Contents
What is safflower oil
Safflower (Carthamus tinctorius) is a highly branched, herbaceous, thistle-like annual plant. Safflower is commercially cultivated for vegetable oil extracted from the seeds – safflower oil. Safflower plants are 30 to 150 cm (12 to 59 in) tall with globular flower heads having yellow, orange, or red flowers (see Figure 1). Each branch will usually have from one to five flower heads containing 15 to 20 seeds per head. Safflower is native to arid environments having seasonal rain. It grows a deep taproot which enables it to thrive in such environments.
Traditionally, the safflower crop was grown for its seeds and used for coloring and flavoring foods, in medicines and making red (carthamin) and yellow dyes, especially before cheaper aniline dyes became available. For the last fifty years or so, the plant has been cultivated mainly for the vegetable oil extracted from its seeds.
Safflower seed oil is flavorless and colorless and nutritionally similar to sunflower oil. Safflower oil is used mainly in cosmetics and as a cooking oil, in salad dressing, and for the production of margarine.
There are two types of safflower that produce different kinds of oil: one high in monounsaturated fatty acid (oleic acid) and the other high in polyunsaturated fatty acid (linoleic acid). Currently the predominant edible oil market is for the polyunsaturated fatty acid (linoleic acid), which is lower in saturated fats than olive oil. The latter is used in painting in the place of linseed oil, particularly with white paints, as it does not have the yellow tint which linseed oil possesses.
Oils rich in polyunsaturated fatty acids, notably linoleic acid, are considered to have some health benefits. One human study compared high-linoleic safflower oil with conjugated linoleic acid (CLA), showing that body fat decreased and adiponectin levels increased in obese postmenopausal women with type 2 diabetes mellitus consuming safflower oil 1. The dietary oil, conjugated linoleic acid (CLA), has reduced body weight and body fat in some clinical studies 2, 3 and animal models 4 for diet-induced obesity. Therefore, CLA (conjugated linoleic acid) has been promoted as a weight-loss supplement.
Conjugated linoleic acid (CLA) is a group of polyunsaturated fatty acids found in beef, lamb and dairy products that exist as positional and stereo-isomers of octadecadienoate (18:2) 5.
Figure 1. Safflower

Safflower Oil
Safflower oil is available in U.S. grocery stores and is rich in the essential n-6 polyunsaturated fatty acid (PUFA) linoleic acid (LA). Omega-6 polyunsaturated fatty acid (PUFA) are characterized by the presence of at least 2 carbon-carbon double bonds, with the first bond at the sixth carbon from the methyl terminus. Linoleic acid (LA), an 18-carbon fatty acid with 2 double bonds (18:2 omega-6 polyunsaturated fatty acid), is the primary dietary omega-6 PUFA. Linoleic acid cannot be synthesized by humans, and although firm minimum requirements have not been established for healthy adults, estimates derived from studies in infants and hospitalized patients receiving total parenteral nutrition suggest that an linoleic acid intake of ≈0.5% to 2% of energy is likely to suffice. Dietary recommendations for omega-6 PUFAs traditionally focused on the prevention of essential fatty acid deficiency but are now increasingly seeking to define “optimal” intakes to reduce risk for chronic disease, particularly coronary heart disease. The Institute of Medicine’s Food and Nutrition Board, in their Dietary Reference Intake Report for Energy and Macronutrients 6, defines an adequate intake of Linoleic acid (LA) as 17 g/d for men and 12 g/d for women (5% to 6% of energy) 19 to 50 years of age, approximately the current median US intake. The average daily intake of linoleic acid for women ages 51–70 in the U.S. is 12.6 g, which equates to 5.7% of energy in a 2,000 kilocalorie diet 7.
Other governmental health recommendations for omega-6 fatty acid intakes (on a percent energy basis) are as follows: European Commission, 4% to 8% 8; Food and Agriculture Organization/World Health Organization, 5% to 8% 9; British Nutrition Foundation, 6% to 6.5% (maximum, 10%) 10; the Department of Health and Ageing, Australia and New Zealand, 4% to 5% (maximum, 10%) 11; and the American Dietetic Association/Dietitians of Canada, 3% to 10% 12. The American Heart Association places primary emphasis on healthy eating patterns rather than on specific nutrient targets.
After consumption, linoleic acid can be desaturated and elongated to form other omega-6 PUFAs such as γ-linolenic and dihomo-γ-linolenic acids. The latter is converted to the metabolically important omega-6 PUFA arachidonic acid (AA; 20:4 omega-6), the substrate for a wide array of reactive oxygenated metabolites. Because linoleic acid accounts for 85% to 90% of the dietary omega-6 PUFA, dietary arachidonic acid [a polyunsaturated omega-6 fatty acid 20:4(ω-6)], which can affect tissue arachidonic acid [a polyunsaturated omega-6 fatty acid 20:4(ω-6)] levels 13, may have physiological sequelae. Linoleic acid (LA) comes primarily from vegetable oils (eg, corn, sunflower, safflower, soy). The average US intake of LA, according to National Health and Nutrition Examination Survey 2001 to 2002 data for adults ≥19 years of age, is 14.8 g/d.9 On the basis of an average intake of 2000 kcal/d, LA intake is 6.7% of energy. AA (≈0.15 g/d) is consumed preformed in meat, eggs, and some fish. Numerous health organizations have recommendations for dietary linoleic acid (LA) intake, generally falling within the range of 3–10% of total energy consumption 14.
Table 1. Safflower oil nutrition facts
| Nutrient | Unit | Value per 100 g | tablespoon 13.6 g | ||||||||
| Approximates | |||||||||||
| Water | g | 0 | 0 | ||||||||
| Energy | kcal | 884 | 120 | ||||||||
| Protein | g | 0 | 0 | ||||||||
| Total lipid (fat) | g | 100 | 13.6 | ||||||||
| Carbohydrate, by difference | g | 0 | 0 | ||||||||
| Fiber, total dietary | g | 0 | 0 | ||||||||
| Sugars, total | g | 0 | 0 | ||||||||
| Minerals | |||||||||||
| Calcium, Ca | mg | 0 | 0 | ||||||||
| Iron, Fe | mg | 0 | 0 | ||||||||
| Magnesium, Mg | mg | 0 | 0 | ||||||||
| Phosphorus, P | mg | 0 | 0 | ||||||||
| Potassium, K | mg | 0 | 0 | ||||||||
| Sodium, Na | mg | 0 | 0 | ||||||||
| Zinc, Zn | mg | 0 | 0 | ||||||||
| Vitamins | |||||||||||
| Vitamin C, total ascorbic acid | mg | 0 | 0 | ||||||||
| Thiamin | mg | 0 | 0 | ||||||||
| Riboflavin | mg | 0 | 0 | ||||||||
| Niacin | mg | 0 | 0 | ||||||||
| Vitamin B-6 | mg | 0 | 0 | ||||||||
| Folate, DFE | µg | 0 | 0 | ||||||||
| Vitamin B-12 | µg | 0 | 0 | ||||||||
| Vitamin A, RAE | µg | 0 | 0 | ||||||||
| Vitamin A, IU | IU | 0 | 0 | ||||||||
| Vitamin E (alpha-tocopherol) | mg | 34.1 | 4.64 | ||||||||
| Vitamin D (D2 + D3) | µg | 0 | 0 | ||||||||
| Vitamin D | IU | 0 | 0 | ||||||||
| Vitamin K (phylloquinone) | µg | 7.1 | 1 | ||||||||
| Lipids | |||||||||||
| Fatty acids, total saturated | g | 7.541 | 1.026 | ||||||||
| Fatty acids, total monounsaturated | g | 75.221 | 10.23 | ||||||||
| Fatty acids, total polyunsaturated | g | 12.82 | 1.744 | ||||||||
| Fatty acids, total trans | g | 0.096 | 0.013 | ||||||||
| Cholesterol | mg | 0 | 0 | ||||||||
| Other | |||||||||||
| Caffeine | mg | 0 | 0 | ||||||||
Safflower Oil Omega-6 PUFAs and Inflammation
Arguments for reduced Linoleic acid (Omega-6 PUFA) intakes are based on the assumption that because coronary artery disease has an inflammatory component 16 and because the omega-6 fatty acid, arachidonic acid (AA), is the substrate for the synthesis of a variety of proinflammatory molecules, reducing linoleic acid (Omega-6 PUFA) intakes should reduce tissue arachidonic acid (AA) content, which should reduce the inflammatory potential and therefore lower the risk for coronary heart disease. The evidence, derived primarily from human studies, regarding this line of reasoning is examined below.
Arachidonic acid (AA) is the substrate for the production of a wide variety of eicosanoids (20-carbon AA metabolites). Some are proinflammatory, vasoconstrictive, and/or proaggregatory, such as prostaglandin E2, thromboxane A2, and leukotriene B4. However, others are antiinflammatory/antiaggregatory, such as prostacyclin, lipoxin A4 17 and epoxyeicosatrienoic acids 18. Epoxyeicosatrienoic acids are fatty acid epoxides produced from AA by a cytochrome P450 epoxygenase. Epoxyeicosatrienoic acids also have important vasodilator properties via hyperpolarization and relaxation of vascular smooth muscle cells 19. Importantly, because the production of AA from LA is tightly regulated 20, wide variations in dietary LA (above minimal essential intakes) do not materially alter tissue AA content 21. In tracer studies, the extent of conversion of LA to AA is ≈0.2% 22.
In studies with vascular endothelial cells, omega-6 PUFA had antiinflammatory properties, suppressing the production of adhesion molecules, chemokines, and interleukins, all key mediators of the atherosclerotic process 23. In human studies, higher plasma levels of omega-6 PUFAs, mainly AA, were associated with decreased plasma levels of serum proinflammatory markers, particularly interleukin-6 and interleukin-1 receptor antagonist, and increased levels of antiinflammatory markers, particularly transforming growth factor-β 24. When healthy volunteers were given ≈7 times the usual intake of AA (ie, 1.5 g/d) in a 7-week controlled feeding study, no effects on platelet aggregation, bleeding times, the balance of vasoactive metabolites, serum lipid levels, or immune response were observed 13. Likewise, in a recent study from Japan, AA supplementation (840 mg/d for 4 weeks) had no effect on any metabolic parameter or platelet function.19 Consistent with this, in observational studies, higher omega-6 PUFA consumption was associated with unaltered or lower levels of inflammatory markers 25.
Diets high in LA can increase the ex vivo susceptibility of low-density lipoprotein (LDL “bad” cholesterol) to oxidation 26 and oxidized LDL can promote vascular inflammation 27. Therefore, oxidized LDL may play some role in the etiology of coronary heart disease 28. However, the extent of LDL oxidation at higher LA intakes (5% to 15% of energy) has not been established, and its clinical relevance is in question owing to the general failure of antioxidant treatments to mitigate coronary artery disease risk in most randomized trials 29. At present, little direct evidence supports a net proinflammatory, proatherogenic effect of LA in humans 30, 31.
Omega-6 PUFA Consumption and Other Coronary Heart Disease Risk Factors/Markers
The cholesterol-lowering effect of Linoleic acid (Omega-6 PUFA) is well established from human trials. In a meta-analysis of 60 feeding studies including 1672 volunteers, the substitution of PUFA (largely omega-6, varying from 0.6% to 28.8% energy) for carbohydrates had more favorable effects on the ratio of total to high-density lipoprotein cholesterol (perhaps the best lipid predictor of coronary heart disease risk) than any class of fatty acids 32. Higher plasma PUFA levels are associated with a reduced ratio of total to high-density lipoprotein cholesterol 33, and epidemiologically, the replacement of 10% of calories from saturated fatty acid with omega-6 PUFA is associated with an 18-mg/dL decrease in LDL “bad” cholesterol, greater than that observed with similar replacement with carbohydrate 34. These findings confirm an LDL-lowering effect of omega-6 PUFA beyond that produced by the removal of saturated fatty acids. Favorable effects of Linoleic acid (Omega-6 PUFA) on cholesterol levels are thus well documented and would predict significant reductions in coronary artery disease risk. Additionally, higher Linoleic acid (Omega-6 PUFA) intakes may improve insulin resistance 35 and reduce the incidence of diabetes mellitus 36 and higher serum LA levels are associated with lower blood pressure 37. Nevertheless, not all studies support a beneficial effect of LA on coronary artery disease risk markers. For example, an angiographic study reported a direct association between PUFA intakes and luminal narrowing in women with coronary heart disease 38. However, effects on markers do not always translate into effects on actual clinical end points; thus, it is essential to evaluate the relations between LA consumption and cornary artery disease events.
These observational studies use the strongest designs, minimizing both selection and recall bias. No significant associations between LA or omega-6 PUFA intake and coronary artery disease risk were seen in the Finnish Alpha-Tocopherol, Beta-Carotene Cancer Prevention Study 39, Lipid Research Clinics study 40, or Honolulu Heart Program 41. Modest, nonsignificant inverse associations were observed in the Multiple Risk Factor Intervention Trial 42, the Irish-Boston Heart Study 43 and the Health Professionals Follow-Up Study 44. In the Health Professionals Follow-Up Study, coronary artery disease rates were lowest in participants with higher intake of both omega-3 and omega-6 PUFAs 45 and in the Western Electric Study47 and the Kupio Heart Study 46, higher LA intakes or serum levels were associated with lower risk of coronary heart disease or total mortality. In the Nurses’ Health Study, in which diet was assessed multiple times over 20 years 47, coronary heart disease risk was ≈25% lower comparing the 95th and 5th percentiles of LA intake (7.0% versus 2.8% of energy, respectively). Most prospective cohort studies have not found significant associations between omega-6 fatty acid intakes and ischemic 48 or hemorrhagic 48 stroke or stroke mortality 49. In 1 prospective study, serum LA levels predicted lower risk of stroke, particularly ischemic stroke 50. LA intakes are not associated with risk for cancer 31. Therefore, observational studies generally suggest an overall modest benefit of omega-6 PUFA intake on coronary artery disease risk and no significant effect on stroke or cancer. These studies, some of which included LA intakes of up to 10% to 12% of energy, contradict the supposition that higher omega-6 PUFA intakes increase risk for coronary artery disease.
Several randomized trials have evaluated the effects of replacing saturated fatty acids with PUFAs on coronary artery disease events 51. Intakes of PUFA (almost entirely omega-6 PUFA) ranged from 11% to 21%. In addition to the inability to double-blind these studies, many had design limitations such as small sample size (n=54), the provision of only ≈50% of meals, outcomes composed largely of “soft” ECG end points 52, randomization of sites rather than individuals with open enrollment and high turnover of subjects, use of vegetable oils that also contained the plant omega-3 fatty acid α-linolenic acid (ALA) 53 and simultaneous recommendations to increase fish and cod liver oil use 54. Nevertheless, a meta-analysis including 6 of these trials indicated that replacing saturated fatty acids with PUFAs lowered the risk for coronary artery disease events by 24% 55. Of the remaining 4 studies, 1 reported a significant 45% reduction in risk 52, whereas no significant effect was seen in the others 56.
CLA safflower oil
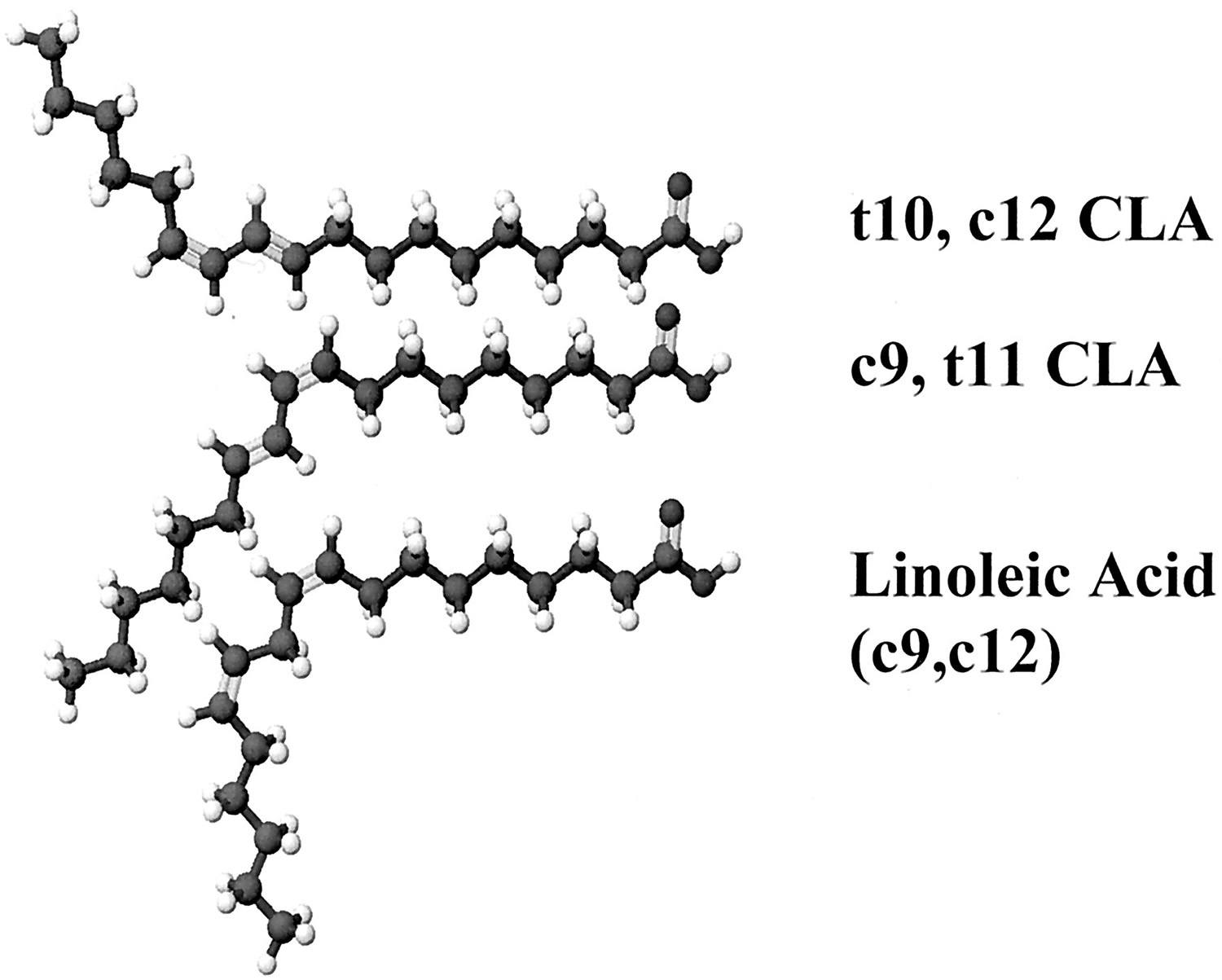
CLA (conjugated linoleic acid) is a natural, but minor, component of fats from ruminant animals that enters the human diet primarily in meat and dairy products 57. CLA has been shown to have many biological effects, including anticarcinogenisis, antiatherogenesis, immune modulation, and changes in body composition, and is commercially available as an over-the-counter supplement 58. CLA (conjugated linoleic acid) is not a single substance. CLA is a collective term for a class of conjugated dieonic isomers of linoleic acid. It is possible that a number of these CLA isomers have biological activity. However, all of the known physiologic effects of CLA are induced by 2 isomers: c9,t11-CLA and t10,c12-CLA (see Figure 2) 59.
In some cases an effect is produced by one of these isomers acting alone. For example, it is apparent that t10,c12-CLA is solely responsible for the reduction of body fat gain 60, whereas the c9,t11-isomer enhances growth and feed efficiency in young rodents 59. In other cases the isomers act together to induce an effect. For example, both c9,t11- and t10,c12-CLA appear to be equally effective in inhibiting chemically induced mammary carcinogenesis in rodent models 61, in part by inhibiting angiogenesis 62, whereas t10,c12-CLA appears to be more effective than c9,t11-CLA in inhibiting the proliferation of MCF-7 breast cancer cells by way of elicitation of a p53 response 63. In still other instances the 2 biologically active CLA isomers appear to act in apparent opposition 64. Hence, the multiple physiologic effects that are reported for CLA (Table 1 below) appear to be the result of multiple interactions of the biologically active CLA isomers with numerous metabolic signaling pathways 59.
Figure 2. CLA (conjugated linoleic acid) isomers
In nature, the most abundant isomer is cis-9,trans-11 (c9,t11), whereas in supplement forms CLA is typically sold as an equal mix of the 2 predominant isomers c9,t11 and t10,c12 66.
The discovery that CLA inhibited carcinogenesis in several animal models led to an investigation into the biochemical mechanisms of action of CLA. In the course of research of many scientists, a number of additional potential applications were identified, as indicated in Table 2.
The potential use of CLA to control body fat gain in humans and animals has received the most recent attention in both popular and scientific publications.
Table 2. Some of the reported physiologic effects of CLA (conjugated linoleic acid)
| Provides anticarcinogenic effect |
| Enhances immune function |
| Reduces inflammation |
| Reduces catabolic effects of immune stimulation |
| Reduces asthma in animal models |
| Reduces atherosclerosis |
| Enhances growth of young rodents |
| Reduces body fat gain |
| Enhances lean body mass gain |
| Reduces negative effects of weight-loss diets |
| Reduces symptoms of diabetes in some models |
| Reduces hypertension |
CLA and weight loss
Despite the multitude of human clinical trials testing the effect of CLA on body composition, the effect of CLA has been controversial because significant effects of CLA on body fat have not been consistently reported 66. An analysis of multiple studies indicates that there is a significant CLA dose effect in humans. In the one human study in which doses were directly compared, however, a dose of 3.4 g/d resulted in a weight loss of 0.14 kg/wk, whereas the 6.8 g/d dose resulted in a weight loss of 0.11 kg/wk 67. The failure to show a dose effect in this single study compared with the cumulative data from multiple studies reflects the inherent variability of fat loss in free-living humans. The highest dose provided in a human trial to date is 6.8 g/d (50:50 mixture of the t10, c12 and c9, t11 isomers) 67. There is insufficient human data to determine whether higher doses will produce more weight loss. Based on animal studies, it is possible that doses higher than 6.8 g CLA/day would produce additional fat loss. It is difficult to predict, however, because it is not obvious how to scale the doses between mice and humans. In animal studies that showed larger relative effects on fat mass than those we summarize here for human studies, doses have been provided in the range of 0.1% to 1% of the diet as CLA. Based on dose per body weight, these doses in a mouse provide 0.2 to 3 g/kg and are much larger than the 0.015 to 0.1 g/kg doses used in these human studies. On the basis of percentage energy intake, however, the 0.1% to 1% of diet doses in the mouse corresponds to doses between 0.2% and 2% of energy. An effective dose of CLA for loss of weight and adipose in humans may be between 0.5 and 5 g CLA mixed isomers per day 3.
Most CLA studies reviewed were ≤12 wk in length. Overall, fat loss was nearly linear for the first 6 mo of treatment and then began decelerate and to approach an asymptote, based largely on the single 2 year study 68. In contrast, most control groups would be predicted to gain a small amount of fat mass during a 2-y interval, so preventing gains in fat mass during long-term CLA treatment has a potential health advantage. Unfortunately, this single 2-year study was performed open label and did not include a placebo group for the second year 68. Therefore, it is not possible to reach definitive conclusions about potential body-composition benefits of CLA consumption for longer periods of time.
Very few data are available on individual CLA isomers and body composition. The results of the 3 single isomer studies, however, are not inconsistent with animal studies showing the t10, c12 isomer to be the efficacious isomer for body composition 69. For most human studies, the t10, c12 isomer was provided as an equal mix with the c9, t11 isomer. There are inadequate data to indicate an ideal mix of isomers for body composition, but the data available to date indicate that a mixture of t10, c12 and c9, t11 results in no severe adverse events, although the one human study that used the t10, c12 isomer alone did result in transient insulin resistance within 12 weeks 70.
CLA safflower oil safety and side effects
CLA safety has been evaluated in several well-conducted animal toxicologic studies.
Scimeca 71 conducted a 36-wk feeding trial in which Fischer 344 rats were fed either control diet or diet supplemented with 1.5% CLA, a level ≈30 times greater than humans would ingest at 3 g CLA/d. Food disappearance, body weights, cageside examinations, and hematologic and histopathologic analyses of 15 major organs were conducted. No adverse effects were observed.
O’Hagan and Menzel 72 conducted a subchronic 90-d oral rat toxicity study, accompanied by a battery of in vitro genotoxicity studies that are typical for assessment of food ingredient safety, on a commercial preparation of CLA that consisted of equal amounts of the c9,t11- and t10,c12-CLA isomers in the form of glycerides (rather than free fatty acids). They concluded that the no observed adverse effect levels for male and female rats were 2433 and 2728 mg/kg body weight per day, respectively.
In addition to these peer-reviewed published studies, there are 2 abstracts of note that relate to CLA safety assessment in animal models. Schulte et al 73 and Pfeiffer et al 74 conducted comprehensive toxicologic evaluations of CLA methyl esters in dogs and pigs, using standard toxicologic protocols approved by European Organisation for Economic Co-operation and Development Guidelines. They concluded that CLA methyl esters did not produce adverse effects in these species even when fed at 5% of the diet. These findings should, of course, be considered preliminary until the full-length manuscripts are available for review.
A number of human clinical trials that relate to safety and efficacy were also conducted. In designing human trials, CLA quality is a topmost issue. The most successful clinical studies were conducted with high-quality CLA preparations that consist almost entirely (ie, >90%) of the 2 biologically active isomers (Figure 2 above) in approximately equal amounts (ie, about 45% each), as reviewed by Gaullier et al 75. It should also be noted that such high-quality CLA, when consumed at 3–6 g/d, does not appear to induce adverse effects in humans 76, 77.
Despite these conclusions some researchers have recently raised concerns about the potential safety of CLA for humans 78. The concerns include the induction of fatty liver, insulin resistance, and lipodystrophy in mice fed CLA-supplemented diets and in some human trials enhanced C-reactive protein, lipid peroxidation, unfavorable changes in serum lipids, and reduced milk fat.
Fatty liver is induced in mice fed CLA-supplemented diets [Pariza et al 79]. However, this finding appears limited to mice in that it has not been reported for other species. Hamsters fed CLA and female rats fed diet supplemented with 15% CLA also exhibit enlarged livers, but this result is due to hypertrophy, not fat accumulation 72. It should be noted that neither fatty liver nor liver hypertrophy is considered by toxicologists to be a toxic effect 80. O’Hagan and Menzel 72 reported that the liver hypertrophy observed in female rats fed diet supplemented with 15% CLA was completely reversible when the animals were switched to a diet free of CLA.
CLA has also been reported to increase insulin resistance 70, 81. This has been most notable in studies of short duration 82, those that used single isomers 70, 81, or both. For example, in one study, insulin resistance was reported in individuals supplemented with only the t10, c12 isomer for 12 wk, but not with a mixed preparation of predominantly the c9, t11 and t10, c12 isomers 70. In a later study, the same enriched t10, c12 supplement was given for 18 wk and did not result in insulin resistance 83. Many studies either have not found significant changes in fasting glucose or insulin or in measures of insulin sensitivity 84, 85 or have found an improvement 86. With regard to both safety and efficacy, it has been suggested that CLA preparations enriched in c9, t11 and t10, c12 isomers are preferable to preparations containing 4 isomers 87, and this may also be true compared with single isomer preparations. Further investigation into the safety of CLA is warranted.
A related effect, lipodystrophy, was reported in mice fed a diet supplemented with CLA. Like fatty liver, lipodystrophy has not been reported to occur in other species, and it is possible that lipodystrophy is seen in mice because mice are so sensitive to CLA-induced body fat reduction. Increasing the amount of fat in CLA-supplemented diet substantially reduces the lipodystrophy effect 88.
With regard to these seemingly negative effects, it should be noted that dietary CLA significantly extended the life span of NZB/WF1 mice, which are prone to developing lupus erythematosus 89. This finding is consistent with the conclusion that CLA does not induce toxic effects and is important because mice appear to be the most sensitive and responsive known species to the effects of CLA on lipid metabolism 90.
Concern about elevations in oxidative stress and unfavorable changes in blood lipids has arisen from studies by Riserus et al 91 who investigated the effects of CLA in men with metabolic syndrome. They compared a typical high-quality CLA preparation consisting of equal amounts of c9,t11- and t10,c12-CLA with a supplement that is not commercially available, enriched for t10,c12-CLA but containing very little c9,t11-CLA. Riserus et al 91 observed evidence of enhanced lipid peroxidation (measured as urinary isoprostane), enhanced C-reactive protein in serum, and elevated VLDL coupled with reduced HDL. These negative effects were significant relative to placebo for the patients taking the t10,c12-CLA supplement but were reduced (in some cases below statistical significance) for patients taking the typical commercially available CLA supplement relative to placebo. Interestingly, the apparent t10,c12-CLA-induced oxidative stress did not result in reduced blood antioxidants but rather was correlated with increased blood vitamin E.
Riserus et al 91 concluded that these findings indicate that CLA could enhance inflammation and cardiovascular disease risk. However, other groups that have studied this issue have concluded that CLA reduces inflammation. For example, pigs fed a commercial mixture of CLA isomers displayed reduced inflammation 92, and dietary CLA not only reduced atherosclerosis in animal models 93 but also reduced preestablished atherosclerotic lesions in rabbits 93 and mice 94. Additionally, the researchers of a comprehensive clinical study of the effects on serum lipids of a high-quality CLA preparation consisting of c9,t11- and t10,c12-CLA in approximately equal amounts concluded, “The study confirms that some of the cardioprotective effects of CLA that were shown in animal studies are relevant to man” 95.
Riserus et al 91 also reported that the men in their study who were given the t10,c12-CLA supplement exhibited enhanced insulin resistance. Again, there was no significant difference in this condition between the placebo group and the group receiving the typical commercially available high-quality CLA isomer mixture, a finding that is also consistent with a previous report from Riserus’s group 96. Evidence of enhanced insulin resistance has not been observed in other CLA clinical trials either 95, 76.
It is well documented that t10,c12-CLA reduces milk fat. This effect has been most thoroughly studied in cows 97 but is also observed in lactating women who consume CLA supplements 98. The researchers of the latter study 99 concluded that the reduction of milk fat might lead to less energy availability for the nursing infant. However, in a study with rats 99 it was found that the pups nursing dams fed CLA-supplemented diet actually grew to a larger body size. Because very little t10,c12-CLA carries over to milk, whereas the c9,t11-CLA isomer is concentrated in milk, it could be concluded that c9,t11-CLA could be a growth factor for young rats, as it appears to be for young mice 79. Similar findings were obtained in a study with pigs in which the researchers concluded, “Irrespective of the dietary fat supplied in the starter period, piglets reared on the CLA sows had greater final body and warm carcass weights (P <0.01), and greater feed intake (P = 0.02) than piglets reared on the [control] sows” 100. It seems likely that in these studies 100 nursing animals compensated for reduced calories because of milk fat reduction by consuming more milk.
- Norris LE, Collene AL, Asp ML, et al. Comparison of dietary conjugated linoleic acid with safflower oil on body composition in obese postmenopausal women with type 2 diabetes mellitus. The American Journal of Clinical Nutrition. 2009;90(3):468-476. doi:10.3945/ajcn.2008.27371. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2728639/[↩]
- Dietary conjugated linoleic acid in health: physiological effects and mechanisms of action. Belury MA. Annu Rev Nutr. 2002; 22():505-31. https://www.ncbi.nlm.nih.gov/pubmed/12055356/[↩]
- Efficacy of conjugated linoleic acid for reducing fat mass: a meta-analysis in humans. Whigham LD, Watras AC, Schoeller DA. Am J Clin Nutr. 2007 May; 85(5):1203-11. http://ajcn.nutrition.org/content/85/5/1203.long[↩][↩]
- Changes in body composition in mice during feeding and withdrawal of conjugated linoleic acid. Park Y, Albright KJ, Storkson JM, Liu W, Cook ME, Pariza MW. Lipids. 1999 Mar; 34(3):243-8. https://www.ncbi.nlm.nih.gov/pubmed/10230717/[↩]
- DIETARY CONJUGATED LINOLEIC ACID IN HEALTH: Physiological Effects and Mechanisms of Action. Annual Review of Nutrition Vol. 22:505-531 (Volume publication date July 2002). https://doi.org/10.1146/annurev.nutr.22.021302.121842[↩]
- Food and Nutrition Board, Institute of Medicine. Dietary Reference Intakes for Energy, Carbohydrate, Fiber, Fat, Fatty Acids, Cholesterol, Protein and Amino Acids. Washington, DC: National Academies Press; 2002. Available at: http://books.nap.edu/catalog.php?record_id=10490[↩]
- Moshfegh A, Goldman J, Cleveland L. What we eat in America, NHANES 2001–2002: Usual nutrient intakes from food compared to dietary reference intakes. U.S. Department of Agriculture, Agricultural Research Service; 2005.[↩]
- Eurodiet Core Report. Available at: http://eurodiet.med.uoc.gr/eurodietcorereport.pdf.[↩]
- Joint WHO/FAO Expert Consultation. Diet, nutrition and the prevention of chronic diseases. Geneva, Switzerland: World Health Organization; 2003.[↩]
- British Nutrition Foundation. Nutrient requirements and recommendations.[↩]
- https://www.nhmrc.gov.au/guidelines-publications/n35-n36-n37[↩]
- Kris-Etherton PM, Innis S, for the American Dietetic Association, Dietitians of Canada. Position of the American Dietetic Association and Dietitians of Canada: dietary fatty acids. J Am Diet Assoc. 2007; 107: 1599–1611.[↩]
- Nelson GJ, Schmidt PC, Bartolini G, Kelley DS, Phinney SD, Kyle D, Silbermann S, Schaefer EJ. The effect of dietary arachidonic acid on plasma lipoprotein distributions, apoproteins, blood lipid levels, and tissue fatty acid composition in humans. Lipids. 1997; 32: 427–433.[↩][↩]
- Omega-6 fatty acids and risk for cardiovascular disease: a science advisory from the American Heart Association Nutrition Subcommittee of the Council on Nutrition, Physical Activity, and Metabolism; Council on Cardiovascular Nursing; and Council on Epidemiology and Prevention. Harris WS, Mozaffarian D, Rimm E, Kris-Etherton P, Rudel LL, Appel LJ, Engler MM, Engler MB, Sacks F. Circulation. 2009 Feb 17; 119(6):902-7. http://circ.ahajournals.org/content/119/6/902.long[↩]
- United States Department of Agriculture Agricultural Research Service. National Nutrient Database for Standard Reference Release 28. https://ndb.nal.usda.gov/ndb/search/list[↩]
- Libby P. Inflammation and cardiovascular disease mechanisms. Am J Clin Nutr. 2006; 83: 456S–460S.[↩]
- Serhan CN. Lipoxins and aspirin-triggered 15-epi-lipoxins are the first lipid mediators of endogenous anti-inflammation and resolution. Prostaglandins Leukot Essent Fatty Acids. 2005; 73: 141–162.[↩]
- Node K, Huo Y, Ruan X, Yang B, Spiecker M, Ley K, Zeldin DC, Liao JK. Anti-inflammatory properties of cytochrome P450 epoxygenase-derived eicosanoids. Science. 1999; 285: 1276–1279.[↩]
- Oltman CL, Weintraub NL, VanRollins M, Dellsperger KC. Epoxyeicosatrienoic acids and dihydroxyeicosatrienoic acids are potent vasodilators in the canine coronary microcirculation. Circ Res. 1998; 83: 932–939.[↩]
- Mohrhauer H, Holman RT. The effect of dose level of essential fatty acids upon fatty acid composition of rat liver. J Lipid Res. 1963; 4: 151–159.[↩]
- Sarkkinen ES, Agren JJ, Ahola I, Ovaskainen ML, Uusitupa MI. Fatty acid composition of serum cholesterol esters, and erythrocyte and platelet membranes as indicators of long-term adherence to fat-modified diets. Am J Clin Nutr. 1994; 59: 364–370.[↩]
- Hussein N, Ah-Sing E, Wilkinson P, Leach C, Griffin BA, Millward DJ. Long-chain conversion of [13C]linoleic acid and alpha-linolenic acid in response to marked changes in their dietary intake in men. J Lipid Res. 2005; 46: 269–280.[↩]
- De Caterina R, Liao JK, Libby P. Fatty acid modulation of endothelial activation. Am J Clin Nutr. 2000; 71: 213S–223S.[↩]
- Ferrucci L, Cherubini A, Bandinelli S, Bartali B, Corsi A, Lauretani F, Martin A, Andres-Lacueva C, Senin U, Guralnik JM. Relationship of plasma polyunsaturated fatty acids to circulating inflammatory markers. J Clin Endocrinol Metab. 2006; 91: 439–446.[↩]
- Pischon T, Hankinson SE, Hotamisligil GS, Rifai N, Willett WC, Rimm EB. Habitual dietary intake of n-3 and n-6 fatty acids in relation to inflammatory markers among US men and women. Circulation. 2003; 108: 155–160.[↩]
- Tsimikas S, Philis-Tsimikas A, Alexopoulos S, Sigari F, Lee C, Reaven PD. LDL isolated from Greek subjects on a typical diet or from American subjects on an oleate-supplemented diet induces less monocyte chemotaxis and adhesion when exposed to oxidative stress. Arterioscler Thromb Vasc Biol. 1999; 19: 122–130.[↩]
- Steinberg D, Parthasarathy S, Carew TE, Khoo JC, Witztum JL. Beyond cholesterol: modifications of low-density lipoprotein that increase its atherogenicity. N Engl J Med. 1989; 320: 915–924.[↩]
- Tsimikas S. Oxidative biomarkers in the diagnosis and prognosis of cardiovascular disease. Am J Cardiol. 2006; 98: 9P–17P.[↩]
- Bleys J, Miller ER 3rd, Pastor-Barriuso R, Appel LJ, Guallar E. Vitamin-mineral supplementation and the progression of atherosclerosis: a meta-analysis of randomized controlled trials. Am J Clin Nutr. 2006; 84: 880–887.[↩]
- Galassetti P, Pontello A. Dietary effects on oxidation of low-density lipoprotein and atherogenesis. Curr Atheroscler Rep. 2006; 8: 523–529.[↩]
- Zock PL, Katan MB. Linoleic acid intake and cancer risk: a review and meta-analysis. Am J Clin Nutr. 1998; 68: 142–153.[↩][↩]
- Mensink RP, Zock PL, Kester AD, Katan MB. Effects of dietary fatty acids and carbohydrates on the ratio of serum total to HDL cholesterol and on serum lipids and apolipoproteins: a meta-analysis of 60 controlled trials. Am J Clin Nutr. 2003; 77: 1146–1155.[↩]
- Siguel E. A new relationship between total/high density lipoprotein cholesterol and polyunsaturated fatty acids. Lipids. 1996; 31 (suppl): S51–S56.[↩]
- Mensink RP, Katan MB. Effect of dietary fatty acids on serum lipids and lipoproteins: a meta-analysis of 27 trials. Arterioscler Thromb. 1992; 12: 911–919.[↩]
- Summers LK, Fielding BA, Bradshaw HA, Ilic V, Beysen C, Clark ML, Moore NR, Frayn KN. Substituting dietary saturated fat with polyunsaturated fat changes abdominal fat distribution and improves insulin sensitivity. Diabetologia. 2002; 45: 369–377.[↩]
- Salmeron J, Hu FB, Manson JE, Stampfer MJ, Colditz GA, Rimm EB, Willett WC. Dietary fat intake and risk of type 2 diabetes in women. Am J Clin Nutr. 2001; 73: 1019–1026.[↩]
- Grimsgaard S, Bonaa KH, Jacobsen BK, Bjerve KS. Plasma saturated and linoleic fatty acids are independently associated with blood pressure. Hypertension. 1999; 34: 478–483.[↩]
- Mozaffarian D, Rimm EB, Herrington DM. Dietary fats, carbohydrate, and progression of coronary atherosclerosis in postmenopausal women. Am J Clin Nutr. 2004; 80: 1175–1184.[↩]
- Pietinen P, Ascherio A, Korhonen P, Hartman AM, Willett WC, Albanes D, Virtamo J. Intake of fatty acids and risk of coronary heart disease in a cohort of Finnish men: the Alpha-Tocopherol, Beta-Carotene Cancer Prevention Study. Am J Epidemiol. 1997; 145: 876–887.[↩]
- Esrey KL, Joseph L, Grover SA. Relationship between dietary intake and coronary heart disease mortality: Lipid Research Clinics Prevalence Follow-Up Study. J Clin Epidemiol. 1996; 49: 211–216.[↩]
- McGee DL, Reed DM, Yano K, Kagan A, Tillotson J. Ten-year incidence of coronary heart disease in the Honolulu Heart Program: relationship to nutrient intake. Am J Epidemiol. 1984; 119: 667–676.[↩]
- Dolecek TA. Epidemiological evidence of relationships between dietary polyunsaturated fatty acids and mortality in the Multiple Risk Factor Intervention Trial. Proc Soc Exp Biol Med. 1992; 200: 177–182.[↩]
- Kushi LH, Lew RA, Stare FJ, Ellison CR, el Lozy M, Bourke G, Daly L, Graham I, Hickey N, Mulcahy R. Diet and 20-year mortality from coronary heart disease: the Ireland-Boston Diet-Heart Study. N Engl J Med. 1985; 312: 811–818.[↩]
- Ascherio A, Rimm EB, Giovannucci EL, Spiegelman D, Stampfer M, Willett WC. Dietary fat and risk of coronary heart disease in men: cohort follow up study in the United States. BMJ. 1996; 313: 84–90.[↩]
- Mozaffarian D, Ascherio A, Hu FB, Stampfer MJ, Willett WC, Siscovick DS, Rimm EB. Interplay between different polyunsaturated fatty acids and risk of coronary heart disease in men. Circulation. 2005; 111: 157–164.[↩]
- Laaksonen DE, Nyyssonen K, Niskanen L, Rissanen TH, Salonen JT. Prediction of cardiovascular mortality in middle-aged men by dietary and serum linoleic and polyunsaturated fatty acids. Arch Intern Med. 2005; 165: 193–199.[↩]
- Oh K, Hu FB, Manson JE, Stampfer JM, Willett WC. Dietary fat intake and risk of coronary heart disease in women: 20 years of follow-up of the Nurses’ Health Study. Am J Epidemiol. 2005; 161: 672–679.[↩]
- Iso H, Stampfer MJ, Manson JE, Rexrode K, Hu F, Hennekens CH, Colditz GA, Speizer FE, Willett WC. Prospective study of fat and protein intake and risk of intraparenchymal hemorrhage in women. Circulation. 2001; 103: 856–863.[↩][↩]
- Sauvaget C, Nagano J, Hayashi M, Yamada M. Animal protein, animal fat, and cholesterol intakes and risk of cerebral infarction mortality in the Adult Health Study. Stroke. 2004; 35: 1531–1537.[↩]
- Iso H, Sato S, Umemura U, Kudo M, Koike K, Kitamura A, Imano H, Okamura T, Naito Y, Shimamoto T. Linoleic acid, other fatty acids, and the risk of stroke. Stroke. 2002; 33: 2086–2093.[↩]
- Dayton S, Pearce ML, Goldman H, Harnish A, Plotkin D, Shickman M, Winfield M, Zager A, Dixon W. Controlled trial of a diet high in unsaturated fat for prevention of atherosclerotic complications. Lancet. 1968; 2: 1060–1062.[↩]
- Turpeinen O, Karvonen MJ, Pekkarinen M, Miettinen M, Elosuo R, Paavilainen E. Dietary prevention of coronary heart disease: the Finnish Mental Hospital Study. Int J Epidemiol. 1979; 8: 99–118.[↩][↩]
- Controlled trial of soya-bean oil in myocardial infarction. Lancet. 1968; 2: 693–699.[↩]
- Leren P. The Oslo Diet–Heart Study: eleven-year report. Circulation. 1970; 42: 935–942.[↩]
- Gordon DJ. Lowering cholesterol and total mortality. In: Rifkin BM, ed. Lowering Cholesterol in High-Risk Individuals and Populations. New York, NY: Marcel Dekker, Inc; 1995: 33–48.[↩]
- Miettinen M, Turpeinen O, Karvonen MJ, Pekkarinen M, Paavilainen E, Elosuo R. Dietary prevention of coronary heart disease in women: the Finnish Mental Hospital Study. Int J Epidemiol. 1983; 12: 17–25.[↩]
- Chin SF, Liu W, Storkson JM, Ha YL, Pariza MW. Dietary sources of conjugated dienoic isomers of linoleic acid, a newly recognised class of anticarcinogens. J Food Compos Anal 1992;5:185–97.[↩]
- Pariza MW. Perspective on the safety and effectiveness of conjugated linoleic acid. Am J Clin Nutr 2004;79(suppl):1132S–6S.[↩]
- Pariza MW, Park Y, Cook ME. The biologically-active isomers of conjugated linoleic acid. Prog Lipid Res2001;40:283–98. https://www.ncbi.nlm.nih.gov/pubmed/11412893[↩][↩][↩]
- Park Y, Storkson JM, Albright KJ, Liu W, Pariza MW. Evidence that the trans-10,cis-12 isomer of conjugated linoleic acid induces body composition changes in mice. Lipids1999;34:235–41. https://www.ncbi.nlm.nih.gov/pubmed/10230716[↩]
- Ip C, Dong Y, Ip MM, et al. Conjugated linoleic acid isomers and mammary cancer prevention. Nutr Cancer2002;43:52–8. https://www.ncbi.nlm.nih.gov/pubmed/12467135[↩]
- Masso-Welch PA, Zangani D, Ip C, et al. Inhibition of angiogenesis by the cancer chemopreventive agent conjugated linoleic acid. Cancer Res2002;62:4383–9.[↩]
- Kemp MQ, Jeffy BD, Romagnolo DF. Conjugated linoleic acid inhibits cell proliferation through a p53-dependent mechanism: effects on the expression of G1-restriction points in breast and colon cancer cells. J Nutr2003;133:3670–7.[↩]
- Roche HM, Noone E, Sewter C, et al. Isomer-dependent metabolic effects of conjugated linoleic acid: insights from molecular markers sterol regulatory element-binding protein-1c and LXR. Diabetes2002;51:2037–44.[↩]
- Perspective on the safety and effectiveness of conjugated linoleic acid. Am J Clin Nutr June 2004, vol. 79 no. 6 1132S-1136S. http://ajcn.nutrition.org/content/79/6/1132S.full[↩][↩]
- Efficacy of conjugated linoleic acid for reducing fat mass: a meta-analysis in humans. Am J Clin Nutr May 2007, vol. 85 no. 5 1203-1211. http://ajcn.nutrition.org/content/85/5/1203.long[↩][↩]
- Blankson H, Stakkestad JA, Fagerton H, Thom E, Wadstein J, Gudmundsen O. Conjugated linoleic acid reduces body fat mass in overweight and obese humans. J Nutr 2000;130:2943–8.[↩][↩]
- Gaullier JM, Halse J, Høye K, et al. Supplementation with conjugated linoleic acid for 24 months is well tolerated by and reduces body fat mass in healthy, overweight humans. J Nutr 2005;135:778–84.[↩][↩]
- Gavino VC, Gavino G, Leblanc MJ, Tuchweber B. An isomeric mixture of conjugated linoleic acids but not pure cis-9, trans-11-octadecadienoic acid affects body weight gain and plasma lipids in hamsters. J Nutr 2000;130:27–9.[↩]
- Riserus U, Arner P, Brismar K, Vessby B. Treatment with dietary trans10cis12 conjugated linoleic acid causes isomer-specific insulin resistance in obese men with the metabolic syndrome. Diabetes Care 2002;25:1516–21.[↩][↩][↩][↩]
- Scimeca JA. Toxicological evaluation of dietary conjugated linoleic acid in male Fischer 344 rats. Food Chem Toxicol1998;36:391–5.[↩]
- O’Hagan S, Menzel A. A subchronic 90-day oral rat toxicity study and in vitro genotoxicity studies with a conjugated linoleic acid product. Food Chem Toxicol2003;41:1749–60.[↩][↩][↩]
- Schulte S, Hasselwander O, Rensmann F-W, Kaesler B, Pfeiffer AM. Safety assessment of conjugated linoleic acid (CLA) esters in the future application field as a feed additive in growing pigs. https://www.aocs.org [↩]
- Pfeiffer AM, Kaufmann W, Braun J, Kaesler B. Target animal safety of conjugated linoleic acid (CLA) on young growing pigs.[↩]
- Gaullier J-M, Breven G, Blankson H, Gudmondsen O. Clinical trial results support a preference for using CLA preparations enriched with two isomers rather than four isomers in human studies. Lipids2002;37:1019–25.[↩]
- Kamphuis MMJW, Lejeune MPGM, Saris WHM, Westerterp-Plantenga MS. The effect of conjugated linoleic acid supplementation after weight loss on body weight regain, body composition, and resting metabolic rate in overweight subjects. Int J Obesity2003;27:840–7.[↩][↩]
- Kamphuis MMJW, Lejeune MPGM, Saris WHM, Westerterp-Plantenga MS. Effect of conjugated linoleic acid supplementation after weight loss on appetite and food intake in overweight subjects. Eur J Clin Nutr2003;57:1268–74.[↩]
- Larsen TM, Toubro S, Astrup A. Efficacy and safety of dietary supplements containing conjugated linoleic acid (CLA) for the treatment of obesity: evidence from animal and human studies. J Lipid Res2003;44:2234–41.[↩]
- Pariza MW, Park Y, Cook ME. The biologically-active isomers of conjugated linoleic acid. Prog Lipid Res2001;40:283–98.[↩][↩]
- Plaa GL. Toxic responses of the liver. In: Klaassen CD, Amdur MO, Doull J, eds. Casarett and Doull’s toxicology, the basic science of poisons. 3rd ed. New York: Macmillan Publishing Company, 1986:286–309.[↩]
- Riserus U, Vessby B, Arnlov J, Basu S. Effects of cis-9,trans-11 conjugated linoleic acid supplementation on insulin sensitivity, lipid peroxidation, and proinflammatory markers in obese men. Am J Clin Nutr 2004;80:279–83.[↩][↩]
- Moloney F, Yeow TP, Mullen A, Nolan JJ, Roche HM. Conjugated linoleic acid supplementation, insulin sensitivity, and lipoprotein metabolism in patients with type 2 diabetes mellitus. Am J Clin Nutr 2004;80:887–95.[↩]
- Malpuech-Brugere C, Verboeket-van de Venne WP, Mensink RP, et al. Effects of two conjugated linoleic acid isomers on body fat mass in overweight humans. Obes Res 2004;12:591–8.[↩]
- Gaullier JM, Halse J, Hoye K, et al. Conjugated linoleic acid supplementation for 1 y reduces body fat mass in healthy overweight humans. Am J Clin Nutr 2004;79:1118–25.[↩]
- Song HJ, Grant I, Rotondo D, et al. Effect of CLA supplementation on immune function in young healthy volunteers. Eur J Clin Nutr 2005;59:508–17.[↩]
- Belury MA. Dietary conjugated linoleic acid in health: physiological effects and mechanisms of action. Annu Rev Nutr 2002;22:505–31.[↩]
- Gaullier JM, Berven G, Blankson H, Gudmundsen O. Clinical trial results support a preference for using CLA preparations enriched with two isomers rather than four isomers in human studies. Lipids 2002;37:1019–25.[↩]
- Tsuboyama-Kasaoka N, Miyazaki H, Kasaoka S, Ezaki O. Increasing the amount of fat in a conjugated linoleic acid-supplemented diet reduces lipodystrophy in mice. J Nutr2003;133:1793–9.[↩]
- Yang MD, Cook ME. Dietary CLA decreased weight loss and extended survival following outset of kidney failure in NZB/WF1 mice. Lipids2003;38:21–4.[↩]
- Kim MR, Park Y, Albright KJ, Pariza MW. Differential responses of hamsters and rats fed high-fat or low-fat diets supplemented with conjugated linoleic acid. Nutr Res2002;22:715–22.[↩]
- Riserus U, Basu S, Jovinge S, Fredrikson GN, Arnlov J, Vessby B. Supplementation with conjugated linoleic acid causes isomer-dependent oxidative stress and elevated C-reactive protein: a potential link to fatty acid-induced insulin resistance. Circulation2002;106:1925–9.[↩][↩][↩][↩]
- Bassaganya-Riera J, Hontecillas R, Beitz DC. Colonic anti-inflammatory mechanisms of conjugated linoleic acid. Clin Nutr2002;21:451–9.[↩]
- Kritchevsky D. Conjugated linoleic acid in experimental atherosclerosis In: Sebedio JL, Christie WW, Adlof R, eds. Advances in conjugated linoleic acid research. Vol 2. Champaign, IL: AOCS Press, 2003:293–301.[↩][↩]
- Toomey S, Roche H, Fitzgerald D, Belton O. Regression of pre-established atherosclerosis in the apoE(−/−) mouse by conjugated linoleic acid. Biochem Soc Trans2003;31:1075–9.[↩]
- Noone EJ, Roche HM, Nugent AP, Gibney MJ. The effect of dietary supplementation using isomeric blends of conjugated linoleic acid on lipid metabolism in healthy human subjects. Br J Nutr2002;88:243–51.[↩][↩]
- Riserus U, Berglund L, Vessby B. Conjugated linoleic acid (CLA) reduced abdominal adipose tissue in obese middle-aged men with signs of the metabolic syndrome: a randomised controlled trial. Int J Obes Relat Metab Disord2001;25:1129–35.[↩]
- Peterson DG, Matitashvili EA, Bauman DE. Diet-induced milk fat depression in dairy cows results in increased trans-10, cis-12 CLA in milk fat and coordinate suppression of mRNA abundance for mammary enzymes involved in milk fat synthesis. J Nutr2003;133:3098–102.[↩]
- Masters N, McGuire MA, Beerman KA, Dasgupta N, McGuire MK. Maternal supplementation with CLA decreases milk fat in humans. Lipids2002;37:133–8.[↩]
- Chin SF, Storkson JM, Albright KJ, Cook ME, Pariza MW. Conjugated linoleic acid is a growth factor for rats as shown by enhanced weight gain and improved feed efficiency. J Nutr1994;124:2344–9.[↩][↩]
- Bee G. Dietary conjugated linoleic acid consumption during pregnancy and lactation influences growth and tissue composition in weaned pigs. J Nutr2000;130:2981–9.[↩][↩]





{kind=link}