
Contents
What is Schnitzler syndrome
Schnitzler syndrome is a rare acquired autoinflammatory disorder characterized by a chronic reddish rash that resembles hives (urticaria) and elevated levels of immunoglobulin M (IgM) monoclonal gammopathy 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12. Schnitzler syndrome’s other features include recurrent fever, joint pain (arthralgia) and joint inflammation (arthritis) and bone pain associated with abnormal bone remodeling and other findings such as enlarged lymph nodes (lymphadenopathy); organomegaly (abnormally enlarged organs); and/or blood abnormalities 13, 1. A monoclonal IgM gammopathy refers to the uncontrolled growth of a single clone (monoclonal) of plasma cells, which results in the abnormal accumulation of M-proteins also known as immunoglobulin M or IgM in the blood. However, the specific role these proteins play and the exact cause of Schnitzler syndrome is unknown; however, most cases occur sporadically in people with no family history of the condition.
Schnitzler syndrome was first described in the medical literature in 1972, by a French dermatologist named Liliane Schnitzler 14. Most of the reported cases of Schnitzler syndrome are of Caucasian descent and have been from Europe, particularly France, but cases have been described in more than 25 countries around the world including Australia, Japan and the United States 15. The average age of onset of Schnitzler syndrome is 50 to 55 years with a slight male predominance. However, only approximately 160 cases of this rare disorder have been reported in the medical literature so no definitive conclusions can be made about ethnic or gender predispositions. Less often, symptoms have been noted in individuals before the age of 35. In one reported case, symptoms were identified in an individual 12 years old. It is to be questioned whether these cases were classical Schnitzler syndrome. Because of the varied symptoms and rarity of Schnitzler syndrome, a diagnosis is usually delayed by several years and researchers believe that the disorder is underdiagnosed, making it difficult to determine its true frequency in the general population.
Schnitzler syndrome shares strong clinicopathologic similarities with monogenic interleukin-1 (IL-1) mediated autoinflammatory disorders and is now considered an acquired adult-onset autoinflammatory disease 1. Autoinflammatory diseases are a group of disorders characterized by recurrent episodes of inflammation due to abnormal activation of the innate immune system leading to sustained systemic inflammation 1. Autoinflammatory diseases are not the same as autoimmune disorders, in which the adaptive immune system malfunctions and mistakenly attacks healthy tissue.
Schnitzler syndrome shares strong clinicopathologic similarities with cryopyrin-associated periodic syndrome (CAPS). Cryopyrin-associated periodic syndrome (CAPS) is a monogenic IL-1-mediated autoinflammatory disorder caused by a gain-of-function mutation in the gene NOD-like receptor family, pyrin domain containing 3 (NLRP3), which encodes a protein called NLRP3 or cryopyrin 1. Cryopyrin-associated periodic syndrome (CAPS) is characterized by an urticaria-like rash from early infancy, fever, and inflammation involving many organ systems, and is associated with significant risk of development of amyloid A (AA) amyloidosis. A further similarity between Schnitzler syndrome and cryopyrin-associated periodic syndrome (CAPS) is their dramatic response to IL-1 antagonists, implying a pivotal role of excess IL-1 production in their pathogenesis 16, 17, 18.
Severe impairment of quality of life and AA amyloidosis used to be the major complications of persistent inflammation in people with Schnitzler syndrome. Amyloid A (AA) amyloidosis also known as secondary amyloidosis, is a rare disease that occurs when proteins in the body mutate and build up in organs and tissues.
Schnitzler syndrome treatment is focused on alleviating the signs and symptoms associated with the condition and may include various medications and/or phototherapy. Treatment with IL-1-blocking drugs has dramatically improved the care of Schnitzler patients by minimizing the risk of these complications.
Schnitzler syndrome prognosis is mostly related to the potential development of a B-cell lymphoproliferative disease, most commonly Waldenström’s macroglobulinemia.
Figure 1. Schnitzler syndrome urticarial skin rash
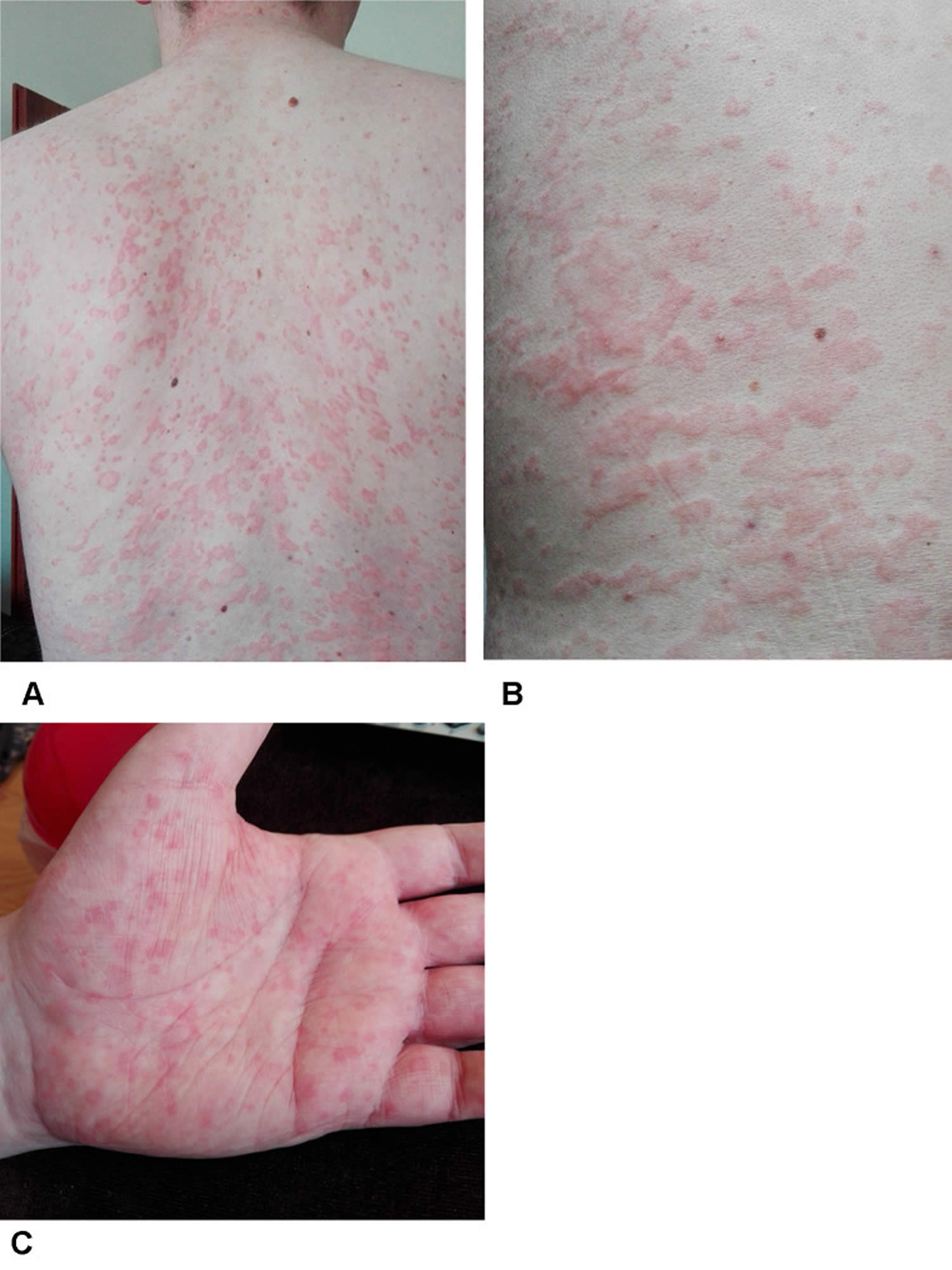
Footnotes: A 32-year-old-man, with a history of chronic urticaria from the age of 27, diagnosed with an adult-onset Still’s disease and received a low dose of glucocorticoids, methotrexate and tocilizumab. Despite the long-term combined treatments, he suffered from chronic urticaria, low-grade fever and bone pain. He was found to have high inflammatory markers, hypogammaglobulinemia, monoclonal IgM – kappa light chain in serum and increased radiotracer uptake in the whole bone scintigraphy. The trunk (A and B) and palm (C) of the hand covered in urticarial rash observed in a Schnitzler syndrome patient during treatment with tocilizumab.
[Source 10 ]Figure 2. Schnitzler syndrome urticarial skin rash (before and after treatment with IL-1-blocking drug anakinra
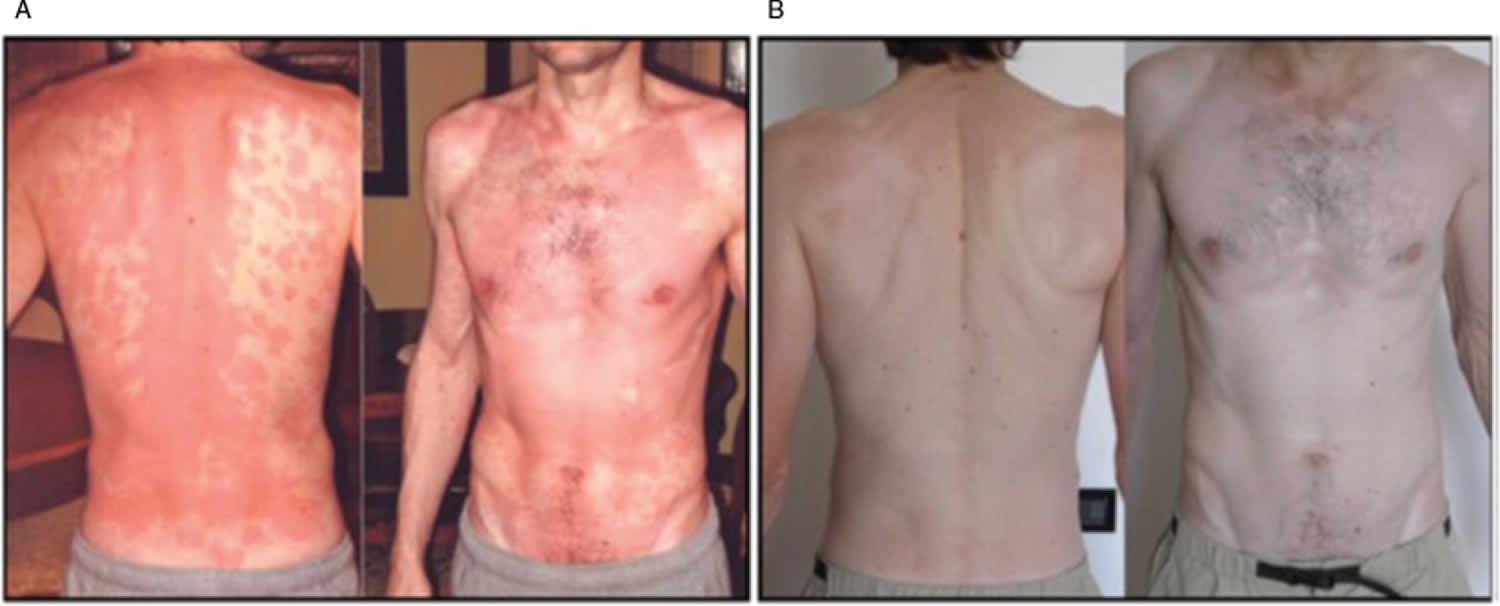
Footnotes: (A) Urticarial skin rash on the trunk of patient with Schnitzler syndrome. (B) Resolution of skin rash after treatment with anakinra, an IL-1-blocking drug.
[Source 11 ]Schnitzler syndrome causes
The exact cause of Schnitzler syndrome is unknown 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11. Researchers believe that specific parts of the immune system may not function properly, eventually causing Schnitzler syndrome.
Certain cytokines (specialized proteins secreted from certain immune system cells that either stimulate or inhibit the function of other immune system cells) play a role in the development of Schnitzler syndrome 2, 19, 20, 21, 22, 23. The cytokine interleukin-1 (IL-1), is an important mediator of the inflammation in Schnitzler syndrome. Abnormal clinical findings involving interleukin-1 (IL-1) have been found in some individuals with Schnitzler syndrome and therapy with drugs that block the activity of interleukin-1 (IL-1) have brought about complete remission.
Individuals with Schnitzler syndrome also have a clinical finding called monoclonal IgM gammopathy, in which abnormalities affecting the production of immunoglobulins result in elevated levels of a specific immunoglobulin M (IgM) in the body. Immunoglobulins are proteins produced by certain white blood cells. There are five classes of immunoglobulins known as IgA, IgD, IgE, IgG, and IgM. Immunoglobulins play a role in defending the body against foreign substances or microorganisms by destroying them or coating them so they are more easily destroyed by white blood cells.
At the time of diagnosis, IgM levels may only be slightly elevated and may remain stable for years. A variant form of Schnitzler syndrome has been reported in which individuals have a monoclonal gammopathy of IgG instead of IgM 24.
The IgM paraprotein was initially thought to be the cause of the skin lesion. It has been shown that IgM deposits can be detected in the skin with the same isotype as the monoclonal gammopathy, but at different sites and with different antigen targets 25. More recently, Pathak et al. 26 performed deep sequencing of the immunoglobulin heavy chain from 10 patients and a protein microarray using isolated IgM from 3 patients: both analyses failed to identify a shared B-cell clonality.
Delayed detection of IgM paraprotein up to 4 years after symptom onset has been reported 27. These results do not support the assertion that the IgM paraprotein is the original causative agent in the pathogenesis of Schnitzler syndrome. On the contrary, descriptions of remission of Schnitzler syndrome symptoms after treatment with chemotherapy (cyclophosphamide +/− rituximab), though rare, could argue for a pathogenic role of gammopathy 28, 29.
Schnitzler syndrome signs and symptoms
The symptoms associated with Schnitzler syndrome can vary from one person to another. The symptoms can occur all at once or, because they often come and go, the symptoms can occur at different times. The symptoms tend to persist for many years (chronic disease).
A pink to reddish rash that resembles hives (urticaria) is the hallmark finding associated with Schnitzler syndrome. The distinctive rash usually consists of raised, reddish bumps (papules) and flatter, wider lesions (plaques) with no change in the skin surface. The rash are monomorphic, confluent, and located on the limbs and trunk, often sparing the face, palms, and soles. Individual lesions last less than 24 hour and resolve without scarring. A halo of vasoconstriction and dermographism may be seen, but angioedema (swelling under the skin or in mucous membranes) is rare. In contrast to classic urticaria (hives), itch (pruritus) is usually absent. Mild itching or burning may develop over time in a subset of Schnitzler syndrome patients. The frequency of eruptions is variable, ranging from daily to several times a year. Antihistamines are ineffective.
In most cases, a rash is the first symptom to appear in individuals with Schnitzler syndrome. The rash usually lasts for a day to two and then disappears without scarring. However, a new rash often develops each day so that a rash is a constant occurrence but the frequency of the rash can vary greatly from one person to another and some people only develop a rash a few times during the year.
When the rash first develops, it usually is not itchy (not pruritic). However, in approximately 45 percent of cases, the rash will become itchy within a few years. The trunk, arms and legs are most often affected. The head, neck, palms and soles are usually spared. Some affected individuals have reported that alcohol, spicy foods and stress have aggravated the rash.
Fevers that come and go over a period of time (chronic, intermittent fevers) are the second most common symptom in individuals with Schnitzler syndrome. The body temperature can rise above 40 °C but is usually well tolerated without chills. The frequency of fevers varies greatly without a periodic pattern, ranging from being a daily occurrence to only a couple times per year. Fever flares can be accompanied by a rash or musculoskeletal pain.
Musculoskeletal involvement is another feature Schnitzler syndrome (affecting more than two-thirds of patients) include bone pain, most often affecting the lower legs and hips and may also occur in the spine, forearm, or clavicle, and joint pain (arthralgia), most often affecting the large joints such as the hips, knees, wrists and ankles. In some cases, inflammation of the joints (arthritis) may develop with accompanying swelling, redness and a feeling of heat or warmth in the joint. Despite joint involvement, joint degeneration or destruction is not a feature of Schnitzler syndrome.
Abnormal enlargement of the lymph nodes (lymphadenopathy) can be found in about 25% of patients, usually in the axilla or groin. Enlarged lymph nodes may be multiple, permanent, and suggestive of a lymphoproliferative disorder. Lymph node biopsy shows reactive lymphadenitis. Enlarged liver (hepatomegaly) and enlarged spleen (splenomegaly) may also occur in a small number of patients 30. Additional nonspecific symptoms that have been reported in individuals with Schnitzler syndrome include unintended weight loss, fatigue and a general feeling of poor health (malaise). Rapid swelling due to fluid accumulation just beneath the surface skin (angioedema) is very rare.
Neuropathy has also been reported in a minority of patients, usually in the form of a symmetrical sensory polyneuropathy. A case of Schnitzler syndrome associated with aortitis, with both conditions responding immediately to IL-1 blockade, has been reported 31. Pancreatitis has been reported in one case of Schnitzler syndrome 32, but the pancreatitis preceded other symptoms by 15 years and the patient had a clear family history of pancreatitis, making it unlikely to be linked with Schnitzler syndrome.
The main hematological (blood) abnormality of Schnitzler syndrome is monoclonal gammopathy. This usually means a raised level of immunoglobulin M (IgM) with a kappa light chain (85% of cases), but raised immunoglobulin G (IgG) or combinations of IgM and IgA or IgM and IgG have also been reported 15, 24, 33. Bone marrow tests are normal in 80% at the time of diagnosis.
Other hematological abnormalities in Schnitzler syndrome may include:
- Elevated C-reactive protein (CRP) or erythrocyte sedimentation rate (ESR)
- Lowered complement levels (C4)
- Anemia of chronic disease
- Thrombocytosis (raised platelet count)
- Neutrophilic leucocytosis (raised neutrophil white blood cells)
Most cases of Schnitzler syndrome have a chronic, benign course. However, over a period of 10 years, approximately 10-15 percent of affected individuals developed cancer, most often cancer caused by the overproduction of white blood cells (lymphoproliferative disorders) such as lymphoplasmacytic lymphoma, Waldenström macroglobulinemia or IgM myeloma 34.
Some individuals with Schnitzler syndrome have elevated levels of a different protein than individuals with classic Schnitzler syndrome. These individuals are classified as having variant Schnitzler syndrome and have very similar symptoms to classic Schnitzler syndrome.
The signs and symptoms of Schnitzler syndrome vary but may include 35:
- Red raised patches of skin (urticaria) that may become itchy. Chronic recurrent, urticarial eruption occurs in all patients, usually as the first sign of Schnitzler syndrome; primarily affects the trunk and the extremities and spares the palms, soles, and head and neck areas.
- Pruritus (itch): Usually absent at disease onset, but lesions may become mildly pruritic in approximately 45% of patients after 3-4 years.
- Recurrent fevers in approximately 90% of patients.
- Join pain and inflammation concurrent with fever; reported in 80% of patients.
- Organomegaly (enlarged internal organs) often involving the lymph nodes (lymphadenopathy), liver (hepatomegaly) and/or spleen (splenomegaly)
- Bone pain concurrent with fever; reported in 70% of patients.
- Blood abnormalities
- Muscle aches (myalgia) concurrent with fever
- Fatigue
- Weight loss
- Angioedema: Very rare
People affected by Schnitzler syndrome also have an increased risk of developing certain lymphoproliferative disorders 12. A monoclonal IgM gammopathy refers to the uncontrolled growth of a single clone (monoclonal) of plasma cells, which results in the abnormal accumulation of M-proteins (also known as immunoglobulin M or IgM) in the blood. However, the specific role these proteins play in Schnitzler syndrome is unknown.
Schnitzler syndrome diagnosis
A diagnosis of Schnitzler syndrome is based upon a thorough clinical evaluation, a detailed patient history, exclusion of other disorders, and identification of characteristic findings, specifically a urticarial rash, an immunoglobulin M (IgM) protein and at least two of the following findings – fever, joint pain or inflammation, bone pain, palpable lymph nodes, enlargement of the liver or spleen, elevated numbers of white blood cells (leukocytosis), elevated red blood cell (erythrocyte) sedimentation rate or abnormalities on bone morphological study, which can reveal increased bone density (osteosclerosis).
Sedimentation rate measures how long it takes red blood cells to settle in a test tube over a given period. Many individuals with Schnitzler syndrome have an elevated sedimentation rate, which is an indication of inflammation.
Histopathologic examination reveals a neutrophilic urticarial dermatosis 30. The dermis contains a neutrophilic perivascular and interstitial infiltrate with leukocytoclasis. There is little to no edema and no vasculitis. The perivascular neutrophilic infiltrate associated with leukocytoclasis should not be confused with vasculitis, as there are no fibrinoid changes in the vessel walls in neutrophilic urticarial dermatosis. Neutrophilic epitheliotropism is highly suggestive, especially around the sweat glands. This histopathologic pattern of neutrophilic urticarial dermatosis is not specific to Schnitzler syndrome and may be seen in cryopyrin-associated periodic syndrome (CAPS), adult-onset Still’s disease, or systemic lupus erythematosus (SLE).
In younger patients, careful attention should be paid because alternative diagnosis is much more likely and often overlooked – such as urticarial vasculitis, hematological disease or chronic idiopathic urticaria – which needs a different approach to treatment – so a diagnosis of Schnitzler’s syndrome in younger patients should only be made after extensive work on exclusion of other diagnoses.
Schnitzler syndrome diagnostic criteria were established by Lipsker et al. in 2001 36. The Lipsker diagnostic criteria of Schnitzler syndrome were updated in 2012 at an expert meeting in Strasbourg 37, with the main difference being the inclusion of IgG monoclonal gammopathy in addition to IgM. Both diagnostic criteria were later validated in 2017 in a cohort of 42 already-diagnosed patients 38. It is important to remember that the reliability of these diagnostic criteria has not been evaluated in recent-onset disease. Patients may not fully meet all criteria at presentation. In the case of a neutrophilic urticarial dermatosis associated with an IgM monoclonal gammopathy, Schnitzler’s syndrome must be suspected, even if the minor criteria are not sufficient.
Lipsker diagnostic criteria of Schnitzler syndrome
Urticarial rash and monoclonal IgM component and at least 2 of the following criteria 36:
- Fever
- Arthralgia or arthritis
- Bone pain
- Palpable lymph nodes
- Liver or spleen enlargement
- Elevated ESR
- Leukocytosis
- Abnormal findings on bone morphologic investigations
Footnote: In patients treated with IL-1 inhibitors, a rapid and immediate response is supportive of the diagnosis. In case of unresponsiveness to anakinra, the diagnosis should be reconsidered.
Strasbourg diagnostic criteria of Schnitzler syndrome
Obligate criteria:
- Chronic urticarial rash and
- Monoclonal IgM or IgG
Minor criteria:
- Recurrent fever (>38 °C, otherwise unexplained)
- Objective findings of abnormal bone remodeling with or without bone pain. (Assessed by bone scintigraphy, MRI, or elevation of bone alkaline phosphatase)
- Neutrophilic urticarial dermatosis on skin biopsy
- Neutrophils > 10,000/mm³ and/or CRP > 30 mg/L
Definite diagnosis of Schnitzler syndrome if the following are present:
- Two obligate criteria AND at least two minor criteria if IgM and three minor criteria if IgG
Probable diagnosis of Schnitzler’s syndrome if the following are present:
- Two obligate criteria AND at least one minor criterion if IgM and two minor criteria if IgG
Schnitzler syndrome differential diagnosis
Schnitzler syndrome differential diagnosis include 15:
Immunological disorders
- Adult-onset Still’s disease (AOSD)
- Systemic lupus erythematosus (SLE)
- Acquired C1 esterase deficiency
Hematological disorders
- Monoclonal gammopathy of unknown significance (MGUS)
- Polyneuropathy, organomegaly, endocrinopathy, monoclonal gammopathy, and skin changes (POEMS) syndrome
- Waldenström’s macroglobulinemia
- Lymphoma
- Multiple myeloma
Hereditary auto-inflammatory syndromes
- Cryopyrin-associated periodic syndrome (CAPS)
Infectious diseases
- Hepatitis B and hepatitis C
- Chronic meningococcemia
Other
- Chronic spontaneous urticaria
- Hypocomplementaemic urticarial vasculitis
- Delayed pressure urticaria
- Cryoglobulinemia
- Erdheim-Chester disease
- Mastocytosis
Schnitzler syndrome treatment
The treatment of Schnitzler syndrome is aimed at alleviating the signs and symptoms associated with the condition. The following medications have been used with variable success 34, 39:
- Nonsteroidal anti-inflammatory drugs (NSAIDs)
- Corticosteroids
- Immunosuppressive agents
- Interleukin-1 receptor antagonists (medications that inhibit the cytokine IL-1)
- Colchicine
- Dapsone
- Thalidomide
- Rituximab
Some studies suggest that phototherapy may improve the rash in some affected people 34.
First-line treatment in mild cases is with nonsteroidal anti-inflammatory drugs (NSAIDs). But this is often not sufficient.
In more severe cases, the standard treatment is with therapy to inhibit the cytokine IL-1. Patients with Schnitzler syndrome are successfully treated with anakinra, an interleukin-1 receptor antagonist. Anakinra is a drug that blocks the activity of interleukin-1, which some researchers believe plays a key role in the development of Schnitzler syndrome. There have also been at least 2 studies showing the efficacy of the interleukin-1 beta antibody canakinumab.
High-dose regimens of corticosteroids have temporarily improved symptoms in some cases, but usually must be stopped due to side effects. In a small percentage of cases, colchicine (a medication used to suppress inflammation in acute gout) and dapsone were effective in treating some individuals with Schnitzler syndrome. Interleukin-6 is a cytokine that can be induced by interleukin-1; , anti-interleukin-6 therapy was also recently tried in three patients with Schnitzler syndrome, in which it was effective.
At least three individuals with Schnitzler syndrome have been successfully treated with thalidomide, a drug that affects how the immune system works (immunomodulatory drugs). Thalidomide induced a complete resolution of the rash and dramatic improvement of other symptoms in three individuals who received the drug as a therapy for Schnitzler syndrome. However, thalidomide is often associated with significant side effects including pain, numbness and a tingling sensation in the hands and feet (peripheral neuropathy). Two of the three patients had to stop thalidomide therapy because of side effects. In addition, two additional individuals with Schnitzler syndrome did not improve after treatment with thalidomide. More research is necessary to determine the long-term safety, effectiveness and role, if any, of thalidomide in treating individuals with Schnitzler syndrome.
A small study investigated the effectiveness of the antibiotic drug, pefloxacine, for the treatment of Schnitzler syndrome. Eleven affected individuals received pefloxacine, which caused rapid and dramatic improvement of both the rash and systemic symptoms associated with the disorder. More research is necessary to determine the long-term safety and effectiveness of pefloxacine in the treatment of individuals with Schnitzler syndrome.
Interleukin (IL) inhibitors
Inhibitors of interleukin 1 (IL-1) (anakinra, rilonacept and canakinumab) appear to be particularly effective and have dramatically changed the management of these patients 40. IL-1 inhibitors are now the first-line treatment for Schnitzler syndrome, with high efficacy, a rapid response, and few side effects. IL-6 anatoganists have been tried for non-responders to IL-1 responders.
Anakinra
Anakinra is a recombinant human interleukin-1 receptor antagonist (IL-1RA). Anakinra has the same amino acid sequence as native recombinant human interleukin-1 receptor antagonist (IL-1RA) with the addition of an N-terminal methionine residue. Anakinra acts as a competitive inhibitor by binding to interleukin-1 receptor (IL-1R), thereby inhibiting the biological activity of interleukin-1 alpha (IL-1α) and interleukin-1 beta (IL-1β). Anakinra has been approved by the U.S. Food and Drug Administration (FDA) for the treatment of rheumatoid arthritis, Neonatal-Onset Multisystem Inflammatory Disease (NOMID), the most severe form of cryopyrin-associated periodic syndrome (CAPS), and more recently for the treatment of deficiency interleukin-1 receptor antagonist (DIRA). In Europe, anakinra is also approved for the treatment of Familial Mediterranean Fever and Still’s disease.
The efficacy of anakinra in Schnitzler syndrome was first reported in 2005 41 and it has since become the main treatment for Schnitzler syndrome. Anakinra is administered subcutaneously and has a half-life of 3 to 9.5 hour. Symptoms resolve within hours of injection, but relapse usually occurs within 24–48 hours if treatment is not continued. Therefore, injections given daily or every other day are usually required to maintain remission. Most patients respond to anakinra, and anakinra itself serves as a diagnostic test. Resistance to anakinra should prompt a review of the diagnosis.
In Schnitzler syndrome, anakinra subcutaneous dose of 100 mg/day allows a complete control of all symptoms including 35:
- chronic urticarial rash with a monoclonal IgM component
- intermittent fever
- arthralgia or arthritis
- bone pain
- lymphadenopathy
- leukocytosis
- elevated ESR
- spleen or liver enlargement
Complete remissions have been reported in at least 10 patients with anakinra at a daily subcutaneous dose of 100 mg. Some patients have experienced a recurrence of signs and symptoms within 1 day of stopping treatment; anakinra must be given on a continuous basis. Localized painful erythematous injection site reactions may occur.
There are no major contraindications to anakinra except hypersensitivity to the drug. Anakinra is usually well tolerated with the exception of frequent injection site reactions. The neutrophil count should be assessed before starting the treatment and then monitored as neutropenia has been described with anakinra. Rare cases of serious infections or hepatitis have been reported.
Canakinumab
Canakinumab is a human anti-IL-1β monoclonal antibody. Canakinumab has been approved by the FDA for the treatment of several periodic fever syndromes (CAPS, Familial Mediterranean Fever, Tumor Necrosis Factor Receptor-Associated Periodic Syndrome [TRAPS], Hyperimmunoglobulin D Syndrome [HDS], and Mevalonate Kinase Deficiency [MKD]), as well as Still’s disease and gout.
Compared to anakinra, canakinumab has a longer half-life of 22.9 to 25.7 days. In Schnitzler syndrome, the efficacy and safety of canakinumab were demonstrated in a randomized, placebo-controlled trial 42 and the 4-year extension study confirmed its sustained effects 43. The interval between injections in the latter study was 62 days.
Canakimumab has the advantage of requiring fewer injections than anakinra. However, in the event of complications, the short half-life of anakinra is an advantage, as it is completely cleared within 48 hours. In addition, canakinumab is an expensive treatment. In France, the cost of 150 mg of canakinumab is EURO 11,364, compared to EURO 32 for 100 mg of anakinra (i.e., EURO 1920 for 60 daily injections of anakinra).
Rilonacept
Rilonacept is a chimeric recombinant fusion protein combining the extracellular ligand binding domain of interleukin-1 receptor (IL-1R) and the IL-1R accessory protein (IL-1RAcP). It acts as a soluble decoy receptor that binds to IL-1α and IL-1β. Rilonacept was approved by the FDA in 2008 for cryopyrin-associated periodic syndrome (CAPS) and in 2021 for recurrent pericarditis. The efficacy of rilonacept was reported in an open-label study that included eight patients treated with a loading dose of 320 mg followed by a weekly dose of 160 mg for 1 year 44.
Colchicine
Colchicine at approximately 1 mg per day may be effective in a subset of Schnitzler syndrome patients and may be considered as a first-line treatment in patients with mild disease and no persistent elevation of inflammatory markers, or as an adjunct in patients who do not fully respond to IL-1 inhibition 39.
Tocilizumab
Tocilizumab is a humanized anti-IL-6R monoclonal antibody used primarily for the treatment of rheumatoid arthritis, giant cell arteritis, and juvenile idiopathic arthritis. The efficacy of tocilizumab was evaluated in an open-label study involving nine Schnitzler syndrome patients treated with weekly subcutaneous injections of 162 mg 45. Tocilizumab was associated with a clinical and biological response in most patients, but a loss of efficacy was observed over time. Tocilizumab may be considered alone or in association in the rare cases of Schnitzler syndrome patients who do not respond to interleukin-1 inhibitors 45.
Ibrutinib
Ibrutinib is an irreversible inhibitor of Bruton’s tyrosine kinase (BTK) approved for the treatment of several lymphoproliferative disorders, including Waldenström’s macroglobulinemia. Bruton’s tyrosine kinase (BTK) has been shown to be a regulator of the NLRP3 inflammasome, and its blockade by ibrutinib has been shown in test tube study to reduce IL-1β release by immune cells 46. Partial or complete efficacy of ibrutinib has been reported in a few Schnitzler syndrome case reports 47, 48.
Follow-Up
Schnitzler syndrome is a recurrent/chronic disease, and only one case of complete and prolonged spontaneous remission has been reported in the literature 49.
Serum AA protein (SAA) is a protein produced during inflammation that can form insoluble fibrils that accumulate in tissues. AA amyloidosis resulting from these pathogenic amyloid fibrils is a rare complication of chronic inflammation. AA amyloidosis has been described in most subtypes of cryopyrin-associated periodic syndrome (CAPS) 50 and a few cases have been described in patients with Schnitzler syndrome after several years of untreated symptoms 51, 15, 52. Interleukin-1 inhibitors are highly effective in preventing AA amyloidosis. Light-chain (AL) amyloidosis, which is secondary to the deposition of amyloid fibrils derived from the light chain of monoclonal immunoglobulin, has not been reported so far in patients with Schnitzler syndrome.
Schnitzler syndrome prognosis
The long-term outlook (prognosis) for people with Schnitzler syndrome is generally good. Schnitzler syndrome does not affect lifespan in most cases, but requires periodic follow up because of the increased risk of developing cancer. Although Schnitzler syndrome is chronic and symptoms can be a nuisance, it generally does not progress to severe disease in most affected people. However, approximately 10-15% of people with Schnitzler syndrome develop a lymphoproliferative disorder, most commonly Waldenström’s macroglobulinemia 34. Due to the rarity of Schnitzler syndrome and the lack of published follow-up data, the exact frequency of progression is unknown. The development of a hematologic malignancy has been reported in 35 of 281 patients (12%) with a median follow-up of 8 years after disease onset, but the true frequency is probably higher 15. The risk is likely to be similar to the risk of progression in IgM monoclonal gammopathy of undetermined significance (MGUS). Most data suggest that suppression of inflammation with IL-1 or IL-6 inhibitors does not affect the monoclonal gammopathy and does not prevent the development of lymphoproliferative disease. Long-term follow-up of IgM gammopathy in patients with Schnitlzer syndrome is needed.
Schnitzler’s original patient died at age 88 years, with a diffuse lymphoplasmacytic infiltration of his liver and bone marrow 53. Thus, the initial workup of a Schnitzler syndrome patient should include an examination of the bone marrow, immunoelectrophoresis of serum, and a urinary protein level. A lymph node biopsy should be performed if the nodes are enlarged.
Kidney involvement has been described as a rare complication, but it improved with treatment in the cases reported 54.
- Braud A, Lipsker D. Schnitzler Syndrome: Insights into Its Pathogenesis, Clinical Manifestations, and Current Management. Biomolecules. 2024 May 31;14(6):646. doi: 10.3390/biom14060646[↩][↩][↩][↩][↩][↩]
- Rowczenio DM, Pathak S, Arostegui JI, et al. Molecular genetic investigation, clinical features, and response to treatment in 21 patients with Schnitzler syndrome. Blood. 2018 Mar 1;131(9):974-981. doi: 10.1182/blood-2017-10-810366[↩][↩][↩]
- Szklarz M, Gontarz-Nowak K, Kieroński A, Golon K, Górny J, Matuszewski W, Bandurska-Stankiewicz E. The co-occurrence of SAT, hypophysitis, and Schnitzler syndrome after COVID-19 vaccination: the first described case. Hormones (Athens). 2024 Dec;23(4):735-752. doi: 10.1007/s42000-024-00567-6[↩][↩]
- Nakaizumi H, Kambe N, Irie H, Kaku Y, Fujimoto M, Yoshifuji H, Kazuma Y, Katagiri K, Kanekura T, Kabashima K. Neutrophilic epitheliotropism, proposed as an auto-inflammatory condition of neutrophilic urticarial dermatosis including Schnitzler syndrome, is also observed in Japanese cases. J Dermatol. 2024 Apr;51(4):592-596. doi: 10.1111/1346-8138.17067[↩][↩]
- Huang Y, Wang Y, Yu F, Mao X, Wang B, Li J, Li L. Case Report: Therapeutic Use of Ibrutinib in a Patient With Schnitzler Syndrome. Front Immunol. 2022 Apr 20;13:894464. doi: 10.3389/fimmu.2022.894464[↩][↩]
- Darrieutort-Laffite C, Ansquer C, Aubert H, Kraeber-Bodéré F, Masseau A, Agard C, Hamidou M, Bernier C, Berthelot JM, Le Goff B, Barbarot S, Néel A. Rheumatic involvement and bone scan features in Schnitzler syndrome: initial and follow-up data from a single-center cohort of 25 patients. Arthritis Res Ther. 2020 Nov 18;22(1):272. doi: 10.1186/s13075-020-02318-5[↩][↩]
- Kano Y, Sugihara M. Schnitzler Syndrome Presenting as a Fever of Unknown Origin with Elevated Alkaline Phosphatase Levels. Intern Med. 2023 May 1;62(9):1361-1364. doi: 10.2169/internalmedicine.0359-22[↩][↩]
- Hodl I, Bosch P, Dreo B, Stradner MH. Case Report: Extensive Phosphorylation of Interleukin-1 Receptor-Associated Kinase 4 in a Patient With Schnitzler Syndrome. Front Immunol. 2020 Sep 30;11:576200. doi: 10.3389/fimmu.2020.576200[↩][↩]
- Puxkandl V, Currie A, Hoetzenecker W, Altrichter S. Therapy resistant urticaria as a long-term symptom of an incomplete Schnitzler syndrome. Allergy Asthma Clin Immunol. 2023 Jul 26;19(1):64. doi: 10.1186/s13223-023-00819-x[↩][↩]
- Więsik-Szewczyk E, Felis-Giemza A, Dziuk M, Jahnz-Różyk K. Schnitzler Syndrome in a 27-Year-Old Man: Diagnostic and Therapeutic Dilemma in Adult Auto-Inflammatory Syndromes A Case Report and Literature Review. Int J Gen Med. 2020 Sep 25;13:713-719. doi: 10.2147/IJGM.S265482[↩][↩][↩]
- Chu CQ. Schnitzler syndrome and Schnitzler-like syndromes. Chin Med J (Engl). 2022 May 20;135(10):1190-1202. doi: 10.1097/CM9.0000000000002015[↩][↩][↩]
- Schnitzler Syndrome. https://rarediseases.org/rare-diseases/schnitzler-syndrome[↩][↩]
- Schnitzler syndrome. https://rarediseases.info.nih.gov/diseases/12390/schnitzler-syndrome[↩]
- Schnitzler L., Schubert B., Boasson M., Gardais J., Tourmen A. Urticaire chronique, lésions osseuses, macroglobulinémie IgM: Maladie de Waldenström? 2ème présentation. Bull. Soc. Fr. Dermatol. Syphiligr. 1974;81:363.[↩]
- de Koning HD. Schnitzler’s syndrome: lessons from 281 cases. Clin Transl Allergy. 2014 Dec 5;4:41. doi: 10.1186/2045-7022-4-41[↩][↩][↩][↩][↩]
- Hawkins PN, Lachmann HJ, McDermott MF. Interleukin-1-receptor antagonist in the Muckle-Wells syndrome. N Engl J Med. 2003 Jun 19;348(25):2583-4. doi: 10.1056/NEJM200306193482523[↩]
- Lachmann HJ, Kone-Paut I, Kuemmerle-Deschner JB, Leslie KS, Hachulla E, Quartier P, Gitton X, Widmer A, Patel N, Hawkins PN; Canakinumab in CAPS Study Group. Use of canakinumab in the cryopyrin-associated periodic syndrome. N Engl J Med. 2009 Jun 4;360(23):2416-25. doi: 10.1056/NEJMoa0810787[↩]
- Hoffman HM, Throne ML, Amar NJ, Sebai M, Kivitz AJ, Kavanaugh A, Weinstein SP, Belomestnov P, Yancopoulos GD, Stahl N, Mellis SJ. Efficacy and safety of rilonacept (interleukin-1 Trap) in patients with cryopyrin-associated periodic syndromes: results from two sequential placebo-controlled studies. Arthritis Rheum. 2008 Aug;58(8):2443-52. doi: 10.1002/art.23687[↩]
- Baroja-Mazo A, Martín-Sánchez F, Gomez AI, Martínez CM, Amores-Iniesta J, Compan V, Barberà-Cremades M, Yagüe J, Ruiz-Ortiz E, Antón J, Buján S, Couillin I, Brough D, Arostegui JI, Pelegrín P. The NLRP3 inflammasome is released as a particulate danger signal that amplifies the inflammatory response. Nat Immunol. 2014 Aug;15(8):738-48. doi: 10.1038/ni.2919[↩]
- Krause K, Sabat R, Witte-Händel E, Schulze A, Puhl V, Maurer M, Wolk K. Association of CCL2 with systemic inflammation in Schnitzler syndrome. Br J Dermatol. 2019 Apr;180(4):859-868. doi: 10.1111/bjd.17334[↩]
- Masson Regnault M, Frouin E, Jéru I, et al. Cytokine Signature in Schnitzler Syndrome: Proinflammatory Cytokine Production Associated to Th Suppression. Front Immunol. 2020 Nov 26;11:588322. doi: 10.3389/fimmu.2020.588322[↩]
- de Koning HD, van Vlijmen-Willems IM, Rodijk-Olthuis D, van der Meer JW, Zeeuwen PL, Simon A, Schalkwijk J. Mast-cell interleukin-1β, neutrophil interleukin-17 and epidermal antimicrobial proteins in the neutrophilic urticarial dermatosis in Schnitzler’s syndrome. Br J Dermatol. 2015 Aug;173(2):448-56. doi: 10.1111/bjd.13857[↩]
- Nakamura Y, Kambe N, Saito M, Nishikomori R, Kim YG, Murakami M, Núñez G, Matsue H. Mast cells mediate neutrophil recruitment and vascular leakage through the NLRP3 inflammasome in histamine-independent urticaria. J Exp Med. 2009 May 11;206(5):1037-46. doi: 10.1084/jem.20082179. Epub 2009 Apr 13. Erratum in: J Exp Med. 2009 May 11;206(5):1205. Nishikomiri, Ryuta [corrected to Nishikomori, Ryuta].[↩]
- Kaganov E., Jhaveri D., Peters P., IJdo J.W. An Unusual Presentation of Immunoglobulin A Gammopathy in a Patient with Schnitzler’s Syndrome. Int. J. Rheum. Dis. 2023;26:2085–2088. doi: 10.1111/1756-185X.14718[↩][↩]
- Lipsker D., Spehner D., Drillien R., Schmitt P., Cribier B., Heid E., Humbel R.L., Grosshans E. Schnitzler Syndrome: Heterogeneous Immunopathological Findings Involving IgM-Skin Interactions. Br. J. Dermatol. 2000;142:954–959. doi: 10.1046/j.1365-2133.2000.03477.x[↩]
- Pathak S., Rowczenio D., Lara-Reyna S., Kacar M., Owen R., Doody G., Krause K., Lachmann H., Doffinger R., Newton D., et al. Evidence of B Cell Clonality and Investigation into Properties of the IgM in Patients With Schnitzler Syndrome. Front. Immunol. 2020;11:569006. doi: 10.3389/fimmu.2020.569006[↩]
- Mulla E., Neame R. Delayed Development of the IgM Paraprotein in Schnitzler’s Syndrome. Scand. J. Rheumatol. 2015;44:521–522. doi: 10.3109/03009742.2015.1071421[↩]
- Peterlana D., Puccetti A., Tinazzi E., Simeoni S., Lunardi C. Schnitzler’s Syndrome Treated Successfully with Intravenous Pulse Cyclophosphamide. Scand. J. Rheumatol. 2005;34:328–330. doi: 10.1080/03009740510017733[↩]
- Aouba A., Pressiat C., Pricopi M., Georgin-Lavialle S., Boue F., Lievre-Castilla M.-A., Marfaing-Koka A., Prevot S., Decottignies A. Complete Remission of Schnitzler Syndrome and Waldenström Macroglobulinemia under Rituximab-Cyclophosphamide-Dexamethasone. Dermatology. 2014;230:18–22. doi: 10.1159/000368349[↩]
- Kieffer C., Cribier B., Lipsker D. Neutrophilic Urticarial Dermatosis: A Variant of Neutrophilic Urticaria Strongly Associated with Systemic Disease. Report of 9 New Cases and Review of the Literature. Medicine. 2009;88:23–31. doi: 10.1097/MD.0b013e3181943f5e[↩][↩]
- Bursztejn A.-C., Imperiale A., Lipsker D. Aortitis: A New Feature of Schnitzler Syndrome. JAAD Case Rep. 2017;3:454–456. doi: 10.1016/j.jdcr.2017.06.016[↩]
- Larocca C.A., McEvoy J.W., Ellis C.L., Junkins-Hopkins J., Kolb T., Baer A.N., Garibaldi B.T. Schnitzler’s Syndrome Associated with Pancreatitis: A Disease of IL-1 Dysregulation. Clin. Rheumatol. 2012;31:169–174. doi: 10.1007/s10067-011-1804-4[↩]
- Carlesimo M., Abruzzese C., Narcisi A., La Verde G., De Marco G., Verga E., Fidanza L., Camplone G. Chronic Vasculitis Urticaria Associated to a Monoclonal Gammopathy of IgM and IgA Type, a Schnitzler Syndrome? Eur. J. Dermatol. EJD. 2010;20:838–839. doi: 10.1684/ejd.2010.1091[↩]
- Schnitzler Syndrome. https://emedicine.medscape.com/article/1050761-overview[↩][↩][↩][↩]
- Schnitzler syndrome. https://www.dermnetnz.org/topics/schnitzler-syndrome/[↩][↩]
- Lipsker D., Veran Y., Grunenberger F., Cribier B., Heid E., Grosshans E. The Schnitzler Syndrome. Four New Cases and Review of the Literature. Medicine. 2001;80:37–44. doi: 10.1097/00005792-200101000-00004[↩][↩]
- Simon A., Asli B., Braun-Falco M., De Koning H., Fermand J.-P., Grattan C., Krause K., Lachmann H., Lenormand C., Martinez-Taboada V., et al. Schnitzler’s Syndrome: Diagnosis, Treatment, and Follow-Up. Allergy. 2013;68:562–568. doi: 10.1111/all.12129[↩][↩]
- Gusdorf L., Asli B., Barbarot S., Néel A., Masseau A., Puéchal X., Gottenberg J.-E., Grateau G., Blanchard-Delaunay C., Rizzi R., et al. Schnitzler Syndrome: Validation and Applicability of Diagnostic Criteria in Real-Life Patients. Allergy. 2017;72:177–182. doi: 10.1111/all.13035[↩]
- Lipsker D., Lenormand C. Management of Schnitzler’s Syndrome. Expert Opin. Orphan Drugs. 2014;2:947–955. doi: 10.1517/21678707.2014.939170[↩][↩]
- Krause, K, Tsianakas A, Wagner, N, et al. Effectiveness of canakinumab treatment in Schnitzler’s syndrome: a multi-center randomized placebo controlled study. Pediatric Rheumatology. 2015. 13 (supplement 1):066.[↩]
- Martinez-Taboada V.M., Fontalba A., Blanco R., Fernández-Luna J.L. Successful Treatment of Refractory Schnitzler Syndrome with Anakinra: Comment on the Article by Hawkins Et Al. Arthritis Rheum. 2005;52:2226–2227. doi: 10.1002/art.21101[↩]
- Krause K., Tsianakas A., Wagner N., Fischer J., Weller K., Metz M., Church M.K., Maurer M. Efficacy and Safety of Canakinumab in Schnitzler Syndrome: A Multicenter Randomized Placebo-Controlled Study. J. Allergy Clin. Immunol. 2017;139:1311–1320. doi: 10.1016/j.jaci.2016.07.041[↩]
- Krause K., Bonnekoh H., Ellrich A., Tsianakas A., Wagner N., Fischer J., Maurer M. Long-Term Efficacy of Canakinumab in the Treatment of Schnitzler Syndrome. J. Allergy Clin. Immunol. 2020;145:1681–1686.e5. doi: 10.1016/j.jaci.2019.12.909[↩]
- Krause K., Weller K., Stefaniak R., Wittkowski H., Altrichter S., Siebenhaar F., Zuberbier T., Maurer M. Efficacy and Safety of the Interleukin-1 Antagonist Rilonacept in Schnitzler Syndrome: An Open-Label Study. Allergy. 2012;67:943–950. doi: 10.1111/j.1398-9995.2012.02843.x[↩]
- Bonnekoh H., Frischbutter S., Roll S., Maurer M., Krause K. Tocilizumab Treatment in Patients with Schnitzler Syndrome: An Open-Label Study. J. Allergy Clin. Immunol. Pract. 2021;9:2486–2489.e4. doi: 10.1016/j.jaip.2021.01.024[↩][↩]
- Liu X., Pichulik T., Wolz O.-O., Dang T.-M., Stutz A., Dillen C., Garcia M.D., Kraus H., Dickhöfer S., Daiber E., et al. Human NACHT, LRR, and PYD Domain–Containing Protein 3 (NLRP3) Inflammasome Activity Is Regulated by and Potentially Targetable through Bruton Tyrosine Kinase. J. Allergy Clin. Immunol. 2017;140:1054–1067.e10. doi: 10.1016/j.jaci.2017.01.017[↩]
- Jani P., Vissing M.B., Ahmed S., Sluzevich J.C., Aulakh S., Alegria V., Ailawadhi M., Chanan-Khan A., Ailawadhi S. Ibrutinib for the Management of Schnitzler Syndrome: A Novel Therapy for a Rare Condition. J. Oncol. Pract. 2018;14:387–388. doi: 10.1200/JOP.18.00050[↩]
- Wang C. Killing Two Birds with One Stone: The Therapeutic Role of Ibrutinib in Schnitzler Syndrome. J. Clin. Immunol. 2021;41:1706–1707. doi: 10.1007/s10875-021-01105-4[↩]
- Asli B., Brouet J.C., Fermand J.P. Spontaneous Remission of Schnitzler Syndrome. Ann. Allergy Asthma Immunol. 2011;107:87–88. doi: 10.1016/j.anai.2011.04.006[↩]
- Rodrigues F., Cuisset L., Cador-Rousseau B., Giurgea I., Neven B., Buob D., Quartier P., Hachulla E., Lequerré T., Cam G., et al. AA Amyloidosis Complicating Cryopyrin-Associated Periodic Syndrome: A Study of 86 Cases Including 23 French Patients and Systematic Review. Rheumatology. 2022;61:4827–4834. doi: 10.1093/rheumatology/keac145[↩]
- Claes K., Bammens B., Delforge M., Evenepoel P., Kuypers D., Vanrenterghem Y. Another Devastating Complication of the Schnitzler Syndrome: AA Amyloidosis. Br. J. Dermatol. 2008;158:182–184. doi: 10.1111/j.1365-2133.2007.08251.x[↩]
- Palladini G., Merlini G. The Elusive Pathogenesis of Schnitzler Syndrome. Blood. 2018;131:944–946. doi: 10.1182/blood-2018-01-824862[↩]
- Schnitzler L, Schubert B, Boasson M. Urticaire chronique, lons osseuses, macroglobuline IgM: maladie de Waldenstrom. Bull Soc Franc Derm Syph. 1974. 81:363.[↩]
- Basile C, Rossi L, Casucci F, Teutonico A, Libutti P, Lisi P, et al. Kidney involvement in the Schnitzler syndrome, a rare disease. Clin Kidney J. 2017 Dec. 10(6):723-727.[↩]





{kind=link}