Contents
- What is shoulder arthroscopy
- Shoulder arthroscopy anatomy
- Shoulder arthroscopy operation
- Shoulder arthroscopy rotator cuff repair
- Shoulder arthroscopic shoulder stabilization
- Shoulder arthroscopy for subacromial decompression
- Shoulder arthroscopy complications
- Shoulder arthroscopy recovery
- Shoulder arthroscopy recovery time
- Shoulder arthroscopy rehab protocol
- Shoulder arthroscopy long-term outcomes
What is shoulder arthroscopy
Shoulder arthroscopy is surgery that uses a small camera called an arthroscope to examine or repair the tissues inside or around your shoulder joint.
Shoulder arthroscopy only requires small cuts to insert the instruments. For this reason it is often referred to as ‘key hole surgery’.
Your doctor may recommend shoulder arthroscopy if you have a painful condition that does not respond to nonsurgical treatment. Nonsurgical treatment includes rest, physical therapy, and medications or injections that can reduce inflammation. Inflammation is one of your body’s normal reactions to injury or disease. In an injured or diseased shoulder joint, inflammation causes swelling, pain, and stiffness.
Injury, overuse, and age-related wear and tear are responsible for most shoulder problems. Shoulder arthroscopy may relieve painful symptoms of many problems that damage the rotator cuff tendons, labrum, articular cartilage, and other soft tissues surrounding the joint.
Using arthroscopic shoulder surgery, a surgeon can perform a number of procedures, including:
- Rotator cuff repair.
- Shoulder stabilization or repair for recurrent shoulder dislocation.
- Capsular Release.
- Acromioplasty (subacromial Decompression).
- Bone spur removal.
- Removal or repair of the labrum
- Repair of ligaments
- Removal of inflamed tissue or loose cartilage.
Less common procedures such as nerve release, fracture repair, and cyst excision can also be performed using an arthroscope. Some surgical procedures, such as shoulder replacement, still require open surgery with more extensive incisions.
You may benefit from a shoulder arthroscopy surgery, if:
- Have pain when lifting arms above shoulder height or lying on your side.
- Have damaged your rotator cuff.
- Your shoulder has dislocated multiple times.
The following conditions may be helped with a shoulder arthroscopy:
- Certain types of shoulder instability
- Rotator cuff tears
- Bursitis or Impingement syndrome (arthroscopic subacromial decompression)
- Biceps tendonitis
- Frozen shoulder
Surgery may be necessary if your symptoms are severe. There are however some alternatives to surgery which may help with the symptoms of your shoulder problem. These include:
- Pain killers – such as paracetamol.
- Anti-inflammatories – these medications can be harmful if used long term and you should discuss the use of these medications with your doctor before
starting. - Physiotherapy – exercises to improve muscle strength may help with mobility and reduce pain.
- Cortisone injection – an injection into the shoulder may help to relieve your pain. This may be short term.
Shoulder arthroscopy benefits
A shoulder arthroscopy is usually a very successful operation and can help to:
- Reduce pain
- Improve mobility: You should be able to move your arm more freely after your operation.
- Improve your quality of life: With less pain and better mobility, you be able to carry out your daily tasks more easily.
Before the shoulder arthroscopy operation
Preadmission clinic
Before your shoulder arthroscopy procedure, you will be seen at the preadmission clinic to make sure you are fit for the operation and all the necessary tests are performed in preparation for the operation.
During the visit, you will be seen by a:
- Doctor
- Nurse
- Anesthetist (if necessary)
Tests:
Tests that may be ordered for you may include:
- Shoulder x-ray
- Shoulder ultrasound
- Shoulder MRI
- Blood tests
- ECG
Preparing your skin:
- Your skin should not have any infections or irritations before surgery. If either is present, contact your orthopaedic surgeon for a program to improve your skin before surgery.
Medications:
- Our doctors can advise you which medications to stop, and which medications to continue prior to surgery.
Shoulder arthroscopy anatomy
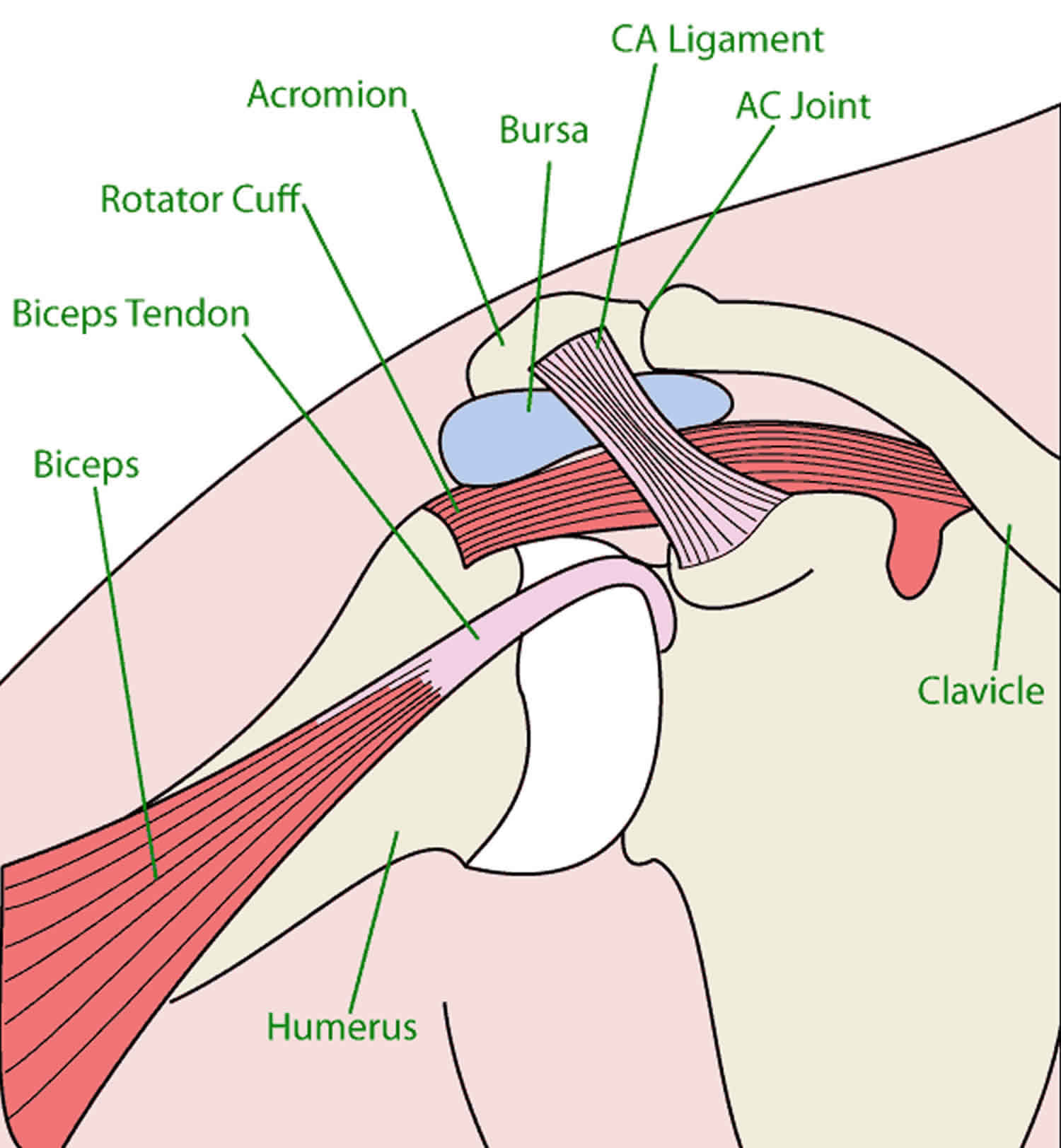
Your shoulder is a complex joint that is capable of more motion than any other joint in your body. It is made up of three bones: your upper arm bone (humerus), your shoulder blade (scapula), and your collarbone (clavicle).
Ball and socket. The head of your upper arm bone fits into a rounded socket in your shoulder blade. This socket is called the glenoid. A slippery tissue called articular cartilage covers the surface of the ball and the socket. It creates a smooth, frictionless surface that helps the bones glide easily across each other.
The glenoid is ringed by strong fibrous cartilage called the labrum. The labrum forms a gasket around the socket, adds stability, and cushions the joint.
Shoulder capsule. The joint is surrounded by bands of tissue called ligaments. They form a capsule that holds the joint together. The undersurface of the capsule is lined by a thin membrane called the synovium. It produces synovial fluid that lubricates the shoulder joint.
Rotator cuff. Four tendons surround the shoulder capsule and help keep your arm bone centered in your shoulder socket. This thick tendon material is called the rotator cuff. The cuff covers the head of the humerus and attaches it to your shoulder blade.
Bursa. There is a lubricating sac called a bursa between the rotator cuff and the bone on top of your shoulder (acromion). The bursa helps the rotator cuff tendons glide smoothly when you move your arm.
Figure 1. Shoulder arthroscopy anatomy
Shoulder arthroscopy operation
Admission
- Most people are admitted to hospital on the day of their surgery.
Anesthesia
The anesthetic team will see you and decide the type of anesthetic that’s best for you.
The different types of anaesthesia include:
- General Anaesthetic. This type of anaesthetic puts you asleep during the whole procedure and a machine controls your breathing.
- Nerve Blocks. This special injection is used to help with your pain after the operation and often used in conjunction with a general anaesthetic.
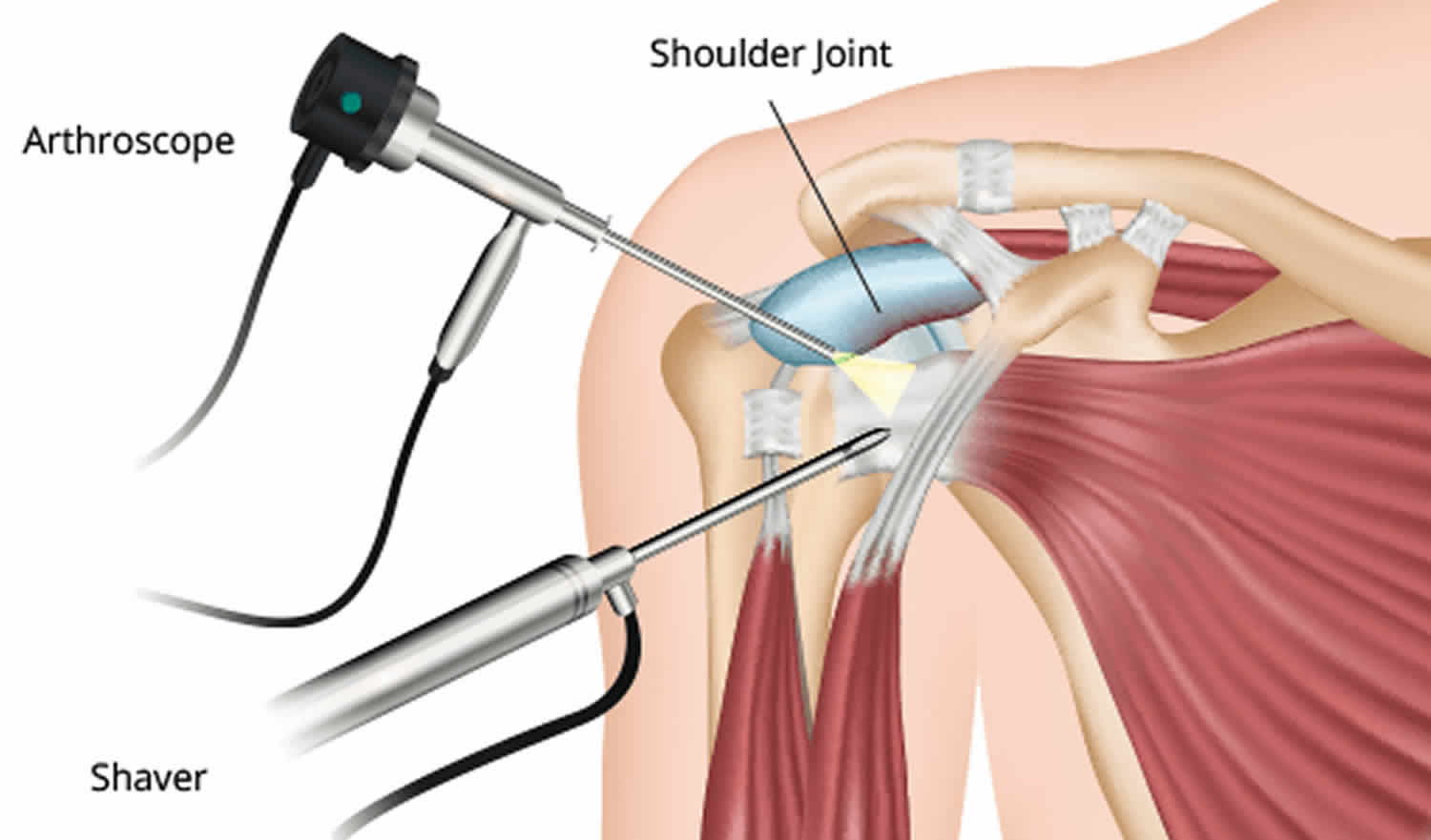
Shoulder arthroscopy procedure
Positioning and Preparation
Once in the operating room, you will be positioned so that your surgeon can easily adjust the arthroscope to have a clear view of the inside of your shoulder. The two most common patient positions for arthroscopic shoulder surgery are:
- Beach chair position. This is a semi-seated position similar to sitting in a reclining chair.
- Lateral decubitius position. In this position the patient lies on his or her side on an operating table.
Each position has some slight advantages. Surgeons select positions based on the procedure being performed, as well as their individual training.
Once you are positioned, the surgical team will remove hair, if needed, and then spread an antiseptic solution over your shoulder to clean the skin. They will cover your shoulder and arm with sterile drapes, and will most likely place your forearm in a holding device to ensure your arm stays still.
Procedure
Your surgeon will first inject fluid into the shoulder to inflate the joint. This makes it easier to see all the structures of your shoulder through the arthroscope. Then your surgeon will make a small puncture in your shoulder (about the size of a buttonhole) for the arthroscope. Fluid flows through the arthroscope to keep the view clear and control any bleeding. Images from the arthroscope are projected on the video screen showing your surgeon the inside of your shoulder and any damage.
Once the problem is clearly identified, your surgeon will insert other small instruments through separate incisions to repair it. Specialized instruments are used for tasks like shaving, cutting, grasping, suture passing, and knot tying. In many cases, special devices are used to anchor stitches into bone.
Your surgeon will:
- Insert the arthroscope into your shoulder through a small incision.
- Inspect all the tissues of your shoulder joint and the area above the joint
cartilage, bones, tendons, and ligaments. - Repair any damaged tissues.
- To do this, your surgeon will make 1 to 3 more small incisions and insert other instruments through them. A tear in a muscle, tendon, or cartilage will be fixed. Damaged tissue may need to be removed.
Your surgeon may do one or more of these procedures during your surgery:
- Rotator cuff repair. The edges of the muscles are brought together. The tendon is attached to the bone with sutures. Small rivets (called suture anchors) are often used to help attach the tendon to the bone. The anchors can be made of metal or plastic. They do not need to be removed after surgery.
- Surgery for bursitis. Damaged or inflamed tissue is cleaned out in the area above the shoulder joint itself. Your surgeon will then shave off the under part of the bone causing irritation of the bursae. This under part of the bone is called the acromion.
- Surgery for shoulder instability. If you have a torn labrum (the rim of the shoulder joint that is made out of cartilage) your surgeon will repair it. Ligaments that attach to this area will also be repaired.
Your surgeon may close your incisions with stitches or steri-strips (small Band-Aids) and cover them with a large, soft bandage.
Shoulder arthroscopy rotator cuff repair
Rotator cuff repair is a type of surgery to fix a torn tendon in the shoulder. Shoulder arthroscopy rotator cuff repair operation is performed to reduce the pain in your shoulder in the long term and improve the strength of your shoulder.
It is also beneficial for people who are engaged in activities that require overhead work, such as swimming, painting, plastering or tennis.
The rotator cuff is a group of muscles and tendons that form a cuff over the shoulder joint. These muscles and tendons hold the arm in its “ball and socket” joint and help the shoulder to rotate. The role of the tendons is to hold the powerful shoulder muscles to the shoulder and arm bones. The tendons can be torn from overuse or injury.
Rotator cuff repair procedure can be done with a large (“open”) incision or with shoulder arthroscopy, which uses small button-hole sized incisions. Most rotator cuff repairs are performed using arthroscopy or ‘key hole surgery’.
Some injuries require that the tendon be reattached directly to a bone in the shoulder, whereas some injuries require the two torn ends of the tendon to be stitched back together. In some instances, when there is only a partial tear in the rotator cuff tendons, the tendons are trimmed down and no major reattachment is necessary.
Not all people who have injured their rotator cuff will require surgery. You may need surgery if you have torn or ruptured your rotator cuff and fit into one of the following categories:
- People suffering from shoulder pain lasting between 6 – 12 months.
- People who have sustained a rotator cuff as a result of trauma – (a fall, sporting injury or a car accident ect).
- People who have rotator cuff tears and have suffered a loss of function or quality of life.
- People who have sustained large tears to their rotator cuff.
Shoulder arthroscopy rotator cuff repair complications
The complication rate following shoulder cuff repair is very low. However like all surgery, there are risks that need to be considered when deciding to have shoulder cuff repair surgery.
Side effects
Side effects are symptoms that occur due to the surgery and are a normal part of the recovery from the operation. The main side effects of rotator cuff repair are:
- A sore shoulder which may last for several weeks after the operation.
- Swelling of the shoulder which may last for several days.
Complications
Complications are problems that occur during or after the operation. Most people having shoulder cuff repair surgery aren’t affected. There are some complications that may occur for any operation. These include:
- A reaction to the anesthetic
- Infection of the wound or joint
- Excessive blood loss
- A blood clot, usually in a vein of the leg (known as a deep vein thrombosis or DVT)
Specific complications of shoulder stabilization arthroscopy are very uncommon, but can include the following:
- Re-ruptures: The tendon that is being fixed may tear again after the operation. This occurs in roughly 10% of people having the operation. It is important that you follow the surgeons advice in order to make sure the chance of this happening is minimized.
- Shoulder stiffness: Occasionally your shoulder may be stiff after this operation. It is important to complete the physiotherapy exercises in order to avoid this.
- Damage to nerves: This occurs very rarely in less than 1% of cases. Damage to nerves can lead to an area of numbness over the shoulder or a weak muscle.
Shoulder arthroscopy rotator cuff repair recovery and rehabilitation
For the first 4-6 weeks after the operation, the arm needs to be in a sling to protect it from regular use. During this time, a physiotherapist can outline appropriate exercises that encourage increasing the range of motion of the shoulder. It is important to follow the advice of your surgeon and physiotherapist as your shoulder is vulnerable to re-injury in the first 6 weeks following the operation.
After 6 weeks, exercises that promote strengthening of the muscles around the shoulder are encouraged. Your physiotherapist will give you an exercise program in order to help build up the strength in the shoulder.
It is important to complete the required physiotherapy exercises in order to get the best outcome after the operation.
If you participate in competitive sport it may take 6 months to return to these activities.
Shoulder arthroscopic shoulder stabilization
An arthroscopic shoulder stabilization is a procedure whereby small cuts are made around the shoulder in order to place a camera and specialized instruments inside the shoulder joint. Surgeons use these special instruments to tighten the shoulder joint, to make it less prone to dislocating in the future.
Shoulder arthroscopic shoulder stabilization operation aims to improve the pain for people suffering with shoulder instability. It should also improve the feeling of shoulder looseness that these people get.
An arthroscopic shoulder stabilization procedure is for people with:
- Shoulder instability: This means that the shoulder is too loose and may pop out or dislocate even when performing normal tasks. In some cases, the shoulder is not loose enough to dislocate but may move too far and almost dislocate. This is known as a subluxation. An unstable shoulder is often very painful and more prone to wearing out.
- Shoulder dislocation: If you have dislocated your shoulder you may have torn cartilage or ligaments surrounding the shoulder joint which will need to be repaired.
The shoulder is a very mobile joint. It consists of a ball (from the long arm bone, the humerus) and a socket (formed out of the shoulder blade). Whilst it is able to move freely in every direction, this does make it vulnerable to ‘pop out of place’, or dislocate. In healthy shoulder joints, there are soft-tissue structures, such as ligaments, tendons and muscles, that help hold the ball inside the socket.
For various reasons, the soft tissue supporting structures of the shoulder can become damaged. This may be due to dislocating the shoulder (e.g.. on the football field), or it may be due to more long term damage. Once these structures are damaged, the shoulder is more likely to dislocate.
Shoulder arthroscopic shoulder stabilization complications
The complication rate following shoulder stabilisation arthroscopy is very low. However like all surgery, there are risks that need to be considered when deciding to have shoulder stabilisation arthroscopy surgery.
Side effects
Side effects are symptoms that occur due to the surgery and are a normal part of the recovery from the operation. The main side effects of shoulder stabilization arthroscopy are:
- A sore shoulder which may last for several weeks after the operation.
- Swelling of the shoulder which may last for several days.
Complications
Complications are problems that occur during or after the operation. Most people having knee arthroscopy surgery aren’t affected. There are some complications that may occur for any operation. These include:
- A reaction to the anesthetic
- Infection of the wound or joint
- Excessive blood loss
- A blood clot, usually in a vein of the leg (known as a deep vein thrombosis or DVT)
Specific complications of shoulder stabilization arthroscopy are very uncommon, but can include the following:
- Shoulder stiffness: Occasionally you shoulder may be stiff after this operation. It is important to complete the physiotherapy exercises
- Damage to nerves: This occurs very rarely in roughly 0.3% of cases.
- Re-dislocation: After the operation, you shoulder may dislocate again. This is a rare complication occuring in roughly 0.4% of cases.
Shoulder arthroscopic shoulder stabilization recovery and rehabilitation
For the first 4-6 weeks after the operation, the arm needs to be in a sling to protect it from regular use. During this time, a physiotherapist can outline appropriate exercises that encourage increasing the range of motion of the shoulder. It is important to follow the advice of your surgeon and physiotherapist as your shoulder is vulnerable to re-injury in the first 6 weeks following the operation.
After 6 weeks, exercises that promote strengthening of the muscles around the shoulder are encouraged. Your physiotherapist will give you an exercise program in order to help build up the strength in the shoulder.
It is important to complete the required physiotherapy exercises in order to get the best outcome after the operation.
If you participate in competitive sport it may take 6 months to return to these activities.
Shoulder arthroscopy for subacromial decompression
Subacromial decompression, also known as anterior acromioplasty, is an operation that involves removing a small section of bone from the shoulder. The aim of the procedure is to increase the space for the rotator cuff tendons to glide. The main benefit of the surgery is that it should improve the pain associated with shoulder impingement.
Risks of not having the subacromial decompression surgery:
- Continued pain
- Progression to rotator cuff tears
Subacromial decompression is performed for patients suffering from shoulder impingement, who haven’t responded to conservative management.
Shoulder impingement is a condition whereby the tendons of the rotator cuff don’t have enough room to freely glide within the shoulder. At the shoulder, the rotator cuff tendons travel through a rigid arcade made of bone. Sufferers of shoulder impingement have an arcade that is too small for their rotator cuff tendons, so they experience pain, stiffness and/or weakness when they use the affected shoulder. In other words, it is due to the bones in the shoulder ‘impinging’ on the rotator cuff tendons.
Shoulder impingement can affect young people and older people alike, especially those who are involved in sports demanding repetitive overhead work.
Subacromial decompression is generally performed arthroscopically – that is, small incisions are made around the shoulder to allow access for a camera and specialized surgical instruments. This is otherwise known as keyhole, or minimally invasive, surgery.
Shoulder arthroscopy for subacromial decompression complications
The incisions made for subacromial decompression are very small, so complications are uncommon.
As with any surgery, there are some risks, which include:
- Problems with anesthetic
- Shoulder stiffness
- Injury to nerves: The musculocutaneous and axillary nerves are most at risk in this procedure. Injury to these nerves may cause pain or loss of sensation in the shoulder or forearm, or weakness of part of the arm. Injury to these nerves are uncommon, and the effects are often temporary, though they may be permanent.
- Injury to bone: rarely too much bone is removed from the shoulder
- Injury to the soft tissues in and around the shoulder joint: This may result in pain or instability in the joint. Again, the risk of this occurring is low.
- Infection: With any surgical procedure, infection is a risk. However, with the small incisions made with shoulder arthroscopy, infections are very rare.
- Damage to blood vessels: This is a very rare complication.
Shoulder arthroscopy for subacromial decompression recovery and rehabilitation
You will be encouraged to start using the affected shoulder from day 1 after the operation. These will involve passive and active assisted exercises that will have you moving your shoulder in different planes.
The aim is for you to have full range of motion in your shoulder by 6 weeks. After this, you will be encouraged to do shoulder strengthening exercises, leading up to repetitive overhead exercises 3 months after the operation.
Shoulder arthroscopy complications
The complication rate following shoulder arthroscopy is very low. However like all surgery, there are risks that need to be considered when deciding to have the operation.
Side effects
Side effects are symptoms that occur after every operation and are a normal part of the recovery from the operation. The main side effects of shoulder arthroscopy are:
- A sore shoulder which may last for several weeks after the operation
- Swelling in the upper arm which will also last for several weeks after the operation
Complications
Complications are uncommon problems that occur during or after the operation. Most people having a shoulder arthroscopy aren’t affected.
The general complications for all operations are:
- A reaction to the anesthetic
- Infection of the wound or joint
- Excessive blood loss
Specific complications of shoulder arthroscopy are:
- Shoulder stiffness
- Failure of the surgery to relieve symptoms
- Injury to nerves: this may leave the shoulder weak or an area of skin over the shoulder numb. This is a very rare complication.
- Injury to the cartilage inside the shoulder joint: This may result in pain or instability in the joint. Again, the risk of this occurring is low.
Shoulder arthroscopy recovery
After the operation, you are cared for in the theater recovery room. You will usually only spend 1-2 hours in the recovery room.
Most people wake up fully when back in their rooms on the ward. Whilst on the ward, the nurses will take care of your every need. It usually takes a few hours to recover fully from the anesthetic, and the nurse with regularly check on your recovery.
Most people go home after one night at the hospital.
Most people go home with a sling after this operation. If you had a rotator cuff repair or labrum repair you may have to wear a sling for up to 6 weeks after the operation.
If you only had the bursa cleaned up and the bone spur shaved, you may not need a sling after a few days.
Although recovery from arthroscopy is often faster than recovery from open surgery, it may still take weeks for your shoulder joint to completely recover.
What to expect at home
You will need to wear a sling when you leave the hospital. You may also need to wear a shoulder immobilizer. This keeps your shoulder from moving. Wear the sling or immobilizer at all times, unless your surgeon says you do not have to.
Although it does not affect how your shoulder heals, lying flat may pull on your shoulder and cause discomfort. Some patients are more comfortable sleeping in a reclining chair or propped up in bed during the first days after surgery.
Pain
You can expect some pain and discomfort for at least a week after surgery. If you have had a more extensive surgery, however, it may take several weeks before your pain subsides. Ice will help relieve pain and swelling. Your doctor may prescribe pain medicine, if needed.
Many types of pain medication are available to help control pain, including opioids, nonsteroidal anti-inflammatory drugs (NSAIDs) and local anesthetics. Treating pain with medications can help you feel more comfortable, which will help your body heal faster and recover from surgery faster.
Your doctor will usually give you a prescription for pain medicines. Get it filled when you go home so you have it when you need it. Take the pain medicine when you start having pain so it doesn’t get too bad.
Narcotic pain medicine (codeine, hydrocodone, and oxycodone) can make you constipated and can be addictive. It is important to use opioids only as directed by your doctor. You should stop taking these medications as soon as your pain starts to improve. If you are taking them, drink plenty of fluids and eat fruits and vegetables and other high-fiber foods to help keep your stools loose.
DO NOT drink alcohol or drive if you are taking these pain medicines.
Taking ibuprofen (Advil, Motrin) or other anti-inflammatory medicines with your prescription pain medicine may help also. Ask your doctor about using them. Follow instructions exactly on how to take your medicines.
Wound Care
Place ice packs on the dressing (bandage) over your wound (incision) 4 to 6 times a day for about 20 minutes each time. Wrap the ice packs in a clean towel or cloth. DO NOT place it directly on the dressing. Ice helps keep swelling down.
Your sutures (stitches) will be removed about 1 to 2 weeks after surgery.
Keep your bandage and your wound clean and dry. Ask your doctor if it is OK to change the dressing. Keeping a gauze pad under your arm may help absorb sweat and keep your underarm skin from getting irritated or sore. DO NOT place any lotion or ointment on your incision.
You will most likely need a sling or special immobilizer to protect your shoulder. Your surgeon will discuss with you how long the sling will be needed.
Check with your doctor about when you can start taking showers if you have a sling or shoulder immobilizer. Take sponge baths until you can shower. When you do shower:
- Place a waterproof bandage or plastic wrap over the wound to keep it dry.
- When you can shower without covering the wound, do not scrub it. Gently wash your wound.
- Be careful to keep your arm by your side. To clean under this arm, lean to the side, and let it hang down away from your body. Reach under it with your other arm to clean under it. DO NOT raise it as you clean it.
- DO NOT soak the wound in a bath tub, hot tub, or swimming pool.
Follow-up
You will probably see the surgeon every 4 to 6 weeks until you are recovered.
Call the surgeon or nurse if you have any of the following:
- Bleeding that soaks through your dressing and does not stop when you place pressure over the area
- Pain that does not go away when you take your pain medicine
- Swelling in your arm
- Numbness or tingling in your fingers or hand
- Your hand or fingers are darker in color or feel cool to the touch
- Redness, pain, swelling, or a yellowish discharge from any of the wounds
- Temperature higher than 101°F (38.3°C)
Activity
If you had rotator cuff or other ligament or labral surgery, you need to be careful with your shoulder. Follow instructions on what arm movements are safe.
Consider making some changes around your home so it is easier for you to take care of yourself.
Keep doing the exercises you were taught for as long as you were told. This helps strengthen the muscles that support your shoulder and ensures it heals well.
You may not be able to drive for a few weeks. Your doctor or physical therapist will tell you when it is OK.
Ask your doctor about which sports and other activities are OK for you after you recover.
Shoulder arthroscopy recovery time
Back to work and sport
If you work in an office environment, you should be able to return to work within a week of the operation.
The time to return to sport or heavy manual work varies depending on what structures were repaired.
If you had a bursae cleaned up and a spur removed, you should be able to get back to most activities within 4 weeks of the operation.
If you had a rotator cuff repair or a labrum repair, it may take 3 months to return to most activities.
Shoulder arthroscopy rehab protocol
Shoulder arthroscopy rehabilitation program varies depending on what was operated on during the arthroscopy.
Rehabilitation plays an important role in getting you back to your daily activities. An exercise program will help you regain shoulder strength and motion. Your surgeon will develop a rehabilitation plan based on the surgical procedures you required.
If you have had a more complicated surgical repair, your surgeon may recommend a physical therapist to supervise your exercise program.
It is important that you make a strong effort at rehabilitation in order for your surgery to succeed.
Your physiotherapist will give you exercises to help to improve the flexibility and strength of the shoulder. It is important to follow the advise of the physio and make sure that you complete the recommended exercises in order to get the best outcome from the operation.
Shoulder arthroscopy long-term outcomes
Because patients have varied health conditions, complete recovery time is different for everyone.
If you have had a minor repair, you may not need a sling and your strength may return after a short period of rehabilitation. You may be able to return to work or school within a few days of your procedure.
It takes longer to recover from more complicated procedures. Although the incisions are small in arthroscopy, extensive damage within the joint can be repaired with the procedure. Full recovery may take several months. Although it can be a slow process, following your surgeon’s guidelines and rehabilitation plan is vital to a successful outcome.




{kind=link}