Contents
What is a separated shoulder
A separated shoulder actually refers to an injury not to the shoulder joint but to the acromioclavicular joint, a joint formed by the acromion of the scapula and the acromial end of the clavicle. A separated shoulder is an injury to the ligaments that hold your collarbone (clavicle) to your shoulder blade. A separated shoulder injury actually involves the acromioclavicular joint (also called the AC joint) (see Figures 1 to 3). The acromioclavicular (AC) joint is where the collarbone (clavicle) meets the highest point of the shoulder blade (acromion). This condition is usually the result of forceful trauma to the joint, as when the shoulder strikes the ground in a fall. Separated shoulder (acromioclavicular) joint dislocation is a common injury, which accounts for about 9% of all shoulder injuries 1. It ranks second only to shoulder (glenohumeral) joint dislocation, with a higher incidence in athletes. Treatment options are similar to those for treating a dislocated shoulder, although surgery is rarely needed.
A shoulder separation is the partial or complete separation of two parts of the shoulder: the collarbone (clavicle) and the end (acromion) of the shoulder blade (scapula). A shoulder separation can be type I, in which the acromioclavicular (AC) ligament is partially torn, but the coracoclavicular (CC) ligament is not injured (Figure 1). In a type II shoulder separation, the acromioclavicular (AC) ligament is completely torn, and the coracoclavicular (CC) ligament is either partially torn or not injured. A type III shoulder separation occurs when both the acromioclavicular and coracoclavicular ligaments are completely torn.
In most people, a separated shoulder doesn’t usually require surgery. Instead, conservative treatment — such as rest, ice and pain relievers — is often enough to relieve the pain. Most people regain full shoulder function within a few weeks after having a separated shoulder.
Separated shoulder anatomy
Biomechanical studies found that the horizontal stability of the acromioclavicular (AC) joint was mainly mediated by the acromioclavicular ligament. The superior and posterior acromioclavicular ligaments are the major structures responsible for limiting the posterior translation of the distal clavicle 2, producing 56% and 25% of the limitation, respectively 3, indicating that the acromioclavicular ligaments can effectively control the posterior translation of the distal clavicle. Although the inferior acromioclavicular ligament is thin, it is the main structure that limits the anterior translation of the distal clavicle 4. Debski et al. 5 found that transection of the acromioclavicular joint capsule resulted in a significant increase in anterior translation (6.4 mm) and posterior translation (3.6 mm) but not in superior translation. Anterior and posterior loading leads to significantly increased forces in the coracoclavicular ligaments, suggesting that the coracoclavicular ligaments can partially compensate for the injured capsule in resisting horizontal loading conditions. However, the significant increases in the anterior translation and posterior translation demonstrate that the vertical coracoclavicular ligament cannot effectively restrain against anteroposterior instability. The main vertical stabilizer of the acromioclavicular joint is the coracoclavicular ligament, in which the conoid ligament served as a primary restraint against vertical loading, followed by the trapezoid ligament.
Figure 1. Shoulder anatomy
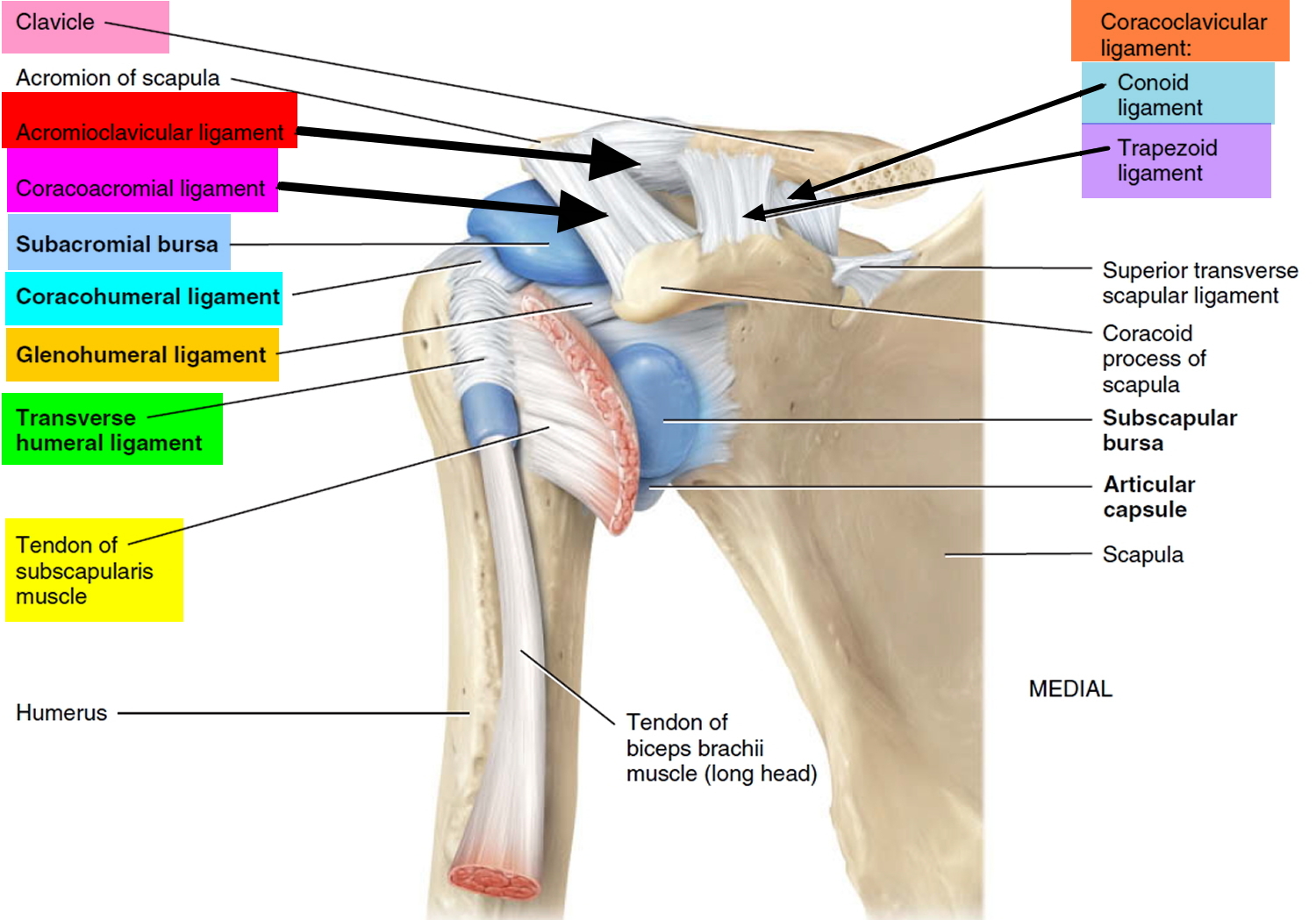
Figure 2. Separated shoulder types
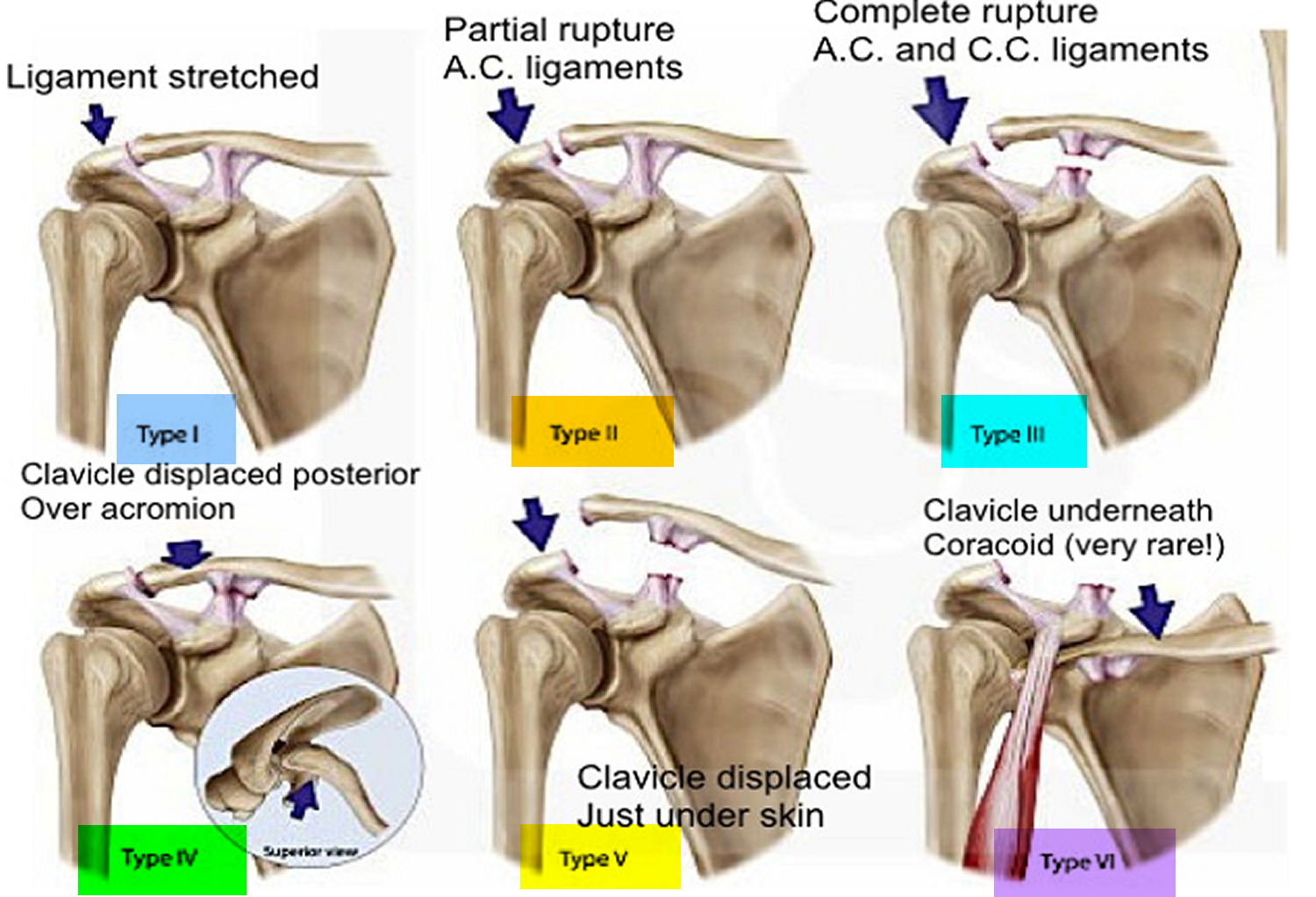
Figure 3. Separated shoulder

Separated shoulder recovery time
Most people recover from a shoulder separation without surgery, within 2 to 12 weeks. You will be treated with ice, medicines, a sling, and then exercises as you continue to heal.
Your recovery may be slower if you have:
- Arthritis in your shoulder joint
- Damaged cartilage (cushioning tissue) between your collarbone and top of your shoulder blade
- A severe shoulder separation
You may need surgery right away if you have:
- Numbness in your fingers
- Cold fingers
- Muscle weakness in your arm
- Severe deformity of the joint
Separated shoulder cause
The most common cause for a separation of the acromioclavicular (AC) joint is from a fall directly onto the shoulder. The fall injures the ligaments that surround and stabilize the acromioclavicular joint. The injury may stretch or tear the ligaments that hold your collarbone to your shoulder blade.
If the force is severe enough, the ligaments attaching to the underside of the clavicle are torn. This causes the separation of the collarbone and the shoulder blade. The shoulder blade (scapula) actually moves downward from the weight of the arm. This creates a bump or bulge above the shoulder (see Figure 3 above).
The injury can range from a mild sprain without a bump to a complete disruption with a very large bump. Good pain-free function often returns even with a very large bump. The greater the deformity, the longer it takes for pain-free function to return.
- A mild shoulder separation involves a sprain of the acromioclavicular (AC) ligament that does not move the collarbone and looks normal on X-rays.
- A more serious injury tears the acromioclavicular ligament and sprains or slightly tears the coracoclavicular (CC) ligament, putting the collarbone out of alignment to some extent with a smaller bump.
- The most severe shoulder separation completely tears both the acromioclavicular and coracoclavicular ligaments and puts the acromioclavicular (AC) joint noticeably out of position, with a larger bump.
Risk factors for separated shoulder
Participating in contact sports, such as football and hockey, or in sports that can involve falls — such as downhill skiing, gymnastics and volleyball — might put you at higher risk of a separated shoulder.
Separated shoulder symptoms
Signs and symptoms of a separated shoulder might include:
- Shoulder pain
- Shoulder or arm weakness
- Shoulder bruising or swelling
- Limited shoulder movement
- A bump and swelling at the top of your shoulder.
Separated shoulder complications
Most people fully recover from a separated shoulder with conservative treatment. Continued shoulder pain is possible, however, if:
- You have a severe separation that involves significant displacement or fracture of the collarbone
- You develop arthritis in your shoulder
- Other structures around your shoulder, such as the rotator cuff, are damaged
Separated shoulder diagnosis
Diagnosis of acromioclavicular joint dislocation relied on physical examination and radiographic inspection. Clinical signs included swelling of the injured shoulder, tenderness of the acromioclavicular joint, a positive piano-key sign, a bone rubbing feeling and limitation of shrug activity.
The injury is easy to identify when it causes deformity. When there is less deformity, the location of pain and x-rays help the doctor make the diagnosis. Sometimes having the patient hold a weight in the hand can increase the deformity, which makes the injury more obvious on x-rays.
Radiographic evaluations included anteroposterior X-ray of the bilateral acromioclavicular joint, Zanca view oblique X-ray, and an additional stress X-ray for the dislocation with unknown classification. If separated shoulder type IV injury with horizontal instability was suspected during the examination, computerized tomography (CT) and three-dimensional imaging were performed to identify the posterior translation of the distal clavicle.
Separated shoulder treatment
Most people enjoy a full recovery after conservative treatment. A minor separation usually heals within a few weeks. A more severe separation might take several weeks to months to heal. You might always have a noticeable bump on the affected shoulder, but it shouldn’t affect your ability to use that shoulder.
Whether treated conservatively or with surgery, the shoulder will require rehabilitation to restore and rebuild motion, strength, and flexibility.
Nonsurgical Treatment
Nonsurgical treatments, such as a sling, cold packs, and medications can often help manage the pain. Rarely, a doctor may use more complicated supports to help lessen acromioclavicular (AC) joint motion and pain.
Medications
Over-the-counter pain relievers, such as acetaminophen (Tylenol, others), ibuprofen (Advil, Motrin IB, others) and naproxen sodium (Aleve), may help ease shoulder pain.
Therapy
- Rest. Avoid activities that aggravate your shoulder pain, especially crossing the affected arm in front of your body. You might want to temporarily immobilize your arm in a sling to take pressure off your shoulder and promote healing.
- Ice. Ice can reduce shoulder pain and swelling. Use a cold pack for 15 to 20 minutes at a time.
- Physical therapy. Stretching and strengthening exercises can help restore strength and motion in your shoulder.
Most people return to near full function with this injury, even if there is a persistent, significant deformity/bump. Some people have continued pain in the area of the acromioclavicular (AC) joint, even with only a mild deformity. This may be due to:
- Abnormal contact between the bone ends when the joint is in motion
- Development of arthritis
- Injury to a disk-like piece of cushioning cartilage that is often found between the bone ends of this joint
It is often worthwhile to wait and see if reasonable function returns without surgical treatment. Most patients, even with very severe injuries, are often managed effectively without surgery.
Separated shoulder self-care at home
Make an ice pack by putting ice in a sealable plastic bag and wrapping a cloth around it. DO NOT put the bag of ice directly on the area, as the ice could damage your skin.
On the first day of your injury, apply the ice every 10 to 15 minutes, for 20 minutes each time. After the first day, ice the area every 3 to 4 hours for 20 minutes each time. Do this for 2 days or longer, or as instructed by your provider.
For pain, you can take ibuprofen (Advil, Motrin), naproxen (Aleve, Naprosyn), aspirin, or acetaminophen (Tylenol). You can buy these pain medicines without a prescription.
- Talk with your doctor before using these medicines if you have heart disease, high blood pressure, kidney disease, or have had stomach ulcers or bleeding.
- DO NOT take more than the amount recommended on the bottle.
- DO NOT give aspirin to children.
You may be given a shoulder sling to use for a few weeks.
- Once you have less pain, begin range of motion exercises so that your shoulder does not get stuck in place. This is called contracture. Check with your provider before doing any of these motions.
- After your injury has healed, DO NOT lift heavy objects for 8 to 12 weeks.
Separated shoulder surgery
Surgery can be considered if pain persists or the deformity is severe. A surgeon might recommend trimming back the end of the collarbone so that it does not rub against the shoulder blade bone (acromion).
Where there is significant deformity, reconstructing the ligaments that attach to the underside of the collarbone is helpful. This type of surgery works well even if it is done long after the problem started. These operations can be done arthroscopically or open, with a plate or without. Sometimes, if a plate is used to assist with the surgery, it is usually removed after healing of the shoulder separation.
Surgical techniques for reconstructing or repairing acromioclavicular joint dislocation have evolved over the last decades 6. However, a golden standard procedure has not emerged. The majority of previous procedures focus on reconstruction of the coracoclavicular ligament to recover the stability of acromioclavicular joint, but few studies are reported regarding acromioclavicular ligament reconstruction. Moreover, biomechanical studies demonstrate that the horizontal stability of the acromioclavicular ligament cannot be completely restored by reconstruction of other ligaments 7.
Figure 4. Acromioclavicular ligament reconstruction (Kirschner’s wire). (A) Anteroposterior view; (B) vertical view.
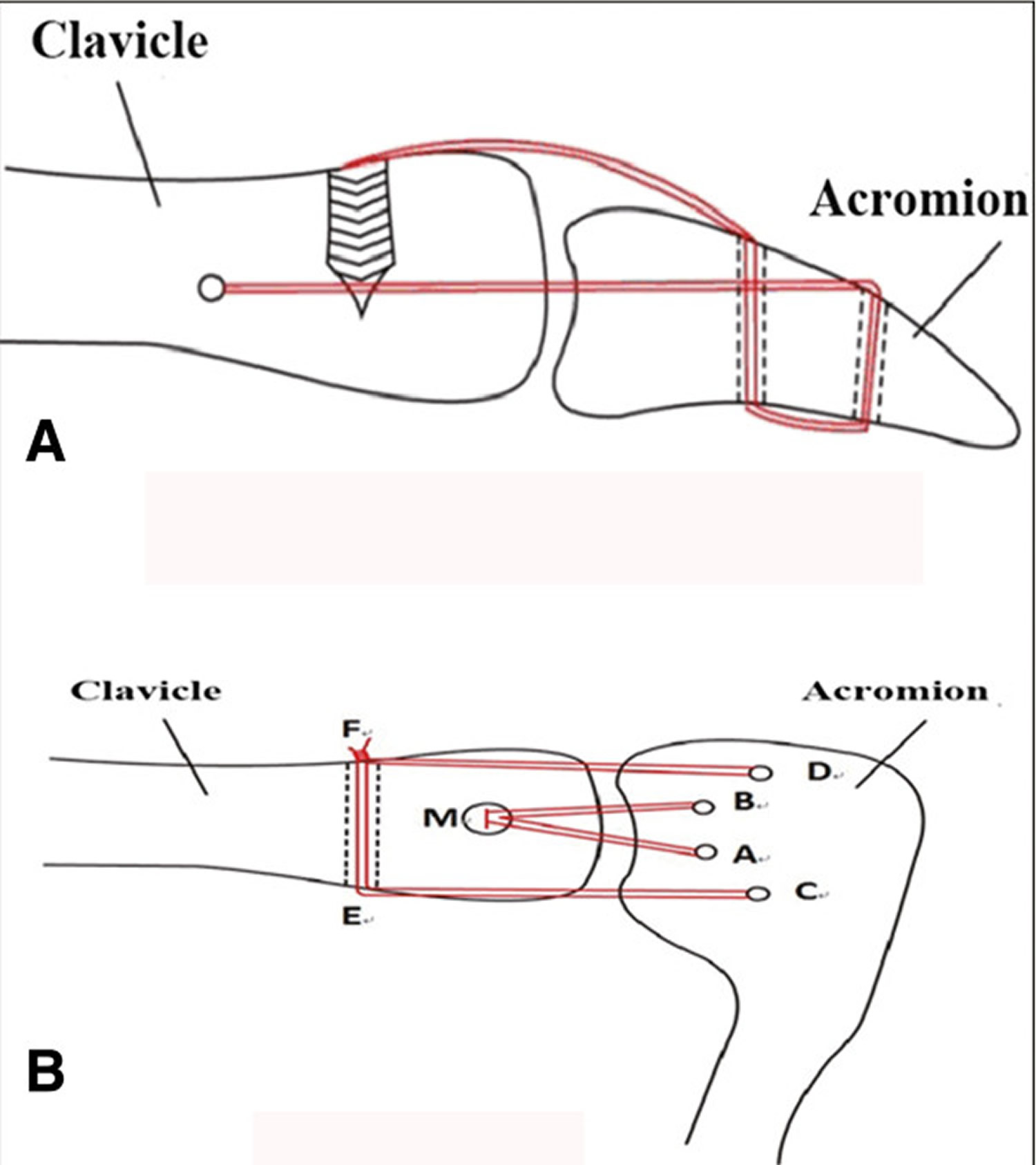
Kirschner’s wire and tension band are commonly used at an early stage, and these exhibit advantages of easy performance and low cost. However, Kirschner’s wire may destroy the acromioclavicular joint surface and fibrocartilage plate, and is prone to induce acromioclavicular joint degeneration and traumatic arthritis. Considering that the acromioclavicular joint is a type of amphiarthrosis, rigid fixation via this joint leads to a high incidence of Kirschner’s wire breakage or loosening. A high incidence of complications is reported, and Kirschner’s wire may translate into the pleural cavity, spinal cord, and subclavicular space.
The Bosworth screw method is a stabilization, with screws between the clavicle and the coracoid. Such a fixation impedes the synchronous rotation function of the clavicle and scapula 8, and leads to screw loosening or cut-out. This method is rarely applied currently.
Stabilization of the coracoclavicular interval with a steel or titanium loop is a form of extra-acromioclavicular joint fixation, which does not aggravate the acromioclavicular joint degeneration, and enables movement in the acromioclavicular joint. However, the fixation has common complications of loop rupture, clavicle or coracoid fracture, and sub coracoid neurovascular injury. Moreover, loop stabilization is a non-anatomical reconstruction method, which leads to the anterior displacement of the distal clavicle in comparison with its normal anatomical location 9. Since the clavicle hook plate was first used by Hachkenbruch et al. 10 to treat acromioclavicular joint dislocation and good efficacy was achieved, it has been widely applied in clinical practices, and better results were achieved by surgical treatment with the hook plate than by conservative treatment although the coracoclavicular ligament was not reconstructed. However, this method has problems of postoperative shoulder pain, acromial impingement, clavicle bone erosion, and fracture surrounding the fixator. The clavicle hook plate should be removed before the motion of the shoulder joint recovers to the point that the forearm extends to the vertex, namely about 8 to 12 weeks after surgery, while the premature removal of the plate may lead to the risk of loss of reduction 11. The classical Weaver-Dunn procedure is to resect the distal clavicle, and transfer the coracoacromial ligament to reconstruct coracoclavicular ligament. Such a technique shows high efficacy in the treatment of chronic painful acromioclavicular joint dislocations 12. Many biomechanical studies demonstrated weakness of the coracoacromial ligament after reconstruction, which was about 75% that of the intact coracoclavicular ligament 13. It is reported that the postoperative failure of acromioclavicular joint reduction is 20%. In recent years, anatomical reconstruction of coracoclavicular ligaments with autologous tendon has been applied more and more widely 14. Clinical and biomechanical studies showed that, compared with other methods, such a reconstruction obtained a strength and stiffness that was better approximated to the native structure, with obviously better clinical outcomes than that of the modified Weaver-Dunn procedure 15. However, the reconstruction has the disadvantage of potential problems of complications on the donor sites 16. In addition, the aforementioned methods only focus on coracoclavicular ligament reconstruction, without reference to acromioclavicular ligament reconstruction.
For acute acromioclavicular joint dislocation, particularly severe injuries of Rockwood type IV or greater, owing to ruptures of the acromioclavicular ligament, coracoclavicular ligament and delta-trapezius fascia, both static and dynamic stability of the acromioclavicular joint are destroyed; therefore, the acromioclavicular joint is unstable. The ideal treatment is to reconstruct each component of the acromioclavicular joint, that is, both the coracoclavicular ligament and the acromioclavicular ligament. This study presents a novel acromioclavicular ligament reconstruction technique designed by the authors, in combination with a double endobutton technique for coracoclavicular ligament reconstruction, to treat acute complete acromioclavicular dislocation. A double endobutton technique was used to restore the function of the conoid ligament anatomically, and its strength and stiffness exceeded the native ligament complex by approximately 40% 17, which provided good instant stability and enhanced the ligament’s endurance to cyclic loads. The weight of the upper limb and the loads produced by activities are distributed onto two button plates, which reduce the risk of clavicle or coracoid fractures. The plate of the endobutton is very thin, and this low-profile design reduces irritation of the surrounding tissues by the implants. The loop on the endobutton is a knotless design, which avoids soft tissue reactions caused by knotting. Such a method allows a certain motion in the acromioclavicular joint during abduction and elevation of the shoulder, which is in agreement with the physiological characteristic that the acromioclavicular joint belongs to amphiarthrosis 18. Moreover, this method can be developed to provide an arthroscopic minimally invasive operation using suitable technology and equipment, and many studies report that arthroscopically endobutton reconstruction achieves satisfactory efficacy 19.
There are few studies reported in the literature regarding acromioclavicular joint reconstruction. Two previous studies selected the bone hole in the clavicle during coracoclavicular ligament reconstruction as the clavicular insertion site for acromioclavicular ligament reconstruction 20. This bone hole is about 20 to 25 mm medially from the acromioclavicular joint, while the anatomical distance between the clavicular insertion of the normal acromioclavicular ligament and the acromioclavicular joint was 5.2 mm (women) and 7.6 mm (men) 21. A longer distance between the clavicular insertion and acromial insertion of the ligament leads to poorer horizontal stability. In this study, the insertion site of the clavicle and acromion was reduced to within 8 mm, which was approximate to the anatomical position, to achieve better stability.
Separated shoulder rehab
The period of immobilization following reduction is variable, though immobilization in a standard sling. Immobilization is usually achieved using a sling to maintain a position of internal rotation. Plenty of early rest is needed. The sore area can be iced 3 to 4 times a day.
The period of immobilization is followed by rehabilitation with physiotherapy targeted towards restoring the range of motion and improving the strength of the shoulder joint to maximize its stability.
After the pain and swelling go down, the doctor will prescribe rehabilitation exercises for you. These help restore the shoulder’s range of motion and strengthen the muscles. Rehabilitation will begin with gentle muscle toning exercises. Later, weight training can be added.
- After your injury has healed, DO NOT lift heavy objects for 8 to 12 weeks.
Follow-up
If you continue to have pain, your provider will probably ask you to come back in 1 week to decide if you need to:
- See an orthopedist (bone doctor)
- Begin physical therapy or range of motion exercises
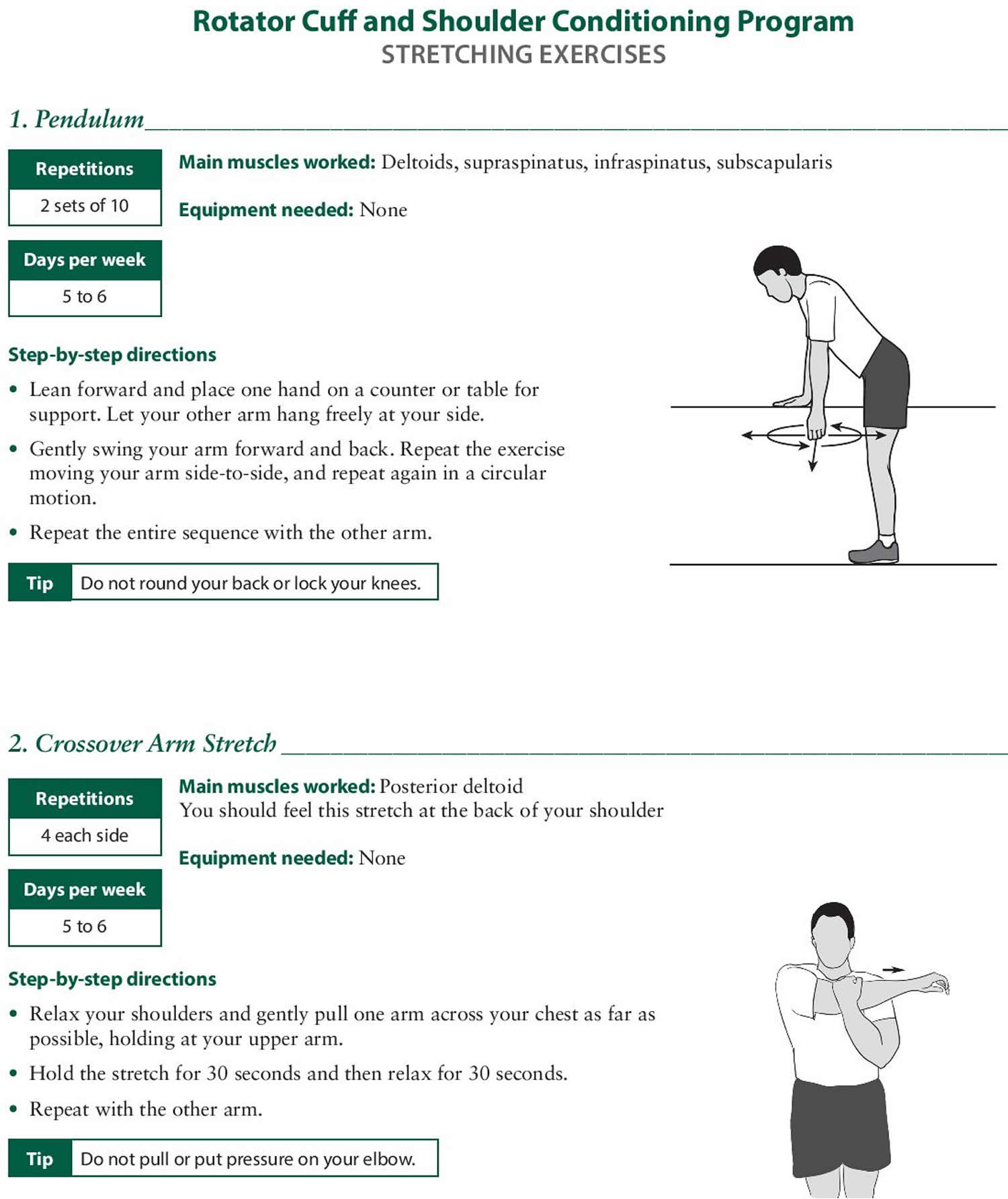
Separated shoulder exercises
- Evaluation and treatment of acromioclavicular joint injuries. Mazzocca AD, Arciero RA, Bicos J. Am J Sports Med. 2007 Feb; 35(2):316-29. https://www.ncbi.nlm.nih.gov/pubmed/17251175/[↩]
- Beitzel K, Sablan N, Chowaniec DM, Obopilwe E, Cote MP, Arciero RA, Mazzocca AD. Sequential resection of the distal clavicle and its effects on horizontal acromioclavicular joint translation. Am J Sports Med. 2012;40:681–685. doi: 10.1177/0363546511428880. https://www.ncbi.nlm.nih.gov/pubmed/22156172[↩]
- Klimkiewicz JJ, Williams GR, Sher JS, Karduna A, Des Jardins JD, Iannotti JP. The acromioclavicular capsule as a restraint to posterior translation of the clavicle: a biomechanical analysis. J Shoulder Elbow Surg. 1999;8:119–124. doi: 10.1016/S1058-2746(99)90003-4. https://www.ncbi.nlm.nih.gov/pubmed/10226962[↩]
- Lee K-W, Debski RE, Chen C-H, Woo SL-Y, Fu FH. Functional evaluation of the ligaments at the acromioclavicular joint during anteroposterior and superoinferior translation. Am J Sports Med. 1997;25:858–862. doi: 10.1177/036354659702500622. https://www.ncbi.nlm.nih.gov/pubmed/9397278[↩]
- Debski RE, Parsons I, Woo SL, Fu FH. Effect of capsular injury on acromioclavicular joint mechanics. J Bone Joint Surg Am. 2001;83:1344–1351. https://www.ncbi.nlm.nih.gov/pubmed/11568197[↩]
- Outcome of conjoined tendon and coracoacromial ligament transfer for the treatment of chronic type V acromioclavicular joint separation. Kim SH, Lee YH, Shin SH, Lee YH, Baek GH. Injury. 2012 Feb; 43(2):213-8. https://www.ncbi.nlm.nih.gov/pubmed/21890137/[↩]
- Effect of capsular injury on acromioclavicular joint mechanics. Debski RE, Parsons IM 4th, Woo SL, Fu FH. J Bone Joint Surg Am. 2001 Sep; 83-A(9):1344-51. https://www.ncbi.nlm.nih.gov/pubmed/11568197/[↩]
- Gong X, Jiang C, Wang M. Diagnosis and treatment of acromioclavicular joint dislocation. Chin J Orthop. 2005;4:240–244.[↩]
- Baker JE, Nicandri GT, Young DC, Owen JR, Wayne JS. A cadaveric study examining acromioclavicular joint congruity after different methods of coracoclavicular loop repair. J Shoulder Elbow Surg. 2003;12:595–598. doi: 10.1016/S1058-2746(03)00050-8. https://www.ncbi.nlm.nih.gov/pubmed/14671525[↩]
- Gstettner C, Tauber M, Hitzl W, Resch H. Rockwood type III acromioclavicular dislocation: surgical versus conservative treatment. J Shoulder Elbow Surg. 2008;17:220–225. doi: 10.1016/j.jse.2007.07.017. https://www.ncbi.nlm.nih.gov/pubmed/18249565[↩]
- Nadarajah R, Mahaluxmivala J, Amin A, Goodier D. Clavicular hook-plate: complications of retaining the implant. Injury. 2005;36:681–683. doi: 10.1016/j.injury.2004.08.010. https://www.ncbi.nlm.nih.gov/pubmed/15826633[↩]
- Kumar S, Penematsa S, Selvan T. Surgical reconstruction for chronic painful acromioclavicular joint dislocations. Arch Orthop Trauma Surg. 2007;127:481–484. doi: 10.1007/s00402-007-0298-7. https://www.ncbi.nlm.nih.gov/pubmed/17639430[↩]
- Grutter PW, Petersen SA. Anatomical acromioclavicular ligament reconstruction a biomechanical comparison of reconstructive techniques of the acromioclavicular joint. Am J Sports Med. 2005;33:1723–1728. doi: 10.1177/0363546505275646. https://www.ncbi.nlm.nih.gov/pubmed/16093536[↩]
- Deshmukh AV, Wilson DR, Zilberfarb JL, Perlmutter GS. Stability of acromioclavicular joint reconstruction biomechanical testing of various surgical techniques in a cadaveric model. Am J Sports Med. 2004;32:1492–1498. doi: 10.1177/0363546504263699. https://www.ncbi.nlm.nih.gov/pubmed/15310576[↩]
- Tauber M, Gordon K, Koller H, Fox M, Resch H. Semitendinosus tendon graft versus a modified Weaver-Dunn procedure for acromioclavicular joint reconstruction in chronic cases: a prospective comparative study. Am J Sports Med. 2009;37:181–190. https://www.ncbi.nlm.nih.gov/pubmed/18818433[↩]
- Freedman JA, Adamson GJ, Bui C, Lee TQ. Biomechanical evaluation of the acromioclavicular capsular ligaments and reconstruction with an intramedullary free tissue graft. Am J Sports Med. 2010;38:958–964. doi: 10.1177/0363546509355056. https://www.ncbi.nlm.nih.gov/pubmed/20139471[↩]
- Wei H-F, Chen Y-F, Zeng B-F, Zhang C-Q, Chai Y-M, Wang H-M, Lu Y. Triple endobutton technique for the treatment of acute complete acromioclavicular joint dislocations: preliminary results. Int Orthop. 2011;35:555–559. doi: 10.1007/s00264-010-1057-x. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3066326/[↩]
- Zhao L, Zhang Y, Yin Z, Shi L, Wang L, Xue Q. The early results of total arthroscopic double endobutton technique for acute acromioclavicular joint dislocation. Chin J Joint Surg. 2010;4:18–24.[↩]
- Venjakob AJ, Salzmann GM, Gabel F, Buchmann S, Walz L, Spang JT, Vogt S, Imhoff AB. Arthroscopically assisted 2-bundle anatomic reduction of acute acromioclavicular joint separations 58-month findings. Am J Sports Med. 2013;41:615–621. doi: 10.1177/0363546512473438. https://www.ncbi.nlm.nih.gov/pubmed/23371472[↩]
- Carofino BC, Mazzocca AD. The anatomic coracoclavicular ligament reconstruction: surgical technique and indications. J Shoulder Elbow Surg. 2010;19:37–46. doi: 10.1016/j.jse.2010.01.004. https://www.ncbi.nlm.nih.gov/pubmed/20188267[↩]
- Renfree KJ, Riley MK, Wheeler D, Hentz JG, Wright TW. Ligamentous anatomy of the distal clavicle. J Shoulder Elbow Surg. 2003;12:355–359. doi: 10.1016/S1058-2746(03)00029-6. https://www.ncbi.nlm.nih.gov/pubmed/12934030[↩]





{kind=link}