Contents
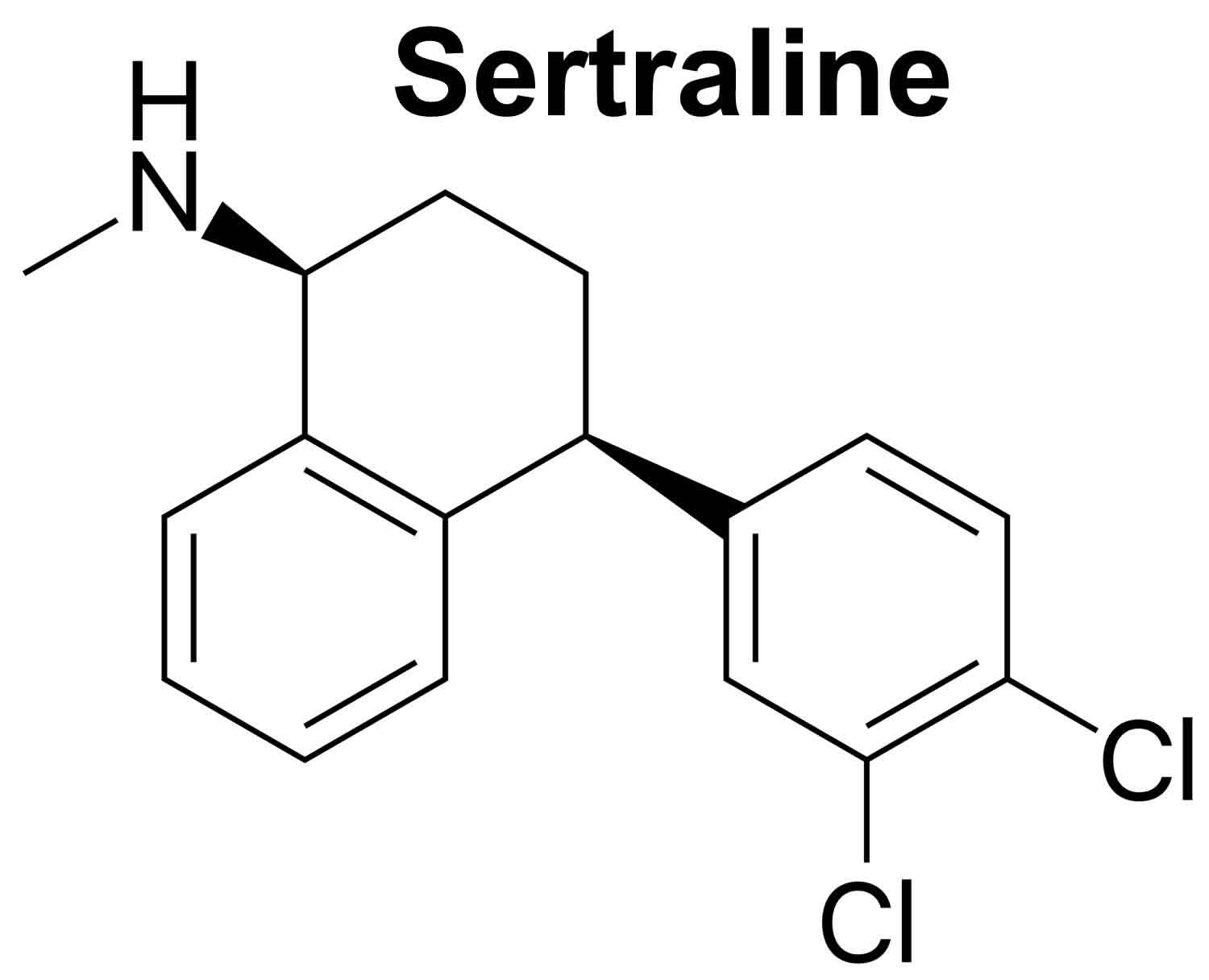
Sertraline
Sertraline is a selective serotonin reuptake inhibitor (SSRI) medication that has been used to treat depression, obsessive-compulsive disorder (OCD, bothersome thoughts that won’t go away and the need to perform certain actions over and over), panic attacks (sudden, unexpected attacks of extreme fear and worry about these attacks), and major anxiety disorders including social anxiety disorder, post-trauma stress disorder (PTSD, disturbing psychological symptoms that develop after a frightening experience) and generalized anxiety disorder (GAD), panic disorder, premenstrual dysphoric disorder [PMDD] (a severe form of premenstrual syndrome [PMS] with mood swings, irritability, bloating, and breast tenderness), and social anxiety disorder (extreme fear of interacting with others or performing in front of others that interferes with normal life) 1. Sertraline is also used for headache, diabetic neuropathy and premature ejaculation. Sertraline works by blocking the reuptake of serotonin in your brain neurons, thus increasing serotonin levels in your brain which is associated with its psychiatric effects.
Sertraline was approved for use in the United States in 1991, and it remains in wide use, with almost 40 million prescriptions being filled yearly 2.
Sertraline is available as tablets of 25, 50 and 100 mg and as an oral suspension (liquid) in multiple generic forms and under the brand name of Zoloft. Sertraline is usually taken once daily in the morning or evening. The recommended dosage for depression in adults is 50 or 100 mg once daily, increasing the dosage by 25 or 50 mg increments to a maximum of 200 mg. Take sertraline at around the same time every day. Follow the directions on your prescription label carefully, and ask your doctor or pharmacist to explain any part you do not understand. Take sertraline exactly as directed. Do not take more or less of it or take it more often than prescribed by your doctor.
To treat premenstrual dysphoric disorder (PMDD), sertraline is taken once a day, either every day of the month or on certain days of the month.
Sertraline concentrate must be diluted before use. Immediately before taking it, use the provided dropper to remove the amount of concentrate your doctor has told you to take. Mix the concentrate with 4 ounces (1/2 cup [120 milliliters]) of water, ginger ale, lemon or lime soda, lemonade, or orange juice. After mixing, the diluted solution may be hazy; this is normal. Do not mix the concentrate with any liquids other than the ones listed. Drink the diluted solution immediately.
Your doctor may start you on a low dose of sertraline and gradually increase your dose, not more than once a week.
It may take a few weeks or longer before you feel the full benefit of sertraline. Continue to take sertraline even if you feel well. Do not stop taking sertraline without talking to your doctor. If you suddenly stop taking sertraline, you may experience withdrawal symptoms such as nausea, sweating, depression, mood changes, frenzied or abnormally excited mood, irritability, anxiety, confusion, dizziness, headache, tiredness, seizures, ringing in the ears, numbness or tingling in the arms, legs, hands, or feet, difficulty falling asleep or staying asleep.
Common side effects of Sertraline are drowsiness, dyspepsia, nausea, headache, increased sweating, increased appetite, weight gain and sexual dysfunction. Rare but potentially severe adverse events include suicidal ideation and behavior, activation of mania, serotonin syndrome, discontinuation syndrome, increased risk of bleeding, seizures, acute glaucoma, hypersensitivity reactions and embryo-fetal toxicity.
A small number of children, teenagers, and young adults (up to 24 years of age) who took antidepressants (‘mood elevators’) such as sertraline during clinical studies became suicidal (thinking about harming or killing oneself or planning or trying to do so). Children, teenagers, and young adults who take antidepressants to treat depression or other mental illnesses may be more likely to become suicidal than children, teenagers, and young adults who do not take antidepressants to treat these conditions. However, experts are not sure about how great this risk is and how much it should be considered in deciding whether a child or teenager should take an antidepressant.
You should know that your mental health may change in unexpected ways when you take sertraline or other antidepressants even if you are an adult over 24 years of age. You may become suicidal, especially at the beginning of your treatment and any time that your dose is increased or decreased. You, your family, or your caregiver should call your doctor right away if you experience any of the following symptoms: new or worsening depression; thinking about harming or killing yourself, or planning or trying to do so; extreme worry; agitation; panic attacks; new or worsening anxiety; difficulty falling asleep or staying asleep; aggressive behavior; irritability; acting without thinking; severe restlessness; and frenzied abnormal excitement. Be sure that your family or caregiver knows which symptoms may be serious so they can call the doctor if you are unable to seek treatment on your own.
Your doctor will want to see you often while you are taking sertraline, especially at the beginning of your treatment. Be sure to keep all appointments for office visits with your doctor.
The doctor or pharmacist will give you the manufacturer’s patient information sheet (Medication Guide) when you begin treatment with sertraline. Read the information carefully and ask your doctor or pharmacist if you have any questions.
No matter what your age, before you take an antidepressant, you, your parent, or your caregiver should talk to your doctor about the risks and benefits of treating your condition with an antidepressant or with other treatments. You should also talk about the risks and benefits of not treating your condition. You should know that having depression or another mental illness greatly increases the risk that you will become suicidal. This risk is higher if you or anyone in your family has or has ever had bipolar disorder (mood that changes from depressed to abnormally excited) or mania (frenzied, abnormally excited mood) or has thought about or attempted suicide. Talk to your doctor about your condition, symptoms, and personal and family medical history. You and your doctor will decide what type of treatment is right for you.
How does Sertraline work?
Sertraline is an antidepressant medication within the selective serotonin reuptake inhibitors (SSRIs) class. Sertraline is an antidepressant with primarily inhibitory effects on presynaptic serotonin reuptake. This inhibition of serotonin reuptake results in an accumulation of serotonin in your brain neurons. Serotonin in the central nervous system plays a role in regulating mood, personality, and wakefulness, which is why blocking serotonin reuptake is beneficial in disorders such as major depression 3.
Sertraline also has minimal effects on norepinephrine and dopamine uptake, and research has shown that Sertraline has more dopaminergic activity than other medications in the same SSRI class. Sertraline’s mechanism of action makes it highly efficacious when used in the treatment of various psychiatric conditions 4, 5.
What is Sertraline used for?
Sertraline is a selective serotonin reuptake inhibitor (SSRI) medication that has been used to treat depression, obsessive-compulsive disorder (OCD, bothersome thoughts that won’t go away and the need to perform certain actions over and over), panic attacks (sudden, unexpected attacks of extreme fear and worry about these attacks), and major anxiety disorders including social anxiety disorder, post-trauma stress disorder (PTSD, disturbing psychological symptoms that develop after a frightening experience) and generalized anxiety disorder (GAD), panic disorder, premenstrual dysphoric disorder [PMDD] (a severe form of premenstrual syndrome [PMS] with mood swings, irritability, bloating, and breast tenderness), and social anxiety disorder (extreme fear of interacting with others or performing in front of others that interferes with normal life) 1. Sertraline is also used for headache, diabetic neuropathy and premature ejaculation. Sertraline works by blocking the reuptake of serotonin in your brain neurons, thus increasing serotonin levels in your brain which is associated with its psychiatric effects.
FDA-approved uses
- Sertraline is an antidepressant used as a first-line treatment of major depressive disorder 3
- Obsessive-compulsive disorder (OCD) 6, 7
- Panic disorder 8
- Post-traumatic stress disorder (PTSD) 9
- Premenstrual dysphoric disorder (PMDD), a severe form of premenstrual syndrome (PMS) characterized by significant mood disturbances, irritability, and other symptoms that interfere with daily life, occurring in the week or two before menstruation
- Social anxiety disorder (social phobia)
Non-FDA-approved uses
- Binge eating disorder 10
- Body dysmorphic disorder
- Bulimia nervosa 10
- Generalized anxiety disorder (GAD)
- Premature ejaculation.
Sertraline Contraindications
Sertraline is contraindicated in patients with documented hypersensitivity to the drug or its components. The coadministration of sertraline with thioridazine, pimozide, or monoamine oxidase inhibitors (MAOIs), including linezolid or methylene blue, is also contraindicated. Patients who are taking other serotonergic medications should receive education regarding the risks of coadministration with sertraline 11.
Sertraline solution is contraindicated with disulfiram as solution form contains 12% alcohol, and it may cause an alcohol-disulfiram reaction.
Sertraline therapy should not start within two weeks of discontinuing any monoamine oxidase (MAO) inhibitor such as isocarboxazid (Marplan), linezolid (Zyvox), methylene blue, rasagiline, phenelzine (Nardil), selegiline (Emsam, Zelapar), and tranylcypromine (Parnate) to prevent toxicity with serotonin syndrome 11. Wait at least 14 days after stopping an MAO inhibitor before you take sertraline.
There is a US black box warning for use in children and young adults. Use caution in patients ages 18 to 24 years old due to the risk of an increase in suicidal ideation 12.
Before taking Sertraline
You should not use sertraline if you are allergic to it, or if you also take pimozide. Do not use the liquid form of Sertraline if you take disulfiram (Antabuse).
if you have used an monoamine oxidase (MAO) inhibitor in the past 14 days, a dangerous drug interaction could occur. Monoamine oxidase (MAO) inhibitors include isocarboxazid, linezolid, methylene blue injection, phenelzine, and tranylcypromine. Wait at least 14 days after stopping an MAO inhibitor before you take sertraline.
Tell your doctor if you also take stimulant medicine, opioid medicine, herbal products, or medicine for depression, mental illness, Parkinson’s disease, migraine headaches, serious infections, or prevention of nausea and vomiting. An interaction with sertraline could cause a serious condition called serotonin syndrome.
To make sure sertraline is safe for you, tell your doctor if you have ever had:
- An allergy or sensitivity to aspirin or tartrazine (food dye) or latex (Zoloft oral solution – the dropper dispenser contains natural rubber)
- Bipolar disorder (mood disorder with mania and depression)
- Bleeding problems or if you take warfarin (Coumadin, Jantoven)
- Diabetes
- Angle-closure glaucoma. You should know that Paroxetine may cause angle-closure glaucoma, a condition where the fluid is suddenly blocked and unable to flow out of the eye causing a quick, severe increase in eye pressure which may lead to a loss of vision. Talk to your doctor about having an eye examination before you start taking Paroxetine. If you have nausea, eye pain, changes in vision, such as seeing colored rings around lights, and swelling or redness in or around the eye, see your doctor or get emergency medical treatment right away.
- Heart rhythm problems (eg, long QT syndrome)
- High blood pressure
- Hyponatremia (low sodium in the blood)
- Mania or hypomania
- Purpura (purplish or brownish-red discoloration of the skin)
- Seizures
- Sexual problems: Use with caution. May make these conditions worse.
- Kidney disease: Product labeling does not report any dose adjustment based on the patient’s renal function.
- Liver disease: Use with caution. The effects may be increased because of slower removal of the medicine from the body.
- Stroke
Some young people may have increased suicidal thoughts when first starting a medicine to treat depression. Your doctor will need to check your progress on a regular basis. Your family or caregivers should also watch for sudden changes in your behavior.
Sertraline is approved for use in children at least 6 years old, only to treat obsessive-compulsive disorder but not depression.
Allergies
Tell your doctor if you have ever had any unusual or allergic reaction to Sertraline or any other medicines. Also tell your health care professional if you have any other types of allergies, such as to foods, dyes, preservatives, or animals. For non-prescription products, read the label or package ingredients carefully.
Children
Appropriate studies have not been performed on the relationship of age to the effects of sertraline in children with depression, panic disorder, premenstrual dysphoric disorder (PMDD), posttraumatic stress disorder (PTSD), and social anxiety disorder (SAD), and in children younger than 6 years of age with obsessive-compulsive disorder. Safety and efficacy have not been established.
Elderly
Appropriate studies performed to date have not demonstrated geriatric-specific problems that would limit the usefulness of sertraline in the elderly. However, elderly patients are more likely to have hyponatremia (low sodium in the blood), age-related kidney, liver, or heart problems which may require caution and an adjustment in the dose for patients receiving sertraline.
Pregnancy
It is not known if sertraline can make it harder to get pregnant. One study found that women who take SSRIs have a slightly lower chance of getting pregnant. However, some conditions, including depression, can make it harder to get pregnant. This makes it hard to know if the medication, the condition being treated, or other factors might affect fertility.
Miscarriage is common and can occur in any pregnancy for many different reasons. Use of sertraline and the chance of miscarriage has not been well studied. One study found no differences in the chance of miscarriage in women who filled prescriptions for sertraline during the first 35 days of pregnancy and those who stopped filling prescriptions before pregnancy. Also, some conditions, including depression, may increase the chance of miscarriage. This makes it hard to know if the medication, the condition being treated, or other factors might affect the chance of miscarriage.
Every pregnancy starts out with a 3-5% chance of having a birth defect. This is called the background risk. There are reports of more than 25,000 pregnancies exposed to sertraline. Some studies have suggested an increased chance for heart defects or other birth defects. However, most studies have not found an increased chance of birth defects when sertraline is used in pregnancy. Overall, the available data does not suggest that sertraline increases the chance of birth defects above the background risk.
Some studies suggest a higher chance for pregnancy-related problems, such as preterm delivery (birth before week 37) or low birth weight (weighing less than 5 pounds, 8 ounces [2500 grams] at birth) with the use of sertraline in pregnancy. However, research has also shown that when conditions such as depression or anxiety are untreated or undertreated during pregnancy, there could be an increased chance for pregnancy complications. This makes it hard to know if it is the medication, the underlying condition, or other factors that might increase the chance for these problems.
Some, but not all, studies have suggested that when women who are pregnant take SSRIs during the second half of pregnancy, their babies might have an increased chance for a serious lung condition called persistent pulmonary hypertension (PPH). Persistent pulmonary hypertension happens in 1 or 2 out of 1,000 births. A recent report that combined results from several studies suggested the chance for persistent pulmonary hypertension might be increased if an SSRI was used during pregnancy. However, it was not clear if this was due to medication exposure or to other exposures that people who take SSRIs have in common, such as higher rates of smoking. Data from studies suggest the overall chance for persistent pulmonary hypertension when an SSRI is used in pregnancy is less than 1/100 (less than 1%).
The use of sertraline during pregnancy can cause temporary symptoms in newborns soon after birth. These symptoms are sometimes referred to as withdrawal. Symptoms can include irritability, jitteriness, tremors (shivering), constant crying, changes in sleep patterns, lower muscle tone (hypotonia), skin discoloration (cyanosis), problems with eating, trouble controlling body temperature, and problems with breathing (apnea). In most cases, these symptoms are mild and go away within a couple weeks with no treatment required. Some babies may need to stay in the nursery or neonatal intensive care unit (NICU) until the symptoms go away. Not all babies exposed to sertraline will have these symptoms. It is important that your doctor know you are taking sertraline so that if symptoms do occur, your baby can get the care that is best for them.
One study on a small number of children who were exposed to SSRIs during pregnancy reported a lower score on motor skill tests than other children. Another small study looked at behaviors in children ages 4-5 years old. This study found no difference in behavior between children who were exposed to sertraline or other SSRIs during pregnancy and those children who were not.
Breastfeeding
Sertraline gets into breastmilk in small amounts 13. Most reports show no problems for babies who are exposed to sertraline through breast milk 14. Babies who were also exposed to sertraline in the third trimester of pregnancy may have a lower chance of withdrawal after birth if they are breastfed. Most reviewers consider sertraline a preferred antidepressants during breastfeeding 15, 16, 17, 18, 19, 14, 20, 21, 22. Be sure to talk to your doctor about all your breastfeeding questions.
Drug Interactions
Although certain medicines should not be used together at all, in other cases two different medicines may be used together even if an interaction might occur. In these cases, your doctor may want to change the dose, or other precautions may be necessary. When you are taking Sertraline, it is especially important that your doctor know if you are taking any of the medicines listed below. The following interactions have been selected on the basis of their potential significance and are not necessarily all-inclusive.
Using Sertraline with any of the following medicines is not recommended. Your doctor may decide not to treat you with this medication or change some of the other medicines you take.
- Bepridil
- Bromopride
- Cisapride
- Dronedarone
- Fluconazole
- Furazolidone
- Iproniazid
- Isocarboxazid
- Ketoconazole
- Levoketoconazole
- Linezolid
- Mesoridazine
- Methylene Blue
- Metoclopramide
- Ozanimod
- Phenelzine
- Pimozide
- Piperaquine
- Posaconazole
- Procarbazine
- Rasagiline
- Safinamide
- Saquinavir
- Selegiline
- Sparfloxacin
- Terfenadine
- Thioridazine
- Toloxatone
- Tranylcypromine
- Ziprasidone
Using Sertraline with any of the following medicines is usually not recommended, but may be required in some cases. If both medicines are prescribed together, your doctor may change the dose or how often you use one or both of the medicines.
- Abciximab
- Aceclofenac
- Acemetacin
- Acenocoumarol
- Adagrasib
- Alfentanil
- Alfuzosin
- Almotriptan
- Amineptine
- Amiodarone
- Amisulpride
- Amitriptyline
- Amitriptylinoxide
- Amoxapine
- Amphetamine
- Amtolmetin Guacil
- Anagrelide
- Anileridine
- Apixaban
- Apomorphine
- Ardeparin
- Argatroban
- Aripiprazole
- Aripiprazole Lauroxil
- Arsenic Trioxide
- Asenapine
- Aspirin
- Astemizole
- Atazanavir
- Atomoxetine
- Avacopan
- Azithromycin
- Bedaquiline
- Bemiparin
- Benzhydrocodone
- Benzphetamine
- Betrixaban
- Bivalirudin
- Bromfenac
- Brompheniramine
- Plus many more not on this list.
Using Sertraline with any of the following medicines may cause an increased risk of certain side effects, but using both drugs may be the best treatment for you. If both medicines are prescribed together, your doctor may change the dose or how often you use one or both of the medicines.
- Alprazolam
- Cimetidine
- Fluphenazine
- Ginkgo
- Lamotrigine
- Mavacamten
- Rifampin
Sertraline dosage
The dose of Sertraline will be different for different patients. Follow your doctor’s orders or the directions on the label. The following information includes only the average doses of Sertraline. If your dose is different, do not change it unless your doctor tells you to do so.
The amount of medicine that you take depends on the strength of the medicine. Also, the number of doses you take each day, the time allowed between doses, and the length of time you take the medicine depend on the medical problem for which you are using the medicine.
For oral dosage forms (solution or tablets)
- For depression
- Adults: At first, 50 milligrams (mg) once a day, taken either in the morning or evening. Your doctor may adjust your dose as needed. However, the dose is usually not more than 200 mg per day.
- Children: Use and dose must be determined by your doctor.
- For obsessive-compulsive disorder (OCD)
- Adults and teenagers: At first, 50 milligrams (mg) once a day, taken either in the morning or evening. Your doctor may adjust your dose as needed. However, the dose is usually not more than 200 mg per day.
- Children 6 to 12 years of age: At first, 25 mg once a day, taken either in the morning or evening. Your doctor may adjust your dose as needed. However, the dose is usually not more than 200 mg per day.
- Children younger than 6 years of age: Use and dose must be determined by your doctor.
- For panic disorder, posttraumatic stress disorder (PTSD) or social anxiety disorder
- Adults: At first, 25 milligrams (mg) once a day, taken either in the morning or evening. Your doctor may adjust your dose as needed. However, the dose is usually not more than 200 mg per day.
- Children: Use and dose must be determined by your doctor.
- For premenstrual dysphoric disorder (PMDD)
- Adults: At first, 50 milligrams (mg) once a day throughout your menstrual cycle or just during the premenstrual time. Your doctor may adjust your dose as needed. However, the dose is usually not more than 150 mg per day throughout your menstrual cycle or 100 mg per day if you are only taking it during your premenstrual time.
- Children: Use and dose must be determined by your doctor.
Missed Dose
If you miss a dose of Sertraline, take it as soon as possible. However, if it is almost time for your next dose, skip the missed dose and go back to your regular dosing schedule. Do not double doses.
Monitoring
It is essential to monitor patients for unusual changes in behavior, anxiety, suicidality, or any other clinical signs of worsening illness. Regularly evaluate for depression and suicidality, especially when changing the dose of sertraline. Sertraline may also precipitate mania in patients at risk for bipolar disorder. Monitor for symptoms of mania in patients who are started on sertraline, especially if they have a family history of mania or bipolar disorder 23.
Monitor for abnormal bleeding, adverse effects of medication use, or withdrawal symptoms from abrupt discontinuation in patients taking sertraline. The abnormal bleeding may primarily occur if used concurrently with aspirin, non-steroidal anti-inflammatory drugs (NSAIDs), warfarin, or other anticoagulants, as sertraline may impair platelet aggregation and cause bruising, epistaxis, or hemorrhage 24.
For geriatric patients, monitor for changes in mental status, and check their sodium concentration regularly due to the risk of syndrome of inappropriate antidiuretic hormone secretion (SIADH) or hyponatremia.
Sertraline is considered safe in patients with a history of myocardial infarction, heart failure, and other cardiac conditions. However, due to the minor effect of QT prolongation, it may benefit the provider to monitor the QT interval with electrocardiograms 25, 26.
When treating pregnant women with sertraline during the third trimester, the physician should consider tapering sertraline in the third trimester by risk-benefit analysis 27, 14.
Sertraline side effects
Sertraline may cause side effects. See your doctor if any of these symptoms are severe or do not go away:
- nausea
- diarrhea
- constipation
- vomiting
- difficulty falling asleep or staying asleep
- dry mouth
- heartburn
- loss of appetite
- weight changes
- dizziness
- excessive tiredness
- headache
- nervousness
- uncontrollable shaking of a part of the body
- sexual problems in males; decreased sex drive, inability to get or keep an erection, or delayed or absent ejaculation
- sexual problems in females; decreased sex drive, or delayed orgasm or unable to have an orgasm
- excessive sweating
Some side effects can be serious. If you experience any of the following symptoms or those listed in the IMPORTANT WARNING or SPECIAL PRECAUTIONS section, see your doctor immediately:
- seizures
- abnormal bleeding or bruising
- agitation, hallucinations, fever, sweating, confusion, fast heartbeat, shivering, severe muscle stiffness or twitching, loss of coordination, nausea, vomiting, or diarrhea
- headache, weakness, unsteadiness, confusion, or memory problems
- rash
- hives
- swelling
- difficulty breathing
Sertraline may decrease appetite and cause weight loss in children. Your child’s doctor will watch his or her growth carefully. Talk to your child’s doctor if you have concerns about your child’s growth or weight while he or she is taking this medication. Talk to your child’s doctor about the risks of giving sertraline to your child.
Sertraline may cause other side effects. Call your doctor if you have any unusual problems while taking Sertraline.
Sertraline Withdrawal
Discontinuation of serotonergic antidepressants may cause adverse reactions, particularly when the discontinuation is abrupt. Symptoms include nausea, diaphoresis, dysphoric mood, irritability, agitation, vertigo, sensory disturbances (e.g., paresthesia, electric shock sensations), tremor, anxiety, confusion, cephalgia, lethargy, emotional lability, sleep disorder, hypomania, tinnitus, and seizures. Therefore, it is preferable to reduce the dosage gradually rather than stop immediately whenever possible.
Sertraline Overdose
The overdose of sertraline is generally well-tolerated. Sertraline overdose may result in serotonin syndrome, resulting in myoclonus, muscle rigidity, diaphoresis, tremor, hyperreflexia, agitated delirium, and hyperthermia. Treatment of serotonin syndrome requires discontinuing the medication and supportive care. Consider antiemetics (non-serotonergic), benzodiazepines, and standard cooling measures for symptom relief. The patient can also receive serotonin antagonists such as cyproheptadine. If severe serotonin syndrome and the patient develops muscular rigidity and hyperthermia with body temperatures higher than 41 degrees C, consider sedation, endotracheal intubation, external cooling, and neuromuscular paralysis. It is important to note that antipyretics are likely not beneficial to patients experiencing hyperthermia due to serotonin syndrome 28.
- Singh HK, Saadabadi A. Sertraline. [Updated 2023 Feb 13]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK547689[↩][↩]
- LiverTox: Clinical and Research Information on Drug-Induced Liver Injury [Internet]. Bethesda (MD): National Institute of Diabetes and Digestive and Kidney Diseases; 2012-. Sertraline. [Updated 2020 Apr 8]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK548513[↩]
- Cipriani A, La Ferla T, Furukawa TA, Signoretti A, Nakagawa A, Churchill R, McGuire H, Barbui C. Sertraline versus other antidepressive agents for depression. Cochrane Database Syst Rev. 2010 Apr 14;(4):CD006117. doi: 10.1002/14651858.CD006117.pub4[↩][↩]
- Kitaichi Y, Inoue T, Nakagawa S, Boku S, Kakuta A, Izumi T, Koyama T. Sertraline increases extracellular levels not only of serotonin, but also of dopamine in the nucleus accumbens and striatum of rats. Eur J Pharmacol. 2010 Nov 25;647(1-3):90-6. doi: 10.1016/j.ejphar.2010.08.026[↩]
- Sanchez C, Reines EH, Montgomery SA. A comparative review of escitalopram, paroxetine, and sertraline: Are they all alike? Int Clin Psychopharmacol. 2014 Jul;29(4):185-96. doi: 10.1097/YIC.0000000000000023[↩]
- Fenske JN, Schwenk TL. Obsessive compulsive disorder: diagnosis and management. Am Fam Physician. 2009 Aug 1;80(3):239-45. https://www.aafp.org/pubs/afp/issues/2009/0801/p239-s1.html[↩]
- Semenya AM, Bhatnagar P. Diagnosis and Management of Obsessive-Compulsive Disorder in the Primary Care Setting. Am Fam Physician. 2024 Oct;110(4):385-392. https://www.aafp.org/pubs/afp/issues/2024/1000/obsessive-compulsive-disorder.html[↩]
- Hobgood CD, Clayton AH. Sertraline in the treatment of panic disorder. Drugs Today (Barc). 2009 May;45(5):351-61. doi: 10.1358/dot.2009.45.5.1362066[↩]
- Buhmann CB, Andersen HS. [Diagnosing and treating post-traumatic stress disorder]. Ugeskr Laeger. 2017 Jun 12;179(24):V12160914. Danish.[↩]
- Aigner M, Treasure J, Kaye W, Kasper S; WFSBP Task Force On Eating Disorders. World Federation of Societies of Biological Psychiatry (WFSBP) guidelines for the pharmacological treatment of eating disorders. World J Biol Psychiatry. 2011 Sep;12(6):400-43. doi: 10.3109/15622975.2011.602720[↩][↩]
- Sola CL, Bostwick JM, Hart DA, Lineberry TW. Anticipating potential linezolid-SSRI interactions in the general hospital setting: an MAOI in disguise. Mayo Clin Proc. 2006 Mar;81(3):330-4. doi: 10.4065/81.3.330[↩][↩]
- DeVane CL, Liston HL, Markowitz JS. Clinical pharmacokinetics of sertraline. Clin Pharmacokinet. 2002;41(15):1247-66. doi: 10.2165/00003088-200241150-00002[↩]
- Drugs and Lactation Database (LactMed®) [Internet]. Bethesda (MD): National Institute of Child Health and Human Development; 2006-. Sertraline. [Updated 2025 Feb 15]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK501191[↩]
- Pinheiro E, Bogen DL, Hoxha D, Ciolino JD, Wisner KL. Sertraline and breastfeeding: review and meta-analysis. Arch Womens Ment Health. 2015 Apr;18(2):139-146. doi: 10.1007/s00737-015-0499-y[↩][↩][↩]
- Weissman AM, Levy BT, Hartz AJ, Bentler S, Donohue M, Ellingrod VL, Wisner KL. Pooled analysis of antidepressant levels in lactating mothers, breast milk, and nursing infants. Am J Psychiatry. 2004 Jun;161(6):1066-78. doi: 10.1176/appi.ajp.161.6.1066[↩]
- Academy of Breastfeeding Medicine Protocol Committee. ABM clinical protocol #18: use of antidepressants in nursing mothers. Breastfeed Med. 2008 Mar;3(1):44-52. doi: 10.1089/bfm.2007.9978[↩]
- Berle JO, Spigset O. Antidepressant Use During Breastfeeding. Curr Womens Health Rev. 2011 Feb;7(1):28-34. doi: 10.2174/157340411794474784[↩]
- Larsen ER, Damkier P, Pedersen LH, Fenger-Gron J, Mikkelsen RL, Nielsen RE, Linde VJ, Knudsen HE, Skaarup L, Videbech P; Danish Psychiatric Society; Danish Society of Obstetrics and Gynecology; Danish Paediatric Society; Danish Society of Clinical Pharmacology. Use of psychotropic drugs during pregnancy and breast-feeding. Acta Psychiatr Scand Suppl. 2015;(445):1-28. doi: 10.1111/acps.12479[↩]
- Orsolini L, Bellantuono C. Serotonin reuptake inhibitors and breastfeeding: a systematic review. Hum Psychopharmacol. 2015 Jan;30(1):4-20. doi: 10.1002/hup.2451[↩]
- McAllister-Williams RH, Baldwin DS, Cantwell R, Easter A, Gilvarry E, Glover V, Green L, Gregoire A, Howard LM, Jones I, Khalifeh H, Lingford-Hughes A, McDonald E, Micali N, Pariante CM, Peters L, Roberts A, Smith NC, Taylor D, Wieck A, Yates LM, Young AH; endorsed by the British Association for Psychopharmacology. British Association for Psychopharmacology consensus guidance on the use of psychotropic medication preconception, in pregnancy and postpartum 2017. J Psychopharmacol. 2017 May;31(5):519-552. doi: 10.1177/0269881117699361[↩]
- Molenaar NM, Kamperman AM, Boyce P, Bergink V. Guidelines on treatment of perinatal depression with antidepressants: An international review. Aust N Z J Psychiatry. 2018 Apr;52(4):320-327. doi: 10.1177/0004867418762057[↩]
- Uguz F. A New Safety Scoring System for the Use of Psychotropic Drugs During Lactation. Am J Ther. 2021 Jan-Feb 01;28(1):e118-e126. doi: 10.1097/MJT.0000000000000909[↩]
- Leverich GS, Altshuler LL, Frye MA, Suppes T, McElroy SL, Keck PE Jr, Kupka RW, Denicoff KD, Nolen WA, Grunze H, Martinez MI, Post RM. Risk of switch in mood polarity to hypomania or mania in patients with bipolar depression during acute and continuation trials of venlafaxine, sertraline, and bupropion as adjuncts to mood stabilizers. Am J Psychiatry. 2006 Feb;163(2):232-9. doi: 10.1176/appi.ajp.163.2.232[↩]
- Andrade C, Sandarsh S, Chethan KB, Nagesh KS. Serotonin reuptake inhibitor antidepressants and abnormal bleeding: a review for clinicians and a reconsideration of mechanisms. J Clin Psychiatry. 2010 Dec;71(12):1565-75. doi: 10.4088/JCP.09r05786blu[↩]
- Glassman AH, O’Connor CM, Califf RM, Swedberg K, Schwartz P, Bigger JT Jr, Krishnan KR, van Zyl LT, Swenson JR, Finkel MS, Landau C, Shapiro PA, Pepine CJ, Mardekian J, Harrison WM, Barton D, Mclvor M; Sertraline Antidepressant Heart Attack Randomized Trial (SADHEART) Group. Sertraline treatment of major depression in patients with acute MI or unstable angina. JAMA. 2002 Aug 14;288(6):701-9. doi: 10.1001/jama.288.6.701. Erratum in: JAMA 2002 Oct 9;288(14):1720.[↩]
- O’Connor CM, Jiang W, Kuchibhatla M, Silva SG, Cuffe MS, Callwood DD, Zakhary B, Stough WG, Arias RM, Rivelli SK, Krishnan R; SADHART-CHF Investigators. Safety and efficacy of sertraline for depression in patients with heart failure: results of the SADHART-CHF (Sertraline Against Depression and Heart Disease in Chronic Heart Failure) trial. J Am Coll Cardiol. 2010 Aug 24;56(9):692-9. doi: 10.1016/j.jacc.2010.03.068[↩]
- Paulzen M, Goecke TW, Stickeler E, Gründer G, Schoretsanitis G. Sertraline in pregnancy – Therapeutic drug monitoring in maternal blood, amniotic fluid and cord blood. J Affect Disord. 2017 Apr 1;212:1-6. doi: 10.1016/j.jad.2017.01.019[↩]
- Wang RZ, Vashistha V, Kaur S, Houchens NW. Serotonin syndrome: Preventing, recognizing, and treating it. Cleve Clin J Med. 2016 Nov;83(11):810-817. doi: 10.3949/ccjm.83a.15129[↩]



{kind=link}