Contents
What is retinal detachment
Retinal detachment refers to an eye condition in which the eye’s retina becomes detached from the vitreous fluid and layers of tissue that surround and support it. The retina is a layer of tissue in the back of your eye that senses light and sends images to your brain. It provides the sharp, central vision needed for reading, driving, and seeing fine detail. If your retina is damaged, you can lose you vision.
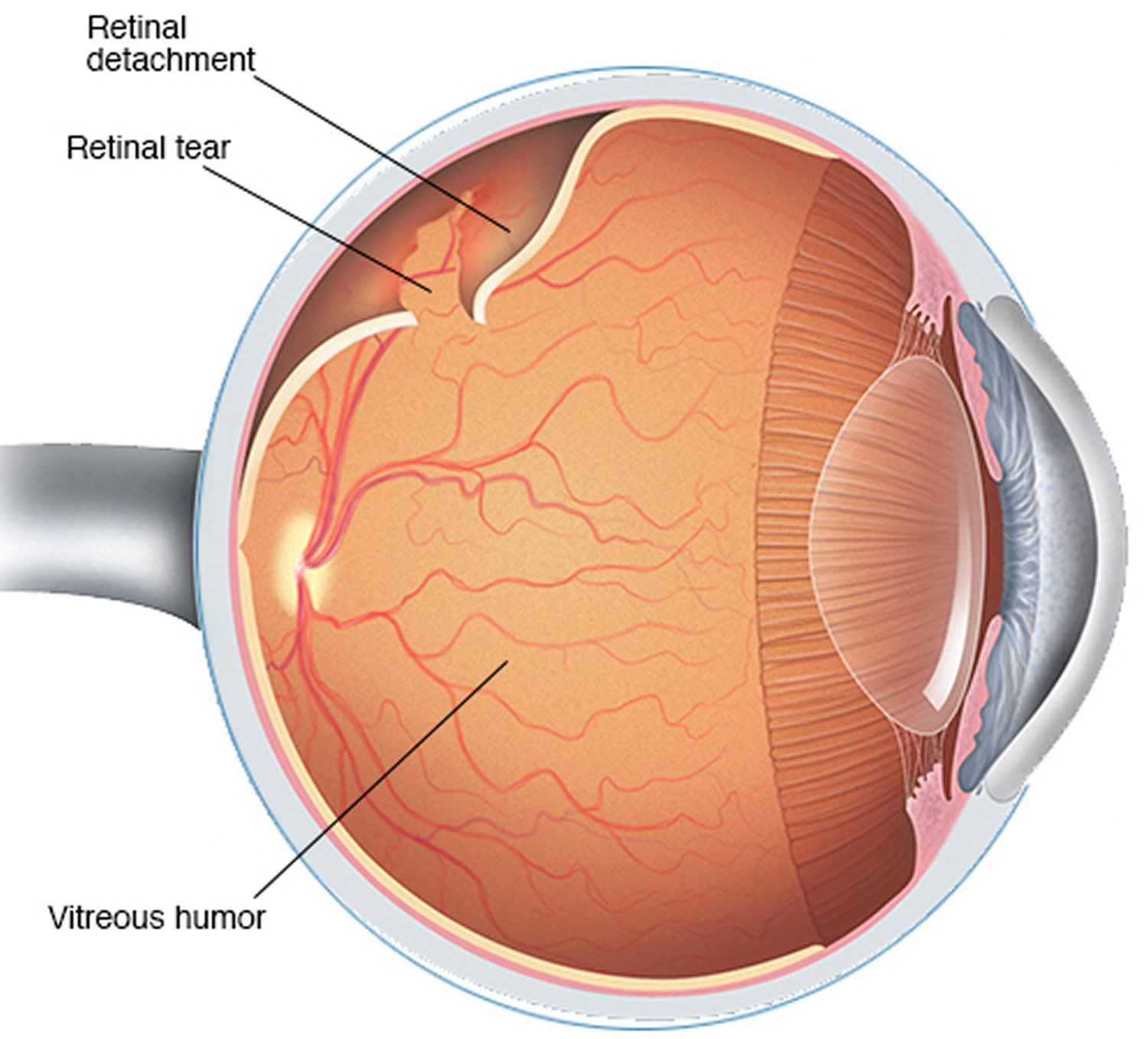
Retinal detachment often occurs as a result of a tear or hole in the retina, through which fluid can leak. The fluid creates pressure which causes the retina to move away and detach from the tissues which surround it. The condition may cause blurred vision and/or floating spots, blind spots or shadows in the vision.
- Retinal detachment is a medical emergency and needs to be treated quickly to stop it permanently affecting your sight.
Retinal detachment typically requires surgical treatment. Most of the time, retinal detachment is treated successfully. But the longer the delay before surgery, the harder it is to fix.
Retinal detachment can occur at any age, but it is more common in people over age 40. It affects men more than women and whites more than African Americans. A retinal detachment is also more likely to occur in people who:
- Are extremely nearsighted (myopia)
- Have had a retinal detachment in the other eye
- Have a family history of retinal detachment
- Have had cataract surgery
- Have other eye diseases or disorders
- Have had an eye injury
Retinal detachment itself is painless. But warning signs almost always appear before it occurs or has advanced, such as:
- The sudden appearance of many floaters — tiny specks that seem to drift through your field of vision
- Flashes of light or “cobwebs” in one or both eyes
- Blurred vision
- Gradually reduced side (peripheral) vision
- A curtain-like shadow over your visual field
A retinal detachment is a medical emergency. Anyone experiencing the symptoms of a retinal detachment should see an eye care professional immediately.
Get an urgent medical attention if:
- dots or lines (floaters) suddenly appear in your vision or suddenly increase in number
- you get flashes of light in your vision
- you have a dark “curtain” or shadow moving across your vision
These could be symptoms of a detached retina.
Retinal detachment is a medical emergency in which you can permanently lose your vision.
Figure 1. Structure of the human eye
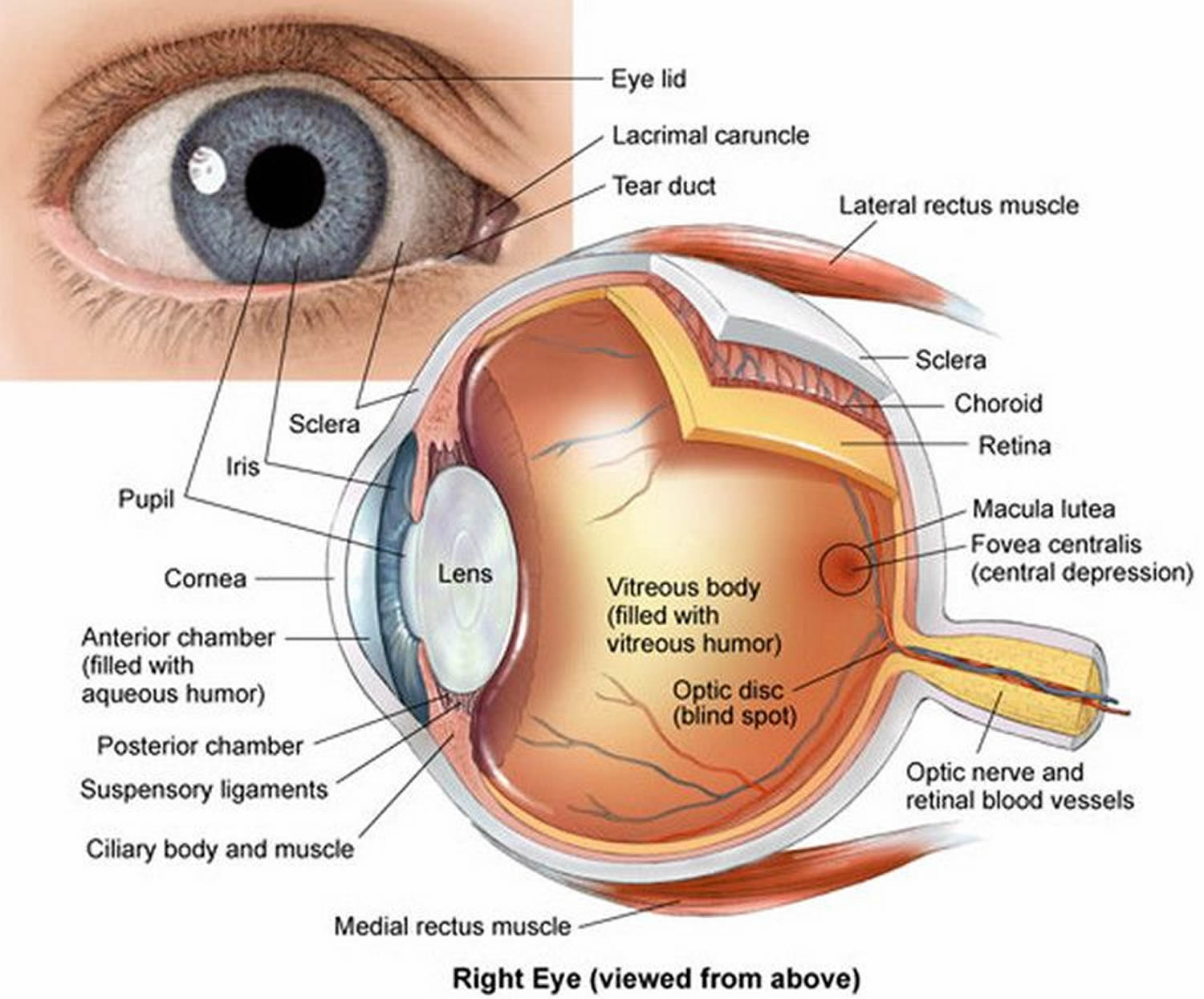
Figure 2. The retina (inside human eye) – the retina is the section of the eye that processes light signals and converts them to nerve impulses for processing in the brain.
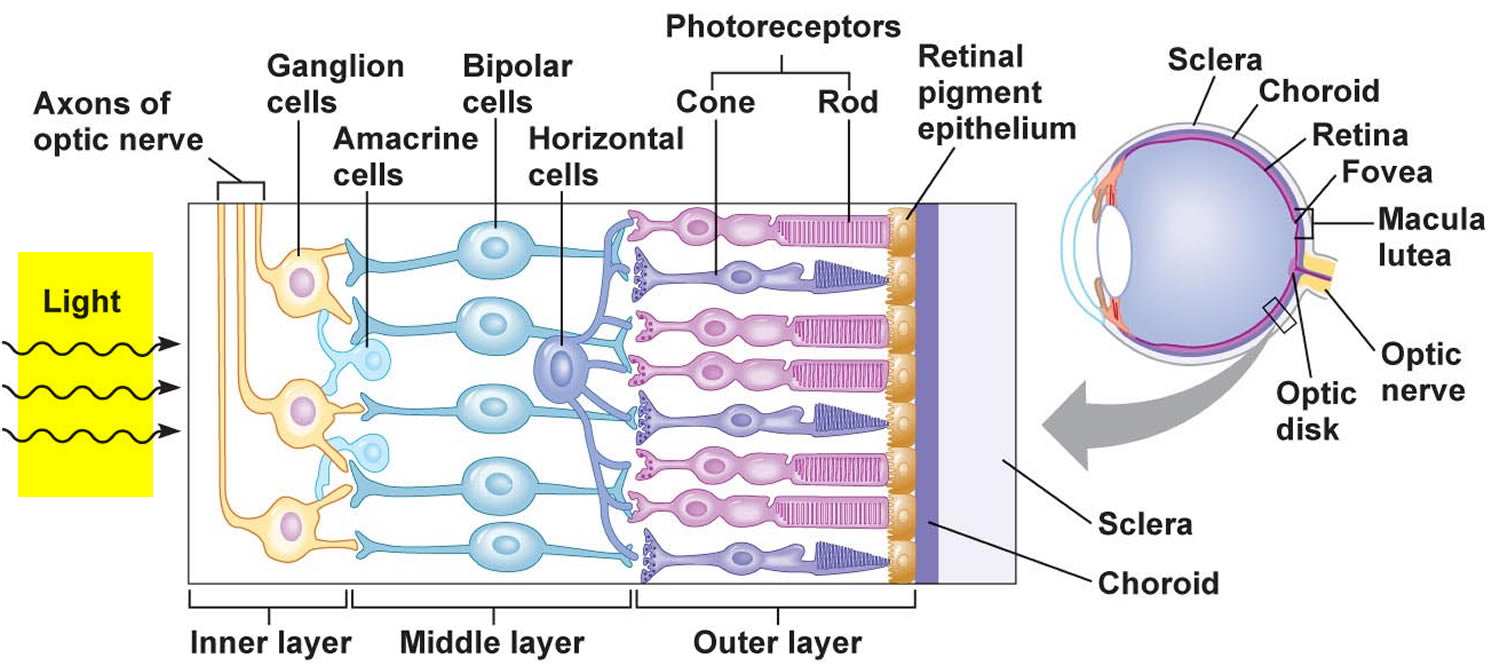
Figure 3. Normal eye refraction (perfect image on the Macula’s Fovea)
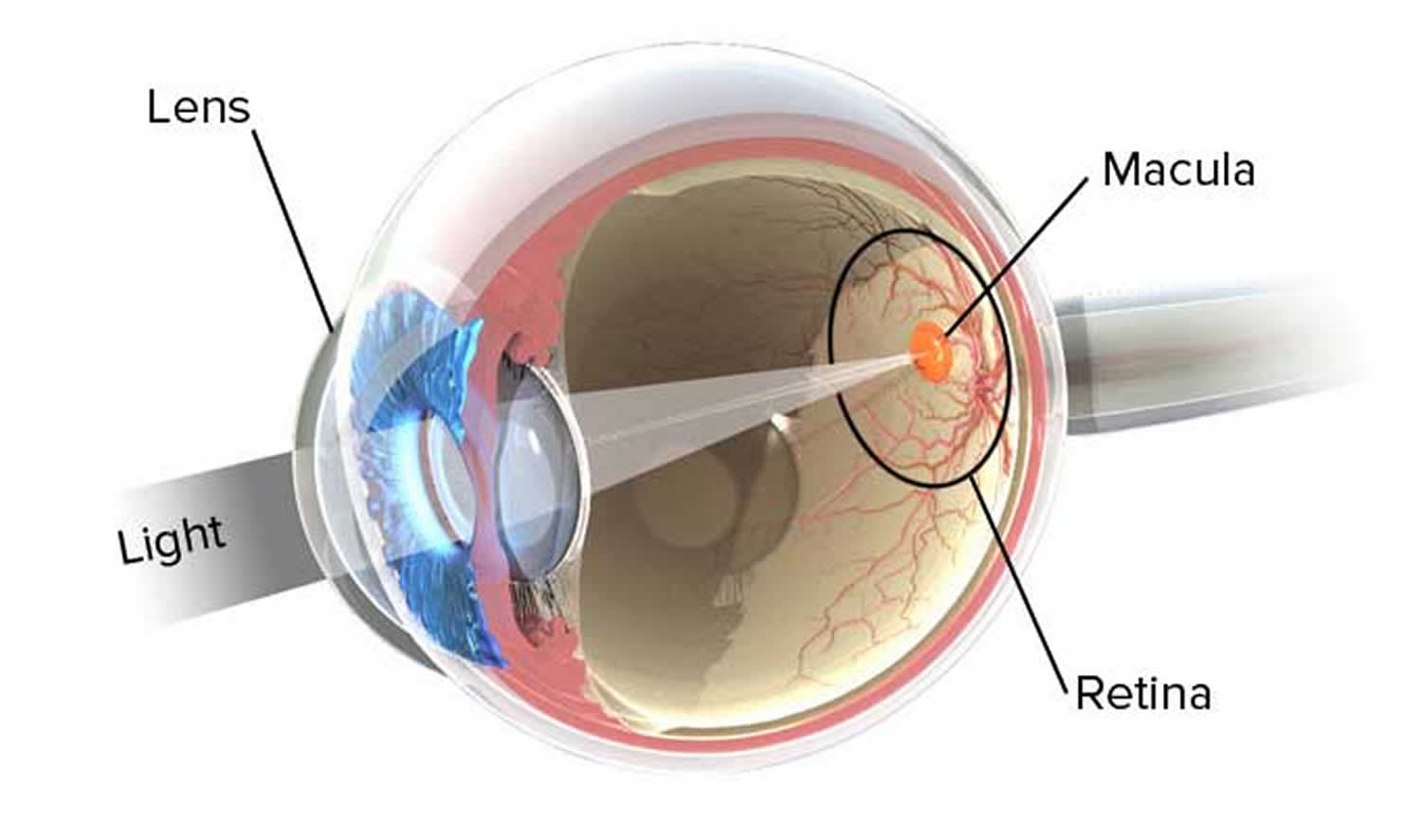
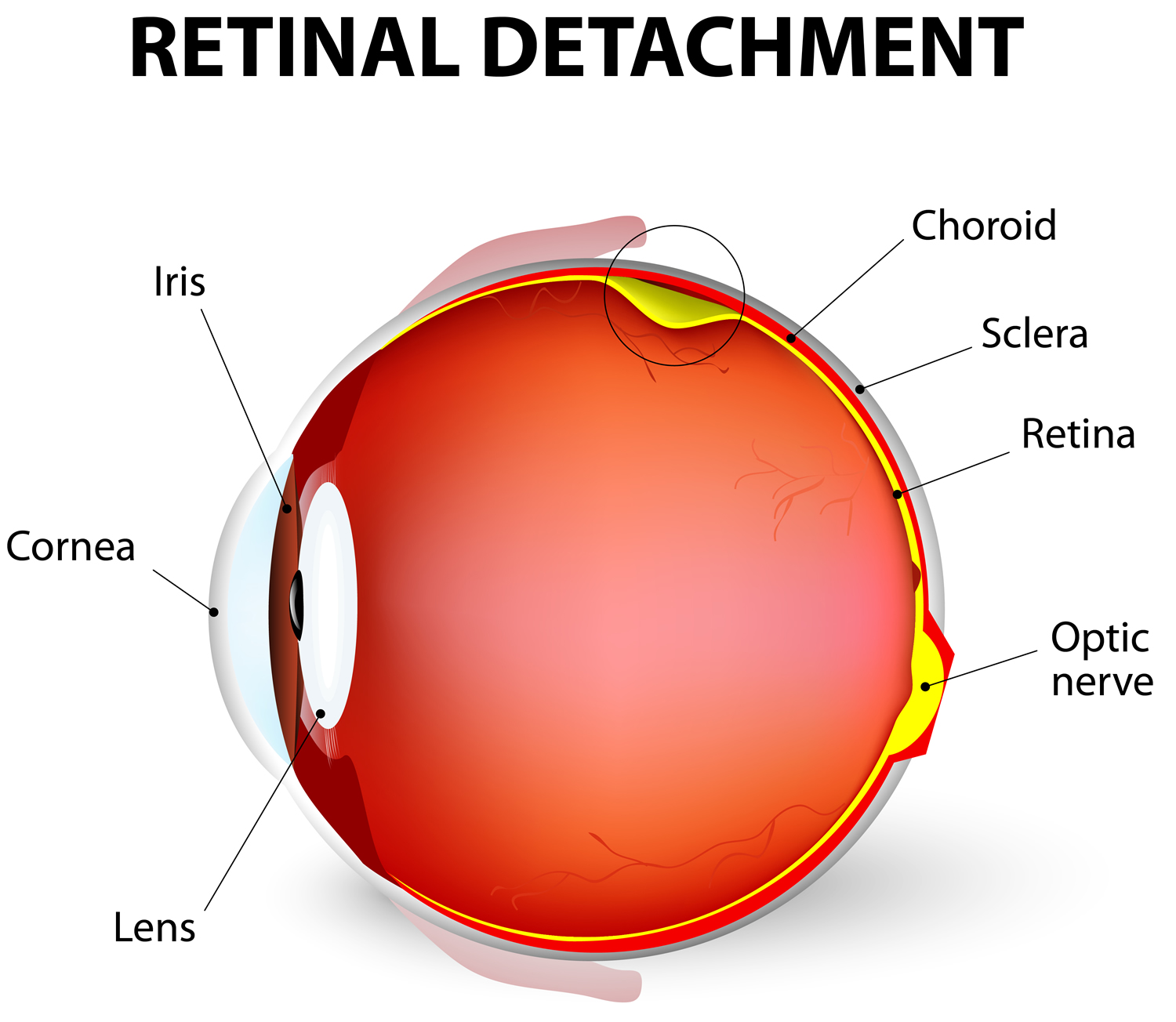
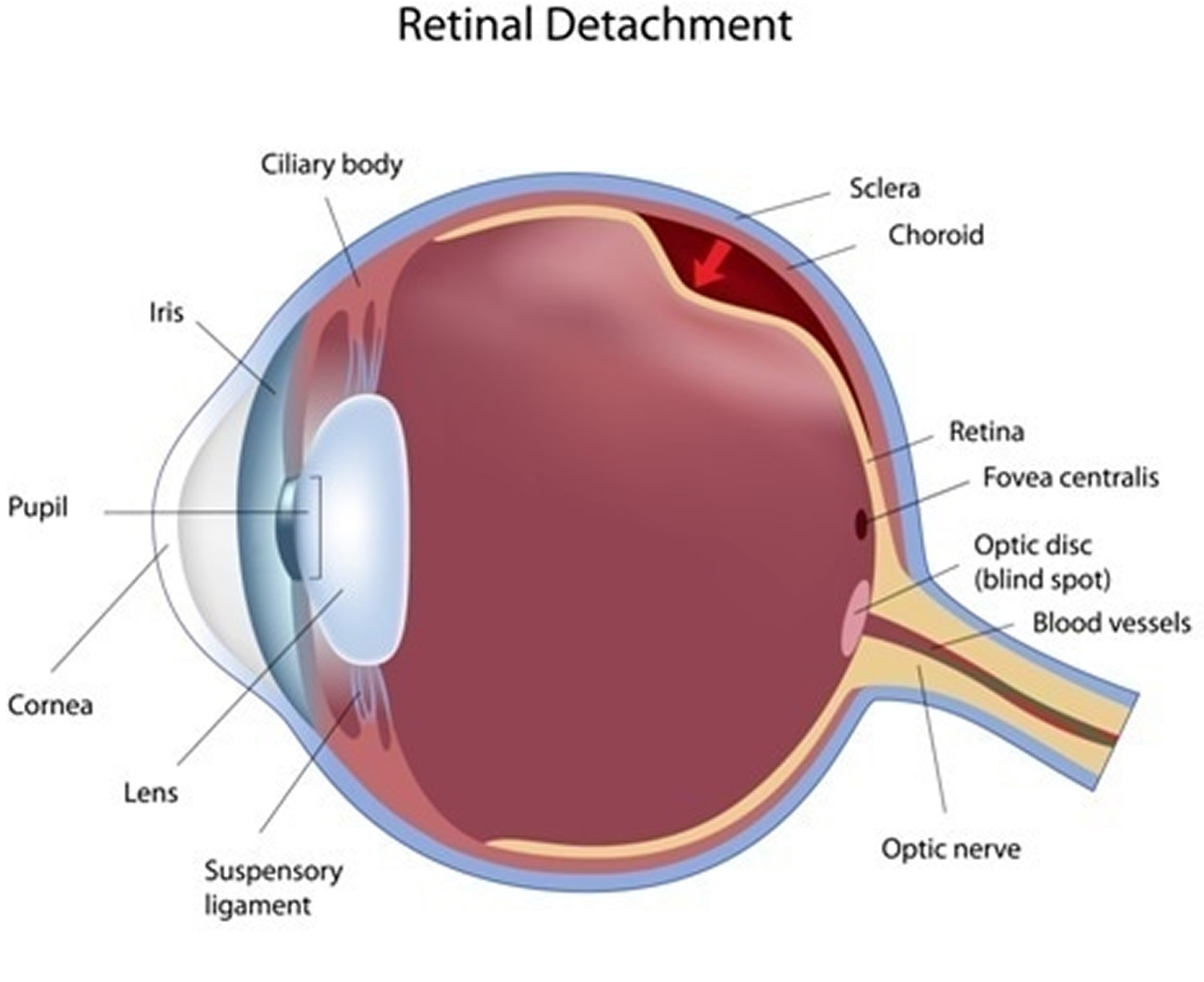
Figure 4. Retinal detachment
 Retinal detachment types
Retinal detachment types
There are three different types of retinal detachment:
Rhegmatogenous retinal detachment
Rhegmatogenous retinal detachment refers to detachment of the retina, caused by a hole or tear in the retina. A tear or hole in the retina allows fluid to get under the retina and separate it from the retinal pigment epithelium (RPE), the pigmented cell layer that nourishes the retina. These types of retinal detachments are the most common.
Tractional retinal detachment
In Tractional retinal detachment, scar tissue on the retina’s surface contracts and causes the retina to separate from the retinal pigment epithelium (RPE). This type of detachment is less common.
Serous retinal detachment
Serous retinal detachment is also called exudative retinal detachment is frequently caused by retinal diseases, including inflammatory disorders and injury/trauma to the eye. In this type, fluid leaks into the area underneath the retina, but there are no tears or breaks in the retina.
Retinal detachment causes
Retinal detachment can occur when the gel-like material (vitreous) leaks through a retinal hole or tear and collects underneath the retina.
Aging or retinal disorders can cause the retina to thin. Retinal detachment due to a tear in the retina typically develops when the vitreous collapses and tugs on the retina with enough force to create a tear.
Fluid inside the vitreous then finds its way through the tear and collects under the retina, peeling it away from the underlying tissues. These tissues contain a layer of blood vessels called the choroid. The areas where the retina is detached lose this blood supply and stop working, so you lose vision.
Aging-related retinal tears that lead to retinal detachment
As you age, your vitreous may change in consistency and shrink or become more liquid. Eventually, the vitreous may separate from the surface of the retina — a common condition called posterior vitreous detachment.
As the vitreous separates or peels off the retina, it may tug on the retina with enough force to create a retinal tear. Left untreated, fluid from the vitreous cavity can pass through the tear into the space behind the retina, causing the retina to become detached.
Posterior vitreous detachment can cause visual symptoms. You may see sudden new floaters or flashes of lights (photopsia). These may be visible even in daylight. The flashes may be more noticeable when your eyes are closed or you’re in a darkened room.
Risk factors for retinal detachment
The following factors increase your risk of retinal detachment:
- Aging — retinal detachment is more common in people over age 50
- Previous retinal detachment in one eye
- A family history of retinal detachment
- Extreme nearsightedness (myopia)
- Previous eye surgery, such as cataract removal
- Previous severe eye injury
- Previous other eye disease or inflammation.
How to prevent retinal detachment
It’s not clear exactly why posterior vitreous detachment can lead to retinal detachment in some people and there’s nothing you can do to prevent it. But it’s more likely to happen if you:
- Are near-sighted (myopia)
- Have had an eye operation (such as cataract surgery)
- Have had an eye injury
- Have a family history of retinal detachment
- Have a sagging vitreous — the gel-like material that fills the inside of your eye
- Have advanced diabetes
Signs of retinal detachment
Retinal detachment itself is painless. But warning signs almost always appear before it occurs or has advanced, such as:
- The sudden appearance of many floaters — tiny specks that seem to drift through your field of vision
- Flashes of light or “cobwebs” in one or both eyes
- Blurred vision
- Gradually reduced side (peripheral) vision
- A curtain-like shadow over your visual field.
Retinal detachment diagnosis
Your doctor may use the following tests, instruments and procedures to diagnose retinal detachment:
- Retinal examination. The doctor may use an instrument with a bright light and a special lens (ophthalmoscope) to examine the back of your eye, including the retina. The ophthalmoscope provides a highly detailed view, allowing the doctor to see any retinal holes, tears or detachments.
- Ultrasound imaging. Your doctor may use this test if bleeding has occurred in the eye, making it difficult to see your retina.
Your doctor will likely examine both eyes even if you have symptoms in just one. If a tear is not identified at this visit, your doctor may ask you to return within a few weeks to confirm that your eye has not developed a delayed tear as a result of the same vitreous separation. Also, if you experience new symptoms, it’s important to return to your doctor right away.
Retinal detachment treatment
Retinal holes and tears can be treated in an eye specialist’s office with a laser surgery (photocoagulation) or a freeze treatment called cryopexy. During laser surgery tiny burns are made around the hole to “weld” the retina back into place. Cryopexy freezes the area around the hole and helps reattach the retina. However, retinal detachment usually requires surgery in an operating theater.
Surgery to re-attach the retina or fix a retinal tear may involve:
- Attaching a small synthetic band around outside of your eyeball to push the wall of your eye and retina closer together (scleral buckling).
- Removing and replacing the jelly inside your eye (vitrectomy). During a vitrectomy, the doctor makes a tiny incision in the sclera (white of the eye). Next, a small instrument is placed into the eye to remove the vitreous, a gel-like substance that fills the center of the eye and helps the eye maintain a round shape. Gas is often injected to into the eye to replace the vitreous and reattach the retina; the gas pushes the retina back against the wall of the eye. During the healing process, the eye makes fluid that gradually replaces the gas and fills the eye.
- Injecting a bubble of gas into your eye to push the retina against the back of your eye (pneumatic retinopexy)
- Sealing the tear in your retina with laser or freezing treatment (cryotherapy)
With all of these procedures, either laser (photocoagulation) or cryopexy is used to “weld” the retina back in place. It’s usually done with local anesthetic, so you’re awake but your eye is numbed. You don’t normally need to stay in hospital overnight.
After your procedure, you’ll likely be advised to avoid activities that might jar the eyes — such as running — for a couple of weeks or so.
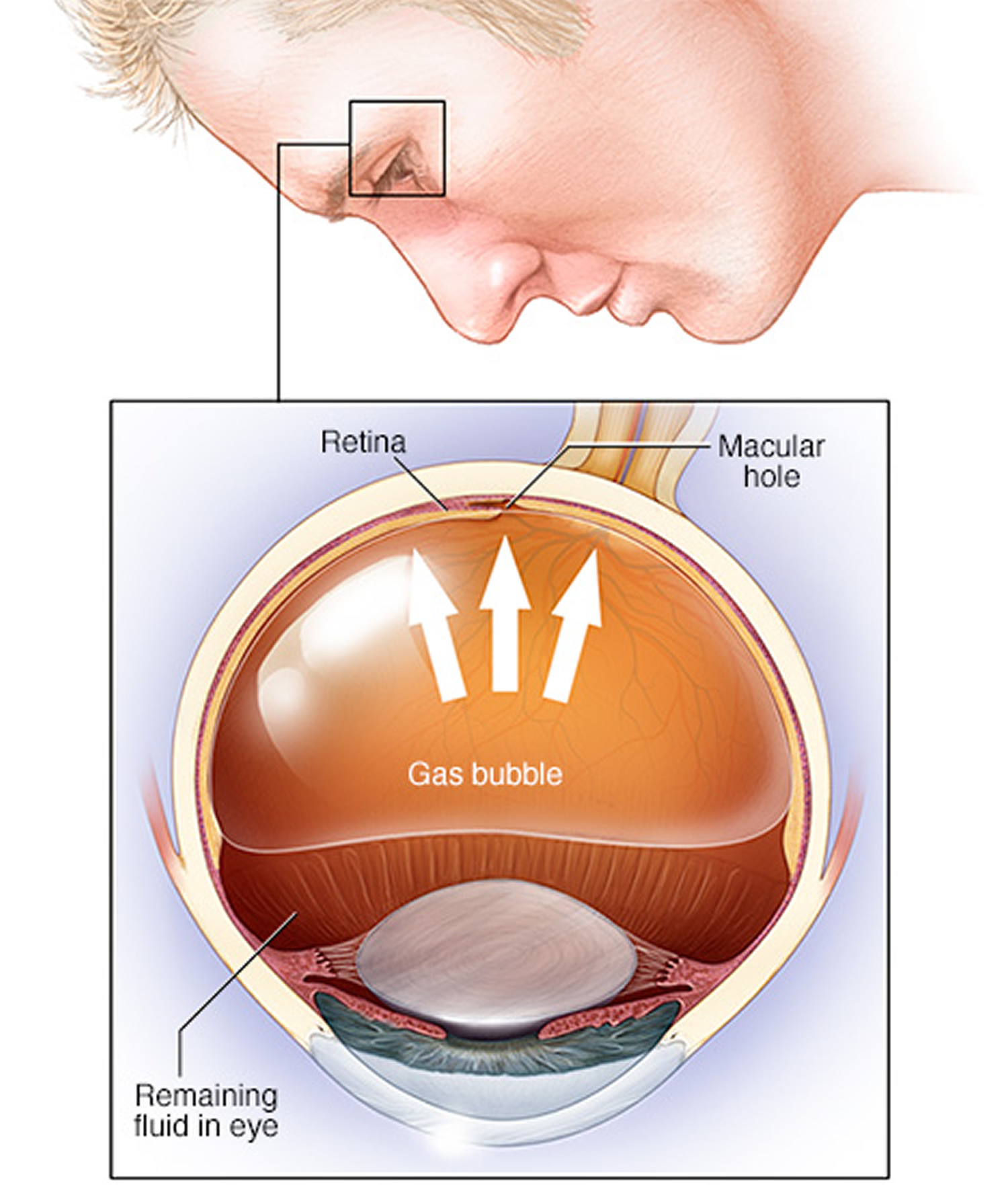
Figure 5. Pneumatic retinopexy – retinal detachment surgery
Retinal detachment surgery
If your retina has detached, you’ll need surgery to repair it, preferably within days of a diagnosis. The type of surgery your surgeon recommends will depend on several factors, including how severe the detachment is.
- Injecting air or gas into your eye. In this procedure, called pneumatic retinopexy, the surgeon injects a bubble of air or gas into the center part of the eye (the vitreous cavity). If positioned properly, the bubble pushes the area of the retina containing the hole or holes against the wall of the eye, stopping flow of fluid into the space behind the retina. Your doctor also uses cryopexy during the procedure to repair the retinal break. Fluid that had collected under the retina is absorbed by itself, and the retina can then adhere to the wall of your eye. You may need to hold your head in a certain position for up to several days to keep the bubble in the proper position. The bubble eventually will reabsorb on its own.
- Indenting the surface of your eye. This procedure, called scleral buckling, involves the surgeon sewing (suturing) a piece of silicone material to the white of your eye (sclera) over the affected area. This procedure indents the wall of the eye and relieves some of the force caused by the vitreous tugging on the retina. If you have several tears or holes or an extensive detachment, your surgeon may create a scleral buckle that encircles your entire eye like a belt. The buckle is placed in a way that doesn’t block your vision, and it usually remains in place permanently.
- Draining and replacing the fluid in the eye. In this procedure, called vitrectomy, the surgeon removes the vitreous along with any tissue that is tugging on the retina. Air, gas or silicone oil is then injected into the vitreous space to help flatten the retina. Eventually the air, gas or liquid will be absorbed, and the vitreous space will refill with body fluid. If silicone oil was used, it may be surgically removed months later. Vitrectomy may be combined with a scleral buckling procedure.
These procedures are often done on an outpatient basis.
After surgery your vision may take several months to improve. You may need a second surgery for successful treatment. Some people never recover all of their lost vision.
Recovery time after surgery varies. But as a general guide, for 2 to 6 weeks after surgery:
- your vision may be blurry
- your eye may be sore and red – take paracetamol if you need to
- you may need to take time off work
- you may not be able to drive
- you may need to avoid flying (if you have had a bubble of gas put into your eye)
Over 90 percent of those with a retinal detachment can be successfully treated and most people are eventually able to return to all their normal activities. Although sometimes a second treatment is needed. However, the visual outcome is not always predictable. The final visual result may not be known for up to several months following surgery. Even under the best of circumstances, and even after multiple attempts at repair, treatment sometimes fails and vision may eventually be lost. Visual results are best if the retinal detachment is repaired before the macula (the center region of the retina responsible for fine, detailed vision) detaches. That is why it is important to contact an eye care professional immediately if you see a sudden or gradual increase in the number of floaters and/or light flashes, or a dark curtain over the field of vision.
Retinal detachment surgery complications
Proliferative retinopathy is the most common cause of repair failure and occurs in about 8–10% of patients undergoing primary retinal detachment repair 1. Risk factors for proliferative retinopathy include:
- Age
- Giant retinal tears
- Retinal detachments involving more than 2 quadrants
- Previous retinal detachment repair
- Use of cryotherapy
- Vitreous hemorrhage
- Choroidal detachment.
Proliferative retinopathy requires surgical intervention to release the traction caused by membranes and has a poor visual prognosis 2.
Coping and support
Retinal detachment may cause you to lose vision. Depending on your degree of vision loss, your lifestyle might change significantly.
You may find the following ideas useful as you learn to live with impaired vision:
- Check into transportation. Investigate vans and shuttles, volunteer driving networks, or ride shares available in your area for people with impaired vision.
- Get glasses. Optimize the vision you have with glasses that are specifically tailored for your eyes.
- Get help from technology. Digital talking books and computer screen readers can help with reading, and other new technology continues to advance.
- Brighten your home. Have proper light in your home for reading and other activities.
- Make your home safer. Eliminate throw rugs and place colored tape on the edges of steps. Consider installing motion-activated lights.
- Enlist the help of others. Tell friends and family members about your vision problems so they can help you.
- Talk to others with impaired vision. Take advantage of online networks, support groups and resources for people with impaired vision.





{kind=link}