
Contents
What are rheumatoid nodules
Rheumatoid nodules are firm, noticeable lumps that form underneath the skin of some rheumatoid arthritis patients. Rheumatoid nodules generally form on or near the base of the arthritic joints. Rheumatoid nodules may be present in 20 to 40% of patients with rheumatoid arthritis; these occur over extensor surfaces at elbows, heals, and toes and their severity can vary from patient to patient 1.
The exact cause of rheumatoid nodules is unknown. Rheumatoid nodules are composed of inflammatory cells, fibrin, and necrotic proteinaceous debris 2. Most patients with rheumatoid nodules are seropositive for rheumatoid factor and anticyclic citrullinated peptide antibodies (anti-CCP antibodies) 3. Patients with rheumatoid nodules typically have a more severe course and more rapid progression of rheumatoid arthritis than patients without rheumatoid nodules 4. Rheumatoid nodules range from 2 mm to 5 cm and are firm, usually non-tender, and mobile, although they may become fixed to the underlying periosteum 5. Occasionally, rheumatoid nodules may be painful or large enough to limit range of motion or compress nearby nerves, necessitating treatment.
Although rheumatoid nodules are generally not dangerous or debilitating, there are treatment options available if it becomes necessary to have them reduced or removed.
Typically, rheumatoid nodules appear in the following locations:
- Fingers and knuckles
- Elbows
- Forearms
- Knees
- Backs of heels
Less commonly, nodules may form in the eyes, lungs and vocal cords but these represent severe cases. Pulmonary rheumatoid nodules occur in less than 1% of patients with rheumatoid arthritis 6. Lung rheumatoid nodules can rupture into the pleural cavity and cause pneumothorax, empyema, and bronchopleural fistula 7.
Furthermore, rheumatoid nodules can vary in size and shape. Most nodules have a circular shape, however, some can be linear in shape as well. Also, they can range from small and pea-sized to as large as a walnut. When rheumatoid nodules form a cluster of tiny nodules, they are referred to as micro-nodules. This severe, less common case of micro-nodules generally occurs around the arthritic finger joints.
Though nodules are firm or even doughy to the touch and don’t cause any feelings of tenderness, they can occasionally be painful. Pain typically occurs when flare-ups are active and the joints become inflamed such that it impacts the nodules and the area around them.
Rheumatoid nodules are capable of moving around but some form a connection with the tendons or tissue beneath the skin and become fixed.
For the most part, rheumatoid nodules do not cause severe pain for most patients and are not usually a health concern. However, on rare occasions, the skin over top of the nodule can become infected or ulcerated and this only occurs if an excessive amount of pressure is placed on the nodule. If nodules develop in sensitive areas, then increased pressure resulting in infection would be more likely to occur.
Rheumatoid nodules have also been known to form in areas of the body other than the joints. One location where nodules develop, leading to severe symptoms, are the eyes. The autoimmune process in rheumatoid arthritis causes inflammation, eye dryness, and pain.
Though it is rare, rheumatoid nodules are capable of forming on the vocal cords and also in the lungs, heart and other internal organs. Because of this involvement of multiple organs, diagnosis can be challenging. Symptoms are not always obvious and sometimes mimic other illnesses.
Figure 1. Rheumatoid arthritis nodules fingers

Footnote: Dorsum of hands showing multiple rheumatoid nodules involving the proximal and distal interphalangeal joints and metacarpophalangeal joints. These nodules take on an appearance not dissimilar to gout. A 57-year-old man presented for review in the rheumatology outpatients clinic. He had a 30-year history of rheumatoid arthritis and was known to be positive for rheumatoid factor and anticitrullinated protein antibodies (anti-CCP antibodies). He had been treated over the past 30 years with various immunosuppression regimens, including long-term methotrexate, leflunomide and sulfasalazine. His disease had been stable for the past 2 years with no recent increase in nodules or episodes of acute synovitis. Several times in the past 15 years his diagnosis of rheumatoid arthritis had come into question due to the atypical appearance of his hands which closely resembled gout. On two occasions, excision of rheumatoid nodules was sent for histology to exclude other diagnoses such as gout and multicentric reticulohistiocytosis. In both specimens, there was no evidence of birefringent urate crystals when exposed to polarised light. While reticulohistiocytosis also shows a proliferation of histiocytes, they are typically nodular and scattered. The characteristic pattern of pallisading histiocytes was consistent with rheumatoid nodules.
[Source 8 ]Figure 2. Rheumatoid nodules elbow

Figure 3. Rheumatoid nodules lung
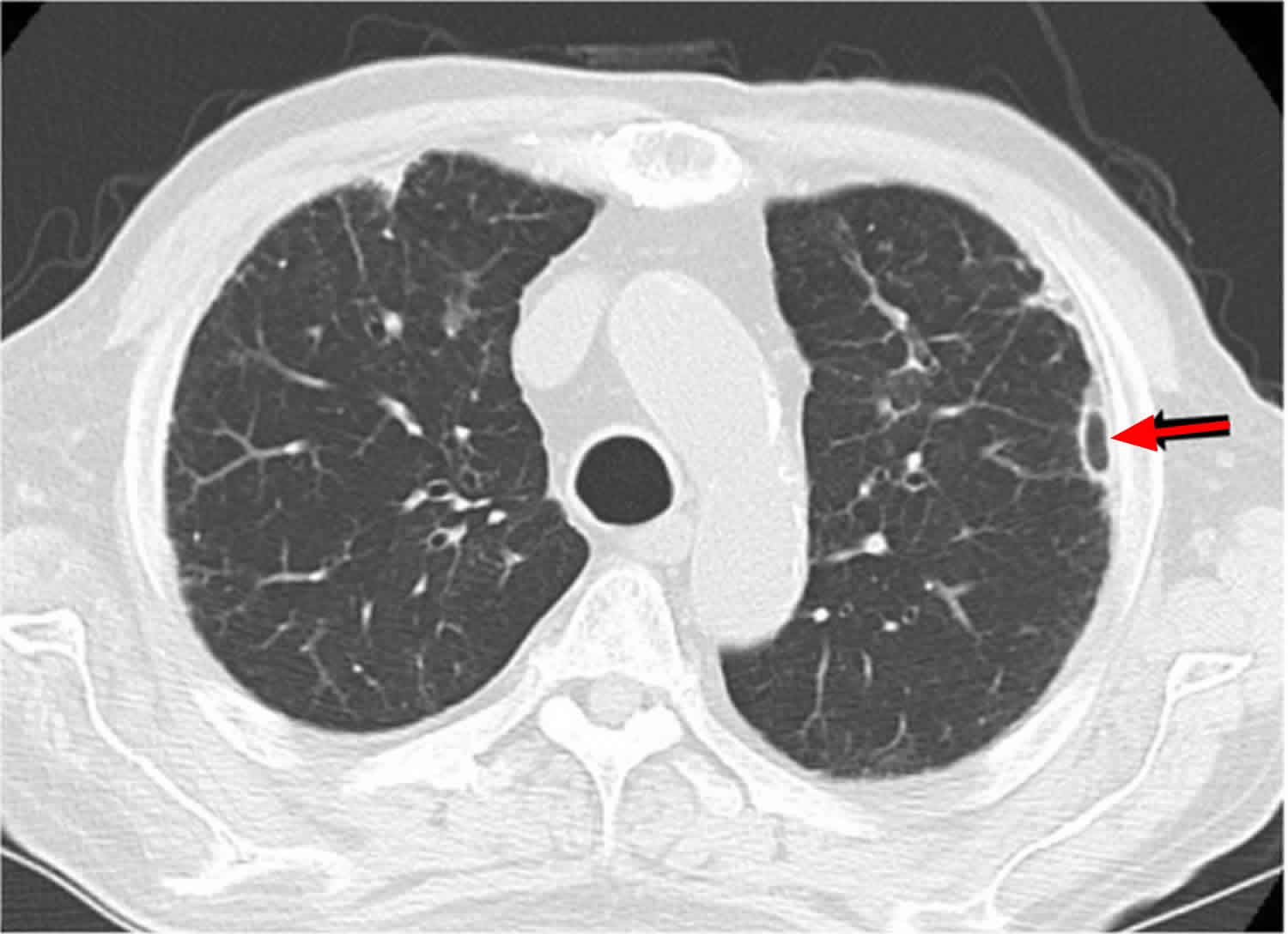
Footnote: Chest computed tomography before pneumothorax showing a subpleural rheumatoid nodule with cavitation (arrow). A 75-year-old man with a medical history of rheumatoid arthritis, acute coronary syndrome, and diabetes was admitted to our hospital because of left chest pain and dyspnea. A chest X-ray and chest computed tomography (CT) scan showed a left pneumothorax and several small subpleural nodules with cavitation. Repeated pleurodesis via a chest tube failed to improve the pneumothorax, so we decided to perform thoracoscopic surgery. Air leakage was detected in the left upper lobe where the subpleural nodule was visible on chest CT. Resection of the lesion successfully resulted in resolution of the air leakage. The final pathological diagnosis of the subpleural nodule was a pulmonary rheumatoid nodule. The patient has had no evidence of recurrence of pneumothorax after surgery.
[Source 7 ]Who develops rheumatoid nodules?
Most commonly, rheumatoid nodules develop in patients already living with rheumatoid arthritis for some time. They generally don’t precede other rheumatoid arthritis symptoms.
Research suggests that rheumatoid nodules are commonly found in patients who possess high levels of the protein rheumatoid factor, an antibody seen in a handful of autoimmune disorders. This may mean that the patients may require treatment with drugs in the class of immunomodulators, such as methotrexate.
Similarly, research has also shown an increased likelihood of developing nodules in rheumatoid arthritis patients who smoke, even though a direct link between smoking and the formation of rheumatoid nodules is still unclear.
What causes rheumatoid nodules?
Currently, research doesn’t clearly indicate a specific cause of rheumatoid nodules and why exactly they develop in some patients and not in others. Given that they generally form on extensor joints, rheumatoid nodules could be the result of repeated pressure on the affected joints over time. Some patients even report a decrease in size or disappearance over time.
Patients who are bedridden, sometimes form rheumatoid nodules on the backs of their elbows, legs, hips and sacrum. There are even reported cases of these nodules on the posterior scalp. These are all the pressure points of bedridden patients and possibly the catalyst to the formation of rheumatoid nodules.
Accelerated nodulosis is a specific condition that occurs with rheumatoid nodules where patients experience the formation of multiple nodules in a centralized location typically on the fingers and backs of the hands.
This is compared to the sporadic appearance of a few rheumatoid nodules that form in patients here and there. In many cases, physicians have found that accelerated rheumatoid nodulosis occurs in patients who are pursuing methotrexate therapy 9.
Rheumatoid nodules treatment
Specific treatment for rheumatoid nodules isn’t generally advised. This is because most nodules are only unsightly as opposed to debilitating, and therefore are not aggressively treated. However, if nodules cause the skin to become infected or ulcerated, then treatment will be necessary.
Rheumatoid nodules that form on the heels or beneath the feet can be debilitating to the patient limiting their mobility. In these cases, treatment would not just be advised but likely necessary.
Treatments include certain disease-modifying antirheumatic drugs (DMARDs) have been known to reduce the appearance of rheumatoid nodules. Other treatments like glucocorticoid injections can also help to decrease the size of rheumatoid nodules 10 and occasionally surgical excision for recalcitrant cases 11.
Some patients report that even after treatment or having their rheumatoid nodules removed, they do grow back. Unfortunately, the nature of rheumatoid arthritis and its symptoms mean that the nodules can recur after treatment.
With this in mind, it is important to have a discussion with your physician about your symptoms, and the available treatment options that can help reduce the size of rheumatoid nodules or even remove them.
- Chansakul T, Dellaripa PF, Doyle TJ, Madan R. Intra-thoracic rheumatoid arthritis: Imaging spectrum of typical findings and treatment related complications. Eur J Radiol. 2015;84(10):1981–1991. doi:10.1016/j.ejrad.2015.07.008 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4629482[↩]
- Athanasou NA, Quinn J, Woods CG, Mcgee JO. Immunohistology of rheumatoid nodules and rheumatoid synovium. Ann Rheum Dis. 1988;47(5):398–403.[↩]
- Kim SK, Park SH, Shin IH, Choe JY. Anti-cyclic citrullinated peptide antibody, smoking, alcohol consumption, and disease duration as risk factors for extraarticular manifestations in Korean patients with rheumatoid arthritis. J Rheumatol. 2008;35(6):995–1001[↩]
- Nyhäll-Wåhlin BM, Turesson C, Jacobsson LT, et al. The presence of rheumatoid nodules at early rheumatoid arthritis diagnosis is a sign of extra-articular disease and predicts radiographic progression of joint destruction over 5 years. Scand J Rheumatol. 2011;40(2):81–87[↩]
- García-Patos V. Rheumatoid nodule. Semin Cutan Med Surg. 2007;26(2):100–107[↩]
- Pulmonary necrobiotic nodules as a presenting feature of rheumatoid arthritis. Hull S, Mathews JA. Ann Rheum Dis. 1982 Feb; 41(1):21-4.[↩]
- Shimomura M, Ishihara S, Iwasaki M. Intractable pneumothorax due to rupture of subpleural rheumatoid nodules: a case report. Surg Case Rep. 2018;4(1):89. Published 2018 Aug 8. doi:10.1186/s40792-018-0502-8 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6082747[↩][↩]
- Chakradeo K, Buzacott K, Soden M. Nodular rheumatoid arthritis resembling gout. Case Reports 2016;2016:bcr2016216967 https://casereports.bmj.com/content/2016/bcr-2016-216967[↩]
- Rheumatoid arthritis: a review of the cutaneous manifestations. Sayah A, English JC 3rd. J Am Acad Dermatol. 2005 Aug; 53(2):191-209; quiz 210-2.[↩]
- Baan H, Haagsma CJ, van de Laar MA. Corticosteroid injections reduce size of rheumatoid nodules. Clin Rheumatol. 2006;25(1):21–23[↩]
- McGrath MH, Fleischer A. The subcutaneous rheumatoid nodule. Hand Clin. 1989;5(2):127–135.[↩]





{kind=link}