) Ear
The outer ear consists of three parts. The first is an outer, funnel-like structure called the auricle or pinna. The second is an S-shaped tube called the external acoustic meatus or external auditory canal, that leads inward through the temporal bone for about 2.5 centimeters (Figure 1). The meatus terminates with the third part, the eardrum or tympanic membrane.
The transmission of vibrations through matter produces sound. These vibrations travel in waves, much like ripples on the surface of a pond. The higher the wave, the louder the sound. The more waves per second, the higher the frequency, or pitch, of the sound. Vibrating strings on a guitar or reeds on an oboe produce the sounds of these musical instruments, and vibrating vocal folds (vocal cords) in the larynx produce the voice. The auricle of the ear helps collect sound waves traveling through the air and directs them into the external acoustic meatus. At the end of the meatus, the sound waves reach the eardrum.
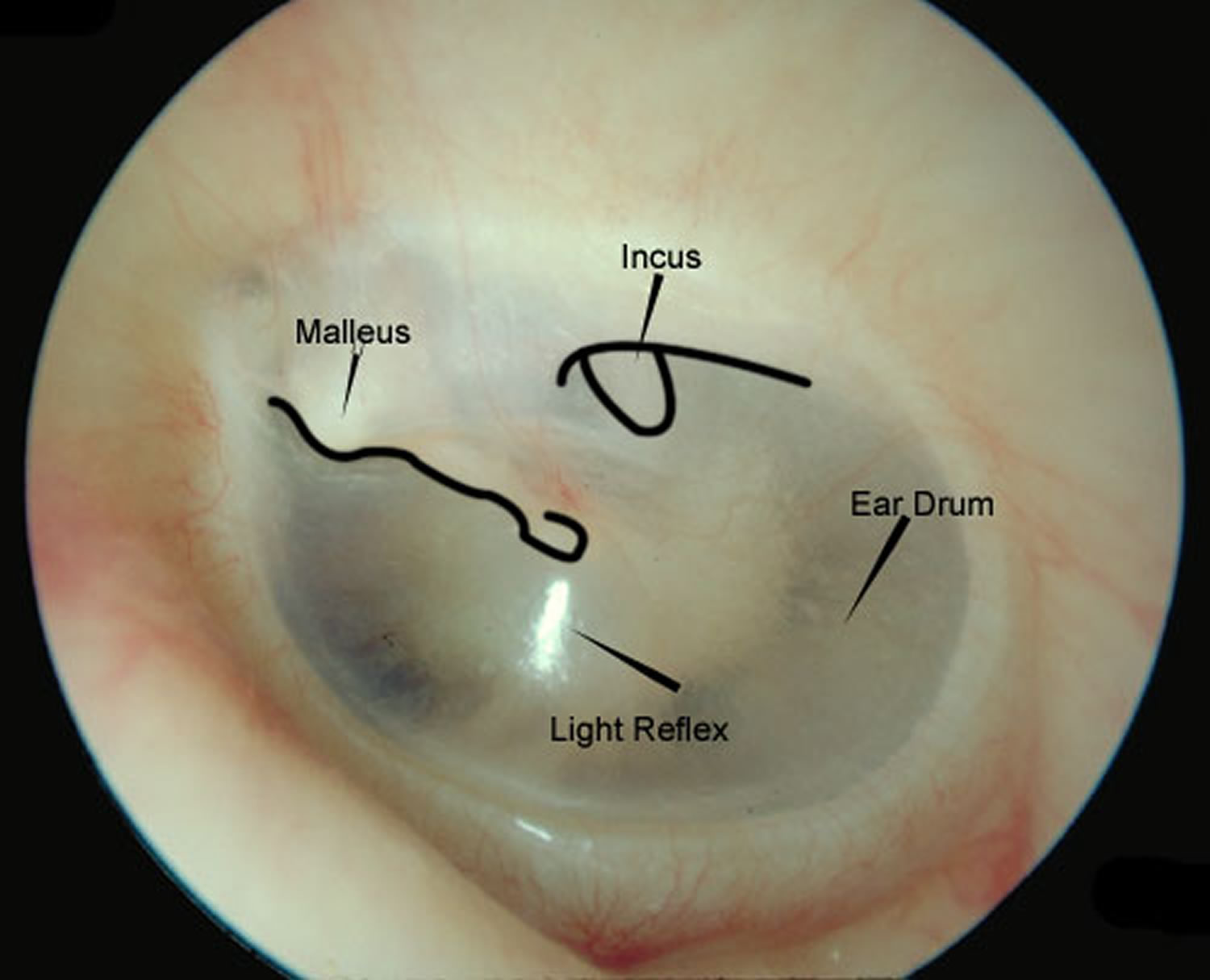
The eardrum is a semitransparent membrane covered by a thin layer of skin on its outer surface and by mucous membrane on the inside. It has an oval margin and is coneshaped, with the apex of the cone directed inward. The attachment of one of the auditory ossicles (the malleus) maintains the eardrum’s cone shape. Sound waves that enter the external acoustic meatus change the pressure on the eardrum, which vibrates back and forth in response and thus reproduces the vibrations of the sound-wave source.
Middle Ear
The middle ear, or tympanic cavity, is an air-filled space in the temporal bone. It contains three small bones called auditory ossicles: the malleus, the incus, and the stapes (Figure 1). Tiny ligaments attach them to the wall of the tympanic cavity, and they are covered by mucous membrane. These bones bridge the eardrum and the inner ear, transferring vibrations between these parts. Specifically, the malleus attaches to the eardrum, and when the eardrum vibrates, the malleus vibrates in unison. The malleus causes the incus to vibrate, and the incus passes the movement on to the stapes. An oval ligament holds the stapes to an opening in the wall of the tympanic cavity called the oval window, which leads into the inner ear. Vibration of the stapes at the oval window moves a fluid in the inner ear, which stimulates the hearing receptors.
The auditory ossicles help increase (amplify) the force of vibrations as they pass from the eardrum to the oval window, in addition to transferring vibrations. The vibrational force concentrates as it moves from the outer to the inner ear because the ossicles transmit vibrations from the relatively large surface of the eardrum to a much smaller area at the oval window. As a result, the pressure (per square millimeter) that the stapes applies on the oval window is many times greater than the pressure that sound waves exert on the eardrum.
Auditory Tube
An auditory tube or eustachian tube, connects each middle ear to the back of the nasal cavity (nasopharynx). This tube conducts air between the tympanic cavity and the outside of the body by way of the nose and mouth. The auditory tube helps maintain equal air pressure on both sides of the eardrum, which is necessary for normal hearing.
The function of the auditory tube is noticeable during rapid changes in altitude. As a person moves from a higher altitude to a lower one, air pressure on the outside of the eardrum increases. This may push the eardrum inward, impairing hearing. When the air pressure difference is great enough, air movement through the auditory tube equalizes the pressure on both sides of the eardrum, and the membrane moves back into its regular position. This restores normal hearing and is associated with a popping sound.
Inner (Internal) Ear
Next to the middle ear in the bone of the skull is a small compartment which contains the hearing and balance apparatus known as the inner ear. The inner ear is a complex system of communicating chambers and tubes called a labyrinth. Each ear has two parts to the labyrinth—the bony (osseus) labyrinth and the membranous labyrinth. The bony labyrinth is a cavity within the temporal bone. The membranous labyrinth is a tube of similar shape that lies within the bony labyrinth. Between the bony and membranous labyrinths is a fluid called perilymph, which is secreted by cells in the wall of the bony labyrinth. The membranous labyrinth contains another fluid, called endolymph.
The parts of the labyrinths include three membranous semicircular ducts within three bony semicircular canals, and a cochlea. The semicircular canals and associated structures provide a sense of equilibrium or balance. The cochlea functions in hearing.
The cochlea is shaped like a snail and is divided into two chambers by a membrane. The chambers are full of fluid which vibrates when sound comes in and causes the small hairs which line the membrane to vibrate and send electrical impulses to the brain.
The semi-circular canals are also known as the labyrinthine. These little canals are lined up at right angles (90°) to each other. This allows the brain to know in which direction the head is moving. These semi-circular canals are filled with fluid and have some small calcium crystals embedded in the lining.
Coming from the inner ear and running to the brain is the eighth cranial nerve, the auditory nerve. This nerve carries both balance and hearing information to the brain. Along with the eighth cranial nerve runs the seventh cranial nerve. The seventh cranial nerve is also known as the facial nerve because it supplies nerve impulses to the muscles of the face.
How does the hearing system work ?
The outer ear captures sound waves. The sound travels down the ear canal and hits the ear drum. The ear drum vibrates which causes the ossicles (middle ear bones) to vibrate. A piston action of the ossicles creates a wave in the fluid in the inner ear. The fluid wave stimulates the hair cells in the cochlea and an electrical impulse is sent through the eighth cranial nerve to the brain.
The balance system works by sending continuous electrical impulses to the brain. Moving the head causes the fluid in the semi-circular canals to shift. This in turn changes the electrical impulses to the brain. The brain uses this information to make any adjustments the body needs for balance.
Figure 1. The Ear showing outer (auricle), middle and inner parts
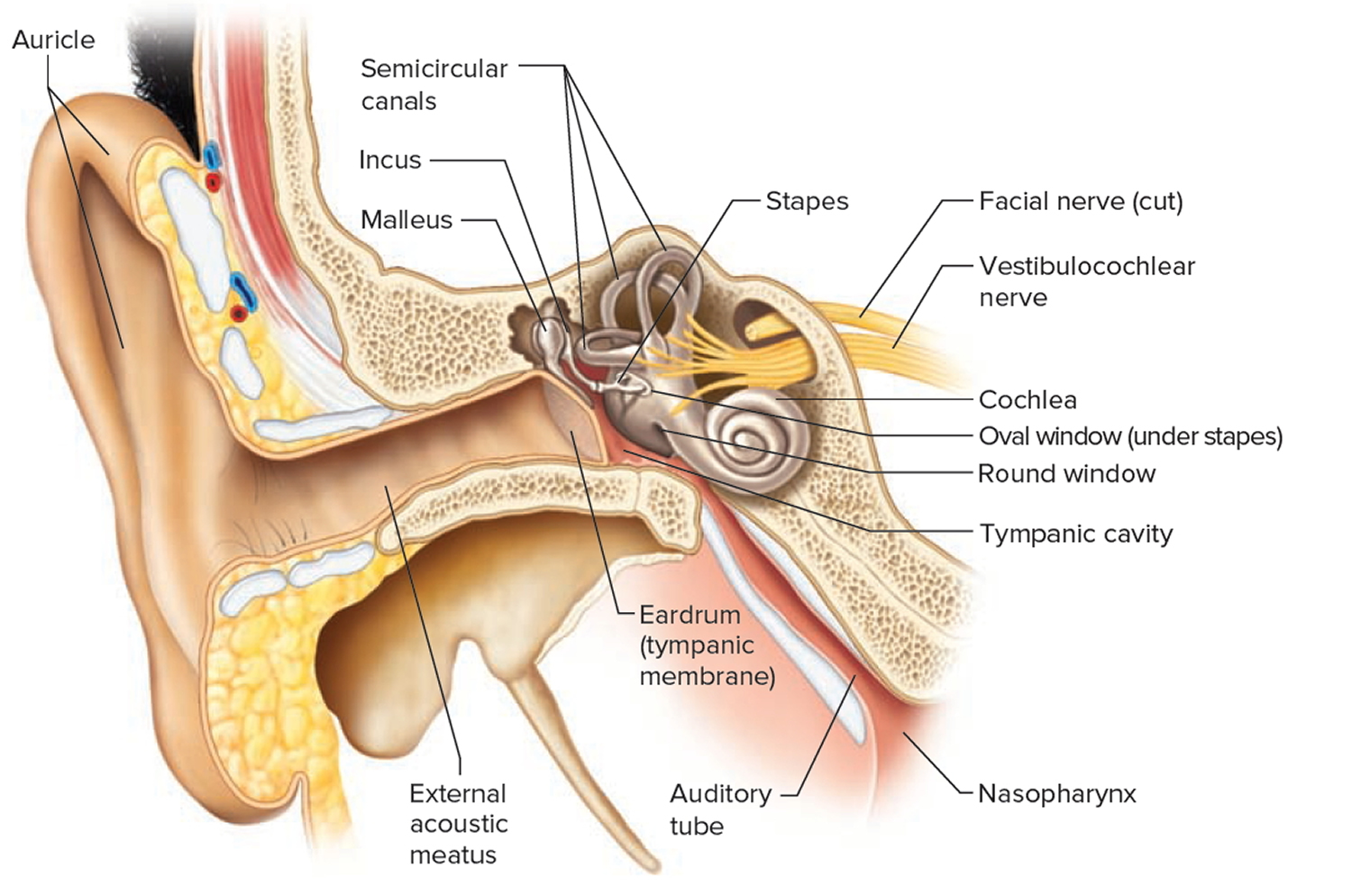
Figure 2. Normal ear drum (tympanic membrane)
Referred ear pain
The nerve fibers supplying to the external auditory canal and the middle ear comes from cranial nerves V (trigeminal), VII (facial), IX (glossopharyngeal), and X (vagus), and from the cervical plexus via the lesser occipital nerve (C2) and the great auricular nerve (C2–3) 3. A small portion of the auricle, the superior and anterior walls of the external canal, and the anterior part of the tympanic membrane are supplied by the third branch of the auriculotemporal branch of the third division of the trigeminal nerve. Practically the whole surface of the auricle receives its sensory innervations from the great auricular and lesser occipital nerves. The inferior and posterior walls of the external canal and the posterior portion of the tympanic membrane are supplied with sensory fibers from the auricular branch of the vagus nerve. It is generally correct to state that the ganglionic representation of the sensation of the auricle and external canal can be divided into the gasserian ganglion in front, the second and third cervical ganglia behind, and jugular ganglion in between. When pain is referred to the ear from a painful lesion elsewhere, it is likely that both the ear and the area containing the lesion receive sensory innervations from the same cranial nerve and that spread occurs by way of central connections within the gray matter of the brainstem.
These nerves have long courses in the head, neck, and chest, which is why so many diseases can cause ear pain. The structures of the inner ear (i.e., cochlea and semicircular canals) are innervated by cranial nerve VIII (vestibulo-cochlear), which has no pain fibers. Therefore, most pathologic processes of the inner ear do not produce pain 4. However, inner ear diseases such as Meniere’s disease can produce other sensations, such as pressure or fullness (see Table 2) 4.
Referred pain is an incompletely understood phenomenon wherein nerve impulses emanating from a distant or deeper structure are localized to a more superficial structure of the body. In each situation, the pain spreads from one area to another through nerve branches that have a common central origin within the same segments of the gray matter of the spinal cord. Under experimental conditions, it can be shown that a projection of pain is learned and that pain impulses conducted in overlapping pathways are simply given the previously learned reference for impulses in that path. Neither habit reference nor any other theory of referred pain can fully explain the phenomena that occur.
The tympanic plexus that lies on the promontory is formed mainly by nerves derived from the tympanic branch of the glossopharyngeal nerve but also receives branches from the geniculate ganglion of the facial nerve. Sympathetic branches from the carotid plexus join the tympanic plexus, although sensory function is doubtful. The skin overlying the mastoid is innervated by the mastoid branches of the great auricular and lesser occipital nerves, while cells in the mastoid receive their sensory supply through a mastoid branch of the tympanic plexus. Sensory branches from the trigeminal to structures within the middle ear are very questionable.
Referred pain pathways responsible for most cases of otalgia involve the same three cranial nerves that innervate the external auditory canal and middle ear. Painful impulses originating in the region of a diseased lower molar tooth or temporomandibular joint would be traced by way of the gasserian ganglion to the spinal nucleus of the trigeminal (fifth cranial) nerve in the brainstem. This nucleus also connects with ear structures by way of other sensory branches of the third division that innervate the wall of the external canal and tympanum.
Irritative impulses from the tongue or tonsil travel through the glossopharyngeal (ninth cranial) nerve and its ganglia to enter the somatic sensory nucleus of that nerve within the medulla. This nucleus also receives the sensory branches of the ninth cranial nerve from the middle ear and adjacent structures. It is clear again, as in referred pain by the fifth nerve, that the pathway must pass through the sensory nucleus in the medulla.
Lesions of the anterior two-thirds of the tongue and inflammatory conditions of the parotid gland refer pain along the auricular branch of the auriculotemporal nerve. Referred pain from the submaxillary and lingual salivary glands via the lingual nerve may cause pain in front of the ear. An inflammation on the anterior one-third of the tongue may cause pain in front of the ear, whereas an ulceration of the posterior one-third of the tongue, such as a beginning carcinoma, may cause pain within the ear itself. This is explained by referral through two different nerve sources.
Patients with acute and chronic infections of the tonsils frequently complain of otalgia. Lesions of the palate, pharynx, or nasopharynx, especially in the region of the eustachian tube, often produce pain deep in the ear, and occasionally growths of the tonsil give rise to earache as the first and only symptom. Otalgia is often the earliest sign of a beginning malignancy in the nasopharynx. The ninth cranial nerve is involved in this referred pain pattern.
Ulcerative lesions of the entrance of the larynx such as tuberculosis or malignancy may cause reflex otalgia, secondary to irritation of the superior laryngeal branch of the vagus nerve.
In the same manner, the somatic afferent pathways of the vagus (tenth cranial) nerve from the larynx ascend through the peripheral ganglia to the spinal nucleus in the medulla and here connect with afferents from the concha and deeper structures of the ear.
The fifth, ninth, and tenth cranial nerves are closely related in their central connection in the brainstem; however, there must be a fair degree of separation within each of the three nerve systems centrally. Otherwise, the localized reference of pain observed clinically would not occur. Beyond a certain level of sensory irritation, there seems to be an overflow into the adjacent centers with more diffuse and poorly localized pain.
The onset, intensity, and duration of ear pain depend on the particular etiology. The cause of all persistent pain must he pursued intensely.
Causes of ear pain
Pain in the ear may be divided into intrinsic (primary otalgia) and extrinsic (secondary otalgia) causes denoting the site of origin. When the ear is the source of the pain (primary otalgia), the ear examination is usually abnormal. When the ear is not the source of the pain (secondary otalgia), the ear examination is typically normal. The cause of primary otalgia (intrinsic causes) is usually apparent on examination; the most common causes are otitis media and otitis externa (see Table 1). The cause of secondary otalgia (extrinsic causes) is often difficult to determine because the innervation of the ear is complex and there are many potential sources of referred pain 2. Extrinsic causes produce pain in the ear reflex by lesions remote from the ear itself. This is often referred to as reflex or referred otalgia. In order to interpret the significance of referred pain in the ear, it is necessary to know the nerve supply of the ear and to know to what other organs the same or related nerves are distributed (see Referred Ear Pain). Lesions in the ear rarely produce pain in more distant areas, but many remote areas refer pain to the ear. When the patient complains of earache though having a normal external canal and drum, a number of sources of pain should come to mind. In about one-half of cases the cause will be of dental origin either occurring from the teeth themselves or from the temporomandibular joint. The temporomandibular joint is the most common site of pain, followed by the lower molar teeth, dental disease, pharyngitis and cervical spine arthritis.
It is often stated that 50 percent of pain in the ear is secondary otalgia (referred ear pain) 4 and that 50 percent of secondary otalgia results from dental causes 5; however, these estimates are not based on published data. In a study of 500 patients visiting an ear, nose, and throat clinic, 58 presented with primary otalgia and 28 with secondary otalgia 6. In another study involving 615 patients, the most common causes of secondary otalgia were dental (38 percent), temporomandibular joint (TMJ) disorders (35 percent), cervical spine disorders (8 percent), and neuralgias (5 percent) 7. The causes of otalgia in children are similar to those in adults, although middle ear disease (especially acute otitis media) is more common in children 8.
To ascertain the cause of otalgia accurately, a detailed history relating to ear, dental, sinus, jaw, neck, tongue, mouth, and neurologic disorders in the head and neck region must be taken. Symptoms referable to one of these sites will usually point to the most likely etiology as listed in Table 1.
If no cause for pain can be found in that area, then the examiner should think of the nerve supply of the ear and the mechanisms of referred pain. Think and check the letter “T” (see Table 3).
Common Causes of Ear Pain
ABNORMAL EAR EXAMINATION
Acute otitis media is probably the most common cause of primary otalgia 4, 9, 10. The tympanic membrane is classically red and bulging, but it can also be white or pink, and the discoloration sometimes involves only part of the tympanic membrane.
Otitis externa (or swimmer’s ear) generally leads to swelling and redness of the ear canal. There is often debris in the ear canal or covering the tympanic membrane 11. Subtle otitis externa can be difficult to identify on inspection, but it usually causes tenderness when the examiner pulls on the auricle or presses on the tragus.
Foreign bodies in the ear canal are most common in children. In one study, the most common objects removed were beads, paper, popcorn kernels, and insects 12. Most foreign bodies can be removed under direct visualization with a curette or alligator forceps. If this is not successful, the child should have removal of the foreign body under sedation and otomicroscopy 12. Although most foreign bodies in the ear canal can be managed nonurgently, hearing-aid batteries should be removed promptly to prevent alkali burns.
Barotrauma typically occurs while scuba diving or during an airplane flight with the onset of pain during descent.10 Eustachian tube dysfunction caused by an upper respiratory infection or allergic rhinitis increases the risk of barotrauma. The tympanic membrane is typically hemorrhagic, and there may be blood or serous fluid in the middle ear.
NORMAL EAR EXAMINATION
Temporomandibular joint (TMJ) syndrome is characterized by pain and crepitus with talking or chewing, and tenderness or crepitus on palpation of the TMJ joint 13. It causes ear pain, especially with chewing 13. However, TMJ crepitus is prevalent, and its presence should not prematurely halt further investigation into other causes of otalgia 4.
Dental causes of otalgia generally involve the molar teeth. A variety of dental diseases can produce otalgia, but the most common are caries, periodontal abscesses, and impacted third molars. The physician should palpate the gingiva and tap on the teeth with a tongue blade to assess for tenderness 5.
Pharyngitis and tonsillitis often cause referred pain to the ear. In some patients with pharyngitis, ear pain can be the primary complaint even when the ear is normal.
Idiopathic otalgia is common, but patients and physicians can be uncomfortable with this diagnosis. If a thorough evaluation is unrevealing and the physician suspects a benign cause, empiric treatment for TMJ syndrome with nonsteroidal anti-inflammatory drugs and a soft diet would be reasonable. If the physician suspects neuropathic pain, a trial of gabapentin (Neurontin) or amitriptyline is reasonable.
Uncommon Causes of Ear Pain
ABNORMAL EAR EXAMINATION
Malignant otitis externa is defined by osteitis of the skull base, typically caused by Pseudomonas infection, and it usually occurs in patients with diabetes or immunocompromise 4. It is characterized by severe, deep, unrelenting pain and by granulation tissue, which can be a subtle finding, on the inferior aspect of the external auditory canal at the bony-cartilaginous junction. Squamous cell carcinoma of the external auditory canal can mimic malignant otitis externa.
Ramsay Hunt syndrome (herpes zoster oticus) typically causes ear pain, facial paralysis, and vesicles in the external auditory canal. Other symptoms can include hearing loss, tinnitus, vertigo, taste disturbance, and decreased tearing 14. The syndrome is caused by herpes zoster involving the geniculate ganglion (cranial nerve VII), and it often involves cranial nerves V, IX, and X in addition to the facial nerve.
Relapsing polychondritis is a systemic disease that involves cartilage. It can affect many organs, including the eyes, nose, heart, kidneys, and nervous system, but the most commonly affected organ is the ear 15. Relapsing polychondritis often affects both ears, producing a red or violaceous auricle. Sparing of the earlobe, which lacks cartilage, helps distinguish auricular chondritis from cellulitis. It is diagnosed by its relapsing course and typical appearance.
Cholesteatomas are epidermal cysts composed of desquamating epithelium. They gradually enlarge and can erode the ossicular chain, inner ear, and bony facial nerve canal. Cholesteatomas generally do not cause severe pain, but may produce a sense of fullness. In patients with otorrhea or conductive hearing loss, it is important to visualize the most superior aspect of the tympanic membrane to exclude a superior retraction pocket leading to a cholesteatoma.
NORMAL EAR EXAMINATION
Tumors in the nose, nasopharynx, oral cavity, oropharynx, hypopharynx, infratemporal fossa, neck, or chest can cause ear pain. The most common sites are the base of the tongue, tonsillar fossa, and hypopharynx 7. Risk factors for head and neck tumors include tobacco or alcohol use, dysphagia, weight loss, radiation exposure, hoarseness, and age older than 50 years 16.
Neuralgias can involve cranial nerves V and IX, the geniculate ganglion (cranial nerve VII), and the sphenopalatine ganglion (cranial nerves V and VII). The best known of these is trigeminal neuralgia (tic douloureux), which is characterized by paroxysmal, sharp, lancinating pain in the distribution of the maxillary and mandibular divisions. Glossopharyngeal neuralgia causes pain in the tonsillar area, pharynx, and, in some patients, the middle ear; this pain may be elicited by palpation of the tonsillar region 5. Sphenopalatine neuralgia results in pain around the eye and nose in addition to the ear and mastoid 5.
Bell’s palsy is characterized by the sudden onset of upper and lower facial paralysis. Postauricular pain occurs in about 25 percent of patients 17. Patients may also have hyperacusis, taste disturbances, and decreased tearing.
Temporal arteritis often causes temporal pain and tenderness that can involve the ear. Other symptoms include malaise, weight loss, fever, and anorexia. It is important to recognize temporal arteritis because it can cause permanent blindness, but this is usually preventable with prompt initiation of systemic corticosteroids. Only about 40 percent of patients have tenderness in the temporal arteries, but 65 percent have at least one temporal artery abnormality (e.g., tenderness, absent pulse, beading, prominence) 18. Although temporal arteritis is unusual in patients younger than 50 years, it should be considered if there are multiple findings indicative of the disease 18. The disease is rare in patients with normal erythrocyte sedimentation rates and unusual if the erythrocyte sedimentation rate is less than 50 mm per hour 18.
Table 1. Causes of Ear Pain
| Lesions of the external auditory canal |
| Furuncle |
| External otitis (eczematoid or swimmer’s ear) |
| Impacted cerumen or foreign body |
| Traumatic effects (perforation from a slap on the ear) |
| Herpes zoster |
| Otomycosis |
| Skin tumors, benign and malignant |
| Granuloma of the ear |
| Malignant otitis externa (in diabetes) |
| Bell’s palsy |
| Bullous myringitis involving the canal |
| Exostoses of the canal with obstruction |
| Cholesteatoma and keratosis of the external canal |
| Local manifestations of generalized skin disorders (psoriasis, lupus, leukemia, mycosis fungoides) |
| Postradiation effects and postsurgical effects |
| Parotid or soft tissue disorders extending into the ear canal |
| Lesions of the middle ear |
| Acute otitis media |
| Otitis media with effusion (serous) |
| Acute exacerbation of chronic otitis media with or without drum perforation |
| Cholesteatoma |
| Polyps arising from tympanum |
| Acute mastoiditis |
| Glomus jugulare tumor or other tumors |
| Previous ventilation tube implant |
| Spasm of middle ear muscles |
Table 2. Conditions That May Cause Ear Pressure or Fullness but Little or No Ear Pain
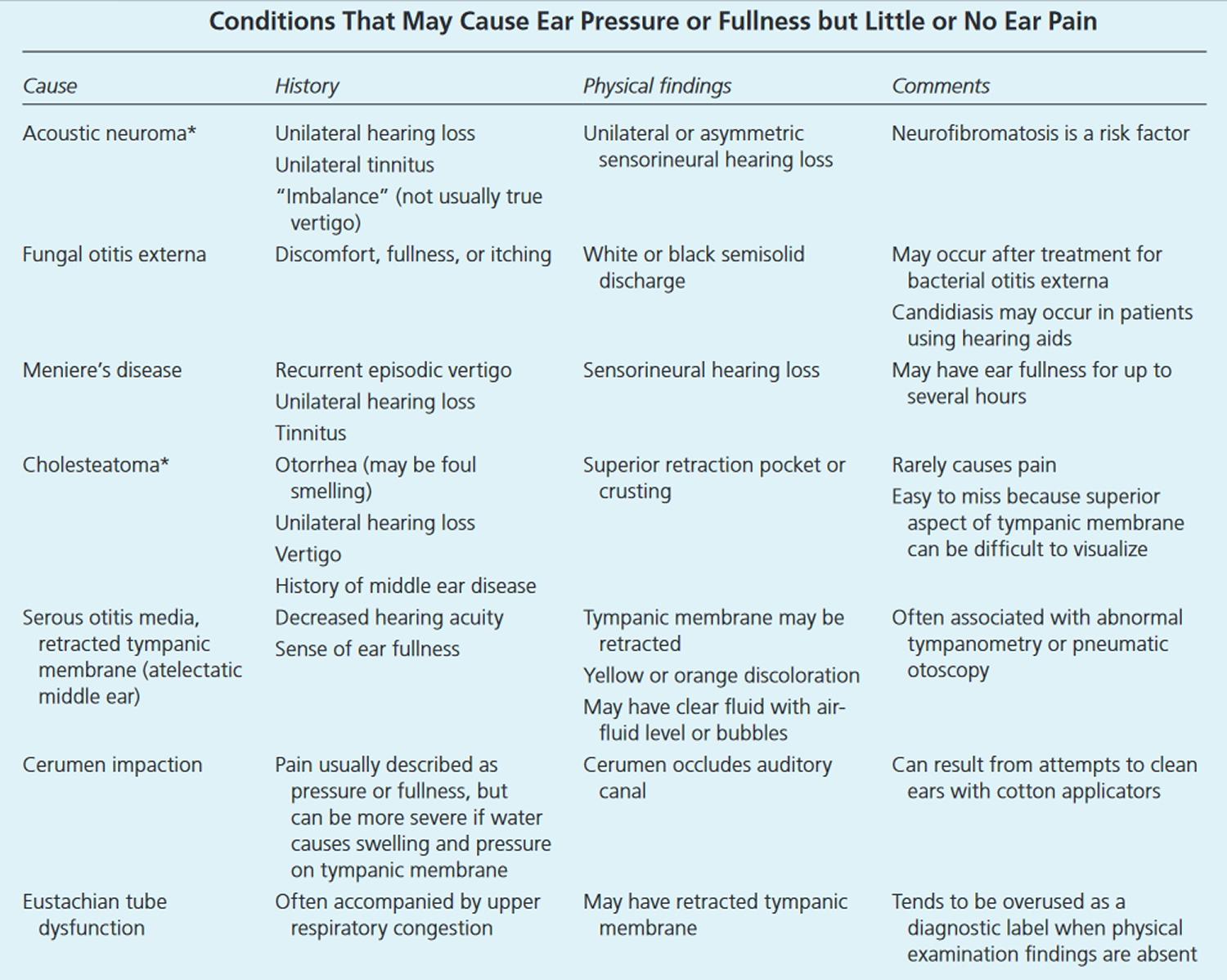
Table 3. Possible origins of referred ear pain
| Teeth | Trachea |
| Tongue | Temporomandibular joint |
| Tonsils | Tendons (hyoid, etc) |
| Tube (eustachian) | Tic (ninth nerve) |
| Throat | Thyroid |
Note: Acute and chronic forms of thyroiditis may present as throat and ear pain, but tenderness will be maximal over the thyroid lobe on that side. Inflammation of the carotid bulb (carotidynia) often presents in a similar manner. An unsuspected source of otalgia is elongation of the styloid process with protrusion into the tonsillar fossa (Eagle’s syndrome). Ear pain combined with throat discomfort should alert the examiner to palpate the tonsillar fossa.
[Source 1]Table 4. Common Causes of Ear Pain: Abnormal Ear Examination
| Cause | History | Physical findings | Comments |
|---|---|---|---|
Otitis media | Recent upper respiratory infection Night restlessness in children | Red or cloudy tympanic membrane that is immobile on pneumatic otoscopy | Most common cause of primary ear pain More common in winter |
Otitis externa | Recent swimming White discharge | Pain elicited by traction on auricle or pressure on tragus External auditory canal swollen and red with white debris1 | Findings can be subtle (consider empiric therapy) More common in summer Consider malignant (necrotizing) otitis externa in patients with diabetes or immunocompromise |
Foreign body | Insects, small objects Commonly occurs in children | Foreign body visible in ear canal | May need sedation for removal |
Barotrauma | Pain onset during descent of airplane or while scuba diving | Tympanic membrane hemorrhage Serous or hemorrhagic middle ear fluid | Otoscopic signs of barotrauma are present in 10 percent of adults and 22 percent of children after an airplane flight. |
Table 5. Common Causes of Ear Pain: Normal Ear Examination
| Cause | History | Physical findings | Comments |
|---|---|---|---|
Temporomandibular joint (TMJ) syndrome | Pain or crepitus with talking or chewing | Tender TMJ Crepitus or clicking on motion of mandible May have restricted jaw movement | Risk factors include clenching and biting inside of lips and mouth |
Dental causes (e.g., caries, periodontal abscess, impacted third molars, pulpitis) | May have dental complaints or history of dental disorders | Caries Abscess Gingivitis Facial swelling Teeth tender to percussion | Caries and abscess most common |
Pharyngitis or tonsillitis | Often accompanied by sore throat | Pharyngeal or tonsillar erythema Swelling Exudate | Otalgia can be the primary symptom even if ear not involved |
Cervical spine arthritis | Crepitus or pain with neck movement | Decreased neck range of motion Tender spinous processes or paraspinal muscles | Pain referred from C2, C3 cervical nerve roots |
Idiopathic | Variable | Normal | In practice, often labeled TMJ syndrome, neuropathic pain, or eustachian tube dysfunction |
Table 6. Uncommon Causes of Ear Pain: Abnormal Ear Examination
| Cause | History | Physical findings | Comments |
|---|---|---|---|
Malignant (necrotizing) otitis externa | Suspect in refractory otitis externa in patients with diabetes, older patients, and those with immunocompromise Pain disproportionate to examination findings | Granulation tissue on floor of external auditory canal | Easy to miss, findings can be subtle Obtain technetium bone scan to determine extent of disease and gallium tagged white-cell scan as baseline to follow response to treatment |
Ramsay Hunt syndrome (herpes zoster oticus) | Pain often precedes vesicles and is much worse than in Bell’s palsy Patient may have vertigo, hearing loss, or tinnitus | Vesicular rash on auricle and external auditory canal Palsy of cranial nerve VII (facial) | Can involve other cranial nerves (e.g., V [trigeminal], IX [glossopharyngeal], X [vagus]) Pain can occur without significant vesicular eruption |
Cellulitis/chondritis/perichondritis | Preceding insect bite, scratch, or piercing Rapid progression Perichondritis characterized by persistent redness, swelling, and pain | Earlobe usually involved with cellulitis | Perichondritis must be treated aggressively; sometimes requires parenteral antibiotics |
Relapsing polychondritis | Recurrent swelling and redness of auricle Hearing loss frequent | Earlobe is spared because it has no cartilage | Noninfectious Can involve other cartilage such as trachea and bronchi |
Trauma | Blunt or sharp trauma Frostbite Burns | Traumatic lesions of auricle, ear canal, or tympanic membrane | Most common injury is laceration of the auricle |
Mastoiditis | Recent or concurrent otitis media Retroauricular pain | Protrusion of auricle Tender edematous mastoid | Prevalence increased in children with limited access to health care |
Tumors or infected cysts in auricle or ear canal | Pain usually well localized to auricle or ear canal | May require meticulous examination of external auditory canal May need to remove cerumen | Diagnosis of ear canal tumors is often delayed because of misdiagnosis as chronic inflammation |
Wegener’s granulomatosis | Arthralgia Hearing loss Myalgias Oral or nasal ulcers Otorrhea Rhinorrhea | Often causes chronic otitis media or serous otitis | Consider testing for antineutrophil cytoplasmic antibodies |
Viral myringitis | Presentation similar to acute otitis media | Tympanic membrane red, but not bulging; landmarks visible |
Table 7. Uncommon Causes of Ear Pain: Normal Ear Examination
| Cause | History | Physical findings | Comments |
|---|---|---|---|
Tumors (e.g., parotid, hypopharynx, nasopharynx, base of tongue, tonsillar fossa, larynx, esophagus, intracranial, cervical spine)4 | Risk factors include smoking, alcohol use, age older than 50 years, hoarseness, dysphagia, radiation exposure, weight loss | May require fiberoptic nasolaryngoscopy | Consider referral for invasive examination and MRI |
Neuralgias (e.g., trigeminal, glossopharyngeal, geniculate, sphenopalatine) | Pain usually brief (seconds), severe, lancing, jabbing, electric-shock–like, episodic | Usually none May have trigger point | Trigeminal neuralgia (tic douloureux) best defined |
Bell’s palsy | Retroauricular pain, less severe than Ramsay Hunt syndrome; can precede or follow the palsy | Peripheral facial palsy (involvement of forehead) | Pain occurs in 25 to 50 percent of patients with Bell’s palsy |
Temporal arteritis | Age older than 50 years Jaw claudication Diplopia | Temporal arteries may be tender, prominent, or beaded | Erythrocyte sedimentation rate usually greater than 50 mm per hour Biopsy and prompt treatment are indicated |
Oral aphthous ulcers | Localized pain in mouth as well as ear | Shallow ulcers with gray, necrotic base | Often recurrent Etiology not well defined |
Cervical adenopathy | May have recent upper respiratory infection or scalp lesion | Tender cervical or periauricular lymph nodes | Consider CT and fine needle aspiration for lymph nodes > 1.5 cm, lasting longer than six weeks |
Myofascial pain, muscle spasm or inflammation of sternocleidomastoid or muscles of mastication | Pain aggravated by chewing or head movement | May have trigger point | Can be caused by clenching, bruxism, TMJ syndrome, and dental or oral disorders |
Eagle’s syndrome (elongation of styloid process) | Deep, unremitting pain exacerbated by swallowing, yawning, or chewing May have pain in neck, foreign body sensation in throat | Reproduce pain with tonsillar fossa palpation | Diagnosed with CT Most patients are 3 to 40 years of age and have had a tonsillectomy Styloid process longer than 1 inch (2.5 cm) |
Sinusitis/sinogenic referred pain from allergy | Nasal congestion Pain in maxillary sinuses | Nasal congestion Tender over maxillary sinuses | Sinusitis is common but otalgia from sinusitis is unusual |
Carotidynia | May have dysphagia and throat tenderness | Tender carotid artery | More common in women May have abnormal enhancement on MRI |
Thyroiditis | May report pain in thyroid | Thyroid may be tender or enlarged | Referred pain from cranial nerve X (vagus) |
Salivary gland disorders (e.g., stones, mumps) | Pain in preauricular area | Prominent, tender parotid glands | There have been recent epidemics of mumps in the United States |
Cricoarytenoid arthritis | Ear pain and hoarseness Pain is worse with speaking, coughing, or swallowing | May have other features of inflammatory arthritis | Often caused by rheumatoid arthritis or systemic lupus erythematosus |
Gastroesophageal reflux | Heartburn Acid reflux | Usually none | Pain caused by irritation of oropharynx (cranial nerves IX [glossopharyngeal] and X) or of eustachian tube orifice |
Angina pectoris, myocardial infarction | Cardiac risk factors | Usually none | If suspected, obtain electrocardiogram and serum troponin level |
Thoracic aneurysms (e.g., innominate artery, thoracic aorta) | More common in older men May have hypertension and other risk factors for atherosclerosis | May have chest or back pain | Obtain chest CT scan or magnetic resonance angiogram; plain chest radiography is insensitive |
Psychogenic (e.g., depression, anxiety) | History of depression or anxiety | Blunted affect Depressed mood | Consider in patients with idiopathic otalgia |
Other rare causes (e.g., subdural hematoma, lung cancer, central line placement, pillow otalgia, carotid artery aneurysm) |
Diagnosis of ear pain
HISTORY
Key points in the history include the patient’s age, the location of pain (asking the patient to point with one finger), the radiation of pain, aggravating factors (e.g., chewing), associated symptoms (otologic and systemic), and risk factors for tumor (e.g., age older than 50 years, tobacco or alcohol use). Otologic symptoms that favor a primary cause include discharge, tinnitus, hearing loss, and vertigo. The severity of pain is not necessarily correlated with the seriousness of the cause. For example, the pain from tumors can be mild, whereas the pain from dental caries and otitis media can be severe.
PHYSICAL EXAMINATION
Key components of the physical examination include inspection of the auricle and periauricular region and a thorough otoscopic examination, which may require cerumen removal. Tenderness that occurs with traction on the auricle or pressure on the tragus indicates a condition of the external auditory canal, usually otitis externa.
When the ear examination is normal, the physician should palpate the temporomandibular joint (TMJ) for tenderness and crepitus as the patient opens and closes the mouth.
In addition, the basic examination should include inspection of the nose and oropharynx, palpation of the head and neck, and examination of the cranial nerves. The gingiva should be inspected and palpated and the teeth inspected and percussed to assess tenderness. Fiberoptic nasolaryngoscopy is not usually necessary. Patients may need this procedure if they have risk factors for tumor or if conservative measures do not resolve symptoms.
DIAGNOSTIC TESTS
An assessment of hearing, by audiometry or simple testing (i.e., finger rub or whispered voice), is indicated in patients who notice hearing loss. An assessment of tympanic membrane mobility with pneumatic otoscopy or tympanometry can be helpful if there is suspicion of middle ear disease. When the physical examination is normal and the goal is to rule out tumor, the patient should have nasolaryngoscopy and magnetic resonance imaging (MRI) of the head and neck with gadolinium contrast 7. When the disease is evident on examination and the goal is to determine the extent of involvement, computed tomography (CT) with contrast media is generally indicated. For example, temporal bone trauma should be evaluated with CT scanning.
RULE OUT WORST-CASE SCENARIO
As with any symptom, a “rule out worst-case scenario” strategy (in which certain diagnoses must be ruled out immediately) may help avoid serious diagnostic errors.40 In patients with otalgia, physicians should rule out several potential causes that can have serious consequences if the diagnosis is delayed; these are malignant (necrotizing) otitis externa, cholesteatoma, myocardial infarction, temporal arteritis, and malignant tumor. However, these diseases can often be ruled out on the basis of a nonworrisome history and physical examination rather than extensive testing. Risk factors that should prompt consideration of these diseases are outlined in Table 8.
Table 8. Risk Factors for “Worst-Case Scenario” Diagnoses in Patients with Ear Pain
| Risk factor | Possible diagnosis |
|---|---|
Age older than 50 years, ESR (erythrocyte sedimentation rate) greater than 50 mm per hour | Temporal arteritis |
Coronary artery disease risk factors | Heart attack |
Diabetes or immunocompromise | Malignant (necrotizing) otitis externa |
Tobacco and alcohol use, dysphagia, weight loss, age older than 50 years | Head or neck tumor |
Superior tympanic membrane retraction pocket, otorrhea | Cholesteatoma |
Unilateral hearing loss | Malignant otitis externa, cholesteatoma |
If the diagnosis is not clear from the history and physical examination, options include a trial of symptomatic treatment without a clear diagnosis; imaging studies; and consultation with an otolaryngologist (ear, nose and throat specialist). Patients who smoke, drink alcohol, are older than 50 years, or have diabetes are at higher risk of a cause of ear pain that needs further evaluation. Patients whose history or physical examination increases suspicion for a serious occult cause of ear pain or whose symptoms persist after symptomatic treatment should be considered for further evaluation, such as magnetic resonance imaging, fiberoptic nasolaryngoscopy, or an erythrocyte sedimentation rate measurement.
Acute otitis externa
Otitis externa, also called swimmer’s ear, involves diffuse inflammation of the external ear canal that may extend distally to the pinna and proximally to the tympanic membrane 21. The acute form has an annual incidence of approximately 1 percent 22 and a lifetime prevalence of 10 percent 23. On rare occasions, the infection invades the surrounding soft tissue and bone; this is known as malignant (necrotizing) otitis externa, and is a medical emergency that occurs primarily in older patients with diabetes mellitus 24. Otitis externa lasting three months or longer, known as chronic otitis externa, is often the result of allergies, chronic dermatologic conditions, or inadequately treated acute otitis externa.
In North America, 98 percent of cases of acute otitis externa are caused by bacteria 25. The two most common isolates are Pseudomonas aeruginosa and Staphylococcus aureus. However, a wide variety of other aerobic and anaerobic bacteria have been isolated 26, 27. Approximately one-third of cases are polymicrobial 25. Fungal pathogens, primarily those of the Aspergillus and Candida species, occur more often in tropical or subtropical environments and in patients previously treated with antibiotics 28, 29, 30. Otomycosis is classically associated with itching, thick material in the ear canal, and failure to improve with use of topical antibacterials. Otomycosis can sometimes be identified during otoscopy, although nonpathogenic saprophytic fungi may also be found. Inflammatory skin disorders and allergic reactions may cause noninfectious otitis externa, which can be chronic.
Malignant otitis externa may be suspected in older patients with diabetes mellitus or immunocompromise who have refractory purulent otorrhea and severe otalgia that may worsen at night. Clinical findings include granulation tissue in the external auditory canal, especially at the bone-cartilage junction. Extension of the infection beyond the auditory canal can cause lymphadenopathy, trismus, and facial nerve and other cranial nerve palsies.
Risk Factors for otitis externa
Several factors may predispose patients to the development of acute otitis externa (Table 9) 25, 31. One of the most common predisposing factors is swimming, especially in fresh water. Other factors include skin conditions such as eczema and seborrhea, trauma from cerumen removal, use of external devices such as hearing aids, and cerumen buildup 25. These factors appear to work primarily through loss of the protective cerumen barrier, disruption of the epithelium (including maceration from water retention), inoculation with bacteria, and increase in the pH of the ear canal 31, 32, 33.
Table 9. Predisposing Factors for Otitis Externa
Anatomic abnormalities |
Canal stenosis |
Exostoses |
Hairy ear canals |
Canal obstruction |
Cerumen obstruction |
Foreign body |
Sebaceous cyst |
Cerumen/epithelial integrity |
Cerumen removal |
Earplugs |
Hearing aids |
Instrumentation/itching |
Dermatologic conditions |
Eczema |
Psoriasis |
Seborrhea |
Other inflammatory dermatoses |
Water in ear canal |
Humidity |
Sweating |
Swimming or other prolonged water exposure |
Miscellaneous |
Purulent otorrhea from otitis media |
Soap |
Stress |
Type A blood |
Prevention of Otitis Externa
A number of preventive measures have been recommended, including use of earplugs while swimming, use of hair dryers on the lowest settings and head tilting to remove water from the ear canal, and avoidance of self-cleaning or scratching the ear canal. Acetic acid 2% (Vosol) otic solutions are also used, either two drops twice daily or two to five drops after water exposure. However, no randomized trials have examined the effectiveness of any of these measures.
Diagnosis of Otitis Externa
Acute otitis externa is diagnosed clinically based on signs and symptoms of canal inflammation. Presentation can range from mild discomfort, itching, and minimal edema to severe pain, complete canal obstruction, and involvement of the pinna and surrounding skin. Pain is the symptom that best correlates with the severity of disease 34. Mild fever may be present, but a temperature greater than 101°F (38.3°C) suggests extension beyond the auditory canal.
Onset of symptoms within 48 hours in the past three weeks and
Symptoms of ear canal inflammation 35:
- Ear pain, itching, or fullness
- With or without hearing loss or jaw pain
and
Signs of ear canal inflammation 35:
- Tenderness of tragus/pinna or ear canal edema/erythema
- With or without otorrhea, tympanic membrane erythema, cellulitis of the pinna, or local lymphadenitis
Table 10. Conditions That May Be Confused with Acute Otitis Externa
| Condition | Distinguishing characteristics | Comment |
|---|---|---|
Acute otitis media | Presence of middle ear effusion, no tragal/pinnal tenderness | Use pneumatic otoscopy or tympanometry, treat with systemic antibiotics |
Chronic otitis externa | Itching is often predominant symptom, erythematous canal, lasts more than three months | Treat underlying causes/conditions |
Chronic suppurative otitis media | Chronic otorrhea, nonintact tympanic membrane | Control otitis externa symptoms, then treat otitis media |
Contact dermatitis | Allergic reaction to materials (e.g., metals, soaps, plastics) in contact with the skin/epithelium; itching is predominant symptom | Check for piercings, hearing aids, or earplug use; discontinue exposure when possible |
Eczema | Itching is predominant symptom; often chronic; history of atopy, outbreaks in other locations | Consider treatment with topical corticosteroids |
Furunculosis | Focal infection, may be pustule or nodule, often in distal canal | Consider treatment with heat, incision and drainage, or systemic antibiotics; can progress to diffuse otitis externa |
Malignant otitis externa | High fever, granulation tissue or necrotic tissue in ear canal, may have cranial nerve involvement; patient with diabetes mellitus or immunocompromise, elevated erythrocyte sedimentation rate, findings on computed tomography | Medical emergency with high morbidity rate and possible mortality; warrants emergent consultation with otolaryngologist, hospitalization, intravenous antibiotics, debridement |
Myringitis | Tympanic membrane inflammation, may have vesicles; pain is often severe, no canal edema | Usually results from acute otitis media or viral infection |
Otomycosis | Itching is predominant symptom, thick material in canal, less edema; may see fungal elements on otoscopy | Can coexist with bacterial infections; treat with acetic acid (Vosol), half acetic acid/half alcohol, or topical antifungals; meticulous cleaning of ear canal |
Ramsay Hunt syndrome | Herpetic ulcers in canal; may have facial numbness/paralysis, severe pain, loss of taste | Treatment includes antivirals, systemic corticosteroids |
Referred pain | Normal ear examination | Look for other causes based on patterns of referred pain |
Seborrhea | Itching and rash on hairline, face, scalp | Treatment includes lubricating or moisturizing the external auditory canal |
Sensitization to otics | Severe itching, maculopapular or erythematous rash in conchal bowl and canal; may have streak on pinna where preparation contacted skin; vesicles may be present | Type IV delayed hypersensitivity reaction to neomycin or other components of otic solutions; discontinue offending agent; treat with topical corticosteroids |
Chronic otitis externa
In chronic otitis externa, the symptoms and signs occur for more than three months. Classic symptoms include itching and mild discomfort; there may also be lichenification on otoscopy.
Treatment of otitis externa
TOPICAL MEDICATIONS
Topical antimicrobials, with or without topical corticosteroids, are the mainstay of treatment for uncomplicated acute otitis externa. Topical antimicrobials are highly effective compared with placebo, demonstrating an absolute increase in clinical cure rate of 46 percent or a number needed to treat of slightly more than two 25. Topical agents come in a variety of preparations and combinations; a recent systematic review included 26 different topical interventions 36. In some studies, ophthalmic preparations have been used off-label to treat otitis externa 37, 36. Ophthalmic preparations may be better tolerated than otic preparations, possibly due to differences in pH between the preparations, and may help facilitate compliance with treatment recommendations. Commonly studied antimicrobial agents include aminoglycosides, polymyxin B, quinolones, and acetic acid. No consistent evidence has shown that any one agent or preparation is more effective than another 25, 38, 37, 36. There is limited evidence that use of acetic acid alone may require two additional days for resolution of symptoms compared with other agents, and that it is less effective if treatment is required for more than seven days 36.
Current guidelines recommend factoring in the risk of adverse effects, adherence issues, cost, patient preference, and physician experience. Some components found in otic preparations may cause contact dermatitis 39. Hypersensitivity to aminoglycosides, particularly neomycin, may develop in up to 15 percent of the population, and has been identified in approximately 30 percent of patients who also have chronic or eczematous otitis externa 39, 40. Adherence to topical therapy increases with ease of administration, such as less frequent dosing 41. The addition of a topical corticosteroid yields more rapid improvement in symptoms such as pain, canal edema, and erythema. Cost varies considerably for the different preparations.
Ear infection pain relief
Pain is a common symptom of acute otitis externa, and can be debilitating 33. Oral analgesics are the preferred treatment. First-line analgesics include nonsteroidal anti-inflammatory drugs and acetaminophen. When ongoing frequent dosing is required to control pain, medications should be administered on a scheduled rather than as-needed basis. Opioid combination pills may be used when symptom severity warrants. Benzocaine otic preparations may compromise the effectiveness of otic antibiotic drops by limiting contact between the drop and the ear canal. The lack of published data supporting the effectiveness of topical benzocaine preparations in otitis externa limits the role of such treatments 21.
CLEANING THE EAR CANAL
Acute otitis externa can be associated with copious material in the ear canal. Consensus guidelines published by the American Academy of Otolaryngology recommend that such material be removed to achieve optimal effectiveness of the topical antibiotics 25, 38. However, no randomized controlled trials have examined the effectiveness of aural toilet, and this is not typically done in most primary care settings 36. Topical medications rely on direct contact with the infected skin of the ear canal; hence, aural toilet takes on greater importance when the volume or thickness of the debris in the ear canal is great. Guidelines recommend aural toilet by gentle lavage suctioning or dry mopping under otoscopic or microscopic visualization to remove obstructing material and to verify tympanic membrane integrity 25. Lavage should be used only if the tympanic membrane is known to be intact, and should not be performed on patients with diabetes because of the potential risk of causing malignant otitis externa 25. Pain medications may be required during the procedure.
Treatment of chronic otitis externa
The treatment of chronic otitis externa depends on the underlying causes. Because most cases are caused by allergies or inflammatory dermatologic conditions, treatment includes the removal of offending agents and the use of topical or systemic corticosteroids. Chronic or intermittent otorrhea over weeks to months, particularly with an open tympanic membrane, suggests the presence of chronic suppurative otitis media. Initial treatment efforts are similar to those for acute otitis media. With control of the symptoms of otitis externa, attention can shift to the management of chronic suppurative otitis media.
Follow-up and Referral
Most patients will experience considerable improvement in symptoms after one day of treatment. If there is no improvement within 48 to 72 hours, physicians should reevaluate for treatment adherence, misdiagnosis, sensitivity to ear drops, or continued canal patency. The physician should consider culturing material from the canal to identify fungal and antibiotic-resistant pathogens if the patient does not improve after initial treatment efforts or has one or more predisposing risk factors, or if there is suspicion that the infection has extended beyond the external auditory canal. There is a lack of data regarding optimal length of treatment; as a general rule, antimicrobial otics should be administered for seven to 10 days, although in some cases complete resolution of symptoms may take up to four weeks 25, 36.
Consultation with an otolaryngologist or infectious disease subspecialist may be warranted if malignant otitis externa is suspected; in cases of severe disease, lack of improvement or worsening of symptoms despite treatment, and unsuccessful lavage; or if the primary care physician determines that aural toilet or ear wick insertion is warranted, but is unfamiliar with or concerned about performing the procedure.
- Turner JS JR.. Otalgia and Otorrhea. In: Walker HK, Hall WD, Hurst JW, editors. Clinical Methods: The History, Physical, and Laboratory Examinations. 3rd edition. Boston: Butterworths; 1990. Chapter 122. Available from: https://www.ncbi.nlm.nih.gov/books/NBK227/[↩][↩][↩]
- Diagnosis of Ear Pain. Am Fam Physician. 2008 Mar 1;77(5):621-628. http://www.aafp.org/afp/2008/0301/p621.html[↩][↩][↩]
- Turner JS JR.. Otalgia and Otorrhea. In: Walker HK, Hall WD, Hurst JW, editors. Clinical Methods: The History, Physical, and Laboratory Examinations. 3rd edition. Boston: Butterworths; 1990. Chapter 122. Available from: https://www.ncbi.nlm.nih.gov/books/NBK227/[↩]
- Shah RK, Blevins NH. Otalgia. Otolaryngol Clin North Am. 2003;36(6):1137–1151.[↩][↩][↩][↩][↩][↩]
- Yanagisawa K, Kveton JF. Referred otalgia. Am J Otolaryngol. 1992;13(6):323–327.[↩][↩][↩][↩]
- Fisher EW, Parikh AA, Harcourt JP, Wright A. The burden of screening for acoustic neuroma: asymmetric otological symptoms in the ENT clinic. Clin Otolaryngol Allied Sci. 1994;19(1):19–21.[↩]
- Leonetti JP, Li J, Smith PG. Otalgia. An isolated symptom of malignant infratemporal tumors. Am J Otol. 1998;19(4):496–498.[↩][↩][↩]
- Leung AK, Fong JH, Leong AG. Otalgia in children. J Natl Med Assoc. 2000;92(5):254–260.[↩]
- Uhari M, Niemelä M, Hietala J. Prediction of acute otitis media with symptoms and signs. Acta Paediatr. 1995;84(1):90–92.[↩]
- Stewart MH, Siff JE, Cydulka RK. Evaluation of the patient with sore throat, earache, and sinusitis: an evidence based approach. Emerg Med Clin North Am. 1999;17(1):153–187, ix.[↩]
- Agius AM, Pickles JM, Burch KL. A prospective study of otitis externa. Clin Otolaryngol Allied Sci. 1992;17(2):150–154.[↩]
- Schulze SL, Kerschner J, Beste D. Pediatric external auditory canal foreign bodies: a review of 698 cases. Otolaryngol Head Neck Surg. 2002;127(1):73–78.[↩][↩]
- Bonjardim LR, Gaviao MB, Carmagnani FG, Pereira LJ, Castelo PM. Signs and symptoms of temporomandibular joint dysfunction in children with primary dentition. J Clin Pediatr Dent. 2003;28(1):53–58.[↩][↩]
- Adour KK. Otological complications of herpes zoster. Ann Neurol. 1994;(35 suppl):S62–S64.[↩]
- Rampelberg O, Gerard JM, Namias B, Gerard M. ENT manifestations of relapsing polychondritis. Acta Otorhinolaryngol Belg. 1997;51(2):73–77.[↩]
- Chida K, Okita N, Takase S. Retroauricular pain preceding Bell’s palsy: report of three cases and clinical analysis. Tohoku J Exp Med. 2002;197(3):139–143.[↩]
- Kasse CA, Cruz OL, Leonhardt FD, Testa JR, Ferri RG, Viertler EY. The value of prognostic clinical data in Bell’s palsy. Rev Bras Otorinolaringol (Engl Ed). 2005;71(4):454–458.[↩]
- Smetana GW, Shmerling RH. Does this patient have temporal arteritis? JAMA. 2002;287(1):92–101.[↩][↩][↩]
- American Academy of Family Physicians. Diagnosis of Ear Pain. http://www.aafp.org/afp/2008/0301/afp20080301p621-s1.pdf[↩]
- American Academy of Family Physicians. Diagnosis of Ear Pain. http://www.aafp.org/afp/2008/0301/p621.html[↩][↩][↩][↩][↩]
- Acute Otitis Externa: An Update. Am Fam Physician. 2012 Dec 1;86(11):1055-1061. http://www.aafp.org/afp/2012/1201/p1055.html[↩][↩][↩][↩]
- Rowlands S, Devalia H, Smith C, Hubbard R, Dean A. Otitis externa in UK general practice: a survey using the UK General Practice Research Database. Br J Gen Pract. 2001;51(468):533–538.[↩]
- Raza SA, Denholm SW, Wong JC. An audit of the management of acute otitis externa in an ENT casualty clinic. J Laryngol Otol. 1995;109(2):130–133.[↩]
- Rubin Grandis J, Branstetter BF IV, Yu VL. The changing face of malignant (necrotising) external otitis: clinical, radiological, and anatomic correlations. Lancet Infect Dis. 2004;4(1):34–39.[↩]
- Rosenfeld RM, Brown L, Cannon CR, et al.; American Academy of Otolaryngology–Head and Neck Surgery Foundation. Clinical practice guideline: acute otitis externa. Otolaryngol Head Neck Surg. 2006;134(4 suppl):S4–S23.[↩][↩][↩][↩][↩][↩][↩][↩][↩][↩]
- Ninkovic G, Dullo V, Saunders NC. Microbiology of otitis externa in the secondary care in United Kingdom and antimicrobial sensitivity. Auris Nasus Larynx. 2008;35(4):480–484.[↩]
- Roland PS, Stroman DW. Microbiology of acute otitis externa. Laryngoscope. 2002;112(7 pt 1):1166–1177.[↩]
- Martin TJ, Kerschner JE, Flanary VA. Fungal causes of otitis externa and tympanostomy tube otorrhea. Int J Pediatr Otorhinolaryngol. 2005;69(11):1503–1508.[↩]
- Pontes ZB, Silva AD, Lima Ede O, et al. Otomycosis: a retrospective study. Braz J Otorhinolaryngol. 2009;75(3):367–370.[↩]
- Ahmad N, Etheridge C, Farrington M, Baguley DM. Prospective study of the microbiological flora of hearing aid moulds and the efficacy of current cleaning techniques. J Laryngol Otol. 2007;121(2):110–113.[↩]
- Russell JD, Donnelly M, McShane DP, Alun-Jones T, Walsh M. What causes acute otitis externa? J Laryngol Otol. 1993;107(10):898–901.[↩][↩]
- Kim JK, Cho JH. Change of external auditory canal pH in acute otitis externa. Ann Otol Rhinol Laryngol. 2009;118(11):769–772.[↩]
- van Asperen IA, de Rover CM, Schijven JF, et al. Risk of otitis externa after swimming in recreational fresh water lakes containing Pseudomonas aeruginosa. BMJ. 1995;311(7017):1407–1410.[↩][↩]
- Halpern MT, Palmer CS, Seidlin M. Treatment patterns for otitis externa. J Am Board Fam Pract. 1999;12(1):1–7.[↩]
- Rosenfeld RM, Brown L, Cannon CR, et al.; American Academy of Otolaryngology–Head and Neck Surgery Foundation. Clinical practice guideline: acute otitis externa. Otolaryngol Head Neck Surg. 2006;134(4 suppl):S5.[↩][↩]
- Kaushik V, Malik T, Saeed SR. Interventions for acute otitis externa. Cochrane Database Syst Rev. 2010(1):CD004740.[↩][↩][↩][↩][↩][↩]
- Rosenfeld RM, Singer M, Wasserman JM, Stinnett SS. Systematic review of topical antimicrobial therapy for acute otitis externa. Otolaryngol Head Neck Surg. 2006;134(4 suppl):S24–S48.[↩][↩]
- Hajioff D, Mackeith S. Otitis externa. Clin Evid (Online). 2010.[↩][↩]
- Smith IM, Keay DG, Buxton PK. Contact hypersensitivity in patients with chronic otitis externa. Clin Otolaryngol Allied Sci. 1990;15(2):155–158.[↩][↩]
- Yariktas M, Yildirim M, Doner F, Baysal V, Dogru H. Allergic contact dermatitis prevalence in patients with eczematous external otitis. Asian Pac J Allergy Immunol. 2004;22(1):7–10.[↩]
- Shikiar R, Halpern MT, McGann M, Palmer CS, Seidlin M. The relation of patient satisfaction with treatment of otitis externa to clinical outcomes: development of an instrument. Clin Ther. 1999;21(6):1091–1104.[↩]





{kind=link}