Contents
What is SHBG
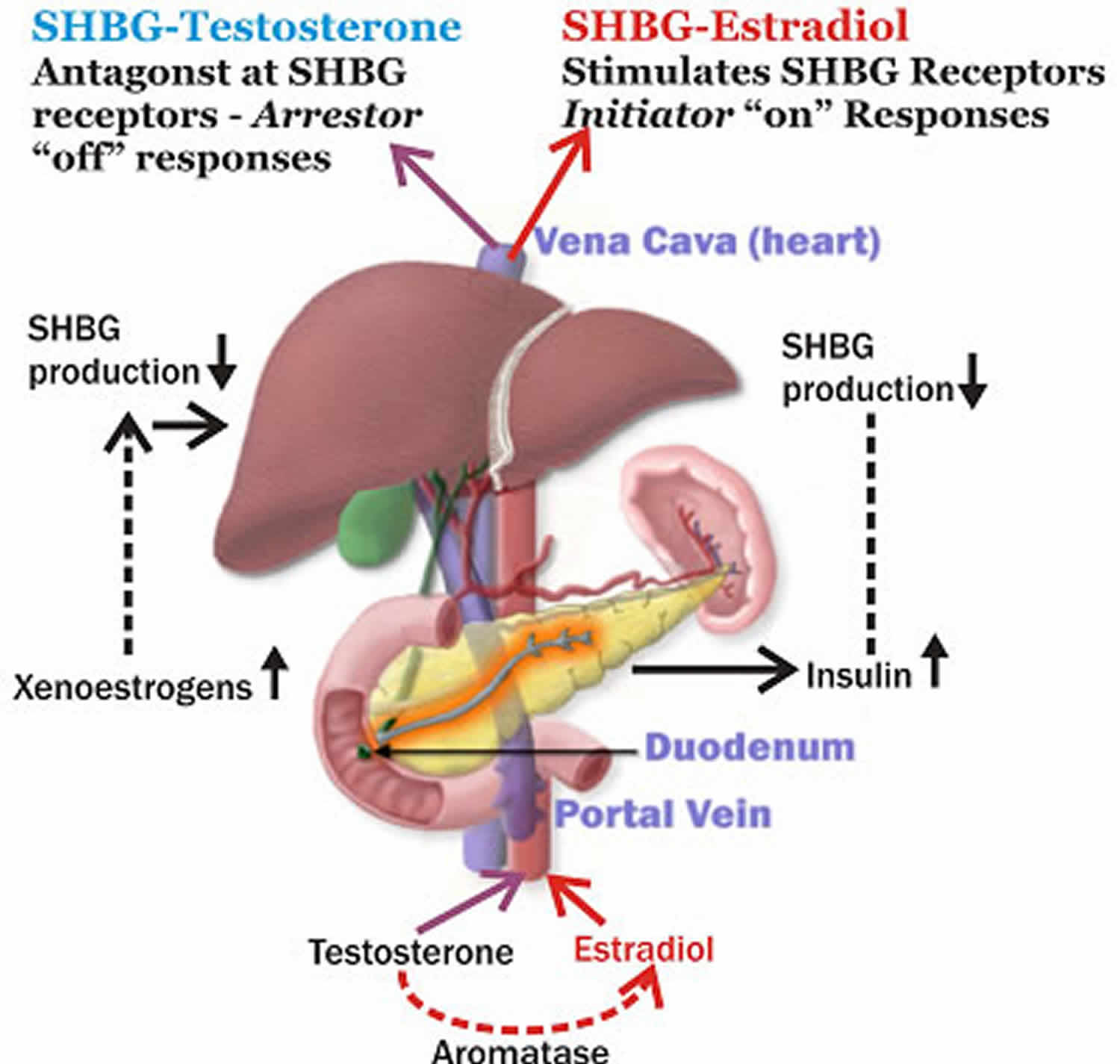
SHBG is short for sex hormone binding globulin is also called Testosterone-Estradiol Binding Globulin, SHBG is a glycoprotein that is produced by the liver and binds tightly to the hormones testosterone, dihydrotestosterone (DHT), and estradiol (an estrogen). In this bound state, SHBG transports these hormones in the blood as biologically inactive forms. SHBG controls how much of these hormones are delivered to your body’s tissues 1. Human SHBG binds sex hormones with high affinity dihydrotestosterone (DHT) > testosterone > estrone/estradiol as well as drugs such as levonorgestrel and fluoxymesterone 1. Changes in SHBG levels can affect the amount of hormone that is available to be used by the body’s tissues.
Although each monomeric subunit contains 1 steroid binding site, the dimer tends to bind only a single sex-steroid molecule. The main function of SHBG is sex-steroid transport within the blood stream and to extravascular target tissues. SHBG also plays a key role in regulating bioavailable sex-steroid concentrations through competition of sex steroids for available binding sites and fluctuations in SHBG concentrations. Because of the higher affinity of SHBG for dihydrotestosterone (DHT) and testosterone, compared to estradiol, SHBG also has profound effects on the balance between bioavailable androgens and estrogens. Increased SHBG levels may be associated with symptoms and signs of hypogonadism in men, while decreased levels can result in androgenization in women.
SHBG binds testosterone with high affinity (~1 nmol/L) and much of the SHBG-binding sites in adult male serum are occupied by testosterone such that the level of SHBG is a major determinant of the total testosterone level in adult men. Eugonadal adult men with low SHBG levels have low total testosterone levels, while men with high SHBG levels have higher testosterone levels. Obesity and hyperthyroidism, respectively, are examples of these effects. SHBG and testosterone are also related in newborn boys 2 during minipuberty but not in prepubertal boys with much lower testosterone levels in whom only a small portion of the SHBG in the plasma is occupied by testosterone.
Sex hormone-binding globulin (SHBG) is a 90-100 KDa homodimeric glycoprotein that is encoded by a single gene on the short arm of chromosome 17 3. Many studies have linked lower circulating levels of SHBG to obesity, type 2 diabetes, metabolic syndrome, non-alcoholic fatty liver disease, polycystic ovary syndrome (PCOS) and early puberty 3.
Circulating SHBG is produced primarily by hepatocytes, however, the gene is also expressed in the brain, uterus, prostate, breast, ovary, and testis 4, as well as in certain ovarian and prostate cancers.
In men, about 45% to 65% of testosterone in blood is normally bound to SHBG, with the remainder weakly and reversibly bound to albumin (the main protein in the blood). Only about 2% to 3% of testosterone is immediately available to the tissues as free testosterone, but testosterone that is weakly bound to albumin is also bioavailable and can be readily taken up by the body’s tissues.
A slightly increased amount of testosterone (66% to 78%) is bound to SHBG in the blood in women, compared to men. In women, SHBG plays an integral role in regulating the levels of bioavailable male sex hormones (androgens) and estrogens circulating throughout the body. SHBG has a higher affinity for the androgens testosterone and dihydrotestosterone (DHT) and so, in the setting of low SHBG, women may have signs and symptoms related to androgen excess.
A total testosterone test does not distinguish between bound and unbound testosterone but determines the overall quantity of testosterone. In many cases, this is sufficient to evaluate excess or deficient testosterone production. However, if a person’s SHBG level is not normal, then the total testosterone may not be an accurate representation of the amount of testosterone that is available to the person’s tissues. An SHBG test may be performed when a person’s signs and symptoms do not correlate with the results of a total testosterone test.
Metabolic clearance of SHBG is biphasic, with a fast initial distribution from vascular compartment into extracellular space (half-life of a few hours), followed by a slower degradation phase (half-life of several days).
SHBG levels in prepubertal children are higher than in adults. With the increase in fat mass during early puberty they begin to fall, a process that accelerates as androgen levels rise. Men have lower levels compared with women and nutritional status is inversely correlated with SHBG levels throughout life, possibly mediated by insulin resistance. Insulin resistance, even without obesity, results in lower SHBG levels. This is associated with increased intra-abdominal fat deposition and an unfavorable cardiovascular risk profile. In postmenopausal women, it may also predict the future development of type 2 diabetes mellitus. Androgens and norethisterone-related synthetic progesterones also decrease SHBG in women.
Endogenous or exogenous thyroid hormones or estrogens increase SHBG levels. In men, there is also an age-related gradual rise, possibly secondary to the mild age-related fall in testosterone production. This process can result in bioavailable testosterone levels that are much lower than would be expected based on total testosterone measurements alone.
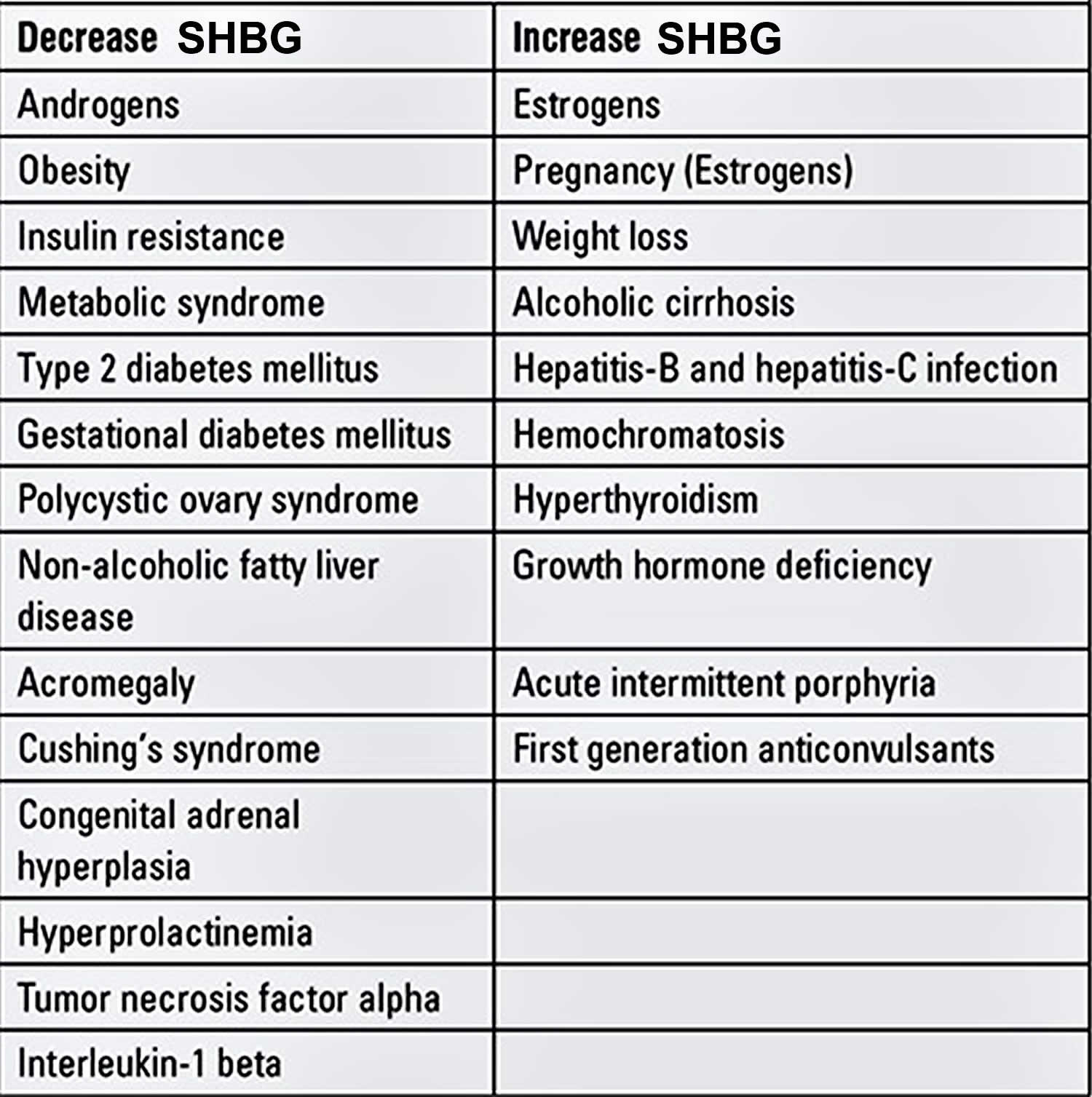
Table 1. Factors that influence the level of sex hormone-binding globulin in blood
What is a Free Androgen Index?
The Free Androgen Index (FAI) is a calculation that provides information on the amount of testosterone that is not bound to SHBG and is available for the body to use (bioavailable). The results of a total testosterone test and the SHBG are used for the calculation: Free Androgen Index = Total Testosterone / SHBG. The Free Androgen Index (FAI) may be useful in cases where tests for free testosterone or bioavailable testosterone are not available. It offers a reasonable substitute for estimating the concentration of bioavailable testosterone, when SHBG is normal.
SHBG test
SHBG test measures the levels of SHBG in your blood and is most often used to help evaluate for testosterone deficiency or excess. The sex hormone binding globulin (SHBG) test may be used to help evaluate men for low testosterone and women for excess testosterone production. It may be ordered in conjunction with other tests to evaluate the status of a person’s sex hormones.
Testing for albumin level and one or more other sex hormones, such as prolactin, estradiol, and LH (luteinizing hormone), may also be performed to evaluate a person’s existing balance of hormones.
- SHBG test is used to diagnose and follow-up of women with symptoms or signs of androgen excess (e.g., polycystic ovarian syndrome (PCOS) and idiopathic hirsutism).
- SHBG test is an adjunct in monitoring sex-steroid and anti-androgen therapy.
- SHBG test is an adjunct in the diagnosis of disorders of puberty.
- SHBG test is an adjunct adjunct in the diagnosis and follow-up of anorexia nervosa.
- SHBG test is an adjunct adjunct in the diagnosis of thyrotoxicosis (tissue marker of thyroid hormone excess).
- SHBG test is a possible adjunct in diagnosis and follow-up of insulin resistance and cardiovascular and type 2 diabetes risk assessment, particularly in women.
SHBG is a protein made by the liver and attaches itself to sex hormones found in both men and women. These hormones are:
- Testosterone, the main sex hormone in men
- Dihydrotestosterone (DHT), another male sex hormone
- Estradiol, a form of estrogen, the main sex hormone in women
SHBG controls how much of these hormones are delivered to the body’s tissues. Although SHBG attaches to all three of these hormones, an SHBG test is mostly used to look at testosterone. SHBG levels can show if there is too much or too little testosterone being used by the body.
Currently, the SHBG test is not performed frequently or routinely. In many cases, health practitioners feel that the total testosterone, and perhaps free testosterone (as measured by a method called equilibrium dialysis), provides sufficient information. SHBG is ordered primarily when the total testosterone results do not seem to be consistent with clinical signs and symptoms, such as infertility, decreased sex drive, and erectile dysfunction in men or infertility, irregular menstrual periods, and excess facial and body hair in women.
In laboratories without access to bioavailable testosterone or equilibrium dialysis-based “true” free testosterone assays, sex hormone-binding globulin measurement is crucial in cases when assessment of the free testosterone fraction (also known as free androgen index or calculated free testosterone) is required. Both bioavailable testosterone (Testosterone, Total and Bioavailable, Serum) and free testosterone (Testosterone, Total and Free, Serum) measurements are available. Free testosterone is measured by equilibrium dialysis, obviating the need for sex hormone-binding globulin measurements to calculate free androgen fractions.
Why do I need an SHBG blood test?
You may need SHBG test if you have symptoms of abnormal testosterone levels, especially if a total testosterone test can’t explain your symptoms. For men, SHBG test is mostly ordered if there are symptoms of low testosterone levels. For women, SHBG test is mostly ordered if there are symptoms of high testosterone levels.
SHBG in men
SHBG and total testosterone levels may be ordered for an adult male to help determine the cause of infertility, a decreased sex drive, or erectile dysfunction. Measurement of SHBG in addition to testosterone is especially helpful when total testosterone results are inconsistent with clinical signs.
Measurement of total testosterone in the blood does not distinguish between bound and unbound (bioavailable) testosterone but, as the name implies, determines the overall quantity of testosterone in the blood. In many cases, this is sufficient to evaluate excessive or deficient testosterone production. However, if a person’s SHBG level is not normal, then the total testosterone may not be an accurate representation of the amount of testosterone that is available to the body’s tissues.
Measurement of SHBG helps health practitioners assess bioavailable testosterone with a simple total testosterone measurement. Increased SHBG in men may be associated with symptoms of low testosterone levels (hypogonadism) because less testosterone is available to the body’s tissues.
The Endocrine Society professional guidelines recommend measuring total testosterone in the initial screen for testosterone deficiency. If abnormal, the test is repeated on another day. If repeat results are low-normal and/or if SHBG is abnormal, they recommend one of the following:
- Measure bioavailable testosterone (using ammonium sulfate precipitation or SHBG)
- Calculate free testosterone from total testosterone and SHBG
- Measure free testosterone (using a method called equilibrium dialysis)
SHBG in women
In women, small amounts of testosterone are produced by the ovaries and adrenal glands. Even slight increases in testosterone production can disrupt the balance of hormones and cause symptoms such as irregular or missed menstrual periods, infertility, acne, and excess facial and body hair (hirsutism). These signs and symptoms and others are often seen with polycystic ovary syndrome (PCOS), a condition characterized by an excess production of male sex hormones (androgens). SHBG and testosterone testing may be useful in helping to detect and evaluate excess testosterone production and/or decreased SHBG concentrations and in evaluating women suspected of having PCOS.
SHBG levels
SHBG levels are normally high in children of both sexes, so the SHBG test is almost always used for adults.
After puberty, SHBG levels decrease more rapidly in males than in females. Levels are normally stable in adults and then begin to increase in the elderly male at the same time that total testosterone levels begin to decrease. In postmenopausal women, SHBG, testosterone, and estrogen concentrations decrease as hormone production by the ovaries tapers off.
Recent studies have identified that there may be a link between SHBG levels and insulin resistance in type 2 diabetes. It has been suggested that SHBG may have a causal role in the risk of type 2 diabetes since Mendelian randomization studies have reported that carrying specific SHBG single-nucleotide polymorphisms affects the risk of type 2 diabetes 5. Carriers of rs6259 polymorphism were shown to have higher SHBG levels and a lower risk of type 2 diabetes, and rs6257 single-nucleotide polymorphism carriers were reported to have lower SHBG levels and higher risk of type 2 diabetes 6. In another larger study including 86138 adults, presence of the rs1799941 SNP was associated with increased SHBG concentrations and reduced risk of type 2 diabetes after correction for age, sex, and BMI 5. In a recent study, Wang et al 7 showed that circulating SHBG levels were predictive for future insulin resistance in healthy young Finnish adults, whereas Mendelian randomization suggested minor, if any, causal effects.
CHILDREN
Males
| Tanner Stages* | Mean Age | Reference Range (nmol/L) |
| Stage I | 7.1 | 31-167 |
| Stage II | 11.5 | 49-179 |
| Stage III | 13.6 | 5.8-182 |
| Stage IV | 15.1 | 14-98 |
| Stage V | 18.0 | 10-57 |
Footnote: *Puberty onset (transition from Tanner stage I to Tanner stage II) occurs for boys at a median age of 11.5 (+/-2) years. For boys, there is no definite proven relationship between puberty onset and body weight or ethnic origin. Progression through Tanner stages is variable. Tanner stage V (young adult) should be reached by age 18.
Females
| Tanner Stages* | Mean Age | Reference Range (nmol/L) |
| Stage I | 7.1 | 43-197 |
| Stage II | 10.5 | 7.7-119 |
| Stage III | 11.6 | 31-191 |
| Stage IV | 12.3 | 31-166 |
| Stage V | 14.5 | 18-144 |
Footnote: *Puberty onset (transition from Tanner stage I to Tanner stage II) occurs for girls at a median age of 10.5 (+/-2) years. There is evidence that it may occur up to 1 year earlier in obese girls and in African American girls. Progression through Tanner stages is variable. Tanner stage V (young adult) should be reached by age 18.
ADULTS
- Males: 10-57 nmol/L
- Females (non-pregnant): 18-144 nmol/L
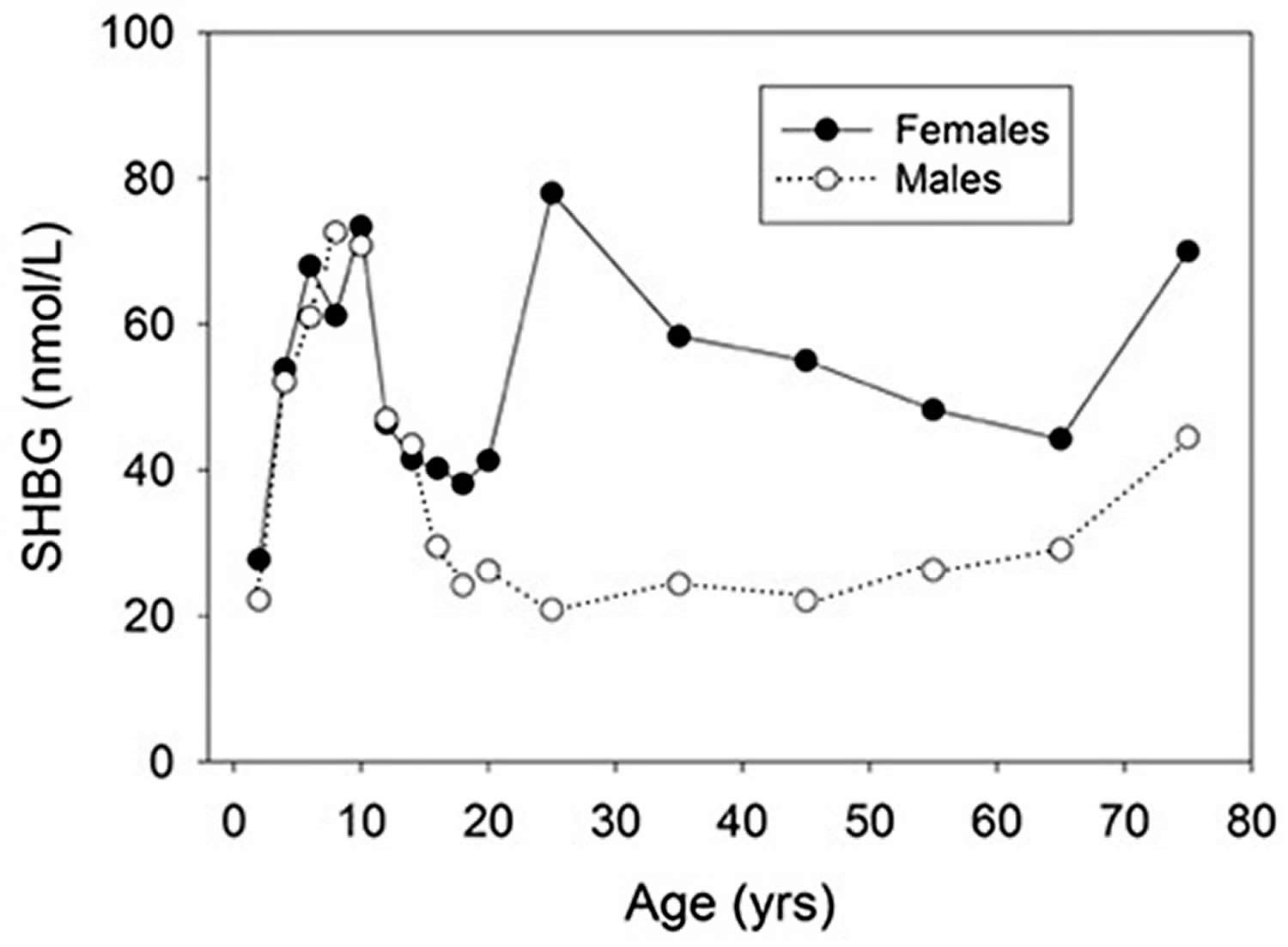
SHBG levels chart
Figure 1. SHBG levels chart (sex hormone-binding globulin levels from birth to old age in males and females)
High SHBG
A high SHBG level means the sex hormone binding globulin protein is attaching itself to too much testosterone. So less of the free testosterone hormone is available, and your tissues may be not be getting enough testosterone.
Increased SHBG levels may be seen in:
- Liver disease
- Hyperthyroidism, a condition in which your body makes too much thyroid hormone
- Eating disorders (anorexia nervosa)
- Corticosteroids or estrogen use (hormone replacement therapy and oral contraceptives)
- Decreased sex hormone production (hypogonadism)
- Pregnancy
- For men, it can mean a problem with the testicles or pituitary gland. The pituitary gland is located beneath the brain and controls many body functions.
- For women, it can mean problem with the pituitary gland, or Addison disease. Addison disease is a disorder in which the adrenal glands are not able to make enough of certain hormones.
Your health practitioners may order additional tests such as total testosterone or estrogen tests to help make a diagnosis. If you have questions about your results, talk to your doctor.
High SHBG symptoms
Symptoms of low testosterone levels in men include:
- Low sex drive
- Difficulty getting an erection
- Fertility problems
High SHBG treatment
Treating an elevated SHBG has more to do with finding and treating the underlying cause of the elevation rather than treating the elevated SHBG itself.
Adult SHBG levels in boys with signs of precocious puberty support that the condition is testosterone driven, rather than representing premature adrenarche.
Patients with anorexia nervosa have high SHBG levels. With successful treatment, levels start to fall as nutritional status improves. Normalization of SHBG precedes, and may be predictive of, future normalization of reproductive function.
SHBG is also produced by placental tissue and therefore values will be elevated during pregnancy. Reference ranges for pregnant females have not been established.
A genetic variant of SHBG (Asp327->Asn) introduces an additional glycosylation site in 10% to 20% of the population, resulting in significantly slower degradation. These individuals tend to have higher SHBG levels for any given level of other factors influencing SHBG.
There are several things you should consider doing:
- 1. Check your Estrogen and Progesterone Levels.
The ratio of these 2 hormones is more important than the numbers themselves.
Check the levels in the middle of your cycle (2 weeks after your last period) for the best results.
If the ratio of estrogen:progesterone is >10:1, you have estrogen dominance that needs to be addressed.
- 2. Check Your Thyroid Levels.
If your estrogen level is normal, then it is highly likely that your thyroid is the culprit of your elevated SHBG. Thyrotoxicosis (hyperthyroidism) increases SHBG levels.
Check a complete thyroid panel, especially free T3 and free T4.
If these are elevated and you are on thyroid medication, you may need to lower your dose or even change your thyroid medication.
If you aren’t on thyroid medication, you need to have more testing done ASAP to find the cause of your elevated thyroid (most likely Grave’s Disease).
In situations when assessment of true functional thyroid status may be difficult (e.g, patients receiving amiodarone treatment, individuals with thyroid hormone transport-protein abnormalities, patients with suspected thyroid hormone resistance or suspected inappropriate thyroid-stimulating hormone [TSH] secretion such as a TSH-secreting pituitary adenoma), an elevated SHBG level suggests tissue thyrotoxicosis, while a normal level indicates euthyroidism or near-euthyroidism. In patients with gradual worsening of thyrotoxicosis (e.g, toxic nodular goiter), serial SHBG measurement, in addition to clinical assessment, thyroid hormone, and TSH measurement, may assist in the timing of treatment decisions. Similarly, SHBG measurement may be of value in fine-tuning suppressive TSH therapy for patients with nodular thyroid disease or treated thyroid cancer. Results are not definitive in the short-term in patients receiving drugs that displace total thyroxine (T4) from albumin.
- 3. Stop Smoking!
- 4. If you are on oral birth control pills, consider using another form of birth control –
- 5. Work on Stress Management
Low SHBG
If your results show your SHBG levels are too low, it may mean the sex hormone binding globulin protein is not attaching itself to enough testosterone. This allows more unattached testosterone to be available in your system. It may cause too much testosterone to go to your body’s tissues.
If your SHBG levels are too low, it can be a sign of:
- Hypothyroidism, a condition in which your body doesn’t make enough thyroid hormones
- Type 2 diabetes
- Overuse of androgen (steroid) medications
- Obesity
- Cushing’s syndrome, a condition in which your body makes too much of a hormone called cortisol
- For men, it can mean cancer of the testicles or adrenal glands. Adrenal glands are located above the kidneys and help control heart rate, blood pressure, and other bodily functions.
- For women, it can mean polycystic ovary syndrome (PCOS). PCOS is a common hormone disorder affecting childbearing women. Polycystic ovary syndrome is one of the leading causes of female infertility.
SHBG levels decrease with increasing obesity 9 and increase with weight loss 10. SHBG is reduced in type 2 diabetes mellitus and the strength of the association is reduced, but not eliminated, after adjustment for age and body mass index (BMI) 11. Notably, a low level of SHBG is a biomarker for the future development of the metabolic syndrome 12, gestational diabetes 13, and type 2 diabetes 6.
In men, low serum SHBG levels are associated with insulin resistance 14, obesity 15, non-alcoholic fatty liver disease (NAFLD) 16, type 2 diabetes 17, and cardiovascular disease 18.
Your health practitioners may order additional tests such as total testosterone or estrogen tests to help make a diagnosis. If you have questions about your results, talk to your doctor.
Low SHBG symptoms
Symptoms of high testosterone levels in women include:
- Excess body and facial hair growth
- Deepening of voice
- Menstrual irregularities
- Acne
- Weight gain
- Fertility problems
How to increase SHBG
Treating of low SHBG has more to do with finding and treating the underlying cause of the low SHBG rather than treating the low SHBG itself.
Many conditions of mild-to-moderate androgen excess in women, particularly polycystic ovarian syndrome (PCOS), are associated with low sex hormone-binding globulin (SHBG) levels. Most of these women are also insulin resistant and many are obese. A defect in SHBG production could lead to bioavailable androgen excess, in turn causing insulin resistance that depresses SHBG levels further. There are rare cases of SHBG mutations that clearly follow this pattern. SHBG levels are typically very low in these individuals. However, in most patients, SHBG levels are mildly depressed or even within the lower part of the normal range. In these patients, the primary problem may be androgen overproduction, insulin resistance, or both. A definitive cause cannot be usually established. Any therapy that either increases SHBG levels (e.g, estrogens or weight loss), reduces bioactivity of androgens (e.g, androgen receptor antagonists, alpha-reductase inhibitors), or reduces insulin resistance (e.g, weight loss, metformin, peroxisome proliferator-activated receptor [PPAR] gamma agonists), can be effective. Improvement is usually associated with a rise in SHBG levels, but bioavailable or free testosterone levels should also be monitored.
The primary method of monitoring sex-steroid or antiandrogen therapy is direct measurement of the relevant sex-steroids and gonadotropins. However, for many synthetic androgens and estrogens (eg, ethinyl-estradiol) clinical assays are not available. In those instances, rises in SHBG levels indicate successful anti-androgen or estrogen therapy, while falls indicate successful androgen treatment.
In patients with known insulin resistance, “metabolic syndrome,” or high risk of type 2 diabetes (e.g, women with a history of gestational diabetes), low SHBG levels may predict progressive insulin resistance, cardiovascular complications, and progression to type 2 diabetes. An increase in SHBG levels may indicate successful therapeutic intervention.
If you have a low SHBG, you should consider the following things:
1. Check a complete thyroid panel
- TSH
- free T4
- free T3
- reverse T3
- TPO antibodies
- thyroglobulin antibodies
Compare these tests with their optimal levels to determine if you have a thyroid issue.
If your thyroid function is low, it is probably affecting your SHBG level and you will need to consider taking a thyroid medication and doing other things to help boost your thyroid function.
2. Check your estrogen/progesterone ratio if you are menopausal
After menopause, your estrogen levels will drop which can drop your SHBG level.
If that is the case in your situation, you might need to consider bioidentical hormone replacement therapy.
3. Check your free testosterone level
If your SHBG level is low, there will be less of it to bind to testosterone, so it may cause your free testosterone level to rise.
This can usually be alleviated by maximizing your thyroid medication which will raise your SHBG level.
- Transport of steroid hormones: binding of 21 endogenous steroids to both testosterone-binding globulin and corticosteroid-binding globulin in human plasma. Dunn JF, Nisula BC, Rodbard D. J Clin Endocrinol Metab. 1981 Jul; 53(1):58-68.[↩][↩]
- Ronde W, Schouw YT, Pierik FH, Pols HA, Muller M, Grobbee DE, Gooren LJ, Weber RF, Jong FH. Serum levels of sex hormone-binding globulin (SHBG) are not associated with lower levels of non-SHBG-bound testosterone in male newborns and healthy adult men. Clinl Endocrinol (Oxf) 2005;62:498–503.[↩]
- Aydın B, Winters SJ. Sex Hormone-Binding Globulin in Children and Adolescents. J Clin Res Pediatr Endocrinol. 2016;8(1):1-12. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4805039/[↩][↩]
- Sex hormone-binding globulin: gene organization and structure/function analyses. Hammond GL, Bocchinfuso WP. Horm Res. 1996; 45(3-5):197-201[↩]
- Perry JR, Weedon MN, Langenberg C, Jackson AU, Lyssenko V, Sparsø T, Thorleifsson G, Grallert H, Ferrucci L, Maggio M, Paolisso G, Walker M, Palmer CN, Payne F, Young E, Herder C, Narisu N, Morken MA, Bonnycastle LL, Owen KR, Shields B, et al. Genetic evidence that raised sex hormone binding globulin (SHBG) levels reduce the risk of type 2 diabetes. Hum Mol Genet. 2010;19:535–544.[↩][↩]
- Ding EL, Song Y, Manson JE, Hunter DJ, Lee CC, Rifai N, Buring JE, Gaziano JM, Liu S. Sex hormone-binding globulin and risk of type 2 diabetes in women and men. N Engl J Med. 2009;361:1152–1163[↩][↩]
- Wang Q, Kangas AJ, Soininen P, Tiainen M, Tynkkynen T, Puukka K, Ruokonen A, Viikari J, Kähönen M, Lehtimäki T, Salomaa V, Perola M, Davey Smith G, Raitakari OT, Järvelin MR, Würtz P, Kettunen J, Ala-Korpela M. Sex hormone-binding globulin associations with circulating lipids and metabolites and the risk for type 2 diabetes: observational and causal effect estimates. Int J Epidemiol. 2015;44:623–637.[↩]
- Elmlinger MW, Kuhnel W, Wormstall H, Döller PC. Reference intervals for testosterone, androstenedione and SHBG levels in healthy females and males from birth until old age. Clin Lab. 2005;51:625–632[↩]
- Glass AR, Swerdloff RS, Bray GA, Dahms WT, Atkinson RL. Low serum testosterone and sex-hormone-binding-globulin in massively obese men. J Clin Endocrinol Metab. 1977;45:1211–1219.[↩]
- Guzick DS, Wing R, Smith D, Berga SL, Winters SJ. Endocrine consequences of weight loss in obese, hyperandrogenic, anovulatory women. Fertil Steril. 1994;61:598–604[↩]
- Barrett-Connor E, Khaw KT, Yen SS. Endogenous sex hormone levels in older adult men with diabetes mellitus. Am J Epidemiol. 1990;132:895–901[↩]
- Brand JS, Grobbee DE, Emmelot-Vonk MH. Testosterone, sex hormone-binding globulin and the metabolic syndrome: a systematic review and meta-analysis of observational studies. Int J Epidemiol. 2011;40:189–207[↩]
- Veltman-Verhulst SM, Haeften TW, van, Eijkemans MJ, Valk HW, de, Fauser BC, Goverde AJ. Sex hormone-binding globulin concentrations before conception as a predictor for gestational diabetes in women with polycystic ovary syndrome. Hum Reprod. 2010;25:3123–3128[↩]
- Wallace IR, McKinley MC, Bell PM, Hunter SJ. Sex hormone binding globulin and insulin resistance. Clin Endocrinol (Oxf). 2013;78(3):321–9. Epub 2012/11/06. doi: 10.1111/cen.12086[↩]
- Caldwell JD, Jirikowski GF. Sex hormone binding globulin and aging. Horm Metab Res. 2009;41(3):173–82. Epub 2008/10/29. doi: 10.1055/s-0028-1093351[↩]
- Flechtner-Mors M, Schick A, Oeztuerk S, Haenle MM, Wilhelm M, Koenig W, et al. Associations of fatty liver disease and other factors affecting serum SHBG concentrations: a population based study on 1657 subjects. Horm Metab Res. 2014;46(4):287–93. Epub 2013/09/04. doi: 10.1055/s-0033-1354369[↩]
- Gyawali P, Martin SA, Heilbronn LK, Vincent AD, Taylor AW, Adams RJT, et al. The role of sex hormone-binding globulin (SHBG), testosterone, and other sex steroids, on the development of type 2 diabetes in a cohort of community-dwelling middle-aged to elderly men. Acta Diabetol. 2018. Epub 2018/05/31. doi: 10.1007/s00592-018-1163-6[↩]
- Simo R, Saez-Lopez C, Barbosa-Desongles A, Hernandez C, Selva DM. Novel insights in SHBG regulation and clinical implications. Trends Endocrinol Metab. 2015;26(7):376–83. Epub 2015/06/06. doi: 10.1016/j.tem.2015.05.001[↩]





{kind=link}